Introduction and Overview of the Current Landscape on Organ Donation and Transplantation in Canada Jag Gill, MD
|
|
|
- Brooke Quinn
- 6 years ago
- Views:
Transcription

1 2017 CST-Astellas Canadian Transplant Fellows Symposium Introduction and Overview of the Current Landscape on Organ Donation and Transplantation in Canada Jag Gill, MD Dr. Gill graduated from Medicine at the University of BC in 2001 and completed his post-graduate training in Internal Medicine and Nephrology at UBC in Dr. Gill completed a post-doctoral fellowship in kidney transplantation at the University of California, Los Angeles as part of the KRESCENT program and obtained a Masters degree in Public Health from Harvard University. He returned to Vancouver in 2008 and has been on staff at St. Paul s Hospital since. His primary clinical focus is in renal transplantation and his research interests are in transplant epidemiology and database analyses, examining access to transplantation, expansion of organ donation, and the impact of donor status on post-transplant health outcomes.
2 Case Studies CST Transplant Fellows Symposium September 25, 2017 Jag Gill
3 Case 1
4 Case 1 46 yo woman with ESRD from ADPKD Family history of ADPKD father with transplant and sister on dialysis Obese No other comorbidities; 1 pregnancy ROS negative for cardiac, respiratory, hematologic, malignancy, or ID concerns
5 Case 1 Preemptive LDKT from her husband No noted surgical complications ~100cc/hr urine output post transplant Pre-op CR was ~330 umol/l Hyperkalemic post-op K 1h 3h shifted with insulin, etc Good UO ~ 100cc/hr 80cc/hr given lasix for K and increases to 110cc/hr K down to 5.8 What do you do next (if anything)?
6 Case 1 Repeat bloodwork at 12 hours post tx K 6.3, Cr 354 What do you do next?
7 Case 1 CR was 333 preop 03:00 06:12 UO ~ 50cc/hr Urgent ultrasound gets ordered
8 Case 1 Ultrasound No hydronephrosis Reversal of flow within main renal artery with no definite flow in main renal vein; loss of flow in the ilac vein concerning for occlusive thrombosis of main renal vein with extension into the iliac vein OR ~ 230pm Poorly perfused kidney with right iliofemoral DVT; entire iliac was filled with clot; some flow still in the kidney No kinking or other technical problems with anastomosis were apparent

9
10 Case 1 Intubated in ICU; maintained on IV heparin MMF/Tac held; given additional dose of basliximab + hydrocortisone CRRT for lactic acidosis POD 3? bleeding heparin held POD 4 heparin restarted and extubated US no venous flow POD 5 renogram no flow POD 6 right transplant nephrouretectomy MMF/pred restarted peri-op
11 Case 1 Hematology assessment Risk factors: Family history of clotting (dad) Obesity Prothrombin gene mutations, FV Lieden, Protein C and S all normal Antithrombin III can t be tested on AC Plan for 6 months of AC with followup US and AT III
12 Case 1 Immunosuppression Maintained on low dose tacrolimus/mmf/pred R/A re repeat transplantation after heme workup completed in 6 months
13 Discussion point # 1 What could have been done differently during the assessment Thrombophlic workup not routinely done Family history of clots was negative on history as per patient Should we broaden criteria for thrombophilia testing pre-transplantation?
14 CST Consensus guidelines, 2005 The routine hematologic assessment of a renal transplant candidate should include a complete blood count, a differential white cell count and assessment of partial thromboplastin time and international normalized ratio. Additional investiga- tions, such as a hypercoagulability screen, bone marrow eval- uation or review by a hematologist, are recommended in cases of thrombophilia or hypercoagulability, monoclonal gammopathy and persistently abnormal blood counts. Increased graft thrombosis and rejection may be seen in patients with thrombophilia or hypercoagulability.218 Rou- tine screening of all kidney transplant candidates is likely to result in a low yield.219 However, those with a prior history of graft thrombosis, arterial or venous thrombosis, recurrent thrombosis of hemodialysis access (other than central ve- nous catheters) or SLE could benefit from screening.
15 Screening in non-tx populations Isolated provoked VTE screening not recommended Patients with VTE and family history or other risk factors should be screened No guidelines recommend routine screening of family members with recurrent DVT? Screening prior to pregnancy on women with family history of DVT
16 Discussion point #2 Evaluation of graft function in pre-emptive LDKT recipients Should SCR be tested more frequently in the first 24 hours (esp. preemptive)?
17 Discussion Point #3 Would you consider a repeat transplant in the patient? What you consider a prioritization for repeat transplantation? What do you do with immunosuppression at this time?
18 Case 2
19 Case 2 27 year old woman with ESRD due to unknown cause Presented with advanced renal dysfunction with a history of hypertension US bilateral shrunken kidneys precluded biopsy No other congenital abnormalities, but does have issues with low IQ and poor memory Presents very well; married, strong social supports with her husband and mother Has not had major issues with non-adherence based on her nephrologists assessment
20 Do you have any concerns regarding her transplant candidacy?
21 Do you have any concerns regarding her transplant candidacy? Unknown primary disease Cognitive issues
22 Case 2 Blood type B 0 PRA egfr 14ml/min Potential living donor Friend, blood type O, 0 DR mismatch; DQ mismatch
23 Case 2 Preemptive live donor kidney transplant What would you give for immunosuppression? What mechanisms would you put in place to ensure adherence and monitor this?
24 Case 2 Basiliximab induction Tacrolimus, MMF Steroid free (given young age, 0 PRA)
25 Case 2 Well post transplant Cr ~ umol/l within 2 days; excellent UO No adverse reactions Tacrolimus levels good in hospital 1 week post discharge, tacrolimus levels ranged from 3 to 14 What do you do?
26 Case 2 10 days post DC Cr increased from baseline of to 94 What do you do now?
27 Biopsy Isolated 2A rejection Focal endarteritis Mononuclear interstitial inflammation; focal tubulitis
28 Solumedrol 500mg IV X 3 doses, prednisone Cr fell to 75umol/L; Stable thereafter Tacrolimus was still erratic What would you do about the erratic tacrolimus levels?
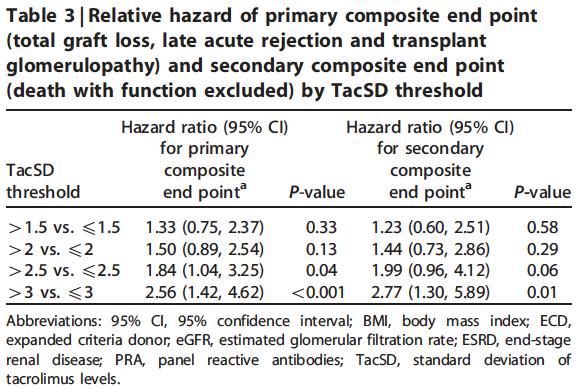
29 Tacrolimus variability wide variations in trough tacrolimus blood levels are associated with acute rejection and allograft failure non-adherence, drug prescription patterns, variability in drug absorption/metabolism, and drug drug interactions may result in IPV in tacrolimus trough levels Hsiau, et al. Transplantation 2011; 92: Pollock-Barziv SM, et al. Pediatr Transplant 2010; 14: Borra et al. Nephrol Dial Transplant 2010; 25:
30 Sapir-Pichhadze, et al. KI 2013
31 Case 2 2 months later, Cr increased to 148 umol/l Repeat biopsy 2A rejection Evidence of glomerulitis; no peri-tubular capillaritis, C4d negative; No anti-hla antibodies found How would you treat?
32 Diagnostic criteria for acute ABMR Histologic evidence of acute tissue injury MVI (glomerulitis and/or peritubular capillaritis Intimal or transmural arteritis Acute TMA without other cause Evidence of current or recent antibody interaction with vascular endothelium Linear C4d staining in peritubular capillaries Serologic evidence of DSA
33 Non-HLA antibody associated AMR Typically have C4d positivity AMR reported with the following antibodies Angiotensin II receptor antibody (HTN) Anti-endothelial antibodies Major histocompatibility complex class I chain related gene A (MICA)
34 Case 2 ratg (6.5mg/kg) + steroids Had a modest improvement in renal function (Cr decreased to 80s) What next?
35 Case 2 Cr stayed at 80 and then climbed to low 100s Repeat biopsy 2A rejection with glomerulitis C4d positive Peritubular capillaritis DSA to DQ4 MFI 2800 What next?
36 Case 2 Treatment for ABMR PLEX/Rituximab/low dose IVIG Renal function deteriorated over 1 week and became dialysis dependent Continued ABMR treatment for 3 weeks How long would you continue treatment?
37 Diagnostic criteria for chronic ABMR Morphologic evidence of chronic tissue injury TG, severe peritubular capillary basement membrane multilayering Arterial intimal fibrosis Evidence of current or recent AB interaction with vascular endothelim (C4d) Serologic evidence of DSA
38 Repeat Biopsy Acute tubular injury Ongoing glomerulitis Double contouring of glomeruli (suggestive of chronic active ABMR) Continued treatment for 2 weeks Tacrolimus level still extremely variable Admitted with urosepsis and pneumonia Feeling unwell on dialysis
39 Case 2 Discontinued PLEX Repeat biopsy 1 month later Significant interstitial fibrosis Dialysis dependent for 7 weeks now What next?
40 Is she a re-transplant candidate?
41 Case 3
42 Case 3 23 yo woman presents as a potential living kidney donor for her brother ABO compatible Brother has type I diabetes - has advanced CKD (egfr 14ml/min) due to DMN Family history of diabetes nil except brother Medical history is otherwise benign No renal issues, no risk factors for kidney disease Cr 73, egfr 84ml/min Nuclear renogram GFR 89ml/min; normalized for BSA 94ml/min What do you tell her about the risks of kidney donation and what are her specific risks?
43 Would you accept her as a donor? What considerations do you have? Size her BMI is 19 ht 5 wt 100lbs her brother s BMI is 24 ht 6 wt 175lbs Level of HLA MM 1 haplotype match ABO Both are blood type O Other options There is another blood type incompatible donor (ABO A) - willing to go in KPD
44 What options would you present?
45 What options would you present? Would you recommend she donate directly? Would you recommend she not donate? Would you recommend the other donor donate through KPD? Would you recommend she donate through KPD?
46 Case 4
47 Case 4 74 yo man previous living kidney donor Donated to his brother (had ESRD from HTN) when he was 48 yo Baseline assessment at time of donation was benign No HTN; family history of HTN and ESRD no diabetic risk factors Slightly overweight Pre-donation Cr ~ 80; post donation Cr ~ 120
48 How would you follow this donor? How frequently What would you check? For how long? Who would coordinate this?
49 KDIGO (draft) 18.1: Living kidney donors should be monitored long-term for hypertension, CKD, and overall health status and well-being. Blood pressure, egfr based on serum creatinine, and urine albumin testing are particularly important parameters to follow in kidney donors due to concerns for the impact of donation on long-term risk for development of hypertension and CKD. Assessment should include not only the absolute level of egfr but also its trajectory over time. (Not Graded) 18.2: The following specific practices should be performed annually for each donor as part of post-donation follow-up care: (Not Graded) Blood pressure measurement Body mass index measurement Serum creatinine testing with estimation of GFR (egfr) Evaluation for albuminuria Evidence of diabetes Review and promotion of healthy lifestyle practices including exercise, diet, avoidance of smoking Review of psychosocial health and well-being as it relates to their donation experience.
50 18.3: Follow-up information should be reported to national and/or regional registries to facilitate aggregation, assessment and dissemination of current donor outcomes data. (Not Graded) 18.4: Donors who develop hypertension or CKD should receive appropriate medical treatment for these conditions according to clinical practice guidelines for the conditions. (Not Graded) 18.5: Donors should receive age-appropriate healthcare maintenance according to clinical practice guidelines for the regional population. (Not Graded) 18.6: Metabolic conditions (e.g., diabetes), cardiovascular diseases (e.g., coronary artery disease, congestive heart failure), and cardiovascular risk factors (e.g,. hyperlipidemia, obesity) or risk behaviors (e.g., smoking, sedentary lifestyle) should be evaluated during post-donation healthcare maintenance assessments and managed according to general population guidelines. (Not Graded) 18.7: Donor education provided prior to and at the time of donation should be reinforced by post-donation educational contacts from the transplant center such as newsletters, links to transplant center health recommendations or national guideline website documents to promote sustained healthy lifestyle choices and behaviors. (Not Graded) : When important new information becomes available on the long-term outcomes of living kidney donors that differs from what a donor was told prior to donation, the transplant program should use reasonable efforts to contact past donors and provide this information. (Not Graded)
51 Follow-up of living donors Extremely variable between regions OPTN (2013) Mandatory 6 month, 1 year and 2 year follow-up
52 Percent Adherence to follow-up is poor Proportion of donors that completed follow-up testing post donation Years post-donation O Brian, Gil J
53 Case 4 Did not adhere to follow-up and presented with hypertension at age 58 Reviewed by nephrologist Poorly adherent with follow-up; Contracted hepatitis C in his 60s 7 years later found to have renal dysfunction not biopsied, but believed to be hepatitis related treated with IFN for HCV with good response but renal function continued to deteriorate Followed by nephrology since then egfr is now 17ml/min; somewhat symptomatic
54 Case 4 Requesting transplant assessment Undergoes transplant assessment and is felt to be suitable to receive a kidney transplant; no potential donors He does not want to do dialysis; will only consider a transplant He asks if he gets a priority on the wait-list since he is a prior living kidney donor
55 Priorities for prior living donors?
56 Would you list him preemptively? What are the considerations?
57 Would you deviate from routine allocation policies Would you allocate and ECD kidney to him? Would you prioritize an SCD kidney for him? What are the considerations?
58 What we did (and our rationale) We prioritized him for an SCD kidney and preemptively listed him Rationale: prior living donors have contributed to the health of kidney patients and society and are therefore owed a prioritization There is a need to standardize what we mean by prioritization for transplantation and be transparent about the rules of application
Statement of Disclosure
 Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Review of Rituximab and renal transplantation. Dr.E Nemati. Professor of Nephrology
 Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
The New Kidney Allocation System: What You Need to Know. Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health
 The New Kidney Allocation System: What You Need to Know Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health ~6% of patients die each year on the deceased donor waiting
The New Kidney Allocation System: What You Need to Know Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health ~6% of patients die each year on the deceased donor waiting
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference
 The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
HLA Part II: My Patient Has DSA, Now What?
 2017 CST-Astellas Canadian Transplant Fellows Symposium HLA Part II: My Patient Has DSA, Now What? James Lan, MD, FRCPC, D(ABHI) Dr. Lan completed his nephrology training at the University of British Columbia.
2017 CST-Astellas Canadian Transplant Fellows Symposium HLA Part II: My Patient Has DSA, Now What? James Lan, MD, FRCPC, D(ABHI) Dr. Lan completed his nephrology training at the University of British Columbia.
Transplant Options for Patients: Choices and Consequences. Olwyn Johnston Medical Director Kidney Transplantation Vancouver General Hospital
 Transplant Options for Patients: Choices and Consequences Olwyn Johnston Medical Director Kidney Transplantation Vancouver General Hospital BC Kidney Days October 6 th 2017 Non contributory Conflict of
Transplant Options for Patients: Choices and Consequences Olwyn Johnston Medical Director Kidney Transplantation Vancouver General Hospital BC Kidney Days October 6 th 2017 Non contributory Conflict of
HLA and Non-HLA Antibodies in Transplantation and their Management
 HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
Living Donor Paired Exchange (LDPE)
") Living Donor Paired Exchange (LDPE) Why do we need Living Donation? 3,796 patients waiting for an organ transplant 2,679 (71%) waiting for a kidney transplant 249 people died while waiting for an organ
Living Donor Paired Exchange (LDPE) Why do we need Living Donation? 3,796 patients waiting for an organ transplant 2,679 (71%) waiting for a kidney transplant 249 people died while waiting for an organ
Update on Transplant Glomerulopathy
 Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University of Tennessee Health Science Center
Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University of Tennessee Health Science Center
Renal Transplant Past Present and Future David Landsberg
 2012 Renal Transplant Past Present and Future David Landsberg Outline Changing pattern of Donors Types of Donors Allocation Results Challenges in the Elderly LDPE Transplants By Year LD LRD LUD NDAD DD
2012 Renal Transplant Past Present and Future David Landsberg Outline Changing pattern of Donors Types of Donors Allocation Results Challenges in the Elderly LDPE Transplants By Year LD LRD LUD NDAD DD
The New Kidney Allocation System: What You Need to Know. Quality Insights Renal Network 3 Annual Meeting October 2, 2014
 The New Kidney Allocation System: What You Need to Know Quality Insights Renal Network 3 Annual Meeting October 2, 2014 Pre Dialysis Era Dialysis Status in USA 500,000 patients on dialysis in 2013 100,000
The New Kidney Allocation System: What You Need to Know Quality Insights Renal Network 3 Annual Meeting October 2, 2014 Pre Dialysis Era Dialysis Status in USA 500,000 patients on dialysis in 2013 100,000
Cases: CMV, HCV, BKV and Kidney Transplantation. Simin Goral, MD University of Pennsylvania Medical Center
 Cases: CMV, HCV, BKV and Kidney Transplantation Simin Goral, MD University of Pennsylvania Medical Center Disclosures Grant support: Otsuka Pharmaceuticals, Astellas Pharma, Angion, AstraZeneca, and Kadmon
Cases: CMV, HCV, BKV and Kidney Transplantation Simin Goral, MD University of Pennsylvania Medical Center Disclosures Grant support: Otsuka Pharmaceuticals, Astellas Pharma, Angion, AstraZeneca, and Kadmon
Interstitial Inflammation
 Interstitial Inflammation Currently considered to be T cell-mediated process Plasma cell rich acute rejection often associated with AMR Preliminary data suggests that interstitial follicular helper T cells
Interstitial Inflammation Currently considered to be T cell-mediated process Plasma cell rich acute rejection often associated with AMR Preliminary data suggests that interstitial follicular helper T cells
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol
 Josep M. Campistol") Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies
 Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Objectives. Kidney Complications With Diabetes. Case 10/21/2015
 Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Management of a Recipient with a Failed Kidney Transplant. Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
 Management of a Recipient with a Failed Kidney Transplant Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Objectives Epidemiology of transplant failure Timing of dialysis
Management of a Recipient with a Failed Kidney Transplant Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Objectives Epidemiology of transplant failure Timing of dialysis
7-2 Transplantation Case-Based Discussion
 The 58 th JSN 2015/6/4@Nagoya APSN Continuing Medical Education Course 2015 7-2 Transplantation Case-Based Discussion Tadashi Sofue, MD, PhD Division of Nephrology and Dialysis, Department of Internal
The 58 th JSN 2015/6/4@Nagoya APSN Continuing Medical Education Course 2015 7-2 Transplantation Case-Based Discussion Tadashi Sofue, MD, PhD Division of Nephrology and Dialysis, Department of Internal
Transplant in Pediatric Heart Failure
 Transplant in Pediatric Heart Failure Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart and Lung Transplantation
Transplant in Pediatric Heart Failure Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart and Lung Transplantation
Pediatric Kidney Transplantation
 Pediatric Kidney Transplantation Vikas Dharnidharka, MD, MPH Associate Professor Division of Pediatric Nephrology Conflict of Interest Disclosure Vikas Dharnidharka, MD, MPH Employer: University of Florida
Pediatric Kidney Transplantation Vikas Dharnidharka, MD, MPH Associate Professor Division of Pediatric Nephrology Conflict of Interest Disclosure Vikas Dharnidharka, MD, MPH Employer: University of Florida
Update on organ donation in British Columbia
 Update on organ donation in British Columbia Jagbir Gill MD MPH FRCPC Associate Professor of Medicine, UBC Vice President, CORR Board 2017 BC Kidney Days October 5, 2017 Canadian Institute for Health Information
Update on organ donation in British Columbia Jagbir Gill MD MPH FRCPC Associate Professor of Medicine, UBC Vice President, CORR Board 2017 BC Kidney Days October 5, 2017 Canadian Institute for Health Information
Kidney Transplant in the Elderly. Robert Santella, M.D., F.A.C.P.
 Kidney Transplant in the Elderly! Robert Santella, M.D., F.A.C.P. Incident Rate of ESRD by Age Age 75+ 65-74 From US Renal Data System, 2012 Should there be an age limit? Various guidelines: Canadian,
Kidney Transplant in the Elderly! Robert Santella, M.D., F.A.C.P. Incident Rate of ESRD by Age Age 75+ 65-74 From US Renal Data System, 2012 Should there be an age limit? Various guidelines: Canadian,
Update on Transplant Glomerulopathy
 Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Methodist University Hospital, Transplant Institute Division of Transplantation, Department
Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Methodist University Hospital, Transplant Institute Division of Transplantation, Department
Overview. Evaluation of Potential Kidney Transplant Recipients. Projected Years of Life in Patients with ESRD
 Evaluation of Potential Kidney Transplant Recipients Donald E. Hricik MD Professor of Medicine and Chief, Division of Nephrology and Hypertension University Hospitals Case Medical Center Conflict of Interest
Evaluation of Potential Kidney Transplant Recipients Donald E. Hricik MD Professor of Medicine and Chief, Division of Nephrology and Hypertension University Hospitals Case Medical Center Conflict of Interest
Kidney Summary. Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA
 Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
Literature Review Transplantation
 Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
PATIENT SELECTION FOR DECEASED DONOR KIDNEY ONLY TRANSPLANTATION
 PATIENT SELECTION FOR DECEASED DONOR KIDNEY ONLY TRANSPLANTATION This policy has been created by the Kidney Advisory Group on behalf of NHSBT. The policy has been considered and approved by the Organ Donation
PATIENT SELECTION FOR DECEASED DONOR KIDNEY ONLY TRANSPLANTATION This policy has been created by the Kidney Advisory Group on behalf of NHSBT. The policy has been considered and approved by the Organ Donation
Biopsy Features of Kidney Allograft Rejection Banff B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Back to dialysis after graft failure: Transplantectomy or not? Stop immunosuppression?
 Back to dialysis after graft failure: Transplantectomy or not? Stop immunosuppression? Laurent WEEKERS CHU SartTilman Layout Introduction Epidemiology A note of caution on causality and bias Patient survival
Back to dialysis after graft failure: Transplantectomy or not? Stop immunosuppression? Laurent WEEKERS CHU SartTilman Layout Introduction Epidemiology A note of caution on causality and bias Patient survival
Management of a Recipient with a Failed Kidney Transplant. Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
 Management of a Recipient with a Failed Kidney Transplant Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Disclosures Grant support: Bristol-Myers and Squibb Pharmaceuticals,
Management of a Recipient with a Failed Kidney Transplant Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Disclosures Grant support: Bristol-Myers and Squibb Pharmaceuticals,
Predictors of cardiac allograft vasculopathy in pediatric heart transplant recipients
 Pediatr Transplantation 2013: 17: 436 440 2013 John Wiley & Sons A/S. Pediatric Transplantation DOI: 10.1111/petr.12095 Predictors of cardiac allograft vasculopathy in pediatric heart transplant recipients
Pediatr Transplantation 2013: 17: 436 440 2013 John Wiley & Sons A/S. Pediatric Transplantation DOI: 10.1111/petr.12095 Predictors of cardiac allograft vasculopathy in pediatric heart transplant recipients
Renal Pathology- Transplantation. Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic
 Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
Case 1 AND. Treatment of HCV: Pre- vs Post- Transplant. 58 yo male, ESRD/diabetic nephropathy, HD for 3 weeks
 Treatment of HCV: Pre- vs Post- Transplant Roy D. Bloom MD Professor of Medicine University of Pennsylvania Roy D. Bloom MD Professor of Medicine Medical Director, Kidney Transplant Program University
Treatment of HCV: Pre- vs Post- Transplant Roy D. Bloom MD Professor of Medicine University of Pennsylvania Roy D. Bloom MD Professor of Medicine Medical Director, Kidney Transplant Program University
Chronic Kidney Disease (CKD) Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.
 Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.") Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
For more information about how to cite these materials visit
 Author(s): Silas P. Norman, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Silas P. Norman, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Should red cells be matched for transfusions to patients listed for renal transplantation?
 Should red cells be matched for transfusions to patients listed for renal transplantation? Dr M.Willicombe Imperial College Renal and Transplant Centre, Hammersmith Hospital Should red cells be matched
Should red cells be matched for transfusions to patients listed for renal transplantation? Dr M.Willicombe Imperial College Renal and Transplant Centre, Hammersmith Hospital Should red cells be matched
Progress in Pediatric Kidney Transplantation
 Send Orders for Reprints to reprints@benthamscience.net The Open Urology & Nephrology Journal, 214, 7, (Suppl 2: M2) 115-122 115 Progress in Pediatric Kidney Transplantation Jodi M. Smith *,1 and Vikas
Send Orders for Reprints to reprints@benthamscience.net The Open Urology & Nephrology Journal, 214, 7, (Suppl 2: M2) 115-122 115 Progress in Pediatric Kidney Transplantation Jodi M. Smith *,1 and Vikas
Home Hemodialysis or Transplantation of the Treatment of Choice for Elderly?
 Home Hemodialysis or Transplantation of the Treatment of Choice for Elderly? Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University
Home Hemodialysis or Transplantation of the Treatment of Choice for Elderly? Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University
Three Sides to Allocation. ECD Extended Criteria Donor
 Kidney Allocation- Optimal Use of Deceased Donors The New US System..and impact on wait list management Three Sides to Allocation Justice Peter G Stock MD, PhD Utility Efficiency Standard Criteria Donor
Kidney Allocation- Optimal Use of Deceased Donors The New US System..and impact on wait list management Three Sides to Allocation Justice Peter G Stock MD, PhD Utility Efficiency Standard Criteria Donor
The New Kidney Allocation Policy: Implications for Your Patients and Your Practice
 The New Kidney Allocation Policy: Implications for Your Patients and Your Practice Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Explain
The New Kidney Allocation Policy: Implications for Your Patients and Your Practice Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Explain
LIVE KIDNEY DONOR RISK PREDICTION ; NEW PARADIGM, NEW CALCULATORS PEDRAM AHMADPOOR MD
 LIVE KIDNEY DONOR RISK PREDICTION ; NEW PARADIGM, NEW CALCULATORS PEDRAM AHMADPOOR MD Outline: PART 1 : Update on safety of nephrectomy for living donor candidate PART 2 : Latest guideline recommendation
LIVE KIDNEY DONOR RISK PREDICTION ; NEW PARADIGM, NEW CALCULATORS PEDRAM AHMADPOOR MD Outline: PART 1 : Update on safety of nephrectomy for living donor candidate PART 2 : Latest guideline recommendation
Strategies for Desensitization
 Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
Getting a New Kidney UHN. Information for patients and families. Is a kidney transplant right for me? Read this booklet to learn:
 Getting a New Kidney UHN Information for patients and families Read this booklet to learn: about kidney transplants who can be donors how to start the transplant process how long the process might take
Getting a New Kidney UHN Information for patients and families Read this booklet to learn: about kidney transplants who can be donors how to start the transplant process how long the process might take
Candidates about. Lung Allocation Policy. for Transplant. Questions & A n s we r s TA L K I N G A B O U T T R A N S P L A N TAT I O N
 TA L K I N G A B O U T T R A N S P L A N TAT I O N Questions & A n s we r s for Transplant Candidates about Lung Allocation Policy U N I T E D N E T W O R K F O R O R G A N S H A R I N G What are the OPTN
TA L K I N G A B O U T T R A N S P L A N TAT I O N Questions & A n s we r s for Transplant Candidates about Lung Allocation Policy U N I T E D N E T W O R K F O R O R G A N S H A R I N G What are the OPTN
Jadranka Buturović-Ponikvar Department of Nephrology, University Medical Center, Ljubljana, Slovenia
 Jadranka Buturović-Ponikvar Department of Nephrology, University Medical Center, Ljubljana, Slovenia Hemodialysis or kidney transplantation what is better? Jadranka Buturović-Ponikvar Department of Nephrology,
Jadranka Buturović-Ponikvar Department of Nephrology, University Medical Center, Ljubljana, Slovenia Hemodialysis or kidney transplantation what is better? Jadranka Buturović-Ponikvar Department of Nephrology,
kidney OPTN/SRTR 2012 Annual Data Report:
 kidney wait list 18 deceased donation 22 live donation 24 transplant 26 donor-recipient matching 28 outcomes 3 pediatric transplant 33 Medicare data 4 transplant center maps 43 A. J. Matas1,2, J. M. Smith1,3,
kidney wait list 18 deceased donation 22 live donation 24 transplant 26 donor-recipient matching 28 outcomes 3 pediatric transplant 33 Medicare data 4 transplant center maps 43 A. J. Matas1,2, J. M. Smith1,3,
Kidney Transplant. November 4 th, 2016
 Kidney Transplant November 4 th, 2016 Brad West, MD, FACP Medical Director of Transplant Services, Memorial Medical Center Chairman Department of Nephrology, Springfield Clinic 1 Adjusted survival: 1993-1997
Kidney Transplant November 4 th, 2016 Brad West, MD, FACP Medical Director of Transplant Services, Memorial Medical Center Chairman Department of Nephrology, Springfield Clinic 1 Adjusted survival: 1993-1997
Transfusion support in Transplantation
 Transfusion support in Transplantation Patricia Campbell University of Alberta Hospitals University of Alberta Objectives UofA transplant programs What we do and why? HLA and ABO incompatible transplants
Transfusion support in Transplantation Patricia Campbell University of Alberta Hospitals University of Alberta Objectives UofA transplant programs What we do and why? HLA and ABO incompatible transplants
Barriers to Transplantation
 Barriers to Transplantation Ruth McCarrell RN BSN CNeph(C) Clinical Nurse Leader Kidney transplant Program St. Paul s Hospital Email: rmccarrell@providencehealth.bc.ca Overview Transplant Basics Living
Barriers to Transplantation Ruth McCarrell RN BSN CNeph(C) Clinical Nurse Leader Kidney transplant Program St. Paul s Hospital Email: rmccarrell@providencehealth.bc.ca Overview Transplant Basics Living
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials
 The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
Simultaneous Pancreas Kidney Transplantation:
 Simultaneous Pancreas Kidney Transplantation: What is the added advantage, and for whom? Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney
Simultaneous Pancreas Kidney Transplantation: What is the added advantage, and for whom? Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney
DSA Positive and then To biopsy or not?
 DSA Positive and then To biopsy or not? Banff SCT 2017 29 March 2017 Peter Nickerson, MD, FRCPC, FCAHS Flynn Family Chair in Renal Transplantation Professor of Internal Medicine and Immunology Relevant
DSA Positive and then To biopsy or not? Banff SCT 2017 29 March 2017 Peter Nickerson, MD, FRCPC, FCAHS Flynn Family Chair in Renal Transplantation Professor of Internal Medicine and Immunology Relevant
The Kidney Allocation System Changed in a Substantive Way on December 5, Your Patients Have Been, and Will Be, Affected by These Changes
 The Kidney Allocation System Changed in a Substantive Way on December 5, 2014 Your Patients Have Been, and Will Be, Affected by These Changes 1 The New Kidney Allocation System Terms of Importance Pediatric
The Kidney Allocation System Changed in a Substantive Way on December 5, 2014 Your Patients Have Been, and Will Be, Affected by These Changes 1 The New Kidney Allocation System Terms of Importance Pediatric
Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients
 Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients Stanley C. Jordan, MD Director, Division of Nephrology Medical Director, Kidney Transplant Program Medical
Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients Stanley C. Jordan, MD Director, Division of Nephrology Medical Director, Kidney Transplant Program Medical
Chapter 6: Transplantation
 Chapter 6: Transplantation Introduction During calendar year 2012, 17,305 kidney transplants, including kidney-alone and kidney plus at least one additional organ, were performed in the United States.
Chapter 6: Transplantation Introduction During calendar year 2012, 17,305 kidney transplants, including kidney-alone and kidney plus at least one additional organ, were performed in the United States.
Kidney Transplant Outcomes In Elderly Patients. Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
 Kidney Transplant Outcomes In Elderly Patients Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case Discussion 70 year old Asian male, neuropsychiatrist, works full
Kidney Transplant Outcomes In Elderly Patients Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case Discussion 70 year old Asian male, neuropsychiatrist, works full
Are two better than one?
 Are two better than one? Disclosures Ryutaro Hirose, MD Professor in Clinical Surgery University of California, San Francisco I have no relevant disclosures related to this presentation The PROBLEM There
Are two better than one? Disclosures Ryutaro Hirose, MD Professor in Clinical Surgery University of California, San Francisco I have no relevant disclosures related to this presentation The PROBLEM There
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Loupy A, Lefaucheur C, Vernerey D, et al. Complement-binding
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Loupy A, Lefaucheur C, Vernerey D, et al. Complement-binding
Dictionary of Organ Donation and Transplantation Terms
 Dictionary of Organ Donation and Transplantation Terms Acute Rejection: The body s attempt to destroy the transplanted organ. Acute rejection usually occurs in the first year after transplant. Adverse
Dictionary of Organ Donation and Transplantation Terms Acute Rejection: The body s attempt to destroy the transplanted organ. Acute rejection usually occurs in the first year after transplant. Adverse
Renal Transplant. Tony Chacon. Program Head BCIT Nephrology Nursing Program.
 Renal Transplant Tony Chacon Program Head BCIT Nephrology Nursing Program Email: tony_chacon@bcit.ca Summary of CNA Renal Transplant Competencies Potential contraindications to renal transplant. Assessment/selection
Renal Transplant Tony Chacon Program Head BCIT Nephrology Nursing Program Email: tony_chacon@bcit.ca Summary of CNA Renal Transplant Competencies Potential contraindications to renal transplant. Assessment/selection
BK Viral Infection and Malignancy in Renal Transplantation ~A Case History~
 BK Viral Infection and Malignancy in Renal Transplantation ~A Case History~ Mariko Toyoda, MD Department of Nephrology, Japanese Red Cross Kumamoto Hospital Statement of Disclosure The author does not
BK Viral Infection and Malignancy in Renal Transplantation ~A Case History~ Mariko Toyoda, MD Department of Nephrology, Japanese Red Cross Kumamoto Hospital Statement of Disclosure The author does not
No evidence of C4d association with AMR However, C3d and AMR correlated well
 C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Long-term prognosis of BK virus-associated nephropathy in kidney transplant recipients
 Original Article Kidney Res Clin Pract 37:167-173, 2018(2) pissn: 2211-9132 eissn: 2211-9140 https://doi.org/10.23876/j.krcp.2018.37.2.167 KIDNEY RESEARCH AND CLINICAL PRACTICE Long-term prognosis of BK
Original Article Kidney Res Clin Pract 37:167-173, 2018(2) pissn: 2211-9132 eissn: 2211-9140 https://doi.org/10.23876/j.krcp.2018.37.2.167 KIDNEY RESEARCH AND CLINICAL PRACTICE Long-term prognosis of BK
Immunopathology of T cell mediated rejection
 Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Certified Clinical Transplant Nurse (CCTN) * Detailed Content Outline
 * Detailed Content Outline") I. PRETRANSPLANTATION CARE 9 11 3 23 A. Evaluate End-Stage Organ Failure 1 1 1 3 1. History and physical assessment 2. Vital signs and / or hemodynamic parameters 3. Lab values 4. Diagnostic tests B. Monitor
I. PRETRANSPLANTATION CARE 9 11 3 23 A. Evaluate End-Stage Organ Failure 1 1 1 3 1. History and physical assessment 2. Vital signs and / or hemodynamic parameters 3. Lab values 4. Diagnostic tests B. Monitor
A Tolerance Approach to the Transplantation of Vascularized Tissues
 A Tolerance Approach to the Transplantation of Vascularized Tissues The 9th New Jersey Symposium on Biomaterials Science and Regenerative Medicine October 29-31, 2008 David H. Sachs, M.D. Harvard Medical
A Tolerance Approach to the Transplantation of Vascularized Tissues The 9th New Jersey Symposium on Biomaterials Science and Regenerative Medicine October 29-31, 2008 David H. Sachs, M.D. Harvard Medical
Green Light to Transplant: A Stepwise Approach
 Green Light to Transplant: A Stepwise Approach Andrea O Shaughnessy RN, BSN, PGDip. ICU/ER, Transplant Coordinator Vancouver General Hospital Sharon Duncan BA, RN, BSN, Patient Services/Transplant Coordinator/Educator
Green Light to Transplant: A Stepwise Approach Andrea O Shaughnessy RN, BSN, PGDip. ICU/ER, Transplant Coordinator Vancouver General Hospital Sharon Duncan BA, RN, BSN, Patient Services/Transplant Coordinator/Educator
Glossary. Anesthesiologist A doctor who puts you or parts of your body to sleep during surgery.
 1-Glossary Glossary Acute rejection A type of rejection that occurs when immune cells from your body attack the transplanted organ(s). Acute rejection may occur at any time after a transplant. But it usually
1-Glossary Glossary Acute rejection A type of rejection that occurs when immune cells from your body attack the transplanted organ(s). Acute rejection may occur at any time after a transplant. But it usually
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
NHS RightCare scenario: The variation between standard and optimal pathways
 NHS RightCare scenario: The variation between standard and optimal pathways Abdul s story: Progressive Chronic Kidney Disease Appendix 2: Short summary slide pack January 2018 Abdul and the sub-optimal
NHS RightCare scenario: The variation between standard and optimal pathways Abdul s story: Progressive Chronic Kidney Disease Appendix 2: Short summary slide pack January 2018 Abdul and the sub-optimal
Update on Kidney Allocation
 Update on Kidney Allocation 23rd Annual Conference Association for Multicultural Affairs in Transplantation Silas P. Norman, M.D., M.P.H. Associate Professor Division of Nephrology September 23, 2015 Disclosures
Update on Kidney Allocation 23rd Annual Conference Association for Multicultural Affairs in Transplantation Silas P. Norman, M.D., M.P.H. Associate Professor Division of Nephrology September 23, 2015 Disclosures
Should Pediatric Patients Wait for HLA-DR-Matched Renal Transplants?
 American Journal of Transplantation 2008; 8: 2056 2061 Wiley Periodicals Inc. C 2008 The Authors Journal compilation C 2008 The American Society of Transplantation and the American Society of Transplant
American Journal of Transplantation 2008; 8: 2056 2061 Wiley Periodicals Inc. C 2008 The Authors Journal compilation C 2008 The American Society of Transplantation and the American Society of Transplant
Surgery in the renal transplant patient
 Surgery in the renal transplant patient Prevalence of renal transplants in Australia Prevalence according to State/Territory Overall patient and graft survival following renal transplantation: short term
Surgery in the renal transplant patient Prevalence of renal transplants in Australia Prevalence according to State/Territory Overall patient and graft survival following renal transplantation: short term
Recognition and Treatment of Chronic Allograft Dysfunction
 Recognition and Treatment of Chronic Allograft Dysfunction Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs
Recognition and Treatment of Chronic Allograft Dysfunction Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs
Risk Factors in Long Term Immunosuppressive Use and Advagraf. Daniel Serón Nephrology department Hospital Universitari Vall d Hebron
 Risk Factors in Long Term Immunosuppressive Use and Advagraf Daniel Serón Nephrology department Hospital Universitari Vall d Hebron Progressive well defined diseases ABMR GN Polyoma Non-specific Findings
Risk Factors in Long Term Immunosuppressive Use and Advagraf Daniel Serón Nephrology department Hospital Universitari Vall d Hebron Progressive well defined diseases ABMR GN Polyoma Non-specific Findings
Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification
 Banff 1 Banff Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification Department of Nephrology, Japanese Red Cross Nagoya Daini Hospital Morozumi Kunio,
Banff 1 Banff Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification Department of Nephrology, Japanese Red Cross Nagoya Daini Hospital Morozumi Kunio,
BK virus infection in renal transplant recipients: single centre experience. Dr Wong Lok Yan Ivy
 BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
Organ Procurement and Transplantation Network
 OPTN Organ Procurement and Transplantation Network POLICIES This document provides the policy language approved by the OPTN/UNOS Board at its meeting in June 2015 as part of the Operations and Safety Committee
OPTN Organ Procurement and Transplantation Network POLICIES This document provides the policy language approved by the OPTN/UNOS Board at its meeting in June 2015 as part of the Operations and Safety Committee
Kidney Transplantation
 Kidney Transplantation Current Kidney Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr Current Kidney
Kidney Transplantation Current Kidney Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr Current Kidney
Patient Education Transplant Services. Glossary of Terms. For a kidney/pancreas transplant
 Patient Education Glossary of Terms For a kidney/pancreas transplant Glossary of Terms Page 18-2 Antibody A protein substance made by the body s immune system in response to a foreign substance. Antibodies
Patient Education Glossary of Terms For a kidney/pancreas transplant Glossary of Terms Page 18-2 Antibody A protein substance made by the body s immune system in response to a foreign substance. Antibodies
Solid Organ Transplantation 1. Chapter 55. Solid Organ Transplant, Self-Assessment Questions
 Solid Organ Transplantation 1 Chapter 55. Solid Organ Transplant, Self-Assessment Questions Questions 1 to 9 are related to the following case: A 38-year-old white man is scheduled to receive a living-unrelated
Solid Organ Transplantation 1 Chapter 55. Solid Organ Transplant, Self-Assessment Questions Questions 1 to 9 are related to the following case: A 38-year-old white man is scheduled to receive a living-unrelated
Expanded Criteria Recipients: Are there any Limits
 Expanded Criteria Recipients: Are there any Limits Andreas Paul, MD, MSc, FRCS Department of General-, Visceral- and Transplant Surgery, University Hospital Essen Ruhr Area 5.200 000 inhabitants University
Expanded Criteria Recipients: Are there any Limits Andreas Paul, MD, MSc, FRCS Department of General-, Visceral- and Transplant Surgery, University Hospital Essen Ruhr Area 5.200 000 inhabitants University
Case Study: Pediatric Kidney Transplantation Tom Blydt-Hansen, MD
 2017 CST-Astellas Canadian Transplant Fellows Symposium Case Study: Pediatric Kidney Transplantation Tom Blydt-Hansen, MD Dr. Tom Blydt-Hansen received his Medicinæ Doctorem et Chirurgiæ Magistrum from
2017 CST-Astellas Canadian Transplant Fellows Symposium Case Study: Pediatric Kidney Transplantation Tom Blydt-Hansen, MD Dr. Tom Blydt-Hansen received his Medicinæ Doctorem et Chirurgiæ Magistrum from
Literature Review: Transplantation July 2010-June 2011
 Literature Review: Transplantation July 2010-June 2011 James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Kidney Transplant Top 10 List: July Kidney
Literature Review: Transplantation July 2010-June 2011 James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Kidney Transplant Top 10 List: July Kidney
DE-MYSTIFYING THE BLACK BOX OF TRANSPLANT IMMUNOLOGY
 2016 DE-MYSTIFYING THE BLACK BOX OF TRANSPLANT IMMUNOLOGY James H Lan, MD, FRCP(C), D(ABHI) Clinical Assistant Professor, University of British Columbia Nephrology & Kidney Transplantation, Vancouver General
2016 DE-MYSTIFYING THE BLACK BOX OF TRANSPLANT IMMUNOLOGY James H Lan, MD, FRCP(C), D(ABHI) Clinical Assistant Professor, University of British Columbia Nephrology & Kidney Transplantation, Vancouver General
By the way, I have a transplant..
 By the way, I have a transplant.. Transplant patient for non-transplant surgery David Elliott No relevant disclosures Organ donation in Australia - 2017 Survival rates following organ donation have increased
By the way, I have a transplant.. Transplant patient for non-transplant surgery David Elliott No relevant disclosures Organ donation in Australia - 2017 Survival rates following organ donation have increased
The New Kidney Allocation System (KAS) Frequently Asked Questions
 Frequently Asked Questions") The New Kidney Allocation System (KAS) Frequently Asked Questions Contents General: The Need for the New System and Key Implementation Details... 4 Why was the newly revised KAS necessary?... 4 What were
The New Kidney Allocation System (KAS) Frequently Asked Questions Contents General: The Need for the New System and Key Implementation Details... 4 Why was the newly revised KAS necessary?... 4 What were
Caring for the AKI Survivor: What is Required?
 Caring for the AKI Survivor: What is Required? Ron Wald, MDCM MPH FRCPC Division of Nephrology St. Michael s Hospital and University of Toronto February 28, 2019 A patient in your ICU 65M with DM, HTN,
Caring for the AKI Survivor: What is Required? Ron Wald, MDCM MPH FRCPC Division of Nephrology St. Michael s Hospital and University of Toronto February 28, 2019 A patient in your ICU 65M with DM, HTN,
Thanks to our Speakers!
 Thanks to our Speakers! Fizza Naqvi, MD Assistant Professor at the Department of Medicine (Nephrology), Johns Hopkins Attending physician at Johns Hopkins hospital. Involved with kidney recipient evaluation
Thanks to our Speakers! Fizza Naqvi, MD Assistant Professor at the Department of Medicine (Nephrology), Johns Hopkins Attending physician at Johns Hopkins hospital. Involved with kidney recipient evaluation
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Keeping your options open. Transplant In Center Hemodialysis Home Hemodialysis Peritoneal dialysis No dialysis
 Keeping your options open Transplant In Center Hemodialysis Home Hemodialysis Peritoneal dialysis No dialysis Survival With/Without Transplant % of Transplants 45% 40% 35% 30% 25% 20% 15% 10% 5% 0% Recipient
Keeping your options open Transplant In Center Hemodialysis Home Hemodialysis Peritoneal dialysis No dialysis Survival With/Without Transplant % of Transplants 45% 40% 35% 30% 25% 20% 15% 10% 5% 0% Recipient
2017 CST-Astellas Canadian Transplant Fellows Symposium. Management of Renal Dysfunction in Extra Renal Transplants
 2017 CST-Astellas Canadian Transplant Fellows Symposium Management of Renal Dysfunction in Extra Renal Transplants Jeffrey Schiff, MD Dr. Jeffrey Schiff is an Assistant Professor of Medicine at the University
2017 CST-Astellas Canadian Transplant Fellows Symposium Management of Renal Dysfunction in Extra Renal Transplants Jeffrey Schiff, MD Dr. Jeffrey Schiff is an Assistant Professor of Medicine at the University
Risk factors for DVT. Venous thrombosis & pulmonary embolism. Anticoagulation (cont d) Diagnosis 1/5/2018. Ahmed Mahmoud, MD
 Diagnosis 1/5/2018. Ahmed Mahmoud, MD") Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism. Ahmed Mahmoud, MD
 Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Who and When to Refer for a Heart Transplant
 Who and When to Refer for a Heart Transplant Dr Jayan Parameshwar Consultant Cardiologist Papworth Hospital BSH 24 th November 2017 BSH Annual Autumn Meeting 2017 Presentation title: Who and when to refer
Who and When to Refer for a Heart Transplant Dr Jayan Parameshwar Consultant Cardiologist Papworth Hospital BSH 24 th November 2017 BSH Annual Autumn Meeting 2017 Presentation title: Who and when to refer