Dr. Conrad L. Pirani
|
|
|
- Edwin Watts
- 6 years ago
- Views:
Transcription

1 Dr. Conrad L. Pirani

2 Dr. Jacob Churg
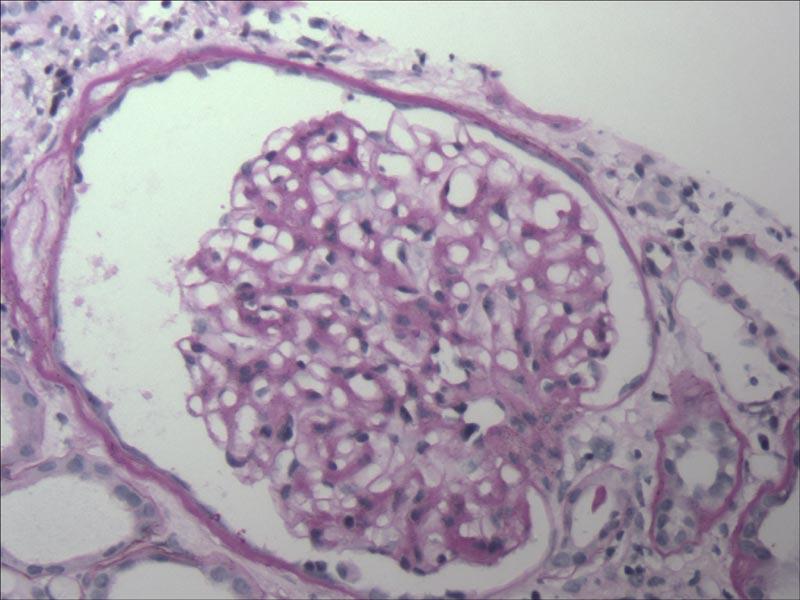
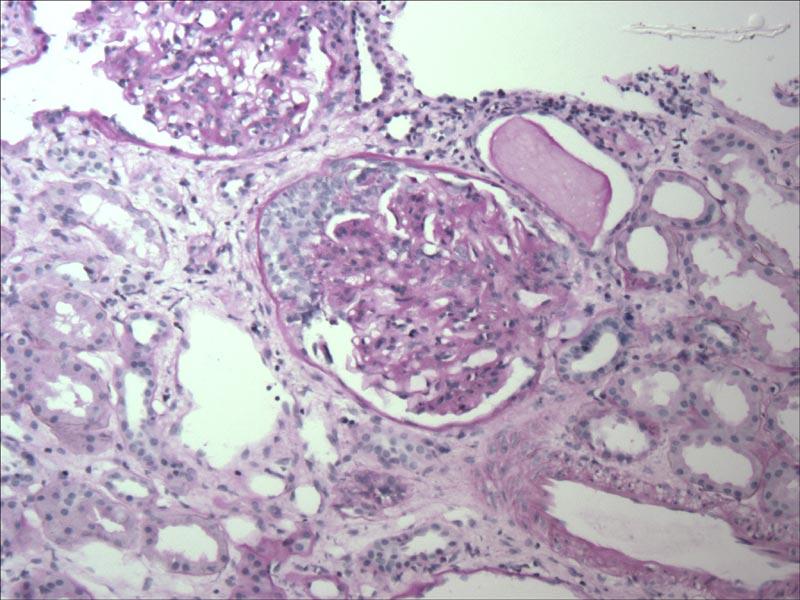
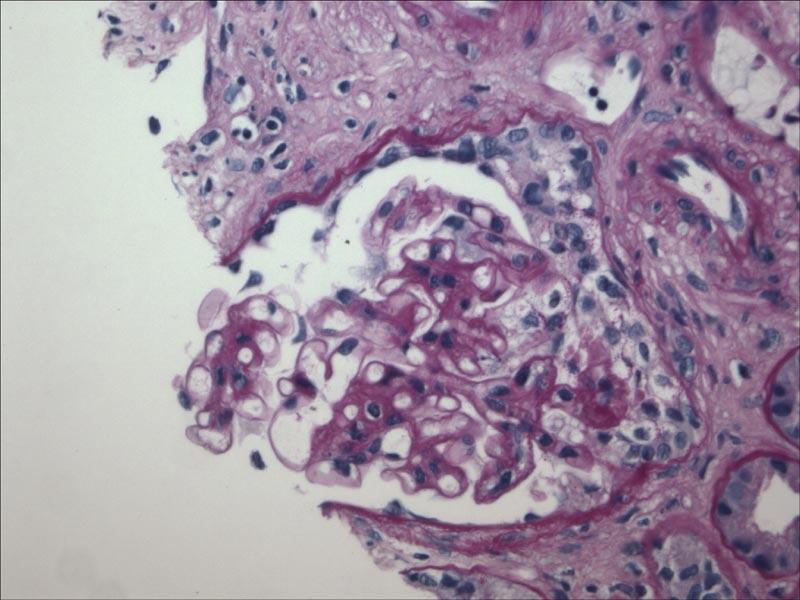
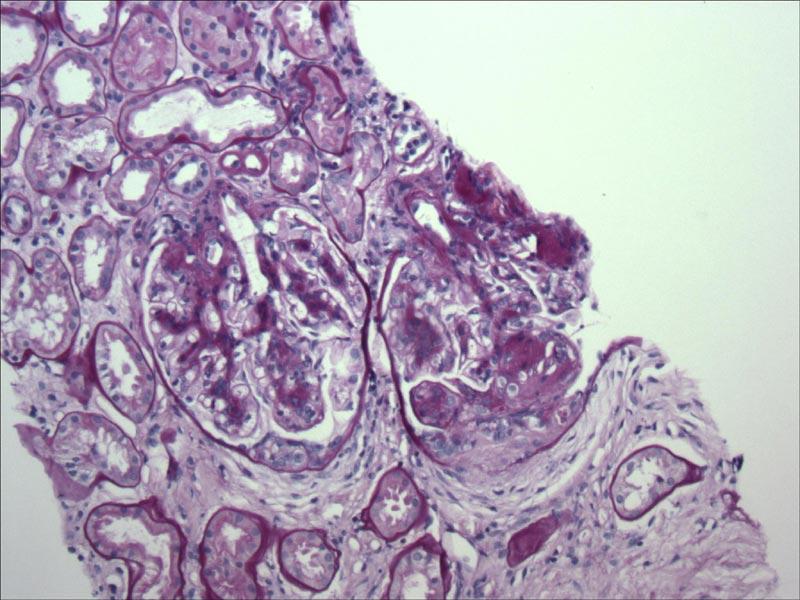
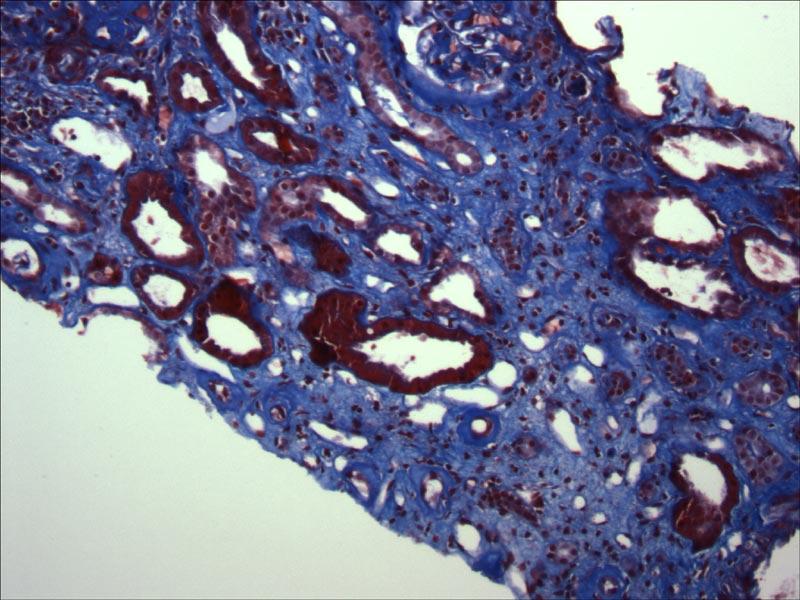
3 CLINICAL HISTORY This 52 year old African American female factory worker was admitted most recently with chest pain/midsternal pressure for one day PTA (10/04). 1.) Past Med Hx: DM type 2 (for a couple of years, most recently started on insulin); uncontrolled hypertension ( / ), and hypothyroidism; eye grounds said to be normal 2.) PE: bipedal edema/ekg and labs: no evidence of MI 3.) Labs: BUN/serum Cr: 8/0.9 (on 7/04), and on this admission and next few days (10/25-11/10, 2004) was 26-39/ ; 4+ proteinuria; remainder normal or negative 4.) Renal Biopsy: (11/09/04) New onset of renal failure and nephrotic syndrome (?thought to be too short a duration of DM as a cause). Other lab tests ordered.
4 BX Nov 9 '04 Oct 30 '04 Oct 31 '04 Oct 28 '04 Oct 24 & 25 '04 Aug 11 '04 July '04 June '04 Jan 12 '04 May 8 '03 Mar 31 '03 Serum Cr 1/Serum Cr
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25 IgGI
26 IgA
27 IgM
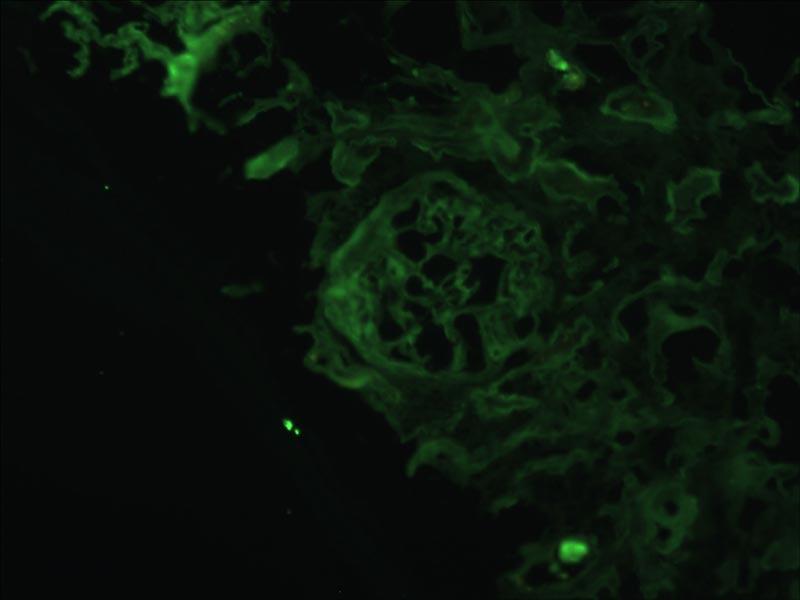
28 kappa
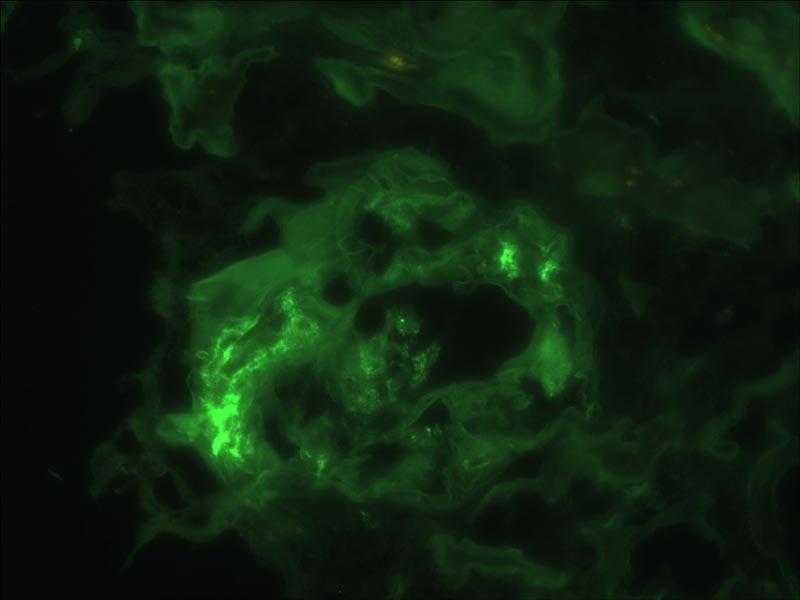
29 lambda
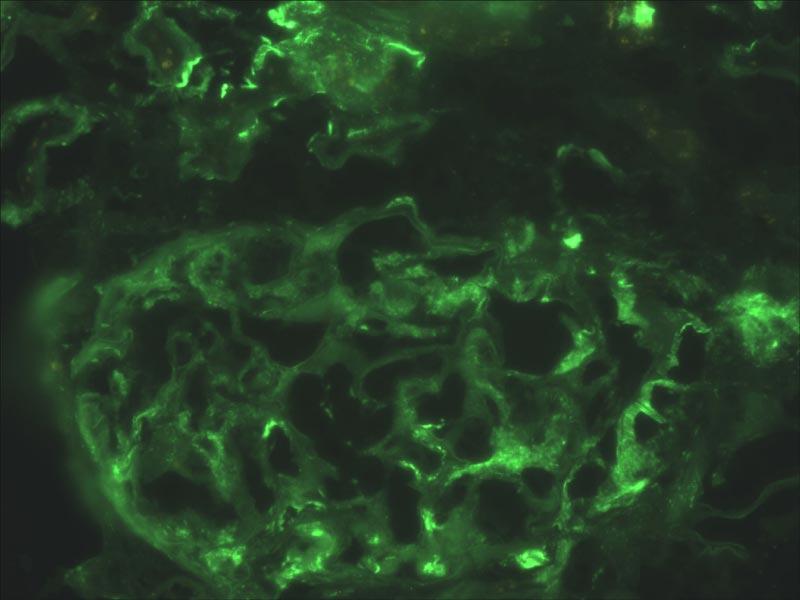
30 C3
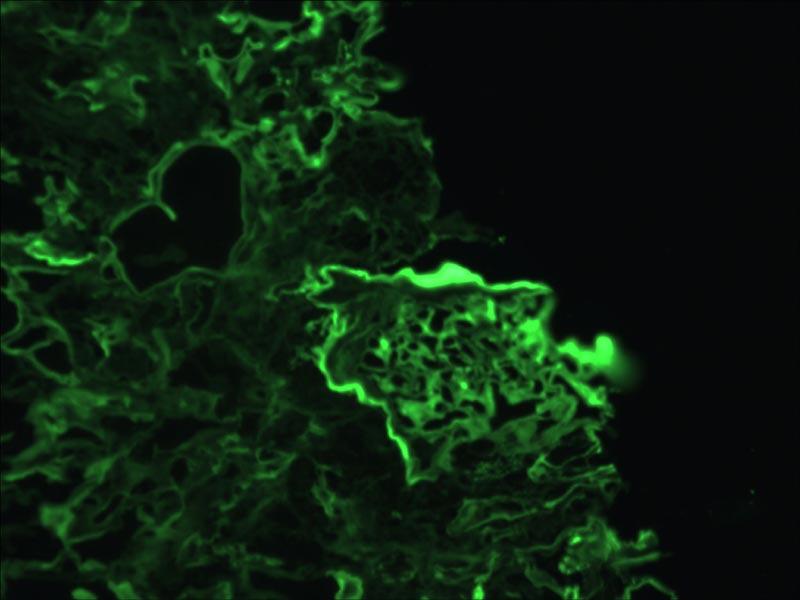
31 ALBUMIN
32 FIBRINOGEN
33 WHY BIOPSY DIABETIC PATIENTS? Most diabetic patients not biopsied at this time Only biopsied if the clinical/laboratory course not typical: e.g., Rapid onset of severe proteinuria Rapid development of acute or chronic renal failure Atypical findings: hematuria, normal fundoscopic exam, etc.
34 Biopsy of a Diabetic Patient Step 1 Is it Diabetic Nephropathy?
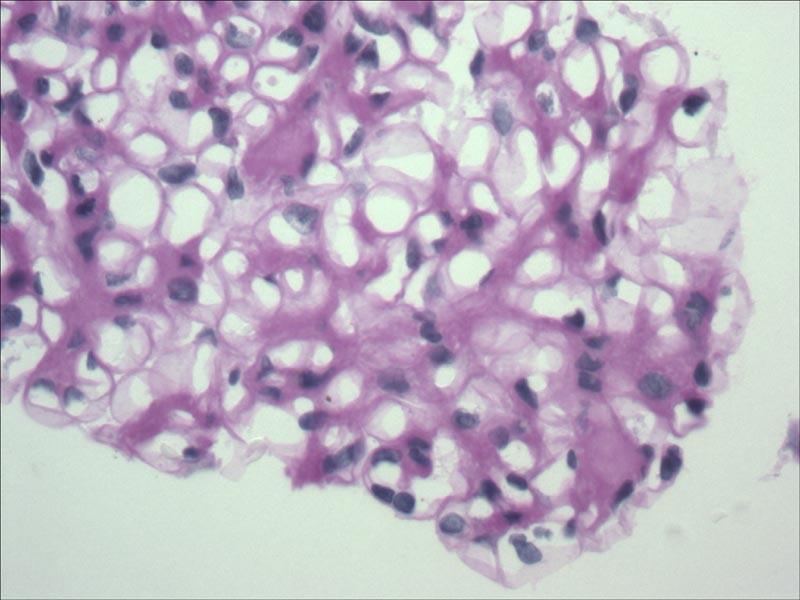
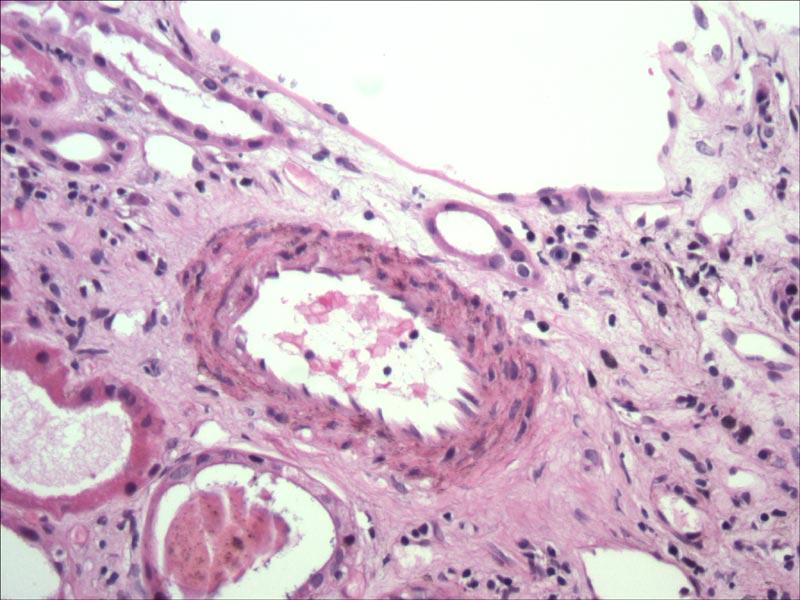
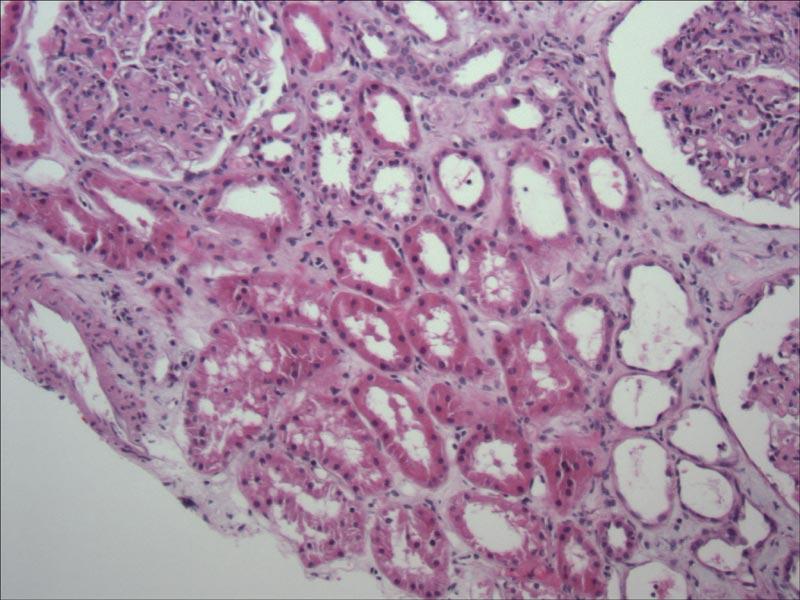
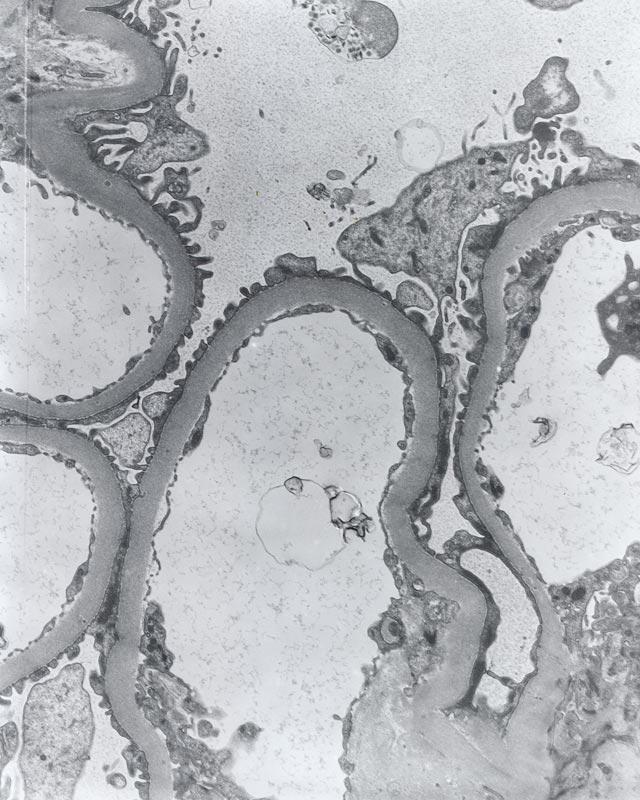
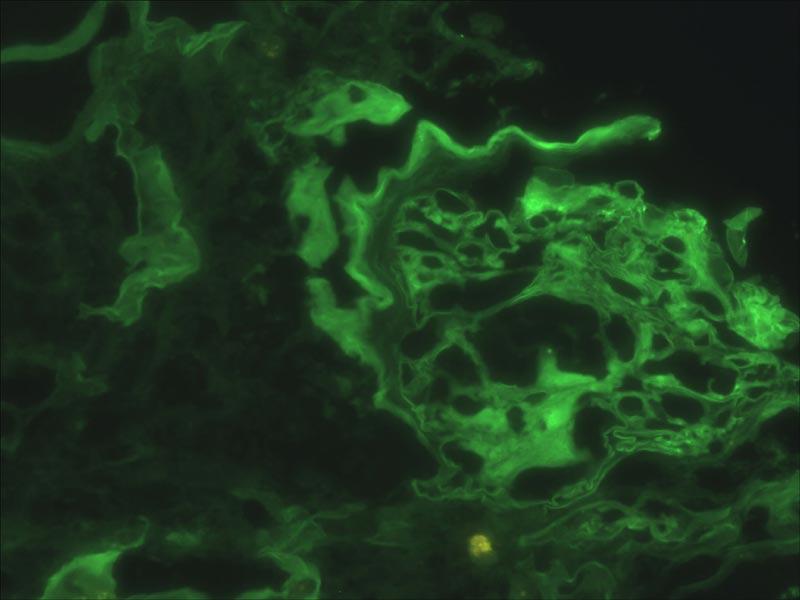
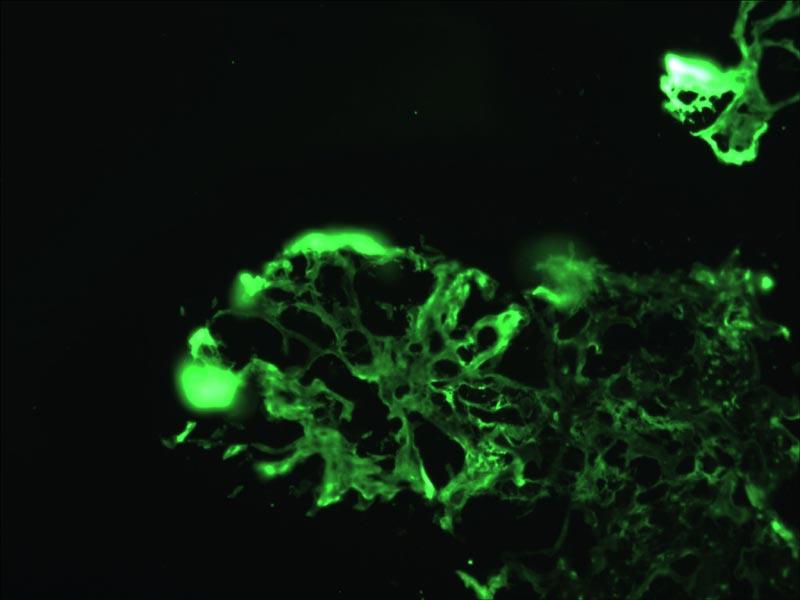
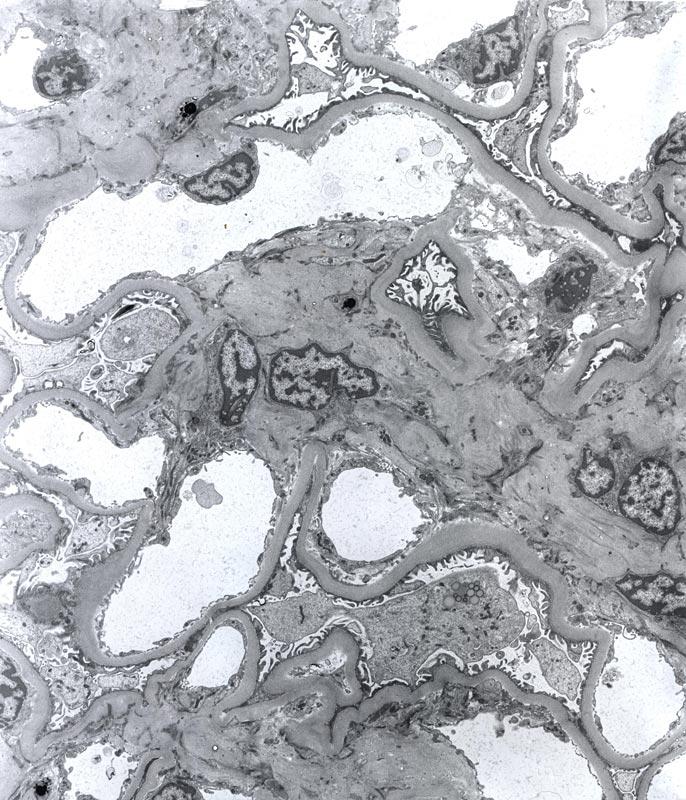
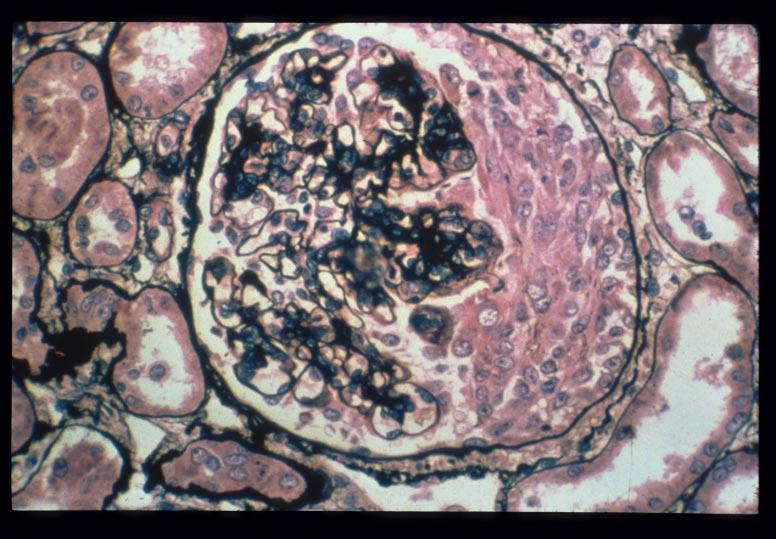
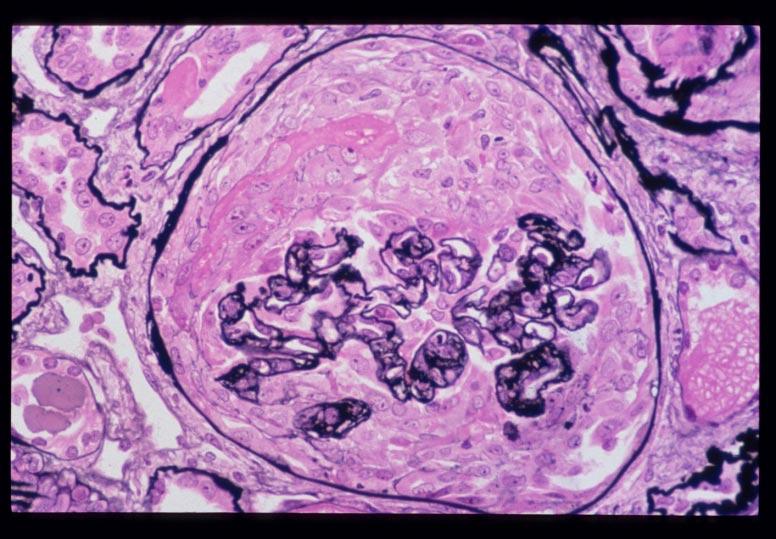
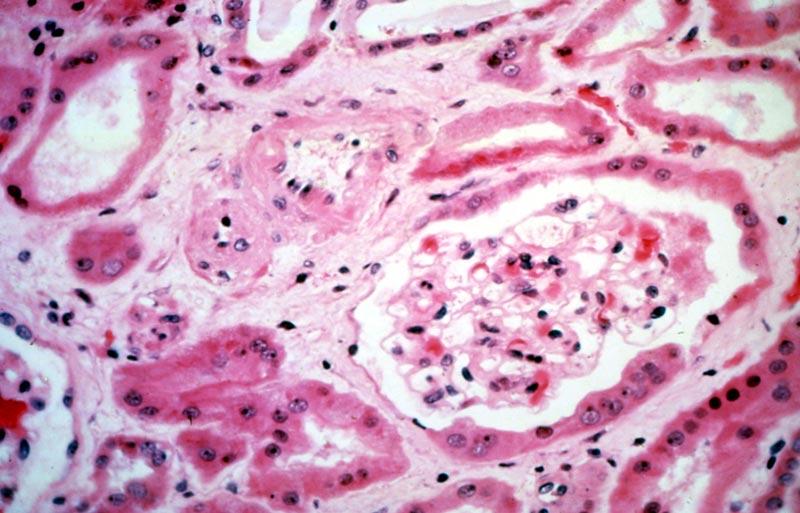
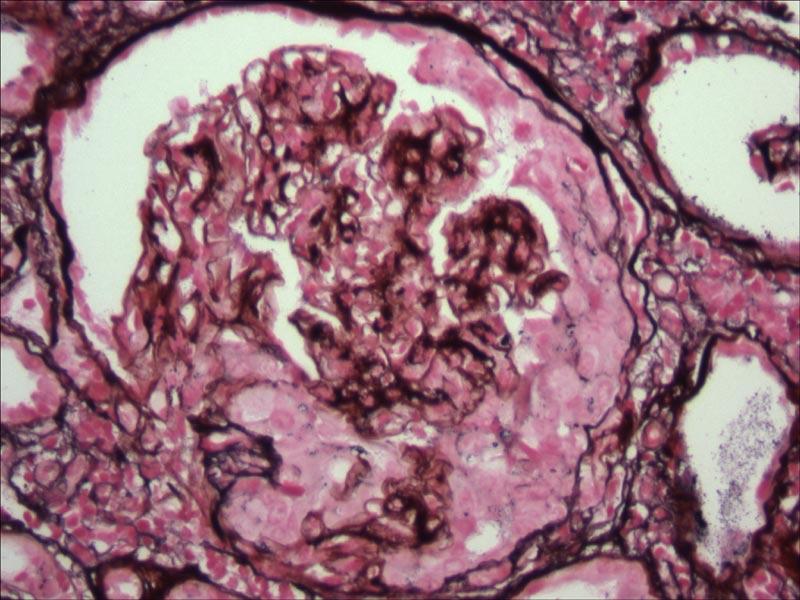
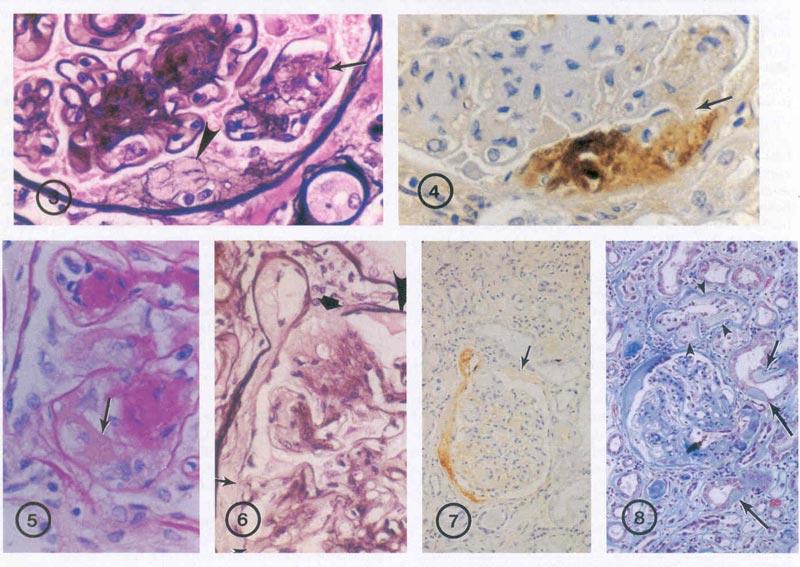
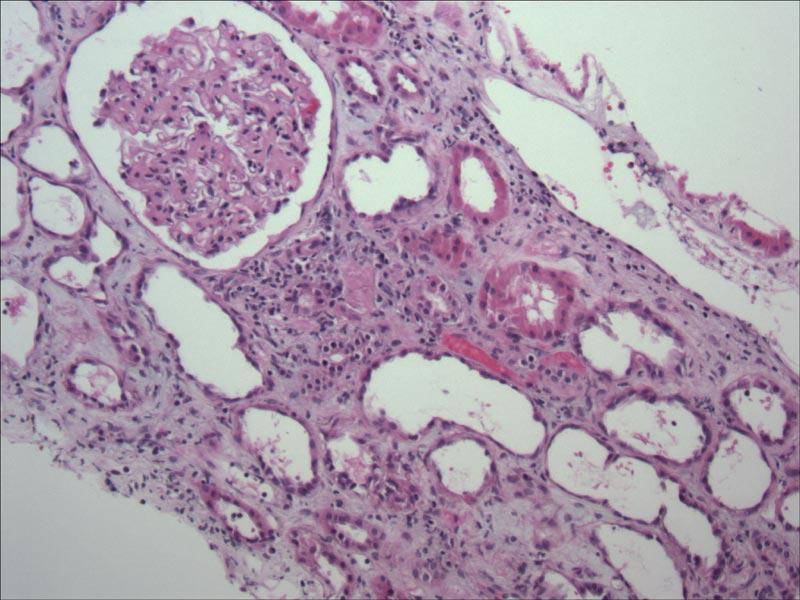
35 DIABETES MELLITUS: PATHOLOGIC CHANGES Early: Large kidneys/glomeruli; increased GFR Microalbuminemia Advancing: 1.) Diffuse Diabetic Glomerulosclerosis 2.) Nodular Diabetic Glomerulosclerosis 3.)Insudative Changes (Fibrin caps; capsular drops; hyaline arteriolosclerosis) 4.) Linear GBM and TBM staining (IgG4; albumin)
36
37
38
39
40 Biopsy of a Diabetic Patient Step 1 Is it Diabetic Nephropathy Step 2 No Yes
41 RENAL BIOPSY IN PROTEINURIC TYPE 2 DIABETICS (Parving et al) 1.) Three-fourths: Typical diabetic nephropathy 2.) One-fourth: Variety of non-diabetic lesions including MCNS, GN, mixed diabetic-gn lesions.
42 RENAL BIOPSY IN DIABETICS (Gambara et al) 1/3: Changes typical of diabetic nephropathy 1/3: Marked increase in the percentage of globally sclerosed glomeruli associated with severe tubulointerstitial lesions, whereas non-sclerosed glomeruli showed only mild diabetic changes 1/3: Changes typical of diabetic nephropathy with superimposed changes of proliferative GN, Membranous GN, and other superimposed diseases
43
44 DIABETES AND OTHER SUPERIMPOSED NON-DIABETIC RENAL CONDITIONS Acute proliferative GN Cryoglobulinemic GN Crescentic GN (-/+ ANCA) MPGN I and II (DDD) and III IgA Nephropathy and HSP (-/+ Crescents/ANCA) Membranous GN (-/+ Amyloid) (including Focal/segmental MGN) Minimal Change Nephrotic Syndrome Focal Segmental Glomerulosclerosis SLE (Class IV) Amyloidosis Mesangial Proliferative GN Sarcoidosis Immune Complex Diseases: Focal GN, OSS and Incidental Healed Postinfectious GN Anti-GBM Disease (Crescentic) Churg-Strauss (Crescentic) Fibrillary GN/Immunotactoid GN Monoclonal Immunoglobulin deposition disease & Heavy (Immunoglobulin) Chain Nodular Glomerulosclerosis Microscopic polyangitis Tubulointerstitial Nephritis/Chronic Pyelonephritis Pre-eclampsia
45 DUAL GLOMERULONEPHROPATHIES: A Partial List SLE & Amyloid Membranous GN & Amyloid Membranous GN & Anti-GBM MCNS & Focal segmental Membranous GN Hereditary Nephropathy & Focal Seg. MGN Hereditary Nephropathy & Dense Dep. Dis. Hereditary Nephropathy & SLE Crescentic GN & Membranous GN ICD & anti-gbm Focal segmental MGN & MCNS Focal segmental MGN & Hereditary Nephropathy
46 DUAL GLOMERULOPATHIES? THE SAME DISEASE OR TWO DIFFERENT DISEASES? IgA Nephropathy (with Minimal Change Nephrotic Syndrome) IgA Nephropathy (with Membranous GN pattern) Focal Segmental Sclerosis in Diabetic Nephropathy, or Membranous GN, or Hypertension Others
47 BIOPSY OF DIABETICS Author % Diabetic % Other Nephropathy Gambara ~ 33% ~ 33% DN + ~ 33% nephrosclerosis Zukowska- 78% (European) 22% (Meta Analysis) 73% (Asian) 27% Tone 36% 17% DN + 48% Other Parving ~ 75% ~ 25 % Ruggenenti 46% 19% (35% Nephroscl.) Suzuki 73% 27% Mazzucco 29% and 51% 33% and 57% (2 Protocols) Castellano 45% 55%
48 BIOPSY OF DIABETICS Author %Diabetic %Other Nephropathy Serra 74% 9% DN+ 17% Other Hironaka 71% 29% DN + (1/2 DN also) Richards 86% (I) 9% DN+/4% Not DN 50% (II) 48% Not DN Waldherr 2% ICD Amoah 88% (1) 12% (1) ±DN 72% (2) 28% (2) ±DN Hommel 31% 69% ±DN (Hematuria) Yum 56% 44%
49
50 TRIPLE RENAL DISEASES: A PARTIAL LISTING INCLUDING DIABETIC NEPHROPATHY IgA Nephropathy/Crescentic/ANCA (Lai) Amyloid, Membranous GN (Bertani/Pirani)
51 Biopsy of a Diabetic Patient Step 1 Is it Diabetic Nephropathy Step 2 No Yes Step 3 Then What? That s all DM Plus (Dual Disease) A B C Etc
52
53
54
55
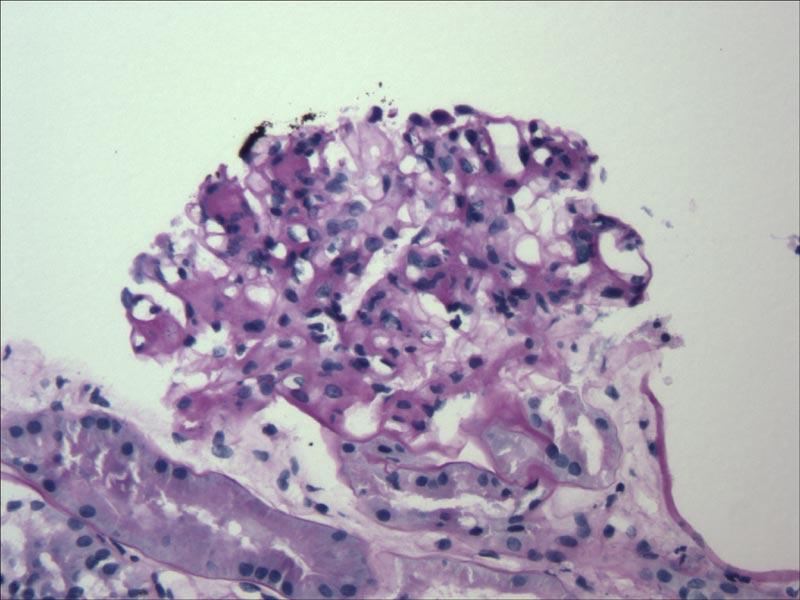
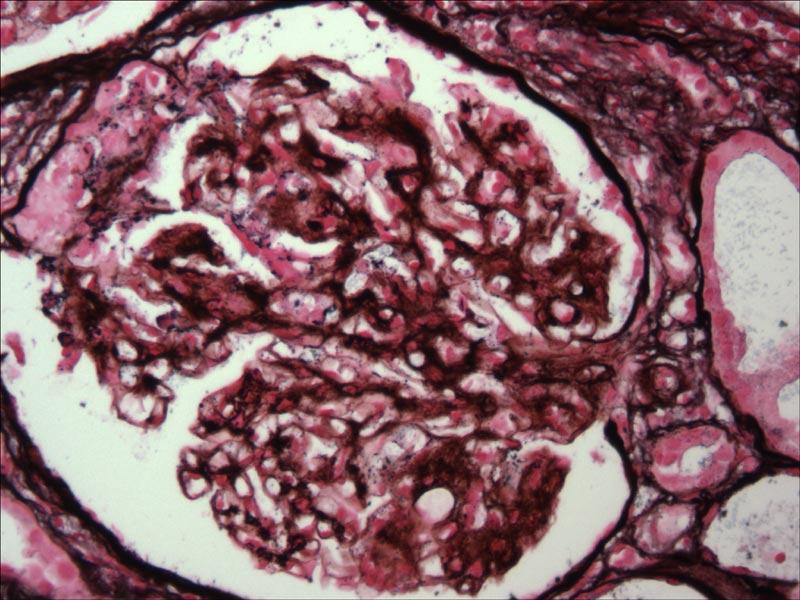
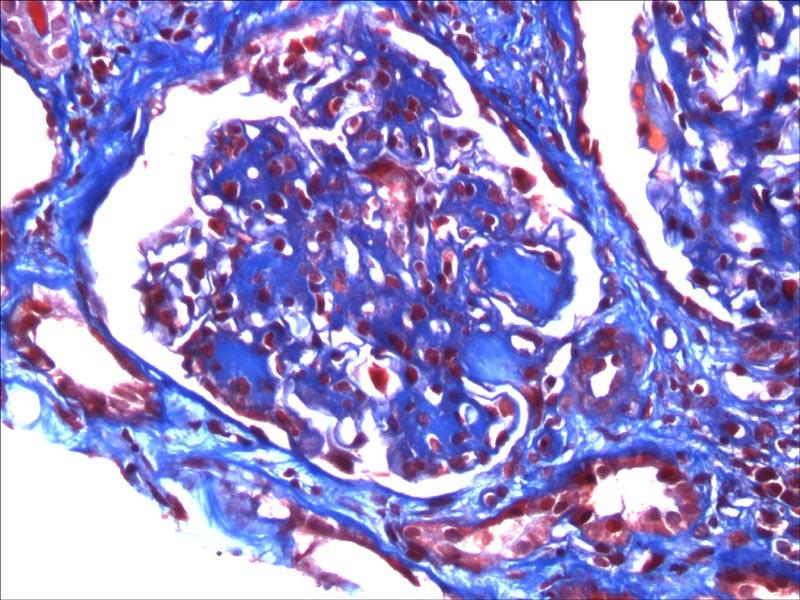
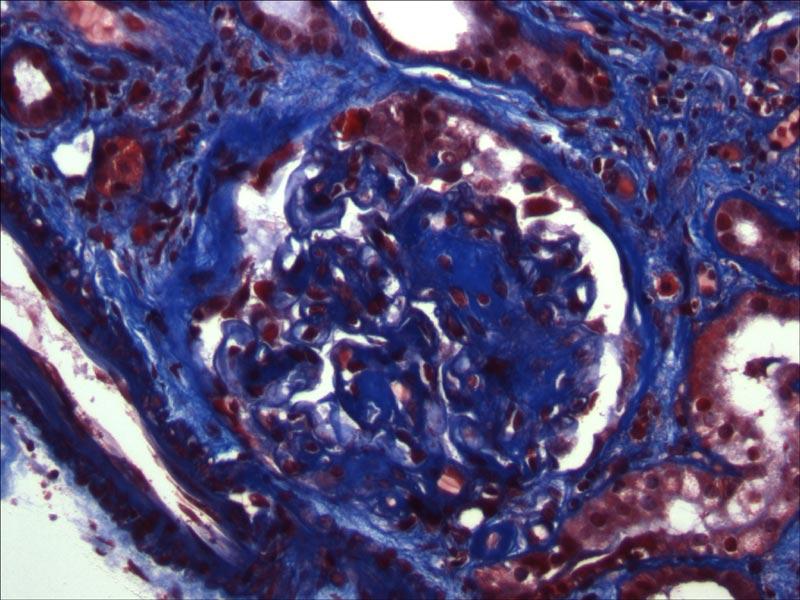
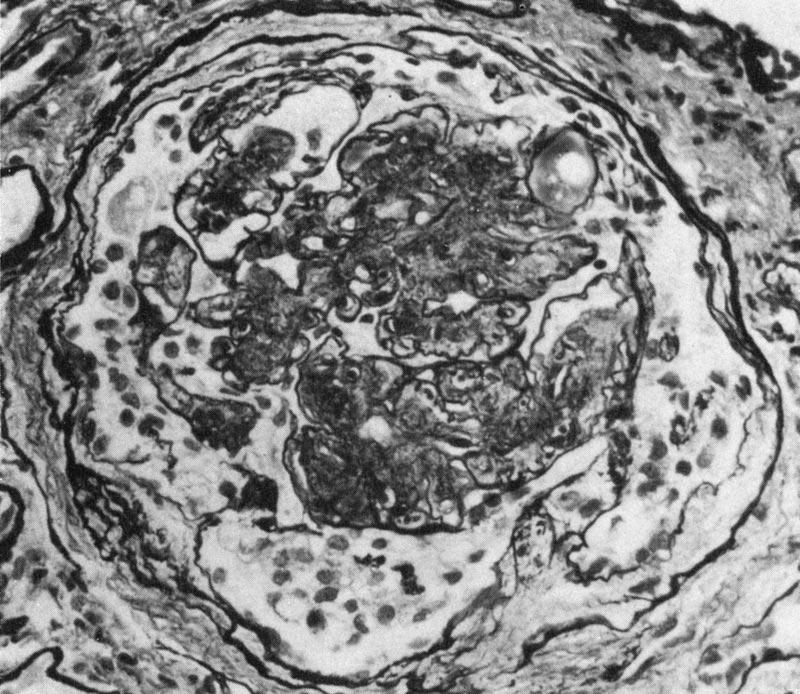
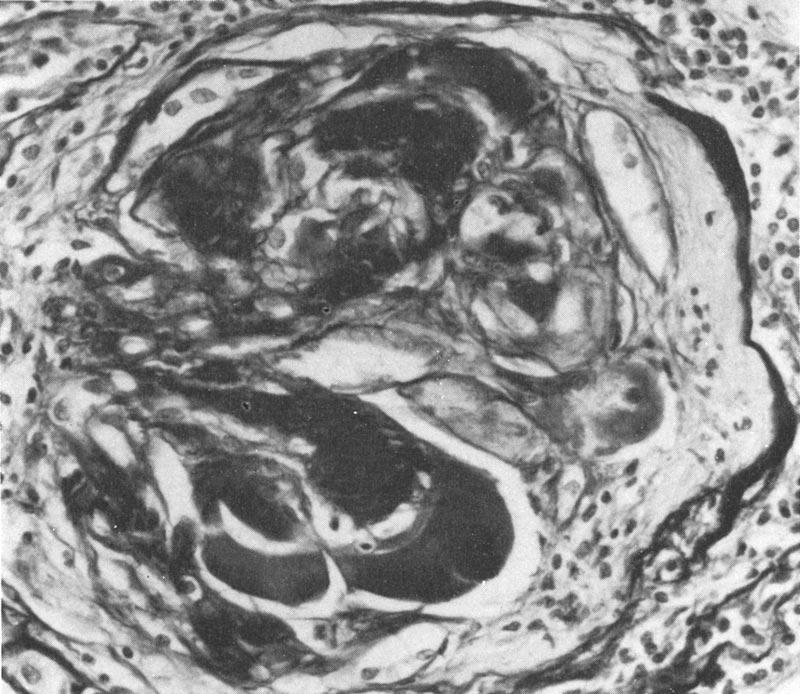
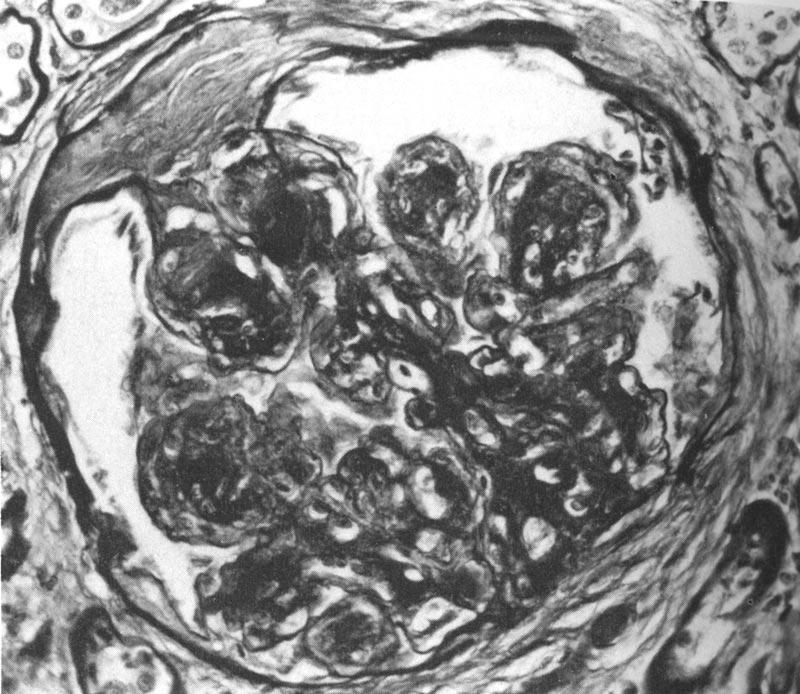
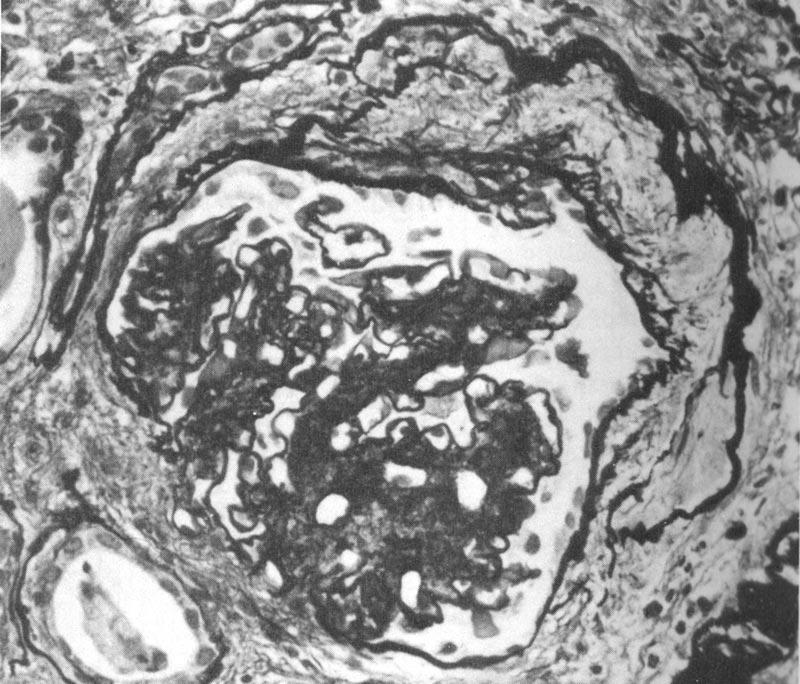
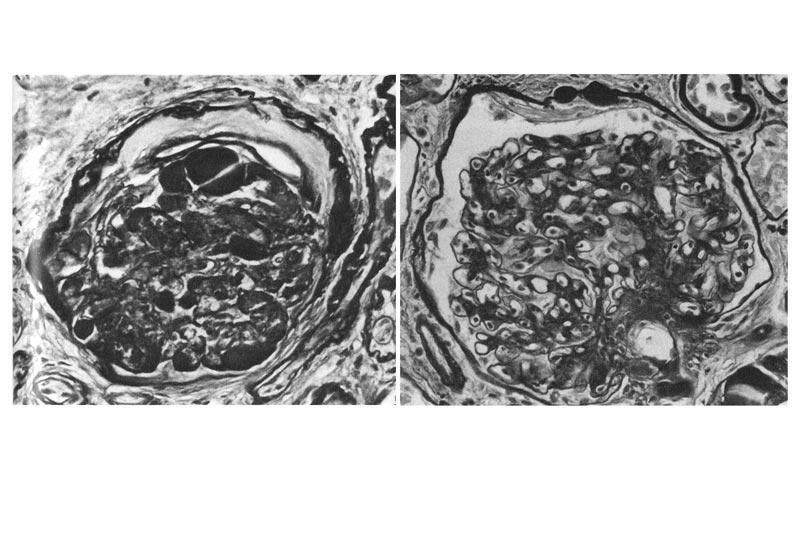
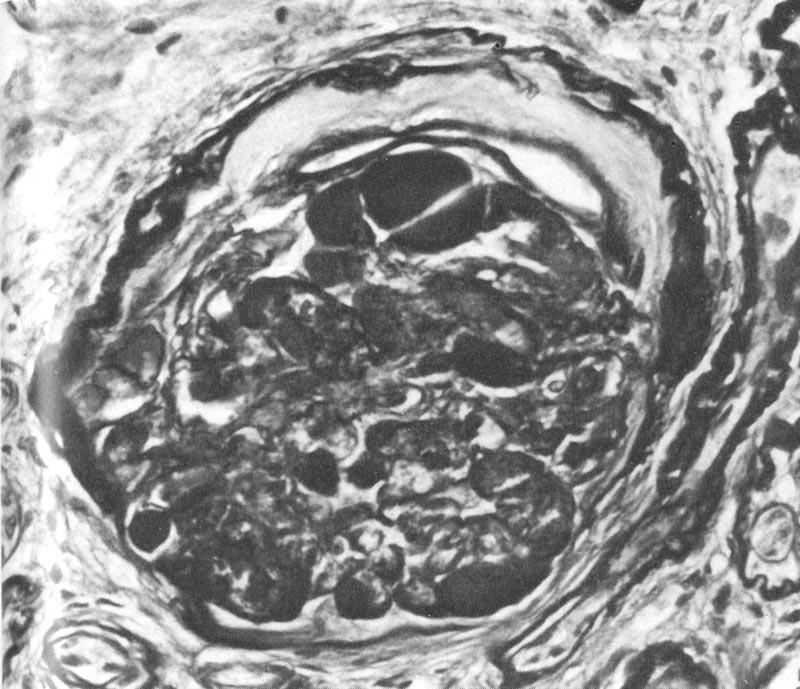
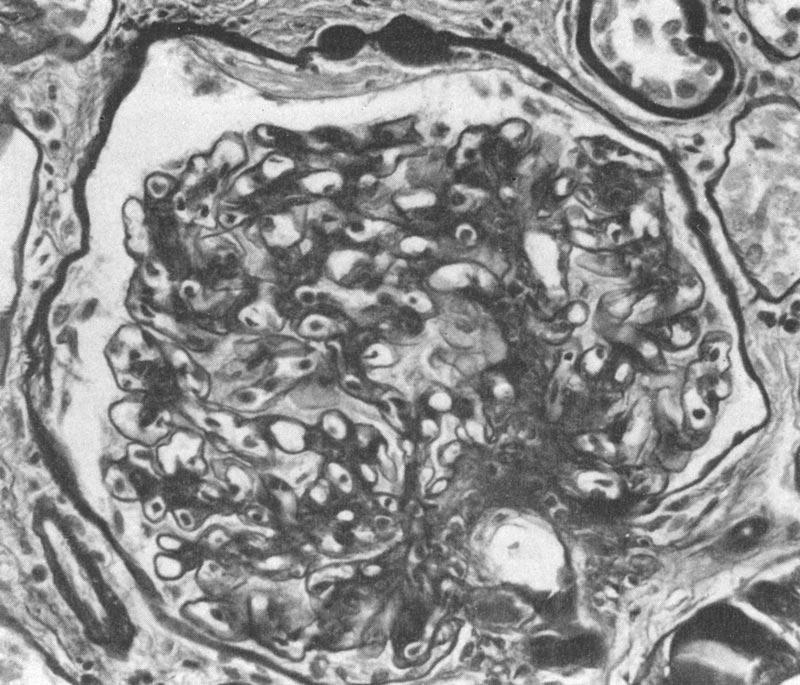
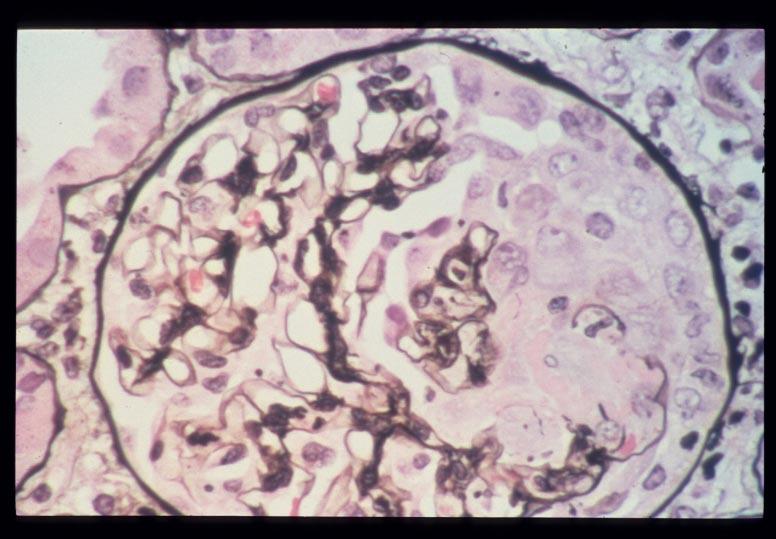
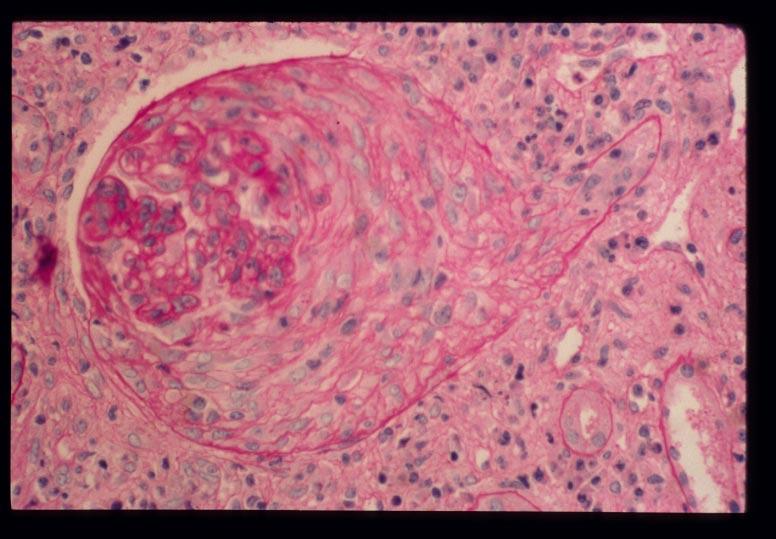
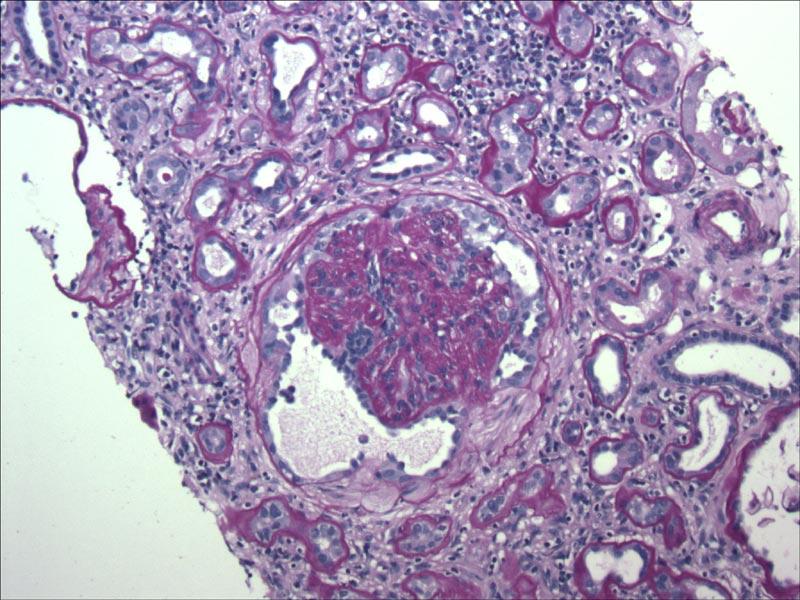
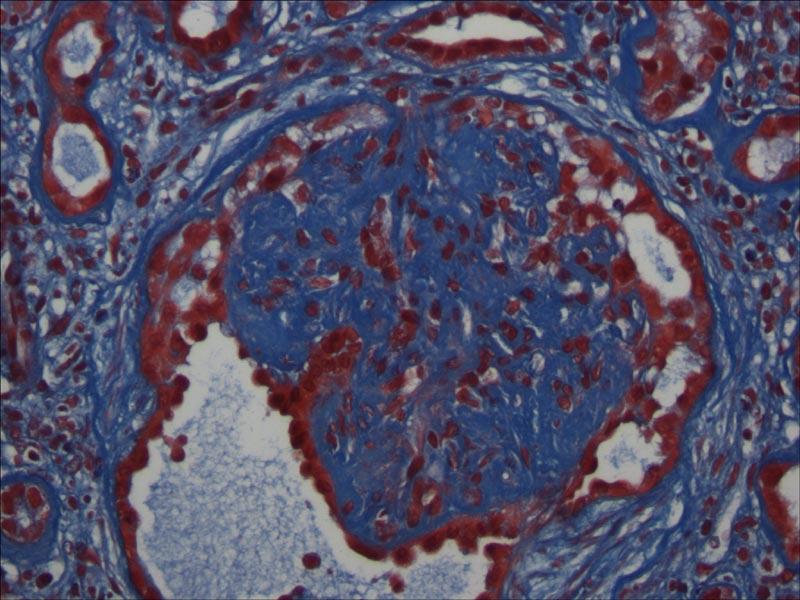
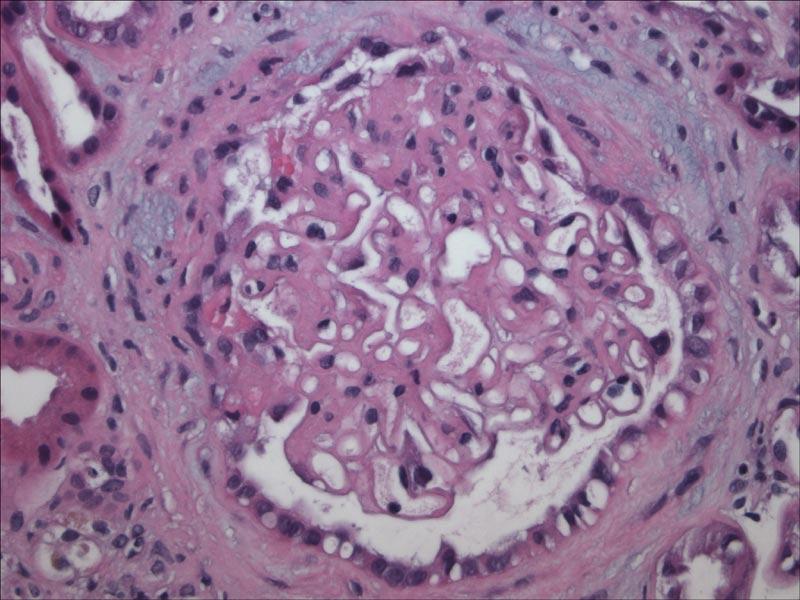
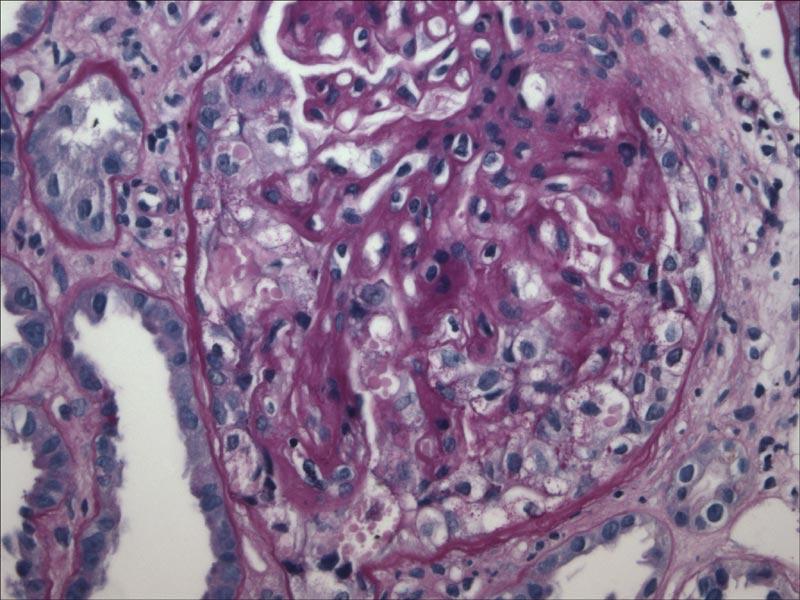
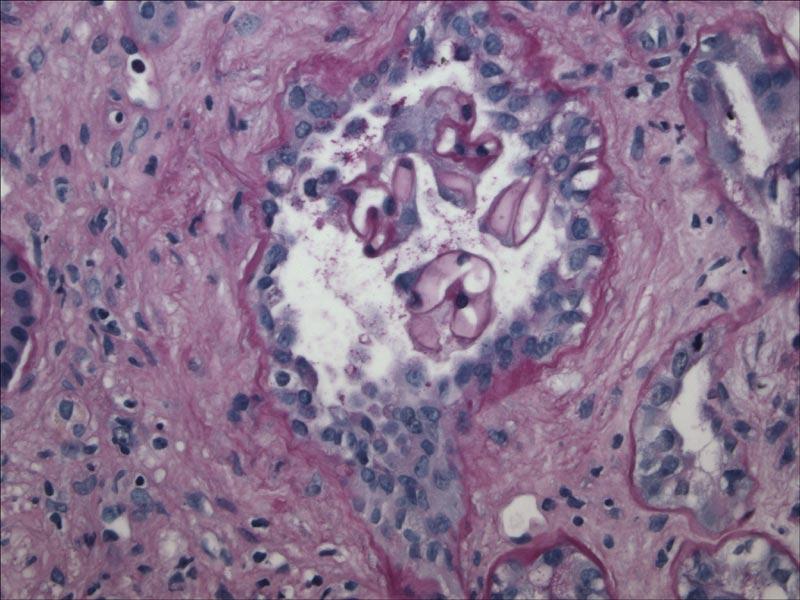
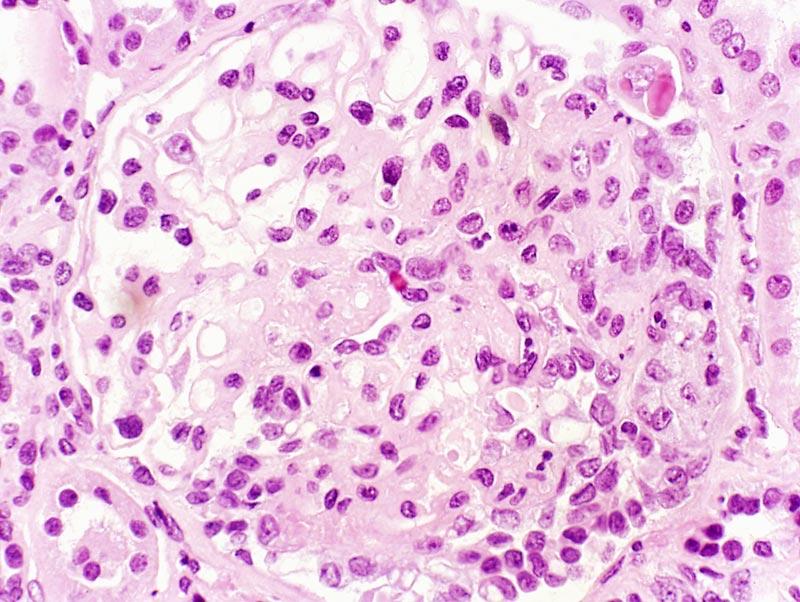
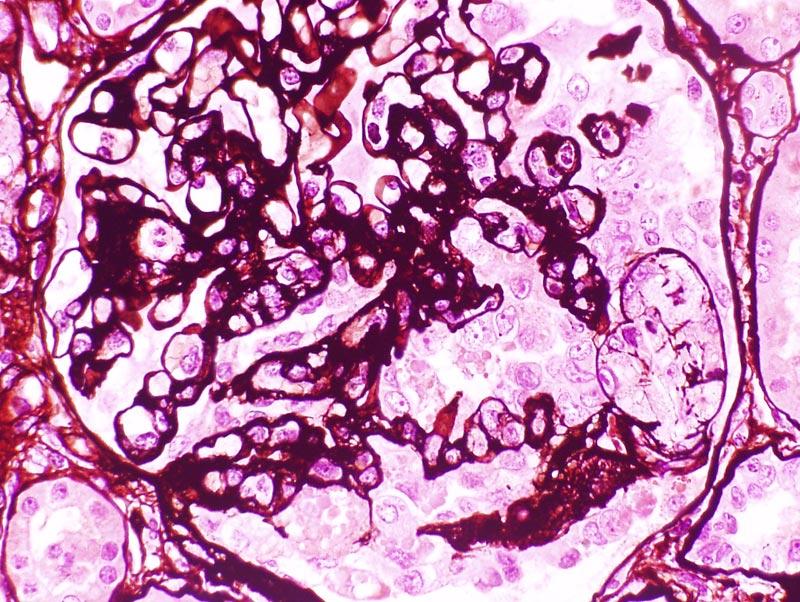
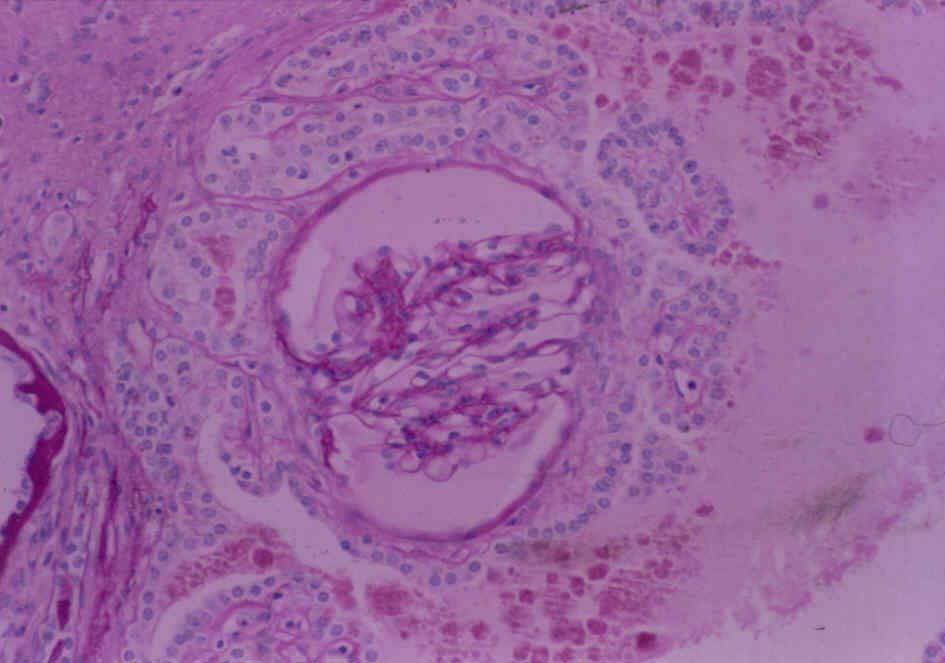
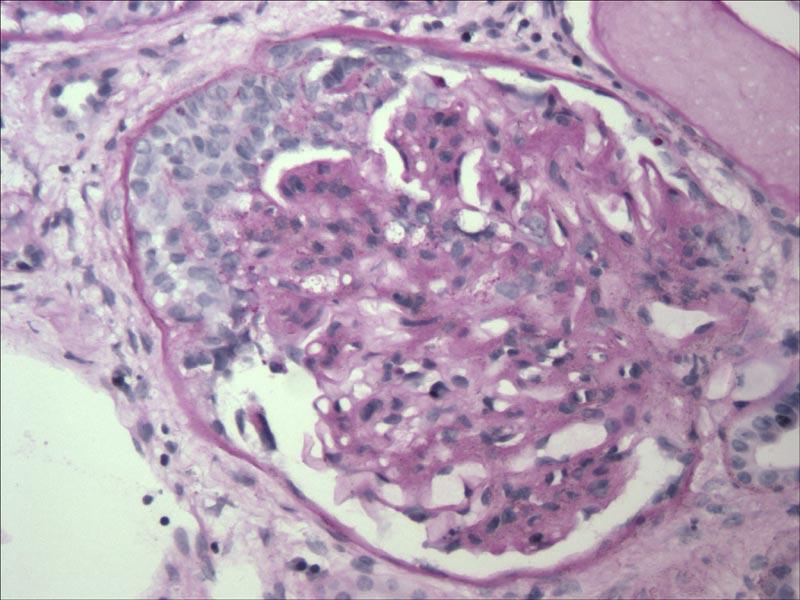
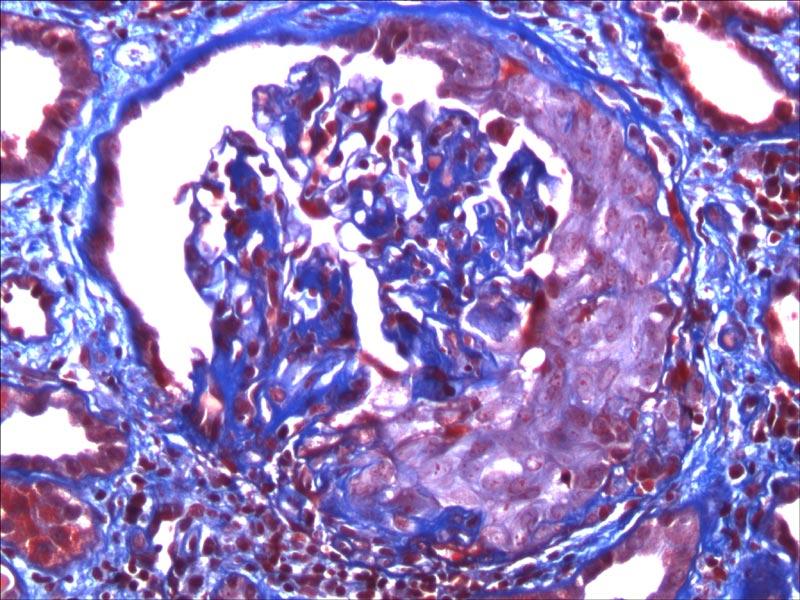
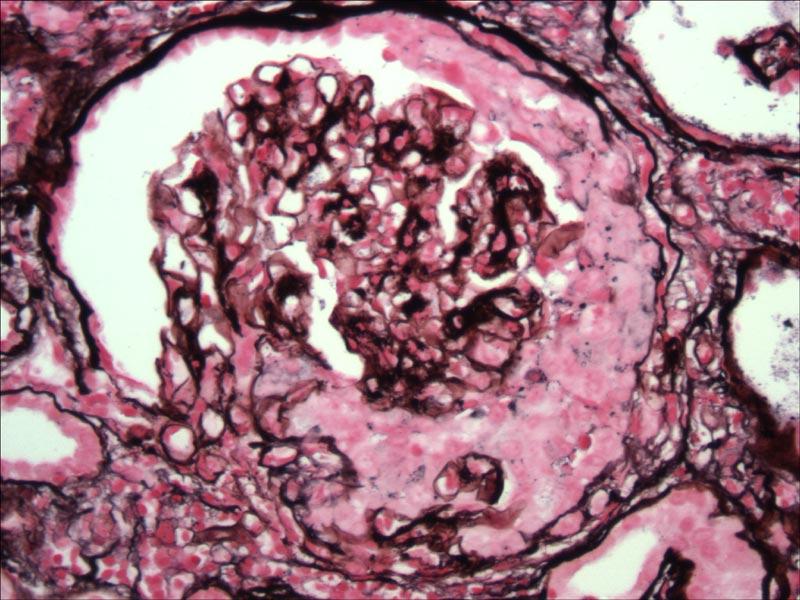
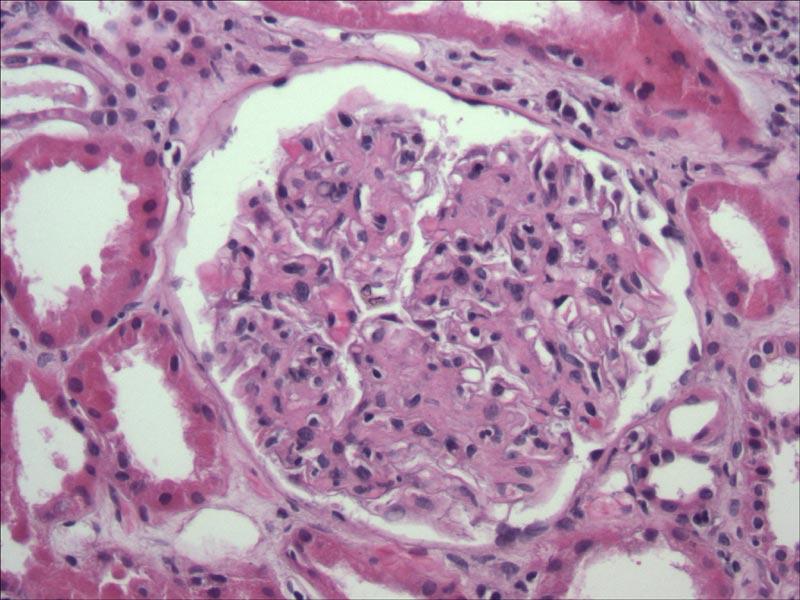
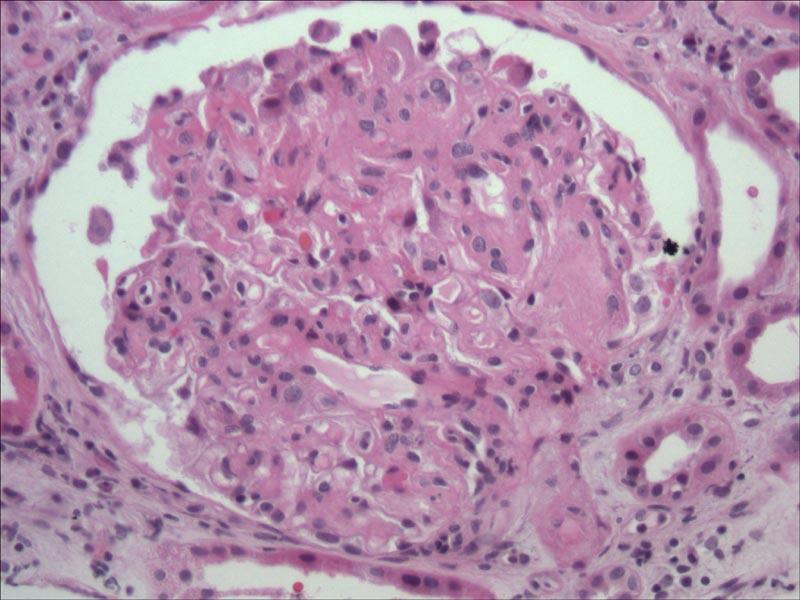
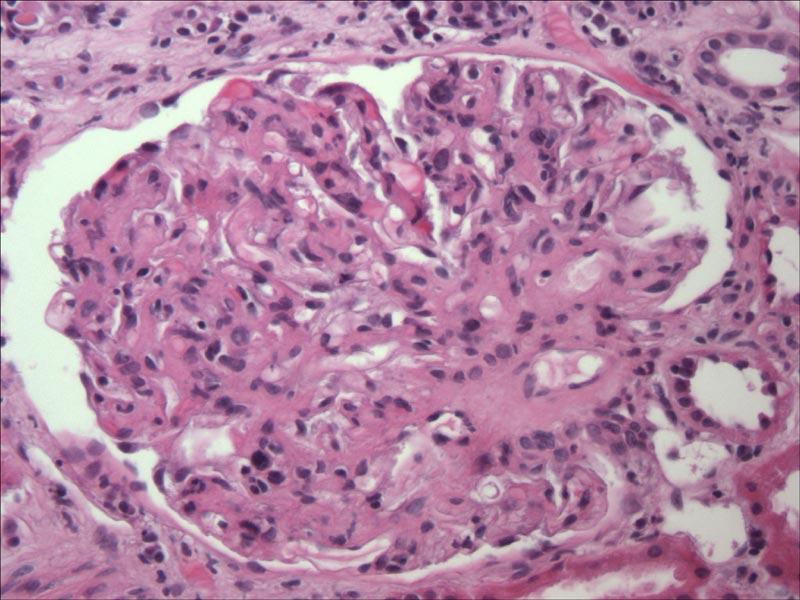
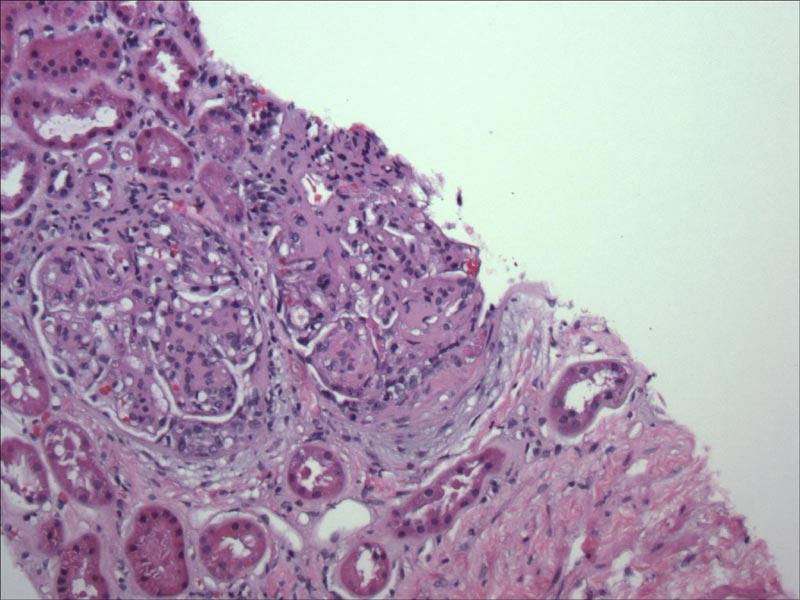
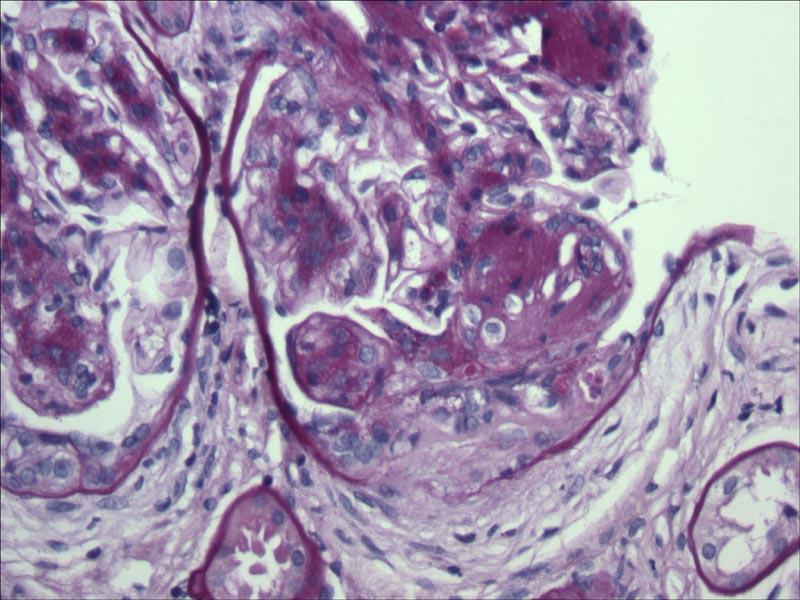
56 ?CRESCENTS IN DIABETIC NEPHROPATHY
57
58

59
60
61
62
63
64
65
66
67
68 IS IT A CRESCENT? A buildup of several cell layers in a crescentic shape, caused by proliferation of parietal cells and probably also of the visceral epithelial cells of the glomerulus. The cells rest in a framework of fibrin, basement membrane, and collagen. A Handbook of Kidney Nomenclature and Nosology International Committee for Nomenclature and Nosology of Renal Disease, 1975
69 DEFINITION OF A CRESCENT (Heptinstall 6 th Edition, 2006) Extracapillary (glomerular) hypercellularity other than the epithelial hyperplasia of collapsing variant of focal segmental glomerulosclerosis
70 TRUE CRESCENTS FROM FOUR OTHER CASES (Next 4 slides)
71
72
73
74
75 Non-Crescent Crescents i.e., Prominent Cells in Bowman s Space: Are all so-called Crescents created equal or really crescents? 1.) Tubularization : ATN, etc 2.) Cellular Caps in FSGS 3.) Cellular Lesions in FSGS; marked extracapillary hypercellularity (as in Virulent, recurrent FSGS) 4.) Marked Extracapillary hypercellularity in HIVAN, collapsing GN. 5.) Hypercellular tubular-like structures in Bowman s Space in ESRD (adenomatoid lesions/pseudotubules; etc) 6.)? ETC
76
77 GLOMERULAR EPITHELIAL HYPERPLASIA FROM OTHER CASES (NOT THIS ONE) : NOT TRUE CRESCENTS 1.) Next two slides: Case of Chronic Sclerosing Lupus GN/approaching ESRD 2.) Other/Next 4: Recurrent (Virulent) Focal segmental sclerosis in a transplant
78
79
80
81
82
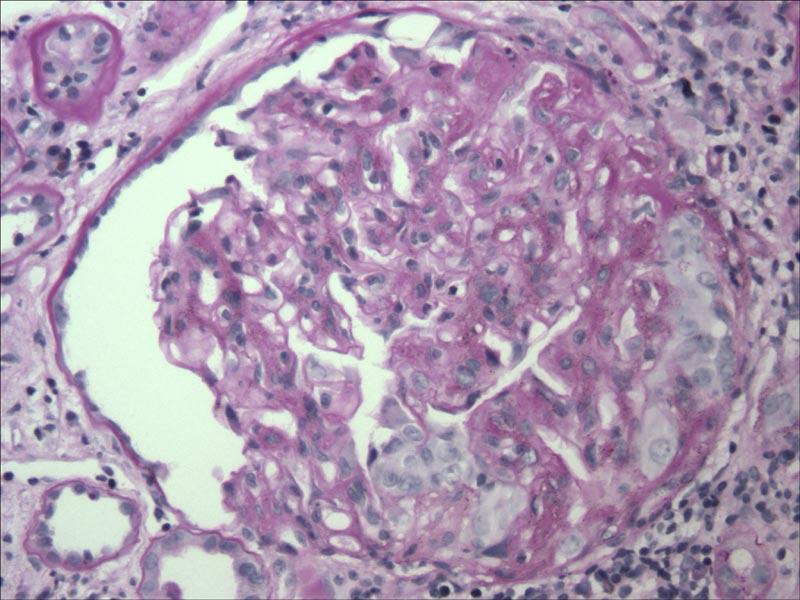
83
84 SLIDES COURTESY OF DR. MELVIN SCHWARTZ 1.) Classic global collapsing FSGS from a nephrotic woman with SLE who had no deposits by IF or EM: not a cellular crescents but just marked hypercellularity in Bowman s Space (one slide). 2.) Next 2 slides: Nephrotic woman with no deposits by EM or IF. Good example of a lesion that looks like segmental necrosis with a crescent, but with the silver stain shows endocapillary foam cells and capillary collapse without breaks.

85
86
87
88 ADENOMATOID HYPERPLASIA SEEN IN ESRD, ETC. (HUGHSON, HENNIGAR X2, MACMANUS, ETC)
89
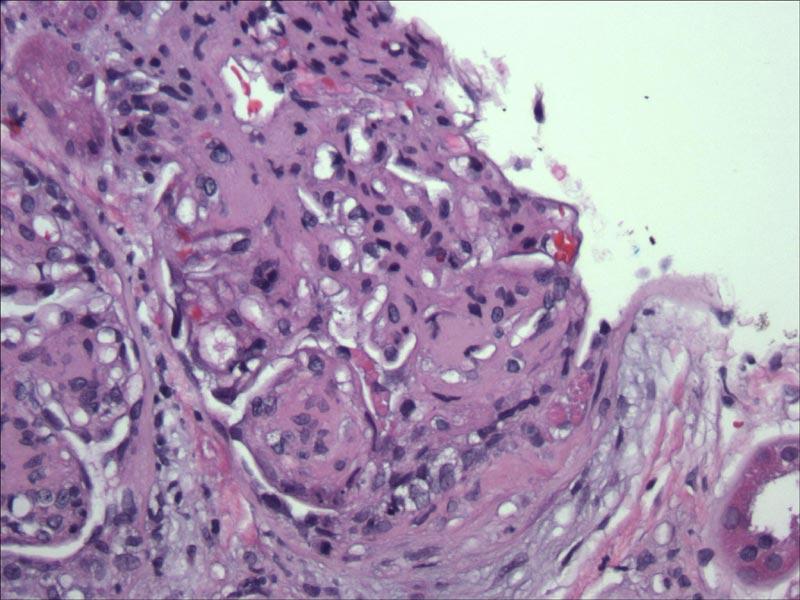
90 OUR PATIENT I interpreted initially as definite crescents
91
92
93
94
95
96
97
98 Biopsy of a Diabetic Patient Step 1 Is it Diabetic Nephropathy Step 2 No Yes Step 3 Then What? That s all DM Plus (Dual Disease) A B C Etc Step 4 What in excess of DM Step 5 Crescents GN Etc
99 CRESCENTIC GN: Mechanisms A.) Immune Complex Deposition B.) Anti-GBM disease C.) ANCA-associated (?pathogenic)
100
101
102
103
104
105
106
107 CRESCENTIC GN: Mechanisms A.) Immune Complex Deposition B.) Anti-GBM disease C.) ANCA-associated (?pathogenic) D.) None of the above (non A, non B, non C) 10-20% of Pauci-Immune Crescentic Glomerulonephritis What is that?
108 DO CRESCENTS MAKE IT A CRESCENTIC GN? What percentage of glomerular involvement is needed? 20-80% or more? 50% or more? 80% or more?
109 Biopsy of a Diabetic Patient Step 1 Is it Diabetic Nephropathy Step 2 No Yes Step 3 Then What? That s all DM Plus (Dual Disease) A B C Etc Step 4 What in excess of DM Step 5 Crescents GN Etc Step 6 No Yes Step 7 ICD Anti-GBM ANCA Something else
110 DIABETES AND CRESCENTS: One Disease or Two? 1.) A severe form of progressive diabetic nephropathy? 2.) Two diseases for the price of one: i.e., diabetic nephropathy and a proliferative GN
111 EVOLUTION OF ONE RENAL DISEASE INTO ANOTHER Membranous GN into Anti-GBM (Klassen)
112 RECENT NEPHNPPT: SUPERIMPOSED GN S?: IGA & SLE Two thirds of the responders indicated that they believed Occam s Razor (i.e., one disease, not two).

113
114 DOES ONE RENAL DISEASE LEAD TO OR ACCENTUATE THE PRODUCTION OF ANOTHER Could it be Autoimmune??Release previously sequestered antigen? Alteration of Self Antigen (Molecular mimicry)? Can autoimmunity wax and wane in a single patient
115 Biopsy of a Diabetic Patient Step 1 Is it Diabetic Nephropathy Step 2 No Yes Step 3 Then What? That s all DM Plus (Dual Disease) A B C Etc Step 4 What in excess of DM Step 5 Crescents GN Etc Step 6 No Yes Step 7 ICD Anti-GBM ANCA Something else Step 8?Severe rare/?post infectious Atypical DM (viral) GN?Stress
116 Case 1: My Diagnosis Diffuse (and early/slight focal/segmental nodular) diabetic glomerulosclerosis with 20% crescent formation (? With superimposed glomerulonephritis) see Above (order anti-gbm and ANCA: please be positive!) Interstitial Inflammation & Fibrosis and Tubular Degeneration
117
118
119 Dr. Clarke Stout I think she does have mild diffuse and nodular diabetic glomerulosclerosis in that several small typical KW nodules are present, and the EM photos are consistent with mild diffuse lesion. It is hard to say how much of the non-nodular mesangial expansion is due to diabetes, and how much is due to the nephritic process, but I suspect most of it is due to the later.
120 Dr. Clarke Stout Crescents are not rare in diabetic glomeruli, and in my experience are almost always associated with an underlying focal mesangiolysis or KW nodule I have never seen crescents as exuberant as the ones in the present case in a diabetic glomerulus, and none of the photos show nodules under the crescents. She appears to have some type of superimposed non-immune mediated glomerulonephritis which I suspect you have a name for
121
122
123
124
125
126
127 Biopsy of a Diabetic Patient Step 1 Is it Diabetic Nephropathy Step 2 No Yes Step 3 Then What? That s all DM Plus (Dual Disease) A B C Etc Step 4 What in excess of DM Step 5 Crescents GN Etc Step 6 No Yes Step 7 ICD Anti-GBM ANCA Something else Step 8?Severe rare/?post infectious Atypical DM (viral) GN?Stress
128 Biopsy of a Diabetic Patient Step 1 Is it Diabetic Nephropathy Step 2 No Yes Step 3 Then What? That s all DM Plus (Dual Disease) A B C Etc Step 4 What in excess of DM Step 5 Crescents GN Etc Step 6 No Yes Step 7 ICD Anti-GBM ANCA Something else Step 8?Severe rare/?post infectious Atypical DM (viral) GN?Stress

129

130
131 SEVERITY OF GN/CRESCENTIC GN GN w/ Crescents Crescentic GN Crescentic DN + DN + DN + GN Crescentic Crescentic in DM GN GN 2 Diseases Crescentic GN DN + DN + DN + DN + Crescents Crescents Crescents Crescents? One or Two Diseases or a Continuation of Changes Mild Mod. Mod. to Severe DN DN Severe DN DN SEVERITY OF DIABETIC NEPHROPATHY
132
133
134 COGNITIVE DIAGNOSTIC ERRORS (Acad.Med.Aug03) 1.) Anchoring: Lock-in too early/fail to adjust to later information 2.) Confirmation: Look for confirming evidence to support Dx/not looking for refutation 3.) Diagnosis Momentum: One Dx label attached: stickier and stickier 4.) Ascertainment Bias: Thinking shaped by prior expectations/stereotyping 5.) Availability: If things rapidly come to mind/recent experience more likely to occur 6.) Base rate neglect: Ignore prevalence of a disease 7.) Commission bias: tendency toward action 8.) Overconfidence: Universal tendency to believe we know more than we do
135 COGNITIVE ERRORS (CONT D) 9.) Premature Closure: when the diagnosis is made, the thinking stops 10.) Fundamental Attribution Error: comorbid medical conditions overlooked 11.) Representativeness Restraint: Looking for prototypical manifestations of disease; leads to missing atypical variants 12.) Search Satifying: Call off search once something is found 13.) Sutton s Slip: When possibilities other than the obvious are not given sufficient consideration 14.) Sunk Costs: The more you invest in a Dx, less likely to release it, and consider alternatives 15.) Vertical Line Failure: Thinking in Silo s: inflexible: what else could it be?
136 COGNITIVE DEBIASING STRATEGIES TO DECREASE DIAGNOSTIC ERRORS 1.) Be aware of bias/approach/experience 2.) Consider alternatives 3.) Metacognition: Step back/reflect on thinking process 4.) Decrease reliance on memory 5.) Training bias/simulations 6.) Strategies to avoid bias 7.) Get more information 8.) Minimize time pressures 9.) Accountability 10.) Feedback
137 WHY PRESENT THIS CASE? 1.) I had it available! (and it intrigued me!) 2.) The Epidemic/Pandemic of Diabetes Mellitus (we re likely to see many more biopsies) 3.) The Differential Diagnosis & Occam s Razor: One or two diseases? (Dr. Pirani s interest and suggestions) 4.) Algorithmic steps/approach 5.) Maybe all crescents are not created equal 6.) Heurism/Missteps/Getting it Right and how will we know? 7.) I d like to know: What do you think it is?
138
139
140 Case 1 Expert Panel Diagnoses Diabetic GS with concurrent ANCA-disease or possibly anti-gbm (2) LCDD with early diabetic change Non-diabetic nodular sclerosis complicated by crescents (vs?chronic TMA)
141 THIS PATIENT 1.) No evidence (clinical or via renal biopsy) of an Immune Complex GN 2.) Anti-GBM: negative (Mayo Labs) 3.) ANCA: negative (Mayo Labs) (Cost of #3 & #4): $ plus shipping
142 FOLLOWUP OF THIS PATIENT 12/04: ANCA and anti-gbm (Mayo Med. Labs): Both Negative 9/16/05: Urine protein: 9.03 grams/24 hrs 9/25/05: Serum creatinine 1.1; BUN 22 Serum albumin 2.7 She was noted to be noncompliant with essentially all her medications due to financial constraints.
143 3/14/2005 4/25/2005 6/9/ /30/ /31/2004 BX 11/9/04 11/10/ /18/ /10/ /12/ /28/ /22/ /25/2004 8/11/2004 6/1/2004 7/10/2004 5/8/2003 1/12/ Serum Cr 1/Serum Cr 3/31/2003
144 6/9/2005 9/15/2005 9/24/ /31/2004 BX 11/9/04 11/10/ /18/ /10/ /12/2004 3/14/2005 4/25/ /28/ /30/ /22/ /25/2004 7/10/2004 8/11/2004 6/1/2004 1/12/2004 5/8/ Serum Cr 1/Serum Cr 3/31/2003
145 9/15/2005 9/24/2005 Dec /9/2005 BX 11/9/04 11/10/ /18/ /10/ /12/2004 3/14/2005 4/25/ /31/ /30/ /28/ /22/ /25/2004 8/11/2004 7/10/2004 6/1/2004 1/12/2004 5/8/ Serum Cr 1/Serum Cr 3/31/2003
146 ACKNOWLEDGEMENTS 1.) Drs. Conrad L. Pirani and Jacob Churg 2.) The Renal Pathology Society, Inc. 3.) Dr. Rory R. Dalton, Dept. of Pathology/MCG 4.) Drs. Clark Stout, Patrick Walker, Charles Jennette, Arthur Cohen, Vivette D Agati, Charles Alpers, Melvin Schwartz, Randy Hennigar, and others 5.) Dr. Agnes Fogo
147 IN HONOR OF DR. CONRAD L. PIRANI AND JACOB CHURG And gladly wolde he lerne, and gladly teche Geoffrey Chaucer The Canterbury Tales (1387)
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
Glomerulonephritis. Dr Rodney Itaki Anatomical Pathology Discipline.
 Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
substance staining with IgG, C3 and IgA (trace) Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ
 Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ") Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Diabetic Nephropathy. Introduction/Clinical Setting. Pathologic Findings Light Microscopy. J. Charles Jennette
 12 Diabetic Nephropathy J. Charles Jennette Introduction/Clinical Setting Diabetic nephropathy is a clinical syndrome in a patient with diabetes mellitus that is characterized by persistent albuminuria,
12 Diabetic Nephropathy J. Charles Jennette Introduction/Clinical Setting Diabetic nephropathy is a clinical syndrome in a patient with diabetes mellitus that is characterized by persistent albuminuria,
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review
 Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Dr Ian Roberts Oxford
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
Membranoproliferative Glomerulonephritis
 Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Lab 3, case 1. Is this an example of nephrotic or nephritic syndrome? Why? Which portion of the nephron would you expect to be abnormal?
 Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Tuesday Conference 7/23/2013. Hasan Fattah
 Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
 C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
29th Annual Meeting of the Glomerular Disease Collaborative Network
 29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME
 CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
CASE OF THE WEEK 1
 www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS
 GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Minimal change disease (MCD) related new electron microscopy findings in a patient on Levothyroxine sodium (LT) for hypothyroidism: A case report Dr. Ali Al-Omari
Enterprise Interest Nothing to declare Minimal change disease (MCD) related new electron microscopy findings in a patient on Levothyroxine sodium (LT) for hypothyroidism: A case report Dr. Ali Al-Omari
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
A Case of IgG2 Heavy Chain Deposition Disease in a Patient with Kappa Positive Plasma Cell Dyscrasia
 Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy?
 CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis with Monoclonal Immunoglobulin Deposits of Lambda Light Chain
 Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
ACUTE GLOMERULONEPHRITIS. IAP UG Teaching slides
 ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
ESRD Dialysis Prevalence - One Year Statistics
 Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Enterprise Interest None
 Enterprise Interest None Lupus Nephritis Ingeborg Bajema Lupus nephritis: the basics Up to 60% of patients with SLE develop lupus nephritis during the course of their disease Lupus nephritis is associated
Enterprise Interest None Lupus Nephritis Ingeborg Bajema Lupus nephritis: the basics Up to 60% of patients with SLE develop lupus nephritis during the course of their disease Lupus nephritis is associated
J Nephropharmacol. 2014; 3(2): Journal of Nephropharmacology
: Journal of Nephropharmacology") J Nephropharmacol. 2014; 3(2): 33 37. NPJ Journal of Nephropharmacology Pathological patterns of mesangioproliferative glomerulonephritis seen at a tertiary care center Ghadeer A. Mokhtar 1*, Sawsan Jalalah
J Nephropharmacol. 2014; 3(2): 33 37. NPJ Journal of Nephropharmacology Pathological patterns of mesangioproliferative glomerulonephritis seen at a tertiary care center Ghadeer A. Mokhtar 1*, Sawsan Jalalah
Dr. Ghadeer Mokhtar Consultant pathologists and nephropathologist, KAU
 Dr. Ghadeer Mokhtar Consultant pathologists and nephropathologist, KAU CLINICAL HISTORY A 4 year old Saudi girl presented to the ER with generalized body swelling, decrease urine output with passing dark
Dr. Ghadeer Mokhtar Consultant pathologists and nephropathologist, KAU CLINICAL HISTORY A 4 year old Saudi girl presented to the ER with generalized body swelling, decrease urine output with passing dark
Histopathology: Hypertension and diabetes in the kidney These presentations are to help you identify basic histopathological features.
 Histopathology: Hypertension and diabetes in the kidney These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need
Histopathology: Hypertension and diabetes in the kidney These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need
Special Challenges and Co-Morbidities
 Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Renal manifestations of IgG4-related systemic disease
 Renal manifestations of IgG4-related systemic disease Lynn D. Cornell, M.D. Mayo Clinic Rochester, MN While autoimmune pancreatitis (AIP) has been recognized since the first description by Sarles et al
Renal manifestations of IgG4-related systemic disease Lynn D. Cornell, M.D. Mayo Clinic Rochester, MN While autoimmune pancreatitis (AIP) has been recognized since the first description by Sarles et al
Glomerular Diseases. Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology
 Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
NORTHWEST AIDS EDUCATION AND TRAINING CENTER. HIV and the Kidney. Leah Haseley, MD. Presentation prepared by: LH NW AETC ECHO June 2012
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and the Kidney Leah Haseley, MD Presentation prepared by: LH NW AETC ECHO June 2012 Etiology of renal disease in HIV 1985- The virus 1995- The antivirals
NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and the Kidney Leah Haseley, MD Presentation prepared by: LH NW AETC ECHO June 2012 Etiology of renal disease in HIV 1985- The virus 1995- The antivirals
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS
 MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA
 C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA C3 Glomerulopathy Overview Discuss C3 Glomerulopathy (C3G) How did we get to the current classification
C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA C3 Glomerulopathy Overview Discuss C3 Glomerulopathy (C3G) How did we get to the current classification
Diabetes on Renal Biopsy-Current Appraisal
 Diabetes on Renal Biopsy-Current Appraisal Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology, retired Washington University School of Medicine St. Louis, MO BNS 2016
Diabetes on Renal Biopsy-Current Appraisal Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology, retired Washington University School of Medicine St. Louis, MO BNS 2016
C3 Glomerulonephritis versus C3 Glomerulopathies?
 Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Clinical pathological correlations in AKI
 Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
The Morphologic Patterns of Diabetic Nephropathy in Koreans
 The Korean Journal of Pathology 2009; 43: 36-42 DOI: 10.4132/KoreanJPathol.2009.43.1.36 The Morphologic Patterns of Diabetic Nephropathy in Koreans Si-Hyong Jang Moon Hyang Park Department of Pathology,
The Korean Journal of Pathology 2009; 43: 36-42 DOI: 10.4132/KoreanJPathol.2009.43.1.36 The Morphologic Patterns of Diabetic Nephropathy in Koreans Si-Hyong Jang Moon Hyang Park Department of Pathology,
Atypical IgA Nephropathy
 Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Transplantation and 6-Month Follow-up of Renal Transplantation from a Donor with Systemic Lupus Erythematosus and Lupus Nephritis
 American Journal of Transplantation 2005; 5: 1772 1776 Blackwell Munksgaard Case Report Copyright C Blackwell Munksgaard 2005 doi: 10.1111/j.1600-6143.2005.00922.x Transplantation and 6-Month Follow-up
American Journal of Transplantation 2005; 5: 1772 1776 Blackwell Munksgaard Case Report Copyright C Blackwell Munksgaard 2005 doi: 10.1111/j.1600-6143.2005.00922.x Transplantation and 6-Month Follow-up
NEPHRITIC SYNDROME. By Dr Mai inbiek
 NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Lupus Nephritis. Ingeborg Bajema
 Lupus Nephritis Ingeborg Bajema Lupus nephritis: the basics Up to 60% of patients with SLE develop lupus nephritis during the course of their disease Lupus nephritis is associated with considerable morbidity
Lupus Nephritis Ingeborg Bajema Lupus nephritis: the basics Up to 60% of patients with SLE develop lupus nephritis during the course of their disease Lupus nephritis is associated with considerable morbidity
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER
: 30 YEARS LATER") HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases
 Kidney International, Vol. 65 (2004), pp. 2145 2152 Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases MARK HAAS and JOSEPH A. EUSTACE Department of Pathology
Kidney International, Vol. 65 (2004), pp. 2145 2152 Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases MARK HAAS and JOSEPH A. EUSTACE Department of Pathology
Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That Showed Predominantly Membranous Features
 Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias
 Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Plasma cell dyscrasias Plasma
Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Plasma cell dyscrasias Plasma
Complement in vasculitis and glomerulonephritis. Andy Rees Clinical Institute of Pathology Medical University of Vienna
 Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG)
") Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors of Renal Outcome
 International Scholarly Research Network ISRN Pediatrics Volume 2011, Article ID 507298, 5 pages doi:10.5402/2011/507298 Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors
International Scholarly Research Network ISRN Pediatrics Volume 2011, Article ID 507298, 5 pages doi:10.5402/2011/507298 Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors
Dr Michael Rayment Chelsea and Westminster Hospital, London
 17 TH ANNUAL CONFERENCE OF THE BRITISH HIV ASSOCIATION (BHIVA) Dr Michael Rayment Chelsea and Westminster Hospital, London 6-8 April 2011, Bournemouth International Centre A decade of renal biopsies in
17 TH ANNUAL CONFERENCE OF THE BRITISH HIV ASSOCIATION (BHIVA) Dr Michael Rayment Chelsea and Westminster Hospital, London 6-8 April 2011, Bournemouth International Centre A decade of renal biopsies in
NEPHROTIC SYNDROME. Presents with the classic tetrad of nephrotic syndrome. Massive proteinuria (>3. 5 g/d) Hypoalbuminemia Edema Hyperlipidemia
 Hypoalbuminemia Edema Hyperlipidemia") PATHOLOGY OF GLOMERULAR DISEASES Disease Etiology Pathophysiology and Clinical Presentation Urinalysis in Nephrotic Syndrome NML excretion: 150 mg/d : < 0.15 g total protein/g urine creatinine Nephrosis
PATHOLOGY OF GLOMERULAR DISEASES Disease Etiology Pathophysiology and Clinical Presentation Urinalysis in Nephrotic Syndrome NML excretion: 150 mg/d : < 0.15 g total protein/g urine creatinine Nephrosis
Renal Disease. Please refer to the assignment page Three online modules TBLs
 Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi
 Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
Renal Pathology Case Conference. Case 2
 Renal Pathology Case Conference Case 2 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN cornell.lynn@mayo.edu March 2, 2008 Clinical presentation 68 year old woman, initially with normal renal function
Renal Pathology Case Conference Case 2 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN cornell.lynn@mayo.edu March 2, 2008 Clinical presentation 68 year old woman, initially with normal renal function
Pathology of Kidney Allograft Dysfunction. B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
CHAPTER 4. Paediatric Renal Biopsies
 2nd Report of the Malaysian Registry of Renal Biopsy 2008 PAEDIATRIC RENAL BIOPSIES CHAPTER 4 Paediatric Renal Biopsies Lee Ming Lee Lim Yam Ngo Lynster Liaw Susan Pee Wan Jazilah Wan Ismail Yap Yok Chin
2nd Report of the Malaysian Registry of Renal Biopsy 2008 PAEDIATRIC RENAL BIOPSIES CHAPTER 4 Paediatric Renal Biopsies Lee Ming Lee Lim Yam Ngo Lynster Liaw Susan Pee Wan Jazilah Wan Ismail Yap Yok Chin
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s. Part 1: Clinical
 Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
WE PRESENT a patient with non insulindependent
 RENAL BIOPSY TEACHING CASE Monoclonal Gammopathy in a Type II Diabetic: A Case of Determined Significance Nancy J. Gritter, MD, Simin Goral, MD, and Agnes Fogo, MD INDEX WORDS: Monoclonal gammopathy; nephrotic
RENAL BIOPSY TEACHING CASE Monoclonal Gammopathy in a Type II Diabetic: A Case of Determined Significance Nancy J. Gritter, MD, Simin Goral, MD, and Agnes Fogo, MD INDEX WORDS: Monoclonal gammopathy; nephrotic