New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
|
|
|
- Coral Watson
- 5 years ago
- Views:
Transcription


1 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am Bayani B. Elma, MD Former Clinical Associate Professor of Medicine University of Maryland School of Medicine
2 Pre-Test Questions 1. The ACC and AHA led the development of the 2017 High Blood Pressure Guidelines with collaboration of the major pharmaceutical companies in order to update the standards of care established in the JNC The increase in the estimate of prevalence of hypertension in American adults and are now classified as having Stage 1 hypertension (SBP of ) OR (DBP mmhg) has resulted in a large increase in the percentage of U.S. adults for whom antihypertensive medication is recommended. 3. In low-risk adults with elevated BP or Stage 1 hypertension with low ASCVD-risk, BP should be repeated after 3-6 months of nonpharmacological therapy. 4. Chlorthalidone ( mg) is the preferred diuretic because of long half-life and proven reduction of CVD risk. 5. The key finding of the ACCORD trial is that lowering systolic blood pressure to 120 mmhg results in significant cardiovascular benefit in high-risk patients hypertension compared with routine blood pressure control to <140 mmhg.
3 At the end of this presentation, you will: 1. Understand the changes to the definition of hypertension 2. Understand the standards for measuring an accurate blood pressure 3. Understand recommendations for management of hypertension from lifestyle intervention to pharmacological therapy
4 Definition 1. Understand the changes to the definition of hypertension 2. Understand the standards for measuring an accurate blood pressure 3. Understand recommendations for management of hypertension from lifestyle intervention to pharmacological therapy

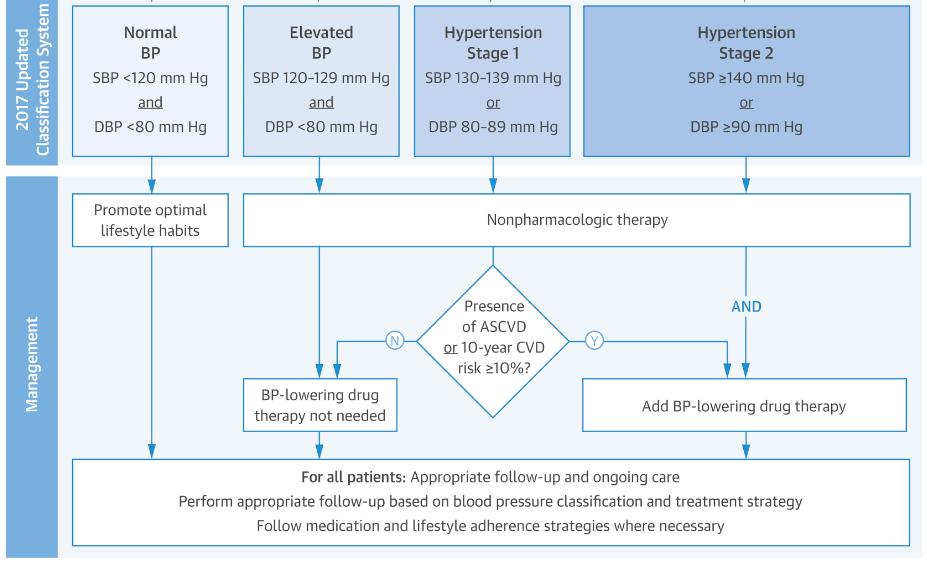
5 Definition of High Blood Pressure BP should be categorized as normal, elevated, or stage 1 or 2 hypertension to prevent and treat high BP.
6
7 ASCVD Risk Estimation Calculated based on the following data: Gender Age Race Total Cholesterol HDL-Cholesterol Systolic Blood Pressure Hypertension Treatment Diabetes Smoker
8 Measurement 1. Understand the changes to the definition of hypertension 2. Understand the standards for measuring an accurate blood pressure 3. Understand recommendations for management of hypertension from lifestyle intervention to pharmacological therapy
9 Accurate Measurement of BP in the Office Recommendation for Accurate Measurement of BP in the Office For diagnosis and management of high BP, proper methods are recommended for accurate measurement and documentation of BP.
10 Checklist for Accurate Measurement of BP Key Steps for Proper BP Measurements Step 1: Properly prepare the patient. Step 2: Use proper technique for BP measurements. Step 3: Take the proper measurements needed for diagnosis and treatment of elevated BP/hypertension. Step 4: Properly document accurate BP readings. Step 5: Average the readings. Step 6: Provide BP readings to patient.
11 Common problems that account for inaccurate blood pressure measurement When the patient has Cuff over clothing A full bladder A conversation or talking Unsupported arm An unsupported back Unsupported feet Crossed legs BP can appear higher by mmhg mmhg mmhg 10 mmhg 5-10 mmhg 5-10 mmhg 2-8 mmhg
12 Corresponding Values of SBP/DBP for Clinic, HBPM, Daytime, Nighttime, and 24-Hour ABPM Measurements Clinic HBPM Daytime Nighttime 24-Hour ABPM ABPM ABPM 120/80 120/80 120/80 100/65 115/75 130/80 130/80 130/80 110/65 125/75 140/90 135/85 135/85 120/70 130/80 160/ /90 145/90 140/85 145/90 ABPM indicates ambulatory blood pressure monitoring; BP, blood pressure; DBP diastolic blood pressure; HBPM, home blood pressure monitoring; and SBP, systolic blood pressure.
13 Masked and White Coat Hypertension Recommendations for Masked and White Coat Hypertension In adults with an untreated SBP greater than 130 mm Hg but less than 160 mm Hg or DBP greater than 80 mm Hg but less than 100 mm Hg, it is reasonable to screen for the presence of white coat hypertension by using either daytime ABPM or HBPM before diagnosis of hypertension. In adults with white coat hypertension, periodic monitoring with either ABPM or HBPM is reasonable to detect transition to sustained hypertension. In adults being treated for hypertension with office BP readings not at goal and HBPM readings suggestive of a significant white coat effect, confirmation by ABPM can be useful.
14 Masked and White Coat Hypertension continued Recommendations for Masked and White Coat Hypertension In adults with untreated office BPs that are consistently between 120 mm Hg and 129 mm Hg for SBP or between 75 mm Hg and 79 mm Hg for DBP, screening for masked hypertension with HBPM (or ABPM) is reasonable. In adults on multiple-drug therapies for hypertension and office BPs within 10 mm Hg above goal, it may be reasonable to screen for white coat effect with HBPM (or ABPM). It may be reasonable to screen for masked uncontrolled hypertension with HBPM in adults being treated for hypertension and office readings at goal, in the presence of target organ damage or increased overall CVD risk. In adults being treated for hypertension with elevated HBPM readings suggestive of masked uncontrolled hypertension, confirmation of the diagnosis by ABPM might be reasonable before intensification of antihypertensive drug treatment.
15 Patient evaluation prior to management of hypertension Before considering treatment options, you should have basic and consider optional laboratory tests for primary hypertension: Basic testing Optional testing Fasting blood glucose* Complete blood count Lipid profile Serum creatinine with egfr* Serum sodium, potassium, calcium* Thyroid-stimulating hormone Urinalysis Electrocardiogram Echocardiogram Uric acid Urinary albumin to creatinine ratio *May be included in a comprehensive metabolic panel. egfr indicates estimated glomerular filtration rate.
16 Management 1. Understand the changes to the definition of hypertension 2. Understand the standards for measuring an accurate blood pressure 3. Understand recommendations for management of hypertension from lifestyle intervention to pharmacological therapy
17 Best Proven Nonpharmacological Interventions for Prevention and Treatment of Hypertension* Nonpharmacological Intervention Dose Weight loss Weight/body fat Best goal is ideal body weight, but aim for at least a 1-kg reduction in body weight for most adults who are overweight. Expect about 1 mm Hg for every 1-kg reduction in body weight. Healthy diet Reduced intake of dietary sodium Enhanced intake of dietary potassium DASH dietary pattern Dietary sodium Dietary potassium Consume a diet rich in fruits, vegetables, whole grains, and lowfat dairy products, with reduced content of saturated and total fat. Optimal goal is <1500 mg/d, but aim for at least a 1000-mg/d reduction in most adults. Aim for mg/d, preferably by consumption of a diet rich in potassium. Approximate Impact on SBP Hypertension Normotension -5 mm Hg -2/3 mm Hg -11 mm Hg -3 mm Hg -5/6 mm Hg -2/3 mm Hg -4/5 mm Hg -2 mm Hg *Type, dose, and expected impact on BP in adults with a normal BP and with hypertension. DASH indicates Dietary Approaches to Stop Hypertension; and SBP, systolic blood pressure. Resources: Your Guide to Lowering Your Blood Pressure With DASH How Do I Make the DASH? Available at: Top 10 Dash Diet Tips. Available at:
18 Best Proven Nonpharmacological Interventions for Prevention and Treatment of Hypertension* continued Physical activity Moderation in alcohol intake Nonpharmacological Dose Intervention Aerobic min/wk 65% 75% heart rate reserve Dynamic resistance min/wk 50% 80% 1 rep maximum 6 exercises, 3 sets/exercise, 10 repetitions/set Isometric resistance 4 2 min (hand grip), 1 min rest between exercises, 30% 40% maximum voluntary contraction, 3 sessions/wk 8 10 wk Alcohol consumption In individuals who drink alcohol, reduce alcohol to: Men: 2 drinks daily Women: 1 drink daily Approximate Impact on SBP Hypertension Normotension -5/8 mm Hg -2/4 mm Hg -4 mm Hg -2 mm Hg -5 mm Hg -4 mm Hg -4 mm Hg -3 mm *Type, dose, and expected impact on BP in adults with a normal BP and with hypertension. In the United States, one standard drink contains roughly 14 g of pure alcohol, which is typically found in 12 oz of regular beer (usually about 5% alcohol), 5 oz of wine (usually about 12% alcohol), and 1.5 oz of distilled spirits (usually about 40% alcohol).
19 Nonpharmacological Interventions Recommendations for Nonpharmacological Interventions Weight loss is recommended to reduce BP in adults with elevated BP or hypertension who are overweight or obese. A heart-healthy diet, such as the DASH (Dietary Approaches to Stop Hypertension) diet, that facilitates achieving a desirable weight is recommended for adults with elevated BP or hypertension. Sodium reduction is recommended for adults with elevated BP or hypertension. Potassium supplementation, preferably in dietary modification, is recommended for adults with elevated BP or hypertension, unless contraindicated by the presence of CKD or use of drugs that reduce potassium excretion.
20 Nonpharmacological Interventions continued Recommendations for Nonpharmacological Interventions Increased physical activity with a structured exercise program is recommended for adults with elevated BP or hypertension. Adult men and women with elevated BP or hypertension who currently consume alcohol should be advised to drink no more than 2 and 1 standard drinks* per day, respectively. In the United States, 1 standard drink contains roughly 14 g of pure alcohol, which is typically found in 12 oz of regular beer (usually about 5% alcohol), 5 oz of wine (usually about 12% alcohol), and 1.5 oz of distilled spirits (usually about 40% alcohol).
21 General Principles of Drug Therapy Recommendation for General Principle of Drug Therapy Simultaneous use of an ACE inhibitor, ARB, and/or renin inhibitor is potentially harmful and is not recommended to treat adults with hypertension. Recommendation for Choice of Initial Medication For initiation of antihypertensive drug therapy, first-line agents include thiazide diuretics, CCBs, and ACE inhibitors or ARBs.
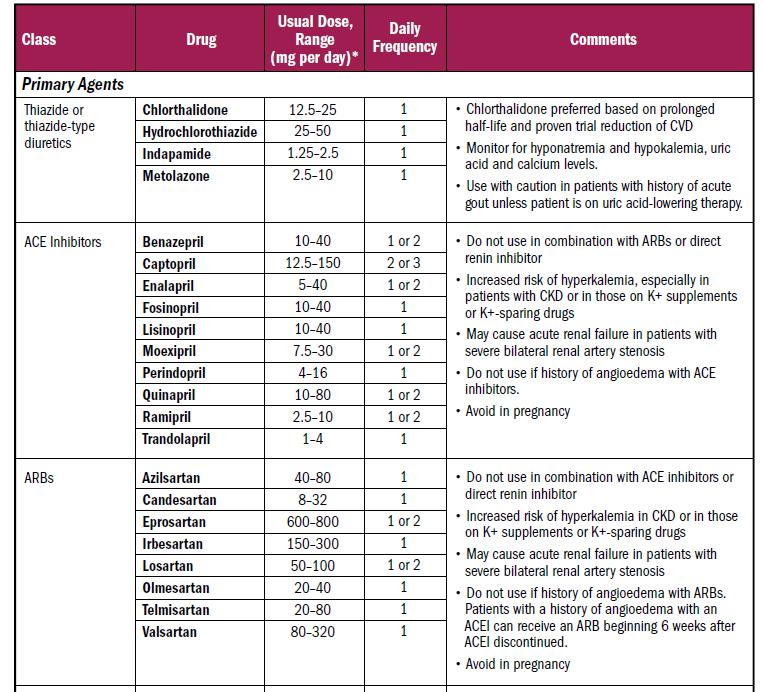
22 Oral Antihypertensive Drugs
23 Oral Antihypertensive Drugs continued
24 Oral Antihypertensive Drugs continued
25 Oral Antihypertensive Drugs continued
26 Frequently Used Medications and Other Substances That May Cause Elevated BP

27 Frequently Used Medications and Other Substances That May Cause Elevated BP Table 14.

28 TOD = Target organ damage
29 Clinician s Sequential Flow Chart for the Management of Hypertension Clinician s Sequential Flow Chart for the Management of Hypertension Measure office BP accurately Detect white coat hypertension or masked hypertension by using ABPM and HBPM Evaluate for secondary hypertension Identify target organ damage Introduce lifestyle interventions Identify and discuss treatment goals Use ASCVD risk estimation to guide BP threshold for drug therapy Align treatment options with comorbidities Account for age, race, ethnicity, sex, and special circumstances in antihypertensive treatment Initiate antihypertensive pharmacological therapy Insure appropriate follow-up Use team-based care Connect patient to clinician via telehealth Detect and reverse nonadherence (e.g. KardiAssure) Detect white coat effect or masked uncontrolled hypertension Use health information technology for remote monitoring and self-monitoring of BP ASCVD indicates atherosclerotic cardiovascular disease; BP, blood pressure; CVD, cardiovascular disease; and SBP, systolic blood pressure.
30 BP Thresholds for and Goals of Pharmacological Therapy in Patients With Hypertension According to Clinical Conditions Clinical Condition(s) BP Threshold, mm Hg BP Goal, mm Hg General Clinical CVD or 10-year ASCVD risk 10% 130/80 <130/80 No clinical CVD and 10-year ASCVD risk <10% 140/90 <130/80 Older persons ( 65 years of age; noninstitutionalized, 130 (SBP) <130 (SBP) ambulatory, community-living adults) Specific comorbidities Diabetes mellitus 130/80 <130/80 Chronic kidney disease 130/80 <130/80 Heart failure 130/80 <130/80 Stable ischemic heart disease 130/80 <130/80 Secondary stroke prevention 140/90 <130/80 Secondary stroke prevention (lacunar) 130/80 <130/80 Peripheral arterial disease 130/80 <130/80 ASCVD indicates atherosclerotic cardiovascular disease; BP, blood pressure; CVD, cardiovascular disease; and SBP, systolic blood pressure.
31 Diabetes Mellitus Recommendations for Treatment of Hypertension in Patients With DM In adults with DM and hypertension, antihypertensive drug treatment should be initiated at a BP of 130/80 mm Hg or higher with a treatment goal of less than 130/80 mm Hg. In adults with DM and hypertension, all first-line classes of antihypertensive agents (i.e., diuretics, ACE inhibitors, ARBs, and CCBs) are useful and effective. In adults with DM and hypertension, ACE inhibitors or ARBs may be considered in the presence of albuminuria.
32 Chronic Kidney Disease Recommendations for Treatment of Hypertension in Patients With CKD Adults with hypertension and CKD should be treated to a BP goal of less than 130/80 mm Hg. In adults with hypertension and CKD (stage 3 or higher or stage 1 or 2 with albuminuria [ 300 mg/d, or 300 mg/g albumin-to-creatinine ratio or the equivalent in the first morning void]), treatment with an ACE inhibitor is reasonable to slow kidney disease progression. In adults with hypertension and CKD (stage 3 or higher or stage 1 or 2 with albuminuria [ 300 mg/d, or 300 mg/g albumin-to-creatinine ratio in the first morning void]), treatment with an ARB may be reasonable if an ACE inhibitor is not tolerated.
33 Management of Hypertension in Patients With CKD Treatment of hypertension in patients with CKD BP goal <130/80 mm Hg (Class I) Albuminuria ( 300 mg/d or 300 mg/g creatinine) Yes ACE inhibitor (Class IIa) No Usual first-line medication choices ACE inhibitor intolerant Yes ARB* (Class IIb) No ACE inhibitor* (Class IIa) *CKD stage 3 or higher or stage 1 or 2 with albuminuria 300 mg/d or 300 mg/g creatinine. ACE indicates angiotensin-converting enzyme; ARB, angiotensin receptor blocker; BP blood pressure; and CKD, chronic kidney disease.
34 Heart Failure Recommendation for Prevention of HF in Adults With Hypertension In adults at increased risk of HF, the optimal BP in those with hypertension should be less than 130/80 mm Hg.
35 1. False. The ACC and AHA led the development of the 2017 High Blood Pressure Guidelines with collaboration of the National Heart, Lung, and Blood Institute (NHLBI) in order to update the standards of care established in the JNC False. The increase in the estimate of prevalence of hypertension in American adults and are now classified as having Stage 1 hypertension (SBP of ) OR (DBP mmhg) has resulted in a small increase in the percentage of U.S. adults for whom antihypertensive medication is recommended. 3. True. 4. True. Post-Test Questions 5. False. It is the SPRINT (Systolic Blood Pressure Intervention Trial) and not the ACCORD (Action to Control Cardiovascular Disease Risk in Diabetes) key finding that lowering systolic blood pressure to 120 mmhg results in a 33% reduction in cardiovascular events and a 25% reduction in death.
36 Thank You
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
2/11/2019 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES DUALITY OF INTEREST
 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
New Hypertension Guidelines. Kofi Osei, MD
 New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
Summary, Scope, BP Classification, BP thresholds and Targets
 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/ PCNA Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults Summary, Scope, BP Classification, BP thresholds
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/ PCNA Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults Summary, Scope, BP Classification, BP thresholds
HTN talk_l Davis_ /28/2018
 1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Pharmacy Updates in Primary Care. Nathan Lamberton Assistant Professor
 Pharmacy Updates in Primary Care January 31 st, 2018 Nathan Lamberton Assistant Professor David N. Ombengi Associate Professor First Metformin, Then? AR is a 57 year old African American male with a PMH
Pharmacy Updates in Primary Care January 31 st, 2018 Nathan Lamberton Assistant Professor David N. Ombengi Associate Professor First Metformin, Then? AR is a 57 year old African American male with a PMH
Hypertension Update. ACOI 2018 John Prior
 Hypertension Update ACOI 2018 John Prior Disclosures Nothing to declare Hypertension - Introduction US population incidence 30% and growing due to an aging and increasingly obese population Poorly controlled
Hypertension Update ACOI 2018 John Prior Disclosures Nothing to declare Hypertension - Introduction US population incidence 30% and growing due to an aging and increasingly obese population Poorly controlled
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
Adult Blood Pressure Clinician Guide June 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups. Lisa Ivy APRN
 Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Clinical Recommendations: Patients with Periodontitis
 The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/
 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults American College of Cardiology Foundation and
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults American College of Cardiology Foundation and
HEART HEALTH UPDATE 2018
 HEART HEALTH UPDATE 2018 Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA 02/20/18 Heart Disease and Stroke Statistics Cardiovascular disease, is theeading cause of death in the US, accounts for nearly
HEART HEALTH UPDATE 2018 Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA 02/20/18 Heart Disease and Stroke Statistics Cardiovascular disease, is theeading cause of death in the US, accounts for nearly
The Road to Improve Cardiovascular Health after Cancer. S. Carolina Masri, MD Cardiology Division University of Washington, Seattle June 2 nd 2018
 The Road to Improve Cardiovascular Health after Cancer S. Carolina Masri, MD Cardiology Division University of Washington, Seattle June 2 nd 2018 Objective What are the cardiac complications in cancer
The Road to Improve Cardiovascular Health after Cancer S. Carolina Masri, MD Cardiology Division University of Washington, Seattle June 2 nd 2018 Objective What are the cardiac complications in cancer
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension JNC 8 (2014)
") Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations
 Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Hypertension with Comorbidities Treatment of Metabolic Risk Factors in Children and Adolescents
 Hypertension with Comorbidities Treatment of Metabolic Risk Factors in Children and Adolescents Stella Stabouli Ass. Professor Pediatrics 1 st Department of Pediatrics Hippocratio Hospital Evaluation of
Hypertension with Comorbidities Treatment of Metabolic Risk Factors in Children and Adolescents Stella Stabouli Ass. Professor Pediatrics 1 st Department of Pediatrics Hippocratio Hospital Evaluation of
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Managing Hypertension in 2018
 MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL
 CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD
 New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
major public health burden
 HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans
 Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
KDIGO Controversies Conference on Blood Pressure in CKD
 KDIGO Controversies Conference on Blood Pressure in CKD September 7-10, 2017 Edinburgh, Scotland Kidney Disease: Improving Global Outcomes (KDIGO) is an international organization whose mission is to improve
KDIGO Controversies Conference on Blood Pressure in CKD September 7-10, 2017 Edinburgh, Scotland Kidney Disease: Improving Global Outcomes (KDIGO) is an international organization whose mission is to improve
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
What s New? Hypertension Canada Guidelines for the Management of Hypertension
 What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
Hypertension Guidelines 2017
 Hypertension Guidelines 2017 (American College of Cardiology and the American Heart Association) In 1977, the 1st comprehensive guideline for detection, evaluation, and management of high BP was published,
Hypertension Guidelines 2017 (American College of Cardiology and the American Heart Association) In 1977, the 1st comprehensive guideline for detection, evaluation, and management of high BP was published,
Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127
 Hypertension in adults: diagnosis and management Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hypertension in adults: diagnosis and management Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Retour sur le congrès de l AHA 2017
 Retour sur le congrès de l AHA 2017 Paul Poirier MD, PhD, FRCPC, FACC, FAHA, FCCS Professeur Faculté de pharmacie Université Laval Responsable du programme de prévention/réadaptation cardiaque Canagliflozin
Retour sur le congrès de l AHA 2017 Paul Poirier MD, PhD, FRCPC, FACC, FAHA, FCCS Professeur Faculté de pharmacie Université Laval Responsable du programme de prévention/réadaptation cardiaque Canagliflozin
Renal Disease through the Ages: From Childbearing years to Old Age. Dr Elizabeth Jarvis, Renal Physician, General Physician, Obstetric Physician.
 Renal Disease through the Ages: From Childbearing years to Old Age Dr Elizabeth Jarvis, Renal Physician, General Physician, Obstetric Physician. Learning Outcomes: Understand the presentation of renal
Renal Disease through the Ages: From Childbearing years to Old Age Dr Elizabeth Jarvis, Renal Physician, General Physician, Obstetric Physician. Learning Outcomes: Understand the presentation of renal
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
TIP. Documentation and coding guide. Disease definitions* Prevalence and statistics associated with HTN**
 Documentation and coding guide Disease definitions* HTN is diagnosed when the average of two or more (systolic of diastolic) blood pressure readings are found to be elevated on two or more office visits
Documentation and coding guide Disease definitions* HTN is diagnosed when the average of two or more (systolic of diastolic) blood pressure readings are found to be elevated on two or more office visits
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH)
") Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Quality ID #122: Adult Kidney Disease: Blood Pressure Management National Quality Strategy Domain: Effective Clinical Care
 Quality ID #122: Adult Kidney Disease: Blood Pressure Management National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Intermediate
Quality ID #122: Adult Kidney Disease: Blood Pressure Management National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Intermediate
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
lyondellbasell.com Managing Hypertension
 Managing Hypertension Managing Hypertension There is a growing evidence that the good health of your heart and circulation will help you to age more successfully. A man is as old as his arteries Thomas
Managing Hypertension Managing Hypertension There is a growing evidence that the good health of your heart and circulation will help you to age more successfully. A man is as old as his arteries Thomas
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Strategies for Managing Hypertension
 Strategies for Managing Hypertension by Marsha K. Millonig, MBA, RPh President,Catalyst Enterprises, LLC E.L.F. Publications, Inc. is accredited by the Accreditation Council for Pharmacy Education as a
Strategies for Managing Hypertension by Marsha K. Millonig, MBA, RPh President,Catalyst Enterprises, LLC E.L.F. Publications, Inc. is accredited by the Accreditation Council for Pharmacy Education as a
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Dr Diana R Holdright. MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION.
 Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Hypertension Clinical case scenarios for primary care
 Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
American Diabetes Association: Standards of Medical Care in Diabetes 2015
 American Diabetes Association: Standards of Medical Care in Diabetes 2015 Synopsis of ADA standards relevant to the 11 th Scope of Work under Task B.2 ASSESSMENT OF GLYCEMIC CONTROL Recommendations: Perform
American Diabetes Association: Standards of Medical Care in Diabetes 2015 Synopsis of ADA standards relevant to the 11 th Scope of Work under Task B.2 ASSESSMENT OF GLYCEMIC CONTROL Recommendations: Perform
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Aquifer Hypertension Guidelines Module
 Aquifer Hypertension Guidelines Module 2018 Aquifer Hypertension Guidelines Module 1 1. Introduction. In 2013 the National Heart Lung and Blood Institute (NHLBI) asked the American College of Cardiology
Aquifer Hypertension Guidelines Module 2018 Aquifer Hypertension Guidelines Module 1 1. Introduction. In 2013 the National Heart Lung and Blood Institute (NHLBI) asked the American College of Cardiology
Primary hypertension in adults
 Primary hypertension in adults NICE provided the content for this booklet which is independent of any company or product advertised Hypertension Welcome NICE published an updated guideline on the diagnosis
Primary hypertension in adults NICE provided the content for this booklet which is independent of any company or product advertised Hypertension Welcome NICE published an updated guideline on the diagnosis
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Impact of Recent Hypertension Guidelines on Clinical Practice
 C H A P T E R 144 Impact of Recent Hypertension Guidelines on Clinical Practice NK Soni, VB Jindal The movement towards evidence-based healthcare has been gaining ground quickly over the past few years,
C H A P T E R 144 Impact of Recent Hypertension Guidelines on Clinical Practice NK Soni, VB Jindal The movement towards evidence-based healthcare has been gaining ground quickly over the past few years,
Randomized Design of ALLHAT BP Trial
 Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
RESISTANT HYPERTENSION
 RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
Primary and Secondary Prevention of Cardiovascular Disease. Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group
 Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Role of Minerals in Hypertension
 Role of Minerals in Hypertension Lecture objectives By the end of the lecture students will be able to Define primary and secondary hypertention and their risk factors. Relate role of minerals with hypertention.
Role of Minerals in Hypertension Lecture objectives By the end of the lecture students will be able to Define primary and secondary hypertention and their risk factors. Relate role of minerals with hypertention.
Hypertension and obesity. Dr Wilson Sugut Moi teaching and referral hospital
 Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI