How to Recognize Adrenal Disease
|
|
|
- Patience Baldwin
- 6 years ago
- Views:
Transcription

1 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi


2 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of Sea Courses Inc. except where permitted by law. Sea Courses is not responsible for any speaker or participant s statements, materials, acts or omissions.

3 Barriers To Change

 of interest: None to")
4 Disclosure of Commercial Support This program has not received financial support, or in-kind support, from any Pharmaceutical Company. Potential for conflict(s) of interest: None to declare

5 Faculty/Presenter Disclosure Faculty: Richard Bebb Relationships with commercial interests: None to report

6 Learning Objectives: Understanding Endocrine Hypertension Recognition of Common Adrenal Disorders

7 Case 1: 42 female 6 months of worsening diarrhea 15 lb weight loss (7 kg) Malaise, amenorrhea O/E BP 105/70 Creatinine 2.0 X normal K 5.3 mmol/l Na 132 mmol/l mild anemia benign urine sediment
8 Case 1: Your Next Step? 1) refer for renal biopsy 2) refer for GI work-up 3) am cortisol 4) ACTH level


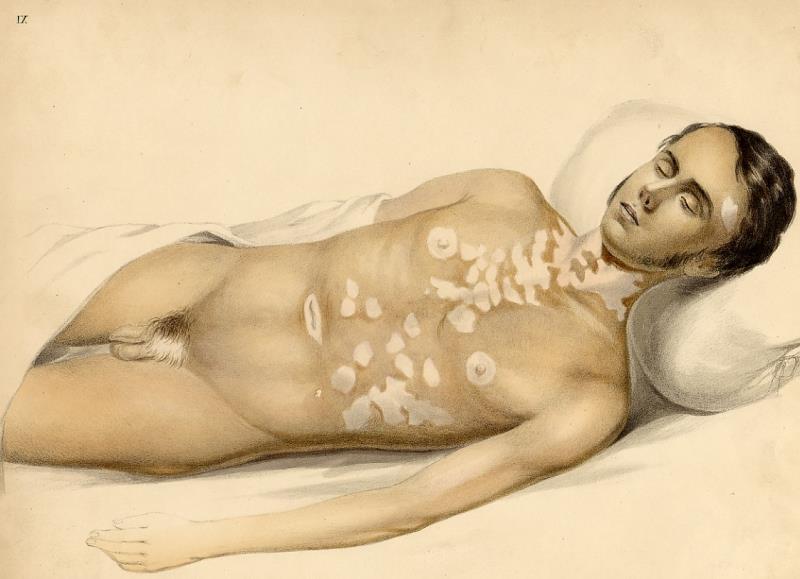
9 Adrenal failure: signs & symptoms Weakness & fatigue Anorexia & weight loss Nausea, vomiting & diarrhea Hyponatremia Hypotension Shock & death Hyperkalemia* Hyperpigmentation* *Only in primary adrenal failure
10

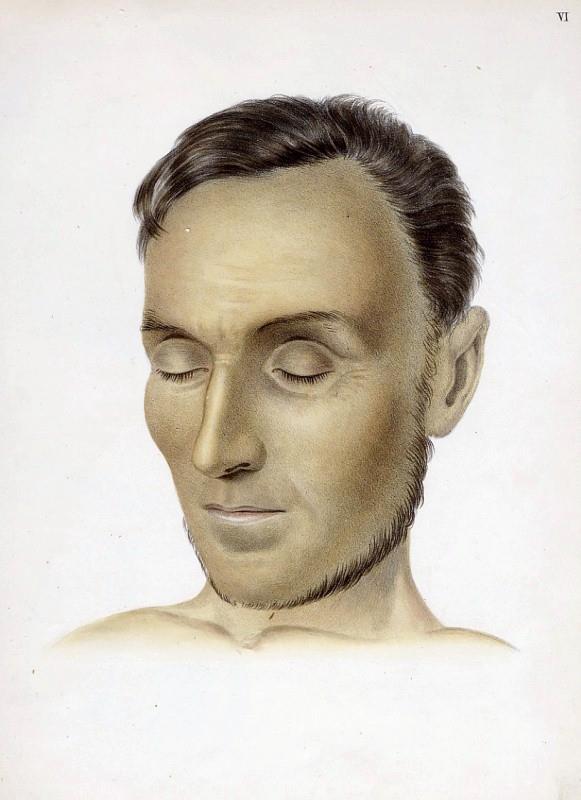
11 Addison s Disease
")
12 Adrenal failure: causes Primary (cortisol & aldosterone deficient) AUTOIMMUNE tuberculosis, fungal infections adrenal hemorrhage Secondary (cortisol deficient) pituitary lesions
 Not sensitive for new onset secondary adrenal failure (after pituitary surgery, pituitary")
13 Adrenal failure: evaluation Cortrosyn stimulation test: Cortrosyn 250 mcg IV Plasma 30 & 60 min Normal: > 550 nmol/l (20mcg/dl) Not sensitive for new onset secondary adrenal failure (after pituitary surgery, pituitary apoplexy)
14 ACTH 8 AM Serum Cortisol Testing In Adrenal Insufficiency Adrenal Insufficiency Primary Secondary Normal Recent Onset 2 0 Adrenal Insufficiency = Normal Range Time minutes Long-Standing 2 0 Adrenal Insufficiency 1 0 Adrenal Insufficiency

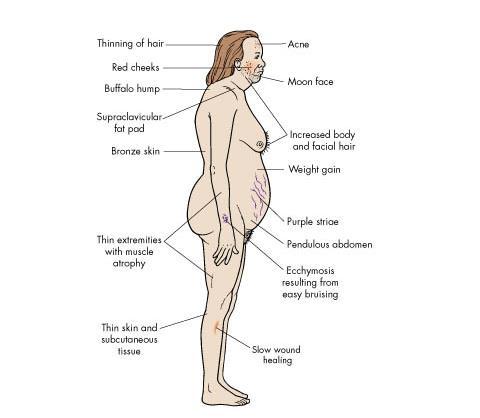
15 Obesity: Differential Diagnosis How to differentiate generic obesity from Cushing s syndrome





16 Cushing s Syndrome
17
 Thin")
")
18 Cushing s Striae 1) Thin depth 2) Wide width 3) Violaceous
 24 hr. Urinary free cortisol Late Night Salivary Cortisol (LNSC) Beware age, DM, BP, Stress, Shift workers Future:? Salivary Cortisone?")
19 Screening for Cushing s Syndrome 3 options: Over night 1 mg dexamethasone suppression testing (normal response is am cortisol < 50 mmol/l; <1.8 mg/dl) 24 hr. Urinary free cortisol Late Night Salivary Cortisol (LNSC) Beware age, DM, BP, Stress, Shift workers Future:? Salivary Cortisone??
")

20 Cortisol (ug/dl) Late Night Cortisol
21 Late-night Salivary Cortisol Evening values discriminated between the groups Morning values were not helpful Raff H et al. J Clin Endocrinol Metab 83: , 1998

22 Salivary Cortisol: Helpful with Pseudo Cushings Putignano P, et al. J Clin Endocrinol Metab 88:4153-7, 2003

23 UFC and LNSC in 43 patients with surgically proven Cushing's disease Salivary cortisol may be elevated when UFC is normal Elias PC et al. J Clin Endocrinol Metab 99: , 2014

24 Case 2: 24 year old female Routine physical BP 170/90 No meds Asymptomatic other than new headaches PRA 5 times upper limit of normal aldosterone high normal
 Fibromuscular dysplasia of renal artery 4) Cocaine")
25 Case 2: Diagnosis 1) Conn s Syndrome 2) Pheochromocytoma 3) Fibromuscular dysplasia of renal artery 4) Cocaine use

26 Secondary Hypertension The Big 3 are: Renal artery stenosis Hyperaldosteronism Pheochromocytoma

27 Hyperaldosteronism

28 Hyperaldosteronism Adenoma Bilateral Hyperplasia Adrenal Carcinoma GRA (Glucocorticoid remedial aldosteronism)
 Patients with sustained blood pressure above 150/100 mm Hg. 4) Patients with resistant hypertension (uncontrolled with three conventional antihypertensive drugs).")
29 Endocrine Society Guidelines: Hyperaldosteronism is often Missed; who to screen 1) Patients with hypertension (>140/90 mm Hg) with hypokalemia. 2) Patients with hypertension and sleep apnea. 3) Patients with sustained blood pressure above 150/100 mm Hg. 4) Patients with resistant hypertension (uncontrolled with three conventional antihypertensive drugs). 5) Patients with hypertension controlled with four or more medications. 6) Patients with hypertension and an adrenal incidentaloma (mass in the adrenal gland). 7) Patients with an early onset of hypertension (<40 years of age) and those with a family history of early-onset hypertension or stroke. 8) Patients with first-degree relatives with hypertension and a diagnosis of primary aldosteronism.

30 Signs and Symptoms in Primary Hyperaldosteronism Hypertension Weakness Muscle Cramps
 (no interfering medications) Clin Endocrinol Metab, May 2016,")
31 Hyper-aldosteronism Screening tests Serum Potassium Random plasma Aldosterone / Renin Ratio (potassium should be normalized) (no interfering medications) Clin Endocrinol Metab, May 2016, 101(5):

32 Adenoma (APA) vs Hyperplasia (IHA) Very High PAC/PRA Adenoma More severe hypertension and lower potassium suggests an adenoma Adrenal Vein Sampling Often Indicated

33 Safe Anti-hypertensives to use while Investigating Verapamil Hydralazine Alpha Blockers Do NOT start spironolactone. It makes investigating hyperaldosteronism impossible and takes 6 weeks to wear off Endocrine Society Guidelines 2016

34 Case 3: 34 year female 10 months of anxiety, headaches and sweating Stock trader Hypertensive for 5 years. BP now up to 160/90

35 Hypertension In Pheochromocytoma Paroxysmal in 48% Persistent in 29% Normal in 13%

36 Pheochromocytoma

37 Pheochromocytoma Symptoms (3 P) Attacks of Headaches (80%) Palpitations (64%) Diaphoresis (57%) Symptomatic Triad Of Headache, Sweating, And Tachycardia In A Hypertensive Patient Sensitivity 90.9% And Specificity 93.8%

38 How To Screen Urine Catecholamines or metabolites: metanephrines, normetanephrines, (VMA less helpful) Plasma Collection: Plasma-Free Metanephrines Are Recommended As The Test Of Choice For Excluding Or Confirming The Diagnosis Of Pheochromocytoma

39 Adrenal Conditions Not to Miss: Addison s Disease Cushing s Syndrome/Disease Conn s Syndrome Pheochromocytoma

40 Endocrine Diseases Often hard to detect THINK about them Order screening tests Do not be afraid to refer early
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management
 C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Update In Hyperthyroidism
 Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES
 HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Southern Derbyshire Shared Care Pathology Guidelines. Secondary Hypertension
 Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
The Adrenal Glands. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement. II.
 The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Endocrine Emergencies: Recognition and Management
 Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Hypertension: Who and How (and Why) to Investigate. Jessica Triay Andy Levy
 to Investigate. Jessica Triay Andy Levy") Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
Adrenal Gland Disorders
 1 Adrenal Gland Disorders Adrenal cortex steroid hormones (corticosteroids) 1. Glucocorticoids Regulate metabolism and blood glucose Critical to physiologic stress response 2. Mineralocorticoids Regulate
1 Adrenal Gland Disorders Adrenal cortex steroid hormones (corticosteroids) 1. Glucocorticoids Regulate metabolism and blood glucose Critical to physiologic stress response 2. Mineralocorticoids Regulate
Sajeev Menon MD ADRENAL INSUFFICIENCY? FATIGUE? OUTLINE OBJECTIVES PATIENT 1 PATIENT 1 : CLINICAL COURSE
 ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Cortisol levels. Naturally produced by the adrenal Cortisol
 1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
COPYRIGHTED MATERIAL. Adrenal Imaging. 1.1 Introduction. Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M.
 1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
ظظظ/ Omar Sami. Hussam Twaissi. Mousa Abbadi
 ظظظ/ 5 Omar Sami Hussam Twaissi Mousa Abbadi The doctor started this lecture by revising what we have taken in lecture number four, I won t re-write these stuff as it becomes boring so often. This sheet
ظظظ/ 5 Omar Sami Hussam Twaissi Mousa Abbadi The doctor started this lecture by revising what we have taken in lecture number four, I won t re-write these stuff as it becomes boring so often. This sheet
Differential Diagnosis of Cushing s Syndrome
 Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
in Primary Care (Part 2) Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University") Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Take Home Messages in Endocrinology
 Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Subclinical Cushing s Syndrome
 Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
ADDISON S DISEASE THE FACTS YOU NEED TO KNOW
 ADDISON S DISEASE THE FACTS YOU NEED TO KNOW WHAT IS Addison's disease is a severe or total deficiency of the hormones made in the adrenal cortex, caused by its destruction. There are normally two adrenal
ADDISON S DISEASE THE FACTS YOU NEED TO KNOW WHAT IS Addison's disease is a severe or total deficiency of the hormones made in the adrenal cortex, caused by its destruction. There are normally two adrenal
57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules. Celeste Thomas November 1, 2012
 57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules Celeste Thomas November 1, 2012 History of Present Illness 8 months prior to presentation developed intermittent right flank
57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules Celeste Thomas November 1, 2012 History of Present Illness 8 months prior to presentation developed intermittent right flank
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL?
 MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
Adrenal Disorders. Disclosure: I do not have any conflicts of interest
 Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
Endocrine Topic Review. Sethanant Sethakarun, MD
 Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
THE FACTS YOU NEED TO KNOW
 PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
Pathophysiology of the th E d n ocr i ne S S t ys em B. Marinov, MD, PhD Endocrine system Central: Hypothalamus
 Pathophysiology of the Endocrine System B. Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv Endocrine system Central: Hypothalamus Pituitary Pineal Peripheral Thymus Thyroid Parathyroid
Pathophysiology of the Endocrine System B. Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv Endocrine system Central: Hypothalamus Pituitary Pineal Peripheral Thymus Thyroid Parathyroid
Adrenal disease Real and Unreal. Objectives. Real
 Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
CPY 605 ADVANCED ENDOCRINOLOGY
 CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Secondary hypertension is defined as being
 Canadian Coalation for High Blood Pressure Prevention and Control Coalition Canadienne pour la Prévention et le Contrôle de l Hypertension Artérielle Secondary Hypertension: Diagnosis and Management Options
Canadian Coalation for High Blood Pressure Prevention and Control Coalition Canadienne pour la Prévention et le Contrôle de l Hypertension Artérielle Secondary Hypertension: Diagnosis and Management Options
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY
 JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
Spectrum of Hypertension & Hypokalemia
 Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
Endocrine Surgery When to Refer and What We Do
 Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Adrenal incidentaloma
 Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
1. Changed level of a certain hormone Stimulation of the oxygen consumption 3. Decoupling of oxidative phosphorylation 2.
 1. How can endocrine disorders be classified? 1. Hereditary, acquired 2. Active, passive 3. Uncompensated, overcompensated 4. Primary, secondary 5.1, 4 6.1, 2, 3, 4. ENDOCRINE SYSTEM 2. Which is the MAIN
1. How can endocrine disorders be classified? 1. Hereditary, acquired 2. Active, passive 3. Uncompensated, overcompensated 4. Primary, secondary 5.1, 4 6.1, 2, 3, 4. ENDOCRINE SYSTEM 2. Which is the MAIN
Adrenal gland Incidentaloma
 Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Pathophysiology of Adrenal Disorders
 Pathophysiology of Adrenal Disorders PHCL 415 Hadeel Alkofide April 2010 Some slides adapted from Rania Aljizani MSc 1 Learning Objectives Describe the roles of the various zones of the adrenal cortex
Pathophysiology of Adrenal Disorders PHCL 415 Hadeel Alkofide April 2010 Some slides adapted from Rania Aljizani MSc 1 Learning Objectives Describe the roles of the various zones of the adrenal cortex
ADRENAL LESIONS 10/09/2012. Adrenal + lesion. Introduction. Common causes. Anatomy. Financial disclosure. Dr. Boraiah Sreeharsha. Nothing to declare
 ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
MedKorat Endocrine Day 2018 Approach to common adrenal disorder
 MedKorat Endocrine Day 2018 Approach to common adrenal disorder Rungnapa Laortanakul, MD Nov.2018 Outline Adrenal insufficiency Cushing s syndrome Pheochromocytoma Primary Aldosteronism Adrenal incidentaloma
MedKorat Endocrine Day 2018 Approach to common adrenal disorder Rungnapa Laortanakul, MD Nov.2018 Outline Adrenal insufficiency Cushing s syndrome Pheochromocytoma Primary Aldosteronism Adrenal incidentaloma
October 13, Surgical Nuances to Managing Cushing s Disease. Cortisol Regulation. Cushing s Syndrome Excess Cortisol. Sandeep Kunwar, M.D.
 Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Morbidity & Mortality. Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005
 Morbidity & Mortality Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005 Case presentation Pt is a xx year old Asian woman who present to the ED with cc of epigastric
Morbidity & Mortality Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005 Case presentation Pt is a xx year old Asian woman who present to the ED with cc of epigastric
Hyperaldosteronism: Conn's Syndrome
 RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
Adrenal Incidentaloma Management
 Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal Gland. Zona Glomerulosa (mineralcorticoids) Zona Fasciculata (glucocorticoids) Zona Reticularis (sexual hormones) Adrenaline and noradrenaline
 Zona Fasciculata (glucocorticoids) Zona Reticularis (sexual hormones) Adrenaline and noradrenaline") n Cortex Zona Glomerulosa (mineralcorticoids) Zona Fasciculata (glucocorticoids) Zona Reticularis (sexual hormones) n Medulla Adrenaline and noradrenaline n Adrenocortical Hyperfunction Hyperaldosteronism
n Cortex Zona Glomerulosa (mineralcorticoids) Zona Fasciculata (glucocorticoids) Zona Reticularis (sexual hormones) n Medulla Adrenaline and noradrenaline n Adrenocortical Hyperfunction Hyperaldosteronism
Pharmacologic Management of Hypertension
 Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Management of adrenal incidentalomas
 31 Management of adrenal incidentalomas KEVIN MURTAGH, NANA MUHAMMAD AND MAREK MILLER The return of a scan result with reference to an incidental finding of an adrenal mass is a common scenario. 1 The
31 Management of adrenal incidentalomas KEVIN MURTAGH, NANA MUHAMMAD AND MAREK MILLER The return of a scan result with reference to an incidental finding of an adrenal mass is a common scenario. 1 The
Adrenal Insufficiency
 Adrenal Insufficiency Normal adrenal physiology Clinical features, Laboratory findings Common causes of primary adrenal insufficiency Evaluation of suspected adrenal insufficiency Acute and chronic management
Adrenal Insufficiency Normal adrenal physiology Clinical features, Laboratory findings Common causes of primary adrenal insufficiency Evaluation of suspected adrenal insufficiency Acute and chronic management
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess
 The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
Clinical Guideline. SPEG MCN Protocols Sub Group SPEG Steering Group
 Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT?
 ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
Assistant Professor of Endocrinology
 Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
The Management of adrenal incidentaloma
 The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
Cushing s syndrome and adrenal insufficiency
 Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
Endocrine Testing. Alice Y.Y. Cheng, MD, FRCP October 14, 2015
 Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE OBJECTIVES
 A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Diseases of the Adrenal Glands. Adrenal Insufficiency. Adrenal Hyperfunction. Hormonally Active Tumors.
 Diseases of the Adrenal Glands. Adrenal Insufficiency. Adrenal Hyperfunction. Hormonally Active Tumors. Essentials of Diagnosis, Treatment and Prevention of Major Endocrine Diseases LECTURE IN INTERNAL
Diseases of the Adrenal Glands. Adrenal Insufficiency. Adrenal Hyperfunction. Hormonally Active Tumors. Essentials of Diagnosis, Treatment and Prevention of Major Endocrine Diseases LECTURE IN INTERNAL
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST: Clinical Chemistry Guidelines
 Adrenocortical Insufficiency Guideline Document Information Policy Reference: Adrenocortical Insufficiency Issue: 1: Version 3 Author Job Title: Peter Prinsloo Consultant in Chemical Pathology STATUS:
Adrenocortical Insufficiency Guideline Document Information Policy Reference: Adrenocortical Insufficiency Issue: 1: Version 3 Author Job Title: Peter Prinsloo Consultant in Chemical Pathology STATUS:
When and how to perform a secondary hypertension work up? Docteur Cédric RAFAT Urgences Néphrologiques et Transplantation rénale Hôpital TENON
 When and how to perform a secondary hypertension work up? Docteur Cédric RAFAT Urgences Néphrologiques et Transplantation rénale Hôpital TENON Conflict of interest None related to the topic When to look
When and how to perform a secondary hypertension work up? Docteur Cédric RAFAT Urgences Néphrologiques et Transplantation rénale Hôpital TENON Conflict of interest None related to the topic When to look
Evaluation of Thyroid Nodules
 Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA
 The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
Managing Addison s Disease
 Managing Addison s Disease Dr Charles R Buchanan Consultant Paediatric Endocrinologist Kings College Hospital, London Thomas Addison 1793-1860 Guy s Hospial Described Symptoms 1855 My experience 25 years
Managing Addison s Disease Dr Charles R Buchanan Consultant Paediatric Endocrinologist Kings College Hospital, London Thomas Addison 1793-1860 Guy s Hospial Described Symptoms 1855 My experience 25 years
Inquadramento Clinico dell IncIdentaloma SurrenalIco
 Ferrara, 7 dicembre 2012 Inquadramento Clinico dell IncIdentaloma SurrenalIco Marta Bondanelli Sezione di Endocrinologia Dip. di Scienze Mediche Università degli Studi di Ferrara ADRENAL INCIDENTALOMA
Ferrara, 7 dicembre 2012 Inquadramento Clinico dell IncIdentaloma SurrenalIco Marta Bondanelli Sezione di Endocrinologia Dip. di Scienze Mediche Università degli Studi di Ferrara ADRENAL INCIDENTALOMA
ADRENAL GLAND. Introduction 4/21/2009. Among most important and vital endocrine organ. Small bilateral yellowish retroperitoneal organ
 Introduction Among most important and vital endocrine organ ADRENAL GLAND D.Hammoudi.MD Small bilateral yellowish retroperitoneal organ Lies just above kidney in gerota s fascia 2 1 The Adrenal Gland Anatomy
Introduction Among most important and vital endocrine organ ADRENAL GLAND D.Hammoudi.MD Small bilateral yellowish retroperitoneal organ Lies just above kidney in gerota s fascia 2 1 The Adrenal Gland Anatomy
Functional Pituitary Adenomas. Fawn M. Wolf, MD 2/2/2018
 Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
4/23/2015. Objectives DISCLOSURES
 2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs
 Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY
 THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
ENDOCRINOLOGY 3. R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice
 Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
Karim Said. 41 year old farmer. Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy
 Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Aldosterone-Producing Adrenocortical Carcinoma with Co-Secretion of Cortisol and Estradiol: A Case Report* Karen Lazaro and Perie Adorable-Wagan
 Case RePort Journal of the ASEAN Federation of Endocrine Societies with Co-Secretion of Cortisol and Estradiol: A Case Report* Karen Lazaro and Perie Adorable-Wagan Section of Endocrinology, Diabetes and
Case RePort Journal of the ASEAN Federation of Endocrine Societies with Co-Secretion of Cortisol and Estradiol: A Case Report* Karen Lazaro and Perie Adorable-Wagan Section of Endocrinology, Diabetes and