New Approaches for Treating Challenging Patients with Diabetes
|
|
|
- Jewel Tucker
- 6 years ago
- Views:
Transcription
1 New Approaches for Treating Challenging Patients with Diabetes Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs
2 Disclosure of Potential Conflicts of Interest Consultantship Abbott Diabetes Care Amgen/Astra Zeneca BD, BI CVS/Caremark FDA Janssen, Lexicon, Lilly Medscape, Merck NovoNordisk OptumRX Sanofi Research Funding Janssen Medtronic Foundation

3 Inzucchi SE, et al. Diabetologia. 2015;58(3):

4 Monotherapy Efficacy * Hypo risk Weight Side effects Costs Dual therapy Efficacy * Hypo risk Weight Side effects Costs Healthy eating, weight control, increased physical activity & diabetes education Metformin high low risk neutral/loss GI / lactic acidosis low If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (order not meant to denote any specific preference - choice dependent on a variety of patient- & disease-specific factors): Metformin + Sulfonylurea high moderate risk gain hypoglycemia low Metformin + Thiazolidinedione high low risk gain edema, HF, fxs low Metformin + DPP-4 inhibitor intermediate low risk neutral rare high Metformin + SGLT2 inhibitor intermediate low risk loss GU, dehydration high Metformin + GLP-1 receptor agonist high low risk loss GI high Metformin + Insulin (basal) highest high risk gain hypoglycemia variable Triple therapy If HbA1c target not achieved after ~3 months of triple therapy and patient: (1) on oral combination, move to injectables, (2) on GLP-1 RA, add basal insulin, or (3) on optimally titrated basal insulin, add GLP-1-RA or mealtime insulin. In refractory patients consider adding TZD or SGLT2-i. Metformin + Basal Insulin + Mealtime Insulin or GLP-1-RA Combination injectable therapy Diabetes Care 2015;38: ; Diabetologia 2015;58:
5 GLP-1 Secretion and Inactivation Mixed meal Intestinal GLP-1 release GLP-1 active GLP-1 Agonists A1c Exenatide reduction Weight Liraglutide loss Albiglutide No hypos Injectable Dulaglutide GI side effects DPP-4 Inhibitors DPP-4 A1c Sitagliptin reduction Weight Saxagliptin neutral No Linagliptin hypos DPP-4 inhibitor GLP-1 inactive Alogliptin Few SE s/pill Adapted from Rothenberg P, et al. Diabetes. 2000;49(suppl 1):A39.
6 The GLP-1 RA Class: Pharmacokinetic Properties GLP-1 RA Short-acting (<24 hours) Long-acting ( 24 hours) Exenatide BID Lixisenatide OD Liraglutide OD Dulaglutide OW Albiglutide OW Semaglutide OW Exenatide OW BID, twice daily; GLP-1, glucagon-like peptide-1; GLP-1RA, glucagon-like peptide-1 receptor agonist; OD, once daily; OW, once weekly 1. Byetta. Summary of Product Characteristics; 2. Lyxumia. Summary of Product Characteristics; 3. Victoza. Summary of Product Characteristics; 4. Barrington P, et al. Diabetes Obes Metab. 2011;13: ; 5. Bush MA, et al. Diabetes Obes Metab. 2009;11: ; 6. Matthews JE, et al. J Clin Endo Metab. 2008;93: ; 7. Novo Nordisk. Data on file; 8. Fineman M, et al. Clin Pharmacokinet 2011;50:65 74.
7 Structure of US Approved GLP-1 RAs Diabetes Metab Syndr Obes May 15;2:37
8 Albiglutide GLP-1 H A E G T F T S D V S S Y L E G Q A A K E F I A W L V K G R G Site of proteolytic inactivation (DPP-4) Albiglutide (7-37) amide H A E G T F T S D V S S Y L E G Q A A K E F I A W L V K G R H A E G T F T S D V S S Y L E G Q A A K E F I A W L V K G R Albumin 2 GLP-1 molecules in tandem Covalently bound to albumin DPP-4 resistant Half-life ~ 6-7 days Drucker D, et al. Lancet. 2006;368: Bush M, et al. Diabetes Obesity Metabolism (in press). Pratley/Endo//14Jun13
9 Dulaglutide: A Recombinant GLP-1 Fc Fusion Protein Dulaglutide is a recombinant fusion protein linking a human GLP-1 peptide analog and a variant of a human IgG4 Fc fragment Dulaglutide was engineered for: Duration of pharmacodynamic activity DPP-IV inactivation Solubility Reduced immunogenic potential GLP-1 peptide Linker peptide Modified IgG4 Fc domain
10 Use of Dulaglutide
11 DUAL-1 Study Design Inclusion criteria Type 2 diabetes Insulin-naïve, Patients treated with with metformin Type ± 2 pioglitazone Diabetes HbA 1c % (n= 1663) BMI 40 kg/m 2 Age 18 years * IDegLira OD + metformin ± pioglitazone (n=834) Degludec OD + metformin ± pioglitazone (n=414) Liraglutide OD (1.8 mg) + metformin ± pio (n=415) 0 26 weeks N=1663, Randomized 2:1:1 Open-label Start dose Max. dose IDeg 10 units Not specified Lira 0.6 mg 1.8 mg IDegLira 10 dose steps (10 units IDeg/ 0.36 mg Lira) 50 dose steps (50 units IDeg/ 1.8 mg Lira) Gough SC, et al. Lancet Diabetes Endocrinol. 2014; 2: Titration algorithm: IDegLira and Basal Mean fasting Insulin PG Dose change mg/dl mmol/l dose steps or U <72 < >90 > Not FDA approved
 Mean values (±SEM) based on FAS and LOCF-imputed data; EOT = end of trial; --- ADA/EASD HbA 1c target <7.0%; AACE HbA 1c target 6.5% -1.91% 6.")
12 DUAL-1 Study Results Liraglutide (n=414) Degludec (n=413) IDegLira* (n=833) 7.5 HbA 1 c (%) 7.0 HbA 1C EOT -1.28% 7.0% -1.44% 6.9% Time (weeks) Mean values (±SEM) based on FAS and LOCF-imputed data; EOT = end of trial; --- ADA/EASD HbA 1c target <7.0%; AACE HbA 1c target 6.5% -1.91% 6.4% p< vs. IDeg and vs. Liraglutide p-values are from an ANCOVA Gough SC, et al. Lancet Diabetes Endocrinol. 2014; 2: *Not FDA approved


13 Intarcia Exenatide Sustained Delivery Device: ITCA 650
14 Extension 1: Sustained Efficacy Over 65 Weeks Change From Baseline HbA1c by Visit (mitt Population) Mean (SE) HbA1c (%) Change From Baseline 0 ITCA mcg/day (N=38) -1-2 Extension Week HBL


15 Filtered glucose load 180 g/day Normal Glucose Homeostasis Depends on Reabsorption in the Kidney Glucose Virtually In healthy all of individuals, the filtered the glucose renal is reabsorbed glomeruli in filter the approximately proximal tubules 162 g through of glucose the sodium per day glucose cotransporters SGLT2 and SGLT1 SGLT 2 ~90% SGLT1 ~10% SGLT1=sodium glucose cotransporter 1; SGLT2=sodium glucose cotransporter 2. Abdul-Ghani MA, DeFronzo RA. Endocr Pract. 2008;14: No Glycosuria 1 5

16 Inhibitors of SGLT-2 Co-Transporter Increases Renal Glucose Excretion In the presence of SGLT-2 inhibitor, the less glucose is reabsorbed. The result is glycosuria SGLT 2 ~90% SGLT1 ~10% Abdul-Ghani MA, DeFronzo RA. Endocr Pract. 2008;14: Glycosuria 1 6
17 SGLT2 Inhibitors Lower Renal Threshold for Glucose Excretion (RT G ) Urinary glucose excretion (g/day) T2DM + SGLT2 inhibition Healthy 180 mg/dl T2DM 240 mg/dl RT G RT G RT G 50 SGLT2 inhibition Plasma glucose (mg/dl) Adapted with permission from Abdul-Ghani MA, DeFronzo RA. T2DM = type 2 diabetes mellitus. 1. Abdul-Ghani MA, DeFronzo RA. Endocr Pract. 2008;14(6): Nair S, Wilding JP. J Clin Endocrinol Metab. 2010;95(1):34-42.
18 Canagliflozin/Dapagliflozin/Empagliflozin Warnings and Precautions o o o o o o Hypoglycemia: risk with secretagogues and/or insulin Genital mycotic infections Volume depletion/orthostatic changes Hypersensitivity Increased LDL Bladder cancer: don t use if active; use with caution if prior history of bladder cancer (dapagliflozin only) RxList, 2014.
19 Dapa/Cana/Empa in Patients with Renal Impairment Canagliflozin Contraindicated in patients with egfr <45 ml/min/1.73 m 2 Dose is limited to 100 mg daily if egfr 45-<60 ml/min/1.73 m 2 Dapagliflozin Contraindicated in patients with egfr <60 ml/min/1.73 m 2 Empagliflozin Contraindicated if egfr <45 ml/min/1.73 m 2 Drugs.com, Bristol-Myers Squibb, 2014.
20 Meta-analysis of intensive glucose control in T2DM: major CV events including heart failure Number of events More intensive Less intensive Difference in HbA1c (%) HR (95% CI) Stroke (0.83, 1.10) Myocardial infarction (0.76, 0.94) Hospitalisation for or death from heart failure (0.86, 1.16) Favours more intensive Favours less intensive Meta-analysis of 27,049 participants and 2370 major vascular events from: ADVANCE UKPDS ACCORD VADT HR, hazard ratio; CV, cardiovascular Turnbull FM et al. Diabetologia 2009;52:
21 EMPA-REG OUTCOME Randomised, double-blind, placebo-controlled CV outcomes trial Objective To examine the long-term effects of empagliflozin versus placebo, in addition to standard of care, on CV morbidity and mortality in patients with type 2 diabetes and high risk of CV events CV, cardiovascular 21
22 Trial design Placebo (n=2333) Screening (n=11531) Randomised and treated (n=7020) Empagliflozin 10 mg (n=2345) Empagliflozin 25 mg (n=2342) Study medication was given in addition to standard of care Glucose-lowering therapy was to remain unchanged for first 12 weeks Treatment assignment double masked The trial was to continue until at least 691 patients experienced an adjudicated primary outcome event 22
23 Key inclusion and exclusion criteria Key inclusion criteria Adults with type 2 diabetes BMI 45 kg/m 2 HbA1c 7 10%* Established cardiovascular disease Prior myocardial infarction, coronary artery disease, stroke, unstable angina or occlusive peripheral arterial disease Key exclusion criteria egfr <30 ml/min/1.73m 2 (MDRD) BMI, body mass index; egfr, estimated glomerular filtration rate; MDRD, Modification of Diet in Renal Disease *No glucose-lowering therapy for 12 weeks prior to randomisation or no change in dose for 12 weeks prior to randomisation or, in the case of insulin, unchanged by >10% compared to the dose at randomisation 23
24 Pre-specified primary and key secondary outcomes Primary outcome 3-point MACE: Time to first occurrence of CV death, non-fatal MI or non-fatal stroke Key secondary outcome 4-point MACE: Time to first occurrence of CV death, non-fatal MI, non-fatal stroke or hospitalisation for unstable angina CV, cardiovascular; MI, myocardial infarction; MACE, Major Adverse Cardiovascular Event 24
25 Baseline characteristics Placebo (n=2333) Empagliflozin 10 mg (n=2345) Empagliflozin 25 mg (n=2342) Age, years 63.2 (8.8) 63.0 (8.6) 63.2 (8.6) Male 1680 (72.0) 1653 (70.5) 1683 (71.9) Region Europe 959 (41.1) 966 (41.2) 960 (41.0) North America* 462 (19.8) 466 (19.9) 466 (19.9) Asia 450 (19.3) 447 (19.1) 450 (19.2) Latin America 360 (15.4) 359 (15.3) 362 (15.5) Africa 102 (4.4) 107 (4.6) 104 (4.4) Data are n (%) or mean (SD) in patients treated with 1 dose of study drug *Includes Australia and New Zealand 25
26 Baseline characteristics: type 2 diabetes Glucose-lowering medication* Placebo (n=2333) Empagliflozin 10 mg (n=2345) Empagliflozin 25 mg (n=2342) HbA1c, % 8.08 (0.84) 8.07 (0.86) 8.06 (0.84) Time since diagnosis of type 2 diabetes, years (18.1) 406 (17.3) 434 (18.6) >5 to (24.5) 585 (24.9) 590 (25.2) > (57.4) 1354 (57.7) 1318 (56.3) Metformin 1734 (74.3) 1729 (73.7) 1730 (73.9) Sulphonylurea 992 (42.5) 985 (42.0) 1029 (43.9) Thiazolidinedione 101 (4.3) 96 (4.1) 102 (4.4) Insulin 1135 (48.6) 1132 (48.3) 1120 (47.8) Mean daily dose, U** 65 (50.6) 65 (47.9) 66 (48.9) Data are n (%) or mean (SD) in patients treated with 1 dose of study drug *Medication taken alone or in combination **Placebo, n=1135; empagliflozin 10 mg, n=1132; empagliflozin 25 mg, n=
27 Baseline characteristics: CV risk factors Placebo (n=2333) Empagliflozin 10 mg (n=2345) Empagliflozin 25 mg (n=2342) Body mass index, kg/m (5.2) 30.6 (5.2) 30.6 (5.3) Weight, kg 86.6 (19.1) 85.9 (18.8) 86.5 (19.0) Waist circumference, cm (14.0) (13.7) (13.7) Systolic blood pressure, mmhg (17.2) (16.8) (17.0) Diastolic blood pressure, mmhg 76.8 (10.1) 76.6 (9.8) 76.6 (9.7) Heart rate, bpm* 70.7 (0.2) 71.0 (0.2) 70.5 (0.2) LDL cholesterol, mg/dl 84.9 (35.3) 86.3 (36.7) 85.5 (35.2) HDL cholesterol, mg/dl 44.0 (11.3) 44.7 (12.0) 44.5 (11.8) egfr, ml/min/1.73m 2 (MDRD) 73.8 (21.1) 74.3 (21.8) 74.0 (21.4) 90 ml/min/1.73m (20.9%) 519 (22.1%) 531 (22.7%) 60 to <90 ml/min/1.73m (53.1%) 1221 (52.1%) 1204 (51.4%) <60 ml/min/1.73m (26.0%) 605 (25.8%) 607 (25.9%) Data are n (%) or mean (SD) in patients treated with 1 dose of study drug *Mean (SE). LDL, low density lipoprotein; HDL, high density lipoprotein; egfr, estimated glomerular filtration rate; MDRD, Modification of Diet in Renal Disease equation 27
28 Baseline characteristics: CV complications Placebo (n=2333) Empagliflozin 10 mg (n=2345) Empagliflozin 25 mg (n=2342) Any CV risk factor 2307 (98.9%) 2333 (99.5%) 2324 (99.2%) Coronary artery disease 1763 (75.6%) 1782 (76.0%) 1763 (75.3%) Multi-vessel coronary artery disease 1100 (47.1%) 1078 (46.0%) 1101 (47.0%) History of MI 1083 (46.4%) 1107 (47.2%) 1083 (46.2%) Coronary artery bypass graft 563 (24.1%) 594 (25.3%) 581 (24.8%) History of stroke 553 (23.7%) 535 (22.8%) 549 (23.4%) Peripheral artery disease 479 (20.5%) 465 (19.8%) 517 (22.1%) Single vessel coronary artery disease 238 (10.2%) 258 (11.0%) 240 (10.2%) Cardiac failure* 244 (10.5%) 240 (10.2%) 222 (9.5%) Data are n (%) in patients treated with 1 dose of study drug *Based on narrow standardised MedDRA query cardiac failure 28
29 Baseline characteristics: CV medication (1) Placebo (n=2333) Empagliflozin 10 mg (n=2345) Empagliflozin 25 mg (n=2342) Anti-hypertensive therapy 2221 (95.2%) 2227 (95.0%) 2219 (94.7%) ACE inhibitors/arbs 1868 (80.1%) 1896 (80.9%) 1902 (81.2%) Beta-blockers 1498 (64.2%) 1530 (65.2%) 1526 (65.2%) Diuretics 988 (42.3%) 1036 (44.2%) 1011 (43.2%) Calcium channel blockers 788 (33.8%) 781 (33.3%) 748 (31.9%) Mineralocorticoid receptor antagonists 136 (5.8%) 157 (6.7%) 148 (6.3%) Renin inhibitors 19 (0.8%) 16 (0.7%) 11 (0.5%) Other 191 (8.2%) 193 (8.2%) 190 (8.1%) Data are n (%) in patients treated with 1 dose of study drug ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blockers 29
30 Baseline characteristics: CV medication (2) Placebo (n=2333) Empagliflozin 10 mg (n=2345) Empagliflozin 25 mg (n=2342) Lipid-lowering drugs 1864 (79.9%) 1926 (82.1%) 1894 (80.9%) Statins 1773 (76.0%) 1827 (77.9%) 1803 (77.0%) Fibrates 199 (8.5%) 214 (9.1%) 217 (9.3%) Ezetimibe 81 (3.5%) 95 (4.1%) 94 (4.0%) Niacin 35 (1.5%) 56 (2.4%) 35 (1.5%) Other 175 (7.5%) 172 (7.3%) 193 (8.2%) Anti-coagulants and antiplatelets 2090 (89.6%) 2098 (89.5%) 2064 (88.1%) Acetylsalicylic acid 1927 (82.6%) 1939 (82.7%) 1937 (82.7%) Clopidogrel 249 (10.7%) 253 (10.8%) 241 (10.3%) Vitamin K antagonists 156 (6.7%) 141 (6.0%) 125 (5.3%) Data are n (%) in patients treated with 1 dose of study drug 30
31 Adjusted mean (SE) HbA1c (%) HbA1c Placebo Empagliflozin 10 mg Empagliflozin 25 mg Week Placebo Empagliflozin 10 mg Empagliflozin 25 mg All patients (including those who discontinued study drug or initiated new therapies) were included in this mixed model repeated measures analysis (intent-to-treat) X-axis: timepoints with reasonable amount of data available for pre-scheduled measurements 31
32 Adjusted mean (SE) weight (kg) Weight Placebo Empagliflozin 10 mg Empagliflozin 25 mg Week Placebo Empagliflozin 10 mg Empagliflozin 25 mg All patients (including those who discontinued study drug or initiated new therapies) were included in this mixed model repeated measures analysis (intent-to-treat) X-axis: timepoints with reasonable amount of data available for pre-scheduled measurements 32
33 Adjusted mean (SE) systolic blood pressure (mmhg) Systolic blood pressure Placebo Empagliflozin 25 mg Empagliflozin 10 mg Week Placebo 2322 Empagliflozin 10 mg 2322 Empagliflozin 25 mg All patients (including those who discontinued study drug or initiated new therapies) were included in this mixed model repeated measures analysis (intent-to-treat) X-axis: timepoints with reasonable amount of data available for pre-scheduled measurements 33
34 Primary outcome: 3-point MACE HR 0.86 (95.02% CI 0.74, 0.99) p=0.0382* Cumulative incidence function. MACE, Major Adverse Cardiovascular Event; HR, hazard ratio. * Two-sided tests for superiority were conducted (statistical significance was indicated if p ) 34
35 CV death HR 0.62 (95% CI 0.49, 0.77) p< Cumulative incidence function. HR, hazard ratio 35
36 CV death Empagliflozin 10 mg HR 0.65 (95% CI 0.50, 0.85) p= Empagliflozin 25 mg HR 0.59 (95% CI 0.45, 0.77) p= Cumulative incidence function. HR, hazard ratio 36
37 CV death, MI and stroke Patients with event/analysed Empagliflozin Placebo HR (95% CI) p-value 3-point MACE 490/ / (0.74, 0.99)* CV death 172/ / (0.49, 0.77) < Non-fatal MI 213/ / (0.70, 1.09) Non-fatal stroke 150/ / (0.92, 1.67) Favours empagliflozin Favours placebo Cox regression analysis. MACE, Major Adverse Cardiovascular Event; HR, hazard ratio; CV, cardiovascular; MI, myocardial infarction *95.02% CI 37
38 Fatal and non-fatal stroke Intent-to-treat population Patients with event/analysed Empagliflozin Placebo HR (95% CI) p-value 164/ / (0.89, 1.56) Numerical difference largely driven by events occurring >30 days after treatment stop On-treatment analysis* Favours empagliflozin Favours placebo 141/ / (0.78, 1.40) Favours empagliflozin Favours placebo Cox regression analysis. MACE, Major Adverse Cardiovascular Event; HR, hazard ratio; *Excluding events >30 days after last intake of study drug and patients who received study drug for <30 days (cumulative)
39 Hospitalisation for heart failure HR 0.65 (95% CI 0.50, 0.85) p= Cumulative incidence function. HR, hazard ratio 39
40 All-cause mortality HR 0.68 (95% CI 0.57, 0.82) p< Kaplan-Meier estimate. HR, hazard ratio 41
41 Number needed to treat (NNT) to prevent one death across landmark trials in patients with high CV risk Simvastatin 1 for 5.4 years Ramipril 2 for 5 years Empagliflozin for 3 years High CV risk 5% diabetes, 26% hypertension Pre-statin era High CV risk 38% diabetes, 46% hypertension Pre-ACEi/ARB era <29% statin T2DM with high CV risk 92% hypertension >80% ACEi/ARB >75% statin S investigator. Lancet 1994; 344: , 2. HOPE investigator N Engl J Med 2000;342:145-53, 42
42 EMPA-REG OUTCOME : Therapeutic considerations Empagliflozin, as used in this trial, for 3 years in 1,000 patients with type 2 diabetes at high CV risk: 25 lives saved (82 vs 57 deaths) 22 fewer CV deaths (59 vs 37) 14 fewer hospitalisations for heart failure (42 vs 28) 53 additional genital infections (22 vs 75) 43
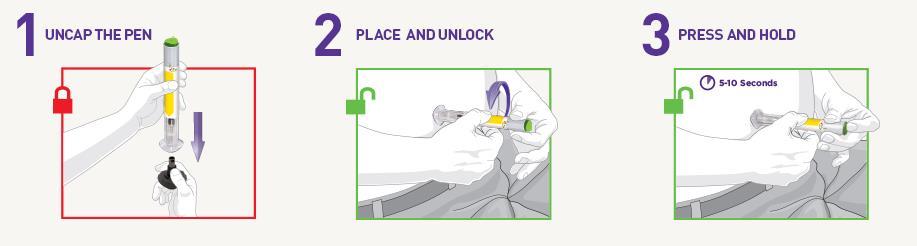
43 Technosphere Inhaler Cavaiola T, Edelman S. Clin Ther 2014;36:
44 Tools for Treating Diabetes Technology ever increasing Pace always far slower than any of us desire Each device approved is still one or two or three versions behind what is possible Tools are only as good as the user can use them education/follow-up/realtime and retrospective interpretation vital elements



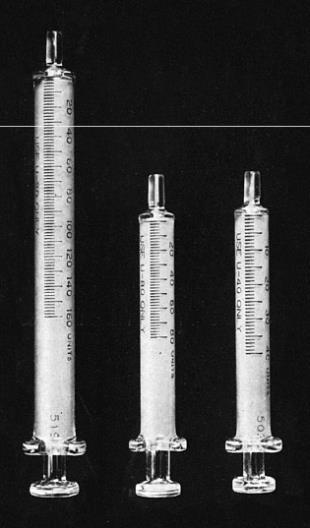
45 Diabetes Care in the 1970s

46 Diabetes Care in 2015



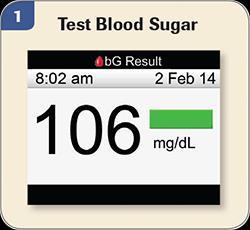
47 Monitoring

48 Abbott Freestyle Libre

49 Easier Communication
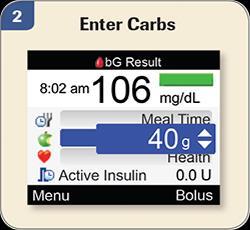
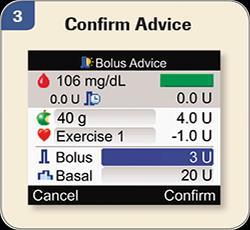
50 Bolus Calculator

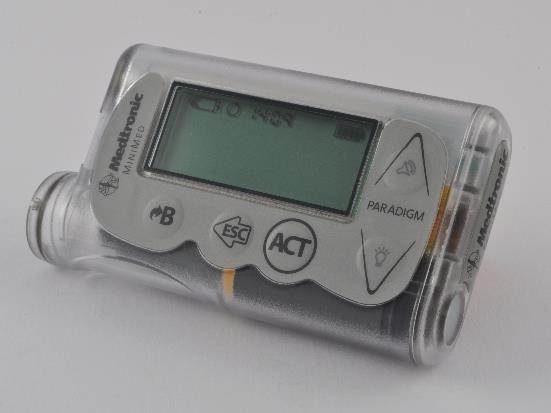
51 Medtronic Pump

52 Patch Pumps

53 Patch Pumps

54 The Value of Continuous Glucose Monitoring

55 CGM: Dexcom Gen 5
")
56 Closed Loop Automatic Systems (Pump-Sensor)
57

58 Sensor Glucose Values During Threshold- Suspend Events Bergenstal RM et al. N Engl J Med 2013;369: Bergenstal RM et al. N Engl J Med 2013;369:
59 Patient: Minimed 530G Threshold Suspend


60 Infusion Site Issues Another Understudied Factor


61 Infusion Site Issues: Another Understudied Factor


62 Technosphere Inhaler: Initial and Gen2 Device Cavaiola T, Edelman S. Clin Ther 2014;36:

63 Afrezza Prescribing information. Dosing of Inhaled Insulin
64 Afrezza Prescribing information. Inhaled Insulin Label
65 Glucose-Infusion Rate and Serum Insulin Concentrations in T1D Afrezza Prescribing information.
66 Technosphere Inhaled Insulin: Clinical Features of Note Compared with Aspart 70/30, inhaled insulin was associated with reduced risk for - Hypoglycemia (0.41 vs 0.61 per patient/per month) - Weight gain (0.9 kg vs 2.5 kg) Increased risk for cough (33% vs 6%) - No change in FEV1 - No difference in URI Rosenstock J et al. Lancet 2010;375:
67 Conclusions New treatments for diabetes continue to evolve The SGLT-2 inhibitor class holds great promise to improve CVD risk as well as BG outcomes. Always individualize treatment and care
68 THANK YOU
The EMPA-REG OUTCOME trial: Design and results. David Fitchett, MD University of Toronto, Canada
 The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Multi-factor approach to reduce cardiovascular risk in diabetes
 Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
SESSION 4 12:30pm 1:45pm
 SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
COPYRIGHT. Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely?
 Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
The Role Of SGLT-2 Inhibitors In Clinical Practice. Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs
 The Role Of SGLT-2 Inhibitors In Clinical Practice Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest Consultantship
The Role Of SGLT-2 Inhibitors In Clinical Practice Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest Consultantship
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
GLP-1RA and insulin: friends or foes?
 Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Diabetes and New Meds for Cardiovascular Risk Reduction. F. Dwight Chrisman, MD, FACC. Disclosures: BI Boehringer Ingelheim speaker
 Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure?
 UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Help the Heart. An Update on GLP-1 Agonists and SGLT2 Inhibitors. Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire
 Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Diabetes and Heart Failure: The Role of SGLT2 Inhibitors
 22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk
 Managing Diabetes & CVD: Expling New Evidence & Opptunities ESC Congress, London, UK 30 August, 2015 SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk Silvio E. Inzucchi MD Yale
Managing Diabetes & CVD: Expling New Evidence & Opptunities ESC Congress, London, UK 30 August, 2015 SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk Silvio E. Inzucchi MD Yale
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes
 LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
Very Practical Tips for Managing Type 2 Diabetes
 Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
Peter Stein, MD Janssen Research and Development
 New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Ertugliflozin (Steglatro ) 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy
 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy") Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM
 Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors. Bryce Fukunaga PharmD April 25, 2018
 Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Safety profile of Liraglutide: Recent Updates. Mohammadreza Rostamzadeh,M.D.
 Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
LEADER and EMPA-REG. John Buse, MD, PhD. University of North Carolina School of Medicine Chapel Hill, NC, USA. Duality of Interest Declaration
 1 LEADER and EMPA-REG John Buse, MD, PhD University of Nth Carolina School of Medicine Chapel Hill, NC, USA Duality of Interest Declaration I rept the following potential duality/dualities of interest
1 LEADER and EMPA-REG John Buse, MD, PhD University of Nth Carolina School of Medicine Chapel Hill, NC, USA Duality of Interest Declaration I rept the following potential duality/dualities of interest
T2 Diabetes in Sep-16. Stephen Leow Disclosures. Why do we treat diabetes? Agenda. Targets
 Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes
 Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Lilly Diabetes: Pipeline Update
 Lilly Diabetes: Pipeline Update June 16, 2014 Safe Harbor Provision This presentation contains forward-looking statements that are based on management's current expectations, but actual results may differ
Lilly Diabetes: Pipeline Update June 16, 2014 Safe Harbor Provision This presentation contains forward-looking statements that are based on management's current expectations, but actual results may differ
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital
 Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD. Disclosures. Objectives 9/1/2015
 Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
Top HF Trials to Impact Your Practice
 Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Joshua Settle, PharmD Clinical Pharmacist Baptist Medical Center South ALSHP Fall Meeting September 30, 2016
 Joshua Settle, PharmD Clinical Pharmacist Baptist Medical Center South jjsettle@baptistfirst.org ALSHP Fall Meeting September 30, 2016 Objectives Describe the current information concerning newly approved
Joshua Settle, PharmD Clinical Pharmacist Baptist Medical Center South jjsettle@baptistfirst.org ALSHP Fall Meeting September 30, 2016 Objectives Describe the current information concerning newly approved
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks
 Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
ANGELA GINN-MEADOW RD LDN CDE
 DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for
DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus
 Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Invokana (canagliflozin) NEW INDICATION REVIEW
 NEW INDICATION REVIEW") Invokana (canagliflozin) NEW INDICATION REVIEW Introduction Brand name: Invokana Generic name: Canagliflozin Pharmacological class: Sodium-glucose cotransporter 2 (SGLT2) inhibitor Strength and Formulation:
Invokana (canagliflozin) NEW INDICATION REVIEW Introduction Brand name: Invokana Generic name: Canagliflozin Pharmacological class: Sodium-glucose cotransporter 2 (SGLT2) inhibitor Strength and Formulation:
Newer Therapies for Type 2 Diabetes
 Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Du gusts is megl che one. Edoardo Mannucci
 Du gusts is megl che one Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer Ingelheim, Eli
Du gusts is megl che one Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer Ingelheim, Eli
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants:
 In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
Basal & GLP-1 Fixed Combination Use
 Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
Dr Brandon Orr-Walker
 Dr Brandon Orr-Walker Endocrinologist Clinical Head of Endocrinology and Diabetes Middlemore Auckland 17:45-18:10 What Can New Agents Offer Us? Diabetes Management What do the new agents offer us? Brandon
Dr Brandon Orr-Walker Endocrinologist Clinical Head of Endocrinology and Diabetes Middlemore Auckland 17:45-18:10 What Can New Agents Offer Us? Diabetes Management What do the new agents offer us? Brandon
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
Dapagliflozin and cardiovascular outcomes in type 2
 EARN 3 FREE CPD POINTS diabetes Leader in digital CPD for Southern African healthcare professionals Dapagliflozin and cardiovascular outcomes in type 2 diabetes Introduction People with type 2 diabetes
EARN 3 FREE CPD POINTS diabetes Leader in digital CPD for Southern African healthcare professionals Dapagliflozin and cardiovascular outcomes in type 2 diabetes Introduction People with type 2 diabetes
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs
 Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
SGLT2 Inhibition in T2DM Management: Current Position and Future Promise
 SGLT2 Inhibition, Diabetes and CVD: Where Does This Fit in CV Risk Management? ESC Congress, Rome, Italy 28 August, 2016 SGLT2 Inhibition in T2DM Management: Current Position and Future Promise Silvio
SGLT2 Inhibition, Diabetes and CVD: Where Does This Fit in CV Risk Management? ESC Congress, Rome, Italy 28 August, 2016 SGLT2 Inhibition in T2DM Management: Current Position and Future Promise Silvio
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes. April 2010
 Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Type 2 Diabetes Management: Case 1: Reducing Hypoglycemic Risk Case 2: Reducing Cardiovascular Risk
 Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
1. Pharmacokinetics. When is steady state achieved? Steady-state was reached after 4 to 5 days of once-daily dosing with Sulisent 100 mg to 300mg.
 1. Pharmacokinetics How is Sulisent metabolized? Sulisent has a novel mechanism of action that targets the kidneys and allows for excess glucose excretion resulting in urinary calorie loss. Sulisent is
1. Pharmacokinetics How is Sulisent metabolized? Sulisent has a novel mechanism of action that targets the kidneys and allows for excess glucose excretion resulting in urinary calorie loss. Sulisent is
3/8/2011. Julie M. Sease, Pharm D, BCPS, CDE Associate Professor of Pharmacy Practice Presbyterian College School of Pharmacy
 Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials
 Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
GLP-1. GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4.
 GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
Achieving and maintaining good glycemic control is an
 Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Terapia con agonisti GLP1 e outcome cardiovascolare. Edoardo Mannucci
 Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study
 for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study") Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
Making Sense of New DM Therapies and Technologies
 Making Sense of New DM Therapies and Technologies Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and
Making Sense of New DM Therapies and Technologies Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and