New Treatment Options for Diabetic Nephropathy patients. Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
|
|
|
- Cori Cole
- 5 years ago
- Views:
Transcription
1 New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
2 Diabetes and nephropathy Diabetic nephropathy is the most common cause of end-stage renal disease 1 About 40% of patients with Type 1 diabetes develop diabetic nephropathy 2 Similarly, 30 40% of patients with Type 2 diabetes develop diabetic nephropathy 1 In type 2 diabetes, the incidence of nephropathy ranges from 25% in people of European origin to 50% in people of Afro-Caribbean or Asian origin 2 1. Rossing K, et al. Diabetes Care 2003; 26(1): Thomas S, Viberti G. Medicine 2006; 34(3):
3 Diabetic nephropathy Stages of diabetic nephropathy: 1. Hypertrophy and hyperfiltration 2. Renal lesions without clinical signs 3. Microalbuminuria (>20 mg/min or 30 mg/24 h) 4. Macroalbuminuria (>200 mg/min or 300 mg/24 h) 5. End-stage renal disease Tagle R, et al. Cleveland Clin J Med 2003; 70:
4 Prevention of diabetic nephropathy: A multifocal approach Blood pressure Proteinuria LDL LDL + VLDL HbA1c < 120/80 mmhg < 0.3 g/24 h < 100 mg/dl < 130 mg/dl < 7.5 % (diabetics) Ruggenenti et al., Lancet, 2001
5 Meta Analysis: Lower Systolic BP Results in Slower Rates of Decline in GFR in Diabetics and Non-Diabetics SBP (mmhg) GFR (ml/min/year) r = 0.69; P <.05 Untreated HTN Bakris GL, et al. Am J Kidney Dis. 2000;36(3):
6 Recommended blood pressure targets JNC-7 1 ESH/ESC 2 WHO-ISH 3 BHS IV/NICE 4 <140/90 mm Hg <130/80 mm Hg in patients with diabetes or renal disease <140/90 mm Hg or lower if tolerated <130/80 mm Hg in patients with diabetes <140/90 mm Hg <130/ <80 mm Hg in patients with diabetes, existing CVD and renal insufficiency <140/90 mm Hg <130/90 mm Hg in patients with diabetes 1. Chobanian AV, et al. JAMA 2003; 289(19): ESH/ESC Guidelines Committee. J Hypertens 2003; 21: WHO. J Hypertens 2003; 21(11): BHS/NICE, 2006: 1 94.
7 Risk of CV death by albuminuria at baseline and achieved during follow-up in ADVANCE At baseline During follow-up Hazard ratio (95% CI) Normo Micro Macro p for trend <0.0001* Normo Micro Macro p for trend <0.0001* Baseline UACR ( g/mg) Achieved UACR ( g/mg) patients with type 2 diabetes *Adjusted for age, sex, HbA 1c, serum lipids, BMI, smoking, alcohol use, and study drug
8 Effect of an intensive vs conventional management of risk factors in type 2 diabetes Nephropathy p = Retinopathy p = 0.02 Autonomic Neuropathy Peripheral Neuropathy p = p = ns 0,0 0,5 1,0 1,5 2,0 2,5 Intensive TTT better Conventional TTT better Goede P et al, NEJM, 2003
9 Incidence of diabetic nephropathy according to onset of type 1 diabetes Cumulative incidence of diabetic nephropathy (%) (n=113, group A) (n=130, group B) (n=113, group C) (n=224, group D) p<0.001, log-rank test, pooled over strata. Not all patients in group D have yet been followed for 20 years Duration of diabetes (years) Hovind P, et al. Diabetes Care 2003; 26:
10 DIABETES Normoalbuminuria Can we prevent? Microalbuminuria Overt nephropathy ERSD
11 Can we prevent the diabetes?
12 Evidence of role of ARBs for the prevention of new-onset diabetes Study Treatment Duration (years) New-onset diabetes (%) p-value LIFE 1 ALPINE 2 VALUE 3 CHARM 4 SCOPE 5 Losartan vs. atenolol Candesartan vs. HCTZ Valsartan vs. amlodipine Candesartan vs. placebo Candesartan vs. placebo vs. 8.0 < vs. 4.1 < vs < vs vs Ong HT. Lancet 2003; 362: Lindholm LH, et al. J Hypertens 2003; 21: Julius S, et al. Lancet 2004; 363: Yusuf S, et al. Circulation 2005; 112: Lithell H, et al. J Hypertens 2003; 21:
13 ALPINE: study design Non-pharmacological treatment HCTZ 25 mg + atenolol 100 mg HCTZ 25 mg + atenolol 50 mg Placebo R HCTZ 25 mg (n=196) Candesartan 16 mg (n=196) Candesartan 16 mg + felodipine 2.5 mg Candesartan 16 mg + felodipine 5 mg Time 4 weeks 0 4 weeks 8 weeks 12 weeks 6 months 12 months No other antihypertensive drugs allowed Goal blood pressure: <135/<85 mm Hg; 65+ years of age <140/<90 mm Hg Lindholm LH, et al. J Hypertens 2003; 21(8):
14 ALPINE: new-onset diabetes Number of patients p<0.05 HCTZ Candesartan 1 0 During follow-up, 1 patient in the candesartan group and 8 patients in the HCTZ group developed diabetes Lindholm LH, et al. J Hypertens 2003; 21(8):
15 Can we prevent the development of microalbuminuria?
16 ACE-I HAS A DIFFERENT EFFECT ON GLOMERULAR INJURY ACCORDING TO THE DIFFERENT PHASE OF THE DISEASE AT WHICH THE TREATMENT IS STARTED 200 * 300 Proteinuria (mg/24h) ACE-I * Diabetes Diabetes + ACE-I Proteinuria (mg/24h) ACE-I Diabetes Diabetes + ACE-I Time (weeks) Time (weeks) Perico et al., J Am Soc Nephrol, 1994
17 The BErgamo NEphrologic DIabetic Complications Trial (BENEDICT) was primarily aimed to assess whether microalbuminuria can be prevented in people with type 2 diabetes and normal urinary albumin excretion Ruggenenti et al, NEJM, 2004
18 Study design RUN-IN RAS inhibitors withdrawal ndccbs withdrawal Randomisation TREATMENT PERIOD Trandolapril (2mg/d) Verapamil S.R. (240 mg/d) Trandolapril (2mg/d) plus Verapamil S.R. (180 mg/d) Placebo weeks months Overnight UAE Blood pressure and routine laboratory tests Ruggenenti et al, NEJM, 2004
19 Efficacy variables Primary - Incidence of persistent microalbuminuria (UAE > 20 µg/min) in 2 of 3 consecutive overnight collections confirmed 2 months apart Secondary - Rate of GFR decline (in a subgroup) - Rate of progression of retinopathy (in a subgroup) - Cumulative incidence of major cardiovascular events - Overall and cardiovascular mortality rate Ruggenenti et al, NEJM, 2004
20 Blood pressure according to treatment group Arterial Blood Pressure (mmhg) Systolic Diastolic Trandolapril Verapamil Trandolapril plus Verapamil Placebo Follow-up (months) Ruggenenti et al, NEJM, 2004
21 15 Placebo (30 events) Cumulative Incidence of Microalbuminuria (%) No. at Risk Follow-up (months) Trandolapril plus verapamil (17 events) Trandolapril plus Verapamil Placebo Ruggenenti et al, NEJM, 2004
22 Cumulative incidence of microalbuminuria (%) No ACE inhibitor (66 events) ACE inhibitor (35 events) No. at Risk Follow-up (months) ACE inhibitor No ACE inhibitor Ruggenenti et al, NEJM, 2004
23 20 Cumulative incidence of microalbuminuria (%) Calcium channel blocker (53 events) No calcium channel blocker (48 events) Follow-up (months) No. at Risk Calcium channel blocker No calcium channel blocker Ruggenenti et al, NEJM, 2004
24
25 Renal outcomes Major composite renal outcome New-onset microalbuminuria (UACR µg/mg) New-onset nephropathy (UACR >300 µg/mg) Doubling of serum creatinine >200 µmol/l (2.3 mg/dl) Requirement for renal replacement therapy or renal death
26 Changes in albuminuria in ADVANCE Progression Regression Annual patient event rate (%) % Perindoprilindapamide Placebo P< Annual patient event rate (%) P= % 0 Progression of 1 albuminuria stage 0 Regression of 1 albuminuria stage
27 New or worsening nephropathy Hazard ratios Annual event rate % BP arm Glucose arm Favours Per-Ind Favours Intensive Favours Placebo All participants 18% (-1 to 32) Standard 18% (-7 to 37) Intensive 17% (-12 to 38) Hazard ratio Favours Standard Relative risk reduction (95% CI) All participants 19% (2 to 34) Placebo 20% (-4 to 39) Per-Ind 18% (-9 to 39) Hazard ratio Relative risk reduction (95% CI) RRR 33%, P= Standard Placebo Glucose Intensive Per-Ind BP P for interaction=0.93
28 Major renal outcomes by systolic blood pressure achieved during follow-up* Annual patient event rate (%) P for trend < Relative risk reduction per 10 mmhg lower systolic BP: 6.9% (95% CI: %), P< Median diastolic BP No. of person-years Achieved systolic blood pressure (mmhg) *Adjusted for age, sex, HbA 1c, serum lipids, BMI, smoking, alcohol use, and study drug
29 IRMA 2: Study Design 590 patients with hypertension, type 2 diabetes, microalbuminuria (albumin excretion rate µg/min), and normal renal function Screening/Enrollment Double-blind Treatment Control group* Irbesartan 150 mg* Up to 5 weeks Irbesartan 300 mg* Follow-up: 2 years * Adjunctive antihypertensive therapies (excluding ACE inhibitors, angiotensin II receptor antagonists, and dihydropyridine calcium channel blockers) could be added to all groups to help achieve equal blood pressure levels. Parving H-H, et al. N Engl J Med 2001;345:
30 IRMA 2 Primary Endpoint Time to Overt Proteinuria Subjects (%) Control Irbesartan 150 mg Irbesartan 300 mg Follow-up (mo) Parving H-H, et al. N Engl J Med 2001;345:
 is not protective in diabetes BMJ 2004;")
31 The DIABHYCAR study: a low dose of ramipril (1.25mg) is not protective in diabetes BMJ 2004; 328:495
32 The DROP study: Objectives Purpose: To assess the ability of high-dose valsartan to reduce proteinuria in subjects with diabetic nephropathy Primary Objective: To compare responses to valsartan at 160, 320, and 640 mg/day in patients with hypertension, type 2 diabetes mellitus, and albuminuria (30 1,000 mg/d) Hollenberg NK et al, J Hypertens, 2007, 25:
33 Study Design Design: multicentre, double-blind, randomized, parallel group study Patient population: subjects with hypertension, proteinuria and T2DM Valsartan 160 mg Valsartan 160 mg Screening Placebo run-in Valsartan 160 mg Valsartan 320 mg Valsartan 160 mg Valsartan 640 mg Week 6 (Visit 1) Week 3 (Visit 3) Week 2 Week 0 (Visit 4) (Visit 6) (Randomisation) Week 4 (Visit 8) Week 16 (Visit 11) Week 30 (Visit 12) Hollenberg NK et al, J Hypertens, 2007, 25:
34 Time Course for Change from Baseline in Urinary Albumin Excretion Rate 0 Week 4 Week 16 Week 30 Change (%) from baseline in UAER Valsartan 160 mg Valsartan 320 mg * -39* * -40* Valsartan 640 mg *p<0.001 (320 mg and 640mg vs baseline); p=0.03 (160 mg vs baseline). Hollenberg NK et al, J Hypertens, 2007, 25:
35 Effect of candesartan and ramipril alone or in combination on urinary protein and TGFbeta1 excretions Song JH et al, NDT, 2006
36 IDNT Time to Doubling of Serum Creatinine 70 Subject s (%) Irbesartan Amlodipine Control RRR 37% P<0.001 P=NS RRR 33% P= Lewis EJ et al. N Engl J Med 2001;345: Follow-up (mo)
37
38 A double-blind, randomized, placebo-controlled study in hypertensive patients with type 2 diabetes and nephropathy Randomization Aliskiren 150 mg (n = 301) Aliskiren 300 mg Placebo (n = 298) + Placebo + Losartan 100 mg and optimal antihypertensive therapy Open-label weeks 0 Double-blind (endpoint) Week Forced titration at week 12 All doses were administered once daily ASN, 2007, oral presentation
39 Aliskiren significantly reduced UACR from baseline to week 24 endpoint compared with placebo Mean change from baseline in UACR (%) 5 2% % reduction in UACR vs placebo % * *p = Data are shown as percentage change in geometric mean Baseline was week 2 value UACR, urinary albumin:creatinine ratio Aliskiren (n = 287) Placebo (n = 289)
40 Study design of the PROTECT study Monocentric study, triple cross-over in non-diabetic patients with proteinuric nephropathies. Randomized sequences Washout Losartan 100 od Losartan 100 bid Losartan lisinopril 20 2 months 2 months 2 months 2 months Proteinuria (D/N) Renal hemodynamics (inulin, PAH clearances) ABPM Meier et al, abstract ASN 2008
41 Effect of a high dose of losartan on proteinuria in patients with diabetic and non-diabetic nephropathies Proteinuria (ug/min) Median (n=20) D N D N D N D N Baseline Losartan 100 Losartan 100 Losartan 100 od bid + Lisinopril 20 Meier et al, abstract ASN 2008
42 EFFECTIVENESS OF RAS INHIBITION IN TYPE 2 DIABETES Preventive Intervention BENEDICT, ADVANCE IRMA-2, ADVANCE RENAAL, IDNT Model structure Normoalbuminuria Microalbuminuria Overt nephropathy D E A T H ERSD
43 Aldosterone Blockade in Diabetic Kidney Disease 54% reduction in proteinuria after 4 weeks add-on treatment with spironolactone. No significant differences in BP or creatinine clearance Chrysostomou et al: N Engl J Med 345: , 2001
44 Metanalysis of studies using mineralocorticoid receptor blockade in diabetic and non-diabetic nephropathies Paralle-group RCTs N Drug Dose Duration Effect on prot. Bianchi et al, Spironolactone m -54 vs 6% Chrysostomou et al, Spironolactone 25 3 m -45 vs -9 Epstein et al, Eplerenone 50/ w -45 vs -7 Van den Meiracker, Spironolactone 25/50 12 m -44 vs -4 Cross-over RCTs Rachmaniet al, Spironolactone 50 24w -38 Rossing et al, Spironolactone 25 8w -33 Schjoedt et al, Spironolactone 25 8w -30 Schjoedt et al, Spironolactone 25 8w -32 Non-RCTs Bianchi et al, Spironolactone 25 8w -50 Chrysostomou et al, Spironolactone 25 4w -54 Furumatsu et al, Spironolactone 25 8w -32 vs 19 Nitta et al, Spironolactone 25 6m -15 Nowicki et alm Spironolactone w -38 Sato et al, Spironolactone 25 12w -38 Shiigai et al, Spironolactone 25 10m -20 Hyperkalemic events were significant in only 1 of 8 randomized controlled trials. Significant decreases in BP and GFR in approximately 40% and 25% of included studies, respectively.
45 Effect of aldactone on proteinuria in patients receiving a blocker of the renin-angiotensin system 10 Ramipril 5 mg Ramipril 5 mg + irbesartan 150 mg Ramipril 5 mg + spironolactone 25 mg Ramipril 5 mg + irbesartan 150 mg + Spiro 25 mg 0 Change in proteinuria at 6 months (%) N=10 patients per group, Double-blind, placebo-controlled Chrysostomou et al, Clin JASN, 2006; 1:

46 Aldosterone Blockade in Diabetic Kidney Disease Be careful of hyperkalemia
47 Conclusions Diabetic nephropathy can be effectively prevented by blockade of the renin angiotensin system prescribed at the right dose Prevention of DN also needs: - a perfect control of BP - a maximal decrease in proteinuria - the control of glycemia - the control of dyslipidemia
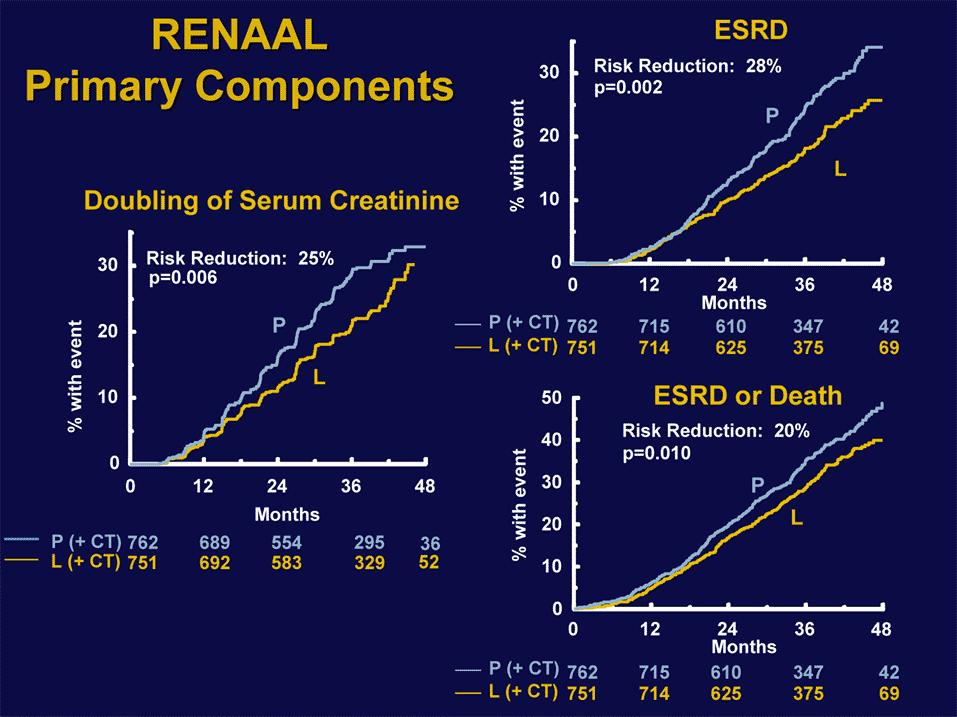
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Diabetes and kidney disease.
 Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Hypertension and diabetic nephropathy
 Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
The hypertensive kidney and its Management
 The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA
 ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kidney Disease, Hypertension and Cardiovascular Risk
 1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Prevention and management of chronic kidney disease in type 2 diabetes
 162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Preventing the cardiovascular complications of hypertension
 European Heart Journal Supplements (2004) 6 (Supplement H), H37 H42 Preventing the cardiovascular complications of hypertension Peter Trenkwalder* Department of Internal Medicine, Starnberg Hospital, Ludwig
European Heart Journal Supplements (2004) 6 (Supplement H), H37 H42 Preventing the cardiovascular complications of hypertension Peter Trenkwalder* Department of Internal Medicine, Starnberg Hospital, Ludwig
The Road to Renin System Optimization: Renin Inhibitor
 The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Optimal blood pressure targets in chronic kidney disease
 Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Keywords albuminuria, hypertension, nephropathy, proteinuria
 Should proteinuria reduction be the criterion for antihypertensive drug selection for patients with kidney disease? Rigas G. Kalaitzidis and George L. Bakris Department of Medicine, Hypertensive Diseases
Should proteinuria reduction be the criterion for antihypertensive drug selection for patients with kidney disease? Rigas G. Kalaitzidis and George L. Bakris Department of Medicine, Hypertensive Diseases
Diabetic Nephropathy 2009
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers. Robert D. Toto, MD
 R e v i e w P a p e r Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers Robert D. Toto, MD Both the prevalence and incidence of end-stage renal disease have been increasing
R e v i e w P a p e r Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers Robert D. Toto, MD Both the prevalence and incidence of end-stage renal disease have been increasing
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Firenze 22 settembre 2007
 Istituto di di medicina dello sport di di Firenze AMES Prevenzione cardiovascolare e cambiamenti negli stili di vita Firenze 22 settembre 2007 Orientamenti attuali per un intervento farmacologico e non
Istituto di di medicina dello sport di di Firenze AMES Prevenzione cardiovascolare e cambiamenti negli stili di vita Firenze 22 settembre 2007 Orientamenti attuali per un intervento farmacologico e non
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Renal Protection Staying on Target
 Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
State of the art treatment of hypertension: established and new drugs. Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland
 State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
The CARI Guidelines Caring for Australasians with Renal Impairment. Antihypertensive therapy in diabetic nephropathy GUIDELINES
 Antihypertensive therapy in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Adequate control of blood pressure (BP) slows progression
Antihypertensive therapy in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Adequate control of blood pressure (BP) slows progression
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
RATIONALE. chapter 4 & 2012 KDIGO
 http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
ACEIs / ARBs NDHP dihydropyridine ( DHP ) ACEIs ARBs ACEIs ARBs NDHP. ( GFR ) 60 ml/min/1.73m ( chronic kidney disease, CKD )
 ACEIs ARBs ACEIs ARBs NDHP. ( GFR ) 60 ml/min/1.73m ( chronic kidney disease, CKD )") 005 16 175-180 1 1 ( chronic kidney disease, CKD ) 003 ( end-stage renal disease, ESRD ) Angiotensin-converting enzyme inhibitors ( ) angiotensin receptor blockers ( ) nondihydropyridine ( NDHP ) / NDHP
005 16 175-180 1 1 ( chronic kidney disease, CKD ) 003 ( end-stage renal disease, ESRD ) Angiotensin-converting enzyme inhibitors ( ) angiotensin receptor blockers ( ) nondihydropyridine ( NDHP ) / NDHP
Renal protection by inhibition of the renin-angiotensinaldosterone
 Renal protection by inhibition of the renin-angiotensinaldosterone system Tomas Berl Key words: angiotensinconverting enzyme inhibitor, angiotensin receptor blocker, combination therapy, direct renin inhibitor,
Renal protection by inhibition of the renin-angiotensinaldosterone system Tomas Berl Key words: angiotensinconverting enzyme inhibitor, angiotensin receptor blocker, combination therapy, direct renin inhibitor,
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension)
") Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
The CARI Guidelines Caring for Australasians with Renal Impairment. Protein Restriction to prevent the progression of diabetic nephropathy GUIDELINES
 Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease
 Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?
 Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Therapeutic approaches to slowing the progression of diabetic nephropathy is less best?
 www.drugsincontext.com The journal of interventions in clinical practice REVIEW Therapeutic approaches to slowing the progression of diabetic nephropathy is less best? FULL TEXT ARTICLE Eva Vivian, 1 Chelsea
www.drugsincontext.com The journal of interventions in clinical practice REVIEW Therapeutic approaches to slowing the progression of diabetic nephropathy is less best? FULL TEXT ARTICLE Eva Vivian, 1 Chelsea
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Clinical Pearls in Renal Medicine
 Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
CARDIO-RENAL SYNDROME
 CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
Cardiovascular Pharmacotherapy in Special Population: Cardio-Nephrology
 49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
(renoprotective (end-stage renal disease, ESRD) therapies) (JAMA)
 therapies) (JAMA)") [1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
[1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Fan Shunan 1, Yuan Jiqing 2 and Dong Xue 3. Introduction. Original Article
 803495JRA0010.1177/1470320318803495Journal of the Renin Angiotensin Aldosterone SystemShunan et al. research-article20182018 Original Article Effects of angiotensin-converting enzyme inhibitors and angiotensin
803495JRA0010.1177/1470320318803495Journal of the Renin Angiotensin Aldosterone SystemShunan et al. research-article20182018 Original Article Effects of angiotensin-converting enzyme inhibitors and angiotensin
ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence?
 Reviews ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence? George L. Bakris, MD; 1 and Matthew Weir, MD 2 Although angiotensin-converting
Reviews ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence? George L. Bakris, MD; 1 and Matthew Weir, MD 2 Although angiotensin-converting
Valsartan Amlodipine HCT Combination: Control To Goal. Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI. Prof of cardiology Ain Shams University
 Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
An acute fall in estimated glomerular filtration rate during treatment with losartan predicts a slower decrease in long-term renal function
 original article http://www.kidney-international.org & 2011 International Society of Nephrology see commentary on page 235 An acute fall in estimated glomerular filtration rate during treatment with losartan
original article http://www.kidney-international.org & 2011 International Society of Nephrology see commentary on page 235 An acute fall in estimated glomerular filtration rate during treatment with losartan
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Renin-Angiotensin-Aldosterone System Blockade in Diabetic Nephropathy. Present Evidences
 J. Clin. Med. 2015, 4, 1908-1937; doi:10.3390/jcm4111908 Review OPEN ACCESS Journal of Clinical Medicine ISSN 2077-0383 www.mdpi.com/journal/jcm Renin-Angiotensin-Aldosterone System Blockade in Diabetic
J. Clin. Med. 2015, 4, 1908-1937; doi:10.3390/jcm4111908 Review OPEN ACCESS Journal of Clinical Medicine ISSN 2077-0383 www.mdpi.com/journal/jcm Renin-Angiotensin-Aldosterone System Blockade in Diabetic
Clinical therapeutic strategies for early stage of diabetic kidney disease
 Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.4239/wjd.v5.i3.342 World J Diabetes 2014 June 15; 5(3): 342-356 ISSN 1948-9358 (online) 2014
Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.4239/wjd.v5.i3.342 World J Diabetes 2014 June 15; 5(3): 342-356 ISSN 1948-9358 (online) 2014
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 7 January 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 7 January 2009 LERCAPRESS 10 mg/10 mg, film-coated tablets Pack of 30 (CIP code: 385 953-3) Pack of 90 (CIP code:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 7 January 2009 LERCAPRESS 10 mg/10 mg, film-coated tablets Pack of 30 (CIP code: 385 953-3) Pack of 90 (CIP code:
Management of Hypertension in Diabetic Nephropathy: How Low Should We Go?
 Review Advances in CKD 216 Published online: January 15, 216 Management of Hypertension in Diabetic Nephropathy: How Low Should We Go? Hillel Sternlicht George L. Bakris Department of Medicine, Section
Review Advances in CKD 216 Published online: January 15, 216 Management of Hypertension in Diabetic Nephropathy: How Low Should We Go? Hillel Sternlicht George L. Bakris Department of Medicine, Section
University of Groningen. Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste
 University of Groningen Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
University of Groningen Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Proteinuria increases the risk for progression of chronic. Review
 Review Annals of Internal Medicine Meta-analysis: Effect of Monotherapy and Combination Therapy with Inhibitors of the Renin Angiotensin System on Proteinuria in Renal Disease Regina Kunz, MD, MSc(Epi);
Review Annals of Internal Medicine Meta-analysis: Effect of Monotherapy and Combination Therapy with Inhibitors of the Renin Angiotensin System on Proteinuria in Renal Disease Regina Kunz, MD, MSc(Epi);
The CARI Guidelines Caring for Australians with Renal Impairment. Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy
 Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All hypercholesterolaemic diabetics
Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All hypercholesterolaemic diabetics
In the Literature 1001 BP of 1.1 mm Hg). The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi
. The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi") Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
Hot Topics in Diabetic Kidney Disease a primary care perspective
 Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Prof. Armando Torres Nephrology Section Hospital Universitario de Canarias University of La Laguna Tenerife, Canary Islands, Spain.
 Does RAS blockade improve outcomes after kidney transplantation? Armando Torres, La Laguna, Spain Chairs: Hans De Fijter, Leiden, The Netherlands Armando Torres, La Laguna, Spain Prof. Armando Torres Nephrology
Does RAS blockade improve outcomes after kidney transplantation? Armando Torres, La Laguna, Spain Chairs: Hans De Fijter, Leiden, The Netherlands Armando Torres, La Laguna, Spain Prof. Armando Torres Nephrology
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor Treatment in Diabetic Nephropathy GUIDELINES
 ACE Inhibitor Treatment in Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All patients with Type 1 or Type 2 diabetes mellitus complicated
ACE Inhibitor Treatment in Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All patients with Type 1 or Type 2 diabetes mellitus complicated
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
2014 HYPERTENSION GUIDELINES
 2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
Diabetic Kidney Disease in the Primary Care Clinic
 Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI. Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona
 PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona Disclosure Dr Massimo Boemi has been granted as speaker
PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona Disclosure Dr Massimo Boemi has been granted as speaker
A Fresh Look at ARBs : Focus on HF survival data
 A Fresh Look at ARBs : Focus on HF survival data Seok-Min Kang, MD, Ph D. Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea HF specialists ARBs,
A Fresh Look at ARBs : Focus on HF survival data Seok-Min Kang, MD, Ph D. Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea HF specialists ARBs,
Hypertension is a major risk factor for
 OPTIMAL RISK MANAGEMENT OF THE HYPERTENSIVE PATIENT WITH MULTIPLE RISK FACTORS * Keith C. Ferdinand, MD, FACC ABSTRACT To determine the risk of cardiovascular disease in patients with hypertension, it
OPTIMAL RISK MANAGEMENT OF THE HYPERTENSIVE PATIENT WITH MULTIPLE RISK FACTORS * Keith C. Ferdinand, MD, FACC ABSTRACT To determine the risk of cardiovascular disease in patients with hypertension, it
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
High-dose monotherapy vs low-dose combination therapy of calcium channel blockers and angiotensin receptor blockers in mild to moderate hypertension
 (2005) 19, 491 496 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE High-dose monotherapy vs low-dose combination therapy of calcium channel blockers
(2005) 19, 491 496 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE High-dose monotherapy vs low-dose combination therapy of calcium channel blockers
6/10/2014. Chronic Kidney Disease - General management and standard of care. Management of CKD according to stage (KDOQI 2002)
") Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
The control of hypertension in the. Reaching for Aggressive Blood Pressure Goals: Role of Angiotensin Receptor Blockade in Combination Therapy REPORTS
 REPORTS Reaching for Aggressive Blood Pressure Goals: Role of Angiotensin Receptor Blockade in Combination Therapy By Richard V. Milani, MD Abstract Elevated blood pressure, particularly systolic blood
REPORTS Reaching for Aggressive Blood Pressure Goals: Role of Angiotensin Receptor Blockade in Combination Therapy By Richard V. Milani, MD Abstract Elevated blood pressure, particularly systolic blood