Drs Maaz Sohail, FAU Resident and Bryan Vinik, Endocrinology
|
|
|
- Amos Mills
- 5 years ago
- Views:
Transcription


1 Drs Maaz Sohail, FAU Resident and Bryan Vinik, Endocrinology
2 HPI: 75M referred for hypoglycemia with symptoms that started 18 months ago. Patient states that after drinking wine at night he would up confused and diaphoretic. EMS found him with B<50 which resolved after getting dextrose. Increased frequency of similar episodes since then. He is on a high protein low sugar/carb diet. Majority of symptoms occur overnight and occasionally mid-am. He feels he needs to eat more frequently to avoid BG drops and using glucose tabs (approx. 1 daily) but without monitoring BG levels. Social drinker, denies any history of liver or pancreatic disease. Denies any hypoglycemic medication.
3 ROS: weight gain PMH: Aortic valve disease, Hypercholesterolemia, Squamous cell skin cancer. PSH: Tonsillectomy, ankle fracture Medications: - Amlodipine-Benazepril HCL 10-20mg daily - Avodart 0.5mg daily - Pravastatin 20mg daily - HCTZ 25mg daily FH: No diabetes in family, noncontributory Social: nonsmoker, social drinker Allergies: Tetracycline Physical Exam BP: 118/70, HR: 70, FS: 75, BMI: 24 HEENT: No adenopathy or thyromegaly C/V: NSR, no murmurs GI: soft, NT, ND, no masses MSK: pulses 2+, no edema Neuro: normal DTR s, no tremors Psych: No depression or anxiety
4 Glucose 53, otherwise normal CMP elevated pro-insulin Normal c-peptide, cortisol, TSH Normal CgA normal Negative SFU screen Normal IGF-2 MRI of the abdomen w/ contrast negative for any pancreatic lesions.
5 Refused hospital stay for hour fasting test. He states his hypoglycemia continues but now more frequent however he is still able to manage it with his diet without any significant low BG levels. Hypoglycemic events occur between meals and early am with average BG levels in 50 s; 37 yesterday with symptoms. He is currently not waking up to eat overnight.
6 Patient referred to GI for an EUS. Findings: No evidence of isolated pancreatic lesions that might account for patient s insulin production. One area biopsied using a 22- gauge needle, not very suspicious however sampled due to lack of other choices. Preliminary diagnosis in the room yielded normal acinar cells, formal pathology pending.
7 Microscopy: Benign acinar cells and a population of atypical cells with mildly pleomorphic nuclei, inconspicuous nucleoli, and a thin rim of cytoplasm. Some atypical cells appear plasmacytoid. Immunohistochemical staining: Atypical cells positive for CD56, chromogranin, synaptophysin and negative for CD45. Immunostain for insulin positive. Diagnosis: well differentiated pancreatic endocrine tumor

8 Patient was seen in JFK medical center for surgical enucleation of his insulinoma.
9 Bryan Vinik MD With gratitude to: Andrew Fischer, M.D. Assistant Professor Clinical Medicine
10 1. Define hypoglycemia: components and severity 2. Explain the normal counter regulatory hormone response to hypoglycemia and defects in diabetes 3. Describe hypoglycemia unawareness and possible etiologies 4. List the causes of non-diabetic hypoglycemia 5. Analyze the biochemical findings in the work-up of hypoglycemia 6. Assess the key components essential in the diagnosis and management of insulinoma and non-insulinoma pancreatogenous hypoglycemia
11 1. DDx and Dx-is it really hypoglycemia and is it causing the Sx 2. Determine the cause, detective. 3. Treatment
12 A clinical syndrome characterized by episodes of low blood glucose. Episodes are typically marked by metabolic encephalopathy (neuroglycopenia). Autonomic manifestations alone do not indicate a hypoglycemic disorder.
13 Whipple s Triad: neurogenic and neuroglycopenic symptoms a low plasma glucose concentration relief by raising plasma glucose It confirms the presence of clinical hypoglycemia, and only those patients in whom Whipple's triad is documented require evaluation and management of hypoglycemia.
14 May be classified as insulin-mediated or noninsulin-mediated. Also classified as fasting or postprandial, but: Insulinoma patients may become hypoglycemic postprandially Factitious hypoglycemia occurs without regard to meals
15 Single episodes Accidental drug ingestion (ethanol, quinine, salicylates, sulfonylurea, glinides/glitinides) Multiple episodes Excessive insulin production (insulinoma or postgastric bypass syndrome) Factitious use of insulin or secretagogue Side effects of treatment for diabetes
16 Advanced liver disease Chronic renal failure Severe congestive heart failure Sepsis Hospitalized patients at risk for iatrogenic hypoglycemia due to inappropriate insulin or oral medication use
17 Low blood glucose may be an artifact resulting from consumption of glucose in blood collection tube by large numbers of nucleated RBC or leukocytes in patients with hemolysis or leukemia
18 Measure blood glucose when possible Detailed history including description of symptoms and circumstances during which symptoms occur Medication history extremely important. All meds need to be reviewed and positively identified

19 Signs: Diaphoresis and pallor are common signs. Heart rates and systolic blood pressures are raised, but not greatly. Neuroglycopenic manifestations are often observable. Occasionally, transient focal neurological deficits occur. Symptoms: Non-specific. Neurogenic symptoms: tremor, palpitations, and anxiety/arousal (catecholamine-mediated, adrenergic) and sweating, hunger, and paresthesias (acetylcholine-mediated, cholinergic). Neuroglycopenic symptoms: cognitive impairment, behavioral changes, psychomotor abnormalities and, at lower plasma glucose concentrations, seizure and coma.
20 In a study of patients with insulinomas, 85% had various combinations of diplopia, blurred vision, sweats, palpitations, weakness 80% had confusion or abnormal behavior 12% had generalized seizures
21 Different patients may have differing symptoms Each patient tends to have same symptoms with each episode Patients who have only autonomic symptoms without neuroglycopenic symptoms are unlikely to have hypoglycemia Many patients have only neuroglycopenic symptoms, which occur at a threshold of about 50 mg/dl
22 Studies with insulin and glucose infusions to normal young adult volunteers show the threshold for secretion of counterregulatory hormones is about at a glucose of 55 mg/dl
23 Insulin is the primary hormone that blunts postprandial hyperglycemia and maintains postabsorptive euglycemia Insulin s effects are counterbalanced by several factors to maintain a minimal level of glycemia
24 Secreted in response to hypoglycemia Effect of hormonal secretion is to raise blood glucose both quickly and over the long term In patients with diabetes, secretion of counterregulatory hormones often cause very high blood glucose values after an episode of severe hypoglycemia (rebound)
25 1 st defense: decrease in insulin secretion as plasma glucose concentrations decline within the physiological range (80-85 mg/dl) 2 nd defense: Increase in glucagon. Acts only on the liver. Increasing glucose production by stimulating both glycogenolysis and gluconeogenesis from alanine, among other amino acids, and glycerol. Glycemic threshold for glucagon is 65 to 70 mg/dl Requires a normally functioning liver.
26 3 rd defense: Increase in epinephrine. Acting via beta-2-adrenergic receptors, epinephrine has similar hepatic effects as glucagon. Also increases the delivery of gluconeogenic substrates from the periphery, inhibits glucose utilization by several tissues, and, via alpha-2- receptors, inhibits insulin secretion. Also requires a normally functioning liver. Glycemic threshold is also at mg/dl.
27 Cortisol and growth hormone work slowly over time to maintain glucose levels. They are not involved in acute raising of glucose Epinephrine secretion is responsible for autonomic symptoms of hypoglycemia Rate of decrease of blood glucose does NOT influence occurrence of symptoms

28
29 Glucagon and epinephrine are the 2 major defense hormones against prolonged hypoglycemia Glucagon secreted by alpha cells of pancreatic islets Glucagon response to hypoglycemia diminishes after a few years of type 1 diabetes Epinephrine alone may provide adequate defense against hypoglycemia
30 Epinephrine response to hypoglycemia can be lost after about 10 years of type 1 diabetes Can be lost with autonomic diabetic neuropathy Hypoglycemia is limiting step in intensive treatment of diabetes (Accord Trial)
31 72 hour fast is the standard evaluation Demonstrate Whipple s triad Determine cause of hypoglycemia Measure Beta-cell peptides and sulfonylurea levels Terminate fast when BS < 55. At this level secretion of Beta-cell polypeptides should be suppressed Terminate fast if patient becomes hypoglycemic Observe closely for signs of neuroglycopenia
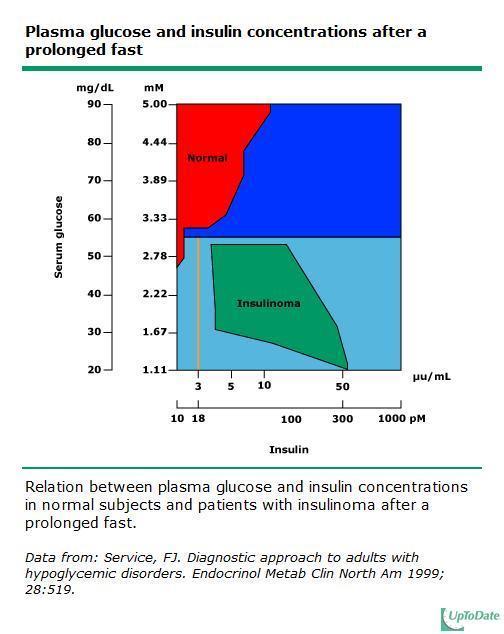
32 Plasma insulin concentration of 3 microu/ml by immunochemiluminometric assay (ICMA) when the plasma glucose concentration is below 55 mg/dl (3.0 mmol/l) indicates an excess of insulin and is consistent with insulinoma. However, plasma glucose concentrations fall below 50 mg/dl (2.8 mmol/l) in some normal subjects and remain above 50 mg/dl in an occasional patient with an insulinoma. Plasma insulin by ICMA may be lowered in a hemolyzed blood sample.
33

34 Plasma C-peptide distinguishes endogenous from exogenous hyperinsulinemia. In patients who become hypoglycemic, a plasma c-peptide concentration above 0.2 nmol/l is suggestive of an insulinoma.
35 For plasma proinsulin, the diagnostic criterion for insulinoma is 5 pmol/l or greater.

36 Because of the antiketogenic effect of insulin, plasma betahydroxybutyrate (BHOB) concentrations are lower in insulinoma patients than in normal subjects. All patients with insulinoma had plasma BHOB values of 2.7 mmol/l or less. Can be used to confirm (as can response to glucagon stimulation) the diagnosis in patients in whom the insulin and C-peptide values are in the borderline range or to indicate the action of an insulin-like factor.
 by releasing glucose.")
37 Recall that insulin is antiglycogenolytic and hyperinsulinemia permits retention of glycogen within the liver. Patients with insulin-mediated hypoglycemia respond to 1 mg of intravenous glucagon (a potent glycogenolytic agent) by releasing glucose. Normal subjects will have released virtually all glucose from the liver at the end of the 72-hour fast and cannot therefore respond as vigorously. At the end of the fast, patients with an insulinoma have an increase in plasma glucose of 25 mg/dl (1.4 mmol/l) or more in 20 to 30 min.
38 Sulfonylureas or meglitanides are used as oral hypoglycemics to treat diabetes Patients with hypoglycemia from inappropriate use of these medications will have concentrations of B-cell peptides identical to those with insulinoma Therefore plasma assays for these drugs are an essential part of an evaluation for hypoglycemia
39 Part of standard workup for hypoglycemia Used to be very common in those receiving insulin injections when beef-pork insulin was standard Current human and analog insulins cause very little antibody production High titers may be diagnostic of insulin autoimmune hypoglycemia
40 Should NOT be used as part of an evaluation for hypoglycemia At least 10% of healthy people have glucose values <50 during this test Results do not correlate with serum glucose responses to a mixed meal
41 For patients with neuroglycopenic symptoms within 5 hrs after eating, a mixed meal test could be performed Test is positive if there are symptoms of neuroglycopenia and a blood glucose <50 Positive test does NOT provide a diagnosis, only biochemical confirmation of the history
42 Incidence 3-10 cases per million people/yr (1:250,000 patient years) (50% of NETs) Mayo clinic data shows patients with insulinoma have age range 8 to 82 8% had multiple endocrine neoplasia type 1 6% had malignant insulinoma Insulinomas have been found in pregnant patients, and in patients with Type 2 diabetes One case of insulinoma in a patient with Type 1 diabetes has been reported
43 Hypoglycemia caused by excessive insulin secretion Islet cell pancreatic tumor secreting insulin Confirmation of diagnosis requires exclusion of hypoglycemia from exogenous sources
44 Transabdominal ultrasound High resolution CT Best localization is intraoperative ultrasound with palpation of pancreas by experienced surgeon This approach has 98% success rate in the identification of insulinoma After localization, patients proceed to surgical removal
45 Surgical removal Medical therapy includes diazoxide, which suppresses insulin secretion Side effects include edema and hirsutism Other meds that have been used include verapamil, phenytoin, and octreotide, all of which inhibit insulin secretion Medical therapy used in patients who are not acceptable surgical risks
46 Noninsulinoma Pancreatogenous Hypoglycemia Syndrome Unique clinical syndrome reported 1999 Typical patient is an adult who does not have insulinoma but who does have hypoglycemia resulting from pancreatic postprandial insulin hypersecretion
47 Ages of patients All have severe neuroglycopenia with loss of consciousness or seizures Predominantly occurs in males (70%) At Mayo clinic it occurs 1/5 th as frequently as insulinoma

48 Symptoms of hypoglycemia occur 2-4 hours after eating Low glucose levels and high insulin levels are found postprandially 72 hour fasts are normal vs Patients with insulinoma very rarely have negative 72 hour fasts Radiographic localization studies are negative
49 Because NIPHS results from diffuse B-cell hyperplasia and no discrete tumor, partial pancreatectomy is the treatment Symptoms may recur after several years
50 Self-induced hypoglycemia More common in women Usually occurs in health care workers or someone with access to medications Factitious hypoglycemia in diabetics probably more common than recognized, since diagnosis very difficult
51 Results from administration of insulin or insulin secretagogues Less often a parent may administer insulin to a child Insulin has been used to attempt suicide or homicide Mistaken prescription for hypoglycemic drugs
52 Should be considered in every patient undergoing evaluation for hypoglycemia Should be especially considered when hypoglycemia episodes have no pattern All medications need to by positively identified Diagnosis can be established by measuring c- peptide, insulin, and sulfonylurea/glitinide when hypoglycemia occurs
53 When due to orally administered pharmacologic agent (sulfonylurea or meglitinide), drug will be present in blood When due to insulin, serum insulin is high and c-peptide is suppressed C-peptide levels are near zero in type 1 diabetics, but confirmation that values are low eliminates consideration of endogenous hyperinsulinism
54 Very rare disorder Usually occurs in persons of Japanese or Korean ethnicity May occur at any age Usually self-limited in Asians, may be persistent in Caucasians No gender predilection
55 Many patients have ongoing autoimmune disorder Some patients have history of treatment with sulfhydryl containing drug such as antithyroid medication No patient has a history of insulin exposure
56 Presence of autoantibodies to insulin or insulin receptor Mechanism for generation of these antibodies is unknown Patients experience postprandial hypoglycemia resulting in neuroglycopenia Serum insulin levels very high because of antibody interference (can be >1000 uu/ml)
57 Very low titers of insulin antibodies may be observed in healthy patients without hypoglycemia Treatment is supportive, including frequent small meals For those with more severe symptoms, partial pancreatectomy is used Medications are of no value
58 Roux-en-Y gastric bypass More often occurs in women Occurs several times more frequently than insulinoma Gastric bypass may lead to increased secretion of gut hormones that stimulate insulin secretion (incretins) such as GLP-1
59 In turn increased GLP-1 may lead to islet cell hypertrophy Some patients may have insulinoma which can lead to overeating and obesity Patients with post bypass hypoglycemia have post-prandial hypoglycemia Insulinoma patients have fasting hypoglycemia Management may include partial pancreatectomy

60
61 Hypoglycemia is a syndrome characterized by episodes of low blood glucose Symptoms can be neuroglycopenic or autonomic Patients with autonomic symptoms only are unlikely to have hypoglycemia
62 Counterregulatory hormones which defend against hypoglycemia include glucagon, epinephrine, cortisol, and growth hormone Epinephrine and glucagon work quickly to raise blood glucose by increasing hepatic glucose output
63 Diabetics lose glucagon production over time Epinephrine becomes main defense against hypoglycemia when glucagon production is lost Epinephrine production can be lost over time When both glucagon and epinephrine are missing, patients have hypoglycemic unawareness
64 Causes of non-diabetic hypoglycemia include Insulinoma Factitious hypoglycemia Medication errors Liver disease, renal disease, congestive heart failure, sepsis Non insulinoma pancreatogenous hypoglycemia
65 Biochemical findings for insulinoma include inappropriately elevated insulin and c- peptide levels when blood glucose is low Key components for diagnosis of hypoglycemia include positive 72 hr fast and insulin secreting islet cell adenoma NIPHS usually causes post-prandial hypoglycemia and 72 hr fast usually negative NIPHS is due to b-cell hyperplasia
66 THANK YOU
Endocrine topic reviews. Artit Sangkakam, MD 19, september 2013
 Endocrine topic reviews Artit Sangkakam, MD 19, september 2013 Hypoglycemia in Non-DM Definition In diabetic mellitus : Plasma glucose 70 mg/dl In Non-diabetic mellitus : Plasma glucose 55 mg/dl Normal
Endocrine topic reviews Artit Sangkakam, MD 19, september 2013 Hypoglycemia in Non-DM Definition In diabetic mellitus : Plasma glucose 70 mg/dl In Non-diabetic mellitus : Plasma glucose 55 mg/dl Normal
Hypoglycaemic disorders
 Hypoglycaemic disorders 1. Hypoglycaemia in patients with diabetes mellitus 2. Hypoglycaemia in non-diabetic patients 3. Clinical, laboratory and imaging diagnosis 4. Case report 5. GLP-1 receptor scintigraphy
Hypoglycaemic disorders 1. Hypoglycaemia in patients with diabetes mellitus 2. Hypoglycaemia in non-diabetic patients 3. Clinical, laboratory and imaging diagnosis 4. Case report 5. GLP-1 receptor scintigraphy
Insulinoma - 72 hour Fast Protocol - RNS Endocrinology
 Page 1 of 9 - RNS Endocrinology Test name 72 hour fast Alternate test names. Related Tests Mixed meal test Indication(s) Differential diagnosis of causes of hypoglycaemia. Hypoglycaemia is rare in persons
Page 1 of 9 - RNS Endocrinology Test name 72 hour fast Alternate test names. Related Tests Mixed meal test Indication(s) Differential diagnosis of causes of hypoglycaemia. Hypoglycaemia is rare in persons
Hypoglycemia in congenital hyperinsulinism
 How a normal body works: Our body is constantly at work. Our cells need a source of energy, and this source of energy is called glucose. The process is quite simple; think of it like an assembly line.
How a normal body works: Our body is constantly at work. Our cells need a source of energy, and this source of energy is called glucose. The process is quite simple; think of it like an assembly line.
David Bruyette, DVM, DACVIM Medical Director
 VCAWLAspecialty.com David Bruyette, DVM, DACVIM Medical Director The pancreas is made up of endocrine and exocrine tissue. The endocrine pancreas is composed of islets of Langerhans, which make up approximately
VCAWLAspecialty.com David Bruyette, DVM, DACVIM Medical Director The pancreas is made up of endocrine and exocrine tissue. The endocrine pancreas is composed of islets of Langerhans, which make up approximately
Proceedings of the Southern European Veterinary Conference - SEVC -
 Close this window to return to IVIS www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 30-Oct. 3, 2010, Barcelona, Spain Next SEVC Conference: Sep. 30-Oct. 2, 2011 -
Close this window to return to IVIS www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 30-Oct. 3, 2010, Barcelona, Spain Next SEVC Conference: Sep. 30-Oct. 2, 2011 -
NEONATAL HYPOGLYCEMIA HEATHER MCKNIGHT-MENCI, MSN, CRNP CHILDREN S HOSPITAL OF PHILADELPHIA
 NEONATAL HYPOGLYCEMIA HEATHER MCKNIGHT-MENCI, MSN, CRNP CHILDREN S HOSPITAL OF PHILADELPHIA WHAT IS NEONATAL HYPOGLYCEMIA? Glucose concentration low enough to cause signs and symptoms of impaired brain
NEONATAL HYPOGLYCEMIA HEATHER MCKNIGHT-MENCI, MSN, CRNP CHILDREN S HOSPITAL OF PHILADELPHIA WHAT IS NEONATAL HYPOGLYCEMIA? Glucose concentration low enough to cause signs and symptoms of impaired brain
Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption),
,") Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption), in which blood glucose predominantly originates from
Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption), in which blood glucose predominantly originates from
Pancreatic Insulinoma Presenting. with Episodes of Hypoinsulinemic. Hypoglycemia in Elderly ---- A Case Report
 2008 19 432-436 Pancreatic Insulinoma Presenting with Episodes of Hypoinsulinemic Hypoglycemia in Elderly ---- A Case Report Chieh-Hsiang Lu 1, Shih-Che Hua 1, and Chung-Jung Wu 2,3 1 Division of Endocrinology
2008 19 432-436 Pancreatic Insulinoma Presenting with Episodes of Hypoinsulinemic Hypoglycemia in Elderly ---- A Case Report Chieh-Hsiang Lu 1, Shih-Che Hua 1, and Chung-Jung Wu 2,3 1 Division of Endocrinology
Pediatric Toxic Hypoglycemia. Sara Kazim, MD, FRCP (EM) Clinical Pharmacology and Medical Toxicology Fellowship IEMC May Antalya
 Clinical Pharmacology and Medical Toxicology Fellowship IEMC May Antalya") Pediatric Toxic Hypoglycemia Sara Kazim, MD, FRCP (EM) Clinical Pharmacology and Medical Toxicology Fellowship IEMC May 2016 - Antalya Conflicts of Interests... None Learning Needs... By the end of this
Pediatric Toxic Hypoglycemia Sara Kazim, MD, FRCP (EM) Clinical Pharmacology and Medical Toxicology Fellowship IEMC May 2016 - Antalya Conflicts of Interests... None Learning Needs... By the end of this
Hypoglycemia. When recognized early, hypoglycemia can be treated successfully.
 Hypoglycemia Introduction Hypoglycemia is a condition that causes blood sugar level to drop dangerously low. It mostly shows up in diabetic patients who take insulin. When recognized early, hypoglycemia
Hypoglycemia Introduction Hypoglycemia is a condition that causes blood sugar level to drop dangerously low. It mostly shows up in diabetic patients who take insulin. When recognized early, hypoglycemia
53 year old Female with Hypoglycemia. Colleen Flynn, MD April 5, 2012
 53 year old Female with Hypoglycemia Colleen Flynn, MD April 5, 2012 HPI 53 yo F referred to the endocrine clinic for hypoglycemia x 1 year. History of a non secreting metastatic neuroendocrine tumor diagnosed
53 year old Female with Hypoglycemia Colleen Flynn, MD April 5, 2012 HPI 53 yo F referred to the endocrine clinic for hypoglycemia x 1 year. History of a non secreting metastatic neuroendocrine tumor diagnosed
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY
 1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS An Overview WHAT IS HOMEOSTASIS? Homeostasis
1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS An Overview WHAT IS HOMEOSTASIS? Homeostasis
An Unexpected Cause of Hypoglycemia
 An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
Overview. o Limitations o Normal regulation of blood glucose o Definition o Symptoms o Clinical forms o Pathophysiology o Treatment.
 Pål R. Njølstad MD PhD KG Jebsen Center for Diabetes Research University of Bergen, Norway Depertment of Pediatrics Haukeland University Hospital Broad Institute of Harvard & MIT Cambridge, MA, USA Hypoglycemia
Pål R. Njølstad MD PhD KG Jebsen Center for Diabetes Research University of Bergen, Norway Depertment of Pediatrics Haukeland University Hospital Broad Institute of Harvard & MIT Cambridge, MA, USA Hypoglycemia
Evaluation and Management of Adult Hypoglycemic Disorders: An Endocrine Society Clinical Practice Guideline
 SPECIAL FEATURE Clinical Practice Guideline Evaluation and Management of Adult Hypoglycemic Disorders: An Endocrine Society Clinical Practice Guideline Philip E. Cryer, Lloyd Axelrod, Ashley B. Grossman,
SPECIAL FEATURE Clinical Practice Guideline Evaluation and Management of Adult Hypoglycemic Disorders: An Endocrine Society Clinical Practice Guideline Philip E. Cryer, Lloyd Axelrod, Ashley B. Grossman,
What systems are involved in homeostatic regulation (give an example)?
?") 1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS (Diabetes Mellitus Part 1): An Overview
1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS (Diabetes Mellitus Part 1): An Overview
This site is intended for healthcare professionals
 This site is intended for healthcare professionals Hypoglycemia Updated: Mar 20, 2018 Author: Osama Hamdy, MD, PhD; Chief Editor: Romesh Khardori, MD, PhD, FACP more... OVERVIEW Practice Essentials Hypoglycemia
This site is intended for healthcare professionals Hypoglycemia Updated: Mar 20, 2018 Author: Osama Hamdy, MD, PhD; Chief Editor: Romesh Khardori, MD, PhD, FACP more... OVERVIEW Practice Essentials Hypoglycemia
Pancreas Fox Chapter 18 part 2 (also Chapter 19.3 & 19.4)
") Vert Phys PCB3743 Pancreas Fox Chapter 18 part 2 (also Chapter 19.3 & 19.4) T. Houpt, Ph.D. Anatomy of Digestive System Peristalsis Stomach and Acid Secretion Liver and Bile Secretion Pancreas and pancreatic
Vert Phys PCB3743 Pancreas Fox Chapter 18 part 2 (also Chapter 19.3 & 19.4) T. Houpt, Ph.D. Anatomy of Digestive System Peristalsis Stomach and Acid Secretion Liver and Bile Secretion Pancreas and pancreatic
Hormonal Regulations Of Glucose Metabolism & DM
 Hormonal Regulations Of Glucose Metabolism & DM What Hormones Regulate Metabolism? What Hormones Regulate Metabolism? Insulin Glucagon Thyroid hormones Cortisol Epinephrine Most regulation occurs in order
Hormonal Regulations Of Glucose Metabolism & DM What Hormones Regulate Metabolism? What Hormones Regulate Metabolism? Insulin Glucagon Thyroid hormones Cortisol Epinephrine Most regulation occurs in order
9/11/2012. Chapter 11. Learning Objectives. Learning Objectives. Endocrine Emergencies. Differentiate type 1 and type 2 diabetes
 Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
بنام خدا هیپوگلیسمی درنوزادان و گاالکتوزمی دکتر انتظاری
 بنام خدا هیپوگلیسمی درنوزادان و گاالکتوزمی دکتر انتظاری Serum glucose< 35 mg/dl 1-3 hr of life < 40 mg/dl 3-24 hr < 45 mg/dl after 24 hr 10% NL newborns can t maintain BS>30 if delayed feeding >3-6 hrs
بنام خدا هیپوگلیسمی درنوزادان و گاالکتوزمی دکتر انتظاری Serum glucose< 35 mg/dl 1-3 hr of life < 40 mg/dl 3-24 hr < 45 mg/dl after 24 hr 10% NL newborns can t maintain BS>30 if delayed feeding >3-6 hrs
Diabetes Review. October 31, Dr. Don Eby Tracy Gaunt Dwayne Cottel
 Diabetes Review October 31, 2012 Dr. Don Eby Tracy Gaunt Dwayne Cottel Diabetes Review Learning Objectives: Describe the anatomy and physiology of the pancreas Describe the effects of hormones on the maintenance
Diabetes Review October 31, 2012 Dr. Don Eby Tracy Gaunt Dwayne Cottel Diabetes Review Learning Objectives: Describe the anatomy and physiology of the pancreas Describe the effects of hormones on the maintenance
For The Management Of. Hypoglycemia
 Guidelines For The Management Of Hypoglycemia By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs Kurdistan Higher Council For
Guidelines For The Management Of Hypoglycemia By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs Kurdistan Higher Council For
Unusual Pancreatic Neoplasms RTC 2/11/2011
 Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Hypoglycemia in Diabetes
 Hypoglycemia in Diabetes Nitin Kapoor, MD, DM, ABBM, Post Doc. Fellowship, Dept. of Endocrinology, Diabetes and Metabolism, CMC, Vellore. Jubbin Jagan Jacob, MD, DNB, Professor and Head, Endocrine and
Hypoglycemia in Diabetes Nitin Kapoor, MD, DM, ABBM, Post Doc. Fellowship, Dept. of Endocrinology, Diabetes and Metabolism, CMC, Vellore. Jubbin Jagan Jacob, MD, DNB, Professor and Head, Endocrine and
HYPOGLYCEMIA and neuroglycopenic symptoms
 0021-972X/00/$03.00/0 Vol. 85, No. 9 The Journal of Clinical Endocrinology & Metabolism Printed in U.S.A. Copyright 2000 by The Endocrine Society Forty-Eight-Hour Fast: The Diagnostic Test for Insulinoma
0021-972X/00/$03.00/0 Vol. 85, No. 9 The Journal of Clinical Endocrinology & Metabolism Printed in U.S.A. Copyright 2000 by The Endocrine Society Forty-Eight-Hour Fast: The Diagnostic Test for Insulinoma
Introduction SHORT COMMUNICATION
 Diabetologia (2005) 48: 2236 2240 DOI 10.1007/s00125-005-1933-x SHORT COMMUNICATION M. E. Patti. G. McMahon. E. C. Mun. A. Bitton. J. J. Holst. J. Goldsmith. D. W. Hanto. M. Callery. R. Arky. V. Nose.
Diabetologia (2005) 48: 2236 2240 DOI 10.1007/s00125-005-1933-x SHORT COMMUNICATION M. E. Patti. G. McMahon. E. C. Mun. A. Bitton. J. J. Holst. J. Goldsmith. D. W. Hanto. M. Callery. R. Arky. V. Nose.
63 year-old Man with Hypoglycemia. Sharon H. Chou, MD Endorama January 5, 2012
 63 year-old Man with Hypoglycemia Sharon H. Chou, MD Endorama January 5, 2012 History of Present Illness 63-year-old man with past medical history significant for systolic CHF (EF 25%), critical aortic
63 year-old Man with Hypoglycemia Sharon H. Chou, MD Endorama January 5, 2012 History of Present Illness 63-year-old man with past medical history significant for systolic CHF (EF 25%), critical aortic
Beyond the Naked Eye: A Case Presentation on a Rare Form of Congenital Hyperinsulinism (HI) Patient Demographics 5/12/2016
 Patient Demographics 5/12/2016") Beyond the Naked Eye: A Case Presentation on a Rare Form of Congenital Hyperinsulinism (HI) Pediatric Endocrine Nursing Society May 14, 2016 Enyo Dzata, MSN, CRNP Congenital Hyperinsulinism Center Division
Beyond the Naked Eye: A Case Presentation on a Rare Form of Congenital Hyperinsulinism (HI) Pediatric Endocrine Nursing Society May 14, 2016 Enyo Dzata, MSN, CRNP Congenital Hyperinsulinism Center Division
Hypoglycaemia mmol/l. 3 Emergency Presentations. Diabetic Emergencies. DG van Zyl. Normal Blood Glucose. Incidence
 Diabetic Emergencies DG van Zyl 3 Emergency Presentations Hypoglycaemia Diabetic keto-acidosis Hyperglycaemic hyperosmolar state Hypoglycaemia Normal Blood Glucose 3.9 5.8 mmol/l Incidence Probably the
Diabetic Emergencies DG van Zyl 3 Emergency Presentations Hypoglycaemia Diabetic keto-acidosis Hyperglycaemic hyperosmolar state Hypoglycaemia Normal Blood Glucose 3.9 5.8 mmol/l Incidence Probably the
A Rare Case Report - Big Insulinoma of Pancreas
 A Rare Case Report - Big Insulinoma of Pancreas Dr Vikalap Gupta 1, Prof Dr Brijesh Sharma 2 Abstract: Insulinomas account for 60% of islet cell tumours (ICT) and are typically hypervascular, solitary
A Rare Case Report - Big Insulinoma of Pancreas Dr Vikalap Gupta 1, Prof Dr Brijesh Sharma 2 Abstract: Insulinomas account for 60% of islet cell tumours (ICT) and are typically hypervascular, solitary
7/28/17. Objectives: Hypoglycemia Unawareness in the Geriatric Patient: A Safety Concern. Disclaimer:
 Hypoglycemia Unawareness in the Geriatric Patient: A Safety Concern 29TH ANNUAL TNP CONFERENCE TRANSFORMING HEALTHCARE IN TEXAS SEPTEMBER 8, 2017 AUSTIN, TEXAS Kenneth Lowrance, DNP, APRN, CNS, FNP-BC,
Hypoglycemia Unawareness in the Geriatric Patient: A Safety Concern 29TH ANNUAL TNP CONFERENCE TRANSFORMING HEALTHCARE IN TEXAS SEPTEMBER 8, 2017 AUSTIN, TEXAS Kenneth Lowrance, DNP, APRN, CNS, FNP-BC,
EAT TO LIVE: THE ROLE OF THE PANCREAS. Felicia V. Nowak, M.D., Ph.D. Ohio University COM 22 January, 2008
 EAT TO LIVE: THE ROLE OF THE PANCREAS Felicia V. Nowak, M.D., Ph.D. Ohio University COM 22 January, 2008 THE ROLE OF THE PANCREAS Exocrine pancreas Endocrine pancreas THE ROLE OF THE PANCREAS EXOCRINE
EAT TO LIVE: THE ROLE OF THE PANCREAS Felicia V. Nowak, M.D., Ph.D. Ohio University COM 22 January, 2008 THE ROLE OF THE PANCREAS Exocrine pancreas Endocrine pancreas THE ROLE OF THE PANCREAS EXOCRINE
- Prof. Dr. A.A.R. Starke Dr. Christiane Saddig Heinrich-Heine-Universität Düsseldorf Medizinische Klinik
 www.insulinoma.net - www.gep-net.com Prof. Dr. A.A.R. Starke Dr. Christiane Saddig Heinrich-Heine-Universität Düsseldorf Medizinische Klinik Insulinoma "endogenous hyperinsulinism", autonomous inadaequate
www.insulinoma.net - www.gep-net.com Prof. Dr. A.A.R. Starke Dr. Christiane Saddig Heinrich-Heine-Universität Düsseldorf Medizinische Klinik Insulinoma "endogenous hyperinsulinism", autonomous inadaequate
Type 2 DM in Adolescents: Use of GLP-1 RA. Objectives. Scope of Problem: Obesity. Background. Pathophysiology of T2DM
 Type 2 DM in Adolescents: Use of GLP-1 RA Objectives Identify patients in the pediatric population with T2DM that would potentially benefit from the use of GLP-1 RA Discuss changes in glycemic outcomes
Type 2 DM in Adolescents: Use of GLP-1 RA Objectives Identify patients in the pediatric population with T2DM that would potentially benefit from the use of GLP-1 RA Discuss changes in glycemic outcomes
Diabetes Mellitus. Diabetes Mellitus. Insulin. Glucose. Classifications of DM. Other glucose regulating Hormones
 Diabetes Mellitus Diabetes Mellitus Pathophysiology Literally sweet urine Defined by excess blood serum glucose Normally all glucose in the PCT is reabsorbed by active transport When blood glucose is elevated,
Diabetes Mellitus Diabetes Mellitus Pathophysiology Literally sweet urine Defined by excess blood serum glucose Normally all glucose in the PCT is reabsorbed by active transport When blood glucose is elevated,
72 hour Fast Protocol
 Page 1 of 5 Principle This procedure provides instruction on how to conduct a prolonged fast. During the fast, a careful record must be kept of exactly what was done, what blood samples were taken and
Page 1 of 5 Principle This procedure provides instruction on how to conduct a prolonged fast. During the fast, a careful record must be kept of exactly what was done, what blood samples were taken and
22 Emerging Therapies for
 22 Emerging Therapies for Treatment of Type 2 Diabetes Siddharth N Shah Abstract: The prevalence of Diabetes is progressively increasing world-wide and the growth of the disease in our country is phenomenal.
22 Emerging Therapies for Treatment of Type 2 Diabetes Siddharth N Shah Abstract: The prevalence of Diabetes is progressively increasing world-wide and the growth of the disease in our country is phenomenal.
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
28 Regulation of Fasting and Post-
 28 Regulation of Fasting and Post- Prandial Glucose Metabolism Keywords: Type 2 Diabetes, endogenous glucose production, splanchnic glucose uptake, gluconeo-genesis, glycogenolysis, glucose effectiveness.
28 Regulation of Fasting and Post- Prandial Glucose Metabolism Keywords: Type 2 Diabetes, endogenous glucose production, splanchnic glucose uptake, gluconeo-genesis, glycogenolysis, glucose effectiveness.
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND THE OLDER ADULT
 Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND THE OLDER ADULT Objectives u At conclusion of the presentation the participant will: 1. Discuss challenges to glycemic control unique in the older population
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND THE OLDER ADULT Objectives u At conclusion of the presentation the participant will: 1. Discuss challenges to glycemic control unique in the older population
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
ESPEN Congress Madrid 2018
 ESPEN Congress Madrid 2018 Dysglycaemia In Acute Patients With Nutritional Therapy Mechanisms And Consequences Of Dysglycaemia In Patients Receiving Nutritional Therapy M. León- Sanz (ES) Mechanisms and
ESPEN Congress Madrid 2018 Dysglycaemia In Acute Patients With Nutritional Therapy Mechanisms And Consequences Of Dysglycaemia In Patients Receiving Nutritional Therapy M. León- Sanz (ES) Mechanisms and
Neonatal Hypoglycaemia
 Neonatal Hypoglycaemia Dr Shubha Srinivasan Paediatric Endocrinologist The Children s Hospital at Westmead Hypoglycaemia and the Brain CSF glucose is 2/3 that of plasma Intracerebral glucose 1/3 that of
Neonatal Hypoglycaemia Dr Shubha Srinivasan Paediatric Endocrinologist The Children s Hospital at Westmead Hypoglycaemia and the Brain CSF glucose is 2/3 that of plasma Intracerebral glucose 1/3 that of
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Post-Bariatric Hypoglycemia (PBH): Diagnostic and Therapeutic Strategies
: Diagnostic and Therapeutic Strategies") Post-Bariatric Hypoglycemia (PBH): Diagnostic and Therapeutic Strategies Mary-Elizabeth Patti MD Investigator and Adult Endocrinologist Research Division Director, Hypoglycemia Clinic Joslin Diabetes Center
Post-Bariatric Hypoglycemia (PBH): Diagnostic and Therapeutic Strategies Mary-Elizabeth Patti MD Investigator and Adult Endocrinologist Research Division Director, Hypoglycemia Clinic Joslin Diabetes Center
Subcutaneous exendin (9-39) effectively treats post-bariatric hypoglycemia
 effectively treats post-bariatric hypoglycemia") Subcutaneous exendin (9-39) effectively treats post-bariatric hypoglycemia C OLLEEN M. CRAIG, M.D. T RACEY L. MC L AUGHLIN, M.D., M.S. Division of Endocrinology, Metabolism & Gerontology Stanford University
Subcutaneous exendin (9-39) effectively treats post-bariatric hypoglycemia C OLLEEN M. CRAIG, M.D. T RACEY L. MC L AUGHLIN, M.D., M.S. Division of Endocrinology, Metabolism & Gerontology Stanford University
An Unusual Case of Concurrent Insulinoma and Nesidioblastosis
 CASE REPORT An Unusual Case of Concurrent Insulinoma and Nesidioblastosis Elizabeth Bright 1, Giuseppe Garcea 1, Seok L Ong 1, Webster Madira 2, David P Berry 1, Ashley R Dennison 1 Departments of 1 Hepatobiliary
CASE REPORT An Unusual Case of Concurrent Insulinoma and Nesidioblastosis Elizabeth Bright 1, Giuseppe Garcea 1, Seok L Ong 1, Webster Madira 2, David P Berry 1, Ashley R Dennison 1 Departments of 1 Hepatobiliary
Combining Complex Pathophysiologic Concepts: Diabetes Mellitus
 Chapter 18 Combining Complex Pathophysiologic Concepts: Diabetes Mellitus KEY TERMS dawn phenomenon diabetes mellitus endocrine pancreas exocrine pancreas hyperglycemia hyperketonemia hypoglycemia insulin
Chapter 18 Combining Complex Pathophysiologic Concepts: Diabetes Mellitus KEY TERMS dawn phenomenon diabetes mellitus endocrine pancreas exocrine pancreas hyperglycemia hyperketonemia hypoglycemia insulin
Dedicated To. Course Objectives. Diabetes What is it? 2/18/2014. Managing Diabetes in the Athletic Population. Aiden
 Managing Diabetes in the Athletic Population Dedicated To Aiden Michael Prybicien, LA, ATC, CSCS, CES, PES Athletic Trainer, Passaic High School Overlook Medical Center & Adjunct Faculty, William Paterson
Managing Diabetes in the Athletic Population Dedicated To Aiden Michael Prybicien, LA, ATC, CSCS, CES, PES Athletic Trainer, Passaic High School Overlook Medical Center & Adjunct Faculty, William Paterson
History of Investigation
 Acini - Pancreatic juice (1º) (2º) Secretions- neuronal and hormonal mechanisms 1) Secretin - bicarbonate rich 2) Cholecystokinin - enzyme rich Islets of Langerhans (contain 4 cell types) Alpha cells (α)-
Acini - Pancreatic juice (1º) (2º) Secretions- neuronal and hormonal mechanisms 1) Secretin - bicarbonate rich 2) Cholecystokinin - enzyme rich Islets of Langerhans (contain 4 cell types) Alpha cells (α)-
Adrenal Hormone Mineralocorticoids Aldosterone
 Adrenal gland Adrenal Hormone Mineralocorticoids Aldosterone Cortex 80 % Glucocorticoids Cortisol Sex hormones Androgen Medulla 20% Catecholamines E, NE 1 2 Adrenal cortex hormones Glucocorticoid Mineralocorticoids
Adrenal gland Adrenal Hormone Mineralocorticoids Aldosterone Cortex 80 % Glucocorticoids Cortisol Sex hormones Androgen Medulla 20% Catecholamines E, NE 1 2 Adrenal cortex hormones Glucocorticoid Mineralocorticoids
Hypoglycemia, Electrolyte disturbances and acid-base imbalances
 Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
ENERGY FROM INGESTED NUTREINTS MAY BE USED IMMEDIATELY OR STORED
 QUIZ/TEST REVIEW NOTES SECTION 1 SHORT TERM METABOLISM [METABOLISM] Learning Objectives: Identify primary energy stores of the body Differentiate the metabolic processes of the fed and fasted states Explain
QUIZ/TEST REVIEW NOTES SECTION 1 SHORT TERM METABOLISM [METABOLISM] Learning Objectives: Identify primary energy stores of the body Differentiate the metabolic processes of the fed and fasted states Explain
Neonatal Hypoglycemia
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Neonatal Hypoglycemia. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Neonatal Hypoglycemia. These podcasts are designed to give medical students an overview of key topics in pediatrics.
associated with serious complications, but reduce occurrences with preventive measures
 Wk 9. Management of Clients with Diabetes Mellitus 1. Diabetes Mellitus body s inability to metabolize carbohydrates, fats, proteins hyperglycemia associated with serious complications, but reduce occurrences
Wk 9. Management of Clients with Diabetes Mellitus 1. Diabetes Mellitus body s inability to metabolize carbohydrates, fats, proteins hyperglycemia associated with serious complications, but reduce occurrences
Diabetes mellitus - diagnosis, classification and acute complications. David Karásek 3rd Department of Internal Medicine University Hospital Olomouc
 Diabetes mellitus - diagnosis, classification and acute complications David Karásek 3rd Department of Internal Medicine University Hospital Olomouc Diabetes mellitus is a group of metabolic diseases, characterized
Diabetes mellitus - diagnosis, classification and acute complications David Karásek 3rd Department of Internal Medicine University Hospital Olomouc Diabetes mellitus is a group of metabolic diseases, characterized
Week 3, Lecture 5a. Pathophysiology of Diabetes. Simin Liu, MD, ScD
 Week 3, Lecture 5a Pathophysiology of Diabetes Simin Liu, MD, ScD General Model of Peptide Hormone Action Hormone Plasma Membrane Activated Nucleus Cellular Trafficking Enzymes Inhibited Receptor Effector
Week 3, Lecture 5a Pathophysiology of Diabetes Simin Liu, MD, ScD General Model of Peptide Hormone Action Hormone Plasma Membrane Activated Nucleus Cellular Trafficking Enzymes Inhibited Receptor Effector
Local Anesthesia for Dental Hygienists Session III. Altered Consciousness and Diabetes Michael E. O Brien, DDS and Frank S.
 Altered Consciousness in General Dr. Michael E. O Brien Dr. Frank S. Drongowski Definitions Confusion - a mental state marked by disturbances in comprehension, understanding, and resulting in bewilderment
Altered Consciousness in General Dr. Michael E. O Brien Dr. Frank S. Drongowski Definitions Confusion - a mental state marked by disturbances in comprehension, understanding, and resulting in bewilderment
Low Blood Sugar in Dogs & Cats Figuring Out Hypoglycemia
 Low Blood Sugar in Dogs & Cats Figuring Out Hypoglycemia Low blood sugar, also known as hypoglycemia, is a relatively common biochemical abnormality documented in sick dogs and cats presented to the emergency
Low Blood Sugar in Dogs & Cats Figuring Out Hypoglycemia Low blood sugar, also known as hypoglycemia, is a relatively common biochemical abnormality documented in sick dogs and cats presented to the emergency
10. ACUTE COMPLICATIONS OF DIABETES MELLITUS
 10. ACUTE COMPLICATIONS OF DIABETES MELLITUS Prof. Oren Zinder, Ph.D. Rambam Medical Center, and the Technion Faculty of Medicine, Haifa, Israel 1.1. Hypoglycaemia Hypoglycaemia is a lowered blood glucose
10. ACUTE COMPLICATIONS OF DIABETES MELLITUS Prof. Oren Zinder, Ph.D. Rambam Medical Center, and the Technion Faculty of Medicine, Haifa, Israel 1.1. Hypoglycaemia Hypoglycaemia is a lowered blood glucose
Insulin, C-peptide and proinsulin for the biochemical diagnosis of hypoglycaemia related to endogenous hyperinsulinism
 European Journal of Endocrinology (2007) 157 75 83 ISSN 0804-4643 CLINICAL STUDY Insulin, C-peptide and proinsulin for the biochemical diagnosis of hypoglycaemia related to endogenous hyperinsulinism D
European Journal of Endocrinology (2007) 157 75 83 ISSN 0804-4643 CLINICAL STUDY Insulin, C-peptide and proinsulin for the biochemical diagnosis of hypoglycaemia related to endogenous hyperinsulinism D
Pancreatic Lesions. Valerie Jefford Pediatric Surgery Rounds June 6, 2003
 Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pathogenesis of Diabetes Mellitus
 Pathogenesis of Diabetes Mellitus Young-Bum Kim, Ph.D. Associate Professor of Medicine Harvard Medical School Definition of Diabetes Mellitus a group of metabolic diseases characterized by hyperglycemia
Pathogenesis of Diabetes Mellitus Young-Bum Kim, Ph.D. Associate Professor of Medicine Harvard Medical School Definition of Diabetes Mellitus a group of metabolic diseases characterized by hyperglycemia
the complete guide for controling hypoglycemia GLUCOSE
 the complete guide GLUCOSE for controling hypoglycemia Personal DATA Name Address Phone Diabetes Treatment Center: Name Address Phone In an urgent case contact with: Name Address Phone Presents other risk
the complete guide GLUCOSE for controling hypoglycemia Personal DATA Name Address Phone Diabetes Treatment Center: Name Address Phone In an urgent case contact with: Name Address Phone Presents other risk
Hypoglycaemia in nondiabetic patients
 clinical Ching Luen Ng Hypoglycaemia in nondiabetic patients An evidence based approach Background Hypoglycaemia can have serious consequences for patients. Hypoglycaemia in nondiabetic patients is not
clinical Ching Luen Ng Hypoglycaemia in nondiabetic patients An evidence based approach Background Hypoglycaemia can have serious consequences for patients. Hypoglycaemia in nondiabetic patients is not
Diabetes Management in Palliative Care. Ryan Liebscher and Carolyn Wilkinson
 Diabetes Management in Palliative Care Ryan Liebscher and Carolyn Wilkinson What are your learning needs? Objectives Review types and prevalence of diabetes Review what is unique to management in the palliative
Diabetes Management in Palliative Care Ryan Liebscher and Carolyn Wilkinson What are your learning needs? Objectives Review types and prevalence of diabetes Review what is unique to management in the palliative
A case of non-islet cell tumor hypoglycemia associated with pancreatic neuroendocrine tumor
 Case Report Page 1 of 5 A case of non-islet cell tumor hypoglycemia associated with pancreatic neuroendocrine tumor Agron Ylli 1, Gerond Husi 1, Renta Sanxhaku 1, Ditila Doracaj 2, Gentian Vyshka 2, Ruden
Case Report Page 1 of 5 A case of non-islet cell tumor hypoglycemia associated with pancreatic neuroendocrine tumor Agron Ylli 1, Gerond Husi 1, Renta Sanxhaku 1, Ditila Doracaj 2, Gentian Vyshka 2, Ruden
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Endo 2 SLO Practice (online) Page 1 of 7
 Page 1 of 7") Endo 2 SLO Practice (online) Page 1 of 7 1. A long- acting insulin, like Lantus is for? A. When the next meal is within 30-60 minutes of the injection B. Over night use or for ½ of the day often combined
Endo 2 SLO Practice (online) Page 1 of 7 1. A long- acting insulin, like Lantus is for? A. When the next meal is within 30-60 minutes of the injection B. Over night use or for ½ of the day often combined
Clinical Features and Causes of Endogenous Hyperinsulinemic Hypoglycemia in Korea
 Original Article Epidemiology Diabetes Metab J 2015;39:126-131 http://dx.doi.org/10.4093/dmj.2015.39.2.126 pissn 2233-6079 eissn 2233-6087 DIABETES & METABOLISM JOURNAL Clinical Features and Causes of
Original Article Epidemiology Diabetes Metab J 2015;39:126-131 http://dx.doi.org/10.4093/dmj.2015.39.2.126 pissn 2233-6079 eissn 2233-6087 DIABETES & METABOLISM JOURNAL Clinical Features and Causes of
Goals & Objectives. Diabetes Mellitus
 Rudy R. Navarro, M.D., CAQSM Department of Family & Community Medicine UT Health Science Center at San Antonio Goals & Objectives Understand the patterns of glucose utilization during exercise and sporting
Rudy R. Navarro, M.D., CAQSM Department of Family & Community Medicine UT Health Science Center at San Antonio Goals & Objectives Understand the patterns of glucose utilization during exercise and sporting
International Journal of Allied Medical Sciences and Clinical Research (IJAMSCR)
") International Journal of Allied Medical Sciences and Clinical Research (IJAMSCR) IJAMSCR Volume 3 Issue 1 Jan-Mar- 2015 www.ijamscr.com Research article Medical research Diabetes mellitus associated mortality:
International Journal of Allied Medical Sciences and Clinical Research (IJAMSCR) IJAMSCR Volume 3 Issue 1 Jan-Mar- 2015 www.ijamscr.com Research article Medical research Diabetes mellitus associated mortality:
I. General Considerations
 1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
Advanced Pharmacology Diabetes Homework
 Advanced Pharmacology Diabetes Homework Points: 25 Comments: Name: Tracy Hill WU ID #: 20015608 E-mail: tracy.hill@washburn.edu _TH I hereby certify that the work submitted is my own, and that I have not
Advanced Pharmacology Diabetes Homework Points: 25 Comments: Name: Tracy Hill WU ID #: 20015608 E-mail: tracy.hill@washburn.edu _TH I hereby certify that the work submitted is my own, and that I have not
Hypoglycemia After Bariatric Surgery: Diagnostic and Therapeutic Strategies
 Hypoglycemia After Bariatric Surgery: Diagnostic and Therapeutic Strategies Mary-Elizabeth Patti MD Investigator and Adult Endocrinologist Research Division Director, Hypoglycemia Clinic Joslin Diabetes
Hypoglycemia After Bariatric Surgery: Diagnostic and Therapeutic Strategies Mary-Elizabeth Patti MD Investigator and Adult Endocrinologist Research Division Director, Hypoglycemia Clinic Joslin Diabetes
Hypoglycemia, Sick Days/DKA and Hospitalization
 Hypoglycemia, Sick Days/DKA and Hospitalization General survival skills for your client with diabetes at home and in Hospital Diabetes Canada guidelines for your client with diabetes while they are in
Hypoglycemia, Sick Days/DKA and Hospitalization General survival skills for your client with diabetes at home and in Hospital Diabetes Canada guidelines for your client with diabetes while they are in
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς
 Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Adrenal gland And Pancreas
 Adrenal gland And Pancreas Structure Cortex Glucocorticoids Effects Control of secretion Mineralocorticoids Effects Control of secretion Sex steroids Medulla Catecholamines Adrenal cortex 80% of an adrenal
Adrenal gland And Pancreas Structure Cortex Glucocorticoids Effects Control of secretion Mineralocorticoids Effects Control of secretion Sex steroids Medulla Catecholamines Adrenal cortex 80% of an adrenal
21/07/2017. CS Verbeke. Non-neoplastic disease of the pancreas PATHOLOGY OF NON-NEOPLASTIC PANCREATIC DISEASES
 Non-neoplastic disease of the pancreas No indication for surgical resection of non-neoplastic disease (except end-stage chronic pancreatitis) Unexpected benign disease in 5-13% of pancreatic resections
Non-neoplastic disease of the pancreas No indication for surgical resection of non-neoplastic disease (except end-stage chronic pancreatitis) Unexpected benign disease in 5-13% of pancreatic resections
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
SHORT COMMUNICATION. J. C. Reubi & A. Perren & R. Rehmann & B. Waser & E. Christ & M. Callery & A. B. Goldfine & M. E. Patti
 Diabetologia (2010) 53:2641 2645 DOI 10.1007/s00125-010-1901-y SHORT COMMUNICATION Glucagon-like peptide-1 (GLP-1) receptors are not overexpressed in pancreatic islets from patients with severe hyperinsulinaemic
Diabetologia (2010) 53:2641 2645 DOI 10.1007/s00125-010-1901-y SHORT COMMUNICATION Glucagon-like peptide-1 (GLP-1) receptors are not overexpressed in pancreatic islets from patients with severe hyperinsulinaemic
Diabetes Mellitus. Raja Nursing Instructor. Acknowledgement: Badil 09/03/2016
 Diabetes Mellitus Raja Nursing Instructor 09/03/2016 Acknowledgement: Badil Objective: Define Diabetes Mellitus (DM) & types of DM. Understand the pathophysiology of Type-I & II DM. List the clinical features
Diabetes Mellitus Raja Nursing Instructor 09/03/2016 Acknowledgement: Badil Objective: Define Diabetes Mellitus (DM) & types of DM. Understand the pathophysiology of Type-I & II DM. List the clinical features
Case- history. Lab results
 Neda Rasouli, M.D. Associate Professor of Medicine Division of Endocrinology, UC Denver VA_ Eastern Colorado Health Care System Case- history 46 y/o AA male with BMI 37 presented in Oct 2001 with polyuria,
Neda Rasouli, M.D. Associate Professor of Medicine Division of Endocrinology, UC Denver VA_ Eastern Colorado Health Care System Case- history 46 y/o AA male with BMI 37 presented in Oct 2001 with polyuria,
Glucagon Administration. Molalla River School District
 Glucagon Administration Molalla River School District Laws that have were created to allow for administration of epinephrine in the school based setting were revised to include glucagon administration
Glucagon Administration Molalla River School District Laws that have were created to allow for administration of epinephrine in the school based setting were revised to include glucagon administration
WHAT IS YOUR DIAGNOSIS?
 WHAT IS YOUR DIAGNOSIS? An 8 year old, female neutered cross breed dog was presented to the R(D)SVS Internal Medicine Service following a 2 month history of ataxia and collapsing episodes which occurred
WHAT IS YOUR DIAGNOSIS? An 8 year old, female neutered cross breed dog was presented to the R(D)SVS Internal Medicine Service following a 2 month history of ataxia and collapsing episodes which occurred
Name: Oasis: Questions EPCP. Professional Development: Diabetes
 EPCP Professional Development: Diabetes Name: Oasis: Questions 1) Type 1 diabetes in characterized by which of the following: 1) adult onset, obesity 2) juvenile onset, lean build 3) auto-immune beta cell
EPCP Professional Development: Diabetes Name: Oasis: Questions 1) Type 1 diabetes in characterized by which of the following: 1) adult onset, obesity 2) juvenile onset, lean build 3) auto-immune beta cell
Changing Diabetes: The time is now!
 Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
Managing Congenital Hyperinsulinism in the Neonatal Period Vall d Hebron Hospital s Approach and Experience
 Managing Congenital Hyperinsulinism in the Alejandro Vargas Pieck Miquel Gussinyer Canadell María Clemente León Diego Yeste Fernández Universidad Autónoma de Barcelona Antonio Carrascosa Lezcano The first
Managing Congenital Hyperinsulinism in the Alejandro Vargas Pieck Miquel Gussinyer Canadell María Clemente León Diego Yeste Fernández Universidad Autónoma de Barcelona Antonio Carrascosa Lezcano The first
Managing Endocrine Related Issues after Bariatric Surgery. Jenny Tong, MD, MPH Division of Endocrinology March 3, 2018
 Managing Endocrine Related Issues after Bariatric Surgery Jenny Tong, MD, MPH Division of Endocrinology March 3, 2018 Bariatric Surgery was Associated with Higher Remission Rate than Usual Care 72.3% 38.1%
Managing Endocrine Related Issues after Bariatric Surgery Jenny Tong, MD, MPH Division of Endocrinology March 3, 2018 Bariatric Surgery was Associated with Higher Remission Rate than Usual Care 72.3% 38.1%
4/23/2015. Linda Steinkrauss, MSN, PNP. No conflicts of interest
 Linda Steinkrauss, MSN, PNP No conflicts of interest 1 5 year old African-American female presented to our Endocrinology Clinic with hypoglycemia Abnormal chromosomes Duplication of 11q13.5-11p14.1 affecting
Linda Steinkrauss, MSN, PNP No conflicts of interest 1 5 year old African-American female presented to our Endocrinology Clinic with hypoglycemia Abnormal chromosomes Duplication of 11q13.5-11p14.1 affecting
Hypoglycemia, diabetic medications
 Hypoglycemia, diabetic medications Michael Hodgman MD Upstate New York Poison Center May 2016 No financial disclosures with regards this presentation Unidentified male in 20s. Driver and only passenger
Hypoglycemia, diabetic medications Michael Hodgman MD Upstate New York Poison Center May 2016 No financial disclosures with regards this presentation Unidentified male in 20s. Driver and only passenger
Diabetes. Analyte Information
 Diabetes Analyte Information -1-2014-05-05 Diabetes Mellitus and other disorders of endocrine pancreas Introduction The pancreas is an important glandular organ of digestive and endocrine systems. Two
Diabetes Analyte Information -1-2014-05-05 Diabetes Mellitus and other disorders of endocrine pancreas Introduction The pancreas is an important glandular organ of digestive and endocrine systems. Two
بسم اهلل الرمحن الرحيم فمن شهد منكم الشهر
 بسم اهلل الرمحن الرحيم فمن شهد منكم الشهر فليصمه Najat Buzaid Introduction Ramadan is a lunar-based month, and its duration varies between 29 and 30 days. The fasting hours vary from 10 hours in a temperature
بسم اهلل الرمحن الرحيم فمن شهد منكم الشهر فليصمه Najat Buzaid Introduction Ramadan is a lunar-based month, and its duration varies between 29 and 30 days. The fasting hours vary from 10 hours in a temperature
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Diabetes in Pregnancy
 Diabetes in Pregnancy Susan Drummond RN MSN C-EFM Objectives 1. Describe types of diabetes and diagnosis of gestational diabetes 2. Identify a management plan for diabetes during pregnancy 3. Describe
Diabetes in Pregnancy Susan Drummond RN MSN C-EFM Objectives 1. Describe types of diabetes and diagnosis of gestational diabetes 2. Identify a management plan for diabetes during pregnancy 3. Describe
B.C. Drug and Poison Information Centre 655 West 12th Avenue, Vancouver, BC V5Z 4R4 Phone: (604) ; Fax: (604) Volume 31 (2) 2011
 ; Fax: (604) Volume 31 (2) 2011") Volume 31 (2) 2011 Editor and author: Barbara Cadario, BSc(Hon), BScPhm., MSc Chairman, Medical Review Laird Birmingham, MD, MHSc, FRCP(C) SYNONYM: NN2211 TRADE NAME: Victoza CLASSIFICATION GLP-1 receptor
Volume 31 (2) 2011 Editor and author: Barbara Cadario, BSc(Hon), BScPhm., MSc Chairman, Medical Review Laird Birmingham, MD, MHSc, FRCP(C) SYNONYM: NN2211 TRADE NAME: Victoza CLASSIFICATION GLP-1 receptor
5/12/2011. Recognize the major types of diabetes: Type 2, Type 1A, Type 1B, MODY, LADA, Pancreatic diabetes, drug-induced DM
 J. Christopher Lynch, Pharm.D. Professor Acting Associate Dean of Student Affairs Southern Illinois University Edwardsville School of Pharmacy The speaker has no conflicts of interest to disclose Recognize
J. Christopher Lynch, Pharm.D. Professor Acting Associate Dean of Student Affairs Southern Illinois University Edwardsville School of Pharmacy The speaker has no conflicts of interest to disclose Recognize