Endocrinology Cases and Clinical Pearls QUANG NGUYEN, DO, FACE, FTOS LAS VEGAS ENDOCRINOLOGY 5/5/18
|
|
|
- Lucas Turner
- 6 years ago
- Views:
Transcription
1 Endocrinology Cases and Clinical Pearls QUANG NGUYEN, DO, FACE, FTOS LAS VEGAS ENDOCRINOLOGY 5/5/18
2 Q1 A 59-year-old man with an 18-year history of diabetes mellits is being treated with inslin glargine and metformin. He has had longstanding hypertension, hyperlipidemia, and renal insfficiency, bt no previos heart attack or stroke. His review of systems is negative. He stopped smoking cigarettes 2 years ago. He asks for recommendations to help him redce his risk of a cardiovasclar event. Both his father and paternal ncle have diabetes and developed coronary artery disease reqiring stenting.
3 Q1 His medication regimen is as follows: inslin glargine, 36 nits at bedtime metformin, 500 mg twice daily atorvastatin lisinopril hydrochlorothiazide amlodipine
4 Q1 Blood pressre is 138/82 mm Hg and plse rate is 88 beats/min. His height is 73.5 in (186.7 cm), and weight is 247 lb (112 kg) (BMI = 32.1 kg/m2). Eye examination reveals bilateral retinal microanerysms. On cardiac examination, he has a reglar rate and rhythm, a lod S4, no S3, and no mrmrs. There are no carotid brits. His abdomen is obese with no striae or renal brits. On nerologic examination, there is symmetric decreased light toch and vibration sense in both feet.
5 Q1 Laboratory test reslts: Hemoglobin A1c = 8.3% (4.0%-5.6%) Fasting glcose = 142 mg/dl (70-99 mg/dl) Serm rea nitrogen = 31 mg/dl (8-23 mg/dl) Creatinine = 1.8 mg/dl ( mg/dl) Estimated glomerlar filtration rate = 40 ml/min per 1.73 m2 (>60 ml/min per 1.73 m2) Liver fnction, normal
6 Q1 Yo decided to add therapy. Which of the following is the best agent for this patient? A. Premeal aspart inslin B. Glipizide C. Acarbose D. Sitagliptin E. Liragltide
7 14 Classes of Drgs Available for the Treatment of Type 2 DM in the USA ### Class A1c Redction Hypoglycemia Weight Change Dosing (times/day) 01 Metformin No Netral-Loss GLP-1 agonists No Loss 1-2, QW Injected 03 DPP-IV inhibitors No Netral 1, QW 04 SGLT2 inhibitors No Loss 1 05 Slfonylreas Yes Gain Repaglinide Yes Gain 3 07 Nateglinide Rare Gain 3 08 Bromocriptine No Netral 1 09 Bile acid seqestrant 0.5 No Netral α-glcosidase inhibitor No Netral 3 11 Thiazolidinediones No Gain 1 12 Amylin mimetics No Loss 3, Injected 13 Inslin, rapid-acting Yes Gain 1-4, Injected 14 Inslin, long-acting Yes Gain 1-2, Injected

8 The Ominos Octet Islet b-cell Impaired Inslin Secretion Islet a-cell Decreased Incretin Effect Increased Lipolysis Increased Glcagon Secretion Increased Glcose Resorption Increased Hepatic Glcose Prodction Nerotransmitter Dysfnction Decreased Glcose Uptake
9 Complementary Mechanisms of Action of Crrent Diabetes Medications Inslin SlfonylreasIslet b-cell Megltinides TZDs GLP-1 RA GLP-1 RA DPP-4 inhibitors Decreased Incretin Effect Impaired Inslin Secretion GLP-1 RA Islet a-cell DPP-4 inhibitors Pramlintide Bromocriptine GLP-1 RA Increased Hepatic Glcose Prodction Nerotransmitter Dysfnction Diabetes 2009;58: Increased Lipolysis SGLT-2 inhibitors Increased Glcose Resorption Increased Glcagon Secretion Metformin Inslin TZD GLP-1RA Inslin TZDs Inslin TZDs Decreased Glcose Uptake
10 Diabetes Cardiovasclar Otcome Trials Drg MACE CV Non-Fatal Non-Fatal Death MI Stroke Empagliflozin SGLT2i Canagliflozin SGLT2i Liragltide GLP-1A Semagltide GLP-1A Exenatide GLP-1A Lixisenatide GLP-1A ITCA 650 GLP-1A Saxagliptin DPP-IVi Sitagliptin DPP-IVi Alogliptin DPP-IVi Acarbose a-glcosidase = speriority = non-inferiority

11 QUESTIONS? Endocr Pract 2016;22 (No. 1)
12 GLP-1 Receptor Agonists Exenatide (Byetta) Lixisenatide (Lyxmia) Liragltide (Victoza) Dlagltide (Trlicity) Exenatide ER (Bydreon) Albigltide (Tanzem) Semagltide (Ozempic)

13 GLP-1 Agonists
14 Incretin Effect in Healthy Sbjects
15 Beta-Cell Workload and Response Are Balanced in Healthy Sbjects Carbohydrate Meal Healthy Sbjects Inslin (µu/ml) Glcagon (pg/ml) Glcose (mg/dl) Meal Time (min) n = 14; Mean (SE) Data from Mϋller WA, et al. N Engl J Med. 1970;283:
16 Beta-Cell Workload Otpaces Response in Type 2 Diabetes Inslin (µu/ml) Glcagon (pg/ml) Carbohydrate Meal Healthy Sbjects Type 2 Diabetes Glcose (mg/dl) Meal Time (min) N = 26; Mean (SE) Data from Mϋller WA, et al. N Engl J Med. 1970;283:
17 GLP-1 Actions Increase inslin secretion in a glcose-dependent manner Decrease glcagon secretion from pancreas Increases B-cell mass, increase inslin secretion Decrease food intake by increasing satiety Promote inslin sensitivity A1c: 1-1.5%


 20 10 0")


 Data from Fehse F,")
18 Exenatide Restores First-Phase Inslin Response Type 2 Diabetes Healthy Controls Placebo Inslin (pm/kg/min) Inslin (pm/kg/min) Exenatide Exenatide 10 Placebo Glcose Time (min) Glcose Time (min) Evalable; N = 25; Mean (SE) Data from Fehse F, et al. Diabetologia. 2004;47 (sppl 1): A279
19 * * * * * * Postprandial GLP-1 Concentrations Are Lower in Patients With IGT and Type 2 Diabetes Meal Healthy (n = 33) IGT (n = 15) Type 2 Diabetes (n = 54) 20 GLP-1 (pmol/l) * * Time (min) Mean ± SE; *P<0.05 between patients with type 2 diabetes and healthy sbjects; IGT indicates impaired glcose tolerance Data from Toft-Nielsen MB, et al. J Clin Endocrinol Metab. 2001;86:
20 The GLP-1 Receptor Agonist Class: Pharmacokinetic Properties GLP-1 Receptor Agonist Short-acting (<24 hors) Long-acting ( 24 hors) Exenatide BID Lixisenatide QDay Liragltide QDay Dlagltide QWeek Albigltide QWeek Semagltide QWeek Exenatide QWeek Byetta. Smmary of Prodct Characteristics 1 ; Lyxmia. Smmary of Prodct Characteristics 2 ; Victoza. Smmary of Prodct Characteristics 3 ; Diabetes Obes Metab 2011;13: ; Diabetes Obes Metab 2009;11: ; J Clin Endo Metab 2008;93: ; Novo Nordisk. Data on file; 8. Clin Pharmacokinet 2011;50:
21 Short- and Long-acting GLP-1 Receptor Agonists Have Different Effects on Glcose GLP-1 Receptor Agonist Short-acting (<24 hors) Long-acting ( 24 hors) FPG PPG FPG PPG Bols > Basal Basal > Bols Diabetes Obes Metab 2012;14:675

22 Q1 Yo decided to add therapy. Which of the following is the best agent for this patient? A. Premeal aspart inslin B. Glipizide C. Acarbose D. Sitagliptin E. Liragltide
23 Diabetes Cardiovasclar Otcome Trials Drg MACE CV Non-Fatal Non-Fatal Death MI Stroke Empagliflozin SGLT2i Canagliflozin SGLT2i Liragltide GLP-1A Semagltide GLP-1A Exenatide GLP-1A Lixisenatide GLP-1A ITCA 650 GLP-1A Saxagliptin DPP-IVi Sitagliptin DPP-IVi Alogliptin DPP-IVi Acarbose a-glcosidase = speriority = non-inferiority
24
25
26 Q2 A previosly healthy 20-year-old African American man comes to clinic for a follow-p visit. He was hospitalized for treatment of diabetic ketoacidosis 4 months ago. Laboratory test reslts at hospital admission: Plasma glcose = 748 mg/dl (70-99 mg/dl) Bicarbonate = 10 meq/l (21-28 meq/l) Anion gap = 22 meq/l (3-11 meq/l) Creatinine = 2.2 mg/dl ( mg/dl) Estimated glomerlar filtration rate = 34 ml/min per 1.73 m2 (>60 ml/min per 1.73 m2) Moderate ketones present in the serm
27 Q2 Admitted to Valley Hospital Medical Center. He was treated with intravenos flids and a continos inslin infsion. The acidosis resolved and he was discharged on basalbols inslin. The total inslin dose at the time of discharge was 1.0 nits/kg per day. He received diabetes edcation and has modified his diet. He has lost 22 lb (10 kg) since hospital discharge. The inslin doses have been gradally redced over time. He is now administering 12 nits of inslin glargine at bedtime and 3 nits of inslin aspart before breakfast and dinner (he only eats 2 meals per day). The 2-week average glcose vale is 107 mg/dl. The fasting glcose vales range from 79 to 106 mg/dl.
28 Q2 On physical examination, his height is 73 in (185 cm) and weight is 142 lb (BMI = 18.7 kg/m2). His blood pressre is 122/83 mm Hg, and plse rate is 82 beats/min. There is no evidence of acanthosis nigricans. The cardiac, lng, abdominal, and nerologic findings on examination are all normal.
29 Q2 Crrent laboratory test reslts (fasting): Hemoglobin A1c = 5.8% (4.0%-5.6%) Creatinine = 1.3 mg/dl ( mg/dl) Estimated glomerlar filtration rate = >60 ml/min per 1.73 m2 (>60 ml/min per 1.73 m2) Electrolytes, normal TSH, normal C-peptide = 3.2 ng/ml ( ng/ml) Glcose = 124 mg/dl (70-99 mg/dl) Gltamic acid decarboxylase antibodies: POSITIVE
30 Q2 Which of the following is the best next step in treating this patient s diabetes? A. Stop inslin and start empagliflozin B. Stop inslin aspart and start glimepiride C. Stop all inslin and start metformin D. Stop inslin aspart and contine diet treatment E. Contine the crrent inslin regimen


31 Honeymoon Phase
32 Honeymoon Phase Period of time shortly following diabetes diagnosis when the pancreas is still able to prodce enogh amont of inslin to aid blood glcose control. Seqence: DKA When a patient starts on inslin injections, the pancreas is nder less pressre to prodce inslin. This period of rest, afforded by the injections, stimlate the pancreas to prodce inslin from the remaining beta cells. However, after a period of months, the vast majority of these remaining beta cells will also be destroyed, and the honeymoon period ends when the pancreas stops prodcing sfficient inslin to aid blood glcose control any more.
33


34
35 Q2 (Honeymoon Phase) Which of the following is the best next step in treating this patient s diabetes? A. Stop inslin and start empagliflozin B. Stop inslin aspart and start glimepiride C. Stop all inslin and start metformin D. Stop inslin aspart and contine diet treatment E. Contine the crrent inslin regimen
36
37 Q3 A 54-year-old man is referred to yo after a low serm testosterone concentration (120 ng/dl [4.2 nmol/l]) was identified dring the workp of new-onset erectile dysfnction. He has noted no change in weight and no new headache pattern. He has no history of hypertension or diabetes mellits.
38 Q3 On physical examination, his blood pressre is 128/75 mm Hg. His height is 69 in (175.3 cm), and weight is 177 lb (80.5 kg) (BMI = 26.1 kg/m2). Examination findings are normal. Testes are 10 ml bilaterally. Formal visal field testing shows a mild bitemporal defect.
39 Q3 Laboratory test reslts: LH = 2.0 miu/ml ( miu/ml) (SI: 2.0 IU/L [ IU/L]) FSH = 4.2 miu/ml ( miu/ml) (SI: 4.2 IU/L [ IU/L]) Prolactin = 81 ng/ml (4-23 ng/ml) (SI: 3.5 nmol/l [ nmol/l]) Cortisol (8 AM) = 21 µg/dl (5-25 µg/dl) (SI: nmol/l [ nmol/l]) Free T4, normal TSH, normal IGF-1, normal

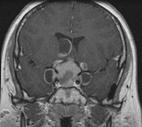
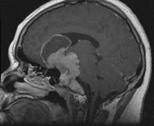
40 Q3 2.3 x 2.2 cm pititary macroademona with sprasellar extension

41 Q3 (bitemporal hemianopsia)
42 Q3 Which of the following is the most appropriate next management step? A. Measre macroprolactin B. Start therapy with bromocriptine or cabergoline C. Refer to nerosrgery D. Start testosterone therapy E. Measre ACTH
43 Q3 (Pititary Adenoma) Common: 10% incidental findings 2 Qestions: 1) Fnctionality Check hormones: (FSH, LH, IGF-1, Prolactin, TSH, ACTH, alpha sbnits) Other tests: CBC, CMP, testosterone, estradiol, am cortisol 2) Physical compression Visal field testing
44 Q3 Testosterone = 120 ng/dl ( ng/dl) LH = 2.0 miu/ml ( miu/ml) FSH = 4.2 miu/ml ( miu/ml) Prolactin = 81 ng/ml (4-23 ng/ml) 1 cm = 200 ng/ml Pearls: Don t act only on a low testosterone Normal vales don t mean they are normal. Evalate in relation to the hormonal abnormalities

45 Q3 Pititary Stalk Compression
46 Q3 Testosterone = 120 ng/dl ( ng/dl) LH = 2.0 miu/ml ( miu/ml) FSH = 4.2 miu/ml ( miu/ml) Prolactin = 81 ng/ml (4-23 ng/ml) 1 cm = 200 ng/ml Pearls: Don t act only on a low testosterone Normal vales don t mean they are normal. Evalate in relation to the hormonal abnormalities Abnormal vales don t mean they are the case. Evalate in relation to the disease process
47 Q3 Which of the following is the most appropriate next management step? A. Measre macro-prolactin B. Start therapy with bromocriptine or cabergoline C. Refer to nerosrgery D. Start testosterone therapy E. Measre ACTH
48

49
50 Q4 29 yo male presented with 3 yr hx of headache, decreased peripheral vision and low libido No meds Exam: BMI: 40.3 kg/m2 BP: 120/82, HR 92 Bitemporal visal loss on confrontation Breast and GU exam: normal
51 Q4 Laboratory data: Prolactin= 36 ng/dl (N: 4-23) Total testosterone= 88 ng/dl (N: ) FSH= 4.2 (N: 1-13) LH= 2.8 (N: 1-9) IGF-1= 188 (N: ) TSH= 2.9 (N: ) 8 am cortisol= 24 (N: 7-26) Free T4: 1.1 (N: )
52 Q4
53 Q4 Radiologist read very big tmor present in the pititary gland extending otside the sella trcica and protrde into the cavernos sinses Measred: 5.0 x 5.2 x 5.6 cm
54 Q4 Qestion: Which one of the following is the next best step? A. Initiate medical therapy with bromocriptine B. Measre 24 hr rinary cortisol C. Re-measre prolactin with serial diltions D. Perform transphenoidal srgery to remove the tmor E. Measre sodim level

55 Q4 HOOK EFFECT
56 Figre 2 Schematic illstrating the principle of a two-site immnometric assay for prolactin Smith TP et al. (2007) Technology Insight: measring prolactin in clinical samples Nat Clin Pract Endocrinol Metab 3: doi: /ncpendmet0447

57 Hook Effect
58
59 Q4 Prolactin was remeasred at 1:10 and 1:100 diltions and the actal vale was 6400 ng/dl (N: 4-23) Final diagnosis: PROLACTINOMA
60 Q4 Qestion: Which one of the following is the next best step? A. Initiate medical therapy with bromocriptine B. Measre 24 hr rinary cortisol C. Re-measre prolactin with serial diltions D. Perform transphenoidal srgery to remove the tmor E. Measre sodim level
61 Q4 (Smmary) Hook effect is present in 6% of clinically nonfnctioning adenomas and 14% of pititary macroadenoma Correct diagnosis is important as prolactinoma can be treated medically whereas nonfnctioning macroadenoma will reqire srgery
62 Clinical Pearls 1. Serial diltions of serm PRL are mandatory in the diagnostic evalation of patients with large pititary tmors 2. Prolactin level correlates with the size of the prolactinoma
63

64 Hang in there
65 Q5 65 yo woman with cc: hypercalcemia Underwent menopase 14 years ago Denies h/o kidney stones or broken bones bt is constipated and always tired
66 Q5 DXA scan 5 years ago revealed osteoporosis at the wrist Hip T: -1.7 Spine T: -1.5 Wrist: T: -2.9
67 Q5 Meds: Calcim carbonate 500 mg tidac Vitamin D3: 2000IU/day Eats 3 cps of yogrt and drinks 2-3 glasses of milk daily Fosamax 70 mg weekly Fmhx: negative Physical Exam: Unremarkable
68 Q5 Labs: CMP NL except: Calcim: 10.4 ( ) Albmin: 4.0 Phosphors: 2.8 Vitamin D: 32 PTH: 46 (10-65) Urinary calcim: 300 mg/24 hr ( mg/24 hr) Urinary Creatinine: 1gm/24 hr
69 Q5 Which one of the following is the most likely case of the patient s hypercalcemia? A. Hypercalcemia of malignancy B. Milk-alkali syndrome C. Primary hyperparathyroidism D. Familial hypocalciric hypercalcemia (FHH) E. Sarcoidosis
70 Q5 Labs: CMP NL except: Calcim: 10.4 ( ) Albmin: 4.0 Phosphors: 2.8 Vitamin D: 32 PTH: 46 (10-65) Urinary calcim: 300 mg/24 hr ( mg/24 hr) Urinary Creatinine: 1gm/24 hr
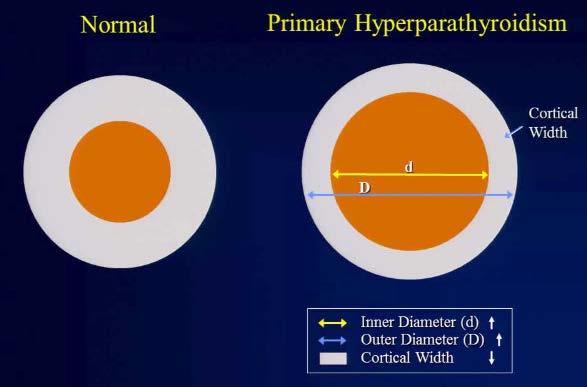
71 Q5 PTH is INAPPROPRIATELY NORMAL in the setting of hypercalcemia Calcim 10.4 (<10.2), PTH 46 (10-65) Occr in 15-20% of all primary hyperparathyroidism cases Main cle: Worst DXA vales at WRIST
72

73 Densitometric Signatre of Primary Hyperparathyroidism Silverberg et al. JBMR, 1989
74 Q5 Workp: History: bones, stones, abdominal moans, and psychological overtones DXA 24 hr rinary calcim with Cr. Sestamibi scan +/- parathyroid Ultrasond CT angiogram of parathyroid 4-D CT with SPECT imaging MRI

75 Withot Parathyroid Srgery 15- Year Natral History

76 Withot Parathyroid Srgery 15- Year Corse of BMD
77 Indications for Srgery in Asymptomatic Primary Hyperparathyroidism Serm Ca > 1.0 mg/dl pper normal BMD < -2.5 at any sites or fractres Urinary calcim excretion (24 hr) > 400 mg/d Age < 50
78 Clinical Pearls Strong correlation between PTH level and calcim concentration, jst becase there is no H or L next to the lab doesn t mean it s normal. Always think abot primary hyperparathyroidism when wrist DXA vale is ot of proportion to the rest of the DXA scan

79 Thank God He Stopped Talking!!!

80
81
82
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
AACE/ACE COMPREHENSIVE TYPE 2 DIABETES MANAGEMENT ALGORITHM. Sherwin D Souza, MD, FACE
 AACE/ACE COMPREHENSIVE TYPE 2 DIABETES MANAGEMENT ALGORITHM Sherwin D Soza, MD, FACE Prediabetes Treatment Algorithm T2DM = type 2 diabetes mellits BP = blood pressre CVD = cardiovasclar disease
AACE/ACE COMPREHENSIVE TYPE 2 DIABETES MANAGEMENT ALGORITHM Sherwin D Soza, MD, FACE Prediabetes Treatment Algorithm T2DM = type 2 diabetes mellits BP = blood pressre CVD = cardiovasclar disease
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
GLP-1 Receptor Agonists and SGLT-2 Inhibitors. Debbie Hicks
 GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
DIABETES: New Insights into Therapeutic Strategies. Lisa Ellard, MSN,CRNP, CDE
 DIABETES: New Insights into Therapetic Strategies Lisa Ellard, MSN,CRNP, CDE NEW, IMPROVED, ME TOO, & NOT ALONE New: Sodim-glcose co-transporter 2 Inhibitors (SGLT 2) Improved: Inslins Delivery, Dration,
DIABETES: New Insights into Therapetic Strategies Lisa Ellard, MSN,CRNP, CDE NEW, IMPROVED, ME TOO, & NOT ALONE New: Sodim-glcose co-transporter 2 Inhibitors (SGLT 2) Improved: Inslins Delivery, Dration,
CURRENT CONTROVERSIES IN DIABETES CARE
 CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
ABFM Diabetes SAM Part 4
 ABFM Diabetes SAM Part 4 37. A 55-year-old male with type 2 diabetes mellitus has a chronic history of reduced libido and erectile dysfunction. On examination you note hepatomegaly and mild testicular
ABFM Diabetes SAM Part 4 37. A 55-year-old male with type 2 diabetes mellitus has a chronic history of reduced libido and erectile dysfunction. On examination you note hepatomegaly and mild testicular
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Application of the Diabetes Algorithm to a Patient
 Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Clinical Cases in Diabetes Management. Joseph Cook D.O.
 Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
Exploring Non-Insulin Therapies in Type 1 Diabetes
 Exploring Non-Insulin Therapies in Type 1 Diabetes Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Disclosures Dr. Cornell: Advanced
Exploring Non-Insulin Therapies in Type 1 Diabetes Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Disclosures Dr. Cornell: Advanced
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
GLMS CME- Cell Group 5 10 April Greenlane Medical Specialists Pui-Ling Chan Endocrinologist
 GLMS CME- Cell Group 5 10 April 2018 Greenlane Medical Specialists Pui-Ling Chan Endocrinologist Pituitary case one Mrs Z; 64F Seen ORL for tinnitus wax impaction MRI Head Pituitary microadenoma (3mm)
GLMS CME- Cell Group 5 10 April 2018 Greenlane Medical Specialists Pui-Ling Chan Endocrinologist Pituitary case one Mrs Z; 64F Seen ORL for tinnitus wax impaction MRI Head Pituitary microadenoma (3mm)
Intensification of Diabetic Therapy. Case studies
 Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Exploring Non-Insulin Therapies in Type 1 Diabetes. Objectives. Pre-Assessment Question #1. Disclosures
 Exploring Non-Insulin Therapies in Type 1 Diabetes Disclosures Dr. Cornell: Advanced Practitioner Advisory Board and Speakers Bureau: Novo Nordisk Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate
Exploring Non-Insulin Therapies in Type 1 Diabetes Disclosures Dr. Cornell: Advanced Practitioner Advisory Board and Speakers Bureau: Novo Nordisk Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
FARXIGA (dapagliflozin) Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)
 Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)") Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Mechanism of hyperprolactinemia
 Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Keep Calm and Focus on the Evidence for the Management of Diabetes. Diabetes Update 2018
 Keep Calm and Focus on the Evidence for the Management of Diabetes Diabetes Update 2018 Nicole C.Pezzino, PharmD, BCACP, CDE Assistant Professor, Wilkes University Pharmacist, Weis Markets Nicole.pezzino@wilkes.edu
Keep Calm and Focus on the Evidence for the Management of Diabetes Diabetes Update 2018 Nicole C.Pezzino, PharmD, BCACP, CDE Assistant Professor, Wilkes University Pharmacist, Weis Markets Nicole.pezzino@wilkes.edu
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
Parathyroid Disease Scenarios for the Practicing Clinician. Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix
 Parathyroid Disease Scenarios for the Practicing Clinician Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix Clinical Scenario-1 73 year man (BK) with hypercalcemia
Parathyroid Disease Scenarios for the Practicing Clinician Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix Clinical Scenario-1 73 year man (BK) with hypercalcemia
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
DIABETES. Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes. November 2013
 DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
Diabetes Mellitus case studies. Jana Vinklerová
 Diabetes Mellitus case studies Jana Vinklerová Definition of diabetes (metabolic disorder) Chronically raised blood glucose (hyperglycaemia) Insulin/Glucagon Insulin is responsible for lowering glucose
Diabetes Mellitus case studies Jana Vinklerová Definition of diabetes (metabolic disorder) Chronically raised blood glucose (hyperglycaemia) Insulin/Glucagon Insulin is responsible for lowering glucose
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Update Diabetes Therapie. Marc Y Donath
 Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA 2012 Virginia Mason Medical
 Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine
 Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine meek.shon@mayo.edu 2016 MFMER 3561772-1 Update on Vitamin D Shon Meek MD, PhD 20 th Annual Endocrine Update January 30-Feb 3, 2017 Disclosure Relevant
Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine meek.shon@mayo.edu 2016 MFMER 3561772-1 Update on Vitamin D Shon Meek MD, PhD 20 th Annual Endocrine Update January 30-Feb 3, 2017 Disclosure Relevant
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs
 Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
8/12/2016. Diabetes Management Across the Spectrum of Kidney Function. Andrew Bzowyckyj. Learning Objectives. Ashley Crowl
 Diabetes Management Across the Spectrum of Kidney Function Andrew Bzowyckyj PharmD, BCPS, CDE Clinical Assistant Professor School of Pharmacy University of Missouri-Kansas City Kansas City, MO Ashley Crowl
Diabetes Management Across the Spectrum of Kidney Function Andrew Bzowyckyj PharmD, BCPS, CDE Clinical Assistant Professor School of Pharmacy University of Missouri-Kansas City Kansas City, MO Ashley Crowl
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
62-year-old woman with severe headache. Celeste Thomas November 1, 2012
 62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
CURRENT ISSUES IN DIABETES MANAGEMENT
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2011 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2011 BMI
Male Sexual Dysfunction: Evaluation,Treatment and the Role of Testosterone. UAPRN Georgia Conference September 24, 2016 Elizabeth H.
 Male Sexal Dysfnction: Evalation,Treatment and the Role of Testosterone UAPRN Georgia Conference September 24, 2016 Elizabeth H. Brgess, MD Learning Objectives I. 3 Types of Male Sexal Dysfnction II. III.
Male Sexal Dysfnction: Evalation,Treatment and the Role of Testosterone UAPRN Georgia Conference September 24, 2016 Elizabeth H. Brgess, MD Learning Objectives I. 3 Types of Male Sexal Dysfnction II. III.
OBESITY IN TYPE 2 DIABETES
 OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology
 Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Sleep and Your Health
 Sleep Chapter 4 Copyright 2015 McGraw-Hill Edcation. All rights reserved. No reprodction or distribtion withot the prior written consent of McGraw-Hill Edcation. 1 Sleep Circadian rhythm: daily 24-hor
Sleep Chapter 4 Copyright 2015 McGraw-Hill Edcation. All rights reserved. No reprodction or distribtion withot the prior written consent of McGraw-Hill Edcation. 1 Sleep Circadian rhythm: daily 24-hor
Diabetes update - Diagnosis and Treatment
 Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
DIABETES UPDATE 2018
 DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
TYP 2 DIABETES. Marc Donath
 TYP 2 DIABETES Marc Donath Treatment of Typ 2 Diabetes GLP-1 Anti-IL-1β Insulin sulfonylureas Metformin UCP-1 IL-1β Sport SGLT2i Bariatric surgery Cardiomyocytes Control Glucose Dyntar et al. Diabetes
TYP 2 DIABETES Marc Donath Treatment of Typ 2 Diabetes GLP-1 Anti-IL-1β Insulin sulfonylureas Metformin UCP-1 IL-1β Sport SGLT2i Bariatric surgery Cardiomyocytes Control Glucose Dyntar et al. Diabetes
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Changing Diabetes: The time is now!
 Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
Update on Diabetes Mellitus
 Update on Diabetes Mellitus Treatment: Targeting the Incretin System Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose control Amylin Incretin Hormones New therapies
Update on Diabetes Mellitus Treatment: Targeting the Incretin System Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose control Amylin Incretin Hormones New therapies
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Preventing Heart Attacks and Strokes Every Day (PHASE) RCHC Medication Titration Algorithm
 RCHC Medication Titration Algorithm") Preventing Heart Attacks and Strokes Every Day (PHASE) RCHC Medication Algorithm Updated 9/13/2017 PHASE Populations DM: type 2 ASCVD: hx heart attack/cad, CVA, TIA, AAA, Sx PAD Lifestyle Modifications
Preventing Heart Attacks and Strokes Every Day (PHASE) RCHC Medication Algorithm Updated 9/13/2017 PHASE Populations DM: type 2 ASCVD: hx heart attack/cad, CVA, TIA, AAA, Sx PAD Lifestyle Modifications
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Metabolic Syndrome. Shon Meek MD, PhD Mayo Clinic Florida Endocrinology
 Metabolic Syndrome Shon Meek MD, PhD Mayo Clinic Florida Endocrinology Disclosure No conflict of interest No financial disclosure Does This Patient Have Metabolic Syndrome? 1. Yes 2. No Does This Patient
Metabolic Syndrome Shon Meek MD, PhD Mayo Clinic Florida Endocrinology Disclosure No conflict of interest No financial disclosure Does This Patient Have Metabolic Syndrome? 1. Yes 2. No Does This Patient
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Disclaimers 22/03/2018. Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2
 Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
RPCC Pharmacy Forum. The Type 2 Diabetes Issue. Type 2 Diabetes: The Basics
 Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Diabetes in Pregnancy
 Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION
 INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
Management: How Can We Do Better? Lori B. Sweeney, MD 2018 Virginia ACP Clinical Update March 17, 2018
 Management: How Can We Do Better? Lori B. Sweeney, MD 2018 Virginia ACP Clinical Update March 17, 2018 Disclosures I have no Objectives Use a case-based format to discuss diabetes management pearls Discuss
Management: How Can We Do Better? Lori B. Sweeney, MD 2018 Virginia ACP Clinical Update March 17, 2018 Disclosures I have no Objectives Use a case-based format to discuss diabetes management pearls Discuss
Pre-diabetes. Pharmacological Approaches to Delay Progression to Diabetes
 Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Clinical Diabetes and Endocrinology in 2017 Pre and Post Test Questions
 1) A 24 year old woman has experienced weakness, light headedness and 6 lb weight loss over the past 6 months. Her past history is unremarkable. Vital Signs: BP 90/65, Pulse 80, T 98.3. PE: skin appears
1) A 24 year old woman has experienced weakness, light headedness and 6 lb weight loss over the past 6 months. Her past history is unremarkable. Vital Signs: BP 90/65, Pulse 80, T 98.3. PE: skin appears
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
CASE A2 Managing Between-meal Hypoglycemia
 Managing Between-meal Hypoglycemia 1 I would like to discuss this case of a patient who, overall, was doing well on her therapy until she made an important lifestyle change to lose weight. This is a common
Managing Between-meal Hypoglycemia 1 I would like to discuss this case of a patient who, overall, was doing well on her therapy until she made an important lifestyle change to lose weight. This is a common
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes. Overview. Prevalence of Overweight in the U.S.
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Diabetes Mellitus in Older Adults. Presenter Disclosure Information
 Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from