MEDICATION MANAGEMENT IN VTE FROM CONVENTIONAL TO NEW
|
|
|
- Tyrone Ford
- 5 years ago
- Views:
Transcription
1 MEDICATION MANAGEMENT IN VTE FROM CONVENTIONAL TO NEW Presented by: David B. Coriale RPh. Pharm D BCPS Clinical Pharmacy Manger Oneida Healthcare Oneida, NY
2

3
4 Presentation John is a 75-year-old man with a recent (4 weeks ago) admission to hospital for hip replacement. The procedure was performed under general anaesthetic. During admission John received the following VTE prophylaxis (to be continued until John no longer had significantly reduced mobility): antiembolism stockings pharmacological VTE prophylaxis. John reports that his right leg has been swollen for over 2 weeks. He thought it was healing after the operation, which is why he has not told anyone sooner. He presented to his FP and the FP has referred him to your ER.
5 John reports that he had a DVT 20 years ago and that he has osteoarthritis. On admission he is apyrexial with a temperature of 37oc and his right calf and ankle are red, blotchy and swollen with pitting edema. His heart rate is 80 beats per minute, respiratory rate 15 breaths per minute, blood pressure is 136/80 mmhg and SpO2 96% in air. Question: You suspect DVT: what medication do you start?
6 Discuss conventional vs. NOAC dosing, interactions and pharmacology Understand risks and benefits for therapy Make a decision on the type of therapy based on the clinical situation Transition to outpatient
7

8 Anticoagulant Selection Algorithm Copyright 2016 by Society of Hospital Medicine. accessed 4/17/18

9 Initiation of Anticoagulation for Acute VTE Copyright 2016 by Society of Hospital Medicine. accessed 4/17/18
10 Presentation Jane is a 65-year-old woman with inoperable ovarian cancer and poor functional status. She presents to your ER following a referral from the oncology outpatient clinic. She complains of pain along the length of her left leg with her left calf feeling particularly painful. She also reports that her left calf feels hot. Question You believe Jane has symptoms of a suspected DVT. What s important in her background?
11 LMWH or fondaparinux suggested if DOAC not possible UFH reserved for: Potential need for invasive procedures Potential for thrombolysis Increased bleeding risk as it has a short ½ life Possible need for reversal Severe renal impairment
12 LMWH monotherapy for first 3-6 months Superior efficacy and safety DOAC trials only evaluated a small number of patients with active malignancy DOAC or warfarin may be used if patient refuses LMWH
13 DOAC not studied in thrombophilia Not enough data to conclude efficacy of DOACs LMWH plus warfarin titration until INR 2-3 recommended

14 Table 6. Effect of Thrombosis and Medications on Thrombophilia Test Results - Laboratory Test for: Factor V Leiden Factor II gene mutation Protein S deficiency Protein C deficiency Antithrombin deficiency Antiphospholipid antibody Lupus anticoagulant 1 LMWH, low-molecular-weight heparin Medications Acute Vitamin K Direct lla Direct Xa Thrombosis Heparin LMWH 1 Antagonist Inhibitor Inhibitor No effect No effect No effect No effect No effect No effect No effect No effect No effect No effect No effect No effect May be low No effect No effect Don t test No effect No effect May be low No effect No effect Don t test No effect No effect May be low Lowered Lowered No effect No effect No effect No effect No effect No effect No effect No effect No effect No effect Don t test Don t test Don t test Don t test Don t test Copyright 2016 by Society of Hospital Medicine. accessed 4/17/18
15 DOAC studies for VTE did not adequately evaluate patients below 40 kg or above 120 kg Fixed doses of DOAC may lead to over or under treatment Edoxaban dose is reduced to 30 mg if patient is <60 kg Fondaparinux (Arixtra ) is contraindicated if patient <50kg Extreme low weight may lead to overtreatment and bleeding complications even at prophylactic doses
16 LMWH, fondaparinux, and DOACs are renally cleared thus not recommended if CrCl < 30 ml/min UFH bridged to warfarin is recommended
17 Apixaban (Eliquis): Age 80 or above PLUS serum creatinine of 1.5 or above
18
19 Active bleeding Severe bleeding diathesis Platelet count <50,000/microL Recent, planned, or emergent high bleeding-risk surgery/procedure Major trauma History of intracranial hemorrhage (ICH) particularly recent ICH
20 Initial therapy (first 10 days) Weigh risk of bleed vs. benefit of therapy PE or DVT Asymptomatic vs. symptomatic Inpatient or Outpatient
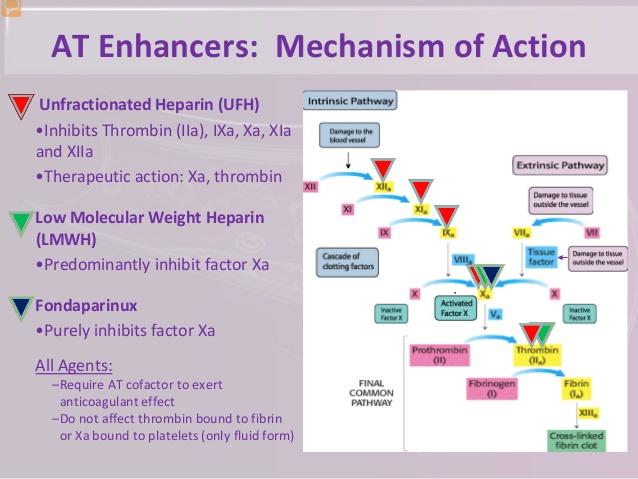
21 Unfractionated Heparin (UFH) Low molecular weight heparin (LMWH) Fondaparinux (Arixtra ) Addition of Warfarin
22 Significant shift in treatment Pharmacokinetics similar to LMWH Parenteral lead in needed only for edoxaban and dabigatran Apixaban and rivaroxaban do not need bridging just initial higher dosing Less labor intensive
23
24
25 Protocol Driven Optimal initial dosing of continuous infusion heparin therapy is controversial Route Reference Bolus dose Maintenance dose Continuous infusion Fixed dose Hull et al. [1] 5000 units units/h a Weight based Raschke et al. [6] 80 units/kg 18 units/kg/h
26 aptt or heparin anti-xa level monitoring may be used Check every 6 hours until two consecutive therapeutic results are obtained, after which the frequency of monitoring can be extended to once daily
27 obese/morbidly obese patient either total body weight or adjusted body weight can be used no increased risk of major bleeding has been reported when morbidly obese patients are managed using total body weight studies have not included patients weighing above 270 kg prompt attention to initial laboratory results is warranted to ensure the therapeutic threshold is exceeded in a timely manner
28 Twice daily dosing Exception severe renal disease all patients, including underweight and obese, LMWH dosing should be based on total body weight For patients <40 kg, UFH may be more appropriate enoxaparin dosing in obese patients, 1 mg/kg BID is preferred over 1.5 mg/kg daily Routine monitoring of peak anti-xa levels is not suggested
29 Renal function should be estimated using the Cockcroft-Gault method In patients with a CrCl < 30 ml/min the use of UFH may be preferred over LMWH If enoxaparin is used, it should be dosed at 1 mg/kg daily May consider a trough anti-xa measurement in patients with severe renal dysfunction if LMWH used beyond 5 7 days of treatment LMWH should be avoided in patients with CrCl < 20 ml/min and those receiving renal replacement therapy.
30 An immune-mediated disorder Typically occurs 4-10 days after exposure to heparin and has life- and limb-threatening thrombotic complications. Previous exposure to heparin can cause HIT to develop earlier May switch to fondaparinux (Arixtra ) Avoid fondaparinux in weight 50kg or CrCl 30 ml/min Alternatives: Argatroban or bivalirudin(angiomax )
![Table 3 History of ACCP recommendations for overlapping parenteral anticoagulants with warfarin for the treatment of VTE Year VTE recommendation Level of evidence 2001 [41] 2004 [10] 2008 [32] 2012](/docs-images/85/92765795/images/31-0.jpg "[11] Treat with heparin or LMWH for at least 5 days and overlap with heparin or LMWH for at least 4-5 days Initiate vitamin K antagonist with LMWH or hepahn on day one and discontinue heparin when")
31 Table 3 History of ACCP recommendations for overlapping parenteral anticoagulants with warfarin for the treatment of VTE Year VTE recommendation Level of evidence 2001 [41] 2004 [10] 2008 [32] 2012 [11] Treat with heparin or LMWH for at least 5 days and overlap with heparin or LMWH for at least 4-5 days Initiate vitamin K antagonist with LMWH or hepahn on day one and discontinue heparin when INR is stable and >2.0 Treat with LMWH, heparin or fondaparinux for at least 5 days and until the INR is 2 for 24 h Recommend early initiation of vitamin K antagonist (same day as parenteral is started) over delayed initiation, and until the INR is 2.0 or above for at least 24 h 1A (in comparison to treatment for 10 days) 1A 1C 1B
32 Started on the same day with LMW heparin or UFH (day 1) Typical initiating dose of 5 mg/day for the first two days (range 2 to 10 mg/day) Dosing is then adjusted until the INR is within the therapeutic range (2 to 3; target 2.5) for two consecutive days Initial doses at the lower range (2 to 5 mg/day) may be considered for high bleeding risk (eg, older adults) Doses in the higher range (5 to 10 mg/day) may be for low risk for bleed
33 Premature discontinuation of heparin (prior to therapeutic INR for two days) may result in inadequate protection against recurrent thrombosis Overlap is required because it takes a time for all of the vitamin K-dependent factors to become depleted (factors II, VII, IX, and X) During the first few days of warfarin therapy, prolongation of the prothrombin time mainly reflects the depression of factor VII Takes approximately five days of adequate dosing to reach therapeutic level Reduction of protein C and S occurs shortly after warfarin therapy and potentially renders a procoagulant state.

34 Suggested protocol for initiating warfarin therapy IN Ft INR Days of warfarin INR INR 1.5 to 2.0 to treatment <1.5 > Suggested initial dose tor days 1 and 2 Normal adult 5 mg* n/a n/a n/a Frail adult, malnourished, elderly, liver disease 2.5 mg* n/a n/a n/a Dosing for day 3 and beyond Day 3 5 to mg 2.5 to mg 0 to mg No dose Day 4 10 mg 5 to 0 to No dose Day 5 10 mg 7.5 to 0 to No dose mg mg 10 mg mg Day to 5 to 0 to No dose 12.5 mg mg mg In this protocol, which is provided for guidance only, suggested doses of warfarin after day 2 are given as ranges. The clinician must judge the rapidity and magnitude of INR changes for the individual patient and make dosage adjustments accordingly. An algorithm for monitoring and adjustment of maintenance warfarin is presented separately. Refer to UpToDate topics on use of warfarin and table on suggested protocol for adjustment of maintenance warfarin. n/a: not applicable. * This table assumes that the patient has started with an INR in the normal range. Copyrights apply See text for details concerning the source for this protocol and relevant references. UpToDate

35 Table 4 Transitions from parenteral to oral anticoagulants in the treatment of VTE To warfarin To dabigatran or edoxaban To rivaroxaban or apixaban Initial Required Required Not required parenteral therapy From Start warfarin and Start heparin alone Stop heparin heparin heparin concurrently Continue heparin for a After a minimum of 5 days of Give first dose of rivaroxaban or minimum of 5 days heparin, start dabigatran or apixaban AND until INR > 2.0 edoxaban and stop heparin From Start warfarin and Start LMWH/fondaparinux alone Stop LMWH/fondaparinux LMWH or fondaparinux LMWH foudaparinux concurrently After a minimum of 5 days, stop LMWH fondaparinux Continue Give first dose of dabigatran or Give first dose of rivaroxaban or LMWH' foudaparinux edoxaban at the time the next dose apixaban at the time the next dose of for a minimum of of LMWH/fondaparinux would LMWH/fondaparinux would have 5 days AND until have been given been given rnr>2.g

36 Free yourself from - conventional thinking
37 Presentation Gary is a 52-year-old man who is an endurance cyclist. He presents to your ER following referral from his FP. He reports shortness of breath at rest and chest pain. On direct questioning he admits to pain in the right calf for a month, which he put down to muscle sprain. Question You believe Gary has symptoms of a suspected PE and DVT. What DOAC can be used?
38 Medication Approved Date Dabigatran (Pradaxa ) 2014 Rivaroxaban (Xarelto ) 2010,2011 Apixaban (Eliquis ) 2014 Edoxaban (Savayasa ) 2015
39 Simple dosing and regimen No dietary restrictions Decreased drug interactions No routine monitoring Less labor for staff Less impact on quality of life Possible improved safety and efficacy
40 Compliance Review contraindications Health literacy Renal and liver function Drug-interactions Disease interactions
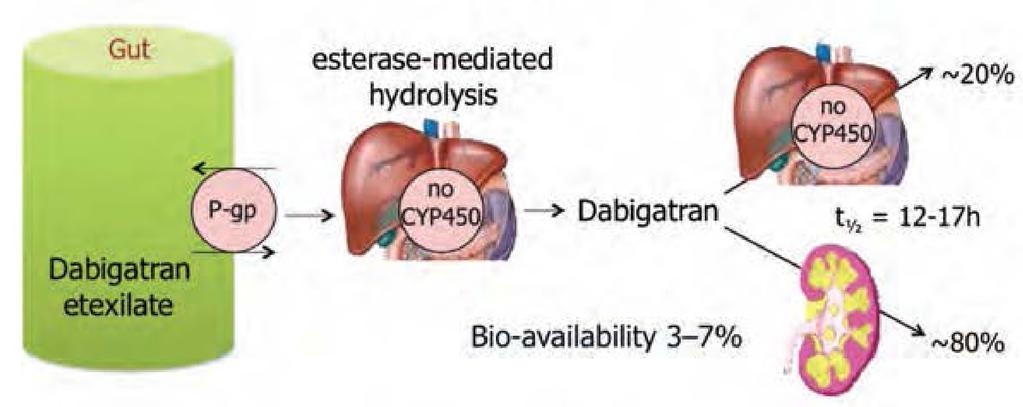
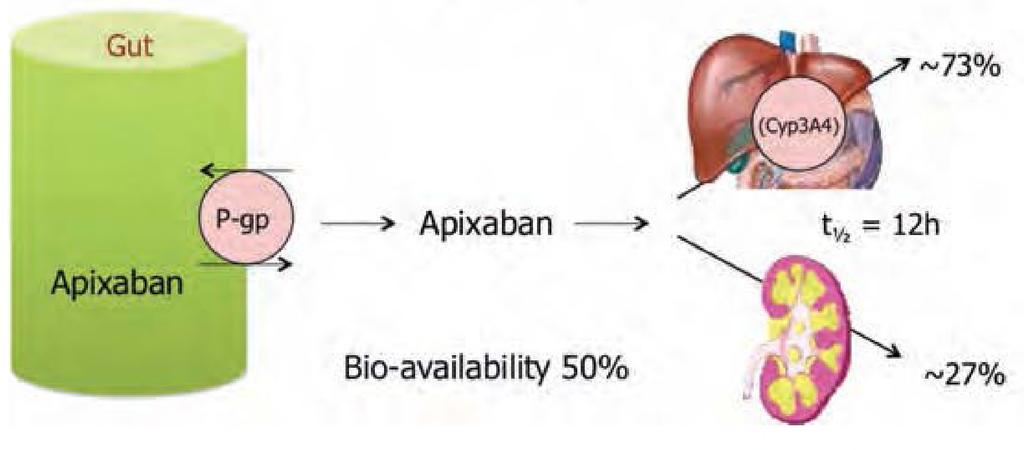
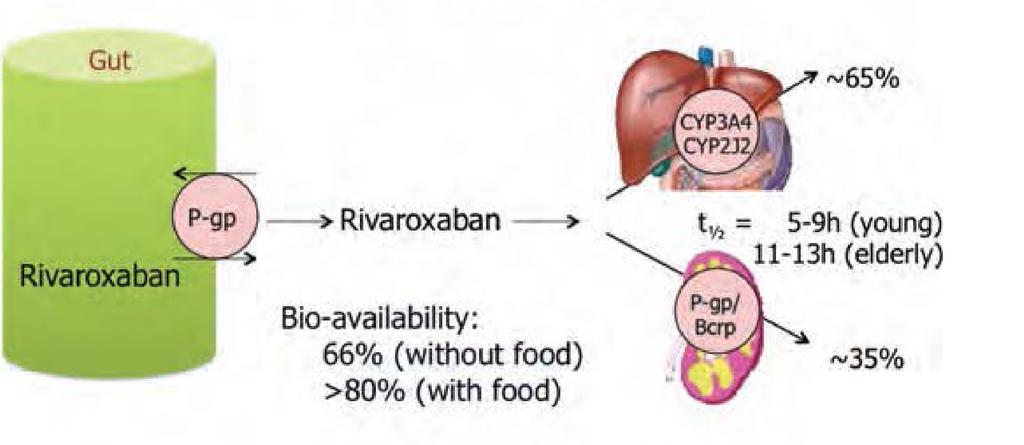
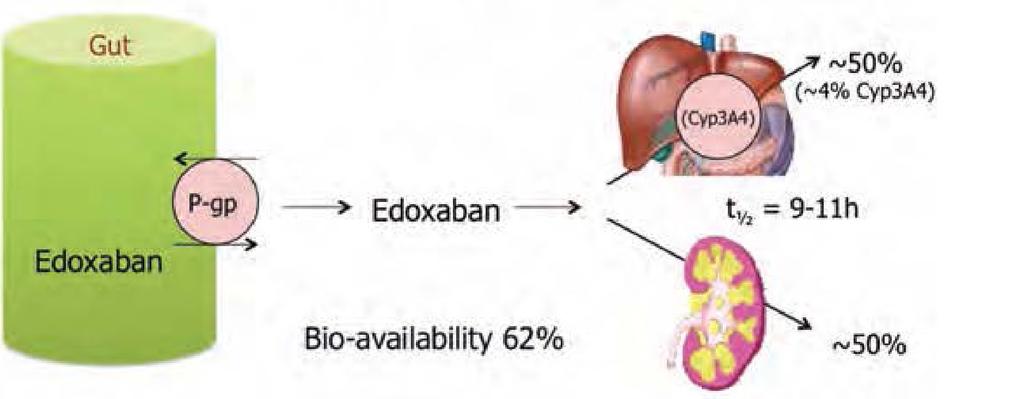
41 Medication Target Renal Clearance Half-Life Metabolism Dabigatran (Pradaxa ) Rivaroxaban (Xarelto ) Apixaban (Eliquis ) Edoxaban (Savayasa ) Thrombin 80% 14-17h P-gp Xa 33% 7-11h CYP3A4 & P-gp Xa 25% 8-12h CYP3A4 & P-gp Xa 35% 8-10h CYP3A4 & P-gp
 Liver metabolism: CYP3A4 involved No Yes (elimination; minor Minimal (<4% of elimination) Yes")
42 Table 4 Absorption and metabolism of the different NOACs Dabigatran Apixaban Edoxaban a Rivaroxaban Bio-availability 3-7% 50% 62% 17 66% without food Prodrug Yes No No No Clearance non-renal/renal of 20%/80% 73%/27% 13 50%/50% 9 65%/35% absorbed dose (if normal renal function; see also Section 8) Liver metabolism: CYP3A4 involved No Yes (elimination; minor Minimal (<4% of elimination) Yes (elimination) CYP3A4 contribution) 19 Absorption with food Intake with food recommended? Absorption with H2B/PPI Asian ethnicity Gl tolerability Elimination half-life No effect No % % 24 Dyspepsia 5-10% No effect No No effect No effect No problem 6-22% more 20 No official recommendation yet No effect No effect 20 No problem +39% more 21 Mandatory Almost 100% with food No effect21, 25 No effect No problem h h 9-11 h h (young) h (elderly) a No EMA approval yet. Needs update after finalization of SmPC. H2B, H2-blocker; PPI, proton-pump inhibitor; Gl, gastro-intestinal. Europace (2013) 15, doi: /europace/eut083
43 Medication Dosing CrCl (Cockcroft-Gault ml/min) Dabigatran (Pradaxa )* 150 mg bid after 5-10 days of parenteral Above Less than 15 Renal Dose Adjustments for maintenance Normal Dose 75 mg BID Not Recommended Rivaroxaban (Xarelto )* 15 mg bid w/food for 21 days then 20 mg daily with food Above Normal Dose 15 mg Daily with evening meal Apixaban (Eliquis ) # 10 mg bid for 7 days then 5 mg bid Must meet 2 factors: Age above 80, Scar 1.5 or weight 60kg 2.5 mg twice a day Edoxaban (Savayasa )* Above 60 kg 60 mg daily 60 kg 30 mg daily *End stage CKD with or w/o dialysis Not recommended # End stage CKD with or w/o dialysis No recommendations Less than 15 CrCL >95 ml/min 60 mg once a day Do NOT USE Do NOT USE
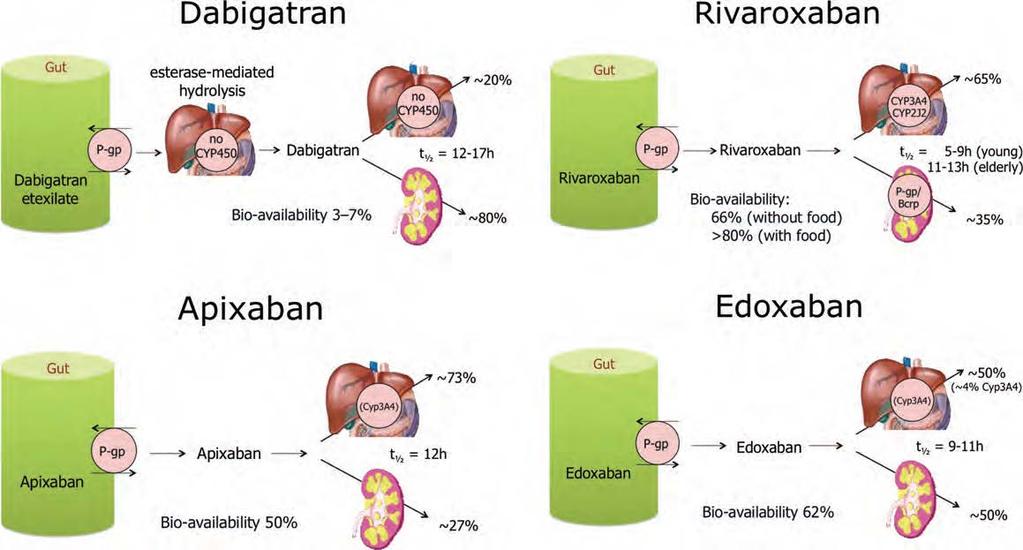
44 Dabigatran Rivaroxaban Apixaban Edoxaban Europace (2013) 15, doi: /europace/eut083
 reduce dose")
45 Drug-Drug Interaction Effects on NOAC - Plasma Levels, and Recommendations - Atorvastatin via Dabigatran Apixaban Edoxaban Rivaroxaban P-gp weak +18% no data no effect no effect CYP3A4 Digoxin p-gp no effect no data no effect no effect p-gp % Verapamil weak reduce dose no data CYP3A4 take together Diltiazem Quinidine p-gp weak CYP3A4 p-gp no effect +50% +40% no data +53% (SR) reduce dose no data +80% reduce dose Amiodarone p-gp % no data no effect Dronedarone p-gp weak CYP3A % no data +88% reduce dose minor effect use with caution if CrCL: 15-50ml/min minor effect use with caution if CrCL: 15-50ml/min +50% minor effect use with caution if CrCL: 15-50ml/min No data yet Heidbuchel H, et al. Europace. 2013;15: [31] Not recommended/contraindicated Reduce dose if 2 factors or more Reduce dose No data yet

46 Possible drug-drug interactions - Effect on NOAC plasma levels part 2 Interaction Dabigatran Apixaban Edoxaban Rivaroxaban Fluconazole CYP3A4 no data no data no data +42% Cyclosporin; tacrolimus - Clarithromycin; - erythromycin - HIV protease inhibitors P-gp no data no data no data +50% P-gp/ CYP3A4 P-gp and BCRP/ CYP3A % no data no data % no data strong increase no data no data up to +153% Rifampicin; - St John's wort; carbamezepine; phenytoin; phenobarbital - P-gp and BCRP/ CYP3A4/CYP2J2-66% -54% -35% up to -50% Antacids GI absorption % no data no effect no effect Red - contraindicated; orange - reduce dose; yellow - consider dose reduction if another yellow factor present; - hatching - no data available; recommendation made from pharmacokinetic considerations -
47

48 Care transitions associated with adverse events - of readmissions that occur within one year after a hospitalization are related 20 % to an adverse drug event % of all medication errors times of care transition. 2 occur during 72% of post-discharge medication-related. 2 adverse events are 1 New England Journal of Medicine. Adherence to medication. 2005; 353: The American Society for Automation in Pharmacy Midyear Conference. Transitional Care: How Pharmacies Can Impact Outcomes for Discharged Patients. Jure 26-28, 2014.
49 Copyrights apply

50 Table 1. Elements of Good Care Transition for Patients Receiving Anticoagulation Accurate and complete information exchange among transferring and receiving provider Medication reconciliation Case management with arrangement for uninterrupted medication supply and laboratory monitoring (e.g., INR for warfarin, renal function) - Education of patient and caregiver(s) about the purpose of the medication, importance of adherence, how to take the medication, signs and symptoms of bleeding, when to seek medical attention and adverse effects Follow-up contact to ensure adherence and continuity of care Copyright 2016 by Society of Hospital Medicine. accessed 4/17/18
51 Evaluate the specific patient Understand the need for conventual and new therapies Keep informed
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015
 Clinical Practice Guideline August 2015") Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Treatment Options and How They Work
 Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
DOAC for VTE. Direct Oral Anticoagulants Clint Shedd DNP, FNP-BC Emory University
 DOAC for VTE Direct Oral Anticoagulants Clint Shedd DNP, FNP-BC Emory University No disclosures Direct Oral Anticoagulants Understand VTE and the ACCP s position on it List the DOACs available in the US
DOAC for VTE Direct Oral Anticoagulants Clint Shedd DNP, FNP-BC Emory University No disclosures Direct Oral Anticoagulants Understand VTE and the ACCP s position on it List the DOACs available in the US
Southern Trust Anticoagulant Team
 CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Anticoagulation- Primary Care Guidance for reviewing patients on DOACs Southern Trust Anticoagulant Team Haematology Acute
CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Anticoagulation- Primary Care Guidance for reviewing patients on DOACs Southern Trust Anticoagulant Team Haematology Acute
The Use of New Anticoagulants in the Elderly NOACs, DOACs,TOACs,TSOACs.
 The Use of New Anticoagulants in the Elderly NOACs, DOACs,TOACs,TSOACs. Chris E. Holmes MD, PhD Assistant Director, Thrombosis and Hemostasis Program University of Vermont Dabigatran (Praxxada) Rivoraxaban
The Use of New Anticoagulants in the Elderly NOACs, DOACs,TOACs,TSOACs. Chris E. Holmes MD, PhD Assistant Director, Thrombosis and Hemostasis Program University of Vermont Dabigatran (Praxxada) Rivoraxaban
Clinical Guideline for Anticoagulation in VTE
 Clinical Guideline for Anticoagulation in VTE These clinical guidelines are intended to provide evidence-based recommendations regarding the anticoagulation in patients with DVT and PE. Please note that
Clinical Guideline for Anticoagulation in VTE These clinical guidelines are intended to provide evidence-based recommendations regarding the anticoagulation in patients with DVT and PE. Please note that
Nibal R. Chamoun, Pharm.D., BCPS Clinical Assistant Professor of Pharmacy Practice at the Lebanese American University Clinical Pharmacy Coordinator
 Nibal R. Chamoun, Pharm.D., BCPS Clinical Assistant Professor of Pharmacy Practice at the Lebanese American University Clinical Pharmacy Coordinator at LAUMCRH Review the mechanism of action, indications
Nibal R. Chamoun, Pharm.D., BCPS Clinical Assistant Professor of Pharmacy Practice at the Lebanese American University Clinical Pharmacy Coordinator at LAUMCRH Review the mechanism of action, indications
Appendix IV - Prescribing Guidance for Apixaban
 Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY
 ASWAN UNIVERSITY") New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
Updates in Management of Venous Thromboembolic Disease
 Updates in Management of Venous Thromboembolic Disease November 7 th 2018 UHN Emergency Conference Susan Jenkins RN(EC) NP-Adult Thrombosis and Hemostasis Program University Health Network Disclosures
Updates in Management of Venous Thromboembolic Disease November 7 th 2018 UHN Emergency Conference Susan Jenkins RN(EC) NP-Adult Thrombosis and Hemostasis Program University Health Network Disclosures
Venous Thromboembolism National Hospital Inpatient Quality Measures
 Venous Thromboembolism National Hospital Inpatient Quality Measures Presentation Overview Review venous thromboembolism as a new mandatory measure set Outline measures with exclusions and documentation
Venous Thromboembolism National Hospital Inpatient Quality Measures Presentation Overview Review venous thromboembolism as a new mandatory measure set Outline measures with exclusions and documentation
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING
 DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
Oral Anticoagulants Update. Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation
 Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
WMC PHARMACY ANTICOAGULATION PROTOCOL Current Revision: July 2017 GENERAL ORDER PROCESSING AND MANAGEMENT
 WMC PHARMACY ANTICOAGULATION PROTOCOL Current Revision: July 2017 GENERAL ORDER PROCESSING AND MANAGEMENT - Entering orders for anticoagulation in Cerner Providers will enter individual orders (oneoffs)
WMC PHARMACY ANTICOAGULATION PROTOCOL Current Revision: July 2017 GENERAL ORDER PROCESSING AND MANAGEMENT - Entering orders for anticoagulation in Cerner Providers will enter individual orders (oneoffs)
New Anticoagulants Therapies
 New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS
 NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
Update on Oral Anticoagulants. Dr. Miten R. Patel Cancer Specialists of North Florida Cell
 Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Clinical issues which drug for which patient
 Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS
: COMPARISON AND FREQUENTLY ASKED QUESTIONS") NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
Preventing Stroke in Patients with Atrial Fibrillation: USING THE EVIDENCE
 Preventing Stroke in Patients with Atrial Fibrillation: USING THE EVIDENCE What Is Atrial Fibrillation? Atrial fibrillation also called AFib or AF is the most common abnormal heart rhythm, affecting an
Preventing Stroke in Patients with Atrial Fibrillation: USING THE EVIDENCE What Is Atrial Fibrillation? Atrial fibrillation also called AFib or AF is the most common abnormal heart rhythm, affecting an
NOACS/DOACS*: COAGULATION TESTS
 NOACS/DOACS*: COAGULATION TESTS OBJECTIVES: To describe the effect of the newer direct oral anticoagulants (DOACs) on laboratory coagulation tests which are widely available: prothrombin time (PT), international
NOACS/DOACS*: COAGULATION TESTS OBJECTIVES: To describe the effect of the newer direct oral anticoagulants (DOACs) on laboratory coagulation tests which are widely available: prothrombin time (PT), international
Are the days of Warfarin numbered?
 2 nd SAVTE Symposium Are the days of Warfarin numbered? YES Dr. Mohamed A. Abdelaal, MD, FRCPath, FRCPI Consultant Haematologist King Abdulaziz Medical City - Jeddah, Saudi Arabia 1 3 May 2012, Casablanca,
2 nd SAVTE Symposium Are the days of Warfarin numbered? YES Dr. Mohamed A. Abdelaal, MD, FRCPath, FRCPI Consultant Haematologist King Abdulaziz Medical City - Jeddah, Saudi Arabia 1 3 May 2012, Casablanca,
Nanik Hatsakorzian Pharm.D/MPH
 Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism
 Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Comparison of novel oral anticoagulants (NOACs)
") Comparison of novel oral anticoagulants (NOACs) For guidance for full information refer to individual SPCs available at www.medicines.org.uk Licensed indications for NOACs Prevention of stroke and systemic
Comparison of novel oral anticoagulants (NOACs) For guidance for full information refer to individual SPCs available at www.medicines.org.uk Licensed indications for NOACs Prevention of stroke and systemic
Direct Oral Anticoagulants
 Direct Oral Anticoagulants Holly Jahn, PharmD, CACP Objectives Identify the FDA approved indications for use, appropriate dosing, and monitoring parameters for each direct oral anticoagulant. Distinguish
Direct Oral Anticoagulants Holly Jahn, PharmD, CACP Objectives Identify the FDA approved indications for use, appropriate dosing, and monitoring parameters for each direct oral anticoagulant. Distinguish
Edoxaban for the treatment and prevention of venous thromboembolism (DVT or PE) or stroke prevention in non-valvular AF
 or stroke prevention in non-valvular AF") Edoxaban for the treatment and prevention of venous thromboembolism (DVT or PE) or stroke prevention in non-valvular AF Traffic light classification- Amber 2 specialist initiation / recommendation Information
Edoxaban for the treatment and prevention of venous thromboembolism (DVT or PE) or stroke prevention in non-valvular AF Traffic light classification- Amber 2 specialist initiation / recommendation Information
Drug Use Criteria: Direct Oral Anticoagulants
 Texas Vendor Drug Program Drug Use Criteria: Oral Anticoagulants Publication History 1. Developed March 2017. 2. Revised February 2018. Notes: Information on indications for use or diagnosis is assumed
Texas Vendor Drug Program Drug Use Criteria: Oral Anticoagulants Publication History 1. Developed March 2017. 2. Revised February 2018. Notes: Information on indications for use or diagnosis is assumed
Appendix 2H - SECONDARY CARE CONVERSION GUIDELINES ORAL ANTICOAGULANTS
 Appendix 2H - SECONDARY CARE CONVERSION GUIDELINES ORAL ANTICOAGULANTS Please note that newer oral anticoagulants e.g. rivaroxaban, dabigatran and apixiban should be only be considered in patients with
Appendix 2H - SECONDARY CARE CONVERSION GUIDELINES ORAL ANTICOAGULANTS Please note that newer oral anticoagulants e.g. rivaroxaban, dabigatran and apixiban should be only be considered in patients with
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
10 Key Things the Vascular Community Should Know about the DOACs Heather Gornik, MD, RVT, RPVI
 10 Key Things the Vascular Community Should Know about the DOACs Heather Gornik, MD, RVT, RPVI Cleveland Clinic Heart and Vascular Institute Heather L. Gornik, MD has the following relationships to disclose:
10 Key Things the Vascular Community Should Know about the DOACs Heather Gornik, MD, RVT, RPVI Cleveland Clinic Heart and Vascular Institute Heather L. Gornik, MD has the following relationships to disclose:
Do s and Don t of DOACs DISCLOSURE
 Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Obesity, renal failure, HIT: which anticoagulant to use?
 Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Choosing and Managing Direct Oral Anticoagulants (DOACs)
") Choosing and Managing Direct Oral Anticoagulants (DOACs) Ana G. Antun, MD, MSc Assistant Professor, Department of Hematology and Medical Oncology Winship Cancer Institute of Emory University 1 Outline
Choosing and Managing Direct Oral Anticoagulants (DOACs) Ana G. Antun, MD, MSc Assistant Professor, Department of Hematology and Medical Oncology Winship Cancer Institute of Emory University 1 Outline
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT
. Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT") Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
New Antithrombotic Agents
 New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
HEPARIN-INDUCED THROMBOCYTOPENIA (HIT)
") HEPARIN-INDUCED THROMBOCYTOPENIA (HIT) OBJECTIVE: To assist clinicians with the investigation and management of suspected and documented heparin-induced thrombocytopenia (HIT). BACKGROUND: HIT is a transient,
HEPARIN-INDUCED THROMBOCYTOPENIA (HIT) OBJECTIVE: To assist clinicians with the investigation and management of suspected and documented heparin-induced thrombocytopenia (HIT). BACKGROUND: HIT is a transient,
Novel Anticoagulant Drugs. by: Dr. M. Kamandi Fellowship of hematology and Oncology
 Novel Anticoagulant Drugs by: Dr. M. Kamandi Fellowship of hematology and Oncology A-Novel Oral Anticoagulants A drug that is: safe and effective has predictable pharmacology has few drug drug and drug
Novel Anticoagulant Drugs by: Dr. M. Kamandi Fellowship of hematology and Oncology A-Novel Oral Anticoagulants A drug that is: safe and effective has predictable pharmacology has few drug drug and drug
Venothromboembolism prophylaxis: Trauma and Orthopaedics Clinical guideline, V2
 Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics 11/11/11 TEMPORARY GUIDANCE There is no prophylactic tinzaparin available in the Trust currently. Please substitute enoxaparin
Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics 11/11/11 TEMPORARY GUIDANCE There is no prophylactic tinzaparin available in the Trust currently. Please substitute enoxaparin
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Change from lovenox to pradaxa
 P ford residence southampton, ny Change from lovenox to pradaxa 14-11-2017 We wanted to put out a friendly reminder that the Ask 3 Teach 3 (A3T3) initiative is indeed full swing. This is an multidisciplinary
P ford residence southampton, ny Change from lovenox to pradaxa 14-11-2017 We wanted to put out a friendly reminder that the Ask 3 Teach 3 (A3T3) initiative is indeed full swing. This is an multidisciplinary
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants. Helen Williams Consultant Pharmacist for CV Disease South London
 An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
La terapia del TEV nel paziente oncologico nell'era dei DOAC
 XXVI CONGRESSO NAZIONALE FCSA Bologna, 5-7 Novembre 2015 Tromboembolismo venoso La terapia del TEV nel paziente oncologico nell'era dei DOAC ANNA FALANGA Immunoematologia e Medicina Trasfusionale e Centro
XXVI CONGRESSO NAZIONALE FCSA Bologna, 5-7 Novembre 2015 Tromboembolismo venoso La terapia del TEV nel paziente oncologico nell'era dei DOAC ANNA FALANGA Immunoematologia e Medicina Trasfusionale e Centro
New Antithrombotic Agents DISCLOSURE
 New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
Rapid Fire-Top Articles You Need to Know
 Rapid Fire-Top Articles You Need to Know TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Rapid Fire-Top Articles You Need to Know TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
New Oral Anticoagulants
 New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Tim Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Akron General Medical Center for Family Medicine Professor, Northeast Ohio
 Tim Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Akron General Medical Center for Family Medicine Professor, Northeast Ohio Medical University Objectives 1. 2. 3. 4. Review and discuss
Tim Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Akron General Medical Center for Family Medicine Professor, Northeast Ohio Medical University Objectives 1. 2. 3. 4. Review and discuss
Updates in Coagulation Thrombophilia testing and direct oral anticoagulants. Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017
 Updates in Coagulation Thrombophilia testing and direct oral anticoagulants Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017 No conflicts of interest Introduction to thrombosis Hemostasis
Updates in Coagulation Thrombophilia testing and direct oral anticoagulants Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017 No conflicts of interest Introduction to thrombosis Hemostasis
Overview of anticoagulants David Perry
 Chapter 2 Overview of anticoagulants David Perry Historically anticoagulation involved the use of heparin and its derivatives or warfarin. However, the past few years have seen the introduction of a number
Chapter 2 Overview of anticoagulants David Perry Historically anticoagulation involved the use of heparin and its derivatives or warfarin. However, the past few years have seen the introduction of a number
These are guidelines only and can be deviated from if it is thought to be in the patient s best interest.
 Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics Venous thromboembolism (VTE) is a recognised complication associated with inactivity and surgical procedures. Therefore, all
Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics Venous thromboembolism (VTE) is a recognised complication associated with inactivity and surgical procedures. Therefore, all
THROMBOPROPHYLAXIS: NON-ORTHOPEDIC SURGERY
 THROMBOPROPHYLAXIS: NON-ORTHOPEDIC SURGERY OBJECTIVE: To outline a practical approach for the prevention of venous thromboembolism (VTE) in patients undergoing non-orthopedic surgery. BACKGROUND: VTE is
THROMBOPROPHYLAXIS: NON-ORTHOPEDIC SURGERY OBJECTIVE: To outline a practical approach for the prevention of venous thromboembolism (VTE) in patients undergoing non-orthopedic surgery. BACKGROUND: VTE is
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE VENOUS THROMBOEMBOLISM PROPHYLAXIS SCOPE Provincial Acute and Sub-Acute Care Facilities APPROVAL AUTHORITY Alberta Health Services Executive Committee SPONSOR Vice President, Quality and Chief Medical
TITLE VENOUS THROMBOEMBOLISM PROPHYLAXIS SCOPE Provincial Acute and Sub-Acute Care Facilities APPROVAL AUTHORITY Alberta Health Services Executive Committee SPONSOR Vice President, Quality and Chief Medical
Advances in Anticoagulation
 May 18, 2017 Advances in Anticoagulation Wei Ling Lau, MD Assistant Professor, Nephrology University of California, Irvine Talk Outline High stroke risk in CKD population Warfarin off-target effects on
May 18, 2017 Advances in Anticoagulation Wei Ling Lau, MD Assistant Professor, Nephrology University of California, Irvine Talk Outline High stroke risk in CKD population Warfarin off-target effects on
Edoxaban Treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism (NICE TA354)
") Rationale for Initiation, Continuation and Discontinuation (RICaD) Edoxaban Treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism (NICE TA354) This document supports the
Rationale for Initiation, Continuation and Discontinuation (RICaD) Edoxaban Treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism (NICE TA354) This document supports the
Survey patients for Sx, signs of AF. Establish AF Dx. Evaluate & Tx underlying heart disease/other causes. Assess adequacy of rate or rhythm control
 Suggested General Approach to Managing Atrial Fibrillation Survey patients for Sx, signs of AF Establish AF Dx ECG Holter Event monitor Implanted device (pacer) Determine & Tx stroke risk (CHA 2 DS 2 VASc)
Suggested General Approach to Managing Atrial Fibrillation Survey patients for Sx, signs of AF Establish AF Dx ECG Holter Event monitor Implanted device (pacer) Determine & Tx stroke risk (CHA 2 DS 2 VASc)
New and old anticoagulants. Anticoagulation Focus on Direct Oral Anticoagulants
 Anticoagulation Focus on Direct Oral Anticoagulants Tzu-Fei Wang, MD Assistant Professor Department of Internal Medicine Division of Hematology The Ohio State University Wexner Medical Center Objectives
Anticoagulation Focus on Direct Oral Anticoagulants Tzu-Fei Wang, MD Assistant Professor Department of Internal Medicine Division of Hematology The Ohio State University Wexner Medical Center Objectives
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture
 Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Reversal of Direct Oral Anticoagulants. Why are we now seeing so many patients on DOACs? Objectives. DOAC: Recurrent VTE. DOAC: Intracranial Bleeding
 Reversal of Direct Oral Anticoagulants Cameron D Griffiths, MD, FRCPC Clinical Assistant Professor Division of Hematology UBC Objectives Review efficacy and safety data for Direct Oral Anticoagulants (DOACs)
Reversal of Direct Oral Anticoagulants Cameron D Griffiths, MD, FRCPC Clinical Assistant Professor Division of Hematology UBC Objectives Review efficacy and safety data for Direct Oral Anticoagulants (DOACs)
a. A pharmacist may order a baseline SCr per protocol
 UNITYPOINT HEALTH - MARSHALLTOWN Marshalltown, Iowa PHARMACY POLICY AND PROCEDURE Subject: Anticoagulant Therapy Per Practice Protocol (Formerly Anticoagulant therapy #NPSG.03.05.01) Inpatient Warfarin
UNITYPOINT HEALTH - MARSHALLTOWN Marshalltown, Iowa PHARMACY POLICY AND PROCEDURE Subject: Anticoagulant Therapy Per Practice Protocol (Formerly Anticoagulant therapy #NPSG.03.05.01) Inpatient Warfarin
Intrinsic + Common = aptt. Extrinsic + Common = PT. Common Pathway
 Anticoagulant Cases 12 11 Intrinsic + Common = aptt 9 8 10 7 4 Extrinsic + Common = PT 5 2 Common Pathway 1 Xa Inhibitors rivaroxaban (Xarelto) apixaban (Eliquis) edoxaban (Savaysa) What is true regarding
Anticoagulant Cases 12 11 Intrinsic + Common = aptt 9 8 10 7 4 Extrinsic + Common = PT 5 2 Common Pathway 1 Xa Inhibitors rivaroxaban (Xarelto) apixaban (Eliquis) edoxaban (Savaysa) What is true regarding
4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients
 4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients Assess Thrombosis risk: baseline risk in an individual patient plus additional thrombotic risk
4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients Assess Thrombosis risk: baseline risk in an individual patient plus additional thrombotic risk
Professional Practice Minutes December 7, 2016
 Professional Practice Minutes December 7, 2016 **New Opportunity for Patient Education** We can now request the educational videos we want our patients to watch after our visit. Video topics include colon
Professional Practice Minutes December 7, 2016 **New Opportunity for Patient Education** We can now request the educational videos we want our patients to watch after our visit. Video topics include colon
Venous Thromboembolic Disease Update
 Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
A Review of Direct-Acting Oral Anticoagulants (DOACs) and Their Use in Special Populations
 and Their Use in Special Populations") A Review of Direct-Acting Oral Anticoagulants (DOACs) and Their Use in Special Populations Allison Bernard, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics October 25 th,
A Review of Direct-Acting Oral Anticoagulants (DOACs) and Their Use in Special Populations Allison Bernard, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics October 25 th,
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease
 Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease Cyrille K. Cornelio, Pharm.D. PGY2 Cardiology Pharmacy Resident The University of Oklahoma College of Pharmacy
Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease Cyrille K. Cornelio, Pharm.D. PGY2 Cardiology Pharmacy Resident The University of Oklahoma College of Pharmacy
Acute VTE Care Transition Order Set (Adult)
") Administration DOCUMENT PURPOSE This order set may be used for adult patients diagnosed with venous thromboembolism (VTE: deep vein thrombosis, pulmonary embolism) who are ready to be transferred from
Administration DOCUMENT PURPOSE This order set may be used for adult patients diagnosed with venous thromboembolism (VTE: deep vein thrombosis, pulmonary embolism) who are ready to be transferred from
Diagnosis and Management of Heparin-Induced Thrombocytopenia (HIT)
") ASH CLINICAL PRACTICE GUIDELINES VENOUS THROMBOEMBOLISM (VTE) POCKET GUIDE Diagnosis and Management of Heparin-Induced Thrombocytopenia (HIT) A POCKET GUIDE FOR THE CLINICIAN DECEMBER 08 Allyson M. Pishko,
ASH CLINICAL PRACTICE GUIDELINES VENOUS THROMBOEMBOLISM (VTE) POCKET GUIDE Diagnosis and Management of Heparin-Induced Thrombocytopenia (HIT) A POCKET GUIDE FOR THE CLINICIAN DECEMBER 08 Allyson M. Pishko,
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS
 GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
Chapter 1 The Reversing Agents
 Available Strategies to Reverse Anticoagulant Medications Michael L. Smith, Pharm. D., BCPS, CACP East Region Pharmacy Clinical Manager Hartford HealthCare Objectives: Describe the pharmacological agents
Available Strategies to Reverse Anticoagulant Medications Michael L. Smith, Pharm. D., BCPS, CACP East Region Pharmacy Clinical Manager Hartford HealthCare Objectives: Describe the pharmacological agents
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Perioperative Management of Anticoagulation
 Perioperative Management of Anticoagulation Presented By: Nibal R. Chamoun, PharmD, BCPS Clinical Assistant Professor, Clinical Coordinator Lebanese American University, School of Pharmacy Presented at:
Perioperative Management of Anticoagulation Presented By: Nibal R. Chamoun, PharmD, BCPS Clinical Assistant Professor, Clinical Coordinator Lebanese American University, School of Pharmacy Presented at:
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Hot Topics: Transitions of Care
 Our quarterly newsletter is a great way to stay up-to-date on emerging clinical information, medication safety issues, and Larkin s Hospital medication policies and procedures. Hot Topics: Transitions
Our quarterly newsletter is a great way to stay up-to-date on emerging clinical information, medication safety issues, and Larkin s Hospital medication policies and procedures. Hot Topics: Transitions
Oral Anticoagulation Drug Class Prior Authorization Protocol
 Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Dr Mammen Ninan GPwSI in Cardiology
 Dr Mammen Ninan GPwSI in Cardiology AF affects up to 835,000 people in England alone and is expected to rise year after year. AF is a known risk factor for stroke, the 3 rd highest cause of mortality in
Dr Mammen Ninan GPwSI in Cardiology AF affects up to 835,000 people in England alone and is expected to rise year after year. AF is a known risk factor for stroke, the 3 rd highest cause of mortality in
Anticoagulation
 041218 Anticoagulation 2018 About This Presentation Strategic Vectors: Clinical Outcomes Patient Safety Physician Engagement Team: Dr. Joseph DeCristofaro Karin Ganetis, RN Dr. Stephen A. Vitkun Dr. Lisa
041218 Anticoagulation 2018 About This Presentation Strategic Vectors: Clinical Outcomes Patient Safety Physician Engagement Team: Dr. Joseph DeCristofaro Karin Ganetis, RN Dr. Stephen A. Vitkun Dr. Lisa
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban
 Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
New Oral Anticoagulant Drugs in the Prevention of DVT
 New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
Individualizing VTE Treatment and Prevention of Recurrence: The Place for Direct Oral Anticoagulants in VTE
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Page 1 of 6. Low 1 (score 0-3) Monitor platelets and signs and symptoms of thrombosis and continue heparin
 Monitor platelets and signs and symptoms of thrombosis and continue heparin") Page 1 of 6 Estimate probability of HIT using the Four T s 1 Low 1 (score 0-3) Intermediate 1 (score 4-5) or High 1 (score 6-8) Monitor platelets and signs and symptoms of thrombosis and continue heparin
Page 1 of 6 Estimate probability of HIT using the Four T s 1 Low 1 (score 0-3) Intermediate 1 (score 4-5) or High 1 (score 6-8) Monitor platelets and signs and symptoms of thrombosis and continue heparin
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
NOACs in AF. Dr Colin Edwards Auckland Heart Group and Waitemata DHB. Dr Fiona Stewart Auckland Heart Group and Auckland DHB
 NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
UHL Guideline for Treatment of Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE) in adults, with Direct Oral Anti-Coagulants
 and Pulmonary Embolism (PE) in adults, with Direct Oral Anti-Coagulants") UHL Guideline for Treatment of Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE) in adults, with Direct Oral Anti-Coagulants Trust Ref B11/2018 1. Introduction and Who Guideline applies to The introduction
UHL Guideline for Treatment of Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE) in adults, with Direct Oral Anti-Coagulants Trust Ref B11/2018 1. Introduction and Who Guideline applies to The introduction
Acute Care: Understanding Direct Oral Anticoagulants (DOACs)
") Acute Care: Understanding Direct Oral Anticoagulants (DOACs) National Conference for Nurse Practitioners (NCNP) October 11, 2017 John Togami, PharmD, PhC Pharmacist Clinician - Outpatient Anticoagulation
Acute Care: Understanding Direct Oral Anticoagulants (DOACs) National Conference for Nurse Practitioners (NCNP) October 11, 2017 John Togami, PharmD, PhC Pharmacist Clinician - Outpatient Anticoagulation
THROMBOSIS AND THE CLOTTING CASCADE AND YOU. William Houck Shenandoah Oncology
 THROMBOSIS AND THE CLOTTING CASCADE AND YOU William Houck Shenandoah Oncology WE LL TALK ABOUT Remembering the clotting cascade and the key players Tests for hypercoagulable states & when to do Remembering
THROMBOSIS AND THE CLOTTING CASCADE AND YOU William Houck Shenandoah Oncology WE LL TALK ABOUT Remembering the clotting cascade and the key players Tests for hypercoagulable states & when to do Remembering
My Cancer Patient Has a Clot- Can I prescribe a Direct Oral Anticoagulant (DOAC)?
?") My Cancer Patient Has a Clot- Can I prescribe a Direct Oral Anticoagulant (DOAC)? November 24, 2018 Erica Peterson MD, FRCPC University of British Columbia Disclosures I participate in clinical research
My Cancer Patient Has a Clot- Can I prescribe a Direct Oral Anticoagulant (DOAC)? November 24, 2018 Erica Peterson MD, FRCPC University of British Columbia Disclosures I participate in clinical research
Managing Perioperative Anticoagulation. Edie Shen MD
 Managing Perioperative Anticoagulation Edie Shen MD Anticoagulation VKA Warfarin (Coumadin) DOACs Direct Thrombin Inhibitor Dabigatran (Pradaxa) Factor Xa Inhibitor Rivaroxaban(Xarelto) Apixaban(Eliquis)
Managing Perioperative Anticoagulation Edie Shen MD Anticoagulation VKA Warfarin (Coumadin) DOACs Direct Thrombin Inhibitor Dabigatran (Pradaxa) Factor Xa Inhibitor Rivaroxaban(Xarelto) Apixaban(Eliquis)
Management of Cancer Associated VTE
 Management of Cancer Associated VTE Jean M. Connors, MD 2017 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine HMS
Management of Cancer Associated VTE Jean M. Connors, MD 2017 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine HMS
Anticoagulation Overview Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita
 Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Post-procedure dose ok after hours. 12 hours (q 24h dosing only) assuming surgical hemostasis; second dose 24 hours after first dose.
 assuming surgical hemostasis; second dose 24 hours after first dose.") Medication Time to wait after last dose Post-procedure dose ok after hours Can pull catheter hours after last dose Can give next dose hours after pulling catheter Enoxaparin (Lovenox) Prophylactic dose
Medication Time to wait after last dose Post-procedure dose ok after hours Can pull catheter hours after last dose Can give next dose hours after pulling catheter Enoxaparin (Lovenox) Prophylactic dose
Suspected Deep Vein Thrombosis (DVT) Assessment
 Assessment") CHI no... First name... DOB... /... /... Last name... Sex: c M c F Address...... Telephone... or attach addressograph label here Hospital/Location: c Hairmyres c Monklands c Wishaw Other (specify)... Ward/Base...
CHI no... First name... DOB... /... /... Last name... Sex: c M c F Address...... Telephone... or attach addressograph label here Hospital/Location: c Hairmyres c Monklands c Wishaw Other (specify)... Ward/Base...
NHS Lanarkshire Guidance on Anticoagulant treatment for patients with non-valvular atrial fibrillation
 1 NHS Lanarkshire Guidance on Anticoagulant treatment for patients with non-valvular atrial fibrillation Atrial fibrillation (AF) affects about 1.2% of the population in the United Kingdom and accounts
1 NHS Lanarkshire Guidance on Anticoagulant treatment for patients with non-valvular atrial fibrillation Atrial fibrillation (AF) affects about 1.2% of the population in the United Kingdom and accounts
Reversal of Anticoagulants at UCDMC
 Reversal of Anticoagulants at UCDMC Introduction: Bleeding complications are a common concern with the use of anticoagulant agents. In selected situations, reversing or neutralizing the effects of an anticoagulant
Reversal of Anticoagulants at UCDMC Introduction: Bleeding complications are a common concern with the use of anticoagulant agents. In selected situations, reversing or neutralizing the effects of an anticoagulant