Glomerular Diseases. Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology
|
|
|
- Brenda Wheeler
- 6 years ago
- Views:
Transcription

1 Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology

2 Classification of Glomerular Diseases
3 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Focal Segmental Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Nodular Glomerulosclerosis Membranous Nephropathy Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Diabetic Nephropathy, Amyloidosis Membranous Nephropathy MPGN IgA Nephropathy Post-infections (Post-Strep) GN Rapidly Progressive GN (RPGN) Nephritic
4 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Minimal Change Disease Focal Segmental Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Nodular Glomerulosclerosis Membranous Nephropathy Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Diabetic Nephropathy, Amyloidosis Membranous Nephropathy MPGN IgA Nephropathy Post-infections (Post-Strep) GN Rapidly Progressive GN (RPGN) Nephritic

5 Minimal Change Disease Case presentation Bella is a 19 year old high school student referred for proteinuria. She developed edema to thighs 3 wks ago. She has been previously healthy. She takes no medications.
6 Minimal Change Disease Case presentation Exam: BP 101/63, exam normal except for 2+ pitting lower extremity edema bilaterally Labs: urine prot 4+, alb 2.2, cholesterol 498, creat 0.6 Diagnosis: Nephrotic syndrome
7 Minimal Change Disease Case presentation Patient started on prednisone 60 mg daily. Returns 1 wk later edema resolved and urine protein is down to trace. Diagnosis: Minimal Change Disease

8 Minimal change disease Definition: Histopathologic lesion with normal glomeruli on light microscopy and diffuse foot process fusion on electron microscopy, associated with nephrotic syndrome.
 targets podocytes disrupting GBM charge barrier and causing")
9 Minimal Change Disease Pathogenesis: leading hypothesis: immune dysfunction/t cell activation leads to release of a cytokine the cytokine ( permeability factor ) targets podocytes disrupting GBM charge barrier and causing proteinuria

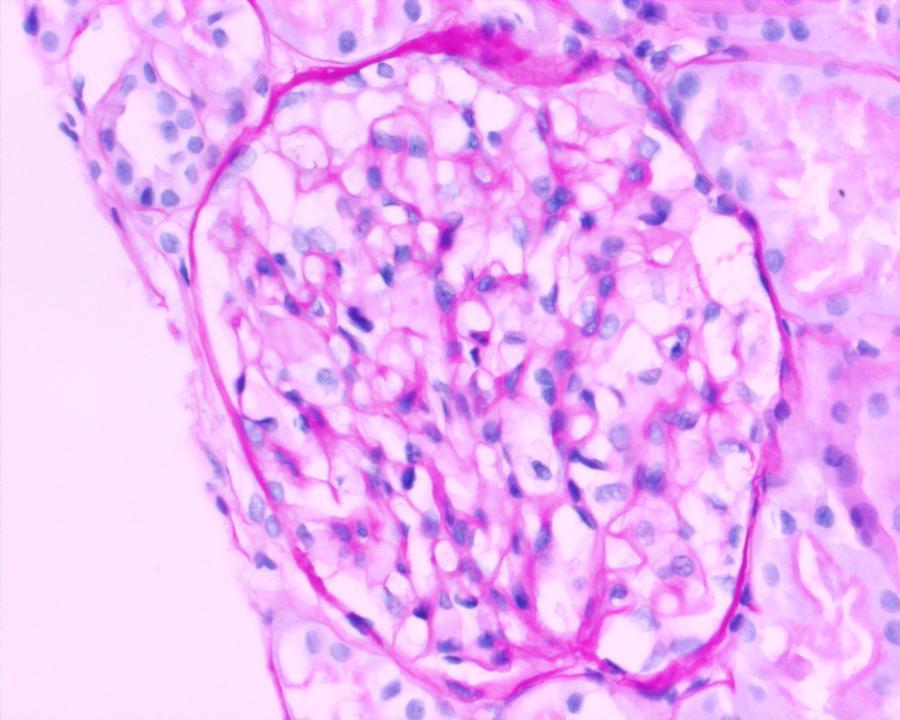
10 Minimal Change Disease, LM Appears normal

11 Minimal Change Disease, LM Proximal tubular epithelial cells filled with lipid and protein ( lipoid nephrosis )

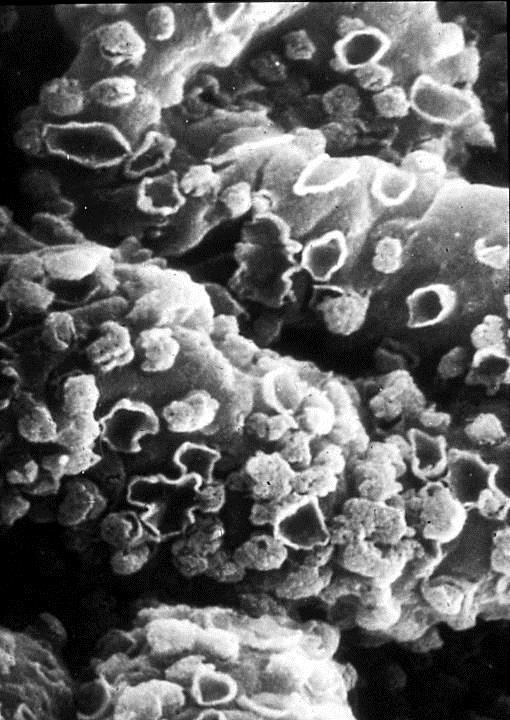
12 Minimal Change Disease, EM
13 Minimal Change Disease Epidemiology: Most common cause of nephrotic syndrome in children Less common in adults Ethiology: Primary - idiopathic Secondary: Drugs: NSAIDs Tumors: lymphomas Immune modulation: vaccinations
14 Minimal Change Disease Clinical characteristics and treatment: Abrupt onset of florid nephrotic syndrome Normal blood pressure Renal function usually remains good 90% respond rapidly to corticosteroids, adults are slower to respond than children Relapses are characteristic and respond to retreatment
15 Minimal Change Disease Clinical characteristics and treatment: Frequently relapsing or steroid-resistant cases respond to other immunosuppressive agents (mycophenolate, cyclosporine, cyclophosphamide) Some become steroid dependent until puberty, when most cases finally remit Long term prognosis is excellent
16 Minimal Change Disease Case follow-up Patient was treated with a 4 months prednisone taper with complete resolution of proteinuria. However, 1 mo after stopping prednisone, her proteinuria increased to 3+, which indicated a relapse. Started on CellCept (Mycophenolate), again with resolution of proteinuria after 1 wk. Pt then treated with CellCept x 1 year. She remains in complete remission.
17 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Focal Segmental Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Nodular Glomerulosclerosis Membranous Nephropathy Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Diabetic Nephropathy, Amyloidosis Membranous Nephropathy MPGN IgA Nephropathy Post-infections (Post-Strep) GN Rapidly Progressive GN (RPGN) Nephritic
18 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Focal Segmental Glomerulosclerosis Nodular Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Diabetic Nephropathy, Amyloidosis Membranous Nephropathy Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Membranous Nephropathy MPGN IgA Nephropathy Post-infections (Post-Strep) GN Rapidly Progressive GN (RPGN) Nephritic

19 Focal Segmental Glomerulosclerosis Case presentation Laurent is a laboratory technician who has diagnosed himself with nephrotic syndrome
20 Focal Segmental Glomerulosclerosis Case presentation He is a 45 year old African American male w h/o HTN, who developed progressively increasing lower extremity edema for the past 6 mo
21 Focal Segmental Glomerulosclerosis Case presentation He was seen by his PCP several times, and his medications were adjusted. However, in spite of proteinuria on UA, no diagnosis was made Medications: verapamil and lasix On exam, his BP is 145/91, remainder unremarkable except for tight 4+ LE edema
22 Focal Segmental Glomerulosclerosis Case presentation Labs 9 mo prior: 2+ protein on UA serum albumin 4 cholesterol 300, LDL 180 Current labs: serum albumin 2.8 cholesterol 396, LDL 270 and creatinine 1.2 Urinalysis 4+ protein and a few granular casts Urine protein/creatinine ratio 12
23 Focal Segmental Glomerulosclerosis Case presentation Diagnosis: Nephrotic syndrome Kidney biopsy was performed, demonstrating focal segmental glomerulosclerosis

 of the glomerular tuft normal")
24 Focal Segmental Glomerulosclerosis Definition: Histopathologic lesion with sclerosis of some but not all (hence focal) glomeruli that involves a portion (segment) of the glomerular tuft normal FSGS
25 Focal Segmental Glomerulosclerosis Ethiology and pathogenesis: Primary: presumed due to a circulating factor (?cytokine) that damages VEC Secondary (associated with other conditions): HIV, heroin abuse, sickle cell disease, massive obesity. maladaptive response to nephron loss Inherited linked to mutations of the VEC proteins nephrin, podocin etc, causing podocytopathy.

26 Secondary Focal Segmental Glomerulosclerosis


27 Focal Segmental Glomerulosclerosis Morpology: Sclerotic segments show basement membrane collapse, increased matrix, trapping of plasma proteins in glomerular capillary walls by light microscopy pronounced tubular atrophy and interstitial fibrosis
28 normal

29 segmentally collapsed unaffected Focal Segmental Glomerulosclerosis


30 Focal Segmental Glomerulosclerosis less affected segment Effacement of VEC in sclerotic and non-sclerotic segments by EM; no deposits. GBM collapse and foot process fusion
31 Focal Segmental Glomerulosclerosis Epidemiology: most common cause of primary nephrotic syndrome in African-American adults Clinical characteristics: Nephrotic syndrome (primary disease or HIV nephropathy) or nephrotic range proteinuria (most secondary forms) Proteinuria is non-selective in contrast with minimal change disease Hypertension, reduced GFR Slow and variable response to steroids Progression to chronic glomerulosclerosis; 50-80% to ESRD within several years Children have better prognosis than adults Recurrence post transplant is common in idiopathic FSGS leading to graft failure
32 Focal Segmental Glomerulosclerosis Treatment: Only idiopathic FGSG has a chance to respond to immunosuppressive treatment. Therefore, it is imperative to determine whether the disease is primary or secondary Primary disease: Steroids Immunosuppressive cytotoxic agents - Cyclosporine, Tacrolimus, Mycophenolate Primary and secondary disease: ACE/ARB and anti-lipid agents HIV-associated FSGS Antiretroviral medications
33 Focal Segmental Glomerulosclerosis Case follow-up Patient was started on prednisone. Two weeks later he was admitted with bacteremia. His prednisone was tapered and he was started on cyclosporine. Patient was unable to tolerate medication, switched to CellCept. This medication was stopped after several months due to lack of efficacy.
34 Focal Segmental Glomerulosclerosis Case follow-up His proteinuria increased to 40 g/24 hrs, and serum creatinine progressively increased to 3. Patient failed other immunosuppressive medications, and had multiple infectious complications. He also had severe complications of nephrotic syndrome resistant anasarca, deep venous thrombosis from hypercoagulable state, pericardial effusion, and chronic hypotension due to low plasma oncotic pressure.
35 Focal Segmental Glomerulosclerosis Case presentation He was started on dialysis to control edema, but could not tolerate fluid removal due to hypotension. After hospitalization that lasted 4 months, patient finally agreed to have bilateral renal artery embolization, a procedure called chemical nephrectomy. He is now hemodialysis-dependent, and has much improved clinically.

36 Now let s see if you ve been paying attention
37 Patient has nephrotic syndrome, biopsy below. Which statement about this disease A. It is the most common cause of nephrotic syndrome in children B. It is characterized by sudden onset of florid nephrotic syndrome C. It is poorly responsive to steroids D. It can be caused by NSAIDs is INCORRECT:


38 Patient has nephrotic syndrome, biopsy below. Which statement about this disease A. It is the most common cause of nephrotic syndrome in children B. It is characterized by sudden onset of florid nephrotic syndrome C. It is poorly responsive to steroids D. It can be caused by NSAIDs is INCORRECT:
39 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Focal Segmental Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Nodular Glomerulosclerosis Membranous Nephropathy Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Diabetic Nephropathy, Amyloidosis Membranous Nephropathy MPGN IgA Nephropathy Post-infections (Post-Strep) GN Rapidly Progressive GN (RPGN) Nephritic
40 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Focal Segmental Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Membranous Nephropathy Nodular Glomerulosclerosis Membranous Nephropathy Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Diabetic Nephropathy, Amyloidosis Membranous Nephropathy MPGN IgA Nephropathy Post-infections (Post-Strep) GN Rapidly Progressive GN (RPGN) Nephritic

41 Membranous Glomerulonephropathy Case presentation Jacob is a 25 yo previously healthy hospital security guard, who was referred for evaluation of proteinuria.
42 Membranous Glomerulonephropathy Case presentation He noticed LE edema several weeks prior. He was hypertensive at 155/90. His serum creatinine was 0.9, alb 2.2, cholesterol 311 w LDL 173, Urine - 5g protein/24 hrs.
43 Membranous Glomerulonephropathy Case presentation Kidney biopsy showed Membranous Glomerulopathy. Clinical course: patient was treated w immunosuppressive regimen consisting of prednisone and cyclophosphamide for 6 months, and responded with markedly decreased proteinuria (0.5 g/24 hrs). He was seen in follow-up several years later and had trace proteinuria and normal creatinine.

44 Membranous Glomerulonephropathy Definition: Histopathologic lesion characterized by glomerular basement membrane thickening due to immune complex entrapment, associated with nephrotic syndrome

 Both activate complement, which damages podocytes and")
45 Membranous Glomerulonephropathy Pathogenesis: A chronic immune-complex nephritis caused by: circulating immune Ab directed against complex entrapment in intrinsic GBM Ag the GBM (secondary) (primary) Both activate complement, which damages podocytes and makes them leaky

46 Pathogenesis of primary membranous GN
 of basement membrane in")
47 Membranous Glomerulonephropathy Pathology: light microscopy: diffuse, uniform thickening of basement membrane with small subepithelial projections ("spikes") of basement membrane in capillary loops.
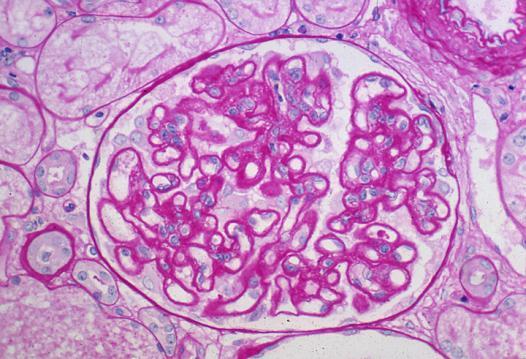
48 normal Membranous Glomerulonephropathy, LM

 side")
49 Membranous Glomerulonephropathy, LM normal Spike formation on subepithelial (urinary) side of GBM, (silver stain)
50 normal Membranous Glomerulonephropathy, LM



51 Membranous Glomerulonephropathy, IF Immunofluorescence microscopy: diffuse, coarsely granular pattern to IgG along capillary loops. normal

52 Membranous Glomerulonephropathy, EM Subepithelial electron-dense immune deposits

53 Membranous Glomerulonephropathy, EM
54 Membranous Glomerulonephropathy Epidemiology: most common cause of primary nephrotic syndrome in Caucasian adults Ethiology: Primary Secondary: Drugs: penicillamine, captopril, gold Malignancy (solid tumors) Infection: hepatitis B, syphilis Autoimmune disease: systemic lupus erythematosus (SLE), rheumatoid arthritis (RA)
55 Membranous Glomerulonephropathy Clinical features: insidious onset of nephrotic syndrome, usually without identifiable preceding illness; variable, but often indolent course Prognosis: Rule of thirds (without treatment): 1/3 Spontaneous remission 1/3 Partial remission / slow deterioration 1/3 Progress to ESRD
56 Membranous Glomerulonephropathy Predictors of poorer outcome are: tubulointerstitial fibrosis elevated cr at diagnosis male sex hypertension older age and heavy proteinuria. Treatment: Steroids alone are not very effective Prednisone alternating with Cyclophosphamide Cyclosporin

57 Now let s see if you ve been paying attention
58 Patient has nephrotic syndrome and biopsy is depicted below. Which statement is INCORRECT: A. It is the most common cause of idiopathic nephrotic syndrome in African American adults B. It is characterized by slow and variable response to steroids C. It can be associated with HIV D. This disease does not affect podocytes

59 Patient has nephrotic syndrome and biopsy is depicted below. Which statement is INCORRECT: A. It is the most common cause of idiopathic nephrotic syndrome in African American adults B. It is characterized by slow and variable response to steroids C. It can be associated with HIV D. This disease does not affect podocytes
60 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Focal Segmental Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Nodular Glomerulosclerosis Membranous Nephropathy Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Diabetic Nephropathy, Amyloidosis Membranous Nephropathy MPGN IgA Nephropathy Post-infections (Post-Strep) GN Rapidly Progressive GN (RPGN) Nephritic
61 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Focal Segmental Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Nodular Glomerulosclerosis Membranous Nephropathy Membranoproliferative Glomerulonephritis Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Diabetic Nephropathy, Amyloidosis Membranous Nephropathy MPGN IgA Nephropathy Post-infections (Post-Strep) GN Rapidly Progressive GN (RPGN) Nephritic

62 Membranoproliferative Glomerulonephritis (Type I) Case presentation Jasper is a 48 year old Caucasian male with h/o polysubstance abuse.
63 Membranoproliferative Glomerulonephritis (Type I) Case presentation He was admitted to the hospital with generalized swelling, hypertensive urgency and pulmonary edema. He was homeless, but is currently living at Rubicon drug treatment center.
64 Membranoproliferative Glomerulonephritis (Type I) Case presentation His serum cr in 2, serum albumin is 2.5, urine protein to creatinine ratio is 10, UA showed proteinuria and hematuria. Further workup revealed that patient is positive for hepatitis C and cryoglobulins.
65 Membranoproliferative Glomerulonephritis (Type I) Case presentation Kidney biopsy revealed membranoproliferative glomerulonephritis (MPGN), type I. Patient was not a candidate for treatment due to poor social situation and history of non-compliance. His renal function has deteriorated and he became dialysisdependent within 6 months.
 of GBM on light")
66 Membranoproliferative Glomerulonephritis (Type I) Definition: histopathologic lesion characterized by mesangial proliferation and interposition into the glomerular capillary wall with double contours ( tram tracking ) of GBM on light microscopy

67 Membranoproliferative Glomerulonephritis (Type I) Pathogenesis: deposition of subendothelial immune complexes in glomerulus with abnormal activation of complement, production of nephritic factors and glomerular injury

68 Mesangial interposition into GBM in MPGN
")

69 Membranoproliferative Glomerulonephritis (Type I) Light microscopy: glomerular hypercellularity and lobular simplification
 is")
70 Membranoproliferative Glomerulonephritis (Type I) Light microscopy: splitting of GBM ("tram-track ) is characteristic

71 Membranoproliferative Glomerulonephritis (Type I) Immunofluorescence: coarse granular staining of IgG and C3 along capillary loops
, EM")

72 Membranoproliferative Glomerulonephritis (Type I), EM Normal GBM Electron Microscopy: subendothelial deposits with new formation of GBM (splitting)
73 Membranoproliferative Glomerulonephritis (Type I), EM, LM
74 Membranoproliferative Glomerulonephritis (Type I) Epidemiology: Primary children and young adults, rare Secondary adults, more common Ethiology: Primary (idiopathic) Secondary (seen in association with other disorders) SLE, hepatitis C (often with cryoglobulinemia), endocarditis Malignancy (lymphoma, leukemia)
75 Membranoproliferative Glomerulonephritis (Type I) Clinical characteristics Nephrotic/nephritic Depressed serum complement levels Few remissions, usually unrelenting course 50% with renal failure in 10 years
76 Treatment: Membranoproliferative Glomerulonephritis (Type I) Primary in children immunosuppression Secondary treat the original disease (antiviral or antibacterial agents), antiplatelet agents, immunomodulation in some cases

77 Now let s see if you ve been paying attention
78 Which statement regarding the disease with LM/IF below is INCORRECT: A. This is the most common cause of primary nephrotic syndrome in Caucasian adults B. 2/3 of patients will develop spontaneous or partial remission without treatment C. Can be associated with solid tumors D. EM would show reduplication of GBM with tram tracking


79 Which statement regarding the disease with LM/IF below is INCORRECT: A. This is the most common cause of primary nephrotic syndrome in Caucasian adults B. 2/3 of patients will develop spontaneous or partial remission without treatment C. Can be associated with solid tumors D. EM would show reduplication of GBM with tram tracking
80 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Focal Segmental Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Nodular Glomerulosclerosis Membranous Nephropathy Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Diabetic Nephropathy, Amyloidosis Membranous Nephropathy MPGN IgA Nephropathy Post-infections (Post-Strep) GN Rapidly Progressive GN (RPGN) Nephritic
81 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Focal Segmental Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Nodular Glomerulosclerosis Membranous Nephropathy Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Diabetic Nephropathy, Amyloidosis Membranous Nephropathy MPGN IgA Nephropathy Post-infections (Post-Strep) GN Rapidly Progressive GN (RPGN) Nephritic

82 IgA Nephropathy (Berger s Disease) Case presentation Alice is a 24 year old white female with history of hypertension, who is 16 wks pregnant. She is referred by her OB for proteinuria, hematuria and hypertension. Patient has a history of gross hematuria following upper respiratory infections.
83 IgA Nephropathy Case presentation Her BP is 155/90, she has trace LE edema, and her UA shows 3+ protein and 20 rbc. Her renal function is normal. She is managed conservatively with labetalol for BP control and bed rest. Her proteinuria is monitored and remains stable throughout the pregnancy. She is delivered via C- section at 37 weeks gestation.
84 IgA Nephropathy Case presentation 6 weeks post-partum her proteinuria remains unchanged at 3g/24 hrs. Kidney biopsy is performed and shows IgA nephropathy with 50% glomerulosclerosis and moderate interstitial fibrosis. She is started on ACE-I, fish oil and prednisone, but then lost to follow-up.

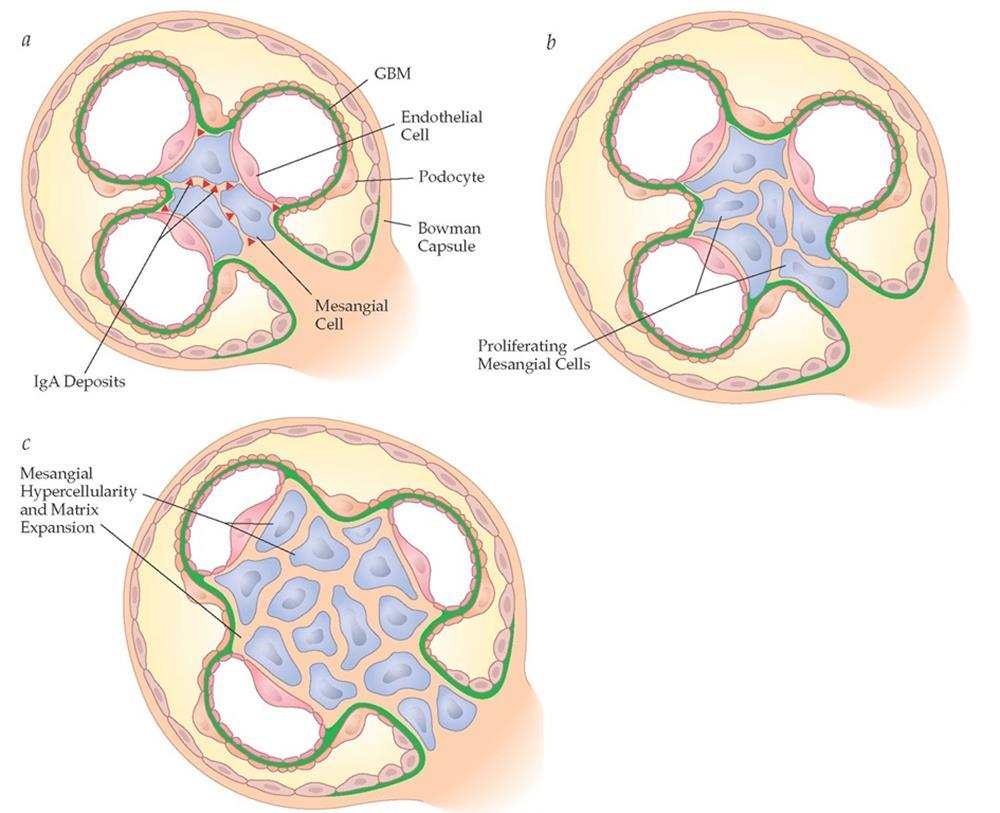
85 IgA Nephropathy Definition: Histopathologic lesion of a glomerulonephritis characterized by prominent IgA containing immune deposits in the mesangium Mesangial IgA deposits
86 Pathogenesis: IgA Nephropathy Error of IgA production and clearance abnormally high production of mucosal and marrow IgA in response to an environmental Ag abnormal glycosylation reduces plasma clearance of IgA by the liver IgA deposition as immune complexes in the mesangium; there it activates complement.
87 IgA Nephropathy

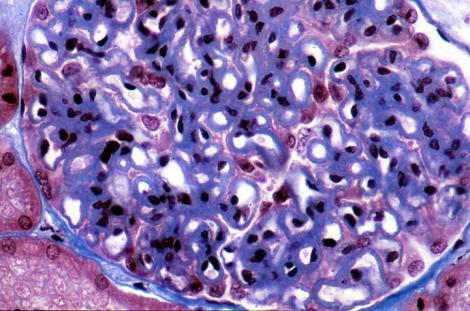
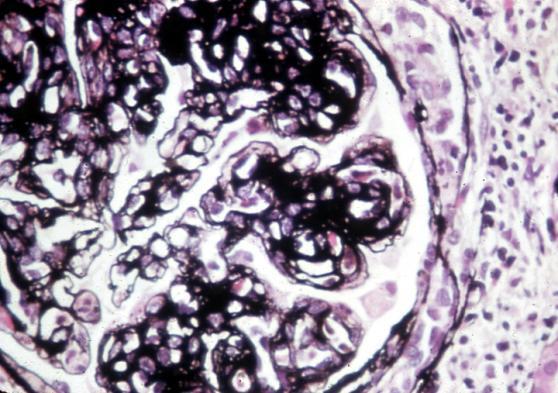
88 IgA Nephropathy normal LM: Mesangial hypercellularity and matrix expansion

89 IgA Nephropathy IF: mesangial IgA, diffuse and granular, in pruned bush pattern
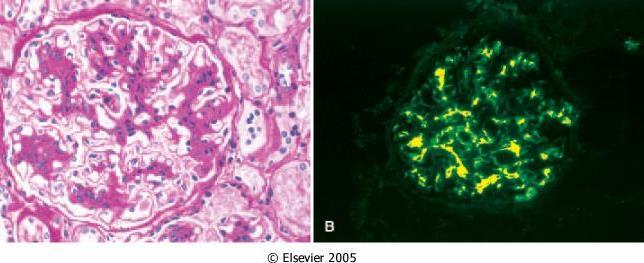
90 IgA Nephropathy, LM, IF

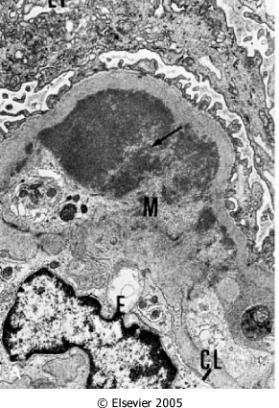
91 IgA Nephropathy EM: mesangial immune deposits
92 IgA Nephropathy Epidemiology: the most common primary GN worldwide Clinical features: The classic presentation is gross hematuria, occurring coincidentally with a upper respiratory infections. Hematuria subsides and recurs every few months. In the background, there is indolent development of mild nephritic or nephrotic features Very rarely develops crescentic RPGN
93 IgA Nephropathy May be associated with Henoch-Schoenlein purpura, a systemic disorder of children that includes purpuric skin lesions, abdominal pain and arthralgia. Prognosis: variable, with many patients maintaining normal renal function for many years; but slow progression to chronic renal failure in 40%. Recurrence post-transplant is frequent.

94 Now let s see if you ve been paying attention
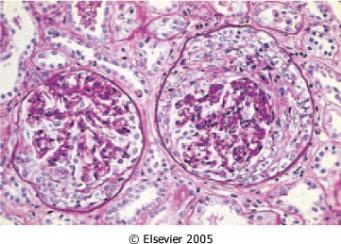
95 Which diagnosis can you suspect from the light microscopy below: A. Membranous nephropathy B. Minimal change disease C. FSGS D. Membranoproliferative Glomerulonephritis (MPGN)

96 Which diagnosis can you suspect from the light microscopy below: A. Membranous nephropathy B. Minimal change disease C. FSGS D. Membranoproliferative Glomerulonephritis (MPGN)
97 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Focal Segmental Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Nodular Glomerulosclerosis Membranous Nephropathy Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Diabetic Nephropathy, Amyloidosis Membranous Nephropathy MPGN IgA Nephropathy Post-infections (Post-Strep) GN Rapidly Progressive GN (RPGN) Nephritic
98 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Focal Segmental Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Nodular Glomerulosclerosis Membranous Nephropathy Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Diabetic Nephropathy, Amyloidosis Membranous Nephropathy MPGN IgA Nephropathy Post-Strep Glomerulonephritis Post-infections (Post-Strep) GN Rapidly Progressive GN (RPGN) Nephritic

99 Acute Post-Streptococcal Glomerulonephritis Case presentation Edward is transferred to VCU from outside hospital for acute glomerulonephritis. He is an 18 year old Caucasian male with h/o tonsillectomy at age 5.
100 Acute Post-Streptococcal Glomerulonephritis Case presentation Ten days prior to admission he had strep throat with positive rapid strep test, and was started on augmentin by his PCP.
101 Acute Post-Streptococcal Glomerulonephritis Case presentation He was referred for admission after he developed tea colored urine, and was found to have hematuria, proteinuria and HTN. Pt reports 20 lbs wt gain in 3 days w periorbital and upper body edema, and abdominal pain. He now denies any sore throat.
102 Acute Post-Streptococcal Glomerulonephritis Case presentation SH is significant for tobacco, alcohol and marijuana use Exam: BP 175/77, ps 49. Young athletic wm in no acute distress. Lungs were clear and heart was regular, with 2/6 systolic murmur at base. Abdomen was soft, diffusely tender, with liver and spleen edges palpable. Trace LE edema. No rash.
103 Acute Post-Streptococcal Glomerulonephritis Case presentation Labs showed cr 1.3, albumin 2.7, urinalysis 178 rbc and 25 wbc, 3+ protein and several red blood cell casts. ASO titer and streptozyme were positive. C3 complement level was low. Diagnosis: Acute post-streptococcal GN.
104 Acute Post-Streptococcal Glomerulonephritis Case presentation Due to worsening renal function, we performed renal biopsy, which confirmed the above diagnosis. Patient was treated with diuretic and ace inhibitor. Patient s condition improved and he was discharged with followup in renal clinic.
105 Acute Post-Streptococcal Glomerulonephritis Case presentation His creatinine normalized after 1 mo. After 4 months, he was off antihypertensives, however his UA still showed 3+ blood and 2+ protein. He was lost to follow-up since that visit.
 GN Definition: acute")

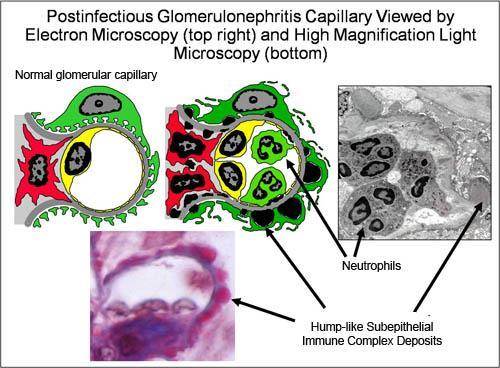
106 Acute Proliferative (Poststreptococcal, Postinfectious) GN Definition: acute nephritic syndrome that develops following infection by nephritogenic strains of strep or other organisms
107 Acute Proliferative (Poststreptococcal, Postinfectious) GN Epidemiology and ethiology: Most common GN in children Incidence declines with age Usually 1 4 weeks post infection casued by nephritogenic strains of strep (usually group A strep) Also reported with pneumococcal and staphylococcal infections, some viral diseases (mumps, measles, chickenpox, and hepatitis B and C).
108 Acute Proliferative (Poststreptococcal, Postinfectious) GN Clinical features: history of infection 1-4 wks prior abrupt onset of nephritic syndrome oliguria hematuria (tea-colored urine) edema hypertension azotemia
 titers in")
109 Acute Proliferative (Poststreptococcal, Postinfectious) GN urinalysis usually reveals proteinuria, red cells, white cells, and casts High antistreptolysin O (ASO) titers in poststreptococcal cases
 activation.")
110 Acute Proliferative (Poststreptococcal, Postinfectious) Glomerulonephritis Pathogenesis: Deposition of immune complexes in capillary loops, with complement (C3) activation. Implicated are planted antigens, like endostreptosin and nephritis-associated plasmin receptor.
111

112 Acute Proliferative (Poststreptococcal, Postinfectious) GN Pathology: light microscopy: enlarged, hypercellular glomeruli with endothelial and mesangial cell proliferation. Neutrophils may be present. Crescents may be seen.


113 Acute Proliferative (Poststreptococcal, Postinfectious) GN
114 Acute Proliferative (Poststreptococcal, Postinfectious) GN Immunofluorescence microscopy: coarsely granular ( lumpy-bumpy ) pattern along capillary loops.


115 Acute Proliferative (Poststreptococcal, Postinfectious) GN Electron microscopy: subepithelial "hump-like" deposits.

116 Acute Proliferative (Poststreptococcal, Postinfectious) GN
117 Acute Proliferative (Poststreptococcal, Postinfectious) GN Treatment: supportive Diuretics Antihypertensives Antibiotics do not change course in post-strep GN Prognosis: majority (especially children) become clinically asymptomatic some may develop rapidly progressive GN adults can progress to chronic GN

118 Now let s see if you ve been paying attention
119 This IF staining pattern is most likely to be seen in: A. RPGN B. Membranous nephropathy C. IgA nephropathy D. FSGS

120 This IF staining pattern is most likely to be seen in: A. RPGN B. Membranous nephropathy C. IgA nephropathy D. FSGS
121 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Focal Segmental Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Nodular Glomerulosclerosis Membranous Nephropathy Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Diabetic Nephropathy, Amyloidosis Membranous Nephropathy MPGN IgA Nephropathy Post-infections (Post-Strep) GN Rapidly Progressive GN (RPGN) Nephritic
122 Classification of pathologic and clinical manifestations of glomerular injury Histopathologic name Minimal Change Disease Focal Segmental Glomerulosclerosis Nephrotic Clinical name Minimal Change Disease FSGS, HIV nephropathy Nodular Glomerulosclerosis Membranous Nephropathy Membranoproliferative GN Mesangioproliferative GN Proliferative GN Crescentic GN Diabetic Nephropathy, Amyloidosis Membranous Nephropathy MPGN IgA Nephropathy Post-infections (Post-Strep) GN Rapidly Progressive GN Rapidly Progressive GN (RPGN) Nephritic

123 Rapidly Progressive Glomerulonephritis Case presentation Carlisle is a 50 year old Caucasian male who is transferred from outside hospital for rapidly progressive renal failure with hematuria and proteinuria.
124 Rapidly Progressive Glomerulonephritis Case presentation He was very fit and healthy until several weeks prior to admission, when he developed a protracted upper respiratory illness requiring several visits to PCP and emergency rooms and several courses of antibiotics.
125 Rapidly Progressive Glomerulonephritis Case presentation He was finally admitted after he was found to have bilateral pulmonary infiltrates, gross hematuria and elevated creatinine. His condition deteriorated and he required mechanical ventilation for acute respiratory failure. Bronchoscopy was consistent with pulmonary hemorrhage.
126 Rapidly Progressive Glomerulonephritis Case presentation His renal function deteriorated and he was started on hemodialysis. His C-ANCA were positive at high titer. Kidney biopsy was performed and showed crescentic pauci-immune glomerulonephritis. Diagnosis: Granulomatosis with polyangiitis, with alveolar hemorrhage and rapidly progressive glomerulonephritis.
127 Rapidly Progressive Glomerulonephritis Case presentation Clinical course: He was treated with intravenous steroids, cyclophosphamide and plasmapheresis with gradual improvement in respiratory and renal function. He recovered completely.
128 Rapidly Progressive Glomerulonephritis Definition: acute nephritic syndrome associated with rapidly deteriorating renal function (over weeks). Histopathologically this is crescentic GN. Ethiology: 1. Anti-GBM disease 2. Immune complex-mediated crescentic GN (any GN that has gone severe - lupus nephritis, post-infectious GN, IgA nephropathy) 3. Pauci-immune GN (vasculitic diseases Granulomatosis with Polyangiitis, Microscopic Polyangiitis)
129 Rapidly Progressive (Crescentic) Glomerulonephritis Clinical features: Rapid and progressive loss of renal function with severe oliguria and death within weeks to months in untreated cases. Treatment: heavy immunosuppression with steroids and cytotoxic agents (cyclophosphamide, mycophenolate), many times plasmapheresis is used to remove anti-gbm antibodies quickly Prognosis: May be related to the number of crescents; those with >80% crescents do more poorly. Recurrence post-transplant is unusual.

130 Rapidly Progressive (Crescentic) Glomerulonephritis

131 Rapidly Progressive (Crescentic) Glomerulonephritis, LM
132 Crescentic GN is a histopathologic equivalent for RPGN Type I Anti-GBM disease Type II Immune-complex GN Type III Pauci-immune GN

133 Anti-GBM Disease, pathogenesis

134 Anti-GBM Disease

135 IF reveals linear (not granular) deposition of IgG and C3 along the GBM EM shows no deposits Anti-GBM Disease

136 Anti-GBM Disease


137 In some cases IgG and C3 may also bind the pulmonary alveolar capillary basement membranes, producing a syndrome (Goodpasture s syndrome) of pulmonary hemorrhage and renal failure. Anti-GBM Disease

138 Crescentic GN type II, Immune-Complex- Mediated GN May be associated with any immune-complex type GN including SLE, IgA nephropathy, or postinfectious GN.


139 Immune-Complex-Mediated Crescentic GN IF will reveal a coarse, granular or lumpy-bumpy staining pattern. Treatment is directed at the underlying disease. Linear Granular

140 Immune-Complex-Mediated Crescentic GN EM usually shows deposits

141 Crescentic GN type III, Pauci-Immune GN Pauci-immune GN shows no antibodies or immune-type complexes in the kidney either by IF or EM. Diagnostic antibodies are in the plasma, and are called Anti-Neutrophil Cytoplasmic Antibodies (ANCA) C-ANCA P-ANCA
, Microscopic Polyangiitis (MPA), or other vasculitic")
142 Pauci-Immnune GN Feature of Granulomatosis with Polyangiitis (GPA), Microscopic Polyangiitis (MPA), or other vasculitic diseases.
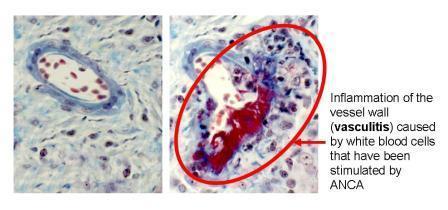
143 Pauci-immune GN
 Pathogenesis Anti-GBM Ab to type IV collagen")


144 Crescentic GN (RPGN) Anti-GBM GN (I) Immune-complex GN (II) Pauci-immune GN (III) Pathogenesis Anti-GBM Ab to type IV collagen Circulating immune complexes Ab against neutrophils (ANCA) Clinical examples Goodpastures Disease Severe Lupus Nephritis, severe Post-Strep GN LM Crescents Crescents Crescents Granulomatosis with Polyangiitis, Microscopic Polyangiitis IF Linear IgG Granular Negative EM No deposits Deposits No deposits

145 Now let s see if you ve been paying attention
146 Which statement regarding the disease depicted on electron micrograph below is INCORRECT: A. This disease has poor prognosis B. This disease is treated in supportive fashion with diuretics and antihypertensives C. Light microscopy would show proliferative GN

147 Which statement regarding the disease depicted on electron micrograph below is INCORRECT: A. This disease has poor prognosis B. This disease is treated in supportive fashion with diuretics and antihypertensives C. Light microscopy would show proliferative GN
148 Chronic Glomerulonephritis (CRGN)

149 Chronic Glomerulonephritis (CRGN) Case presentation Emmett is a 25 year old student with history of HTN self-referred to renal clinic to have his kidneys checked.
150 Chronic Glomerulonephritis (CRGN) Case presentation He reports that he was seen by a private nephrologist in town 2 years prior and had a kidney biopsy, which showed chronic changes. He did not have insurance and could not afford to pay medical bills, therefore he has not followed up. He is not taking any medications.
151 Chronic Glomerulonephritis (CRGN) Case presentation Patient is asymptomatic PE: BP170/110, trace LE edema. Labs BUN 55, creatinine 6.2 UA 3+ protein, 5 rbcs per hpf, and some broad granular casts. Renal ultrasound: 8.5 cm kidneys bilaterally with thin echogenic cortex. Diagnosis: chronic glomerulonephritis


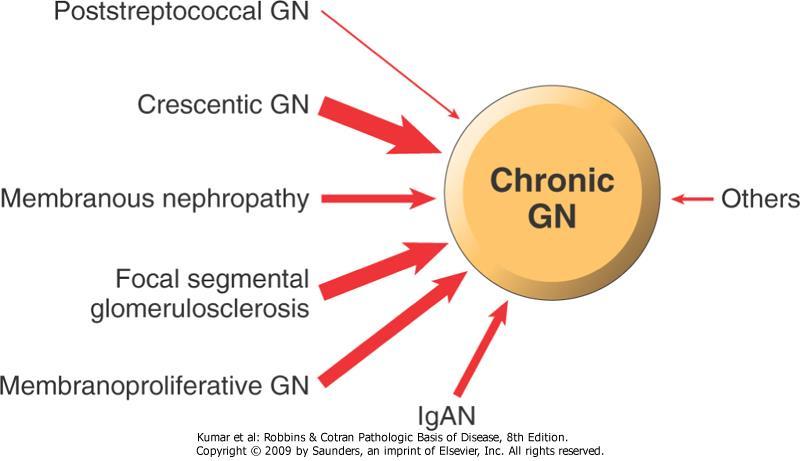
152 Chronic Glomerulonephritis (CRGN) Pathology: kidneys are grossly shrunken, and microscopically show significant and widespread global glomerular sclerosis, with interstitial fibrosis and tubular atrophy, endstage kidney.
153 Chronic Glomerulonephritis (CRGN) Epidemiology: an important cause of endstage renal disease. It is usually first noted in young to middle-age adults. Pathogenesis: usually at time of diagnosis, glomerular changes of CRGN are so far advanced that determination of exactly how they became sclerotic is impossible to work out. It may therefore be the end-stage of such processes as FSGS, MGN, RPGN, or MPGN.
154 Chronic Glomerulonephritis (CRGN) Clinical features : usually insidious onset, and discovered late in its course with renal insufficiency. Patients usually have edema, HTN and heavy proteinuria.
155 Chronic Glomerulonephritis (CRGN) Treatment Control of BP Use of ACE inhibitor Control of hyperlipidemia Avoidance of other nephrotoxic substances Cessation of smoking

156 Chronic Glomerulonephritis (CRGN) Prognosis: poor renal prognosis and patient needs to be prepared for dialysis or kidney transplantation

157 Now let s see if you ve been paying attention
158 Look at biopsy slides below. Which statement about this disease is INCORRECT: A. Plasmapheresis should be started to remove circulating antibodies B. This disease can be associated with pulmonary hemorrhage C. This disease is associated with Antinuclear Cytoplasmic antibodies (ANCA) D. This disease clinically presents as RPGN

 D.")
159 Look at biopsy slides below. Which statement about this disease is INCORRECT: A. Plasmapheresis should be started to remove circulating antibodies B. This disease can be associated with pulmonary hemorrhage C. This disease is associated with Antinuclear Cytoplasmic antibodies (ANCA) D. This disease clinically presents as RPGN

160 THE END YOU MADE IT!
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Membranoproliferative Glomerulonephritis
 Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
ACUTE GLOMERULONEPHRITIS. IAP UG Teaching slides
 ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
Glomerulonephritis. Dr Rodney Itaki Anatomical Pathology Discipline.
 Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephritic vs. Nephrotic Syndrome
 Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s. Part 1: Clinical
 Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
NEPHRITIC SYNDROME. By Dr Mai inbiek
 NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
Lab 3, case 1. Is this an example of nephrotic or nephritic syndrome? Why? Which portion of the nephron would you expect to be abnormal?
 Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi
 Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
Mr. I.K 58 years old
 Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications.
 Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
GLOMERULONEPHRITIS BRRH Grand Rounds January 12, 2016
 GLOMERULONEPHRITIS BRRH Grand Rounds January 12, 2016 Wayne R. Kotzker, M.D. Renal Electrolyte & Hypertension Consultants of South Florida Affiliate Assistant Professor of Clinical Biomedical Sciences,
GLOMERULONEPHRITIS BRRH Grand Rounds January 12, 2016 Wayne R. Kotzker, M.D. Renal Electrolyte & Hypertension Consultants of South Florida Affiliate Assistant Professor of Clinical Biomedical Sciences,
Objectives. Glomerular Diseases. Glomerulonephritis. Microscopic Hematuria 11/6/2016. Discuss diagnosis of glomerular diseases
 Glomerular Diseases in Primary Care Sadiq Ahmed, MD, FACP, FASN Associate Professor of Medicine Division of Nephrology Bone & Mineral Metabolism University of Kentucky Objectives Discuss diagnosis of glomerular
Glomerular Diseases in Primary Care Sadiq Ahmed, MD, FACP, FASN Associate Professor of Medicine Division of Nephrology Bone & Mineral Metabolism University of Kentucky Objectives Discuss diagnosis of glomerular
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
29 Glomerular disease: an overview
 29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
Secondary IgA Nephropathy & HSP
 Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Nephrotic syndrome Dr.Basma Adel FIFTH GRADE
 Nephrotic syndrome Dr.Basma Adel FIFTH GRADE 2017-2018 At the end of this lecture you should know: Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. 12/3/2017
Nephrotic syndrome Dr.Basma Adel FIFTH GRADE 2017-2018 At the end of this lecture you should know: Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. 12/3/2017
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome
 P a g e 1 DEFINITION Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome Definition: nephrotic syndrome is a disorder characterized by heavy proteinuria with hypoprpteinimia,hyper lipidemia and edema. It
P a g e 1 DEFINITION Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome Definition: nephrotic syndrome is a disorder characterized by heavy proteinuria with hypoprpteinimia,hyper lipidemia and edema. It
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Lupus Related Kidney Diseases. Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017
 Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Glomerular Disease. January 16, Katharine Dahl, MD
 Glomerular Disease January 16, 2018 Katharine Dahl, MD kdahl@akdhc.com Glomerular Disease Nomenclature Diffuse >50% glomeruli ---- Focal
Glomerular Disease January 16, 2018 Katharine Dahl, MD kdahl@akdhc.com Glomerular Disease Nomenclature Diffuse >50% glomeruli ---- Focal
Nephrotic syndrome in children. Bashir Admani KPA Nephrology Precongress 24/4/2018
 Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
AN APPROACH TO HEMATURIA. Dr Saima Ali
 AN APPROACH TO HEMATURIA Dr Saima Ali Definition Microscopic hematuria hematuria is defined as the presence of 5 or more RBCs per high-power field in 3 of 3 consecutive centrifuged specimens obtained at
AN APPROACH TO HEMATURIA Dr Saima Ali Definition Microscopic hematuria hematuria is defined as the presence of 5 or more RBCs per high-power field in 3 of 3 consecutive centrifuged specimens obtained at
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS
 GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive Nephrotic Syndrome
 J Korean Med Sci 2009; 24 (Suppl 1): S44-9 ISSN 1011-8934 DOI: 10.3346/jkms.2009.24.S1.S44 Copyright The Korean Academy of Medical Sciences Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive
J Korean Med Sci 2009; 24 (Suppl 1): S44-9 ISSN 1011-8934 DOI: 10.3346/jkms.2009.24.S1.S44 Copyright The Korean Academy of Medical Sciences Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
CASE OF THE WEEK 1
 www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG)
") Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
NEPHROTIC SYNDROME. Presents with the classic tetrad of nephrotic syndrome. Massive proteinuria (>3. 5 g/d) Hypoalbuminemia Edema Hyperlipidemia
 Hypoalbuminemia Edema Hyperlipidemia") PATHOLOGY OF GLOMERULAR DISEASES Disease Etiology Pathophysiology and Clinical Presentation Urinalysis in Nephrotic Syndrome NML excretion: 150 mg/d : < 0.15 g total protein/g urine creatinine Nephrosis
PATHOLOGY OF GLOMERULAR DISEASES Disease Etiology Pathophysiology and Clinical Presentation Urinalysis in Nephrotic Syndrome NML excretion: 150 mg/d : < 0.15 g total protein/g urine creatinine Nephrosis
DIABETES MELLITUS. Kidney in systemic diseases. Slower the progression: Pathology: Patients with diabetes mellitus are prone to other renal diseases:
 Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy?
 CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
Proteinuria Nephrotic syndrome
 Proteinuria Nephrotic syndrome Pathophysiology & management Miriam Davidovits, MD Institute of Nephrology Schneider Children s Medical Center of Israel 1 Abnormal excretion of protein into the urine is
Proteinuria Nephrotic syndrome Pathophysiology & management Miriam Davidovits, MD Institute of Nephrology Schneider Children s Medical Center of Israel 1 Abnormal excretion of protein into the urine is
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Clinical pathological correlations in AKI
 Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Nephrotic Syndrome. Department of pediatrics The first affiliated hospital Sun Yat Sen University. Yue Zhihui ( 岳智慧 )
") Nephrotic Syndrome Department of pediatrics The first affiliated hospital Sun Yat Sen University Yue Zhihui ( 岳智慧 ) yuezhihui810@yahoo.com.cn Contents Definition Pathophysiology Clinical manifestation
Nephrotic Syndrome Department of pediatrics The first affiliated hospital Sun Yat Sen University Yue Zhihui ( 岳智慧 ) yuezhihui810@yahoo.com.cn Contents Definition Pathophysiology Clinical manifestation
Dr P Sigwadi 30 May 2012
 Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Tuesday Conference 7/23/2013. Hasan Fattah
 Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Alterations of Renal and Urinary Tract Function
 Alterations of Renal and Urinary Tract Function Chapter 29 Urinary Tract Obstruction Urinary tract obstruction is an interference with the flow of urine at any site along the urinary tract The obstruction
Alterations of Renal and Urinary Tract Function Chapter 29 Urinary Tract Obstruction Urinary tract obstruction is an interference with the flow of urine at any site along the urinary tract The obstruction
Proteinuria Nephrotic syndrome
 Proteinuria Nephrotic syndrome Pathophysiology & management Miriam Davidovits, MD Institute of Nephrology Schneider Children s Medical Center of Israel 1 Abnormal excretion of protein into the urine is
Proteinuria Nephrotic syndrome Pathophysiology & management Miriam Davidovits, MD Institute of Nephrology Schneider Children s Medical Center of Israel 1 Abnormal excretion of protein into the urine is
Acute Kidney Injury. I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS
 Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
ESRD Dialysis Prevalence - One Year Statistics
 Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Post-infectious (bacterial) Glomerulonephritis
 Glomerulonephritis") Far East Regional Conference Russia Dialysis Society Khabarovsk, Russia October 30, 2015 Post-infectious (bacterial) Glomerulonephritis (An Update) William Couser, MD Affiliate Professor of Medicine University
Far East Regional Conference Russia Dialysis Society Khabarovsk, Russia October 30, 2015 Post-infectious (bacterial) Glomerulonephritis (An Update) William Couser, MD Affiliate Professor of Medicine University
LECTURE IN INTERNAL MEDICINE PROPAEDEUTICS 2017/2018
 SIGNS AND SYMPTOMS OF URINARY SYSTEM DISEASES (urinary syndrome, nephrotic syndrome, nephritic syndrome, urinary tract obstruction syndrome, hypertensive syndrome) LECTURE IN INTERNAL MEDICINE PROPAEDEUTICS
SIGNS AND SYMPTOMS OF URINARY SYSTEM DISEASES (urinary syndrome, nephrotic syndrome, nephritic syndrome, urinary tract obstruction syndrome, hypertensive syndrome) LECTURE IN INTERNAL MEDICINE PROPAEDEUTICS
Proteinuria DR. SANJAY PANDEYA MD. FRCPC.
 Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
1. SIGNIFICANCE 2. PREREQUISITES
 Topic 13: Differential diagnosis of glomerulonephritis in children. Differential approach to treatment of glomerulonephritis in children. Thematic chapter: Differential diagnosis of the most common diseases
Topic 13: Differential diagnosis of glomerulonephritis in children. Differential approach to treatment of glomerulonephritis in children. Thematic chapter: Differential diagnosis of the most common diseases
substance staining with IgG, C3 and IgA (trace) Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ
 Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ") Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Nephrotic Syndrome. Sara Alsharhan PharmD candidate, KSU 2014
 Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
 C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis with Monoclonal Immunoglobulin Deposits of Lambda Light Chain
 Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Evaluation and Management of Proteinuria. Negiin Pourafshar, MD University of Virginia Division of Nephrology
 Evaluation and Management of Proteinuria Negiin Pourafshar, MD University of Virginia Division of Nephrology Case A 30-year-old man, is turned down for life insurance because of the presence of an unspecified
Evaluation and Management of Proteinuria Negiin Pourafshar, MD University of Virginia Division of Nephrology Case A 30-year-old man, is turned down for life insurance because of the presence of an unspecified
Primary Nephrotic Syndrome. Mao Jianhua, Department of Nephrology, The Children s Hospital of Zhejiang University School of Medicine
 Primary Nephrotic Syndrome Mao Jianhua, Department of Nephrology, The Children s Hospital of Zhejiang University School of Medicine Introduction Nephrotic syndrome is a group of symptoms including proteins
Primary Nephrotic Syndrome Mao Jianhua, Department of Nephrology, The Children s Hospital of Zhejiang University School of Medicine Introduction Nephrotic syndrome is a group of symptoms including proteins
GOOD MORNING. Welcome Applicants! Friday, October 31, (Happy Halloween!)
") GOOD MORNING Welcome Applicants! Friday, October 31, 2014 (Happy Halloween!) PREP QUESTION A 14-year-old girl has had 3 days of new, unremitting headache associated with vomiting and awakening from sleep
GOOD MORNING Welcome Applicants! Friday, October 31, 2014 (Happy Halloween!) PREP QUESTION A 14-year-old girl has had 3 days of new, unremitting headache associated with vomiting and awakening from sleep
Proteinuria. Louisiana State University
 Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, ; doi: /kisup.2012.
 2, ; doi: /kisup.2012.") http://www.kidney-international.org chapter 6 & 2012 KDIGO Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, 181 185; doi:10.1038/kisup.2012.19
http://www.kidney-international.org chapter 6 & 2012 KDIGO Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, 181 185; doi:10.1038/kisup.2012.19
PATHOLOGY OF THE URINARY SYSTEM Dr. Ameer Dhahir Part one
 PATHOLOGY OF THE URINARY SYSTEM Dr. Ameer Dhahir Part one Objectives: Defining certain clinical terms related to urinary disorders. Describing the pathogenesis of glomerular diseases Defining certain clinical
PATHOLOGY OF THE URINARY SYSTEM Dr. Ameer Dhahir Part one Objectives: Defining certain clinical terms related to urinary disorders. Describing the pathogenesis of glomerular diseases Defining certain clinical
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab
 TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
INTRODUCTION TO GLOMERULAR DISEASES
 INTRODUCTION TO GLOMERULAR DISEASES Goal: to explain the general mechanisms leading to glomerular diseases and to analyze what is known about their relationship to morphologic and clinical manifestations
INTRODUCTION TO GLOMERULAR DISEASES Goal: to explain the general mechanisms leading to glomerular diseases and to analyze what is known about their relationship to morphologic and clinical manifestations
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
considered for patients with cryoglobulinemic kidney diseases. (Weak)
") http://www.kidney-international.org & 2008 DIGO Guideline 5: Diagnosis and management of kidney diseases associated with HCV infection idney International (2008) 73 (Suppl 109), S69 S77; doi:10.1038/ki.2008.88
http://www.kidney-international.org & 2008 DIGO Guideline 5: Diagnosis and management of kidney diseases associated with HCV infection idney International (2008) 73 (Suppl 109), S69 S77; doi:10.1038/ki.2008.88