Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
|
|
|
- Nicholas Nichols
- 5 years ago
- Views:
Transcription
1 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
2 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis and Etiology, In 2012, Prevalence patients: 5237 Age-standardised rate: 947.6pmp

3 Comparison of Unadjusted ESRD Prevalence Worldwide All rates are unadjusted. Data from Japan are dialysis only. USRDS 2013 Atlas of CKD & ESRD
. *Latest data for Taiwan are from 2010. ^^ Czech Republic: Data on incident ESRD due to diabetes is an estimate.")
4 Percentage of incident patients with ESRD due to diabetes, 2011 Data presented only for countries from which relevant information was available. All rates unadjusted. ^UK: England, Wales, & Northern Ireland (Scotland data reported separately). *Latest data for Taiwan are from ^^ Czech Republic: Data on incident ESRD due to diabetes is an estimate. Data for France include 25 regions in USRDS 2013 Atlas of CKD & ESRD
 Go et al et al.")
5 Age-standardised rate per 100 person years Rates of Death and Cardiovascular Events Rise as Renal Function Declines Death from any cause Cardiovascular events Estimated GFR (ml/min/1.73 m 2 ) Go et al et al. NEJM : 351(13):

6 The outcomes of patients with reduced GFR are uniformly poor Patients with CKD are more likely to die than go onto dialysis Early recognition of CKD permits intervention to alter the Natural History of the disease: renoprotection Cardio-vascular protection N Engl J Med 2004;351:
7 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients >85 Age Dialysis: male Dialysis: female General population: male General population: female Adapted from Levey AS et al. Am J Kidney Dis 1998; 32:



8 Cardiovascular Disease in CKD : Multifactorial Pathogenesis Elevated PTH/ 2 HPT Duration of dialysis Dyslipidemia Oxidative stress Hypertension Diabetes Mellitus Genetics High prevalence of traditional risk factors As renal Cardiovascular function deteriorates, nontraditional factors Disease play an increasing role in GFR loss and cardiovascular damage Anaemia Chronic inflammation Hyperphosphatemia Smoking Exogenous Ca intake Age Elevated Ca P product Traditional risk factors Non Traditional risk factors


 CKD")
9 What is Your Role as a Primary Care Physician in treating CKD? Know early Diagnose early Treat early Refer early Epidemiology of CKD Diagnosis of CKD Mortality and Morbidity Progression of (early) CKD Referral to nephrologist

10 Chronic Kidney Disease (CKD) Abnormalities of kidney structure or function, present for >3 months, with implications for health Nomenclature KDIGO 2012
 http://nkdep.nih.gov/lab-evaluation/gfr-calculators/adults-si-units.asp Ann Intern Med.")
11 GFR MDRD Calculator CKD-EPI GFR (ml/min/1.73 m 2 ) = 175 x (scr/88.4) x (Age) x (0.742 if female) x (1.212 if Black) Ann Intern Med Aug 15;145(4):247 54


12 Random urine tests for Macroscopic/ microscopic evaluation Persistent WBC or RBC; cellular casts KDOQI
13 Definitions of Abnormalities in Albumin Excretion Category Older Terms Spot Collection (mg/g Creatinine) 24-h collection(mg/24h) Timed collection (mcg/min) (Normoalbuminuria) <30 <30 <20 (Increase UAE) >=30 >=30 Moderately Increased Severely Increased (Microalbuminuria) (Macroalbuminuria) >300 >300 >300 Diagnosis of moderately increased albuminuria based of 2 out of 3 urine samples in the absence of UTI After 5 years of diagnosis in T1DM and than annually At the time of diagnosis in T2DM (2014) Diabetes Care American Diabetes (2004) Diabetes Care
14 Cardiovascular Disease in CKD : Multifactorial Pathogenesis Elevated PTH/ 2 HPT Duration of dialysis Dyslipidemia Oxidative stress Hypertension Diabetes Mellitus Genetics High prevalence of traditional risk factors As renal Cardiovascular function deteriorates, nontraditional factors Disease play an increasing role in GFR loss and cardiovascular damage Anaemia Chronic inflammation Hyperphosphatemia Smoking Exogenous Ca intake Age Elevated Ca P product Traditional risk factors Non Traditional risk factors
15 Strategies on Reduction of Progression of Early CKD Role of A Primary Physician 1. Control of blood pressure 2. Use of ACEI/ARB 3. Glycaemic control in DM 4. Control of dyslipidaemia 5. Protein restriction 6. Management of anaemia (CKD3 or above) 7. Control of CaPO4 (CKD 3 or above)
16 Strategies on reduction of progression of CKD 1. Control of blood pressure
17 Goal of BP control in CKD Reduction of Proteinuria Retardation of CKD progression Reduction of Mortality Reduction of CVD


")

")

18 Evaluation of BP Pre-HD CKD and PD Clinic BP (standard vs nonstandard) Home BP Ambulatory BP monitoring (ABPM) Haemodialysis patients Pre-HD Post-HD Home BP ABPM

19 Role of ABPM



20 Is home BP any better? n=217 CKD FU 3.5y DBP did not consistently correlate with outcomes across all BP assessment methods B Agarwal, Am J Nephrol 2006, 26: B Agarwal, KI, 65:
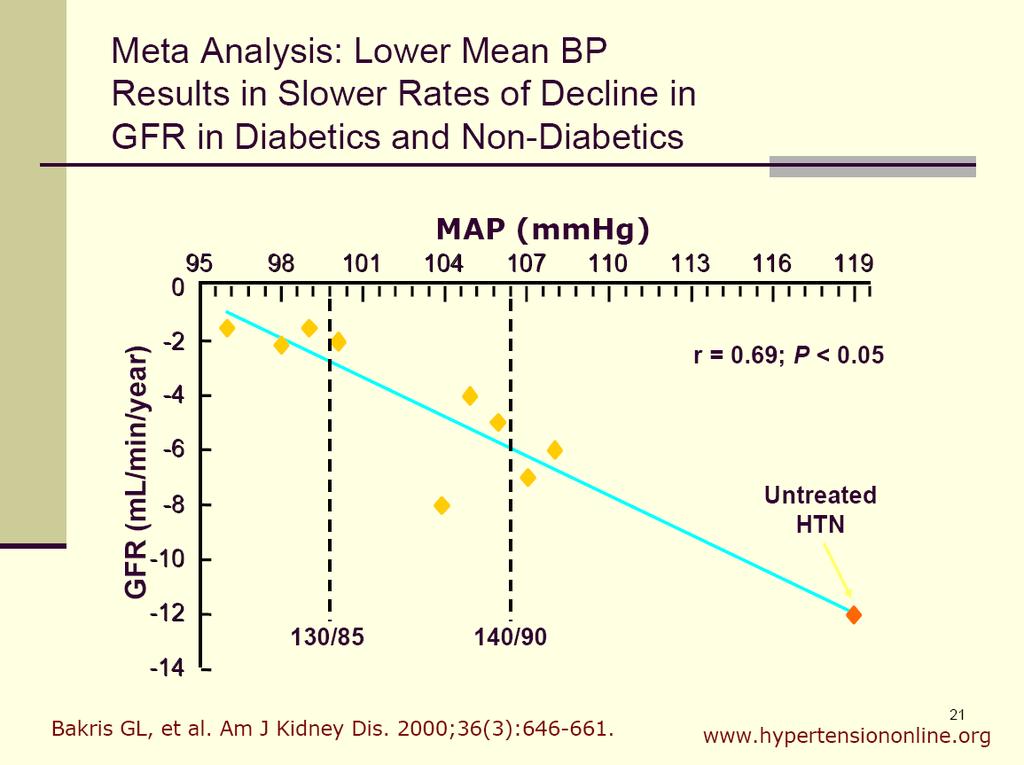
21
22 Blood Pressure Targets and Treatment Recommendations in CKD Guideline Blood pressure target in CKD without proteinuria Blood pressure target in CKD with proteinuria* Recommended first line medication USA JNC8 <140/<90 mmhg <140/<90 mmhg ACEI or ARB KDIGO <140/<90 mmhg <130/<80 mmhg ACEI or ARB NICE <140/<90 mmhg <130/<80 mmhg ACEI or ARB CHEP <140/<90 mmhg <140/<90 mmhg ACEI; ARB if ACEI intolerant ESC/ESH <140 mmhg <130 mmhg ACEI or ARB ASH/ISH <140/<90 mmhg <140/<90 mmhg ACEI or ARB ISHIB <130/<80 mmhg <130/<80 mmhg Diuretic or CCB
23 Strategies on reduction of progression of CKD 2. Use of ACEI/ARB
24 RAAS blockade- GFR decline at the expense of improvement in proteinuria Without RAAS blockade BP>140/90 Without RAAS blockade but BP 130/80 Baseline GFR Baseline proteinuria (g/day) With RAAS blockade BP 130/80 Expected GFR decline/year (normal decline 1mL/min/yr) 5-10mL/min/yr 4-6mmL/min/yr 2-3mL/min/yr GFR after 2 years Proteinuria after 2 years <1 Adapted from MDRD (Peter JC et al, Annal Intern Med 123: , 1994), RENAAL (Brenner BM et al, NEJM 345: , 2001) and IDNT (Lewis EJ et al, NEJM 329: , 2001) studies

25 Renin angiotensin aldosterone blocking trials Clinical trial Captopril trial Lewis EJ et al NEJM 1993 RENAAL-Reduction of Endpoints in NIDDM with Angiogen II Antagonist Losartan Brenner BM et al NEJM 2001 Irbesartan in Patients with DM2Nephropathy Diabetes trial Lewis EJ, NEJM 2001 DM number Type 1DM N=490 BP 135/86 UACR>0.5g/d Crt 220 No CV pts Type 2 DM N=1513 BP150/80 UACR 1.2g/d Crt 170 No CV pts Type 2 DM N=1715 BP 160/85 UACR 1.9g/d Crt 141 No CV pts Protocol FU Outcomes Captopril 25mg tds vs placebo Losartan mg vs placebo Monotherapy wih RAAS blockers slows progression of proteinuric DM nephropathy ARB preferable in type 2 DM CKD Irbesartan mg/d vs Amlodipine 10mg vs Placebo 3y Doubling of Crt 48% Cct 11±21 vs 17±20ml/min/y 3.5y UTP 36% Doubling of Crt 26% ESRD 28% GFR 4.4 vs 5.2ml/min/y 2.6y UTP 33% Doubling of Crt 33-37% ESRD 23% Cct 5.5 vs ml/min/y Cct= creatinine clearance
 noninferior; combination (16.3%) not superior to ramipril (16.")

26 Combinations and SAE (ONTARGET) patients Telmisartan vs. Ramipril vs. combinations Temisartan (16.7%) noninferior; combination (16.3%) not superior to ramipril (16.5%) for primary endpoints (CV death, MI, stroke, heart failure) Combination groups Increased risk of hypotensive symptoms, syncope and renal dysfunction (13.5% vs. 10.2%, P<0.001) Combination drugs more adverse events without an increase in benefit Investigators, Yusuf et al. (2008) N Engl J Med
27 Double RAAS combination trials Clinical trial ONTARGET Yusuf et al, NEJM 2008 VA-NEPHRON- Friend LF et al, NEJM 2013 ALTITUDE Parving HH et al, NEJM 2012 DM number N=25,620 CV pts 85% DM 38% BP 69% Microalb 13% Protocol FU Outcomes Ramipril mg/d vs Telmisartan 40-80mg/d vs combo 2.2y AKI 10.2vs 10.6vs 13.5% Acute dialysis 0.6vs 0.6 vs 0.8% K 3 vs 3 vs 5.6% Type 2 DM N=1448 Losartan mg/d vs 2.2y ΔUACR 128 vs 269 mg/g Dual therapy Crt 132 wih RAAS blockers Lisinopril aggravates (10- renal function in GFR 2.7 vs mildly to UACR moderately 0.9g/d proteinuric 40mg/d) CKD + patients Losartan with high CV 2.9ml/min/yr burden. No BP 137/72 evidence it is harmful in severely proteinuric CKD. ESRD 5.9 vs 3.7% CV pts 38% AKI 11 vs 18% K 4.4 vs 9.9% N= 8561 Type 2 DM CV pts 42.3% UACR 0.2g/d BP 137/74 GFR 57ml/min ACE-I/ARB vs Alikirein mg/d + ACEi/ARB 32.9m Crt 5.1 vs 4.9 K 2.6vs 4.8% ESRD 2.8 vs 2.6 BP 8.3vs 9.8%
28 RAAS Inhibition: What we know Decrease risk of progression from Normoalbuminuria to microalbuminuria Microalbuminuria to overt nephropathy Overt nephropathy to ESRD ACEI comparable to ARB GFR drops by 10% before plateauing Combination therapy is effective in reducing proteinuria; effects on slowing progression is questionable
29 Hyperkalaemia (K>5.5) Dietary indiscretion-eg bananas, potatoes, coconut and Nyoni juice Or NSAIDs, dehydration, absence of a kalliuretic diuretic (thiazide or frusemide) If K 5.5-6, review diet, K binding resins ± hold of RAAS blocker temporarily Longterm K binding resins- Resonium/Kayalexate/ Partiromer/Zirconium cyclosilicate
30 Rising creatinine Always check creatinine 1-2 weeks after starting or changing RAAS blocker <30% is acceptable 30% -dehydration, recent hypotension, ischaemia, NSAID, interstitial nephritis Screening for renal artery stenosis Hold off agent and review in 2-4 weeks and thiazide dose to 12.5mg
31 Strategies on reduction of progression of CKD 3. Glycaemic control in DM
 N Engl")
32 Intensive Diabetes Management UAE > 40mg/d No retinopathy Retinopathy UAE > 300mg/d 1441 IDDM patients 2-3x increase in hypoglycaemia Reduced microalbuminuria by 39% for both groups Reduced macroalbuminuria by 54% for retinopathy group 60% reduction in clinical nephropathy (1993) N Engl J Med
33 Randomised propective trial of treatment strategies in T2DM 5102 patients patient years follow-up Intensive HbA1c 7% 7.9% Conventional Each 1% decrease in HbA1c decreases microvascular complications by 35% Strict BP control decreases microvascular complications (1998) Lancet
 a target hemoglobin A1c (HbA1c) of about 7.")
34 Intensive Insulin/OHA Therapy Partially reverse the glomerular hypertrophy and hyperfiltration Delay the development of elevated albumin excretion Stabilize or decrease protein excretion in patients with increased albumin excretion Slow the progression of glomerular filtration rate decline Recommendation (KDIGO 2012) a target hemoglobin A1c (HbA1c) of about 7.0% to prevent or delay progression of the microvascular complications of diabetes, including diabetic kidney disease. (1A)
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Interventions to reduce progression of CKD what is the evidence? John Feehally
 Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
6/10/2014. Chronic Kidney Disease - General management and standard of care. Management of CKD according to stage (KDOQI 2002)
") Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA
 ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
The hypertensive kidney and its Management
 The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
(renoprotective (end-stage renal disease, ESRD) therapies) (JAMA)
 therapies) (JAMA)") [1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
[1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Chronic Kidney Disease for the Primary Care Physician in What do the Kidneys do? CKD in the US
 1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
New Treatment Options for Diabetic Nephropathy patients. Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
 New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Diabetic Kidney Disease in the Primary Care Clinic
 Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Hypertension and diabetic nephropathy
 Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC.
 Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC. Objectives Review CKD and its implications for the family physician Review the relevance of CKD and ESRD, its complications and management issues in
Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC. Objectives Review CKD and its implications for the family physician Review the relevance of CKD and ESRD, its complications and management issues in
Renoprotective Strategies in Clinical Practice. Dr Michael Clarkson
 Renoprotective Strategies in Clinical Practice Dr Michael Clarkson The Silent Epidemic? ESRD CKD 5% of a UK population Staging of Chronic Kidney Disease Stage Description GFR Evaluation / Plan 0 At risk
Renoprotective Strategies in Clinical Practice Dr Michael Clarkson The Silent Epidemic? ESRD CKD 5% of a UK population Staging of Chronic Kidney Disease Stage Description GFR Evaluation / Plan 0 At risk
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERENCE CARDS Chronic Kidney Disease
 PROVIDER REFERENCE CARDS Chronic Kidney Disease") VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
Kidney Disease, Hypertension and Cardiovascular Risk
 1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
Keywords albuminuria, hypertension, nephropathy, proteinuria
 Should proteinuria reduction be the criterion for antihypertensive drug selection for patients with kidney disease? Rigas G. Kalaitzidis and George L. Bakris Department of Medicine, Hypertensive Diseases
Should proteinuria reduction be the criterion for antihypertensive drug selection for patients with kidney disease? Rigas G. Kalaitzidis and George L. Bakris Department of Medicine, Hypertensive Diseases
Effective Health Care Program
 Comparative Effectiveness Review Number 37 Effective Health Care Program Chronic Kidney Disease Stages 1 3: Screening, Monitoring, and Treatment Executive Summary Objectives This systematic review evaluates
Comparative Effectiveness Review Number 37 Effective Health Care Program Chronic Kidney Disease Stages 1 3: Screening, Monitoring, and Treatment Executive Summary Objectives This systematic review evaluates
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
CARDIO-RENAL SYNDROME
 CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Diabetic Nephropathy 2009
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Morbidity & Mortality from Chronic Kidney Disease
 Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Renal Protection Staying on Target
 Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 7/23/2013. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Management of Hypertension in Diabetic Nephropathy: How Low Should We Go?
 Review Advances in CKD 216 Published online: January 15, 216 Management of Hypertension in Diabetic Nephropathy: How Low Should We Go? Hillel Sternlicht George L. Bakris Department of Medicine, Section
Review Advances in CKD 216 Published online: January 15, 216 Management of Hypertension in Diabetic Nephropathy: How Low Should We Go? Hillel Sternlicht George L. Bakris Department of Medicine, Section
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
RATIONALE. chapter 4 & 2012 KDIGO
 http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers. Robert D. Toto, MD
 R e v i e w P a p e r Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers Robert D. Toto, MD Both the prevalence and incidence of end-stage renal disease have been increasing
R e v i e w P a p e r Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers Robert D. Toto, MD Both the prevalence and incidence of end-stage renal disease have been increasing
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
University of Groningen. Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste
 University of Groningen Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
University of Groningen Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
Outline. Outline. Introduction CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 8/11/2011
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Hot Topics in Diabetic Kidney Disease a primary care perspective
 Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Renin-Angiotensin-Aldosterone System Blockade in Diabetic Nephropathy. Present Evidences
 J. Clin. Med. 2015, 4, 1908-1937; doi:10.3390/jcm4111908 Review OPEN ACCESS Journal of Clinical Medicine ISSN 2077-0383 www.mdpi.com/journal/jcm Renin-Angiotensin-Aldosterone System Blockade in Diabetic
J. Clin. Med. 2015, 4, 1908-1937; doi:10.3390/jcm4111908 Review OPEN ACCESS Journal of Clinical Medicine ISSN 2077-0383 www.mdpi.com/journal/jcm Renin-Angiotensin-Aldosterone System Blockade in Diabetic
CKD and CVD. Jamal Salameh, MD, FACP, FASN First Coast Nephrology
 CKD and CVD Jamal Salameh, MD, FACP, FASN First Coast Nephrology An Epidemic of Kidney Disease Prevalence CKD stages 1-4 10% 1988-94 13% 1999-2004 Coresh, JAMA 298:2038, 2007 Stage 5: GFR
CKD and CVD Jamal Salameh, MD, FACP, FASN First Coast Nephrology An Epidemic of Kidney Disease Prevalence CKD stages 1-4 10% 1988-94 13% 1999-2004 Coresh, JAMA 298:2038, 2007 Stage 5: GFR
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease
 Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Managing patients with renal disease
 Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
Primary Care Approach to Management of CKD
 Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low
Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D.
 Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Outline. Introduction. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 6/26/2012
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Chronic Kidney Disease in Primary Care
 Clinical Stream Chronic Kidney Disease in Primary Care Dr Gerald Waters Dr Gerald Waters Renal Physician Chronic Kidney Disease Chronic Kidney Disease Normal functions of Kidneys Management of CKD Drugs
Clinical Stream Chronic Kidney Disease in Primary Care Dr Gerald Waters Dr Gerald Waters Renal Physician Chronic Kidney Disease Chronic Kidney Disease Normal functions of Kidneys Management of CKD Drugs
Management of Early Kidney Disease: What to do Before Referring to the Nephrologist
 Management of Early Kidney Disease: What to do Before Referring to the Nephrologist Andrew S. Narva, MD, NIDDK Saturday, February 18, 2017 8:45 a.m. 9:30 a.m. Although evidence-based guidelines for managing
Management of Early Kidney Disease: What to do Before Referring to the Nephrologist Andrew S. Narva, MD, NIDDK Saturday, February 18, 2017 8:45 a.m. 9:30 a.m. Although evidence-based guidelines for managing
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection
 SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
Prevention and management of chronic kidney disease in type 2 diabetes
 162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
The CARI Guidelines Caring for Australasians with Renal Impairment. Antihypertensive therapy in diabetic nephropathy GUIDELINES
 Antihypertensive therapy in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Adequate control of blood pressure (BP) slows progression
Antihypertensive therapy in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Adequate control of blood pressure (BP) slows progression
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Chronic kidney disease-what can you do and when to refer?
 Chronic kidney disease-what can you do and when to refer? Dr Goh Heong Keong www.passpaces.com/kidney.htm Outline of Lecture Introduction Epidemiology of CKD in Malaysia/ World Complications of CKD What
Chronic kidney disease-what can you do and when to refer? Dr Goh Heong Keong www.passpaces.com/kidney.htm Outline of Lecture Introduction Epidemiology of CKD in Malaysia/ World Complications of CKD What
Diabetes and kidney disease.
 Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Case #1. Current Management Strategies in Chronic Kidney Disease. Serum creatinine cont. Pitfalls of Serum Cr
 Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
Chronic Kidney Disease
 Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
What should you do next? Presenter Disclosure Information. Learning Objectives. Case: George
 2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
The CARI Guidelines Caring for Australasians with Renal Impairment. Protein Restriction to prevent the progression of diabetic nephropathy GUIDELINES
 Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영
 만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영 Contents Introduction Lifestyle and Pharmacological Tx CKD ND ptswithout diabetes CKD ND ptswith diabetes In elderly ptswith CKD ND 2013 대한고혈압학회진료지침 JNC 8th Introduction
만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영 Contents Introduction Lifestyle and Pharmacological Tx CKD ND ptswithout diabetes CKD ND ptswith diabetes In elderly ptswith CKD ND 2013 대한고혈압학회진료지침 JNC 8th Introduction
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension)
") Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
KDIGO conference on high CV risk associated with CKD. The role of BP in CKD stage 1-4
 KDIGO conference on high CV risk associated with CKD The role of BP in CKD stage 1-4 Johannes Mann, MD & Catherine Clase, MB BChir Friedrich Alexander University, Erlangen-Nuremberg Munich General Hospitals,
KDIGO conference on high CV risk associated with CKD The role of BP in CKD stage 1-4 Johannes Mann, MD & Catherine Clase, MB BChir Friedrich Alexander University, Erlangen-Nuremberg Munich General Hospitals,
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus
 Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
The National Quality Standards for Chronic Kidney Disease
 The National Quality Standards for Chronic Kidney Disease Dr Robert Lewis Chief of Service, Wessex Kidney Centre, Portsmouth Specialist Committee Member Quality Standard for Chronic Kidney Disease, NICE
The National Quality Standards for Chronic Kidney Disease Dr Robert Lewis Chief of Service, Wessex Kidney Centre, Portsmouth Specialist Committee Member Quality Standard for Chronic Kidney Disease, NICE
Faculty/Presenter Disclosure
 CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
Outpatient Management of Chronic Kidney Disease for the Internist
 Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Cardiovascular Protection and the RAS
 Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
Updates in Chronic Kidney Disease Management. Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG
 Updates in Chronic Kidney Disease Management Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG No disclosures Research Funding: NIH, Blue Shield of California Foundation Objectives
Updates in Chronic Kidney Disease Management Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG No disclosures Research Funding: NIH, Blue Shield of California Foundation Objectives
Update on HIV-Related Kidney Diseases. Agenda
 Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Caring for Australians with Renal Impairment. BP lowering and CVD
 Caring for Australians with Renal Impairment BP lowering and CVD Questions: Conflicts of Interest: RH, TN, HHL- no conflict VP- level II conflict Speakers fees: Abbott, Astra Zeneca, Roche, Servier Grant
Caring for Australians with Renal Impairment BP lowering and CVD Questions: Conflicts of Interest: RH, TN, HHL- no conflict VP- level II conflict Speakers fees: Abbott, Astra Zeneca, Roche, Servier Grant
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression
 CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
CKD IN THE CLINIC. Session Content. Recommendations for commonly used medications in CKD. CKD screening and referral
 CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient
CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient