S Nachiappan, A Askari, A Currie, RH Kennedy, O Faiz. 30 th June 2014 Tripartite Colorectal Meeting, Birmingham, UK
|
|
|
- Giles Parrish
- 6 years ago
- Views:
Transcription

1 S Nachiappan, A Askari, A Currie, RH Kennedy, O Faiz 30 th June 2014 Tripartite Colorectal Meeting, Birmingham, UK



2 local recurrence in rectal cancer Long-term cancer specific survival 16% died within 30 days Long-term cancer specific survival 4.5% of elective colorectal surgery underwent a reoperation within 28 days Reoperation often for postop bleeding & anastomotic leaks

3 To detect a possible anastomotic complication during the operation itself & allow remedial action To prevent a postoperative leak or complication To prevent a reoperation To minimise patient morbidity and mortality
4 Ensure Luminal Patency No Mechanical Disruption Anastomotic Integrity No Ischaemia No Bleeding



5 Surgical anastomosis Intraoperative period Anastomotic integrity Colo-colonic Anastomosis Colorectal anastomosis Rectal anastomosis Ileorectal anastomosis Intraoperative care Peroperative procedure Intraoperative Peroperative Integrity Leak Dehiscence Perfusion Ischaemia Bleeding *Latest search performed on 12 th June 2013
6 Inclusion Exclusion RCTs Animal studies Non-randomised comparative studies Case series Case reports/technical tips Unclear postoperative outcomes

7 Clinical Radiological Symptomatic Asymptomatic May have had radiological imaging subsequently Reoperation, Drainage or conservative Mx Radiological imaging planned/routine eg. GG Enema at 8 weeks/prior to reversal
8 37 studies Basic mechanical patency tests (Air/fluid leak) 13 Endoscopic visualisation techniques (intra-op colonoscopy + leak test) 10 Microperfusion techniques Case series 1 Nonrandomised study 2 RCT 5 Case series 5 Nonrandomised studies 11 Case series 2 Nonrandomised studies 1 RCT
 n = 816 Negative IOT 726 47 POL 679 No POL (26CL, 21RL) Total Leak (CL+RL) rate Clinical Leak rate Positive IOT Negative IOT 13/90 47/726 14.4% 6.5% 7/90 26/726 7.7% 3.")
9 Basic Mechanical Patency Tests Case series (10) Intraoperative * With intraoperative rectifications 61 sutured only 20 sutured & defunctioned 4 redone 5 defunctioned only Postoperative Positive IOT* POL 77 No POL (7CL, 6RL) n = 816 Negative IOT POL 679 No POL (26CL, 21RL) Total Leak (CL+RL) rate Clinical Leak rate Positive IOT Negative IOT 13/90 47/ % 6.5% 7/90 26/ % 3.5% IOT: Intraoperative test POL: Postoperative leak CL: Clinical leak RL: Radiological leak
10 Basic Mechanical Patency Tests Nonrandomised study (1) n = 998 Intraoperative IOT group 825 Control group 173 Intraoperative Positive IOT* 65 Negative IOT 760 * With intraoperative rectifications 41 sutured 10 sutured & defunctioned 14 redone Postoperative 5 POL # # All sutured 29 POL 14 POL Total (Clinical) Leak rate Tested Non-tested/Control 34/825 14/ % 8.1% IOT: Intraoperative test POL: Postoperative leak
 9 POL (3CL, 6RL) 27 POL (16CL, 11RL) Total Leak rate Clinical Leak rate Tested Non-tested/Control 14/103 27/100 13.6% 27.0% 6/103 16/100 5.")
11 Basic Mechanical Patency Tests RCTs (2) n = 203 Intraoperative IOT group 103 Control group 100 Intraoperative Positive IOT* 25 Negative IOT 78 * With intraoperative rectifications 25 sutured Postoperative 5 POL (3CL, 2RL) 9 POL (3CL, 6RL) 27 POL (16CL, 11RL) Total Leak rate Clinical Leak rate Tested Non-tested/Control 14/103 27/ % 27.0% 6/103 16/ % 16% IOT: Intraoperative test POL: Postoperative leak CL: Clinical leak RL: Radiological leak
12 37 studies Basic mechanical patency tests (Air/fluid leak) 13 Endoscopic visualisation techniques (intra-op colonoscopy + leak test) 10 Microperfusion techniques Case series 1 Nonrandomised study 2 RCT 5 Case series 5 Nonrandomised studies 11 Case series 2 Nonrandomised studies 1 RCT
13 Endoscopic visualisation (Intraoperative colonoscopy) Intraoperative Case series (5) n = 713 With intraoperative rectifications 10 suturing only 14 haemostasis 20 redone 2 defunctioned only 11 unknown Postoperative Positive IOT* POAC (6CL, 1staple line bleed, 1 pelvic collection, 4 ileus) 45 No POAC Negative IOT POAC 649 No POAC (7CL) Positive IOT Negative IOT POAC rate Clinical leak rate 12/57 7/ % 1.1% 6/57 7/ % 1.1% IOT: Intraoperative test POAC: Postoperative anast complication CL: Clinical leak RL: Radiological leak
 (28 CL) (17 CL) Tested")
14 Endoscopic visualisation (Intraoperative colonoscopy) Nonrandomised studies (5) n = 950 IOT group Control group Intraoperative With intraoperative rectifications 26 sutured 8 haemostasis 1 redone 5 sutured/haemostasis & defunctioned 30 defunctioned Positive IOT* 70 (56 air leaks, 14 staple line bleeds Negative IOT POAC 32 POAC 26 POAC Postoperative (7 CLs) (28 CL) (17 CL) Tested Non-tested/Control POAC rate Clinical leak rate 39/509 26/ % 5.9% 35/509 17/ % 3.9% IOT: Intraoperative test POAC Postoperative anast complication
15 37 studies Basic mechanical patency tests (Air/fluid leak) 13 Endoscopic visualisation techniques (intra-op colonoscopy + leak test) 10 Microperfusion techniques Case series 1 Nonrandomised study 2 RCT 5 Case series 5 Nonrandomised studies 11 Case series 2 Nonrandomised studies 1 RCT
16
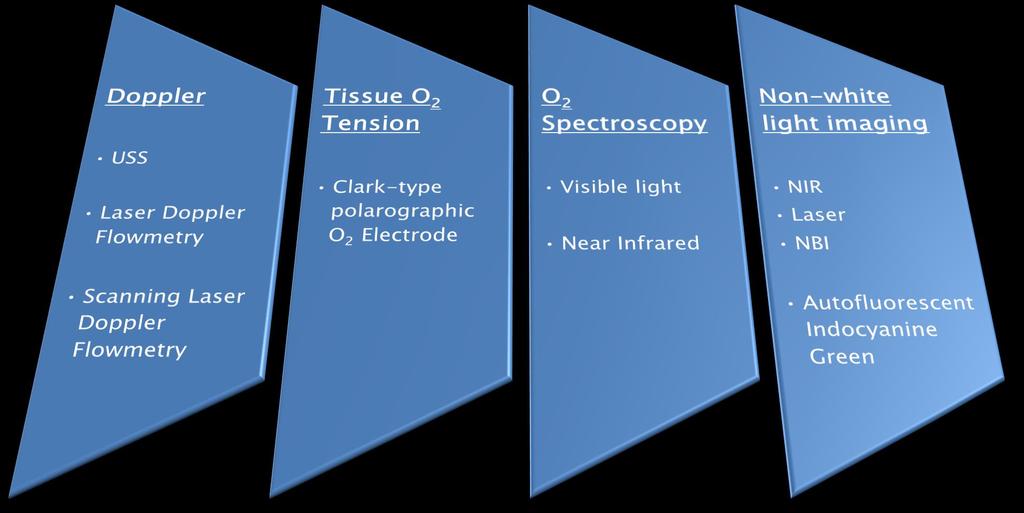
17 First Author Year Perfusion assessment technique Testing Access Study design N (Operative access) Ambrosetti 1994 Doppler USS Open CS 194 Hallbook 1996 LDF Open CS 30 Vignali 2000 LDF Open CS 55 Seike 2007 LDF Open CS 86 Boyle 2000 SLDF Open CS 10 Sheridan 1987 Tissue Oxygen Tension Open CS 50 Hall 1995 Tissue Oxygen Tension Open CS 62 Karliczek 2010 Visible Light O2 Spectroscopy Open CS 77 Hirano 2006 Near Infrared O2 Spectroscopy Open & lap CS 20 Parmeggiani 2012 IOC with Narrow Band Imaging Transanal RCT 47 (27 vs 20) Kudszus 2010 Laser Fluorescence ICG Open & lap Case-Control 402 (201vs 201) Jafari 2013 NIR ICG Robotics Case-Control 38 (16 vs 22) Sherwinter 2012 NIR ICG Transanal CS 7 Sherwinter 2013 NIR ICG + ALT Transanal CS 20 LDF = Laser Doppler Flowmetry SLDF = Scanning LDF NIR = Near Infrared ICG = Indocyanine green ALT = Air leak test

 Jafari 2013 NIR ICG Robotics Case-Control 38 (16 vs 22) Sherwinter 2012 NIR ICG Transanal CS 7 Sherwinter 2013 NIR ICG + ALT Transanal CS 20 LDF = Laser Doppler Flowmetry SLDF = Scanning")
18 First Author Year Perfusion assessment technique Testing Access Study design N (Operative access) Ambrosetti 1994 Doppler USS Open CS 194 Hallbook 1996 LDF Open CS 30 Vignali 2000 LDF Open CS 55 Seike 2007 LDF Open CS 86 Boyle 2000 SLDF Open CS 10 Sheridan 1987 Tissue Oxygen Tension Open CS 50 Hall 1995 Tissue Oxygen Tension Open CS 62 Karliczek 2010 Visible Light O2 Spectroscopy Open CS 77 Hirano 2006 Near Infrared O2 Spectroscopy Open & lap CS 20 Parmeggiani 2012 IOC with Narrow Band Imaging Transanal RCT 47 (27 vs 20) Kudszus 2010 Laser Fluorescence ICG Open & lap Case-Control 402 (201vs 201) Jafari 2013 NIR ICG Robotics Case-Control 38 (16 vs 22) Sherwinter 2012 NIR ICG Transanal CS 7 Sherwinter 2013 NIR ICG + ALT Transanal CS 20 LDF = Laser Doppler Flowmetry SLDF = Scanning LDF NIR = Near Infrared ICG = Indocyanine green ALT = Air leak test

19 First Author Year Perfusion assessment technique Testing Access Study design N (Operative access) Ambrosetti 1994 Doppler USS Open CS 194 Hallbook 1996 LDF Open CS 30 Vignali 2000 LDF Open CS 55 Seike 2007 LDF Open CS 86 Boyle 2000 SLDF Open CS 10 Sheridan 1987 Tissue Oxygen Tension Open CS 50 Hall 1995 Tissue Oxygen Tension Open CS 62 Karliczek 2010 Visible Light O2 Spectroscopy Open CS 77 Hirano 2006 Near Infrared O2 Spectroscopy Open & lap CS 20 Parmeggiani 2012 IOC with Narrow Band Imaging Transanal RCT 47 (27 vs 20) Kudszus 2010 Laser Fluorescence ICG Open & lap Case-Control 402 (201vs 201) Jafari 2013 NIR ICG Robotics Case-Control 38 (16 vs 22) Sherwinter 2012 NIR ICG Transanal CS 7 Sherwinter 2013 NIR ICG + ALT Transanal CS 20 LDF = Laser Doppler Flowmetry SLDF = Scanning LDF NIR = Near Infrared ICG = Indocyanine green ALT = Air leak test

20 First Author Year Perfusion assessment technique Testing Access Study design N (Operative access) Ambrosetti 1994 Doppler USS Open CS 194 Hallbook 1996 LDF Open CS 30 Vignali 2000 LDF Open CS 55 Seike 2007 LDF Open CS 86 Boyle 2000 SLDF Open CS 10 Sheridan 1987 Tissue Oxygen Tension Open CS 50 Hall 1995 Tissue Oxygen Tension Open CS 62 Karliczek 2010 Visible Light O2 Spectroscopy Open CS 77 Hirano 2006 Near Infrared O2 Spectroscopy Open & lap CS 20 Parmeggiani 2012 IOC with Narrow Band Imaging Transanal RCT 47 (27 vs 20) Kudszus 2010 Laser Fluorescence ICG Open & lap Case-Control 402 (201vs 201) Jafari 2013 NIR ICG Robotics Case-Control 38 (16 vs 22) Sherwinter 2012 NIR ICG Transanal CS 7 Sherwinter 2013 NIR ICG + ALT Transanal CS 20 LDF = Laser Doppler Flowmetry SLDF = Scanning LDF NIR = Near Infrared ICG = Indocyanine green ALT = Air leak test

 Jafari 2013 NIR ICG Robotics Case-Control 38 (16 vs 22) Sherwinter 2012 NIR ICG Transanal CS 7 Sherwinter 2013 NIR ICG + ALT Transanal CS 20 LDF = Laser Doppler Flowmetry SLDF = Scanning")
21 First Author Year Perfusion assessment technique Testing Access Study design N (Operative access) Ambrosetti 1994 Doppler USS Open CS 194 Hallbook 1996 LDF Open CS 30 Vignali 2000 LDF Open CS 55 Seike 2007 LDF Open CS 86 Boyle 2000 SLDF Open CS 10 Sheridan 1987 Tissue Oxygen Tension Open CS 50 Hall 1995 Tissue Oxygen Tension Open CS 62 Karliczek 2010 Visible Light O2 Spectroscopy Open CS 77 Hirano 2006 Near Infrared O2 Spectroscopy Open & lap CS 20 Parmeggiani 2012 IOC with Narrow Band Imaging Transanal RCT 47 (27 vs 20) Kudszus 2010 Laser Fluorescence ICG Open & lap Case-Control 402 (201vs 201) Jafari 2013 NIR ICG Robotics Case-Control 38 (16 vs 22) Sherwinter 2012 NIR ICG Transanal CS 7 Sherwinter 2013 NIR ICG + ALT Transanal CS 20 LDF = Laser Doppler Flowmetry SLDF = Scanning LDF NIR = Near Infrared ICG = Indocyanine green ALT = Air leak test
22 Basic mechanical patency testing (leak testing) is beneficial & reduces postoperative anastomotic leak rates A normal/negative intraoperative endoscopic visualisation test (intraoperative endoscopy) is associated with highly infrequent postoperative anastomotic complications Greater use of intraoperative endoscopy to assess anastomosis, may prevent/reduce rates of anastomotic dehiscence. Microperfusion assessment techniques are currently still experimental but hold potential for reducing anastomotic complications.
23 Academic Supervisors Mr Omar Faiz Professor Charles Vincent Surgical Consultants and colleagues
24 S Nachiappan, A Askari, A Currie, RH Kennedy, O Faiz 30 th June 2014 Tripartite Colorectal Meeting, Birmingham, UK
25 The decision to divert is dependent on several factors In the review Basic: CS = 5 out of 10 = 36 patients out of 150 patients Patient age/ comorbidities/ ability to withstand the sequelae of a leak NRCT = 0 out of 1 Elective/emergency setting RCT= 1 out of 2= 18 out of 143 patients Intraoperative parameters IOC: Height of anastomosis Possible adjuvant chemotherapy CS = Info not available in most NRCT = Info not available in most
26 I was not able to ascertain total numbers of defunctioning ileostomies made prior to intraoperative test. However what I noted was that patients who did have an ileostomy formed as a result of the IOT/rectification, Had no leak or had a attenuated effect from any subsequent leaks. The question I suppose would be whether we defunction anyone where we have concerns? But there is the morbidity of an ileostomy we need to take note of as well. So if we can target the specific patients who are at risk of a leak - and defunction them And avoid defunctioning those at minimal risk, that would be ideal. In this sense, intraoperative assessment of the anastomosis gives the surgeon more information at that point itself and allows an immediate rectification/action to be taken at the same sitting/operation
27 The older studies routinely bowel prepped the patients, especially for the left sided resections However, with the introduction of ERAS, this has reduced substantially. Of note studies: Cochrane review in 2011 noted no significant benefit of bowel prep. Selective use in rectal surgery may be beneficial, but no significant effect was found. For the purposes of this review. I did not look at bowel prep specifically KF Guenaga, D Matos Database Syst Rev, 2011
28 How was bleeding stopped? Endoluminally APC Transabdominally with sutures Li et al - Use of routine intraoperative endoscopy in elective laparoscopic colorectal surgery: can it further avoid anastomotic failure? Surg Endosc 2009 Routine IOE for patients undergoing elective laparoscopic colorectal surgery with distal anastomosis can detect abnormalities at or around the anastomosis. Although the RIOE group had fewer postoperative anastomotic complications, due to the small sample size, the 5.7-fold increase in anastomotic failure did not translate into significantly better postoperative outcomes than the SIOE group experienced. A larger-scale single or multicenter prospective randomized study or a metaanalysis including similar studies is necessary for further investigation of this issue.

29 Important point Currently: it is mostly subjective and comparisons are made with a control eg the caecum The fluorescence for example can be measured and this is an area which has been exploited by laser fluouresence and ICG technology Some authors have suggested subjective scoring systems too
Incidence and risk factors of anastomotic leaks. By: khaled Said Assistant professor of colorectal surgery Alexandria
 Incidence and risk factors of anastomotic leaks By: khaled Said Assistant professor of colorectal surgery Alexandria Anastomotic leakage after colorectal surgery is a major and potentially life-threatening
Incidence and risk factors of anastomotic leaks By: khaled Said Assistant professor of colorectal surgery Alexandria Anastomotic leakage after colorectal surgery is a major and potentially life-threatening
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Fluorescence Guided Surgery To Reduce Complications
 To Reduce Complications Luigi Boni, MD, FACS Associate Professor of Surgery Department of Surgery - IRCCS Policlinico Hospital University of Milan The Dream of a Surgeon Image Guided Surgery Basic Principles
To Reduce Complications Luigi Boni, MD, FACS Associate Professor of Surgery Department of Surgery - IRCCS Policlinico Hospital University of Milan The Dream of a Surgeon Image Guided Surgery Basic Principles
University of Groningen. Colorectal Anastomoses Bakker, Ilsalien
 University of Groningen Colorectal Anastomoses Bakker, Ilsalien IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
University of Groningen Colorectal Anastomoses Bakker, Ilsalien IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better!
 Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better! Francis Seow- Choen Medical Director Seow-Choen Colorectal Centre Singapore In all situations: We have to use the right tool for the job
Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better! Francis Seow- Choen Medical Director Seow-Choen Colorectal Centre Singapore In all situations: We have to use the right tool for the job
Anterior Resection for Rectal Cancer and Visceral
 692SJS0010.1177/1457496915593692Visceral blood flow after anterior resectionm. Rutegård, et al. Original Article Anterior Resection for Rectal Cancer and Visceral Blood Flow: An Explorative Study M. Rutegård
692SJS0010.1177/1457496915593692Visceral blood flow after anterior resectionm. Rutegård, et al. Original Article Anterior Resection for Rectal Cancer and Visceral Blood Flow: An Explorative Study M. Rutegård
DIVERTICULAR DISEASE. Dr. Irina Murray Casanova PGY IV
 DIVERTICULAR DISEASE Dr. Irina Murray Casanova PGY IV Diverticular Disease Colonoscopy Abdpelvic CT Scan Surgical Indications Overall, approximately 20% of patients with diverticulitis require surgical
DIVERTICULAR DISEASE Dr. Irina Murray Casanova PGY IV Diverticular Disease Colonoscopy Abdpelvic CT Scan Surgical Indications Overall, approximately 20% of patients with diverticulitis require surgical
Anastomotic Complications after Esophagectomy. Bryan Meyers, MD MPH Thoracic Surgery Washington University School of Medicine
 Anastomotic Complications after Esophagectomy Bryan Meyers, MD MPH Thoracic Surgery Washington University School of Medicine Use of Stomach as Conduit Simplest choice after esophagectomy Single anastomosis
Anastomotic Complications after Esophagectomy Bryan Meyers, MD MPH Thoracic Surgery Washington University School of Medicine Use of Stomach as Conduit Simplest choice after esophagectomy Single anastomosis
Yorihiko Muto, Hideaki Miyauchi, Gaku Ohira, Koichi Hayano. Kazuo Narushima, Kazufumi Suzuki and Hisahiro Matsubara. Abstract
 Chiba Medical J. 94E:25-31,2018 doi:10.20776s03035476-94e-3-p25 Original Article Evaluation of the anastomotic blood flow with near-infrared ICG fluorescence angiography with intraoperative transanal endoscopy
Chiba Medical J. 94E:25-31,2018 doi:10.20776s03035476-94e-3-p25 Original Article Evaluation of the anastomotic blood flow with near-infrared ICG fluorescence angiography with intraoperative transanal endoscopy
Innovations in Rectal Cancer Surgery
 Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
The Binational Colorectal Cancer Audit. A/Prof Paul McMurrick Head, Cabrini Monash University Dept of Surgery 2017
 The Binational Colorectal Cancer Audit A/Prof Paul McMurrick Head, Cabrini Monash University Dept of Surgery 2017 Binational Colorectal Cancer Database 2010 First Patient 2011 Contract between CMUDS and
The Binational Colorectal Cancer Audit A/Prof Paul McMurrick Head, Cabrini Monash University Dept of Surgery 2017 Binational Colorectal Cancer Database 2010 First Patient 2011 Contract between CMUDS and
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Innovations in rectal cancer surgery TAMIS and transanal TME
 Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings?
 Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings? Kate Willcutts, DCN, RD, CNSC University of Virginia Health System Charlottesville, VA kfw3w@virginia.edu Objectives 1. Discuss
Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings? Kate Willcutts, DCN, RD, CNSC University of Virginia Health System Charlottesville, VA kfw3w@virginia.edu Objectives 1. Discuss
Motility Disorders. Pelvic Floor. Colorectal Center for Functional Bowel Disorders (N = 701) January 2010 November 2011
 January 2010 November 2011") Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
State-of-the-art of surgery for resectable primary tumors
 Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Delayed anastomotic leakage following laparoscopic intersphincteric resection for lower rectal cancer: report of four cases and literature review
 Iwamoto et al. World Journal of Surgical Oncology (2017) 15:143 DOI 10.1186/s12957-017-1208-2 CASE REPORT Open Access Delayed anastomotic leakage following laparoscopic intersphincteric resection for lower
Iwamoto et al. World Journal of Surgical Oncology (2017) 15:143 DOI 10.1186/s12957-017-1208-2 CASE REPORT Open Access Delayed anastomotic leakage following laparoscopic intersphincteric resection for lower
Can Robotics be useful to a General Surgeon Performing Colorectal Surgery? Curtis L. Peery MD April 27 th 2018 Throckmorton Surgical Society
 Can Robotics be useful to a General Surgeon Performing Colorectal Surgery? Curtis L. Peery MD April 27 th 2018 Throckmorton Surgical Society 1.Intuitive Surgical 2.C-Sats 3.Virtual Incision Study comparing
Can Robotics be useful to a General Surgeon Performing Colorectal Surgery? Curtis L. Peery MD April 27 th 2018 Throckmorton Surgical Society 1.Intuitive Surgical 2.C-Sats 3.Virtual Incision Study comparing
Surgery for Ulcerative Colitis 11/14/10. Colectomy for Ulcerative Colitis: What your patient should know. Surgery for Ulcerative Colitis
 Colectomy for Ulcerative Colitis: What your patient should know Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Surgery for Ulcerative
Colectomy for Ulcerative Colitis: What your patient should know Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Surgery for Ulcerative
Acute Care Surgery: Diverticulitis
 Acute Care Surgery: Diverticulitis Madhulika G. Varma, MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment of Diverticular Disease Increasing
Acute Care Surgery: Diverticulitis Madhulika G. Varma, MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment of Diverticular Disease Increasing
LONG TERM OUTCOME OF ELECTIVE SURGERY
 LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic Surgery for Colorectal Disease
 ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2018;21(1):38-42 Journal of Minimally Invasive Surgery Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic
ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2018;21(1):38-42 Journal of Minimally Invasive Surgery Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic
SMJ Singapore Medical Journal
 SMJ Singapore Medical Journal ONLINE FIRST PUBLICATION Online first papers have undergone full scientific review and copyediting, but have not been typeset or proofread. To cite this article, use the DOIs
SMJ Singapore Medical Journal ONLINE FIRST PUBLICATION Online first papers have undergone full scientific review and copyediting, but have not been typeset or proofread. To cite this article, use the DOIs
Citation for published version (APA): Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects
: Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects") UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
Hester Cheung Memorial Lecture
 Hester Cheung Memorial Lecture STEVEN D WEXNER, MD, PHD (HON),FACS, FRCS, FRCS(ED) Director, Digestive Disease Center; Chairman, Department of Colorectal Surgery; Cleveland Clinic Florida Professor of
Hester Cheung Memorial Lecture STEVEN D WEXNER, MD, PHD (HON),FACS, FRCS, FRCS(ED) Director, Digestive Disease Center; Chairman, Department of Colorectal Surgery; Cleveland Clinic Florida Professor of
Rectal Cancer. About the Colon and Rectum. Symptoms. Colorectal Cancer Screening
 Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Karen Lok Man Tung, Michael Ka Wah Li. Introduction
 Original Article Page 1 of 5 Hybrid natural orifice transluminal endoscopic surgery colectomy versus conventional laparoscopic colectomy for left-sided colonic tumors: intermediate follow up of a randomized
Original Article Page 1 of 5 Hybrid natural orifice transluminal endoscopic surgery colectomy versus conventional laparoscopic colectomy for left-sided colonic tumors: intermediate follow up of a randomized
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT. Simon Radley Consultant Surgeon March 2013
 DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
ENHANCED RECOVERY AFTER SURGERY (ERAS) PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY
 PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY") Department of Surgery Divison of General Surgery ENHANCED RECOVERY AFTER SURGERY (ERAS) PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY December 2016 Disclosure Paresh
Department of Surgery Divison of General Surgery ENHANCED RECOVERY AFTER SURGERY (ERAS) PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY December 2016 Disclosure Paresh
Management of colorectal anastomotic leakage: differences between salvage and anastomotic takedown
 The American Journal of Surgery (2012) 204, 671 676 Clinical Science Management of colorectal anastomotic leakage: differences between salvage and anastomotic takedown Domenico Fraccalvieri, M.D., Sebastiano
The American Journal of Surgery (2012) 204, 671 676 Clinical Science Management of colorectal anastomotic leakage: differences between salvage and anastomotic takedown Domenico Fraccalvieri, M.D., Sebastiano
Stapled transanal rectal resection for obstructed defaecation syndrome
 Stapled transanal rectal resection for obstructed Issued: June 2010 www.nice.org.uk/ipg351 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
Stapled transanal rectal resection for obstructed Issued: June 2010 www.nice.org.uk/ipg351 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
COLORECTAL CANCER COMPARATIVE AUDIT REPORT SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT. Mr B.J. Mander SCAN Group Chair
 SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT COLORECTAL CANCER 2013-2014 COMPARATIVE AUDIT REPORT Mr B.J. Mander SCAN Group Chair Mr K Pal, NHS Borders Mr S Whitelaw, NHS Dumfries & Galloway
SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT COLORECTAL CANCER 2013-2014 COMPARATIVE AUDIT REPORT Mr B.J. Mander SCAN Group Chair Mr K Pal, NHS Borders Mr S Whitelaw, NHS Dumfries & Galloway
Colorectal Surgery in the Elderly. Stephen Smith
 Colorectal Surgery in the Elderly Stephen Smith Scope WHO >65 Social definition No COI Age specific incidence of CRC in Australia 2016 (new cases/100,000) My data: elective bowel resections
Colorectal Surgery in the Elderly Stephen Smith Scope WHO >65 Social definition No COI Age specific incidence of CRC in Australia 2016 (new cases/100,000) My data: elective bowel resections
Is using peritoneal drains in bowel surgeries beneficial?
 International Surgery Journal Bhoir LN et al. Int Surg J. 17 Feb;4():- http://www.ijsurgery.com pissn 349-33 eissn 349-9 Original Research Article DOI: http://dx.doi.org/.13/349-9.isj17 Is using peritoneal
International Surgery Journal Bhoir LN et al. Int Surg J. 17 Feb;4():- http://www.ijsurgery.com pissn 349-33 eissn 349-9 Original Research Article DOI: http://dx.doi.org/.13/349-9.isj17 Is using peritoneal
Prof. Dr. Ahmed ElGeidie Professor of General surgery GEC Dr. Ahmed Abdelrafee
 Prof. Dr. Ahmed ElGeidie Professor of General surgery GEC Dr. Ahmed Abdelrafee Diverticulosis of the colon is the presence of pockets in the wall of the colon called diverticula which may, or may not,
Prof. Dr. Ahmed ElGeidie Professor of General surgery GEC Dr. Ahmed Abdelrafee Diverticulosis of the colon is the presence of pockets in the wall of the colon called diverticula which may, or may not,
Case discussion. Anastomotic leakage. intern superviser
 Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Posterior Deep Endometriosis. What is the best approach? Posterior Deep Endometriosis. Should we perform a routine excision of the vagina??
 Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst Polyclinique Hotel Dieu CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix -Rectum
Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst Polyclinique Hotel Dieu CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix -Rectum
The management and outcome of anastomotic leaks in colorectal surgery
 Original article doi:10.1111/j.1463-1318.2007.01417.x The management and outcome of anastomotic leaks in colorectal surgery A. A. Khan*, J. M. D. Wheeler, C. Cunningham, B. George, M. Kettlewell and N.
Original article doi:10.1111/j.1463-1318.2007.01417.x The management and outcome of anastomotic leaks in colorectal surgery A. A. Khan*, J. M. D. Wheeler, C. Cunningham, B. George, M. Kettlewell and N.
UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication
 Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication") UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication Citation for published version (APA): van Koperen, P. J. (2010). Surgical
UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication Citation for published version (APA): van Koperen, P. J. (2010). Surgical
Disclosures. Personalized Approaches to Gastrointestinal Cancers. Objectives. What is personalized cancer care. Go through some genomic studies
 Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
Acute Diverticulitis. Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh
 Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Bile Duct Injury during Lap Chole. Bile Duct Injury during cholecystectomy TOPICS. 1. Prevalence, mechanisms, prevention and diagnosis
 Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Fluid Balance in an Enhanced Recovery Pathway. Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017
 Fluid Balance in an Enhanced Recovery Pathway Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017 No Disclosures 2 Introduction The optimal intravenous fluid regimen
Fluid Balance in an Enhanced Recovery Pathway Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017 No Disclosures 2 Introduction The optimal intravenous fluid regimen
Clinical Study Laparoscopic versus Open Surgery for Colorectal Cancer: A Retrospective Analysis of 163 Patients in a Single Institution
 Minimally Invasive Surgery, Article ID 530314, 6 pages http://dx.doi.org/10.1155/2014/530314 Clinical Study Laparoscopic versus Open Surgery for Colorectal Cancer: A Retrospective Analysis of 163 Patients
Minimally Invasive Surgery, Article ID 530314, 6 pages http://dx.doi.org/10.1155/2014/530314 Clinical Study Laparoscopic versus Open Surgery for Colorectal Cancer: A Retrospective Analysis of 163 Patients
Henrique Prata Director General
 PROGRAM ADVANCED COURSE IIN COLORECTAL SURGERY SEPTEMBER 12 TT HH TO 14 TT HH,, 2019 CHAIRMAN Henrique Prata Director General Hospital de Amor - Barretos PRESIDENT DIRECTOR COURSE DIRECTOR Jacques Marescaux
PROGRAM ADVANCED COURSE IIN COLORECTAL SURGERY SEPTEMBER 12 TT HH TO 14 TT HH,, 2019 CHAIRMAN Henrique Prata Director General Hospital de Amor - Barretos PRESIDENT DIRECTOR COURSE DIRECTOR Jacques Marescaux
Laparoscopic Bladder-Preserving Surgery for Enterovesical Fistula Complicated with Benign Gastrointestinal Disease
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES. Devon Paula Richardson
 NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
Fast Track Surgery at the University Teaching Hospital of Kigali: A Randomized Controlled Trial Study in Abdominal Surgery
 12 Fast Track Surgery at the University Teaching Hospital of Kigali: A Randomized Controlled Trial Study in Abdominal Surgery L Ndayizeye, A K Kiswezi University Teaching Hospital of Butare, Rwanda. Correspondence
12 Fast Track Surgery at the University Teaching Hospital of Kigali: A Randomized Controlled Trial Study in Abdominal Surgery L Ndayizeye, A K Kiswezi University Teaching Hospital of Butare, Rwanda. Correspondence
COLORECTAL SURGERY. Solutions for minimally invasive colorectal surgery
 COLORECTAL SURGERY Solutions for minimally invasive colorectal surgery The da Vinci Surgical System High-definition 3D vision One Stapler 45 Skills Simulator instrumentation Firefly Fluorescence Imaging
COLORECTAL SURGERY Solutions for minimally invasive colorectal surgery The da Vinci Surgical System High-definition 3D vision One Stapler 45 Skills Simulator instrumentation Firefly Fluorescence Imaging
Short and longterm outcomes after endoscopic resection of malignant polyps.
 Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN
 LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN MCQ A 78 yr. old man (HT, DM, 2 coronary stents) has 3 mos. of irregular bowel habits and 72 hrs. of LBO. Distended, non-tender. Normal blood work. Plain xray,
LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN MCQ A 78 yr. old man (HT, DM, 2 coronary stents) has 3 mos. of irregular bowel habits and 72 hrs. of LBO. Distended, non-tender. Normal blood work. Plain xray,
Feasibility of Emergency Laparoscopic Reoperations for Complications after Laparoscopic Surgery for Colorectal Cancer
 ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2018;21(2):70-74 Journal of Minimally Invasive Surgery Feasibility of Emergency Laparoscopic Reoperations for Complications after
ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2018;21(2):70-74 Journal of Minimally Invasive Surgery Feasibility of Emergency Laparoscopic Reoperations for Complications after
Teamwork radiology and surgery
 Catchment area Teamwork radiology and surgery Jigsaw TRAUMA Cholecystitis Perforation Appendicitis OP X-ray Abdominal wall Endoscopy GI bleeding Diverticulitis Pancreatitis Ileus Complex and timeconsuming
Catchment area Teamwork radiology and surgery Jigsaw TRAUMA Cholecystitis Perforation Appendicitis OP X-ray Abdominal wall Endoscopy GI bleeding Diverticulitis Pancreatitis Ileus Complex and timeconsuming
The effect of laxative use in length of hospital stay and complication rate in patients undergoing elective colorectal surgery within an ERAS setting.
 The effect of laxative use in length of hospital stay and complication rate in patients undergoing elective colorectal surgery within an ERAS setting. { Thalia Petropoulou, Clinical Fellow Paul Hainsworth,Colorectal
The effect of laxative use in length of hospital stay and complication rate in patients undergoing elective colorectal surgery within an ERAS setting. { Thalia Petropoulou, Clinical Fellow Paul Hainsworth,Colorectal
Intraoperative contrast-enhanced sonography of bowel blood flow: preliminary experience
 Title Intraoperative contrast-enhanced sonography of bowel blood flow: preliminary experience Author(s) Swift, AJ; Parker, P; Chiu, WHK; Hunter, IA; Hartley, JE; Byass, OR Citation Journal of Ultrasound
Title Intraoperative contrast-enhanced sonography of bowel blood flow: preliminary experience Author(s) Swift, AJ; Parker, P; Chiu, WHK; Hunter, IA; Hartley, JE; Byass, OR Citation Journal of Ultrasound
Audit Report. Colorectal Cancer Quality Performance Indicators. Patients diagnosed April 2016 March Published: March 2018
 Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2016 March 2017 Published: March 2018 Mr Michael Walker NOSCAN MCN Clinical
Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2016 March 2017 Published: March 2018 Mr Michael Walker NOSCAN MCN Clinical
Perforated diverticulitis: Washout it s happening
 Perforated diverticulitis: Washout it s happening or maybe not! Ori D. Rotstein, M.D. Department of Surgery St. Michael s Hospital University of Toronto 62 year old male 24 hour history of LLQ pain Now-
Perforated diverticulitis: Washout it s happening or maybe not! Ori D. Rotstein, M.D. Department of Surgery St. Michael s Hospital University of Toronto 62 year old male 24 hour history of LLQ pain Now-
Disclosures. I am a paid consultant for:
 Surgical Sub-specialization: Colorectal Specialist Peter W. Marcello, M.D. Vice Chairman, Department of Colon & Rectal Surgery Lahey Clinic Burlington, Massachusetts Disclosures I am a paid consultant
Surgical Sub-specialization: Colorectal Specialist Peter W. Marcello, M.D. Vice Chairman, Department of Colon & Rectal Surgery Lahey Clinic Burlington, Massachusetts Disclosures I am a paid consultant
How the ANZGOSA audit can benefit your practice: a look at GIST surgery from an Australian and NZ perspective. Aravind Suppiah; Sarah K.
 How the ANZGOSA audit can benefit your practice: a look at GIST surgery from an Australian and NZ perspective Aravind Suppiah; Sarah K. Thompson ANZGOSA database Commenced 2010; 1469 cases (2002 2014)
How the ANZGOSA audit can benefit your practice: a look at GIST surgery from an Australian and NZ perspective Aravind Suppiah; Sarah K. Thompson ANZGOSA database Commenced 2010; 1469 cases (2002 2014)
Anastomotic Leakage Following Low Anterior Resection of Rectal Cancer Considering the Role of Protective Stoma
 Anastomotic Leakage Following Low Anterior Resection of Rectal Cancer Considering the Role of Protective Stoma Mozafar M 1, Sobhiyeh MR 1, Heibatollahi M 2 Original Article Abstract Background and aims:
Anastomotic Leakage Following Low Anterior Resection of Rectal Cancer Considering the Role of Protective Stoma Mozafar M 1, Sobhiyeh MR 1, Heibatollahi M 2 Original Article Abstract Background and aims:
11/13/11. Biologics for CD and CUC: The Impact on Surgical Outcomes. Principles of Successful Intestinal Surgery
 Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Comparison of Loop Ileostomy and Loop Colostomy as Defunctioning Stoma in Low Rectal Cancer Surgery NCI Experience
 Kasr El Aini Journal of Surgery VOL., 12, NO 1 January 2011 75 Comparison of Loop Ileostomy and Loop Colostomy as Defunctioning Stoma in Low Rectal Cancer Surgery NCI Experience Ahmed Abbas, MD MRCS General
Kasr El Aini Journal of Surgery VOL., 12, NO 1 January 2011 75 Comparison of Loop Ileostomy and Loop Colostomy as Defunctioning Stoma in Low Rectal Cancer Surgery NCI Experience Ahmed Abbas, MD MRCS General
Investigations and management of severe endometriosis
 Investigations and management of severe endometriosis Dr Jim Tsaltas Head of Gynaecological Endoscopy and Endometriosis Surgery Monash Health Monash University Dept of O&G Melbourne IVF Freemasons Hospital
Investigations and management of severe endometriosis Dr Jim Tsaltas Head of Gynaecological Endoscopy and Endometriosis Surgery Monash Health Monash University Dept of O&G Melbourne IVF Freemasons Hospital
Colorectal Cancer Comparative Audit Report
 SOUTH EAST SCOTLAND CANCER NETWORK (SCAN) PROSPECTIVE CANCER AUDIT Colorectal Cancer 2014 2015 Comparative Audit Report Mr B.J. Mander, NHS Lothian, Lead Colorectal Cancer Clinician, SCAN Group Chair Mr
SOUTH EAST SCOTLAND CANCER NETWORK (SCAN) PROSPECTIVE CANCER AUDIT Colorectal Cancer 2014 2015 Comparative Audit Report Mr B.J. Mander, NHS Lothian, Lead Colorectal Cancer Clinician, SCAN Group Chair Mr
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY 2013/12/21
 THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
Bowel Prep Prior to Colon/Rectal Surgery: Valuable vs. Overrated
 Bowel Prep Prior to Colon/Rectal Surgery: Valuable vs. Overrated Alian Garay-Valuable Annie Kulungowski-Overrated Department of Surgery Grand Rounds September 24, 2007 Bowel Preps are Overrated History
Bowel Prep Prior to Colon/Rectal Surgery: Valuable vs. Overrated Alian Garay-Valuable Annie Kulungowski-Overrated Department of Surgery Grand Rounds September 24, 2007 Bowel Preps are Overrated History
Influence of multiple stapler firings used for rectal division on colorectal anastomotic leak rate
 Surg Endosc (2017) 31:5318 5326 DOI 10.1007/s00464-017-5611-0 and Other Interventional Techniques Influence of multiple stapler firings used for rectal division on colorectal anastomotic leak rate Tamara
Surg Endosc (2017) 31:5318 5326 DOI 10.1007/s00464-017-5611-0 and Other Interventional Techniques Influence of multiple stapler firings used for rectal division on colorectal anastomotic leak rate Tamara
CTC vs. Colonoscopy for Surveillance After CRC? David Weinberg, MD, MSc June 1, 2018
 CTC vs. Colonoscopy for Surveillance After CRC? David Weinberg, MD, MSc June 1, 2018 Goals of Post-operative CRC surveillance: Prevention or early detection of metachronous disease 30%-50% will suffer
CTC vs. Colonoscopy for Surveillance After CRC? David Weinberg, MD, MSc June 1, 2018 Goals of Post-operative CRC surveillance: Prevention or early detection of metachronous disease 30%-50% will suffer
Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma?
 17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
Temporary Diverting Stoma Improves Recovery of Anastomotic Leakage after Anterior Resection for Rectal Cancer
 www.nature.com/scientificreports Received: 5 April 2017 Accepted: 7 November 2017 Published: xx xx xxxx OPEN Temporary Diverting Stoma Improves Recovery of Anastomotic Leakage after Anterior Resection
www.nature.com/scientificreports Received: 5 April 2017 Accepted: 7 November 2017 Published: xx xx xxxx OPEN Temporary Diverting Stoma Improves Recovery of Anastomotic Leakage after Anterior Resection
Sleeve Gastrectomy: Harmful. John C. Eun, PGY-5 General Surgery Grand Rounds University of Colorado Denver 11/22/10
 Sleeve Gastrectomy: Harmful John C. Eun, PGY-5 General Surgery Grand Rounds University of Colorado Denver 11/22/10 Background Obesity: Body Mass Index >30 Risk factor for CAD, DM, Cancers Obesity Trends*
Sleeve Gastrectomy: Harmful John C. Eun, PGY-5 General Surgery Grand Rounds University of Colorado Denver 11/22/10 Background Obesity: Body Mass Index >30 Risk factor for CAD, DM, Cancers Obesity Trends*
The incidence of incisional hernias following ileostomy reversal in colorectal cancer patients treated with anterior resection
 GENERAL SURGERY Ann R Coll Surg Engl 2017; 99: 319 324 doi 10.1308/rcsann.2016.0347 The incidence of incisional hernias following ileostomy reversal in colorectal cancer patients treated with anterior
GENERAL SURGERY Ann R Coll Surg Engl 2017; 99: 319 324 doi 10.1308/rcsann.2016.0347 The incidence of incisional hernias following ileostomy reversal in colorectal cancer patients treated with anterior
Introduction E335. Authors Naoki Asayama, Shinji Nagata, Kenjiro Shigita, Taiki Aoyama, Akira Fukumoto, Shinichi Mukai
 Effectiveness and safety of endoscopic radial incision and cutting for severe benign anastomotic stenosis after surgery for colorectal carcinoma: a three-case series Authors Naoki Asayama, Shinji Nagata,
Effectiveness and safety of endoscopic radial incision and cutting for severe benign anastomotic stenosis after surgery for colorectal carcinoma: a three-case series Authors Naoki Asayama, Shinji Nagata,
Laparoscopic Colorectal Surgery
 Laparoscopic Colorectal Surgery 20 th November 2015 Dr Adam Cichowitz General Surgeon Laparoscopic Colorectal Surgery Introduced in early 1990s Uptake slow Steep learning curve Requirement for equipment
Laparoscopic Colorectal Surgery 20 th November 2015 Dr Adam Cichowitz General Surgeon Laparoscopic Colorectal Surgery Introduced in early 1990s Uptake slow Steep learning curve Requirement for equipment
Colorectal non-inflammatory emergencies
 Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Optimising Perioperative Pain Management And Surgical Outcomes
 Optimising Perioperative Pain Management And Surgical Outcomes Dr Chew Ghee Kheng MBBS FRCOG MD FAMS Senior Consultant Gynaecologist Subspecialist in Gynaecology Oncology Surgery Singapore General Hospital
Optimising Perioperative Pain Management And Surgical Outcomes Dr Chew Ghee Kheng MBBS FRCOG MD FAMS Senior Consultant Gynaecologist Subspecialist in Gynaecology Oncology Surgery Singapore General Hospital
The Laparoscopic Approach in the Treatment of Distal Colorectal Cancer
 The Open Colorectal Cancer Journal, 2011, 4, 13-17 13 Open Access The Laparoscopic Approach in the Treatment of Distal Colorectal Cancer Alexander Lebedyev 1, Damien Urban 2, Danny Rosin 1, Amram Ayalon
The Open Colorectal Cancer Journal, 2011, 4, 13-17 13 Open Access The Laparoscopic Approach in the Treatment of Distal Colorectal Cancer Alexander Lebedyev 1, Damien Urban 2, Danny Rosin 1, Amram Ayalon
Thirty-Day Outcomes of Laparoscopic vs. Open Total Proctocolectomy with Ileoanal Anastomosis in Children
 Thirty-Day Outcomes of Laparoscopic vs. Open Total Proctocolectomy with Ileoanal Anastomosis in Children Jeremy D. Kauffman MD, Paul D. Danielson MD, Nicole M. Chandler MD Johns Hopkins All Children s
Thirty-Day Outcomes of Laparoscopic vs. Open Total Proctocolectomy with Ileoanal Anastomosis in Children Jeremy D. Kauffman MD, Paul D. Danielson MD, Nicole M. Chandler MD Johns Hopkins All Children s
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University.
 Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age. Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010
 Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Bowel Preparation for Elective Colorectal Surgery: Helpful or Harmful? Michael J Stamos, MD University of California, Irvine
 Bowel Preparation for Elective Colorectal Surgery: Helpful or Harmful? Michael J Stamos, MD University of California, Irvine History of Colon Surgery Early 20 th Century mortality rates for colorectal
Bowel Preparation for Elective Colorectal Surgery: Helpful or Harmful? Michael J Stamos, MD University of California, Irvine History of Colon Surgery Early 20 th Century mortality rates for colorectal
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Complications of laparoscopic protective loop ileostomy in patients with colorectal cancer
 ISPUB.COM The Internet Journal of Surgery Volume 19 Number 2 Complications of laparoscopic protective loop ileostomy in patients with colorectal cancer F Puccio, M Solazzo, G Pandolfo, P Marcianò Citation
ISPUB.COM The Internet Journal of Surgery Volume 19 Number 2 Complications of laparoscopic protective loop ileostomy in patients with colorectal cancer F Puccio, M Solazzo, G Pandolfo, P Marcianò Citation
Colorectal Cancer Quality Performance Indicators
 Publication Report Colorectal Cancer Quality Performance Indicators Patients diagnosed between April 2013 and March 2016 Publication date 27th June 2017 An Official Statistics Publication for Scotland
Publication Report Colorectal Cancer Quality Performance Indicators Patients diagnosed between April 2013 and March 2016 Publication date 27th June 2017 An Official Statistics Publication for Scotland
Is the routine use of a water-soluble contrast enema prior to closure of a loop ileostomy necessary? A review of a single institution experience
 Dimitriou et al. World Journal of Surgical Oncology (2015) 13:331 DOI 10.1186/s12957-015-0742-z RESEARCH Open Access Is the routine use of a water-soluble contrast enema prior to closure of a loop ileostomy
Dimitriou et al. World Journal of Surgical Oncology (2015) 13:331 DOI 10.1186/s12957-015-0742-z RESEARCH Open Access Is the routine use of a water-soluble contrast enema prior to closure of a loop ileostomy
The effect of rectal washout on local recurrence following rectal cancer surgery
 COLORECTAL SURGERY Ann R Coll Surg Engl 208; 00: 46 5 doi 0.308/rcsann.207.0202 The effect of rectal washout on local recurrence following rectal cancer surgery SR Moosvi, K Manley, J Hernon Norfolk and
COLORECTAL SURGERY Ann R Coll Surg Engl 208; 00: 46 5 doi 0.308/rcsann.207.0202 The effect of rectal washout on local recurrence following rectal cancer surgery SR Moosvi, K Manley, J Hernon Norfolk and
Surgical Management of CBD Injury Jin Seok Heo
 Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
THE BEST OF TISSUE REGENERATION FOCUSED ON PATIENTS NEEDS
 THE BEST OF TISSUE REGENERATION FOCUSED ON PATIENTS NEEDS Tissue regeneration is a natural process by which the body forms a functional neo-tissue to repair a wound. This process requires the patient s
THE BEST OF TISSUE REGENERATION FOCUSED ON PATIENTS NEEDS Tissue regeneration is a natural process by which the body forms a functional neo-tissue to repair a wound. This process requires the patient s
Comparison of Risk Factors for Unplanned Conversion from Laparoscopic and Robotic to Open Colorectal Surgery
 Comparison of Risk Factors for Unplanned Conversion from Laparoscopic and Robotic to Open Colorectal Surgery Abdullah Wafa, M.D. General Surgery Resident, PGY2 St. Joseph Mercy Health System Ann Arbor
Comparison of Risk Factors for Unplanned Conversion from Laparoscopic and Robotic to Open Colorectal Surgery Abdullah Wafa, M.D. General Surgery Resident, PGY2 St. Joseph Mercy Health System Ann Arbor
Quality assurance in PROCARE Surgery for rectal cancer.
 Quality assurance in PROCARE Surgery for rectal cancer www.kankerregister.org to measure is to know Why to measure? if you cannot measure it, you cannot improve it when you can measure what you are speaking
Quality assurance in PROCARE Surgery for rectal cancer www.kankerregister.org to measure is to know Why to measure? if you cannot measure it, you cannot improve it when you can measure what you are speaking
Inadvertent Enterotomy in Minimally Invasive Abdominal Surgery
 SCIENTIFIC PAPER Inadvertent Enterotomy in Minimally Invasive Abdominal Surgery Steven J. Binenbaum, MD, Michael A. Goldfarb, MD ABSTRACT Background: Inadvertent enterotomy (IE) in laparoscopic abdominal
SCIENTIFIC PAPER Inadvertent Enterotomy in Minimally Invasive Abdominal Surgery Steven J. Binenbaum, MD, Michael A. Goldfarb, MD ABSTRACT Background: Inadvertent enterotomy (IE) in laparoscopic abdominal
Keywords: stoma closure; ileostomy closure; purse-string wound closure; linear wound closure
 Gastroenterology Report 3 (2014) 156 161, doi:10.1093/gastro/gou038 Advance access publication 10 July 2014 Meta-analysis Systematic review and meta-analysis of published randomized controlled trials comparing
Gastroenterology Report 3 (2014) 156 161, doi:10.1093/gastro/gou038 Advance access publication 10 July 2014 Meta-analysis Systematic review and meta-analysis of published randomized controlled trials comparing
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 4, Issue 2 2014 Article 1 Surgical Management of Colorectal Cancer In Nonagenarian Patients Yair Edden Shlomo Yellinek Oded Olsha Joseph Alberton Petachia Reissman
World Journal of Colorectal Surgery Volume 4, Issue 2 2014 Article 1 Surgical Management of Colorectal Cancer In Nonagenarian Patients Yair Edden Shlomo Yellinek Oded Olsha Joseph Alberton Petachia Reissman
JMSCR Volume 03 Issue 05 Page May 2015
 www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x Colon Surgery with & without Mechanical Bowel Preparation: A Comparative Study Authors L. Manikandan, Rajan Kumar T, Prathapan V.K, M.P.
www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x Colon Surgery with & without Mechanical Bowel Preparation: A Comparative Study Authors L. Manikandan, Rajan Kumar T, Prathapan V.K, M.P.