Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias
|
|
|
- Derek Kelley
- 6 years ago
- Views:
Transcription




1 Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic



2 Plasma cell dyscrasias Plasma cell dyscrasias represent a clonal expansion of abnormal plasma cells which produce a monoclonal protein that could be either the whole immunoglobulin (Ig) or a fragment of Ig (monoclonal free light or heavy chain in a variable quantity). LCs are removed from circulation by the kidneys, renal damage is a common complication and can by very heterogeneous.
, together with κ or λ molecules and create immunoglobulins After binding of the")
 and change to a memory cell Second contact with antigen: IgG almost")
3 Plasma cell function Normally plasma cells, and in lesser extent some type of B-cells, produce one of five heavy chain types (G, A, M, E, D), together with κ or λ molecules and create immunoglobulins After binding of the antigen ( ), a naive B cell is changed to a plasma cell Signal to the nucleus 2-3days After 10 days there will occur IgM Switch to produce IgG (2-3 weeks) and change to a memory cell Second contact with antigen: IgG almost immediately

4 Plasma cell dyscrasias Antibody molecules are composed of two identical heavy and light chains, each containing variable and constant domains. The variable domains - form an antigen-binding site, Light chains are of two types, κ and λ, and in any given antibody molecule only one type occurs.

5 Discovery of Bence-Jones protein: who is behid it? more than 150 years ago, the presence of Bence Jones protein was discovered the first in vitro cancer test Dr. Henry Bence Jones - In 1845, Dr William MacIntyre, a physician in London, was called to see a 45 year-old patient, - general practitioner, Dr Thomas Watson - Edema- possibility of nephrosis, he tested the urine for albumin - Both Dr MacIntyre and Dr Watson then sent urine samples to the Dr. Henry Bence Jones - The patient died, Dr MacIntyre subsequently published the post-mortem examination in Henry Bence Jones had already described the patient s urinary findings in two, single-author articles (one in The Lancet, in 1847). - Bence Jones s reputation was assured, while the contributions of his colleagues a footnote in the history of medicine.
. In 1922, Bayne-Jones and Wilson characterized two types of BJ protein (using antisera).")

6 Discovery of Bence-Jones protein It had taken more than 100 years from the original observation than the features of Bence Jones protein were finally determined. Waldayer first identified - the protein originate in bone marrow plasma cells (1875). In 1922, Bayne-Jones and Wilson characterized two types of BJ protein (using antisera). The proteins were classified as group I and group II types. In 1956 Korngold and Lipari showed that antisera against the different groups also reacted with myeloma proteins. As a tribute to their observations the 2 types of BJ protein were designated: kappa and lambda. Edelman and Gally, in 1962, subsequently showed that FLCs prepared from IgG monoclonal proteins were the same as BJ protein.
7 Classification of monoclonal gammopathies, multiple myeloma (MM) and related disorders include following groups: 1.Monoclonal gammopathy of undetermined significance (MGUS) 2.Smouldering (asymptomatic) multiple myeloma 3.Symptomatic multiple myeloma 4.Nonsecretory multiple myeloma 5.Solitary plasmacytoma of bone 6.Extramedullary plasmacytoma 7.Multiple solitary plasmacytoma 8.Plasma cell leukaemia
8 Hematology classification & Several problems in daily practice nephropathology The clonal expansion of cluster of plasma cells is not only benign or malignant production of Igs or FLCs and these light chains can be deposited important facts were not incorporated in the classification schema MGUS and AL amyloidosis the term MG of renal significance The prevalence of plasma cell dyscrasias increases with advancing age Disorders associated with plasma cell dyscrasias often have NS or severe PU
9 The most frequent categories of renal diseases associated with MGUS and MM FLCs are nephrotoxic and can damage all kidney compartments: gli, tubuli and vessels. glomerulopathic FLCs 1. AL amyloidosis 2. LCDD 3. GN with monoclonal deposits tubulopathic FLCs 1. cast nephropathy 2. proximal tubulopathy 3. TIN associated with M protein + Combinations of the above diagnoses + Combinations with other diseases (hypertension, vascular nephrosclerosis, DM) Kidney involvement may represent the first manifestation of hematological disease.



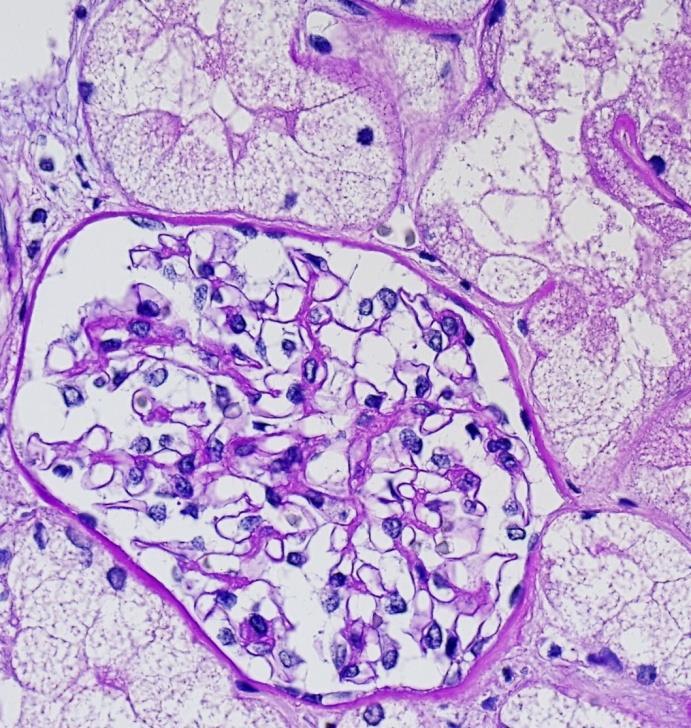
10 AL amyloidosis The kidney is the most common organ involved in several types of systemic amyloidosis
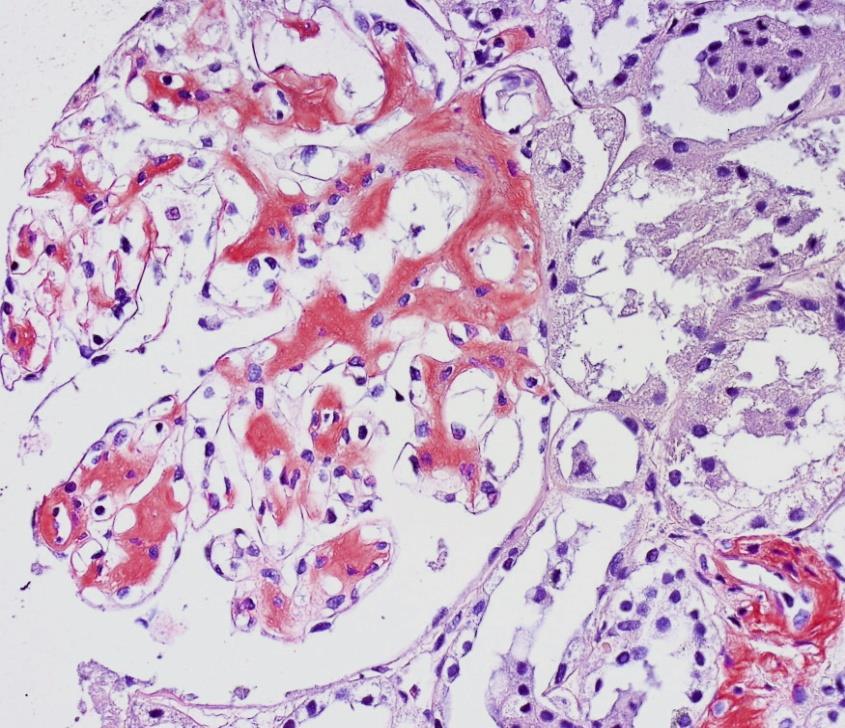
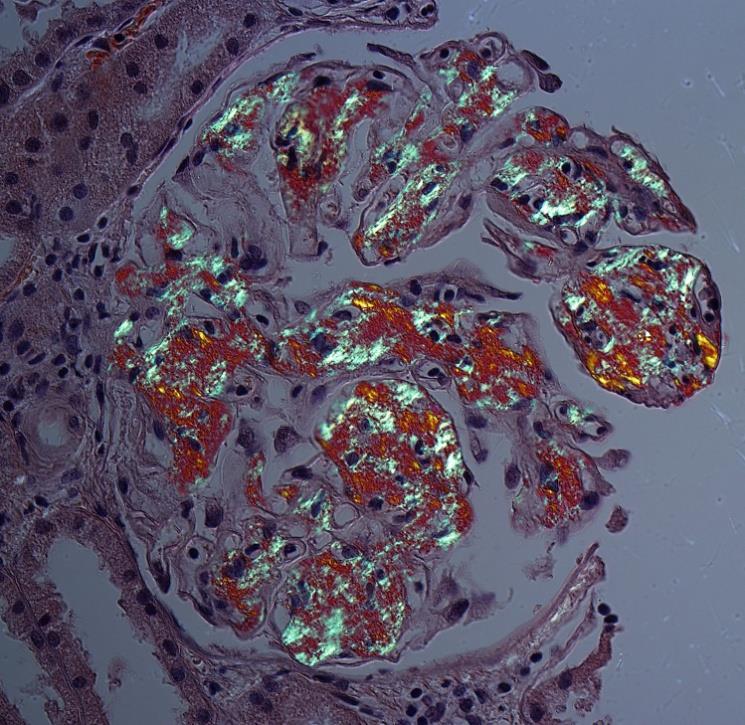
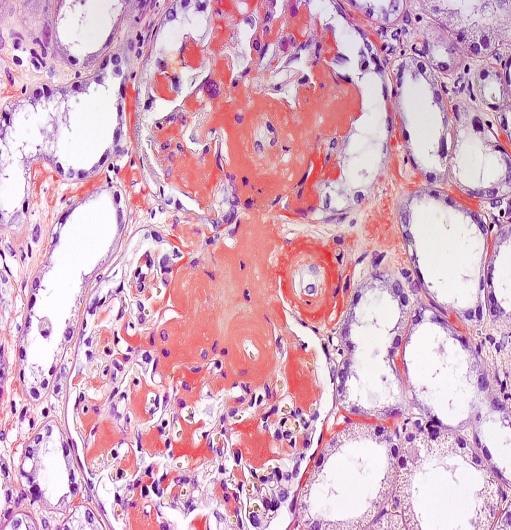
11 Amyloidosis: detection of amyloid
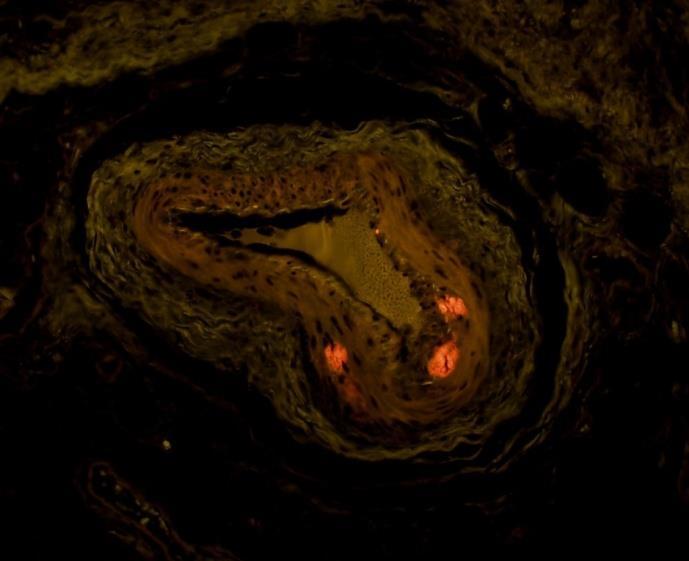

12 Amyloidosis: diagnosis



13 Amyloidosis: typing IF is the best method for typing amyloid. It allows to classify more than 90% of amyloid in kidney biopsy samples.



14 Fascinating story of amyloidos Only a small number of patients with preconditions suffer from amyloidosis Per Westermark Comparison with prion diseases: change in the protein structure, conformational diseases Prion diseases are transmissible by food Amyloid enhancing factor (amyloid fibrils) Is amyloidosis transmissible? Yes, very probably Westermark GT, Westermark P. Serum amyloid A and protein AA: molecular mechanisms of a transmissible amyloidosis. FEBS Lett. 2009;583: AA amyloidosis is transmissible in several animal experimental models AA amyloid can occur in human food (ducks, geese: pate de foie gras; cattle) AA amyloidosis is transmissible by blood monocytes



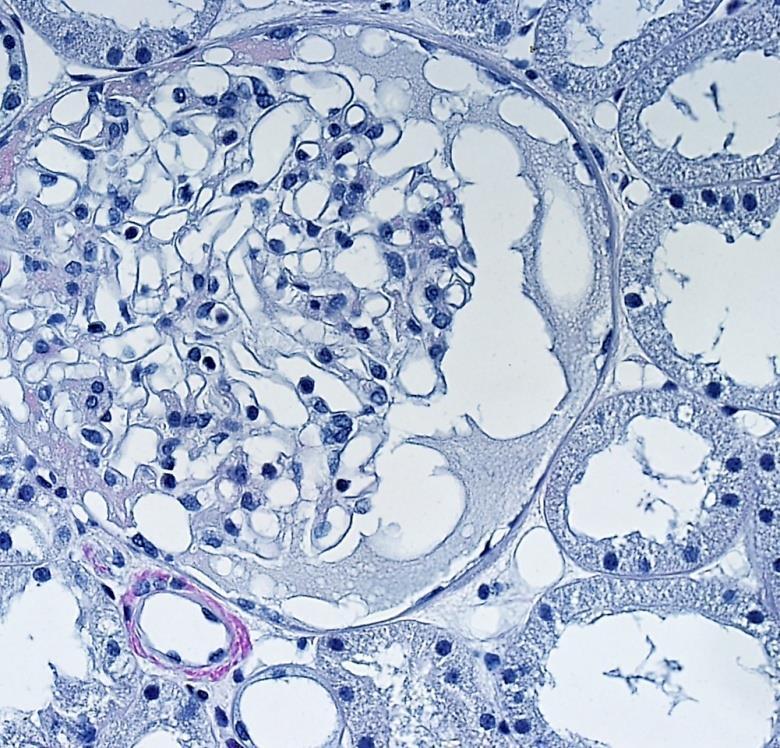
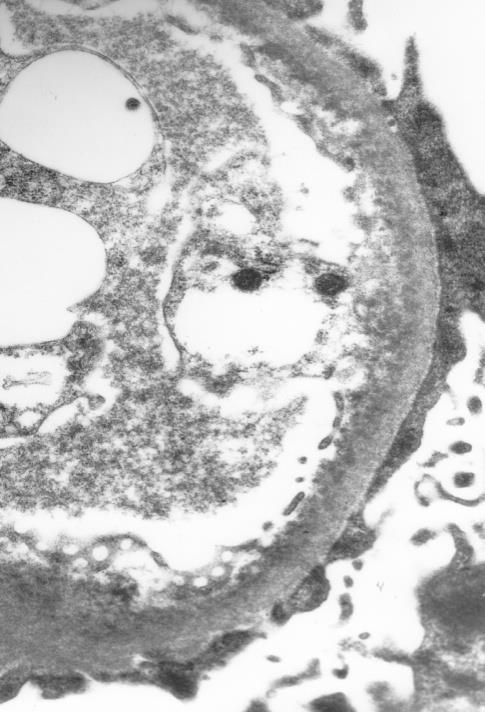
15 AL amyloidosis and LCDD Experimental works showed that LCs can transform the phenotype of mesangial cells. In cases of AL amyloidosis the phenotype evolves toward macrophages with development of lysosomes within which degradation and remodeling of LCs into amyloid occur. Amyloid deposition in the extracellular matrix results in activation of metalloproteinases followed by destruction of the native mesangial matrix. The normal mesangium is replaced by amyloid and mesangial cells disappear. In cases of LCDD, mesangial cells evolve into a myofibroblast phenotype, and mesangial cells proliferate under the influence of overproduction of TGF-β, resulting in the formation of mesangial nodules.

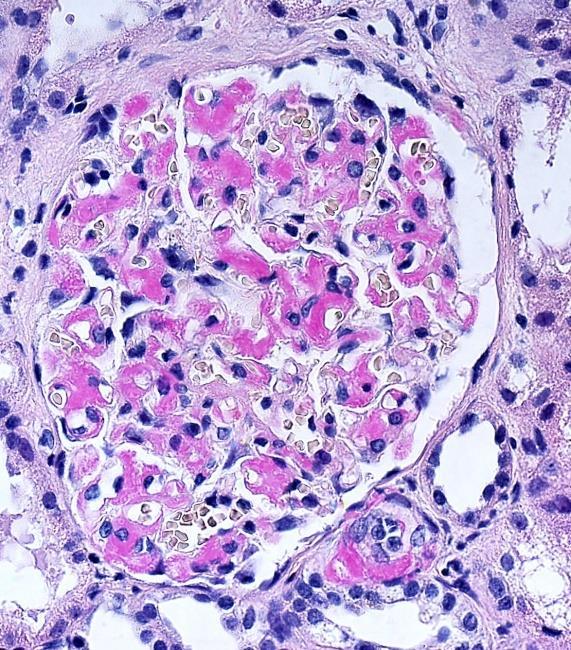
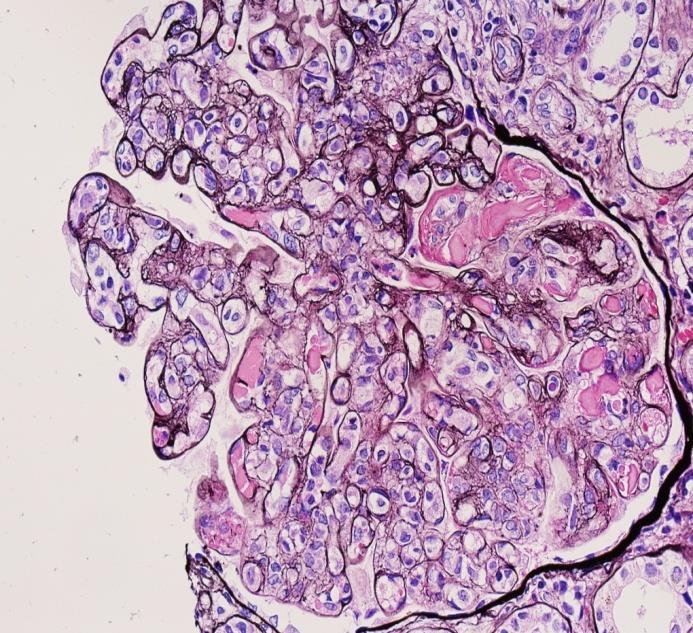
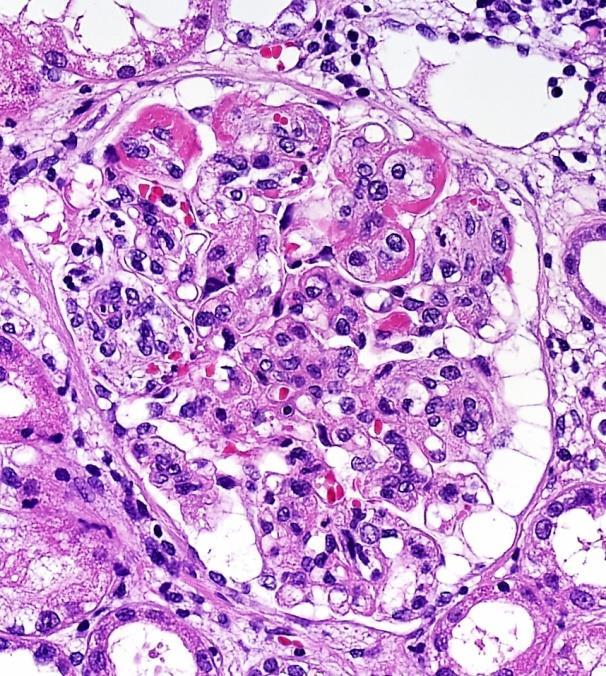
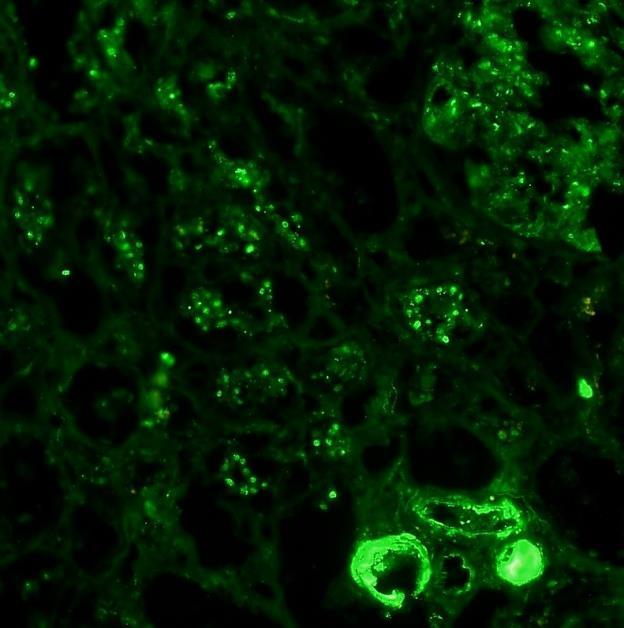
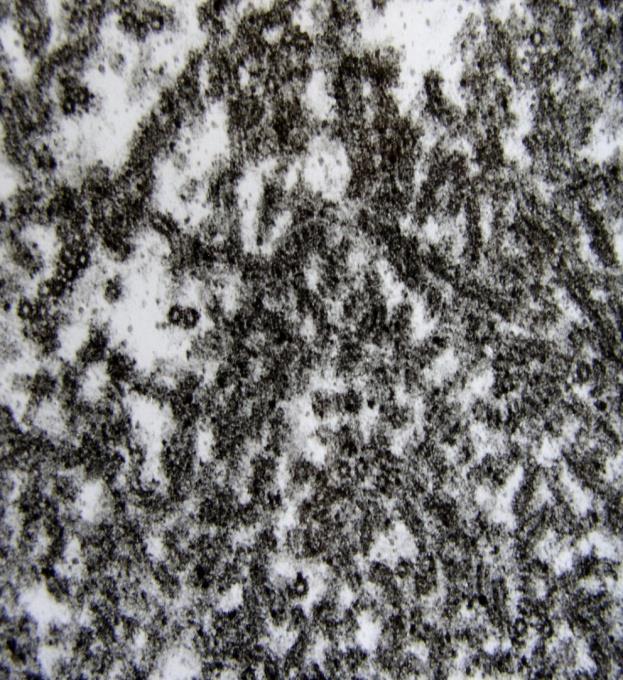
16 LCDD kappa

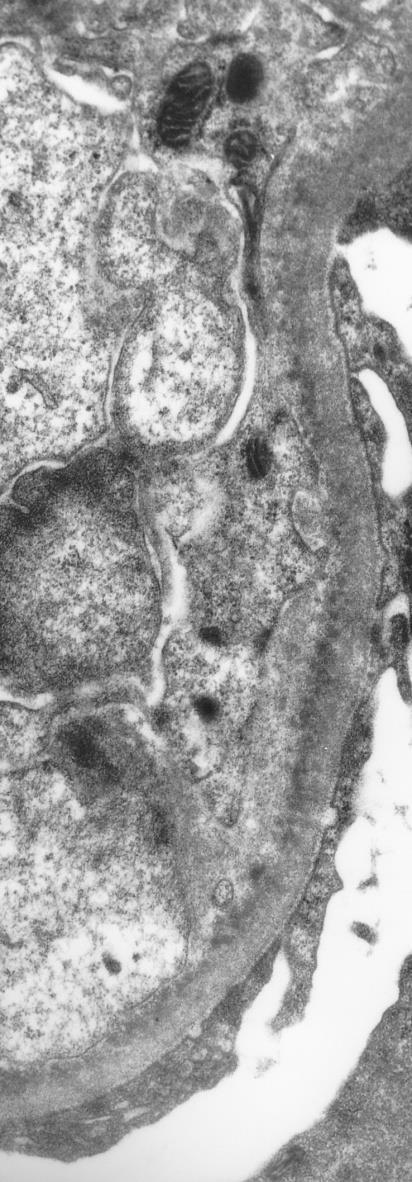
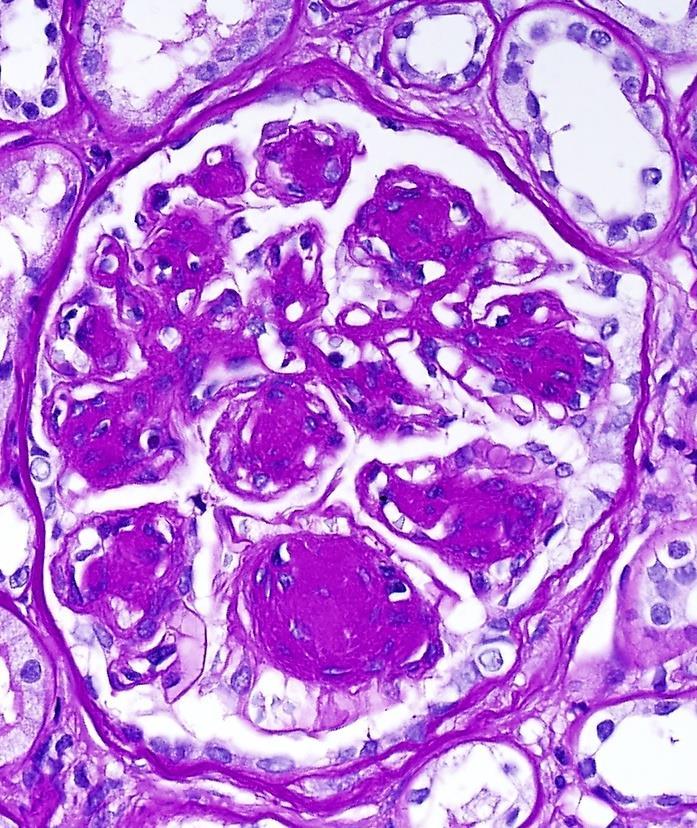
17 LCDD GBM DM!!! TBM
 Mimics immune-complex GN (MPGN, MGN).")


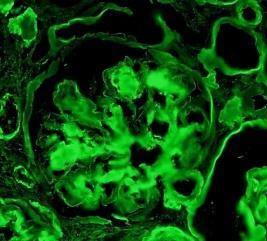
18 Proliferative GN with monoclonal deposits (IgG3 kappa) Mimics immune-complex GN (MPGN, MGN). Restriction of LC: IF positive is only kappa or less frequently only lambda IgG3 or IgG1 Proteinurie or NS, 50% have monoclonal protein in serum More frequent than LCDD (20 AL amyloidosis, 8 GN with monoclonal dep., 5 LCDD)
 IgG IgG3 C3")

19 Proliferative GN with monoclonal deposits (IgG3 kappa) IgG IgG3 C3 C1q The key to the diagnosis: recognition of single light chain restriction
20 Proliferative GN with monoclonal deposits IgG3: greatest complement fixing ability Most positively charged subtype of IgG (can interact with negatively charged GBM) Highest MW (size restricted by glom. filter) Ability to self-aggregate spontaneously through Fc-Fc fragment interactions Monoclonal gamapaties can lead to proliferative GN via 2 mechanisms: 1. deposition of monoclonal Igs in the mesangium and along capillary walls activation of complement proliferative GN 2. monoclonal Igs cause the activation of alternative complement pathway by acting as autoantibodies (to complementregulating proteins) deposition of C3 (C3 GN) without Igs

 was the first renal complication to be recognized in")

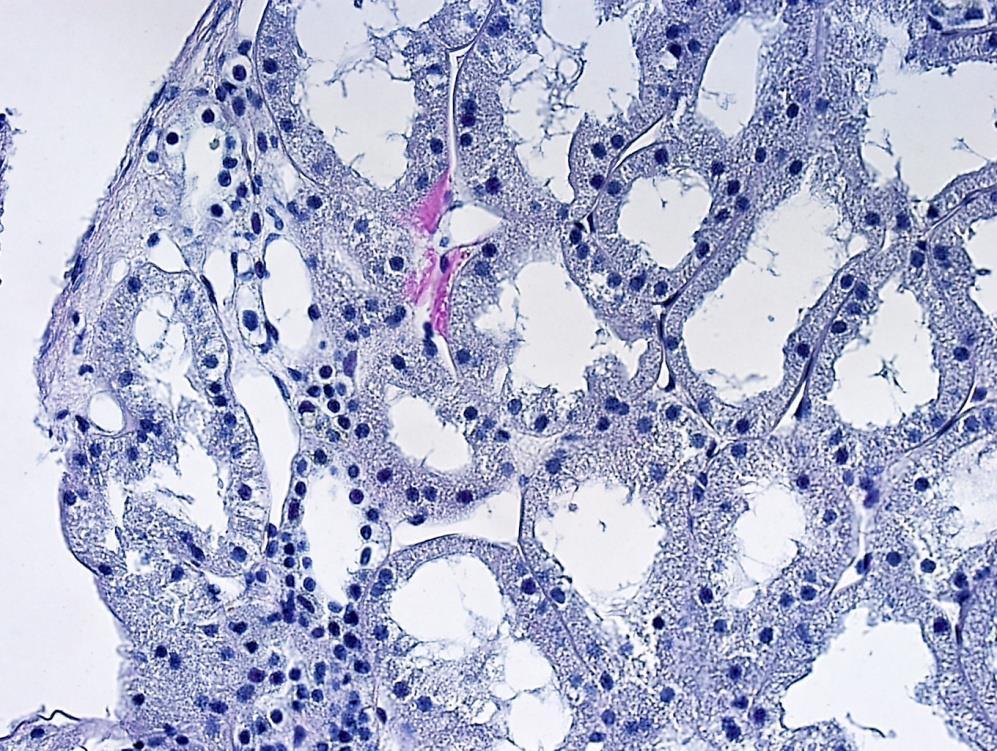
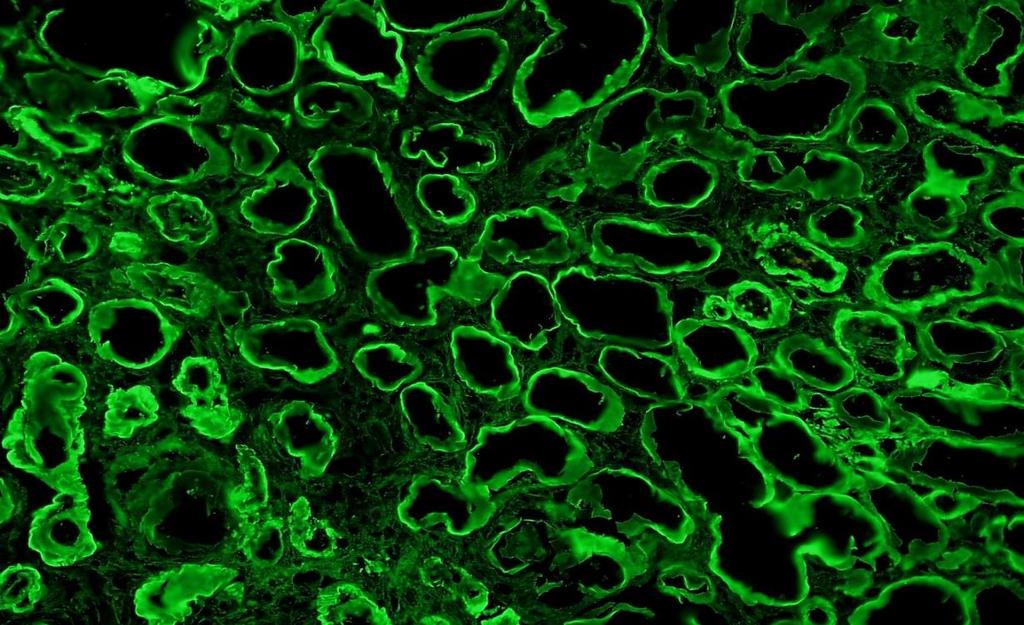
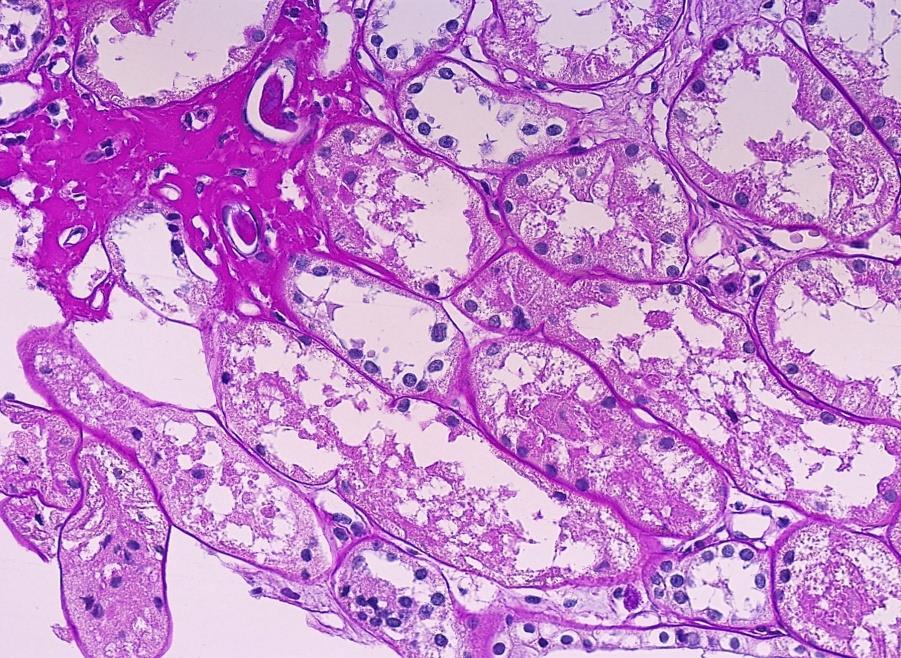
21 Group II, tubulopathic light chains 1. cast nephropathy 2. proximal tubulopathy 3. TIN associated with M protein cast nephropathy (historically called myeloma kidney) was the first renal complication to be recognized in patients with myeloma Higher concentration of sodium changes the consistency of T-H protein from a fluid to the gel The development of the casts involves binding of T-H protein to the CDR3 region of Ig free LCs

 no")


22 Cast nephropathy (myeloma kidney) no guidelines for how many cast must be present in a biopsy sample




23 Proximal tubulopathy Two morphological patterns Kappa light chains IF remains the most sensitive method for the detection of LCs restriction


24 and many others: cryoglobulins, Waldenstrom GN, Lc crystal storage disease, ect.



25 Combined patterns Combined patterns of glomerulopathic and tubulopathic LCs injury (such as LCDD and LC cast nephropathy, amyloidosis and LC cast nephropathy) Because especially older patients suffer from plasma cell dyscrasias, differential diagnosis can be also more complicated by vascular diseases, DM and other glomerulopathies.



26 The diagnoses do not jump from the microscope???
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Jo Abraham MD Division of Nephrology University of Utah
 Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Forms Revision: Myeloma Changes
 Sharing knowledge. Sharing hope. Forms Revision: Myeloma Changes J. Brunner, PA-C and A. Dispenzieri, MD February 2013 Disclosures Janet Brunner, PA-C I have no relevant conflicts of interest to disclose.
Sharing knowledge. Sharing hope. Forms Revision: Myeloma Changes J. Brunner, PA-C and A. Dispenzieri, MD February 2013 Disclosures Janet Brunner, PA-C I have no relevant conflicts of interest to disclose.
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME
 CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT
 The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Multiple Myeloma Advances for clinical pathologists & histopathologists
 Multiple Myeloma Advances for clinical pathologists & histopathologists CME in Haematology 2014 IAPP & Dept of Pathology, BVDUMC, Pune Sunday, 4 th May 2014 Dr. M.B. Agarwal, MD, MNAMS Head, Dept of Haematology
Multiple Myeloma Advances for clinical pathologists & histopathologists CME in Haematology 2014 IAPP & Dept of Pathology, BVDUMC, Pune Sunday, 4 th May 2014 Dr. M.B. Agarwal, MD, MNAMS Head, Dept of Haematology
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Lec-14 د.خالد نافع. Medicine. Multiple Myeloma
 Fifth stage Lec-14 د.خالد نافع Medicine 24/4/2016 Multiple Myeloma Plasma cell myeloma Variants Non - secretory myeloma Indolent myeloma Smouldering myeloma Plasma cell leukaemia Plasmacytoma - Solitary
Fifth stage Lec-14 د.خالد نافع Medicine 24/4/2016 Multiple Myeloma Plasma cell myeloma Variants Non - secretory myeloma Indolent myeloma Smouldering myeloma Plasma cell leukaemia Plasmacytoma - Solitary
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
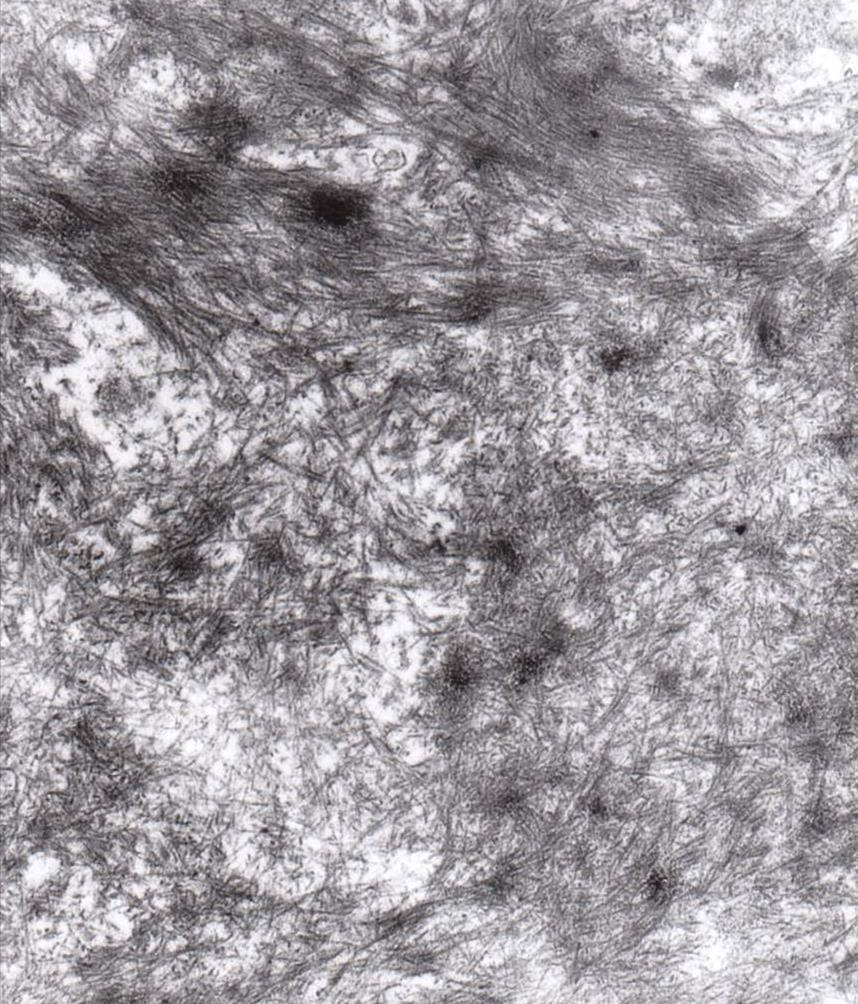
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Sheena Surindran Grand Rounds 2/15/11
 Sheena Surindran Grand Rounds 2/15/11 Affects 5 12 person per million / year 5 10% associated with myeloma Median survival without treatment is 12 40 months Most commonly affected organs are kidney, heart
Sheena Surindran Grand Rounds 2/15/11 Affects 5 12 person per million / year 5 10% associated with myeloma Median survival without treatment is 12 40 months Most commonly affected organs are kidney, heart
A Case of IgG2 Heavy Chain Deposition Disease in a Patient with Kappa Positive Plasma Cell Dyscrasia
 Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Multiple myeloma Biological & Clinical Aspects Isabelle Vande Broek, MD, PhD
 Multiple myeloma Biological & Clinical Aspects Isabelle Vande Broek, MD, PhD Department of Oncology & Hematology AZ Nikolaas Iridium Kanker Netwerk Introduction Multiple myeloma = Kahler s disease Dr.
Multiple myeloma Biological & Clinical Aspects Isabelle Vande Broek, MD, PhD Department of Oncology & Hematology AZ Nikolaas Iridium Kanker Netwerk Introduction Multiple myeloma = Kahler s disease Dr.
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That Showed Predominantly Membranous Features
 Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Instructions for Plasma Cell Disorders (PCD) Post-HCT Data (Form 2116 Revision 3)
 Post-HCT Data (Form 2116 Revision 3)") (Form 2116 Revision 3) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Plasma Cell Disorders (PCD) Post-HCT Data Form. E-mail comments regarding the
(Form 2116 Revision 3) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Plasma Cell Disorders (PCD) Post-HCT Data Form. E-mail comments regarding the
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
GRAND ROUNDS
 GRAND ROUNDS 5.14.13 CASE 64 y.o AAF with h/o HTN, DM, HLD, MGUS referred by PMD for uncontrolled resistant hypertension, new renal failure (Cr of 1.5), hematuria and proteinuria Per patient systolic BP
GRAND ROUNDS 5.14.13 CASE 64 y.o AAF with h/o HTN, DM, HLD, MGUS referred by PMD for uncontrolled resistant hypertension, new renal failure (Cr of 1.5), hematuria and proteinuria Per patient systolic BP
Multiple intra-renal pathological injury patterns in resistant myeloma
 Multiple intra-renal pathological injury patterns in resistant myeloma Dharshan Rangaswamy 1, Mohit Madken 1, Mahesha Vankalakunti 2, Ravindra Prabhu Attur 1, and Shankar Prasad Nagaraju 1 1. Department
Multiple intra-renal pathological injury patterns in resistant myeloma Dharshan Rangaswamy 1, Mohit Madken 1, Mahesha Vankalakunti 2, Ravindra Prabhu Attur 1, and Shankar Prasad Nagaraju 1 1. Department
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Serum free light chain (SFLC) assays. Dr Sarah Sasson SydPath Registrar
 assays. Dr Sarah Sasson SydPath Registrar") Serum free light chain (SFLC) assays Dr Sarah Sasson SydPath Registrar Introduction to SFLC Plasma cell dyscrasias such as monoclonal gammopathy of uncertain significance (MGUS) smouldering/asymptomatic
Serum free light chain (SFLC) assays Dr Sarah Sasson SydPath Registrar Introduction to SFLC Plasma cell dyscrasias such as monoclonal gammopathy of uncertain significance (MGUS) smouldering/asymptomatic
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Multiple Myeloma 101: Understanding Your Labs
 Multiple Myeloma 101: Understanding Your Labs Tim Wassenaar MD MS Hematologist, Director of Clinical Trials UW Cancer Center at ProHealth Care None Disclosures Outline Define hematopoiesis WBCs, RBCs,
Multiple Myeloma 101: Understanding Your Labs Tim Wassenaar MD MS Hematologist, Director of Clinical Trials UW Cancer Center at ProHealth Care None Disclosures Outline Define hematopoiesis WBCs, RBCs,
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016
 + M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
+ M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
Hematology Case Conference 8/5/03
 Hematology Case Conference 8/5/03 Bone Marrow Case Patient: Emmxxx Lylexxx 74 year old AA female S/P craniotomy for SDH. Pt has Hx of HTN, DM, Crohn s disease, (R) nephrectomy. Bone marrow for abnormal
Hematology Case Conference 8/5/03 Bone Marrow Case Patient: Emmxxx Lylexxx 74 year old AA female S/P craniotomy for SDH. Pt has Hx of HTN, DM, Crohn s disease, (R) nephrectomy. Bone marrow for abnormal
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
LIGHT CHAIN DISEASE B. DHANALAKSHMI 1 & V. HEMAVATHY 2
 TJPRC: International Journal of Nursing and Patient Safety & Care (TJPRC: IJNPSC) Vol. 1, Issue 1, Dec 2016, 21-24 TJPRC Pvt. Ltd. LIGHT CHAIN DISEASE B. DHANALAKSHMI 1 & V. HEMAVATHY 2 1 Associate Professor,
TJPRC: International Journal of Nursing and Patient Safety & Care (TJPRC: IJNPSC) Vol. 1, Issue 1, Dec 2016, 21-24 TJPRC Pvt. Ltd. LIGHT CHAIN DISEASE B. DHANALAKSHMI 1 & V. HEMAVATHY 2 1 Associate Professor,
Serum Free Light Chain Assay
 Serum Free Light Chain Assay This Infosheet explains what light chains are, what the Serum Free Light Chain Assay is, and why it is used in AL amyloidosis. In AL amyloidosis, abnormal plasma cells in the
Serum Free Light Chain Assay This Infosheet explains what light chains are, what the Serum Free Light Chain Assay is, and why it is used in AL amyloidosis. In AL amyloidosis, abnormal plasma cells in the
Clinical history. 73 yo man with chest pain Systemic hypertension and WG Stress EKG N Stress echocardiogram: Cardiac catheterization: no CAD
 CASE 8 Clinical history 73 yo man with chest pain Systemic hypertension and WG Stress EKG N Stress echocardiogram: Concentric hypertrophy Hypokinesis of LV-Inf Cardiac catheterization: no CAD Technique
CASE 8 Clinical history 73 yo man with chest pain Systemic hypertension and WG Stress EKG N Stress echocardiogram: Concentric hypertrophy Hypokinesis of LV-Inf Cardiac catheterization: no CAD Technique
Anaemias and other Pesky Haematology Questions
 Anaemias and other Pesky Haematology Questions 3 main topics How do I work out an anaemia.. That oh too common paraprotein patient. Those mildly raised lymphocyte count GP discussed patient with me over
Anaemias and other Pesky Haematology Questions 3 main topics How do I work out an anaemia.. That oh too common paraprotein patient. Those mildly raised lymphocyte count GP discussed patient with me over
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis with Monoclonal Immunoglobulin Deposits of Lambda Light Chain
 Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Southern Derbyshire Shared Care Pathology Guidelines. MGUS (Monoclonal Gammopathy of Undetermined Significance)
") Southern Derbyshire Shared Care Pathology Guidelines MGUS (Monoclonal Gammopathy of Undetermined Significance) Purpose of guideline This guideline provides information about the risk stratification of
Southern Derbyshire Shared Care Pathology Guidelines MGUS (Monoclonal Gammopathy of Undetermined Significance) Purpose of guideline This guideline provides information about the risk stratification of
Understanding the Serum Free Light Chain Assays. Anne L Sherwood, PhD Director of Scientific Affairs The Binding Site, Inc.
 Understanding the Serum Free Light Chain Assays Anne L Sherwood, PhD Director of Scientific Affairs The Binding Site, Inc. AL Amyloidosis: abnormality of proteins from Plasma Cells in the Bone Marrow Red
Understanding the Serum Free Light Chain Assays Anne L Sherwood, PhD Director of Scientific Affairs The Binding Site, Inc. AL Amyloidosis: abnormality of proteins from Plasma Cells in the Bone Marrow Red
Complement in vasculitis and glomerulonephritis. Andy Rees Clinical Institute of Pathology Medical University of Vienna
 Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Renal Pathology- Transplantation. Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic
 Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Antibody-Cytokine- Autoimmune
 Antibody-Cytokine- Autoimmune Surasak Wongratanacheewin, Ph.D Dean, Graduate School, KKU Microbiology, Faculty of Medicine, KKU sura_wng@kku.ac.th การอบรมหล กส ตรประกาศน ยบ ตรการข นทะเบ ยนช วว ตถ ว นท
Antibody-Cytokine- Autoimmune Surasak Wongratanacheewin, Ph.D Dean, Graduate School, KKU Microbiology, Faculty of Medicine, KKU sura_wng@kku.ac.th การอบรมหล กส ตรประกาศน ยบ ตรการข นทะเบ ยนช วว ตถ ว นท
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Beta-2 microglobulin and short Ig chains and organ damage in dialysis patients: An update.
 EURECA-m CME COURSE, Cardiovascular Problems and Solutions in Chronic Kidney Disease Ankara Hilton Hotel, Ankara, September 8, 2012 Beta-2 microglobulin and short Ig chains and organ damage in dialysis
EURECA-m CME COURSE, Cardiovascular Problems and Solutions in Chronic Kidney Disease Ankara Hilton Hotel, Ankara, September 8, 2012 Beta-2 microglobulin and short Ig chains and organ damage in dialysis
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Monoclonal gammopathies consist of. Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis REVIEW
 REVIEW Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis Sanjeev Sethi, MD, PhD, and S. Vincent Rajkumar, MD Abstract Monoclonal gammopathy is characterized by circulating monoclonal immunoglobulin
REVIEW Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis Sanjeev Sethi, MD, PhD, and S. Vincent Rajkumar, MD Abstract Monoclonal gammopathy is characterized by circulating monoclonal immunoglobulin
Importancia del laboratorio en el seguimiento clínico de pacientes con mieloma múltiple
 Importancia del laboratorio en el seguimiento clínico de pacientes con mieloma múltiple Joan Bladé Unidad de Amiloidosis y Mieloma Servicio de Hematología Hospital Clínic de Barcelona Málaga, 16 de noviembre
Importancia del laboratorio en el seguimiento clínico de pacientes con mieloma múltiple Joan Bladé Unidad de Amiloidosis y Mieloma Servicio de Hematología Hospital Clínic de Barcelona Málaga, 16 de noviembre
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
2016: Plasma Cell Disorders Pre-HCT Data
 2016: Plasma Cell Disorders Pre-HCT Data Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Date of HCT for which this form is being completed: / / YYYY MM DD HCT type (check
2016: Plasma Cell Disorders Pre-HCT Data Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Date of HCT for which this form is being completed: / / YYYY MM DD HCT type (check
Malcolm P. McTaggart, PhD, 1 Jindriska Lindsay, FRCPath, 2 and Edward M. Kearney, FRCPath 1 ABSTRACT
 Replacing Urine Protein Electrophoresis With Serum Free Light Chain Analysis as a First-Line Test for Detecting Plasma Cell Disorders Offers Increased Diagnostic Accuracy and Potential Health Benefit to
Replacing Urine Protein Electrophoresis With Serum Free Light Chain Analysis as a First-Line Test for Detecting Plasma Cell Disorders Offers Increased Diagnostic Accuracy and Potential Health Benefit to
Plasma Cell Disorders (PCD) Pre-HCT Data
 Pre-HCT Data") Plasma Cell Disorders (PCD) Pre-HCT Data Registry Use Only Sequence Number: Date Received: CIBMTR Center Number: CIBMTR Recipient ID: Date of HCT for which this form is being completed: HCT type: (check
Plasma Cell Disorders (PCD) Pre-HCT Data Registry Use Only Sequence Number: Date Received: CIBMTR Center Number: CIBMTR Recipient ID: Date of HCT for which this form is being completed: HCT type: (check
Principles of Adaptive Immunity
 Principles of Adaptive Immunity Chapter 3 Parham Hans de Haard 17 th of May 2010 Agenda Recognition molecules of adaptive immune system Features adaptive immune system Immunoglobulins and T-cell receptors
Principles of Adaptive Immunity Chapter 3 Parham Hans de Haard 17 th of May 2010 Agenda Recognition molecules of adaptive immune system Features adaptive immune system Immunoglobulins and T-cell receptors
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL RESPONSE ASSESSMENT MYELOMA CHAPTER 11C REVISED: SEPTEMBER 2016
 MANUAL RESPONSE ASSESSMENT MYELOMA CHAPTER 11C REVISED: SEPTEMBER 2016") MYELOMA Quantitative Markers-Myeloma Assessment Quantitative markers are biochemicals that are recorded in tests on body fluids such as serum and urine. Applicable Disease Sites The myeloma disease site
MYELOMA Quantitative Markers-Myeloma Assessment Quantitative markers are biochemicals that are recorded in tests on body fluids such as serum and urine. Applicable Disease Sites The myeloma disease site
Light-Chain Mediated Acute Tubular Interstitial Nephritis. A Poorly Recognized Pattern of Renal Disease in Patients With Plasma Cell Dyscrasia
 Light-Chain Mediated Acute Tubular Interstitial Nephritis A Poorly Recognized Pattern of Renal Disease in Patients With Plasma Cell Dyscrasia Xin Gu, MD; Guillermo A. Herrera, MD Context. Acute renal failure
Light-Chain Mediated Acute Tubular Interstitial Nephritis A Poorly Recognized Pattern of Renal Disease in Patients With Plasma Cell Dyscrasia Xin Gu, MD; Guillermo A. Herrera, MD Context. Acute renal failure
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
WHO Classification. B-cell chronic lymphocytic leukemia/small T-cell granular lymphocytic leukemia
 Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Immunobiology 7. The Humoral Immune Response
 Janeway Murphy Travers Walport Immunobiology 7 Chapter 9 The Humoral Immune Response Copyright Garland Science 2008 Tim Worbs Institute of Immunology Hannover Medical School 1 The course of a typical antibody
Janeway Murphy Travers Walport Immunobiology 7 Chapter 9 The Humoral Immune Response Copyright Garland Science 2008 Tim Worbs Institute of Immunology Hannover Medical School 1 The course of a typical antibody
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Early View Article: Online published version of an accepted article before publication in the final form.
 Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Oncology Type of Article: Case Report Title:
Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Oncology Type of Article: Case Report Title:
Szervusz [hi]everybody!
![Szervusz [hi]everybody!](/thumbs/89/98111920.jpg "Szervusz [hi]everybody!") Szervusz [hi]everybody! 1 Renal Injury due to Monoclonal Gammopathy Maria M. Picken MD, PhD mpicken@luc.edu MMPicken@aol.com ISA International Kidney Monoclonal Gammopathy Renal Pathology Society International
Szervusz [hi]everybody! 1 Renal Injury due to Monoclonal Gammopathy Maria M. Picken MD, PhD mpicken@luc.edu MMPicken@aol.com ISA International Kidney Monoclonal Gammopathy Renal Pathology Society International
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Serum free light chain ratio is an independent risk factor for progression in monoclonal gammopathy of undetermined significance
 CLINICAL OBSERVATIONS, INTERVENTIONS, AND THERAPEUTIC TRIALS Serum free light chain ratio is an independent risk factor for progression in monoclonal gammopathy of undetermined significance S. Vincent
CLINICAL OBSERVATIONS, INTERVENTIONS, AND THERAPEUTIC TRIALS Serum free light chain ratio is an independent risk factor for progression in monoclonal gammopathy of undetermined significance S. Vincent
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Jonathan Katz, MD CPMC
 Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC First, a bit of background Classic CIDP--TREATABLE MADSAM/Asymmetric Neuropathy Chronic Length Dependent Neuropathy-
Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC First, a bit of background Classic CIDP--TREATABLE MADSAM/Asymmetric Neuropathy Chronic Length Dependent Neuropathy-
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
 C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
Favorable effect of bortezomib in dense deposit disease associated with monoclonal gammopathy: a case report
 Hirashio et al. BMC Nephrology (2018) 19:108 https://doi.org/10.1186/s12882-018-0905-6 CASE REPORT Open Access Favorable effect of bortezomib in dense deposit disease associated with monoclonal gammopathy:
Hirashio et al. BMC Nephrology (2018) 19:108 https://doi.org/10.1186/s12882-018-0905-6 CASE REPORT Open Access Favorable effect of bortezomib in dense deposit disease associated with monoclonal gammopathy:
CELL BIOLOGY - CLUTCH CH THE IMMUNE SYSTEM.
 !! www.clutchprep.com CONCEPT: OVERVIEW OF HOST DEFENSES The human body contains three lines of against infectious agents (pathogens) 1. Mechanical and chemical boundaries (part of the innate immune system)
!! www.clutchprep.com CONCEPT: OVERVIEW OF HOST DEFENSES The human body contains three lines of against infectious agents (pathogens) 1. Mechanical and chemical boundaries (part of the innate immune system)
Test Name Results Units Bio. Ref. Interval
 LL - LL-ROHINI (NATIONAL REFERENCE 135091536 Age 33 Years Gender Male 1/9/2017 120000AM 1/9/2017 105100AM 1/9/2017 25258M Ref By Final LIVER FIBROSIS ANEL ROTHROMBIN TIME STUDIES (hoto optical Clot Detection)
LL - LL-ROHINI (NATIONAL REFERENCE 135091536 Age 33 Years Gender Male 1/9/2017 120000AM 1/9/2017 105100AM 1/9/2017 25258M Ref By Final LIVER FIBROSIS ANEL ROTHROMBIN TIME STUDIES (hoto optical Clot Detection)
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
Leicester. Research Group. Background. Inside. contact. Page 1: Background. Page 2-4: Leicester IgAN individual research
 May 2015 Newsletter Leicester Research Group Inside Page 1: Background Page 2-4: Page 5: Other research in the Group Background contact Dr Jonathan Barratt, The John Walls Renal Unit, Leicester General
May 2015 Newsletter Leicester Research Group Inside Page 1: Background Page 2-4: Page 5: Other research in the Group Background contact Dr Jonathan Barratt, The John Walls Renal Unit, Leicester General
Plasma cell dyscrasia with renal impairment including MGRS
 Plasma cell dyscrasia with renal impairment including MGRS ~ The importance of multi-departmental management ~ Dept. Nephrology, Japan Community Health Care Organization Sendai Hospital Shinichi Mizuno
Plasma cell dyscrasia with renal impairment including MGRS ~ The importance of multi-departmental management ~ Dept. Nephrology, Japan Community Health Care Organization Sendai Hospital Shinichi Mizuno
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Case: The patient is a 73 year old woman with vague complaints of dyspepsia and abdominal pain. Upper endoscopy showed features of gastritis and a
 Case: The patient is a 73 year old woman with vague complaints of dyspepsia and abdominal pain. Upper endoscopy showed features of gastritis and a nodular lesion in the body of the stomach. The patient
Case: The patient is a 73 year old woman with vague complaints of dyspepsia and abdominal pain. Upper endoscopy showed features of gastritis and a nodular lesion in the body of the stomach. The patient
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
SUPPLEMENTARY APPENDIX
 SUPPLEMENTARY APPENDIX The clinical relevance and management of monoclonal gammopathy of undetermined significance and related disorders: recommendations from the European Myeloma Network Niels W.C.J.
SUPPLEMENTARY APPENDIX The clinical relevance and management of monoclonal gammopathy of undetermined significance and related disorders: recommendations from the European Myeloma Network Niels W.C.J.
substance staining with IgG, C3 and IgA (trace) Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ
 Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ") Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Case #1. Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute
 Case #1 Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute Patient History Part I 76 year-old man 1997 diagnosed with MGUS (biclonal) during evaluation of (self-limited) anemia.
Case #1 Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute Patient History Part I 76 year-old man 1997 diagnosed with MGUS (biclonal) during evaluation of (self-limited) anemia.
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
29th Annual Meeting of the Glomerular Disease Collaborative Network
 29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
Amyloid-like Pulmonary Nodules, Including Localized Light-Chain Deposition Clinicopathologic Analysis of Three Cases
 Anatomic Pathology / AMYLOID-LIKE PULMONARY NODULES Amyloid-like Pulmonary Nodules, Including Localized Light-Chain Deposition Clinicopathologic Analysis of Three Cases Andras Khoor, MD, 1 Jeffrey L. Myers,
Anatomic Pathology / AMYLOID-LIKE PULMONARY NODULES Amyloid-like Pulmonary Nodules, Including Localized Light-Chain Deposition Clinicopathologic Analysis of Three Cases Andras Khoor, MD, 1 Jeffrey L. Myers,
Yijuan Sun, Amarpreet Sandhu, Darlene Gabaldon, Jonathan Danaraj, Karen S. Servilla, and Antonios H. Tzamaloukas
 Case Reports in Nephrology Volume 2012, Article ID 573650, 5 pages doi:10.1155/2012/573650 Case Report Development of Renal Failure without Proteinuria in a Patient with Monoclonal Gammopathy of Undetermined
Case Reports in Nephrology Volume 2012, Article ID 573650, 5 pages doi:10.1155/2012/573650 Case Report Development of Renal Failure without Proteinuria in a Patient with Monoclonal Gammopathy of Undetermined
CORE CURRICULUM IN NEPHROLOGY Renal Manifestations of Plasma Cell Disorders
 CORE CURRICULUM IN NEPHROLOGY Renal Manifestations of Plasma Cell Disorders Nelson Leung, MD, 1 and S. Vincent Rajkumar, MD 2 INTRODUCTION Plasma cell dyscrasias represent a group of diseases characterized
CORE CURRICULUM IN NEPHROLOGY Renal Manifestations of Plasma Cell Disorders Nelson Leung, MD, 1 and S. Vincent Rajkumar, MD 2 INTRODUCTION Plasma cell dyscrasias represent a group of diseases characterized
Diabetes. Albumin. Analyte Information
 Diabetes Albumin Analyte Information -1-2014-05-02 Albumin Introduction Albumin consists of a single polypeptide chain of 585 amino acids with molecular weight of 66.5 kda. The chain is characterized by
Diabetes Albumin Analyte Information -1-2014-05-02 Albumin Introduction Albumin consists of a single polypeptide chain of 585 amino acids with molecular weight of 66.5 kda. The chain is characterized by
Laboratory Examination
 Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
Proteinuria (Protein in the Urine) Basics
 Basics") Proteinuria (Protein in the Urine) Basics OVERVIEW Proteinuria is the medical term for protein in the urine Urinary protein is detected by urine dipstick analysis, urinary protein: creatinine ratio (UP:C
Proteinuria (Protein in the Urine) Basics OVERVIEW Proteinuria is the medical term for protein in the urine Urinary protein is detected by urine dipstick analysis, urinary protein: creatinine ratio (UP:C
IMMUNOBIOLOGY, BIOL 537 Exam # 2 Spring 1997
 Name I. TRUE-FALSE (1 point each) IMMUNOBIOLOGY, BIOL 537 Exam # 2 Spring 1997 Which of the following is TRUE or FALSE relating to immunogenicity of an antigen and T and B cell responsiveness to antigen?
Name I. TRUE-FALSE (1 point each) IMMUNOBIOLOGY, BIOL 537 Exam # 2 Spring 1997 Which of the following is TRUE or FALSE relating to immunogenicity of an antigen and T and B cell responsiveness to antigen?
Immunology - Lecture 2 Adaptive Immune System 1
 Immunology - Lecture 2 Adaptive Immune System 1 Book chapters: Molecules of the Adaptive Immunity 6 Adaptive Cells and Organs 7 Generation of Immune Diversity Lymphocyte Antigen Receptors - 8 CD markers
Immunology - Lecture 2 Adaptive Immune System 1 Book chapters: Molecules of the Adaptive Immunity 6 Adaptive Cells and Organs 7 Generation of Immune Diversity Lymphocyte Antigen Receptors - 8 CD markers
κ λ Antigen-Independent B-Cell Development Bone Marrow Ordered Rearrangement of Ig Genes During B-Cell Development in the Bone Marrow
 Antigen-Independent B-Cell Development Bone Marrow 1. DNA rearrangements establish the primary repertoire, creating diversity 2. Allelic exclusion ensures that each clone expresses a single antibody on
Antigen-Independent B-Cell Development Bone Marrow 1. DNA rearrangements establish the primary repertoire, creating diversity 2. Allelic exclusion ensures that each clone expresses a single antibody on
ESRD Dialysis Prevalence - One Year Statistics
 Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540