GRAND ROUNDS
|
|
|
- Helena Stevenson
- 6 years ago
- Views:
Transcription
1 GRAND ROUNDS
2 CASE 64 y.o AAF with h/o HTN, DM, HLD, MGUS referred by PMD for uncontrolled resistant hypertension, new renal failure (Cr of 1.5), hematuria and proteinuria Per patient systolic BP in last 3 months in the range of 200s to 250s requiring multiple antihypertensives LE swelling for last 3 months Periorbital swelling and facial puffiness on waking up Decrease exercise tolerance, DOE, orthopnea, fatigue Noted urine to be frothy but denied increased frequency and hematuria ROS: Negative for fever, chills, chest pain, cough, headache, blurry vision, arthralgias, myalgias, rash, recent infections
3 PMHx HTN DM HLD MGUS( dx in 2011) Meds: ASA 81 mg, Losartan 100 mg daily, Chlorthalidone 25 mg daily, Simvastatin 80 mg daily, Atenolol 75 mg daily FHx: HTN and DM SHx: Denies smoking or recreational drug use. Occassional Etoh
4 PE: VS: 194/85 HR 83 RR 20 T 97.7 So2 99% HEENT: pale conjunctiva, sclera anicteric, periorbital edema Lungs: L left basilar rales Heart: RRR, normal S1S2 Abd: soft, nt, nd, bs+ve LE: 2+ pitting edema up to knees b/l Skin: no rashes
5 D#1 D#2 D#4 D#5 D#6 D# 7 D#8 D#9 Na K Cl CO BUN Cr Ca HB 10.5 WBC 5.4 PLT 207 AST 28 ALT 15 Alk phos 97 TP 5.4 albumin 2.8 LDL 178 Chol 287 HDL 86 TG 116 LDL 178 UA: 2+ blood, 3+ protein, RBC 10-15, no RBC casts Up/c 5.69 g/g
6 Hep C Ab reactive Hep B sag non reactive Hep B sab non reactive C C RF <10.8 c-anca neg p-anca neg ANA neg Kappa mg/l Lambda mg/l /2012 2/7/ k/l SPEP bands with restricted gamma mobility UPEP 2/2011 Free kappa and lambda light chains Serum Immunofixation 2/ monoclonal IgG lambda bands 2/ IgG lambda monoclonal protein bands 2 faint IgA monoclonal bands without corresponding light chains Urine immunofixation 2/2013 albumin and other serum proteins with one distinct and faint peak in gamma region
7 Renal Ultrasound Right kidney 9.9 cm left kidney 10.2 cm Increased echogenicity Few right renal cysts the largest 15 x11 mm in the mid pole There is no hydronephrosis or calculi
8 CXR: cardiomegaly, no effusions 2 D echo: Concentric LVH ef 65%, impaired relaxation pattern, small pericardial effusion, epicardial thickening
9 DIFFERENTIAL DIAGNOSIS Nephrotic syndrome, hypertension, renal insufficiency FSGS Amyloidosis MIDD MPGN Thrombotic microangiopathy
10 IF - 3 glomeruli with nodular sclerosis - There is linear GBM, bowmans capsule and tubular BM staining for lambda EM - 2 glomeruli with nodular sclerosis - GBM within normal thickness -No subepithelial or sub endothelial immune complex deposits -Near complete foot process effacement -Marked increase in mesangial matrix in a nodular pattern -Tubular basements ate thickened and show focal -No evidence of amyloid fibrils
11 RENAL BIOPSY Diagnosis: Light Chain deposition disease LM: 4/38 glomeruli globally sclerotic -Diffuse, moderate to marked increase increase in mesangial matrix and cellularity in a nodular pattern -Glomeruli show lobular pattern -GBM appear irregular with focal corrugation and splitting -There is endocapillary hypercellularity -Arterioles show mild hyalinosis, Interlobular arteries show very mild intimal fibrosis -Congo red stain for amyloid negative
12 LIGHT CHAIN DEPOSITION DISEASE LCDD is one manifestation of monoclonal immunoglobulin deposition disease in the kidney, first reported in 1973 and confirmed by Randall et al who published in 1976 the first description of LCDD The incidence of LCDD in patients with plasma cell dyscrasia is approximately 5% Nodular glomerulosclerosis is the classical lesion in LCDD Mesangial nodularity results from increased deposition of extracellular matrix proteins and monotypic light chains most commonly kappa Deposits are neither fibrillar nor congo red positive Ultrastructurally deposits are seen as punctate granular electron dense material, which is typically present in subendothelial glomerular areas and in the mesangium.
13 CLINICAL FEATURES OF LCDD MIDD most often occur in the sixth and seventh decades of life, but patients in 20s and 90s have been reported Renal involvement is a constant feature and renal failure often dominate the clinical presentation Nephrotic syndrome in 30-50% of cases proteinuria <1 g/day in 25% Hematuria 29-67% Hypertension is variable 60% of cases progress to ESRD J Am Soc Nephrol 12: , 2001
14 Extrarenal manifestations- Liver and cardiac involvement are the most common Hepatomegaly with mild alterations in LFT s are the most usual presentation, but several patients develop hepatic insufficiency and portal hypertension, and of them die of hepatic failure Cardiac manifestations include restrictive cardiomyopathy and MI from light chain deposition in the coronary vasculature Other manifestations include cerebral infarction and hemorrhage, peripheral neuropathy and mononeuritis muliplex. Adrenal insufficiency has also been reported J Am Soc Nephrol 12: , 2001

15 LIGHT CHAIN STRUCTURE An Ig molecule consists of 2 heavy chains and 2 light chains 2 light chain isotypes К and λ 9 heavy chain isotypes Each contain constant and variable region Variable region of each light chain and heavy chain pair constitutes the antigen binding sites Each LC contains 220 amino acids and has a molecular weight of 25kDa There is little variation within the constant regions of the К and λ light chains Variable region of a light chain comprises of four framework region that form a hydrophobic core within which are scattered three hypervariable sequences called complementary determining regions (CDR1 CDR2 CDR3) These regions of Ig chains are encoded by numerous gene segments, the rearrangement of which occurs during the B cell differentiation HC express six VH subgroups, К chain express four Vk subgroups and λ chains express six Vλ subgroups.
16 LIGHT CHAIN PRODUCTION, DISTRIBUTION AND RENAL HANDLING Approximately 500 mg of free light chains is produced by the normal lymphoid system 80% of FLC is extravascular Two thirds of light chain production is kappa ( К/λ 1.8:1) Light chains are filtered and catabolized by the kidney in proximal tubule, such that only approximately 1 to 10 mg of polyclonal light chains normally appear in the urine Internalization in PTECs occurs through rapid and saturable megalin and cubilin receptor mediated endocytosis in clathrin coated pits
17 WHY DO SOME CLONAL FLC CAUSE KIDNEY INJURY FLCs isolated from patients with PCD and renal injury have a greater potential to self aggregate and form higher molecular weight aggregates under physiological conditions than FLCs from patients with PCD but without kidney injury Mice injected with FLCs from patients with renal lesions developed similar renal lesions to the patients indicating that specific clones of FLCs cause distinct transferrable patterns of injury In LCDD, Kappa light chains occur in approximately 80% of cases. VКIV variability subgroup was overrepresented in patients with LCDD. This subgroup features a longer CDR1 loop that contains some hydrophobic residues

18 Data in this study support a single receptor present on mesangial cells for both LCDD and AL- LCs This receptor resides in the caveolae present on the plasma membrane of HMCs and is overexpressed when HMCs are incubated with G-LCs not tubulopathic LCs


19 HMCs incubated with G-LCs


20 HMC simultaneously incubated with AL and LCDD- LCs Colocalization of G-LC with clathrin



21 Colocalization of internalized AL-LC with LAMP Expression of Rabs 7and 9 Internalization of AL-LC in HMCs

22 Dynamic(real time) studies AL- LCs were delivered to the Mature lysosomal system
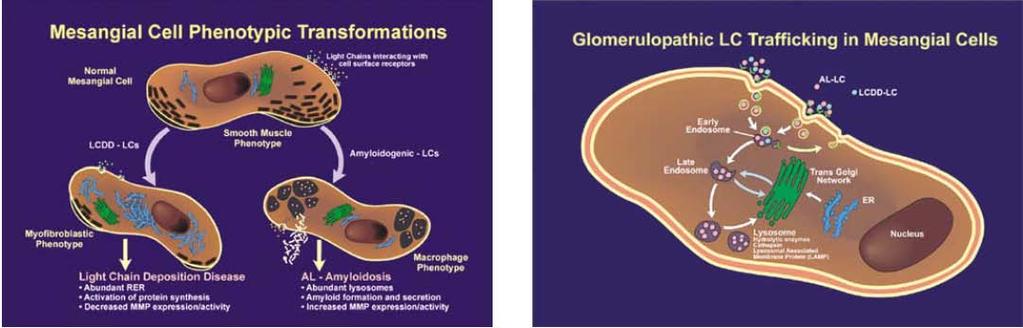
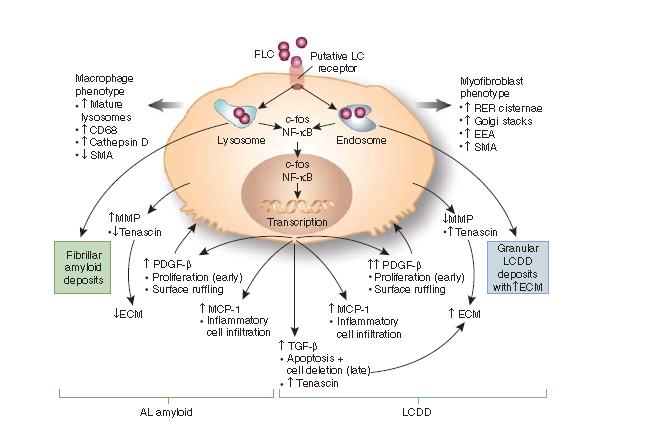
23 HMCs are injured by abnormal light chains with plasma cell dyscrasia. Consequently these mesangial cells undergo phenotypic transformation
24
25

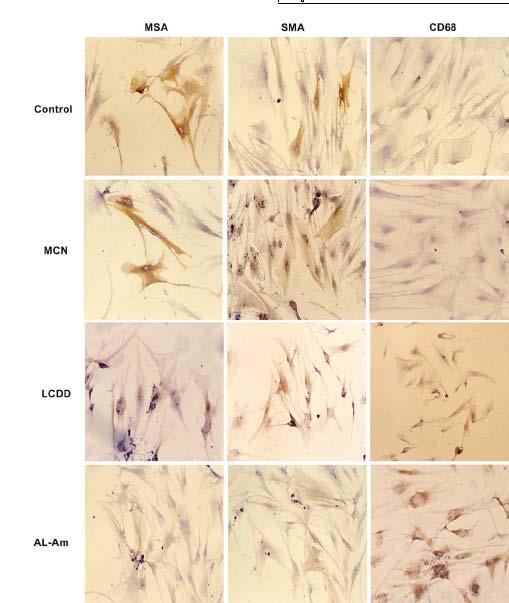
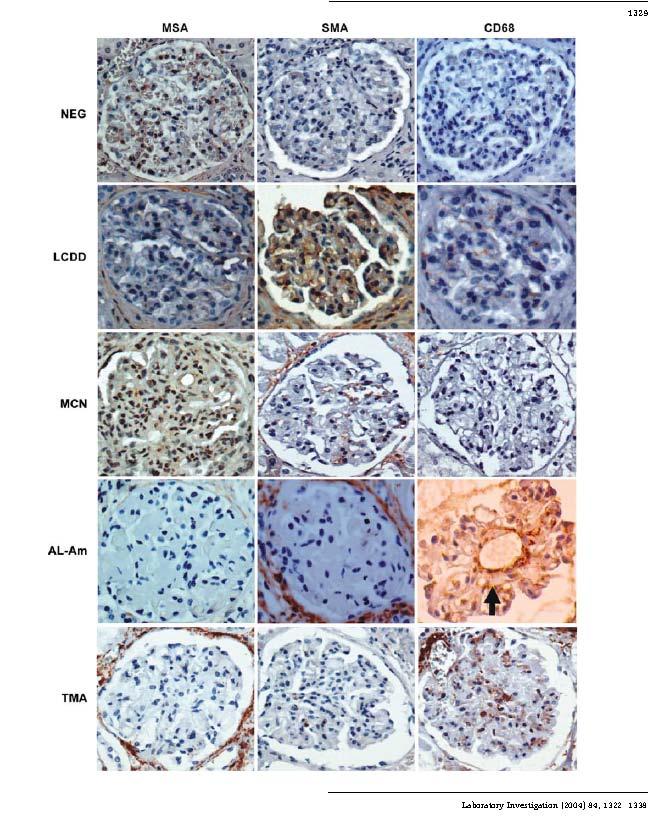
26 HMCs growing on matrigel matrix and incubated with AL-AM LCx for 96h


27 HMCs treated with AL-AM LCs and probed with lysosensor HMCs treated with various LCs and probed with ER tracker
28
29
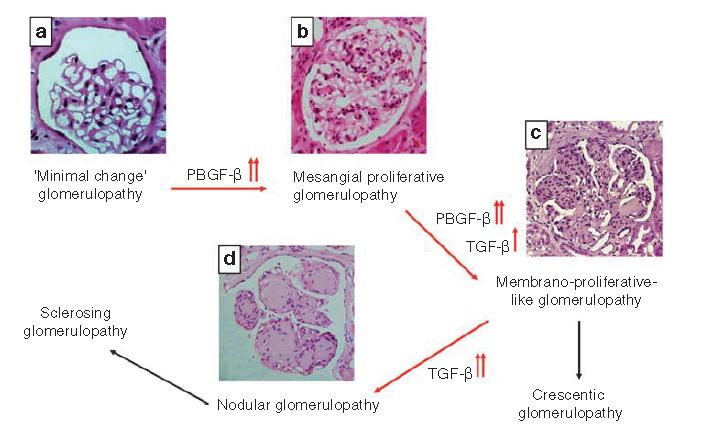
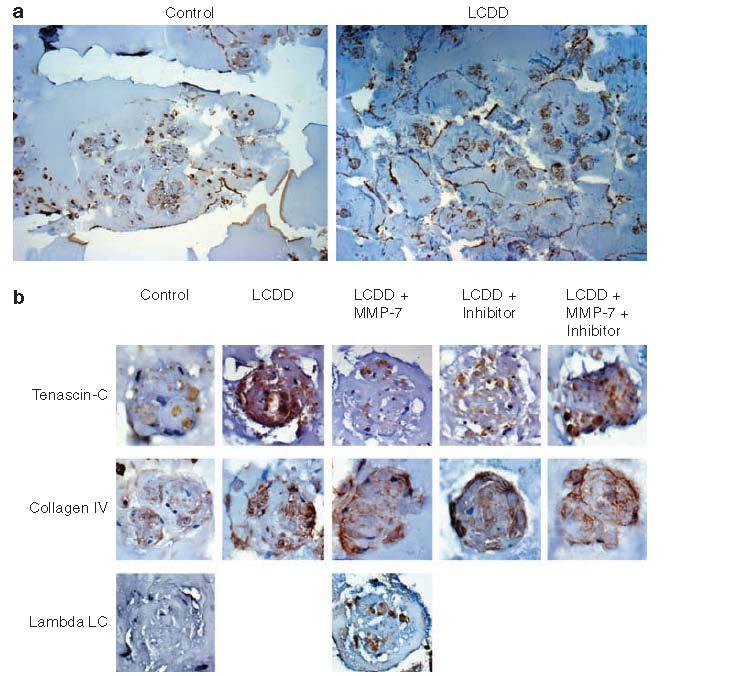
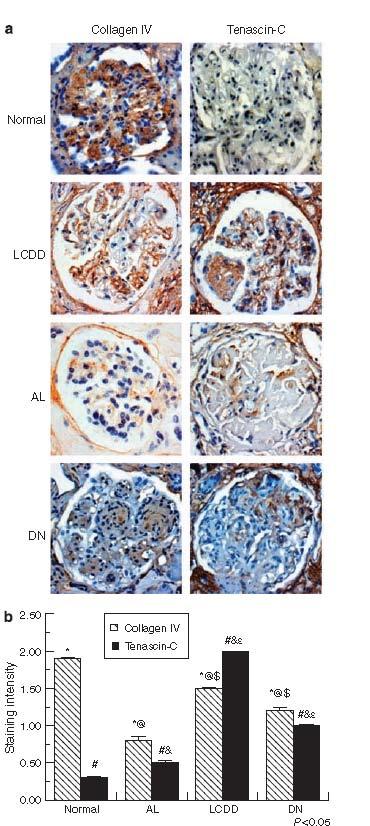
30 Nodular glomerulosclerosis results from increased deposition of extracellular matrix proteins and monotypic light chains Inability of mesangial cells to degrade abnormal levels of Tenascin C-along with increased expression of some growth factors such as PDGF and TGF-ß is crucial to the pathogenesis of LCDD
31
32 PDGF-B expression in conditioned media Obtained from HMCs treated with different types of light chains TGF-B expression in conditioned media obtained from HMCs treated with different types of light chains
33
34
35

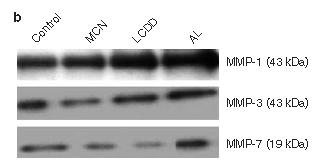
36 MMP-1, -3,-7 expressions in HMCs
Clinical Case Presentation. Dana Assis, MD
 Clinical Case Presentation Dana Assis, MD 4.12.2016 Clinical Presentation 63 year old male with medical history AIDS (CD4 11, VL 62K), Hep C cirrhosis (never treated), DM II c/b diabetic retinopathy, HTN,
Clinical Case Presentation Dana Assis, MD 4.12.2016 Clinical Presentation 63 year old male with medical history AIDS (CD4 11, VL 62K), Hep C cirrhosis (never treated), DM II c/b diabetic retinopathy, HTN,
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME
 CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
Jo Abraham MD Division of Nephrology University of Utah
 Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias
 Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Plasma cell dyscrasias Plasma
Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Plasma cell dyscrasias Plasma
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT
 The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
Lab 3, case 1. Is this an example of nephrotic or nephritic syndrome? Why? Which portion of the nephron would you expect to be abnormal?
 Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis with Monoclonal Immunoglobulin Deposits of Lambda Light Chain
 Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Sheena Surindran Grand Rounds 2/15/11
 Sheena Surindran Grand Rounds 2/15/11 Affects 5 12 person per million / year 5 10% associated with myeloma Median survival without treatment is 12 40 months Most commonly affected organs are kidney, heart
Sheena Surindran Grand Rounds 2/15/11 Affects 5 12 person per million / year 5 10% associated with myeloma Median survival without treatment is 12 40 months Most commonly affected organs are kidney, heart
A Case of IgG2 Heavy Chain Deposition Disease in a Patient with Kappa Positive Plasma Cell Dyscrasia
 Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
Hasan Fattah 4/30/2013
 Hasan Fattah 4/30/2013 49 yo hispanic male, ho HIV(CD4 229), currently on HAART, course c/b AIDS, Presents with two days ho fever, SOB, blood tinged sputum, and visible hematuria. ROS: no skin rash, joint
Hasan Fattah 4/30/2013 49 yo hispanic male, ho HIV(CD4 229), currently on HAART, course c/b AIDS, Presents with two days ho fever, SOB, blood tinged sputum, and visible hematuria. ROS: no skin rash, joint
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016
 + M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
+ M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Glomerulonephritis. Dr Rodney Itaki Anatomical Pathology Discipline.
 Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Laboratory Examination
 Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
substance staining with IgG, C3 and IgA (trace) Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ
 Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ") Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That Showed Predominantly Membranous Features
 Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
LIGHT CHAIN DISEASE B. DHANALAKSHMI 1 & V. HEMAVATHY 2
 TJPRC: International Journal of Nursing and Patient Safety & Care (TJPRC: IJNPSC) Vol. 1, Issue 1, Dec 2016, 21-24 TJPRC Pvt. Ltd. LIGHT CHAIN DISEASE B. DHANALAKSHMI 1 & V. HEMAVATHY 2 1 Associate Professor,
TJPRC: International Journal of Nursing and Patient Safety & Care (TJPRC: IJNPSC) Vol. 1, Issue 1, Dec 2016, 21-24 TJPRC Pvt. Ltd. LIGHT CHAIN DISEASE B. DHANALAKSHMI 1 & V. HEMAVATHY 2 1 Associate Professor,
Tuesday Conference 7/23/2013. Hasan Fattah
 Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Mr. I.K 58 years old
 Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Dr Ian Roberts Oxford
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Multiple Myeloma Advances for clinical pathologists & histopathologists
 Multiple Myeloma Advances for clinical pathologists & histopathologists CME in Haematology 2014 IAPP & Dept of Pathology, BVDUMC, Pune Sunday, 4 th May 2014 Dr. M.B. Agarwal, MD, MNAMS Head, Dept of Haematology
Multiple Myeloma Advances for clinical pathologists & histopathologists CME in Haematology 2014 IAPP & Dept of Pathology, BVDUMC, Pune Sunday, 4 th May 2014 Dr. M.B. Agarwal, MD, MNAMS Head, Dept of Haematology
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
MHD I SESSION X. Renal Disease
 MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
Nephritic vs. Nephrotic Syndrome
 Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Diabetic Nephropathy. Introduction/Clinical Setting. Pathologic Findings Light Microscopy. J. Charles Jennette
 12 Diabetic Nephropathy J. Charles Jennette Introduction/Clinical Setting Diabetic nephropathy is a clinical syndrome in a patient with diabetes mellitus that is characterized by persistent albuminuria,
12 Diabetic Nephropathy J. Charles Jennette Introduction/Clinical Setting Diabetic nephropathy is a clinical syndrome in a patient with diabetes mellitus that is characterized by persistent albuminuria,
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS
 MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
A case of heavy chain deposition disease complicated by acquired angioedema.
 Case Report http://www.alliedacademies.org/pathology-and-disease-biology/ A case of heavy chain deposition disease complicated by acquired angioedema. Rafia Chaudhry 1 *, Gautam Bhave 2, Rachel Fissell
Case Report http://www.alliedacademies.org/pathology-and-disease-biology/ A case of heavy chain deposition disease complicated by acquired angioedema. Rafia Chaudhry 1 *, Gautam Bhave 2, Rachel Fissell
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS. Myriam Farah, MD, FRCPC
 ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
Glomerular Diseases. Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology
 Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
Histopathology: Hypertension and diabetes in the kidney These presentations are to help you identify basic histopathological features.
 Histopathology: Hypertension and diabetes in the kidney These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need
Histopathology: Hypertension and diabetes in the kidney These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need
Diagnostic approach to cardiac amyloidosis: A case report
 Diagnostic approach to cardiac amyloidosis: A case report Georgia Vogiatzi, MD, MSc, PhD 1 st Cardiology Department, Hippokration Hospital, Athens Medical School Disclosures I have no relevant relationships
Diagnostic approach to cardiac amyloidosis: A case report Georgia Vogiatzi, MD, MSc, PhD 1 st Cardiology Department, Hippokration Hospital, Athens Medical School Disclosures I have no relevant relationships
Nephrotic Syndrome. Sara Alsharhan PharmD candidate, KSU 2014
 Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Clinical history. 73 yo man with chest pain Systemic hypertension and WG Stress EKG N Stress echocardiogram: Cardiac catheterization: no CAD
 CASE 8 Clinical history 73 yo man with chest pain Systemic hypertension and WG Stress EKG N Stress echocardiogram: Concentric hypertrophy Hypokinesis of LV-Inf Cardiac catheterization: no CAD Technique
CASE 8 Clinical history 73 yo man with chest pain Systemic hypertension and WG Stress EKG N Stress echocardiogram: Concentric hypertrophy Hypokinesis of LV-Inf Cardiac catheterization: no CAD Technique
C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
 C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
GLOMERULONEPHRITIS CLINICAL APPROACH TO GLOMERULAR DISEASE ACOI 2018
 GLOMERULONEPHRITIS CLINICAL APPROACH TO GLOMERULAR DISEASE ACOI 2018 Disclosures Nothing to declare Case 1 44 yo Caucasian woman admitted from PCP with dyspnea and HTN Has not felt well for 3-4 months
GLOMERULONEPHRITIS CLINICAL APPROACH TO GLOMERULAR DISEASE ACOI 2018 Disclosures Nothing to declare Case 1 44 yo Caucasian woman admitted from PCP with dyspnea and HTN Has not felt well for 3-4 months
Membranoproliferative Glomerulonephritis
 Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
What s hiding behind IgA nephropathy?
 What s hiding behind IgA nephropathy? Bauerova L. Department of Pathology, the First Faculty of Medicine and General Hospital, Charles University Prague (nephropathology training: Department of Clinical
What s hiding behind IgA nephropathy? Bauerova L. Department of Pathology, the First Faculty of Medicine and General Hospital, Charles University Prague (nephropathology training: Department of Clinical
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Minimal change disease (MCD) related new electron microscopy findings in a patient on Levothyroxine sodium (LT) for hypothyroidism: A case report Dr. Ali Al-Omari
Enterprise Interest Nothing to declare Minimal change disease (MCD) related new electron microscopy findings in a patient on Levothyroxine sodium (LT) for hypothyroidism: A case report Dr. Ali Al-Omari
NEPHRITIC SYNDROME. By Dr Mai inbiek
 NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
HRZZ project: Genotype-Phenotype correlation in Alport's syndrome and Thin Glomerular Basement Membrane Nephropathy. Patohistological Aspects
 HRZZ project: Genotype-Phenotype correlation in Alport's syndrome and Thin Glomerular Basement Membrane Nephropathy Patohistological Aspects Petar Šenjug, MD 1 Professor Danica Galešić Ljubanović, MD,
HRZZ project: Genotype-Phenotype correlation in Alport's syndrome and Thin Glomerular Basement Membrane Nephropathy Patohistological Aspects Petar Šenjug, MD 1 Professor Danica Galešić Ljubanović, MD,
Secondary IgA Nephropathy & HSP
 Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
2012/3/22. WBC 7400 /µl RBC /µl Hb 10.9 g/dl Plt /µl
 Case 3 A case of MPGN type 3, second form Post-meeting material onset and course He has been treated with medication against hypertension, hyperlipidemia, and hyperuricemia in clinics from 1994 (40 yrs
Case 3 A case of MPGN type 3, second form Post-meeting material onset and course He has been treated with medication against hypertension, hyperlipidemia, and hyperuricemia in clinics from 1994 (40 yrs
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
29 Glomerular disease: an overview
 29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
A Case of Immunotactoid Glomerulopathy with Rapid Progression to End-Stage Renal Disease
 Case Study TheScientificWorldJOURNAL (2009) 9, 1348 1354 ISSN 1537-744X; DOI 10.1100/tsw.2009.164 A Case of Immunotactoid Glomerulopathy with Rapid Progression to End-Stage Renal Disease Shikha Jain 1,
Case Study TheScientificWorldJOURNAL (2009) 9, 1348 1354 ISSN 1537-744X; DOI 10.1100/tsw.2009.164 A Case of Immunotactoid Glomerulopathy with Rapid Progression to End-Stage Renal Disease Shikha Jain 1,
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Light-Chain Mediated Acute Tubular Interstitial Nephritis. A Poorly Recognized Pattern of Renal Disease in Patients With Plasma Cell Dyscrasia
 Light-Chain Mediated Acute Tubular Interstitial Nephritis A Poorly Recognized Pattern of Renal Disease in Patients With Plasma Cell Dyscrasia Xin Gu, MD; Guillermo A. Herrera, MD Context. Acute renal failure
Light-Chain Mediated Acute Tubular Interstitial Nephritis A Poorly Recognized Pattern of Renal Disease in Patients With Plasma Cell Dyscrasia Xin Gu, MD; Guillermo A. Herrera, MD Context. Acute renal failure
Renal. Pathology. Kris%ne Kra*s, M.D.
 Renal Pathology Kris%ne Kra*s, M.D. Renal Pathology Outline Introductory stuff Glomerular diseases Tubular and inters%%al diseases Diseases involving blood vessels Cys%c diseases Tumors Renal Pathology
Renal Pathology Kris%ne Kra*s, M.D. Renal Pathology Outline Introductory stuff Glomerular diseases Tubular and inters%%al diseases Diseases involving blood vessels Cys%c diseases Tumors Renal Pathology
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
ACCME/Disclosure. Case #1. Case History. Dr. Bracamonte has nothing to disclose
 Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy?
 CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG)
") Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Forms Revision: Myeloma Changes
 Sharing knowledge. Sharing hope. Forms Revision: Myeloma Changes J. Brunner, PA-C and A. Dispenzieri, MD February 2013 Disclosures Janet Brunner, PA-C I have no relevant conflicts of interest to disclose.
Sharing knowledge. Sharing hope. Forms Revision: Myeloma Changes J. Brunner, PA-C and A. Dispenzieri, MD February 2013 Disclosures Janet Brunner, PA-C I have no relevant conflicts of interest to disclose.
Foamy Urine and Sickled Cells. Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA
 Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane University Health
Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane University Health
Some renal vascular disorders
 Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
29th Annual Meeting of the Glomerular Disease Collaborative Network
 29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
Proteinuria. Louisiana State University
 Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
Diabetes on Renal Biopsy-Current Appraisal
 Diabetes on Renal Biopsy-Current Appraisal Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology, retired Washington University School of Medicine St. Louis, MO BNS 2016
Diabetes on Renal Biopsy-Current Appraisal Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology, retired Washington University School of Medicine St. Louis, MO BNS 2016