Chapter-V Drug use in renal and hepatic disorders. BY Prof. C.Ramasamy, Head, Dept of Pharmacy Practice SRM College of Pharmacy, SRM University
|
|
|
- Audrey Norman
- 6 years ago
- Views:
Transcription
1 Chapter-V Drug use in renal and hepatic disorders. BY Prof. C.Ramasamy, Head, Dept of Pharmacy Practice SRM College of Pharmacy, SRM University
2 Estimating renal function An accurate estimation of renal function, or glomerular filtration rate (GFR), requires sophisticated techniques that are unsuitable for routine or repeated use. In practice, the serum creatinine concentration is used for day-to-day assessment of renal function. It has limitations, but it remains a robust and practical parameter for most clinical situations
3 Serum creatinine The serum creatinine concentration has important limitations when used for estimating renal function. 1. There is an inverse relationship between serum creatinine and renal function. A doubling of serum creatinine represents a halving of GFR. A person's serum creatinine can rise from 60 to 120 micromol/l and so still be in the normal range (typically 50 to 120 micromol/l), yet the renal function has deteriorated dramatically. 2. Renal function declines steadily with age in adults, but this is not reflected in the serum creatinine, which remains steady or may only increase slightly with age (in the absence of overt renal disease, where it may rise more obviously). An 80-year-old will have approximately half of the renal function of a 20-year-old, despite both having the same serum creatinine concentration.
4 Serum creatinine 3. Renal function has an approximately linear relationship with lean body mass. In the presence of the same serum creatinine, a 120 kg person will have twice the renal function of a 60 kg person because they have bigger kidneys. 4. Women have a lower muscle mass than men of equivalent weight and age. A woman's serum creatinine represents approximately 0.85 of the renal function of a man with the same serum creatinine. These limitations are particularly relevant and must be addressed when attempting to measure renal function for the purpose of calculating drug doses.
5 Creatinine clearance The serum creatinine concentration represents a balance between its production in the body (from muscle) and its excretion by the kidneys. From this can be derived an estimation of the creatinine clearance by the kidneys, in millilitres per minute (ml/min) or millilitres per second (ml/sec). This is the notional volume of serum that is cleared of creatinine in those times. The creatinine clearance is the 'poor man's' equivalent of the formal measurements of GFR,but for most clinical purposes is an adequate measurement of renal function.
6 Creatinine clearance Manufacturers renal dosing recommendations for medications are based on Cockcroft-Gault estimates of renal function, so this formula is also recommended when estimating creatinine clearance for the purpose of calculating drug doses that vary according to renal function. Some important limitations of the Cockcroft-Gault estimation of renal function. It is: 1. not validated in some populations 2. unreliable in extremes of body size (that is, in severe malnutrition or obesity) 3. imprecise and unreliable for rapidly changing renal function (for example intensive care, acute renal failure).
7 Changes in drug response in renal failure: 1. Brain more sensitive to depressant action of drugsblood brain barrier is less effective 2. Control of body fluid volume affected. If patient hypovolemic due to diuretics, body becomes very sensitive to action of antihypertensives 3. Impairment of coagulation more sensitive to anticoagulants---gi bleed 4. Drugs causing Na + retention---nsaids fluid overload--- CHF 5. Renal failure hyperkalemia---acei, ARBs. 6. Renal failure---acidosis altered response to drugs, especially weak acids 7. Cholinesterase activity more sensitive to AChase drugs e.g. neostigmine
8 General principles of prescribing in renal failure: GOOD KNOWLEDGE OF PHARMACOKINETICS OF THE DRUGS USED IS NECESSARY! Use drugs only if a definite indication is present Choose a drug with no/minimal nephrotoxicity Use recommended regimen given. If no data, use your COMMONSENSE! Use TDM to adjust doses Avoid prolonged courses of potentially toxic drugs Monitor patient for clinical effectiveness & toxicity
9 Modification of dosage regimen: Look at the drug s renal & non renal elimination (%) How toxic the drug is Two approaches: Standard dose -----Extended intervals Reduced dose----usual intervals. LOADING DOSE REMAINS THE SAME! For many drugs, an unchanged loading dose followed by half the usual adult maintenance dose is all that is done! For more toxic drugs use dosage regimen based on GFR. Subsequent dosage based on: Clinical response Signs of toxicity Plasma concentration.
10 Modification of dosage regimen: If antibiotic given in usual doses but at extended intervals-- --there may be considerable periods of sub-inhibitory Concentrations. More frequent doses---toxicity! Measure plasma concentrations frequently. Risk versus benefit
11 Use of tables--- given as appendices in major text books. Following data is given: 1. Elimination t 1/2 ---both normal & in renal failure 2. Unchanged excretion (%) 3. Normal extra renal excretion 4. Normal dose interval (hours) 5. Dose adjustment for renal failure based on Creatinine clearance (ml/min): >50, 10-50, <10.
12 Limitations of tables: 1. Status of renal function should be determined not only before, but also the entire period of treatment 2. These dosage guidelines do not necessarily apply to elderly patients. 3. Many aspects of individual patients influence drug response in uremia 4. Monitor plasma concentration, especially for drugs with a low therapeutic index. 5. Monitor patients for unexpected drug toxicity.
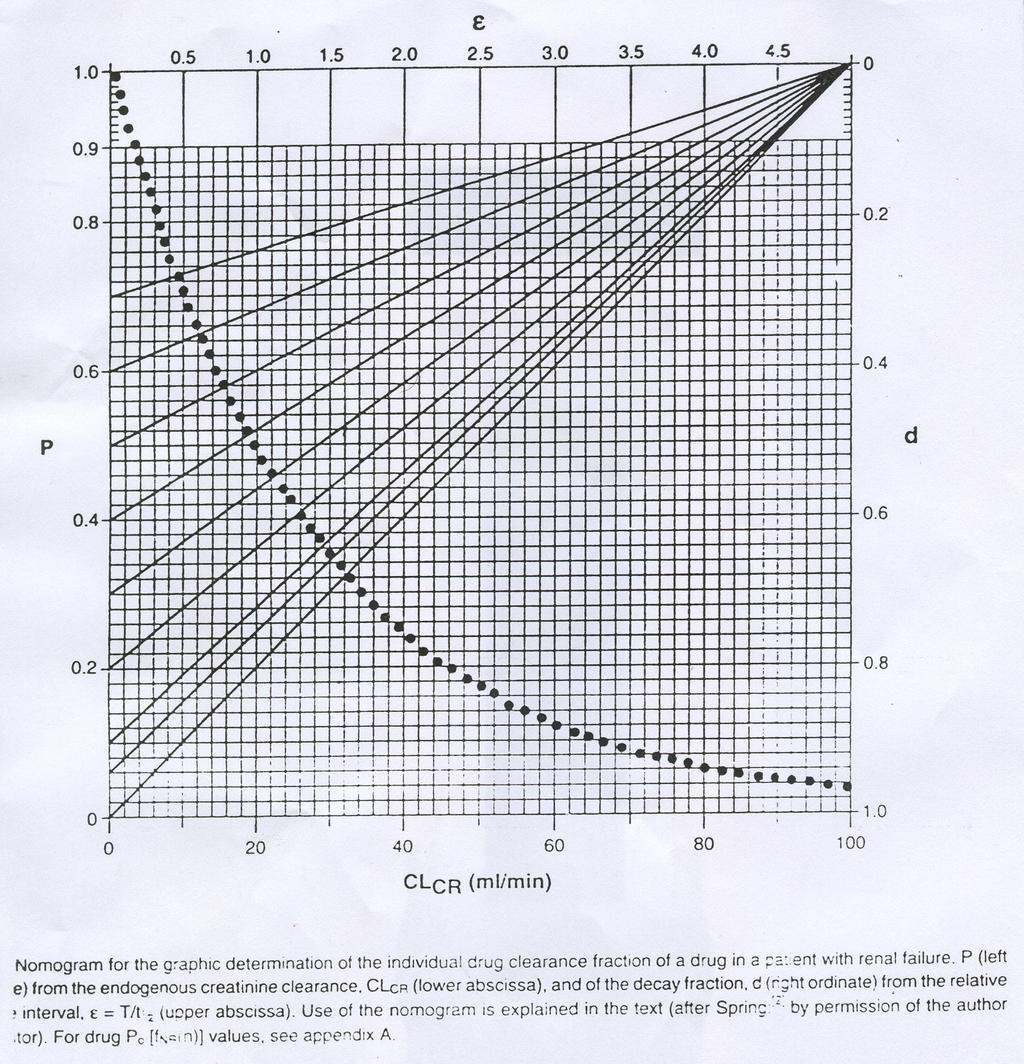
13 Nomogram method: Based on: Linear relationship between total plasma drug clearance and GFR as determined by creatinine clearance. Normal renal function is defined by creatinine clearance = 100 ml/min =6 l/hr.
14
15 Graphic estimation: Individual drug clearance fraction (P), which describes the total clearance of the drug in the patient with renal function as a fraction of its normal clearance is determined in the following way by means of the nomogram: Value of normal non- renal drug clearance fraction f NR(n) (P o ), obtained from appendix in a text book, is plotted on the left ordinate of the nomogram & connected with its right upper corner by a straight line. The point of intersection between the patient s endogenous creatinine clearance Cl CR (lower abscissa) & the estimating line indicates the left ordinate the individual clearance fraction (P) in the patient.
16 The ( t 1/2 ) is calculated from normal t 1/2 as: t 1/2 = t 1/2 / P Dosage rules: Rule 1 : Rule 2 : D * = D* D * = D* D = D.P D = D T = T T = T/P Where D* = Loading dose D is maintenance dose & T = t 1/2. LOADING DOSE IS SAME IN BOTH RULES.
17 Rule1 : Decrease the maintenance dose, dosing Interval unchanged Rule 2 : Normal maintenance dose, dosing interval unchanged.
18 Cockcroft & Gault equation: CL CR (ml/min) = (140-age) x Bodyweight (Kg) 72 X C CR mg/dl. In females multiply the result by 0.85
19 Example:- Administration of cimetidine in a 60 yr old female patient with a bleeding gastric ulcer. Body weight = 70 kg., plasma creatinine C CR = 2 mg/dl Cl CR = (140 60) x 70 x X 7 Cl CR = 33 ml/min Non-renal clearance fraction of cimetidine = 0.25 (P o ). The value P o = 0.25 is plotted on the left ordinate, connected with the upper corner of the monogram by a straight line. The point of intersection between CL = CR 33 ( lower abscissa ) with this estimating line results in the individual drug clearance fraction P = 0.5 at the left ordinate.
20 Assume D* = 200mg D = 200mg & T = 4 as the normal dosage regimen of cimetidine. Rule 1 Rule 2 D * = D * = 200mg D * = D * = 200mg D = D.P = 200 x 0.5 D = D = 200mg = 100mg T = T/P = 4/0.5 T = T = 4 hours T = 8 hours So,give 100 mg cimetidine every 4 hourly or 200 mg every eight hourly
21 Limitations of nomogram: 1. Serum Creatinine should never be used as an estimating parameter in patients with acute renal failure or changing kidney function. 2. Does not obviate need for therapeutic drug monitoring (TDM). 3. Carefully observe patients for unexpected drug toxicity.
22 During usage in hepatic diseases Drug distribution: plasma albumin & bilirubin Decreased plasma protein binding Drug Elimination:- Depends on type & stage of liver disease. There is portal venous perfusion to a liver of cell mass. Intrahepatic shunts with in the liver
23 Drug Elimination: Abnormal sinusoidal membrane loss of fenestration & permeability Extra hepatic shunts. Of all Liver function tests serum albumin concentration & vitamin K corrected prothrombin time provide the best estimates of hepatic metabolic capacity. Decreased intrinsic clearance of many drugs. Drugs with high hepatic clearance show bioavailability Propranolol, pethidine, pentazocine, labetalol, clomethiazole.
24 Drug Elimination: Decreased hepatic metabolism Decreased hepatic clearance of many drugs. Glucuronidation is relatively preserved in patients with liver disease. No single test/ Model/ Marker compound as predictors of hepatic functional reserve! Adjusting dosage is more difficult than in renal disease.
25 Use of tables:- As appendix in Text books. 5 major Pharmacokinetic variables: 1. Clearance 2. Volume of distribution (V D ) 3. Elimination t ½ 4. % unbound drug 5. Bio availability
26 Rate of drug admin = Cl x C SS Cl = clearance Css = concentration at steady state ( ~ 5 t ½ ) Eg:- Css of theophylline is 10mg / L & Cl =3L / h. Dosage rate = 10mg x 3 L = 30mg/h or 180 mg every 6 hourly.
27 V D : of water soluble drugs with small V D will have significant in their V D in patients. With ascites. eg:- aminoglyicosides Altered Pharmacokinetics: Impaired intrinsic hepatic eliminating capacity due to lack of or impaired function of hepatocytes Impaired biliary elimination due to biliary obstruction or transpost abnormalities. Impaired hepatic blood flow due to surgical shunting, collateral circulation or poor hepatic perfusion with cirrhosis & portal hypertension
28 Altered V D due to differences in body composition with ECF ( ascites, edema) & muscle mass. plasma protein binding due to impaired albumin production or drug displacement from accumulated substance normally cleared by the liver Bio avail through first pass metabolism Bioavailability due to malabsorption of fats in cholestatic liver disease.
29 Limitation of tables: Data is generated in small number of patients mostly with alcoholic cirrhosis. Other diseases not well studied. For same degree of liver impairment some patients show impaired ability to clear the drug & other have clearance comparable to healthy controls..
30 Ability to metabolize one drug may not be predictive of their ability to metabolize another agent. One enzyme system may be significantly impaired another may remain intact. Pharmacodynamics: Best eg: is cerebral sensitivity of analgesics antianxiety & hypnosedative drugs in patients with liver disease especially hepatic encephalopathy. Avoidance of these agents is strongly advised
Effects of Liver Disease on Pharmacokinetics
 Effects of Liver Disease on Pharmacokinetics Juan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program October 31, 2013 National Institutes of Health Clinical Center 1 GOALS of Effects of Liver
Effects of Liver Disease on Pharmacokinetics Juan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program October 31, 2013 National Institutes of Health Clinical Center 1 GOALS of Effects of Liver
Effects of Liver Disease on Pharmacokinetics Juan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program November 4, 2010 National
 Effects of Liver Disease on Pharmacokinetics Juan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program November 4, 2010 National Institutes of Health Clinical Center GOALS of Liver Disease
Effects of Liver Disease on Pharmacokinetics Juan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program November 4, 2010 National Institutes of Health Clinical Center GOALS of Liver Disease
Effects of Liver Disease on Pharmacokinetics Juan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program October 29, 2015 National
 Effects of Liver Disease on Pharmacokinetics Juan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program October 29, 2015 National Institutes of Health Clinical Center GOALS of Liver Disease
Effects of Liver Disease on Pharmacokinetics Juan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program October 29, 2015 National Institutes of Health Clinical Center GOALS of Liver Disease
TDM. Generally, hepatic clearance is determined by three main factors: These three factors can be employed in the following equation:
 Lecture 9: Very important supplements TDM Effect of hepatic disease on drugs monitoring: Generally, hepatic clearance is determined by three main factors: - Liver blood flow (LBF). - Intrinsic capacity
Lecture 9: Very important supplements TDM Effect of hepatic disease on drugs monitoring: Generally, hepatic clearance is determined by three main factors: - Liver blood flow (LBF). - Intrinsic capacity
PHA5128 Dose Optimization II Case Study I Spring 2013
 Silsamicin is an investigational compound being evaluated for its antimicrobial effect. The route of administration for this drug is via intravenous bolus. Approximately 99.9% of this drug is eliminated
Silsamicin is an investigational compound being evaluated for its antimicrobial effect. The route of administration for this drug is via intravenous bolus. Approximately 99.9% of this drug is eliminated
Drug Dosing in Renal Insufficiency. Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila
 Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
Basic Concepts of TDM
 TDM Lecture 1 5 th stage What is TDM? Basic Concepts of TDM Therapeutic drug monitoring (TDM) is a branch of clinical pharmacology that specializes in the measurement of medication concentrations in blood.
TDM Lecture 1 5 th stage What is TDM? Basic Concepts of TDM Therapeutic drug monitoring (TDM) is a branch of clinical pharmacology that specializes in the measurement of medication concentrations in blood.
TDM. Measurement techniques used to determine cyclosporine level include:
 TDM Lecture 15: Cyclosporine. Cyclosporine is a cyclic polypeptide medication with immunosuppressant effect. It has the ability to block the production of interleukin-2 and other cytokines by T-lymphocytes.
TDM Lecture 15: Cyclosporine. Cyclosporine is a cyclic polypeptide medication with immunosuppressant effect. It has the ability to block the production of interleukin-2 and other cytokines by T-lymphocytes.
TDM of Aminoglycoside Antibiotics
 TDM Lecture 3 5 th Stage TDM of Aminoglycoside Antibiotics The aminoglycoside antibiotics are widely used for the treatment of gram-negative infections, often in combination with a β-lactam antibiotic
TDM Lecture 3 5 th Stage TDM of Aminoglycoside Antibiotics The aminoglycoside antibiotics are widely used for the treatment of gram-negative infections, often in combination with a β-lactam antibiotic
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
PRESCRIBING IN LIVER AND RENAL DISEASE
 THERAPEUTICS FOR INDEPENDENT PRESCRIBERS PRESCRIBING IN LIVER AND RENAL DISEASE Number 6 in a series of 15 articles on Therapeutics Aims and Objectives To outline the pathophysiological changes that occur
THERAPEUTICS FOR INDEPENDENT PRESCRIBERS PRESCRIBING IN LIVER AND RENAL DISEASE Number 6 in a series of 15 articles on Therapeutics Aims and Objectives To outline the pathophysiological changes that occur
Name: UFID: PHA Exam 2. Spring 2013
 PHA 5128 Exam 2 Spring 2013 1 Carbamazepine (5 points) 2 Theophylline (10 points) 3 Gentamicin (10 points) 4 Drug-drug interaction (5 points) 5 Lidocaine (5 points) 6 Cyclosporine (5 points) 7 Phenobarbital
PHA 5128 Exam 2 Spring 2013 1 Carbamazepine (5 points) 2 Theophylline (10 points) 3 Gentamicin (10 points) 4 Drug-drug interaction (5 points) 5 Lidocaine (5 points) 6 Cyclosporine (5 points) 7 Phenobarbital
Selected Clinical Calculations Chapter 10. Heparin-Dosing calculations
 Selected Clinical Calculations Chapter 10 Heparin-Dosing calculations Heparin is a heterogeneous group of muco-polysaccharides that have anticoagulant properties (slows clotting time). Heparin salt, as
Selected Clinical Calculations Chapter 10 Heparin-Dosing calculations Heparin is a heterogeneous group of muco-polysaccharides that have anticoagulant properties (slows clotting time). Heparin salt, as
TDM Lecture 7 5 th Stage. TDM of Digoxin. Uses: Digoxin is usually used in heart failure associated and atrial fibrillation.
 TDM Lecture 7 5 th Stage TDM of Digoxin Digoxin uses and elimination Uses: Digoxin is usually used in heart failure associated and atrial fibrillation. Elimination: About 75% of digoxin clearance occurred
TDM Lecture 7 5 th Stage TDM of Digoxin Digoxin uses and elimination Uses: Digoxin is usually used in heart failure associated and atrial fibrillation. Elimination: About 75% of digoxin clearance occurred
Basic Pharmacokinetic Principles Stephen P. Roush, Pharm.D. Clinical Coordinator, Department of Pharmacy
 Basic Pharmacokinetic Principles Stephen P. Roush, Pharm.D. Clinical Coordinator, Department of Pharmacy I. General principles Applied pharmacokinetics - the process of using drug concentrations, pharmaco-kinetic
Basic Pharmacokinetic Principles Stephen P. Roush, Pharm.D. Clinical Coordinator, Department of Pharmacy I. General principles Applied pharmacokinetics - the process of using drug concentrations, pharmaco-kinetic
Dr.Nahid Osman Ahmed 1
 1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
PHA Second Exam Fall On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 Second Exam Fall 2013 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Question/Points Set I 20 pts Set II 20 pts Set III 20 pts Set IV 20 pts Set
PHA 5127 Second Exam Fall 2013 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Question/Points Set I 20 pts Set II 20 pts Set III 20 pts Set IV 20 pts Set
LD = (Vd x Cp)/F (Vd x Cp)/F MD = (Css x CL x T)/F DR = (Css x (Vm-DR))/Km Css = (F x D)/(CL x T) (Km x DR)/(Vm DR)
/F (Vd x Cp)/F MD = (Css x CL x T)/F DR = (Css x (Vm-DR))/Km Css = (F x D)/(CL x T) (Km x DR)/(Vm DR)") PHARMKIN WORKSHOP A PHARMACOKINETICS TEACHING SIMULATION Joseph K. Ritter, Ph.D. Associate Professor, Pharmacology and Toxicology MSB 536, 828-1022, jritter@mail2.vcu.edu Tompkins-McCaw Libray Room 2-006
PHARMKIN WORKSHOP A PHARMACOKINETICS TEACHING SIMULATION Joseph K. Ritter, Ph.D. Associate Professor, Pharmacology and Toxicology MSB 536, 828-1022, jritter@mail2.vcu.edu Tompkins-McCaw Libray Room 2-006
Renal Function and Associated Laboratory Tests
 Renal Function and Associated Laboratory Tests Contents Glomerular Filtration Rate (GFR)... 2 Cockroft-Gault Calculation of Creatinine Clearance... 3 Blood Urea Nitrogen (BUN) to Serum Creatinine (SCr)
Renal Function and Associated Laboratory Tests Contents Glomerular Filtration Rate (GFR)... 2 Cockroft-Gault Calculation of Creatinine Clearance... 3 Blood Urea Nitrogen (BUN) to Serum Creatinine (SCr)
PHA Spring First Exam. 8 Aminoglycosides (5 points)
") PHA 5128 Spring 2012 First Exam 1 Aminoglycosides (5 points) 2 Aminoglycosides (10 points) 3 Basic Principles (5 points) 4 Basic Principles (5 points) 5 Bioavailability (5 points) 6 Vancomycin (5 points)
PHA 5128 Spring 2012 First Exam 1 Aminoglycosides (5 points) 2 Aminoglycosides (10 points) 3 Basic Principles (5 points) 4 Basic Principles (5 points) 5 Bioavailability (5 points) 6 Vancomycin (5 points)
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
Adjusting phenytoin dosage in complex patients: how to win friends and influence patient outcomes
 Adjusting phenytoin dosage in complex patients: how to win friends and influence patient outcomes Brian Hardy, PharmD, FCSHP, FCCP Coordinator Education and Clinical Programs Department of Pharmacy Sunnybrook
Adjusting phenytoin dosage in complex patients: how to win friends and influence patient outcomes Brian Hardy, PharmD, FCSHP, FCCP Coordinator Education and Clinical Programs Department of Pharmacy Sunnybrook
TDM of Digoxin. Use of Digoxin Serum Concentrations to Alter Dosages
 TDM Lecture 8 5 th Stage TDM of Digoxin Use of Digoxin Serum Concentrations to Alter Dosages Linear Pharmacokinetics Method This method is used in steady-state condition. We compute the new dose of digoxin
TDM Lecture 8 5 th Stage TDM of Digoxin Use of Digoxin Serum Concentrations to Alter Dosages Linear Pharmacokinetics Method This method is used in steady-state condition. We compute the new dose of digoxin
CLINICAL PHARMACOKINETICS INDEPENDENT LEARNING MODULE
 CLINICAL PHARMACOKINETICS INDEPENDENT LEARNING MODULE Joseph K. Ritter, Ph.D. Assoc. Professor, Pharmacology and Toxicology MSB 536, 828-1022, jritter@vcu.edu This self study module will reinforce the
CLINICAL PHARMACOKINETICS INDEPENDENT LEARNING MODULE Joseph K. Ritter, Ph.D. Assoc. Professor, Pharmacology and Toxicology MSB 536, 828-1022, jritter@vcu.edu This self study module will reinforce the
BIOPHARMACEUTICS and CLINICAL PHARMACY
 11 years papers covered BIOPHARMACEUTICS and CLINICAL PHARMACY IV B.Pharm II Semester, Andhra University Topics: Absorption Distribution Protein binding Metabolism Excretion Bioavailability Drug Interactions
11 years papers covered BIOPHARMACEUTICS and CLINICAL PHARMACY IV B.Pharm II Semester, Andhra University Topics: Absorption Distribution Protein binding Metabolism Excretion Bioavailability Drug Interactions
PHA Second Exam. Fall On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 Second Exam Fall 2010 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /200 pts 1 Question Set I (True or
PHA 5127 Second Exam Fall 2010 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /200 pts 1 Question Set I (True or
Drug dosing in Extremes of Weight
 Drug dosing in Extremes of Weight The Plump & Heavy versus The Skinny & Light Maria Minerva P. Calimag, MD, MSc, PhD, DPBA, FPSECP PROFESSOR Departments of Pharmacology, Anesthesiology and Clinical Epidemiology
Drug dosing in Extremes of Weight The Plump & Heavy versus The Skinny & Light Maria Minerva P. Calimag, MD, MSc, PhD, DPBA, FPSECP PROFESSOR Departments of Pharmacology, Anesthesiology and Clinical Epidemiology
Effects of Renal Disease on Pharmacokinetics
 Effects of Renal Disease on Pharmacokinetics Juan J. L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program October 14, 2010 Office of Clinical Research Training and Medical Education National
Effects of Renal Disease on Pharmacokinetics Juan J. L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program October 14, 2010 Office of Clinical Research Training and Medical Education National
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
Acknowledgements. National Kidney Foundation of Connecticut Mark Perazella. Co-PI Slowing the progression of chronic kidney disease to ESRD
 A Practical Approach to Chronic Kidney Disease Management for the Primary Care Practioner: A web-site sponsored by the National Kidney Foundation of Connecticut Robert Reilly, M.D. Acknowledgements National
A Practical Approach to Chronic Kidney Disease Management for the Primary Care Practioner: A web-site sponsored by the National Kidney Foundation of Connecticut Robert Reilly, M.D. Acknowledgements National
Appendix 5: Hepatic impairment
 Appendix 5: Hepatic impairment Liver disease may alter the response to drugs. However, the hepatic reserve appears to be large and liver disease has to be severe before important changes in drug metabolism
Appendix 5: Hepatic impairment Liver disease may alter the response to drugs. However, the hepatic reserve appears to be large and liver disease has to be severe before important changes in drug metabolism
Filtration and Reabsorption Amount Filter/d
 Renal Physiology 2011 Lisa M. Harrison-Bernard, PhD Contact me at lharris@lsuhsc.edu Renal Physiology Lecture 3 Renal Clearance and Glomerular Filtration Filtration and Reabsorption Amount Filter/d Amount
Renal Physiology 2011 Lisa M. Harrison-Bernard, PhD Contact me at lharris@lsuhsc.edu Renal Physiology Lecture 3 Renal Clearance and Glomerular Filtration Filtration and Reabsorption Amount Filter/d Amount
INTRAVENOUS VANCOMYCIN PRESCRIBING AND MONITORING GUIDELINE FOR ADULT PATIENTS
 Title of guideline (must include the word Guideline (not protocol, policy, procedure etc) INTRAVENOUS VANCOMYCIN PRESCRIBING AND MONITORING GUIDELINE FOR ADULT PATIENTS Author: Contact Name and Job Title
Title of guideline (must include the word Guideline (not protocol, policy, procedure etc) INTRAVENOUS VANCOMYCIN PRESCRIBING AND MONITORING GUIDELINE FOR ADULT PATIENTS Author: Contact Name and Job Title
PHARMACOKINETICS SMALL GROUP II:
 PHARMACOKINETICS SMALL GROUP II: Question 1 Why are some drug therapies initiated with a loading dose? Emphasize that LD establishes initial therapeutic level quickly. The time to reach the steady-state
PHARMACOKINETICS SMALL GROUP II: Question 1 Why are some drug therapies initiated with a loading dose? Emphasize that LD establishes initial therapeutic level quickly. The time to reach the steady-state
BASIC PHARMACOKINETICS
 BASIC PHARMACOKINETICS MOHSEN A. HEDAYA CRC Press Taylor & Francis Croup Boca Raton London New York CRC Press is an imprint of the Taylor & Francis Group, an informa business Table of Contents Chapter
BASIC PHARMACOKINETICS MOHSEN A. HEDAYA CRC Press Taylor & Francis Croup Boca Raton London New York CRC Press is an imprint of the Taylor & Francis Group, an informa business Table of Contents Chapter
Principles of Medication Use in Older Adults ANNE L. HUME, PHARMD PROFESSOR OF PHARMACY UNIVERSITY OF RHODE ISLAND
 Principles of Medication Use in Older Adults ANNE L. HUME, PHARMD PROFESSOR OF PHARMACY UNIVERSITY OF RHODE ISLAND Financial Disclosure None of the planners, speakers, and/or members of the CME committee
Principles of Medication Use in Older Adults ANNE L. HUME, PHARMD PROFESSOR OF PHARMACY UNIVERSITY OF RHODE ISLAND Financial Disclosure None of the planners, speakers, and/or members of the CME committee
General Principles of Pharmacology and Toxicology
 General Principles of Pharmacology and Toxicology Parisa Gazerani, Pharm D, PhD Assistant Professor Center for Sensory-Motor Interaction (SMI) Department of Health Science and Technology Aalborg University
General Principles of Pharmacology and Toxicology Parisa Gazerani, Pharm D, PhD Assistant Professor Center for Sensory-Motor Interaction (SMI) Department of Health Science and Technology Aalborg University
Pharmacology in the Elderly
 Pharmacology in the Elderly James Hardy Geriatrician, Royal North Shore Hospital A recent consultation Aspirin Clopidogrel Warfarin Coloxyl with senna Clearlax Methotrexate Paracetamol Pantoprazole Cholecalciferol
Pharmacology in the Elderly James Hardy Geriatrician, Royal North Shore Hospital A recent consultation Aspirin Clopidogrel Warfarin Coloxyl with senna Clearlax Methotrexate Paracetamol Pantoprazole Cholecalciferol
Full title of guideline INTRAVENOUS VANCOMYCIN PRESCRIBING AND MONITORING GUIDELINE FOR ADULT PATIENTS. control
 Full title of guideline Author: Contact Name and Job Title Division and specialty Scope Explicit definition of patient group to which it applies (e.g. inclusion and exclusion criteria, diagnosis) Changes
Full title of guideline Author: Contact Name and Job Title Division and specialty Scope Explicit definition of patient group to which it applies (e.g. inclusion and exclusion criteria, diagnosis) Changes
Effects of Liver Disease on Pharmacokinetics
 Effects of Liver Disease on Pharmacokinetics Jan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program October 29, 2015 National Instittes of ealth Clinical Center GOALS of Effects of Liver
Effects of Liver Disease on Pharmacokinetics Jan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program October 29, 2015 National Instittes of ealth Clinical Center GOALS of Effects of Liver
WEEK. MPharm Programme. Acute Kidney Injury. Alan M. Green MPHM13: Acute Kidney Injury. Slide 1 of 47
 MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
Cystatin C: A New Approach to Improve Medication Dosing
 Cystatin C: A New Approach to Improve Medication Dosing Erin Frazee Barreto, PharmD, MSc, FCCM Assistant Professor of Pharmacy and Medicine Kern Scholar, Center for the Science of Health Care Delivery
Cystatin C: A New Approach to Improve Medication Dosing Erin Frazee Barreto, PharmD, MSc, FCCM Assistant Professor of Pharmacy and Medicine Kern Scholar, Center for the Science of Health Care Delivery
PHA Second Exam. Fall On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 Second Exam Fall 2012 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /150 pts 1 Question Set I (True or
PHA 5127 Second Exam Fall 2012 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /150 pts 1 Question Set I (True or
Use ideal body weight (IBW) unless actual body weight is less. Use the following equation to calculate IBW:
 unless actual body weight is less. Use the following equation to calculate IBW:") Amikacin is a partially restricted (amber) antibiotic for the treatment of infections due to gentamicin resistant Gram negative bacilli or as advised by microbiology. As with other aminoglycosides, therapeutic
Amikacin is a partially restricted (amber) antibiotic for the treatment of infections due to gentamicin resistant Gram negative bacilli or as advised by microbiology. As with other aminoglycosides, therapeutic
PHARMACOKINETICS SMALL GROUP I:
 PHARMACOKINETICS SMALL GROUP I: Question 1 Absorption of the anti-fungal agent, itraconazole, is dependent on a low gastric ph. Calculate the relative concentrations of a weak acid (with a pka of 5.4)
PHARMACOKINETICS SMALL GROUP I: Question 1 Absorption of the anti-fungal agent, itraconazole, is dependent on a low gastric ph. Calculate the relative concentrations of a weak acid (with a pka of 5.4)
WEEK. MPharm Programme. Liver Biochemistry. Slide 1 of 49 MPHM14 Liver Biochemistry
 MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
Ibuprofen. Ibuprofen and Paracetamol: prescribing overview. Ibuprofen indications CYCLO-OXYGENASE (COX I) CYCLO-OXEGENASE (COX II) INFLAMMATORY PAIN
 CYCLO-OXEGENASE (COX II) INFLAMMATORY PAIN") Ibuprofen Ibuprofen and Paracetamol: prescribing overview Sarah Holloway Macmillan CNS in palliative care NSAID Non-selective COX inhibitor Oral bioavailability: 90% Onset of action: 20-30 mins (can take
Ibuprofen Ibuprofen and Paracetamol: prescribing overview Sarah Holloway Macmillan CNS in palliative care NSAID Non-selective COX inhibitor Oral bioavailability: 90% Onset of action: 20-30 mins (can take
PHA Second Exam. Fall On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 Second Exam Fall 2011 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /200 pts 1 Question Set I (True or
PHA 5127 Second Exam Fall 2011 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /200 pts 1 Question Set I (True or
Renal Excretion of Drugs
 Renal Excretion of Drugs 3 1 Objectives : 1 Identify main and minor routes of Excretion including renal elimination and biliary excretion 2 Describe its consequences on duration of drugs. For better understanding:
Renal Excretion of Drugs 3 1 Objectives : 1 Identify main and minor routes of Excretion including renal elimination and biliary excretion 2 Describe its consequences on duration of drugs. For better understanding:
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE. Jules B. Puschett, M.D.
 DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
1. If the MTC is 100 ng/ml and the MEC is 0.12 ng/ml, which of the following dosing regimen(s) are in the therapeutic window?
 are in the therapeutic window?") Page 1 PHAR 750: Biopharmaceutics/Pharmacokinetics October 23, 2009 - Form 1 Name: Total 100 points Please choose the BEST answer of those provided. For numerical answers, choose none of the above if your
Page 1 PHAR 750: Biopharmaceutics/Pharmacokinetics October 23, 2009 - Form 1 Name: Total 100 points Please choose the BEST answer of those provided. For numerical answers, choose none of the above if your
General Principles of Pharmacology and Toxicology
 General Principles of Pharmacology and Toxicology Parisa Gazerani, Pharm D, PhD Assistant Professor Center for Sensory-Motor Interaction (SMI) Department of Health Science and Technology Aalborg University
General Principles of Pharmacology and Toxicology Parisa Gazerani, Pharm D, PhD Assistant Professor Center for Sensory-Motor Interaction (SMI) Department of Health Science and Technology Aalborg University
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
PHA First Exam Fall 2003
 PHA 5127 First Exam Fall 2003 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Question/Points 1. /14 pts 2. /6 pts 3. /15 pts 4. /12 pts 5. /20 pts 6. /10pts
PHA 5127 First Exam Fall 2003 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Question/Points 1. /14 pts 2. /6 pts 3. /15 pts 4. /12 pts 5. /20 pts 6. /10pts
PHA 5128 Spring 2009 First Exam (Version B)
") Name: UFID: PHA 5128 Spring 2009 First Exam (Version B) On my honor, I have neither given nor received unauthorized aid in doing this assignment. Print: Sign: Version B Q1: Phenytoin (10) Q2: procainamide
Name: UFID: PHA 5128 Spring 2009 First Exam (Version B) On my honor, I have neither given nor received unauthorized aid in doing this assignment. Print: Sign: Version B Q1: Phenytoin (10) Q2: procainamide
Renal Function. 1. Glomerular filtration 2. Active tubular secretion 3. Passive tubular reabsorption 4. Excretion
 59-291 Section 1, Lecture 5 Drug Excretion -most drugs are excreted in urine either as unchanged or drug metabolites Renal Function 1. Glomerular filtration 2. Active tubular secretion 3. Passive tubular
59-291 Section 1, Lecture 5 Drug Excretion -most drugs are excreted in urine either as unchanged or drug metabolites Renal Function 1. Glomerular filtration 2. Active tubular secretion 3. Passive tubular
PHA 5128 Final Exam Spring 2004 Version A. On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5128 Final Exam Spring 2004 Version A On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name There are 18 questions. Total /120 pts Final 2004 1 1. T.P., a 66-year-old,
PHA 5128 Final Exam Spring 2004 Version A On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name There are 18 questions. Total /120 pts Final 2004 1 1. T.P., a 66-year-old,
Evaluation of the Cockroft Gault, Jelliffe and Wright formulae in estimating renal function in elderly cancer patients
 Original article Annals of Oncology 15: 291 295, 2004 DOI: 10.1093/annonc/mdh079 Evaluation of the Cockroft Gault, Jelliffe and Wright formulae in estimating renal function in elderly cancer patients G.
Original article Annals of Oncology 15: 291 295, 2004 DOI: 10.1093/annonc/mdh079 Evaluation of the Cockroft Gault, Jelliffe and Wright formulae in estimating renal function in elderly cancer patients G.
Dosing Information. The First & Only FDA-approved Spironolactone Oral Suspension P HARM A. Exclusively from
 Dosing Information The First & Only FDA-approved Spironolactone Oral Suspension Exclusively from P HARM A The Formulation That s Easy To Prescribe CAROSPIR is an antagonist of aldosterone indicated for:
Dosing Information The First & Only FDA-approved Spironolactone Oral Suspension Exclusively from P HARM A The Formulation That s Easy To Prescribe CAROSPIR is an antagonist of aldosterone indicated for:
Effects of Renal Disease on Pharmacokinetics October 8, 2015 Juan J. L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program
 Effects of Renal Disease on Pharmacokinetics October 8, 2015 Juan J. L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program `Office of Clinical Research Training and Medical Education National
Effects of Renal Disease on Pharmacokinetics October 8, 2015 Juan J. L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program `Office of Clinical Research Training and Medical Education National
CHAPTER 2. GERIATRICS, SELF-ASSESSMENT QUESTIONS
 CHAPTER 2. GERIATRICS, SELF-ASSESSMENT QUESTIONS 1. The following is an accurate description of the aging population: A. The number of older adults will reach 17 million in 2030 B. The ratio of women to
CHAPTER 2. GERIATRICS, SELF-ASSESSMENT QUESTIONS 1. The following is an accurate description of the aging population: A. The number of older adults will reach 17 million in 2030 B. The ratio of women to
Summary of Recommendation Statements Kidney International Supplements (2013) 3, 5 14; doi: /kisup
 3, 5 14; doi: /kisup") http://www.kidney-international.org & 2013 DIGO Summary of Recommendation Statements idney International Supplements (2013) 3, 5 14; doi:10.1038/kisup.2012.77 Chapter 1: Definition and classification of
http://www.kidney-international.org & 2013 DIGO Summary of Recommendation Statements idney International Supplements (2013) 3, 5 14; doi:10.1038/kisup.2012.77 Chapter 1: Definition and classification of
ADME Review. Dr. Joe Ritter Associate Professor of Pharmacology
 ADME Review Dr. Joe Ritter Associate Professor of Pharmacology 828-1022 jkritter@vcu.edu What percent of a weak base (pka = 7.5) and weak acid (pka = 3.5) will be respectively ionized in urine of ph 5.5?
ADME Review Dr. Joe Ritter Associate Professor of Pharmacology 828-1022 jkritter@vcu.edu What percent of a weak base (pka = 7.5) and weak acid (pka = 3.5) will be respectively ionized in urine of ph 5.5?
IV Vancomycin dosing and monitoring Antibiotic Guidelines. Contents. Intro
 IV Vancomycin dosing and Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary Medicine Unique
IV Vancomycin dosing and Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Committee Additional author(s): as above Authors Division: DCSS & Tertiary Medicine Unique
CARBOplatin (AUC5) and Etoposide 100mg/m 2 Therapy-21 day
 and Etoposide 100mg/m 2 Therapy-21 day") INDICATIONS FOR USE: CARBOplatin (AUC5) and 100mg/m 2 Therapy-21 day ICD10 Regimen Code INDICATION Small cell lung cancer (SCLC) extensive disease C34 00271a *If a reimbursement indicator (e.g. ODMS, CDS
INDICATIONS FOR USE: CARBOplatin (AUC5) and 100mg/m 2 Therapy-21 day ICD10 Regimen Code INDICATION Small cell lung cancer (SCLC) extensive disease C34 00271a *If a reimbursement indicator (e.g. ODMS, CDS
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
ECN Protocol Book. Generic Chemotherapy Protocol Guidelines. ECN_Protocol_Book_generic chemotherapy protocol guidelines guidelines_1
 ECN Protocol Book Generic Chemotherapy Protocol Guidelines Name of person presenting document: Reason for document development: Names of development team: Specify groups of staff to whom the document relates:
ECN Protocol Book Generic Chemotherapy Protocol Guidelines Name of person presenting document: Reason for document development: Names of development team: Specify groups of staff to whom the document relates:
Counties in the top and bottom two quintiles of both diabetes and obesity, Age-adjusted percentage of adults aged 20 years who are obese, 2007
 Impact of Obesity on Medication Dosing John C. Williamson, PharmD, BCPS, AAHIVE Wake Forest University Baptist Medical Center Winston-Salem, NC Objectives Determine what constitutes the various forms of
Impact of Obesity on Medication Dosing John C. Williamson, PharmD, BCPS, AAHIVE Wake Forest University Baptist Medical Center Winston-Salem, NC Objectives Determine what constitutes the various forms of
COMPOSITION. A film coated tablet contains. Active ingredient: irbesartan 75 mg, 150 mg or 300 mg. Rotazar (Film coated tablets) Irbesartan
 Irbesartan") Rotazar (Film coated tablets) Irbesartan Rotazar 75 mg, 150 mg, 300 mg COMPOSITION A film coated tablet contains Active ingredient: irbesartan 75 mg, 150 mg or 300 mg. Rotazar 75 mg, 150 mg, 300 mg PHARMACOLOGICAL
Rotazar (Film coated tablets) Irbesartan Rotazar 75 mg, 150 mg, 300 mg COMPOSITION A film coated tablet contains Active ingredient: irbesartan 75 mg, 150 mg or 300 mg. Rotazar 75 mg, 150 mg, 300 mg PHARMACOLOGICAL
Posology. Posology and Dosage Regimen: Factors Affecting Drug Dosage: 08/09/ ) Age: 1. Young s Rule, based on age:
 Age: 1. Young s Rule, based on age:") Posology and Dosage Regimen: Posology Posology: (Derived from the Greek posos- how much, and logos- science) is the branch of medicine/pharmacy dealing with doses. Posology is a branch of medical science
Posology and Dosage Regimen: Posology Posology: (Derived from the Greek posos- how much, and logos- science) is the branch of medicine/pharmacy dealing with doses. Posology is a branch of medical science
Assessing Renal Function: What you Didn t Know You Didn t Know
 Assessing Renal Function: What you Didn t Know You Didn t Know Presented By Tom Wadsworth PharmD, BCPS Associate Clinical Professor UAA/ISU Doctor of Pharmacy Program Idaho State University College of
Assessing Renal Function: What you Didn t Know You Didn t Know Presented By Tom Wadsworth PharmD, BCPS Associate Clinical Professor UAA/ISU Doctor of Pharmacy Program Idaho State University College of
Drug Distribution. Joseph K. Ritter, Ph.D., Assoc. Prof. Medical Sciences Building, Room
 Drug Distribution Joseph K. Ritter, Ph.D., Assoc. Prof. Medical Sciences Building, Room 531 jkritter@vcu.edu 828-1022 Department of Pharmacology and Toxicology Medical College of Virginia Campus Virginia
Drug Distribution Joseph K. Ritter, Ph.D., Assoc. Prof. Medical Sciences Building, Room 531 jkritter@vcu.edu 828-1022 Department of Pharmacology and Toxicology Medical College of Virginia Campus Virginia
Environmental Variability
 1 Environmental Variability Body Size, Body Composition, Maturation and Organ Function Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland 2 Objectives Understand the major sources
1 Environmental Variability Body Size, Body Composition, Maturation and Organ Function Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland 2 Objectives Understand the major sources
Excretion of Drugs. Prof. Hanan Hagar Pharmacology Unit Medical College
 Excretion of Drugs Prof. Hanan Hagar Pharmacology Unit Medical College Excretion of Drugs By the end of this lecture, students should be able to! Identify main and minor routes of excretion including renal
Excretion of Drugs Prof. Hanan Hagar Pharmacology Unit Medical College Excretion of Drugs By the end of this lecture, students should be able to! Identify main and minor routes of excretion including renal
PHA 5127 FINAL EXAM FALL On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 FINAL EXAM FALL 1997 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Question Points 1. /14 pts 2. /10 pts 3. /8 pts 4 /8 pts 5. /12 pts 6. /8 pts
PHA 5127 FINAL EXAM FALL 1997 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Question Points 1. /14 pts 2. /10 pts 3. /8 pts 4 /8 pts 5. /12 pts 6. /8 pts
OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4
![OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4](/thumbs/90/104143670.jpg "OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4") Opioid MCQ OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4 OP02 [Mar96] Which factor does NOT predispose to bradycardia with
Opioid MCQ OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4 OP02 [Mar96] Which factor does NOT predispose to bradycardia with
Identifying and Managing Chronic Kidney Disease: A Practical Approach
 Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Essential Shared Care Agreement: Lithium
 Ref No. E042 Essential Shared Care Agreement: Lithium Please complete the following details: Patient s name, address, date of birth Treatment (indication, dose regimen, brand name) Monitoring (proposed
Ref No. E042 Essential Shared Care Agreement: Lithium Please complete the following details: Patient s name, address, date of birth Treatment (indication, dose regimen, brand name) Monitoring (proposed
PHA Final Exam. Fall On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 Final Exam Fall 2012 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
PHA 5127 Final Exam Fall 2012 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
Special Challenges and Co-Morbidities
 Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
PHAR 7632 Chapter 16
 PHAR 7632 Chapter 16 Routes of Excretion Routes of Excretion Student Objectives for this Chapter After completing the material in this chapter each student should:- be able to describe the various routes
PHAR 7632 Chapter 16 Routes of Excretion Routes of Excretion Student Objectives for this Chapter After completing the material in this chapter each student should:- be able to describe the various routes
StRs and CT doctors in haematology. September Folinic acid dose modified.
 High dose Methotrexate and folinic acid rescue Full Title of Guideline: Author (include email and role): Division & Speciality: Clinical Guideline Review Date September 2018 GUIDELINE FOR THE USE OF HIGH
High dose Methotrexate and folinic acid rescue Full Title of Guideline: Author (include email and role): Division & Speciality: Clinical Guideline Review Date September 2018 GUIDELINE FOR THE USE OF HIGH
PHA Final Exam Fall 2006
 PHA 5127 Final Exam Fall 2006 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
PHA 5127 Final Exam Fall 2006 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
Tamer Barakat. Abdul Aziz ALShamali. Abdul Aziz ALShamali
 10 Tamer Barakat Abdul Aziz ALShamali Abdul Aziz ALShamali Dr. Alia Elimination: Refampin is used to treat TB not malaria (Quinacrine is used for malaria) It s the opposite process of absorption. It's
10 Tamer Barakat Abdul Aziz ALShamali Abdul Aziz ALShamali Dr. Alia Elimination: Refampin is used to treat TB not malaria (Quinacrine is used for malaria) It s the opposite process of absorption. It's
Renal function vs chemotherapy dosing
 Renal function vs chemotherapy dosing Jenny Casanova Senior Clinical Pharmacist Repatriation General Hospital Daw Park 1 Methods of estimating renal function Cockcroft-Gault (1976) C-G using ideal vs actual
Renal function vs chemotherapy dosing Jenny Casanova Senior Clinical Pharmacist Repatriation General Hospital Daw Park 1 Methods of estimating renal function Cockcroft-Gault (1976) C-G using ideal vs actual
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Farmadol. Paracetamol 10 mg/ml INFUSION SOLUTION
 Farmadol Paracetamol 10 mg/ml INFUSION SOLUTION Composition Each ml contains: Paracetamol 10 mg Pharmacology Pharmacodynamic properties The precise mechanism of the analgesic and antipyretic properties
Farmadol Paracetamol 10 mg/ml INFUSION SOLUTION Composition Each ml contains: Paracetamol 10 mg Pharmacology Pharmacodynamic properties The precise mechanism of the analgesic and antipyretic properties
8 th Annual Congress of the Bangladesh Society of Medicine Dhaka, Bangladesh March 23-24, Jeffrey P. Harris MD, FACP
 8 th Annual Congress of the Bangladesh Society of Medicine Dhaka, Bangladesh March 23-24, 2008 The Internist and the Pre-End Stage Renal Disease Patient Jeffrey P. Harris MD, FACP Country: Bangladesh Population:
8 th Annual Congress of the Bangladesh Society of Medicine Dhaka, Bangladesh March 23-24, 2008 The Internist and the Pre-End Stage Renal Disease Patient Jeffrey P. Harris MD, FACP Country: Bangladesh Population:
Introduction to Pharmacokinetics (PK) Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017
 Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017") Introduction to Pharmacokinetics (PK) Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017 1 Outline Definition & Relevance of Pharmacokinetics
Introduction to Pharmacokinetics (PK) Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017 1 Outline Definition & Relevance of Pharmacokinetics
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
AMINOGLYCOSIDES TDM D O N E B Y
 AMINOGLYCOSIDES TDM DONE BY: SARA ALARFAJ 2014 OUTLINE Introduction about Aminoglycosides. Spectrum/uses. TDM Aminoglycosides TDM Pharmacodynamics Pharmacokinetics. Dosing in AG. Sampeling time and Monitoring.
AMINOGLYCOSIDES TDM DONE BY: SARA ALARFAJ 2014 OUTLINE Introduction about Aminoglycosides. Spectrum/uses. TDM Aminoglycosides TDM Pharmacodynamics Pharmacokinetics. Dosing in AG. Sampeling time and Monitoring.
Renal Disease and PK/PD. Anjay Rastogi MD PhD Division of Nephrology
 Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
Pharmacokinetics Overview
 Pharmacokinetics Overview Disclaimer: This handout and the associated lectures are intended as a very superficial overview of pharmacokinetics. Summary of Important Terms and Concepts - Absorption, peak
Pharmacokinetics Overview Disclaimer: This handout and the associated lectures are intended as a very superficial overview of pharmacokinetics. Summary of Important Terms and Concepts - Absorption, peak
Rational Dose Prediction. Pharmacology. φαρμακον. What does this mean? pharmakon. Medicine Poison Magic Spell
 1 Rational Dose Prediction Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland, New Zealand 2 Pharmacology Pharmacology is derived from a Greek word (pharmakon). The Greeks used
1 Rational Dose Prediction Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland, New Zealand 2 Pharmacology Pharmacology is derived from a Greek word (pharmakon). The Greeks used
Elevation of Serum Creatinine: When to Screen, When to Refer. Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC
 Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised
 DABIGATRAN RECOMMENDED What it is Indications Date decision last revised") Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
Dialyzing challenging patients: Patients with hepato-renal conditions
 Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Gemcitabine + Cisplatin Regimen
 Gemcitabine + Cisplatin Regimen Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community Burton out-patient Derby out-patient Indication
Gemcitabine + Cisplatin Regimen Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community Burton out-patient Derby out-patient Indication
Metabolism. Objectives. Metabolism. 26 July Chapter 28 1
 Metabolism bjectives Describe various processes by which drugs are metabolized Describe induction and inhibition of metabolism Use the venous equilibration model to describe hepatic clearance and the effect
Metabolism bjectives Describe various processes by which drugs are metabolized Describe induction and inhibition of metabolism Use the venous equilibration model to describe hepatic clearance and the effect