The hypertensive kidney and its Management
|
|
|
- Gladys Kennedy
- 5 years ago
- Views:
Transcription
1 The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage through the renin-angiotensin system Rate of damage predictable Adequate treatment can reduce rate of progression 1
2 Primary Renal Disease of new patients DM 34% 7% Others 20% Unknown 7% HT / renal vascular 3% Obstructive / 3% Urolithiasis Inherited congenital 2% Infection / reflux 25% GN Hypertensive Kidney Underlying pathology Vascular damage Renin- angiotensin activation Glomerular damage Hyperfiltration and proteinuria Glomerulosclerosis 2
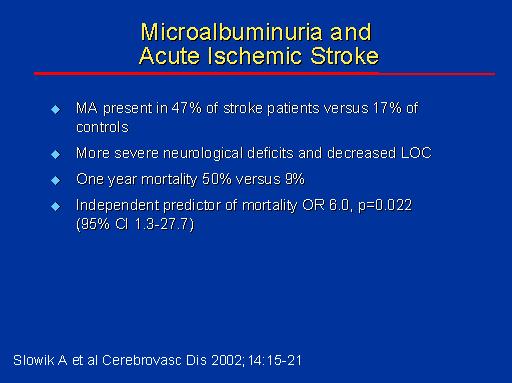
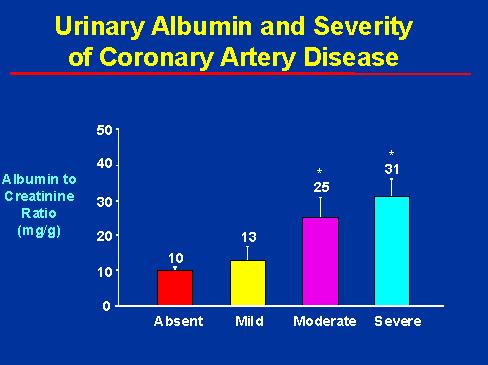
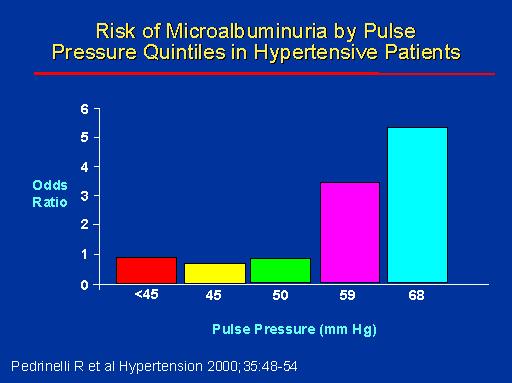
3 Endothelial damage One of the markers of endothelial damage is urine microalbumin In a hypertensive patient develop microalbuminuria, chance of cardiovascular events increased. Microalbuminuria Normal urine contains albumin of 20 mg/litre. Dipsticks can only detect albumin of 150 mg/litre Albumin excretion between mg/litre ( mg/day) is called microalbuminuria. Reversible at this stage 3

4 Microalbuminuria Can be performed in spot urine, need to determine the urine creatinine concentration to correct for urine dilution Urine albumin/creatinine ratio in MA: >30 mg/g or 3.4 mg/mmol 4
5 5
6 6
7 7

8 Hypertensive Kidney Underlying pathology Vascular damage Renin- angiotensin activation Glomerular damage Hyperfiltration and proteinuria Glomerulosclerosis 8



9 Ramipril and Renoprotection Part 1, slide 7 ACE inhibition and glomerular function (I) Afferent Arteriole BP Glomerulus Bowman s Capsule GCP Filtered Proteins EAR Efferent Arteriole Lewis E. Contrib Nephrol 1996;118:
10 Aims of HKD treatment Prevent the development of renal disease Delay the progression of renal disease Prevent the development of cardiovascular events many HKD patients died of cardio-vascular events before ESRD SHAPE UP program Management of hypertensive kidney disease - SHAPE UP program S Staging of renal failure, stop smoking H high BP, BS, cholesterol, high PO4 Rx A Anaemia management P Proteinuria management E Evaluation for renal transplantation U Undo nephrotoxins P Preservation of veins 10

11 Hypertensive Kidney Disease Chronic Kidney Disease renal damage sustained for more than 2 months Divided into 5 stages according to creatinine clearance Hypertensive kidney disease and diabetic nephropathy are major causes 11

12 Renal Function Tests blood urea (normal < 6 mmol/l) affected by the protein intake serum creatinine (normal <120 umol/l) more reliable because less affected by the protein intake affected by muscle mass, remain low despite poor renal function. when the serum creatinine is twice normal, 50% renal function is gone. creatinine clearance 12
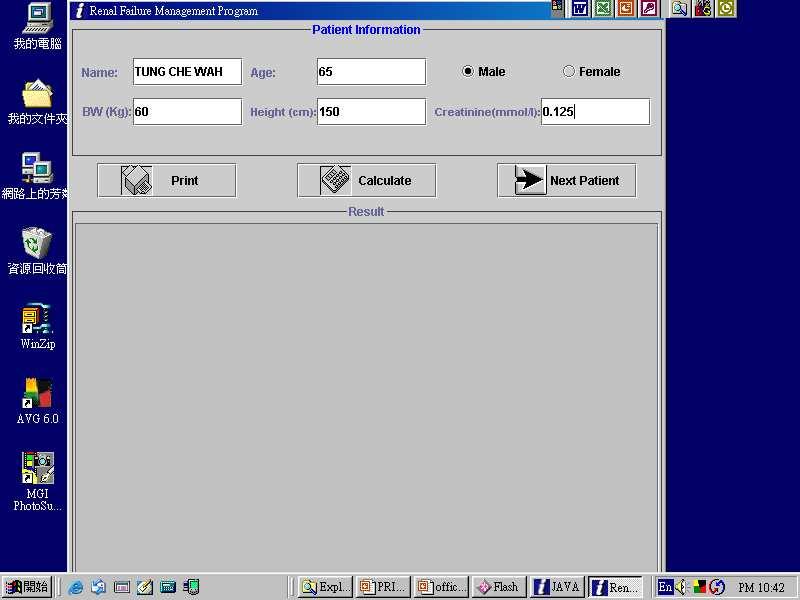
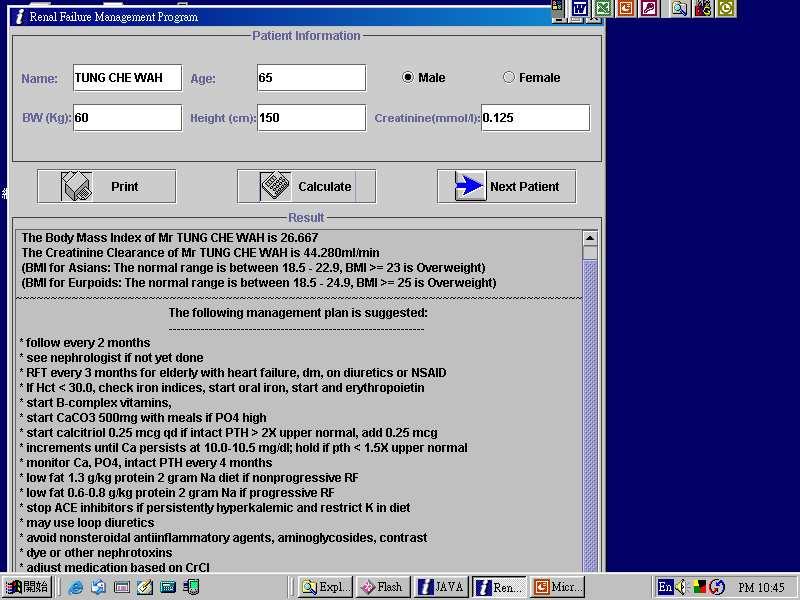
13 Creatinine Clearance Test Most accurate measure of renal function Need to collect 24 hour urine NOT all laboratories in HK can do this test accurately Can also be calculated from BW, age and serum creatinine Interpretation of CCr Normal around 100 ml/minute When CCr falls below 40 ml/minute, started to have symptoms Once CCr falls below 40/minute, downhill course inevitable When falls below 15 ml/minute, dialysis or transplant needed Computer program to calculate CCr and suggest treatment 13
14 14
15 15
16 Management of hypertensive kidney disease - SHAPE UP program S Staging of renal failure, stop smoking H high BP, BS, cholesterol, high PO4 Rx A Anaemia management P Proteinuria management E Evaluation for renal transplantation U Undo nephrotoxins P Preservation of veins Blood pressure Control BP highest in the early morning, lowest at night time Cardio-vascular events highest in the morning Ideal to control 24 hour BP to within target level 24 hour BP recording useful 16
 Complications lowest at systolic BP 120 mm Hg Each 10 mm Hg increase in systolic")
 Summary of Studies on Nephropathy Progression GFR (ml/min/year) SBP (mm")


17 Blood Pressure in Diabetic Nephropathy Each 10 mm Hg systolic reduce complications by 12% (UKPDS) Complications lowest at systolic BP 120 mm Hg Each 10 mm Hg increase in systolic blood pressure associated with 6.7% ESRD (RENNAL ) Summary of Studies on Nephropathy Progression GFR (ml/min/year) SBP (mm Hg) r = 0.69; P < 0.05 Untreated HTN Parving HH et al. Br Med J, 1989 Viberti GC et al. JAMA, 1993 Klahr S et al. N Eng J Med, 1993* Hebert L et al. Kidney Int, 1994 Lebovitz H et al. Kidney Int, 1994 Maschio G et al. N Engl J Med, 1996* Bakris GL et al. Kidney Int, 1996 Bakris GL. Hypertension, 1997 GISEN Group, Lancet, 1997* Bakris GL et.al.am J Kidney Dis, Sept
18 Target for blood pressure control With ACEI or ARB, reduce blood pressure to 130/80 mm Hg If urine protein >1 g/day, 120/75 mm Hg In type 2 diabetics, renal protection more clearly proven with ARB Angiotensin converting enzymes inhibitor For the same degree of BP reduction, also reduce proteinuria Preservation of renal function (small study) Lisinopril (Zestril) slows renal deterioration Can be combined with verapamil or diltiazem 18
19 Angiotensin Receptor Blocker Irbesartan Diabetic nephropathy Trial RENAAL Trial (Reduction of end-points in NIDDM with AA Losartan) Clear renoprotection in diabetic nephropathy in type 2 diabetics No head to head comparison with ACEI IDNT: Time to Doubling of Serum Creatinine Subjects (%) Irbesartan 300 mg/d Amlodipine 10 mg/d Control RRR= 37% P<.001 P= NS RRR= 33% P= Follow-up (mo) Lewis EJ et al. N Engl J Med. 2001;345:
20 RENAAL Time to ESRD from Doubling of Serum Creatinine % with event Risk Reduction: 30% p=0.013 P Months P (+CT) L (+CT) L K/DOQI Clinical practice guidelines Target Reduction of proteinuria <1 g/day blood pressure <130/80 mm Hg Start with ACEI/ARB Add Diuretics Add non-dihydropyridine (verapamil or diltiazem) Add ARB/ACEI 20
21 Drug combinations To reach the target blood pressure, more than one anti-hypertensive drugs need to be used. Drug combination may be convenient ACEI and verapamil both can reduce BP and proteinuria Combination of ACEI and ARB therapy Candesartan and Lisinopril Microalbuminuria Study (CALM) 199 hypertensive type 2 diabetic patients with microalbuminuria, randomly assigned first to ACEI or ARB therapy and then, after 12 weeks, to combination therapy or continued monotherapy Combination therapy afforded greater reductions in blood pressure and albuminuria than either treatment alone. 21
22 Phosphate control Hyper-phosphataemia is a potent cause of coronary calcification and vascular event Preventable with phosphate binder Calcium based phosphate binder can cause hypercalcaemia Aluminum phosphate binder may cause Al accumulation Hyperlipidaemia High blood lipid level accelerate glomerulosclerosis Albumin excretion falls by 25% according to one study The lower the lipid level the better Target cholesterol level 3.5 mmol/l 22

23 Management of hypertensive kidney disease - SHAPE UP program S Staging of renal failure, stop smoking H high BP, BS, cholesterol, high PO4 Rx A Anaemia management P Proteinuria management E Evaluation for renal transplantation U Undo nephrotoxins P Preservation of veins 23
24 Erythropoietin Major site of production is in the kidneys Produced by interstitial fibroblasts in? Proximal tubular cells Production stimulated by hypoxia (hypoxia inducible factor HIF) Use of Erythropoietin Previously used in end-stage renal failure patients Useful also in patients with moderate renal failure when Hb is low Part of the uraemic symptoms are in fact anaemic symptoms correctable by EPO injection 24
25 EPO and its benefits Correct the anaemia, target Hb level 10 to 11 g/dl Increase exercise tolerance Prevent left ventricular hypertrophy a risk factor for cardiac mortality Improved quality of life vitality and sleep Principle of EPO administration Response is dose dependent SC route generally more effective, dose 1/3 less compared with IV route. Response limited by iron store, inflammation, bone marrow fibrosis Hypertension as chief complication Headache (15%), flu like syndrome and seizures rare 25
26 The cardio-renal syndrome Hypertension caused heart failure and renal failure Heart failure aggravate renal failure Control of heart failure and anemia caused an improvement in renal function Management of hypertensive kidney disease - SHAPE UP program S Staging of renal failure, stop smoking H high BP, BS, cholesterol, high PO4 Rx A P Anaemia management Proteinuria management E Evaluation for dialysis/renal transplantation U Undo nephrotoxins P Preservation of veins 26
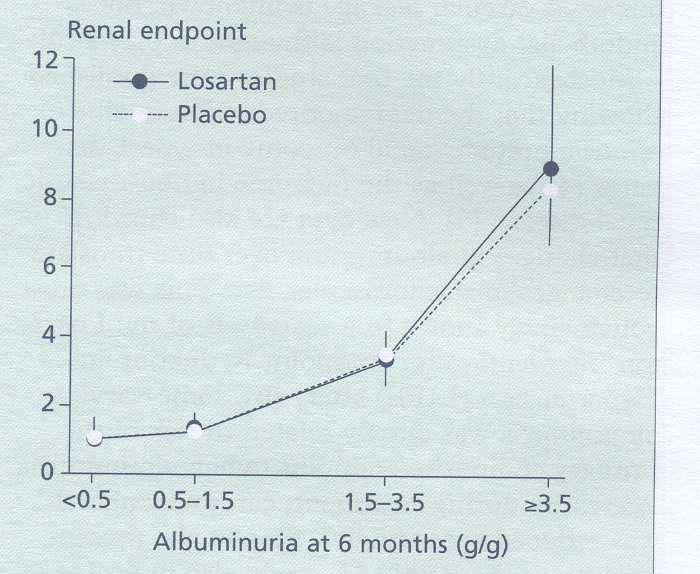
27 RENAAL data revisited Compare degree of proteinuria and occurrence of renal end-points (doubling of serum creatinine, ESRD or death) Compare degree of proteinuria and ESRD De Zeeuuw et al, 2004, Kidney International 27
28 28
29 New findings Albuminuria is the most powerful marker for renal progression in DN Suppression of albuminuria an independent predictor of renal protection Renal protection by losartan explained by anti-proteinuria effect in addition to hypotensive effect. Baseline proteinuria Patient with proteinuria >3.0 g/g creatinine showed 5.2 fold increased risk to renal end-point and 8.1 fold increase risk to ESRD Measurement of urine protein important. Urine protein a measure of glomerular hyperfiltration 29
30 Urine protein measurement In early stage, check for urine microalbumin reversible stage At macro-albumin stage, proteinuria a measure of glomerular pressure Proteinuria proportional to renal risk Reduction of proteinuria proportional to renal protection Proteinuria Estimation Ordinary urine dipstix affected by urine dilution, inaccurate ($0.20) 24 hour urine measurement accurate but expensive ($150) Early morning urine albumin/creatinine ratio ($150) Ho s dry state analysis ($0.75) 30
31 Urine albumin: creatinine ratio ($150/test) Check urine creatinine in addition to albumin, cancel out dilution effect If urine albumin 3 g/l and creatinine 1 g/l, the ratio is 3 g/g 24 hour urine protein excretion= 3 g/day Use early morning urine Useful for progress follow up. Ho s dry state analysis ($0.75/test) Instead of using urine creatinine, use SG instead Done on common urine dipstix Urine albumin expressed as mg/l Probability of significant proteinuria obtained from a curve 31


32 32
33 33
34 Low protein diet 0.6 g/kg/day slow GFR decline (12 ml/minute/year to 3 ml/minute/yr) At risk of protein malnutrition Effect modest 34
35 When to start dialysis? In diabetic patients, start dialysis when CCr around 15 ml/minute Other renal failure patients, start dialysis around 10 ml/minute Nephrologist needs 2 months to prepare patients for dialysis Management of hypertensive kidney disease - SHAPE UP program S Staging of renal failure, stop smoking H high BP, BS, cholesterol, high PO4 Rx A Anaemia management P Proteinuria management E Evaluation for dialysis/renal transplantation U Undo nephrotoxins P Preservation of veins 35

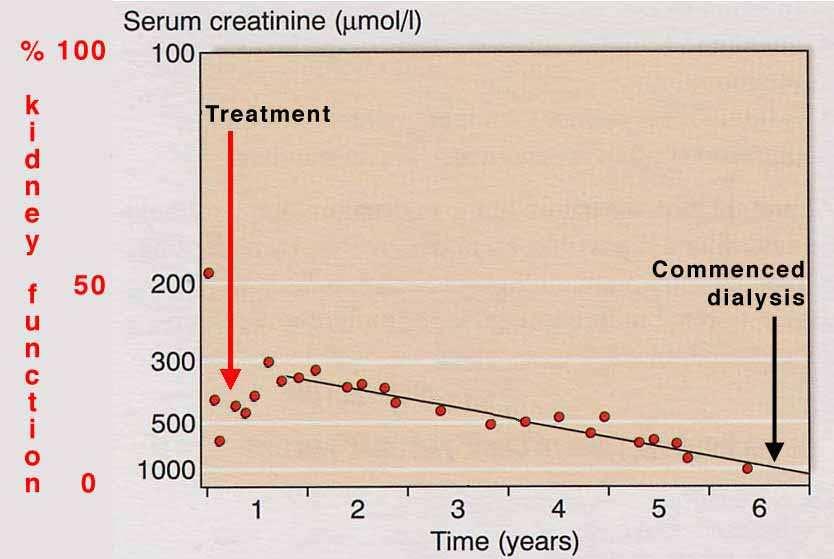
36 Predicting the date of endstage renal failure Creatinine clearance falls linearly with time 1/creatinine falls linearly We can use a computer program to predict the change computer simulation program 36
37 37
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
New Treatment Options for Diabetic Nephropathy patients. Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
 New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
(renoprotective (end-stage renal disease, ESRD) therapies) (JAMA)
 therapies) (JAMA)") [1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
[1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
Kidney Disease, Hypertension and Cardiovascular Risk
 1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
Renal Protection Staying on Target
 Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Firenze 22 settembre 2007
 Istituto di di medicina dello sport di di Firenze AMES Prevenzione cardiovascolare e cambiamenti negli stili di vita Firenze 22 settembre 2007 Orientamenti attuali per un intervento farmacologico e non
Istituto di di medicina dello sport di di Firenze AMES Prevenzione cardiovascolare e cambiamenti negli stili di vita Firenze 22 settembre 2007 Orientamenti attuali per un intervento farmacologico e non
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers. Robert D. Toto, MD
 R e v i e w P a p e r Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers Robert D. Toto, MD Both the prevalence and incidence of end-stage renal disease have been increasing
R e v i e w P a p e r Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers Robert D. Toto, MD Both the prevalence and incidence of end-stage renal disease have been increasing
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
ACEIs / ARBs NDHP dihydropyridine ( DHP ) ACEIs ARBs ACEIs ARBs NDHP. ( GFR ) 60 ml/min/1.73m ( chronic kidney disease, CKD )
 ACEIs ARBs ACEIs ARBs NDHP. ( GFR ) 60 ml/min/1.73m ( chronic kidney disease, CKD )") 005 16 175-180 1 1 ( chronic kidney disease, CKD ) 003 ( end-stage renal disease, ESRD ) Angiotensin-converting enzyme inhibitors ( ) angiotensin receptor blockers ( ) nondihydropyridine ( NDHP ) / NDHP
005 16 175-180 1 1 ( chronic kidney disease, CKD ) 003 ( end-stage renal disease, ESRD ) Angiotensin-converting enzyme inhibitors ( ) angiotensin receptor blockers ( ) nondihydropyridine ( NDHP ) / NDHP
6/10/2014. Chronic Kidney Disease - General management and standard of care. Management of CKD according to stage (KDOQI 2002)
") Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA
 ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012
 Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Chronic Kidney Disease
 Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Chronic Kidney Disease for the Primary Care Physician in What do the Kidneys do? CKD in the US
 1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
Diabetes has become the most common
 P O S I T I O N S T A T E M E N T Diabetic Nephropathy AMERICAN DIABETES ASSOCIATION Diabetes has become the most common single cause of end-stage renal disease (ESRD) in the U.S. and Europe; this is due
P O S I T I O N S T A T E M E N T Diabetic Nephropathy AMERICAN DIABETES ASSOCIATION Diabetes has become the most common single cause of end-stage renal disease (ESRD) in the U.S. and Europe; this is due
Diabetes and kidney disease.
 Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes in Renal Patients. Contents. Understanding Diabetic Nephropathy
 Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Renoprotective Strategies in Clinical Practice. Dr Michael Clarkson
 Renoprotective Strategies in Clinical Practice Dr Michael Clarkson The Silent Epidemic? ESRD CKD 5% of a UK population Staging of Chronic Kidney Disease Stage Description GFR Evaluation / Plan 0 At risk
Renoprotective Strategies in Clinical Practice Dr Michael Clarkson The Silent Epidemic? ESRD CKD 5% of a UK population Staging of Chronic Kidney Disease Stage Description GFR Evaluation / Plan 0 At risk
Diabetes has become the most common
 P O S I T I O N S T A T E M E N T Diabetic Nephropathy AMERICAN DIABETES ASSOCIATION Diabetes has become the most common single cause of end-stage renal disease (ESRD) in the U.S. and Europe; this is due
P O S I T I O N S T A T E M E N T Diabetic Nephropathy AMERICAN DIABETES ASSOCIATION Diabetes has become the most common single cause of end-stage renal disease (ESRD) in the U.S. and Europe; this is due
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERENCE CARDS Chronic Kidney Disease
 PROVIDER REFERENCE CARDS Chronic Kidney Disease") VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
DIABETES AND YOUR KIDNEYS
 DIABETES AND YOUR KIDNEYS OR AS WE CALL IT DIABETIC NEPHROPATHY The latest guidelines to keep you safe, healthy, fit, and out of danger from needing dialysis A UCLA HEALTH EDUCATIONAL SEMINAR Ramy M. Hanna
DIABETES AND YOUR KIDNEYS OR AS WE CALL IT DIABETIC NEPHROPATHY The latest guidelines to keep you safe, healthy, fit, and out of danger from needing dialysis A UCLA HEALTH EDUCATIONAL SEMINAR Ramy M. Hanna
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension)
") Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Diabetic Nephropathy 2009
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Prevalence of anemia and cardiovascular diseases in chronic kidney disease patients: a single tertiary care centre study
 International Journal of Advances in Medicine Sathyan S et al. Int J Adv Med. 2017 Feb;4(1):247-251 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20170120
International Journal of Advances in Medicine Sathyan S et al. Int J Adv Med. 2017 Feb;4(1):247-251 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20170120
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
The CARI Guidelines Caring for Australasians with Renal Impairment. Protein Restriction to prevent the progression of diabetic nephropathy GUIDELINES
 Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
The Heart and the Kidney
 1 3 6 The Heart and the Kidney Martin R. Cowie The Epidemiologic Association Between the Kidney and the Heart............................... 2819 The Burden of Chronic Kidney Disease............ 2820 The
1 3 6 The Heart and the Kidney Martin R. Cowie The Epidemiologic Association Between the Kidney and the Heart............................... 2819 The Burden of Chronic Kidney Disease............ 2820 The
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Kidney Disease. Chronic kidney disease (CKD) requiring dialysis. The F.P. s Role in the Management of Chronic. Stages
 requiring dialysis. The F.P. s Role in the Management of Chronic. Stages") Focus on CME at McMaster University The F.P. s Role in the Management of Chronic Kidney Disease By David N. Churchill, MD, FRCPC, FACP Presented at McMaster University CME Half-Day in Nephrology for Family
Focus on CME at McMaster University The F.P. s Role in the Management of Chronic Kidney Disease By David N. Churchill, MD, FRCPC, FACP Presented at McMaster University CME Half-Day in Nephrology for Family
Hypertension and diabetic nephropathy
 Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence?
 Reviews ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence? George L. Bakris, MD; 1 and Matthew Weir, MD 2 Although angiotensin-converting
Reviews ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence? George L. Bakris, MD; 1 and Matthew Weir, MD 2 Although angiotensin-converting
Diabetic Kidney Disease: Update. GKA Master Class. Istanbul 2011
 Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
CLINICIAN INTERVIEW A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY. Interview with Ralph Rabkin, MD
 A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC.
 Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC. Objectives Review CKD and its implications for the family physician Review the relevance of CKD and ESRD, its complications and management issues in
Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC. Objectives Review CKD and its implications for the family physician Review the relevance of CKD and ESRD, its complications and management issues in
The CARI Guidelines Caring for Australasians with Renal Impairment. Antihypertensive therapy in diabetic nephropathy GUIDELINES
 Antihypertensive therapy in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Adequate control of blood pressure (BP) slows progression
Antihypertensive therapy in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Adequate control of blood pressure (BP) slows progression
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Morbidity & Mortality from Chronic Kidney Disease
 Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Preventing kidney failure: Primary care physicians must intervene earlier
 REVIEW CME CREDIT CHRISTOPHER J. HEBERT, MD Louis Stokes Cleveland VA Medical Center, Cleveland, Ohio Preventing kidney failure: Primary care physicians must intervene earlier ABSTRACT Mild chronic kidney
REVIEW CME CREDIT CHRISTOPHER J. HEBERT, MD Louis Stokes Cleveland VA Medical Center, Cleveland, Ohio Preventing kidney failure: Primary care physicians must intervene earlier ABSTRACT Mild chronic kidney
Interventions to reduce progression of CKD what is the evidence? John Feehally
 Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 7/23/2013. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression
 CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
Keywords albuminuria, hypertension, nephropathy, proteinuria
 Should proteinuria reduction be the criterion for antihypertensive drug selection for patients with kidney disease? Rigas G. Kalaitzidis and George L. Bakris Department of Medicine, Hypertensive Diseases
Should proteinuria reduction be the criterion for antihypertensive drug selection for patients with kidney disease? Rigas G. Kalaitzidis and George L. Bakris Department of Medicine, Hypertensive Diseases
Case #1. Current Management Strategies in Chronic Kidney Disease. Serum creatinine cont. Pitfalls of Serum Cr
 Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Analysis of Factors Causing Hyperkalemia
 ORIGINAL ARTICLE Analysis of Factors Causing Hyperkalemia Kenmei Takaichi 1, Fumi Takemoto 1, Yoshifumi Ubara 1 and Yasumichi Mori 2 Abstract Objective Patients with impaired renal function or diabetes
ORIGINAL ARTICLE Analysis of Factors Causing Hyperkalemia Kenmei Takaichi 1, Fumi Takemoto 1, Yoshifumi Ubara 1 and Yasumichi Mori 2 Abstract Objective Patients with impaired renal function or diabetes
Chronic Kidney Disease - An Overview
 REVIEW ARTICLE KERALA MEDICAL JOURNAL Chronic Kidney Disease - An Overview Rajesh R Nair Department of Nephrology, Amrita Institute of Medical Sciences, Kochi, Kerala* ABSTRACT Published on 28 th December
REVIEW ARTICLE KERALA MEDICAL JOURNAL Chronic Kidney Disease - An Overview Rajesh R Nair Department of Nephrology, Amrita Institute of Medical Sciences, Kochi, Kerala* ABSTRACT Published on 28 th December
Case Study in Chronic Renal Failure
 Case Study in Chronic Renal Failure Development of Knowledge Base: There were over 14,500 articles dealing with chronic renal failure entered into PubMed during 2000 2004. A current concept in this array
Case Study in Chronic Renal Failure Development of Knowledge Base: There were over 14,500 articles dealing with chronic renal failure entered into PubMed during 2000 2004. A current concept in this array
Solving Slowing Progressive Renal Disease
 Focus on CME at Memorial University of Newfoundland Solving Slowing Progressive Risk factors and treatment strategies for patients with kidney and cardiovascular disease overlap. Thus, evaluating renal
Focus on CME at Memorial University of Newfoundland Solving Slowing Progressive Risk factors and treatment strategies for patients with kidney and cardiovascular disease overlap. Thus, evaluating renal
According to the US Renal Data System,
 DIABETIC NEPHROPATHY * Mohamed G. Atta, MD ABSTRACT *Based on a presentation given by Dr Atta at a CME dinner symposium for family physicians. Assistant Professor of Medicine, Division of Nephrology, Johns
DIABETIC NEPHROPATHY * Mohamed G. Atta, MD ABSTRACT *Based on a presentation given by Dr Atta at a CME dinner symposium for family physicians. Assistant Professor of Medicine, Division of Nephrology, Johns
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Objectives. Pre-dialysis CKD: The Problem. Pre-dialysis CKD: The Problem. Objectives
 The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
Protecting the kidneys in lupus nephritis
 Review Protecting the kidneys in lupus nephritis Kidney involvement is common in systemic lupus erythematosus. The inciting event in lupus nephritis is immune complex accumulation in the kidneys. While
Review Protecting the kidneys in lupus nephritis Kidney involvement is common in systemic lupus erythematosus. The inciting event in lupus nephritis is immune complex accumulation in the kidneys. While
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
What should you do next? Presenter Disclosure Information. Learning Objectives. Case: George
 2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
Diabetes is the most common cause of end-stage renal
 Pharmacoeconomic Challenges in the Management of Diabetic Nephropathy ROGER A. RODBY, MD ABSTRACT BACKGROUND: Diabetes is the most common cause of end-stage renal disease (ESRD) kidney failure to the point
Pharmacoeconomic Challenges in the Management of Diabetic Nephropathy ROGER A. RODBY, MD ABSTRACT BACKGROUND: Diabetes is the most common cause of end-stage renal disease (ESRD) kidney failure to the point
Management of Hypertension in Diabetic Nephropathy: How Low Should We Go?
 Review Advances in CKD 216 Published online: January 15, 216 Management of Hypertension in Diabetic Nephropathy: How Low Should We Go? Hillel Sternlicht George L. Bakris Department of Medicine, Section
Review Advances in CKD 216 Published online: January 15, 216 Management of Hypertension in Diabetic Nephropathy: How Low Should We Go? Hillel Sternlicht George L. Bakris Department of Medicine, Section
Renal Failure Update in Treatment Part 1. DANIEL WALTON, DO, FACP,FACOI,FASN PARTNER, AKDHC, LLC PHOENIX AZ (602)
") Renal Failure Update in Treatment Part 1 DANIEL WALTON, DO, FACP,FACOI,FASN PARTNER, AKDHC, LLC PHOENIX AZ (602) 263 5446 dwalton@akdhc.com DISCLOSURES NONE OFF LABEL USE POSSIBLY LEARNING OBJECTIVES USE
Renal Failure Update in Treatment Part 1 DANIEL WALTON, DO, FACP,FACOI,FASN PARTNER, AKDHC, LLC PHOENIX AZ (602) 263 5446 dwalton@akdhc.com DISCLOSURES NONE OFF LABEL USE POSSIBLY LEARNING OBJECTIVES USE
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Managing patients with renal disease
 Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Comparison between the efficacy of double blockade and single blockade of RAAS in diabetic kidney disease
 International Journal of Advances in Medicine Gupta A et al. Int J Adv Med. 2018 Aug;5(4):931-935 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20183122
International Journal of Advances in Medicine Gupta A et al. Int J Adv Med. 2018 Aug;5(4):931-935 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20183122
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영
 만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영 Contents Introduction Lifestyle and Pharmacological Tx CKD ND ptswithout diabetes CKD ND ptswith diabetes In elderly ptswith CKD ND 2013 대한고혈압학회진료지침 JNC 8th Introduction
만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영 Contents Introduction Lifestyle and Pharmacological Tx CKD ND ptswithout diabetes CKD ND ptswith diabetes In elderly ptswith CKD ND 2013 대한고혈압학회진료지침 JNC 8th Introduction
Faculty/Presenter Disclosure
 CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
Office Management of Reduced GFR Practical advice for the management of CKD
 Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
CARDIO-RENAL SYNDROME
 CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
Cardiovascular Disease in CKD. Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center
 Cardiovascular Disease in CKD Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center Objectives Describe prevalence for cardiovascular disease in CKD
Cardiovascular Disease in CKD Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center Objectives Describe prevalence for cardiovascular disease in CKD
Cardiovascular Pharmacotherapy in Special Population: Cardio-Nephrology
 49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Chronic Kidney Disease The 6 Pillars. Dr. Tiina Podymow Associate Professor Division of Nephrology McGill University Health Centre
 Chronic Kidney Disease The 6 Pillars Dr. Tiina Podymow Associate Professor Division of Nephrology McGill University Health Centre None Disclosures Objectives 1. Describe evidence-based measures to slow
Chronic Kidney Disease The 6 Pillars Dr. Tiina Podymow Associate Professor Division of Nephrology McGill University Health Centre None Disclosures Objectives 1. Describe evidence-based measures to slow