THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY 2013/12/21
|
|
|
- Magnus Dorsey
- 5 years ago
- Views:
Transcription

1 THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21

2 THE DIFFICULTY OF PANCREATIC SURGERY
3 ADVANCE OF PANCREATIC SURGERY AFTER WHIPPLE
4 COMPLICATED VESSELS AROUND THE PANCREAS

5 SURGERY FOR RESECTABLE PANCREATIC HEAD/DISTAL TUMOR
6 CLASSIC WHIPPLE OPERATION VS PPPD (PPPD op.) (Classic Whipple op.)

7 PALLIATIVE SURGERY FOR UNRESECTABLE PANCREATIC CANCER
8 THE MORTALITY OF PANCREATIC SURGERY
9 /2045 (61.2%) 60.0 Per rcent (%) /2045 (38.8%) 702/2045 (34.3%) 253/773 (32.7%) 414/1057 (39.2%) /773 (7.1%) M F Gender Resect ability Morbidity Mortality Adjuvant Chemotherapy Important Data of Pancreatic Cancer Surgery in 6 Major Centers in Taiwan
10 /2045 (61.2%) 60.0 Per rcent (%) /2045 (38.8%) 702/2045 (34.3%) 253/773 (32.7%) 414/1057 (39.2%) /773 (7.1%) M F Gender Resect ability Morbidity Mortality Adjuvant Chemotherapy Important Data of Pancreatic Cancer Surgery in 6 Major Centers in Taiwan
11 NO. OF PANCREATIC RESECTED IN CGMH
12 NO. OF TYPES OF SURGERY IN CGMH
13 TYPES & COMPLICATIONS IN CGMH p=0.148
14 1. Bleedings COMPLICATIONS AFTER PANCREATIC SURGERY 2. Fistula: pancreatic, duodenal, biliary / gastric 3. Delay gastric emptying 4. Pancreatitis 5. Metabolic problems: DM, exocrine insufficiency 6. Others: infection marginal ulcer, mesenteric thrombosis, distal CBD stricture, multiple organ failure
15 COMPLICATIONS OF PAN. SURGERY
16 COMPLICATIONS OF PAN. SURGERY
17 1. Bleedings COMPLICATIONS AFTER PANCREATIC SURGERY 2. Fistula: pancreatic, duodenal, biliary / gastric 3. Delay gastric emptying 4. Pancreatitis 5. Metabolic problems: DM, exocrine insufficiency 6. Others: infection marginal ulcer, mesenteric thrombosis, distal CBD stricture, multiple organ failure
18 POSTOPERATIVE BLEEDING Definition: Need for replacement with at least four packed RBC units, at least 24h after the end of operation.
19 TWO MAJOR TYPES OF POSTOPERATIVE BLEEDING 1. Luminal bleeding: Gastric bleeding Anastomotic bleeding 2. Extra-luminal bleeding: Op fields related vascular bleeding
20 TREATMENT OF DELAYED POST-OP. LUMINAL BLEEDING 1. Gastric bleeding: Endoscopic ex. using PPI or endoscopic therapy 2. Anastomotic bleeding: Endoscopic ex. using PPI or endoscopic therapy Interventional radiology - TAE
21
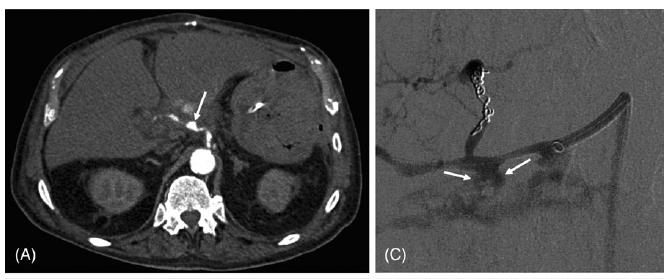
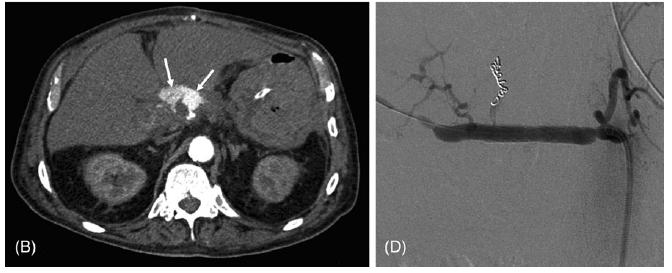
22 BLEEDING SOURCES OF POSTOPERATIVE BLEEDING
23 BLEEDING SOURCES OF POSTOPERATIVE BLEEDING
24 SOURCE OF BLEEDING & MANAGEMENT AFTER PANCREATIC SURGERY (Schafer M, et al. HBP 13:132-38, 2011)
25 Risk Factors of Massive Bleeding Related to Pancreatic Leak after Pancreaticoduodenectomy Risk Factors p value Infectious clinical signs Bile in drainage Type of pancreatic anastomosis 0.12 Texture at neck resection site 0.83 (Tien YW, et al. J Am Coll Surg 201:554--9, 2005)
26 TREATMENT OF OF EXTRA-LUMINAL BLEEDING 1. Conservative treatment: Transfusion, prn 2. Angiographic examination: Using T.A.E.
27 Angiography is Indicated for Every Sentinel Bleed after Pancreaticoduodenectomy Results: Sentinel bleed was detected in 20/283 pts., and pseudoaneurysm was detected in 7 patients (35%) by angio. Conclusions: Bleeding related mortality was significantly less than no angiography (Tien YW, et al. Annals Surgical Oncology 15: , 2008)
28 MANAGEMENT PATHWAY FOR EARLY POST-PANCREATIC OPERATIONAL BLEEDING E.PPOB Lum. bleeding E.L. bleeding Endoscopy Angiography No stop Stop Bleeder:+ Bleeder:- ReEndo/TAE TAE IA Vasopres. or Surgery Stop No stop Stop No stop Surgery Surgery
29 MANAGEMENT PATHWAY FOR EARLY POST-PANCREATIC OPERATIONAL BLEEDING E.PPOB Lum. bleeding E.L. bleeding Endoscopy Re-operation No stop Stop Bleeder:+ Bleeder:- ReEndo/TAE TAE IA Vasopres. or Surgery Stop No stop Stop No stop Surgery Surgery
30 MANAGEMENT PATHWAY FOR DELAYERD POST-PANCREATIC OPERATIONAL BLEEDING D.PPOB Lum. bleeding E.L. bleeding Endoscopy Angiography No stop Stop Bleeder:+ Bleeder:- ReEndo/TAE TAE IA Vasopres. or Surgery Stop No stop Stop No stop Surgery Surgery
31 MANAGEMENT PATHWAY FOR DELAYERD POST-PANCREATIC OPERATIONAL BLEEDING D.PPOB Lum. bleeding E.L. bleeding Endoscopy Angiography No stop Stop Bleeder:+ Bleeder:- ReEndo/TAE TAE IA Vasopres. or Surgery Stop No stop Stop No stop Surgery Surgery
32 MANAGEMENT PATHWAY FOR DELAYERD POST-PANCREATIC OPERATIONAL BLEEDING D.PPOB Lum. bleeding E.L. bleeding Endoscopy Angiography No stop Stop Bleeder:+ Bleeder:- ReEndo/TAE TAE IA Vasopres. or Surgery Stop No stop Stop No stop Surgery Surgery
33 MANAGEMENT PATHWAY FOR DELAYERD POST-PANCREATIC OPERATIONAL BLEEDING D.PPOB Lum. bleeding E.L. bleeding Endoscopy Angiography No stop Stop Bleeder:+ Bleeder:- ReEndo/TAE TAE IA Vasopres. or Surgery Stop No stop Stop No stop Surgery Surgery
34 MANAGEMENT PATHWAY FOR DELAYERD POST-PANCREATIC OPERATIONAL BLEEDING D.PPOB Lum. bleeding E.L. bleeding Endoscopy Angiography No stop Stop Bleeder:+ Bleeder:- ReEndo/TAE TAE IA Vasopres. or Surgery Stop No stop Stop No stop Surgery Surgery
35
36
37
38
39 MORBIDITY OF PATIENTS WITH DIFFERENT OPERATIVE PROCEDURES Postoperative bleeding GI fistula Ventral hernia 1. Sump tube drainage 19.4% 3.3% 4.9% 2. Open packing 10.0% 8.2% 13.9% 3. Irrigation lavage 13.3% Resection debridement 33.3% 0 0 (Hwang TL, et al. Hepato-Gastroenterology 42, 1995)
40 POSTOP. BLEEDING AFTER SURGERY OF AC. PANCREATITIS IN THE PAST 5 YEARS Op. Method Postop. Bleeding Treat. & Result Marsupilization 2 Debridement (2) & Packing Sump Drainage 10 TAE (4) OP with ligation (6) (Hwang TL, et al. Hepato-Gastroenterology 42, 1995)
41 MANAGEMENT OF POSTOP. BLEEDING IN SOME REPORTS
42 1. Bleedings COMPLICATIONS AFTER PANCREATIC SURGERY 2. Fistula: pancreatic, duodenal, biliary / gastric 3. Delay gastric emptying 4. Pancreatitis 5. Metabolic problems: DM, exocrine insufficiency 6. Others: infection marginal ulcer, mesenteric thrombosis, distal CBD stricture, multiple organ failure
43 LOCATIONS OF LEAKAGE AFTER PANCREATIC SURGERY
44 DEFINITION OF PANCREATIC FISTULA Output of any measurable volume of drain fluid on or after postoperative day 3, with amylase content > 3 times the upper normal serum value along with a clinical grading system to assess the impact of fistula on patients postoperative course. (Bassi C, et al. Surgery 138:8-13, 2005)
45 CLASSIFICATION OF PANCREATIC FISUTLA Classification Definition 1 Output > 10 ml/d of amylase-rich fluid after postoperative day 5 or for > 5 days 2 Output > 10 ml/d of amylase-rich fluid after postoperative day 8 or for > 8 days 3 Output > 25 ml/d and 100 ml/d of amylaserich fluid after postoperative day 8 or for > 8 days 4 Output > than 50 ml/d of amylase-rich fluid after postoperative day 11 or for > 11 days
46 MANIFESTAITONS FOR DIFFERENT GRADES OF PANCREATIC FISUTLA (Dellaportas D, et al. World J Gastroenterology 27:381-4, 2010)
47 MANAGEMENT OF PANCREATIC FISTULA A. Conservative management: 1. Nasogastric drainage 2. TPN 3. Reducing pancreatic secretion 4. Percutaneous drainage
48 MANAGEMENT OF PANCREATIC FISTULA B. Surgical management: 1. Repair the site of leakage with wide peripancreatic drainage 2. Alternative pancreatic enteric anastomosis 3. Completion pancreatectomy
49 INCIDENCE AND MANAGEMENT OF PANCREATIC FISUTLA (Dellaportas D, et al. World J Gastroenterology 27:381-4, 2010)
50 1. Bleedings COMPLICATIONS AFTER PANCREATIC SURGERY 2. Fistula: pancreatic, duodenal, biliary / gastric 3. Delay gastric emptying 4. Pancreatitis 5. Metabolic problems: DM, exocrine insufficiency 6. Others: infection marginal ulcer, mesenteric thrombosis, distal CBD stricture, multiple organ failure
51 DEFINITION OF DELAY GASTRIC EMPTYING Persistent secretion of gastric juice more than 500 ml/day for > 5 days or recurrent vomiting in combination with swelling of gastrojejunostomy / duodenojejunostomy and dilatation of the stomach in contrast medium passage studies. (Seiler CA, et al. J Gastrointestinal Surg 4:443-52, 2000)
52 INCIDENCE OF DELAY GASTRIC EMPTYING Authors(Ref) Year Type of study Patient number PPPD WPD PPP D DGE incidence WPD Van Berge HMI et al (3) 1997 Retrospective % 34% Seiler et al (4) 2000 RCT % 45% Tran et al (5) 2004 RCT % 23% Lin et al (6) 2005 RCT % 0% RCT: Randomized controlled trial PPPD:Pylorus preserving pancreaticoduodenectomy WPD:Whipple procedure (Seiler CA, et al. J Gastrointestinal Surg 4:443-52, 2000)
53 FACTORS LELATED TO DELAYED GASTRIC EMPTYING A. Intraoperative factors: 1. Vascular 2. Neural 3. Extent of LNs dissection B. Postoperative factors: 1. Intra-abdominal abdominal sepsis 2. Somatostatin analogue
54 MANAGEMENT OF DELAYED GASTRIC EMPTYING A. Conservative management: 1. Nasogastric drainage 2. TPN or PPN 3. Reducing pancreatic secretion
55 1. Bleedings COMPLICATIONS AFTER PANCREATIC SURGERY 2. Fistula: pancreatic, duodenal, biliary / gastric 3. Delay gastric emptying 4. Pancreatitis 5. Metabolic problems: DM, exocrine insufficiency 6. Others: infection marginal ulcer, mesenteric thrombosis, distal CBD stricture, multiple organ failure
56 THE ANNULAR MORTALITY OF ACUTE PANCREATITIS IN CGMH Total Total Cases Male Female (1.5/1) Mortality Mor. Rate 2.89% 4.06% 2.99% 1.59% 2.04% 2.87%
57 INTENSIVE TREATMENT & OUTCOME OF SEVERE ACUTE PANCREATITIS 3<R. S.<6 R.S.>6 Total Patients no Early complications Late complications Operation Mortality 1 (4.3%) 4 (21%) 5 (12%) (Hwang TL, et al. Hepato-Gastroenterology 42, 1995)


58 THE SEVEREITY GRADING OF PANCREATIC TRAUMA


59 THE COMPLICATIONS AFTER SURGERY FOR PANCREATIC TRAUMA (Al-Ahmadi, Ahmadi, et al. J Can Chir 51, 2008)
60 SUMMARY 1. The complications after pancreatic surgery were not low, which had no relation to the operative types. 2. Endovascular intervention represents the first-line treatment for hemorrhage from pseudoaneurysms after pancreatic surgery. 3. Endovascular embolization or stent-graft placement should be selected individually depending on the involved artery and its vascular anatomy.
61 THE DIFFICULTY OF PANCREATIC SURGERY

62 Thanks for your attention!
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Reinterventions belong to complications
 Reinterventions belong to complications Pancreatic surgery is the archetypus of complex abdominal surgery Mortality (1-4%) and morbidity (7-60%) rates are relevant even at high volume centres Reinterventions
Reinterventions belong to complications Pancreatic surgery is the archetypus of complex abdominal surgery Mortality (1-4%) and morbidity (7-60%) rates are relevant even at high volume centres Reinterventions
Henry A. Pitt, M.D., F.A.C.S. Chief Quality Officer Temple University Health System July 23, 2018 Orlando, Florida
 Are All OSIs Pancreatic Fistulas? Henry A. Pitt, M.D., F.A.C.S. Chief Quality Officer Temple University Health System July 23, 2018 Orlando, Florida DISCLOSURES Leader, ACS-NSQIP HPB Collaborative Hepatectomy
Are All OSIs Pancreatic Fistulas? Henry A. Pitt, M.D., F.A.C.S. Chief Quality Officer Temple University Health System July 23, 2018 Orlando, Florida DISCLOSURES Leader, ACS-NSQIP HPB Collaborative Hepatectomy
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Complex pancreatico- duodenal injuries. Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University
 Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Pancreaticoduodenectomy
 Pancreaticoduodenectomy A Valuable Surgery Paul Montero PGY-III September 11, 2006 Overview Brief History Perils of Early Pancreaticoduodenectomy (PD) Improvements Quality of Life after PD Widened Indications
Pancreaticoduodenectomy A Valuable Surgery Paul Montero PGY-III September 11, 2006 Overview Brief History Perils of Early Pancreaticoduodenectomy (PD) Improvements Quality of Life after PD Widened Indications
Pylorus Preserving Pancreaticoduodenectomy: Superior to Classic Pancreaticoduoenectomy
 Pylorus Preserving Pancreaticoduodenectomy: Superior to Classic Pancreaticoduoenectomy David Mauchley, MD University of Colorado, Denver Department of Surgery Grand Rounds December 14 th, 2009 Pancreatic
Pylorus Preserving Pancreaticoduodenectomy: Superior to Classic Pancreaticoduoenectomy David Mauchley, MD University of Colorado, Denver Department of Surgery Grand Rounds December 14 th, 2009 Pancreatic
Fat Tissue Infiltration into the Pancreas Parenchyme and Its Effect on the Result of Surgery
 Korean Journal of HBP Surgery Vol. 15,. 2, May 2011 O riginal Article Fat Tissue Infiltration into the Pancreas Parenchyme and Its Effect on the Result of Surgery Purpose: In Korea, there are few reports
Korean Journal of HBP Surgery Vol. 15,. 2, May 2011 O riginal Article Fat Tissue Infiltration into the Pancreas Parenchyme and Its Effect on the Result of Surgery Purpose: In Korea, there are few reports
Surgery for pancreatic cancer
 Surgery for pancreatic cancer Andrew Smith 12 September 2018 Leeds Regional Study Day North & West Yorkshire Pancreas Department Pancreatic Surgery Range of pancreatic surgery Pre-op preparation Post op
Surgery for pancreatic cancer Andrew Smith 12 September 2018 Leeds Regional Study Day North & West Yorkshire Pancreas Department Pancreatic Surgery Range of pancreatic surgery Pre-op preparation Post op
GENERAL SURGERY. Introduction. M M Bernon, 1,4 J E J Krige, 1,4 E Jonas, 1,4 J C Kloppers, 1 S Burmeister, 1,4 N G Naidoo, 2 S J Beningfield 3,4
 GENERAL SURGERY Severe post-pancreatoduodenectomy haemorrhage: An analytical review based on 118 consecutive pancreatoduodenectomy patients in a South African Academic Hospital M M Bernon, 1,4 J E J Krige,
GENERAL SURGERY Severe post-pancreatoduodenectomy haemorrhage: An analytical review based on 118 consecutive pancreatoduodenectomy patients in a South African Academic Hospital M M Bernon, 1,4 J E J Krige,
Late Postpancreatectomy Hemorrhage After Pancreaticoduodenectomy: Is It Possible to Recognize Risk Factors?
 ORIGINAL ARTICLE Late Postpancreatectomy Hemorrhage After Pancreaticoduodenectomy: Is It Possible to Recognize Risk Factors? Claudio Ricci, Riccardo Casadei, Salvatore Buscemi, Francesco Minni Department
ORIGINAL ARTICLE Late Postpancreatectomy Hemorrhage After Pancreaticoduodenectomy: Is It Possible to Recognize Risk Factors? Claudio Ricci, Riccardo Casadei, Salvatore Buscemi, Francesco Minni Department
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Surgical Management of CBD Injury Jin Seok Heo
 Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Disclosures. Dr. Hall is a paid consultant to the American College of Surgeons (ACS) as Associate Director of ACS-NSQIP
 as Associate Director of ACS-NSQIP") Does Routine Drainage of the Operative Bed following Elective Distal Pancreatectomy reduce Complications? An Analysis of the ACS-NSQIP Pancreatectomy Demonstration Project Stephen W. Behrman, MD 1, Ben
Does Routine Drainage of the Operative Bed following Elective Distal Pancreatectomy reduce Complications? An Analysis of the ACS-NSQIP Pancreatectomy Demonstration Project Stephen W. Behrman, MD 1, Ben
Prevention Of Pancreaticojejunal Fistula After Whipple Procedure
 ISPUB.COM The Internet Journal of Surgery Volume 4 Number 2 Prevention Of Pancreaticojejunal Fistula After Whipple Procedure N Barbetakis, K Setsiz Citation N Barbetakis, K Setsiz. Prevention Of Pancreaticojejunal
ISPUB.COM The Internet Journal of Surgery Volume 4 Number 2 Prevention Of Pancreaticojejunal Fistula After Whipple Procedure N Barbetakis, K Setsiz Citation N Barbetakis, K Setsiz. Prevention Of Pancreaticojejunal
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Original Article. Gastrointestinal bleeding in acute pancreatitis: etiology, clinical features, risk factors and outcome
 Tropical Gastroenterology 2015;36(1):31 35 Original Article Gastrointestinal bleeding in acute pancreatitis: etiology, clinical features, risk factors and outcome Surinder S Rana 1, Vishal Sharma 1, Deepak
Tropical Gastroenterology 2015;36(1):31 35 Original Article Gastrointestinal bleeding in acute pancreatitis: etiology, clinical features, risk factors and outcome Surinder S Rana 1, Vishal Sharma 1, Deepak
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
Pylorus Preserving Pancreaticoduodenectomy
 REVIEW Pylorus Preserving Pancreaticoduodenectomy Jacqueline M. Garonzik-Wang, M. B. Majella Doyle Pancreaticoduodenectomy (PD) has become the standard of care for resectable pancreatic cancer and premalignant
REVIEW Pylorus Preserving Pancreaticoduodenectomy Jacqueline M. Garonzik-Wang, M. B. Majella Doyle Pancreaticoduodenectomy (PD) has become the standard of care for resectable pancreatic cancer and premalignant
3/28/2012. Periampullary Tumors. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Eric K. Nakakura Ko Olina, HI
 Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
The mortality rate after major pancreatic and biliary surgery
 ORIGINAL ARTICLES After Pancreatic and Biliary Surgery Embolization or Surgery? Steve M. M. de Castro, MD,* Koert F. D. Kuhlmann, MD,* Olivier R. C. Busch, MD,* Otto M. van Delden, MD, Johan S. Laméris,
ORIGINAL ARTICLES After Pancreatic and Biliary Surgery Embolization or Surgery? Steve M. M. de Castro, MD,* Koert F. D. Kuhlmann, MD,* Olivier R. C. Busch, MD,* Otto M. van Delden, MD, Johan S. Laméris,
Chronic Pancreatitis
 Gastro Foundation Fellows Weekend 2017 Chronic Pancreatitis Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Aetiology in SA Alcohol (up to 80%) Idiopathic Tropical Obstruction Autoimmune
Gastro Foundation Fellows Weekend 2017 Chronic Pancreatitis Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Aetiology in SA Alcohol (up to 80%) Idiopathic Tropical Obstruction Autoimmune
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
5/17/2013. Pancreatic Cancer. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Case presentation. Differential diagnosis
 Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
OCTREOTIDE IN THE PREVENTION AND TREATMENT OF GASTROINTESTINAL AND PANCREATIC FISTULAS
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Pancreaticoduodenectomy the anatomy and the surgical approaches
 Pancreaticoduodenectomy the anatomy and the surgical approaches Paul BS LAI Division of Hepato biliary and Pancreatic Surgery Department of Surgery The Chinese Univesity of Hong Kong Whipple s operation
Pancreaticoduodenectomy the anatomy and the surgical approaches Paul BS LAI Division of Hepato biliary and Pancreatic Surgery Department of Surgery The Chinese Univesity of Hong Kong Whipple s operation
Case 37 Clinical Presentation
 Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
P resently, pancreaticoduodenectomy is widely accepted as the standard surgical procedure for patients with
 OPEN SUBJECT AREAS: CANCER THERAPY PANCREATIC CANCER GASTROINTESTINAL CANCER OUTCOMES RESEARCH Received 13 May 2013 Accepted 3 June 2013 Published 25 June 2013 Correspondence and requests for materials
OPEN SUBJECT AREAS: CANCER THERAPY PANCREATIC CANCER GASTROINTESTINAL CANCER OUTCOMES RESEARCH Received 13 May 2013 Accepted 3 June 2013 Published 25 June 2013 Correspondence and requests for materials
Key words: gastric cancer, postoperative complication, total gastrectomy
 Key words: gastric cancer, postoperative complication, total gastrectomy 115 (115) Fig. 1 Technique of esophagojejunostomy (Quotation from Shimotsuma M and Nakamura R')). A, Technique for hand suture for
Key words: gastric cancer, postoperative complication, total gastrectomy 115 (115) Fig. 1 Technique of esophagojejunostomy (Quotation from Shimotsuma M and Nakamura R')). A, Technique for hand suture for
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT
 BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT By: Amy Cisyk Home for the Summer Program July, 2016 Brandon, Manitoba Supervisor: Dr. Marvin Goossen Whipple s Procedure Audit
BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT By: Amy Cisyk Home for the Summer Program July, 2016 Brandon, Manitoba Supervisor: Dr. Marvin Goossen Whipple s Procedure Audit
Postpancreatectomy Hemorrhage: Imaging and Interventional Radiological Treatment
 Postpancreatectomy Hemorrhage: Imaging and Interventional Radiological Treatment Poster No.: C-1422 Congress: ECR 2014 Type: Educational Exhibit Authors: T. Matsuura, K. Takase, T. Hasegawa, H. Ota, K.
Postpancreatectomy Hemorrhage: Imaging and Interventional Radiological Treatment Poster No.: C-1422 Congress: ECR 2014 Type: Educational Exhibit Authors: T. Matsuura, K. Takase, T. Hasegawa, H. Ota, K.
Bile Duct Injury during Lap Chole. Bile Duct Injury during cholecystectomy TOPICS. 1. Prevalence, mechanisms, prevention and diagnosis
 Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Application of a novel embeddedness like pancreaticojejunostomy anastomosis technique used in pancreaticoduodenectomy
 ONCOLOGY LETTERS 15: 8067-8071, 2018 Application of a novel embeddedness like pancreaticojejunostomy anastomosis technique used in pancreaticoduodenectomy XUEFENG XU *, YANG LV *, LEI ZHANG *, BAOBAO XIN,
ONCOLOGY LETTERS 15: 8067-8071, 2018 Application of a novel embeddedness like pancreaticojejunostomy anastomosis technique used in pancreaticoduodenectomy XUEFENG XU *, YANG LV *, LEI ZHANG *, BAOBAO XIN,
BILIARY TRACT & PANCREAS, PART II
 CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
Biliary Anatomy in Living-related Liver Transplantation
 The 5th IHPBA Congress - Istanbul Biliary Anatomy in Living-related Liver Transplantation biliary trees hilar plate Assessment for Vascular Anatomy 1. 3DCT portal vein hepatic vein hepatic artery 2. No
The 5th IHPBA Congress - Istanbul Biliary Anatomy in Living-related Liver Transplantation biliary trees hilar plate Assessment for Vascular Anatomy 1. 3DCT portal vein hepatic vein hepatic artery 2. No
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment)
") Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
DO DRAINS HELP OR HURT IN HPB SURGERY? Henry A. Pitt, M.D. Chief Quality Officer Temple University Health System July 23, 2017
 DO DRAINS HELP OR HURT IN HPB SURGERY? Henry A. Pitt, M.D. Chief Quality Officer Temple University Health System July 23, 217 DISCLOSURES Henry A. Pitt has nothing to disclose Leader of the ACS-NSQIP HPB
DO DRAINS HELP OR HURT IN HPB SURGERY? Henry A. Pitt, M.D. Chief Quality Officer Temple University Health System July 23, 217 DISCLOSURES Henry A. Pitt has nothing to disclose Leader of the ACS-NSQIP HPB
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
Endoscopic Ultrasonography Assessment for Ampullary and Bile Duct Malignancy
 Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: van der Gaag NA, Rauws EAJ, van Eijck CHJ, et al. Preoperative
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: van der Gaag NA, Rauws EAJ, van Eijck CHJ, et al. Preoperative
Obstructive Jaundice; A Clinical Study of Malignant Causes.
 DOI: 10.21276/aimdr.2018.4.1.SG6 Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 Obstructive Jaundice; A Clinical Study of Malignant Causes. Bhuban Mohan Das 1, Sushil Kumar Patnaik 1, Chitta Ranjan
DOI: 10.21276/aimdr.2018.4.1.SG6 Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 Obstructive Jaundice; A Clinical Study of Malignant Causes. Bhuban Mohan Das 1, Sushil Kumar Patnaik 1, Chitta Ranjan
Whipple pancreatoduodenectomy
 Vascular and Interventional Radiology Pictorial Essay Puppala et al. Hemorrhagic Complications After Whipple Surgery Vascular and Interventional Radiology Pictorial Essay Sapna Puppala 1 Jai Patel Simon
Vascular and Interventional Radiology Pictorial Essay Puppala et al. Hemorrhagic Complications After Whipple Surgery Vascular and Interventional Radiology Pictorial Essay Sapna Puppala 1 Jai Patel Simon
Chronic Pancreatitis: Surgical Options. W. Charles Conway MD, FACS Upper GI/HPB Surgical Oncology Ochsner Medical Center New Orleans, LA
 Chronic Pancreatitis: Surgical Options W. Charles Conway MD, FACS Upper GI/HPB Surgical Oncology Ochsner Medical Center New Orleans, LA Chronic Pancreatitis Recurrent, debilitating abdominal pain with
Chronic Pancreatitis: Surgical Options W. Charles Conway MD, FACS Upper GI/HPB Surgical Oncology Ochsner Medical Center New Orleans, LA Chronic Pancreatitis Recurrent, debilitating abdominal pain with
The gastroduodenal artery: Radiological anatomy, imaging and endovascular intervention
 The gastroduodenal artery: Radiological anatomy, imaging and endovascular intervention Poster No.: C-2049 Congress: ECR 2010 Type: Educational Exhibit Topic: Interventional Radiology Authors: R. D. White,
The gastroduodenal artery: Radiological anatomy, imaging and endovascular intervention Poster No.: C-2049 Congress: ECR 2010 Type: Educational Exhibit Topic: Interventional Radiology Authors: R. D. White,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE. PRESENTED BY: Susan DePasquale, CGRN, MSN
 PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
Routine nasogastric suction may be unnecessary after a pancreatic resection
 DOI:10.1111/j.1477-2574.2011.00359.x HPB ORIGINAL ARTICLE Routine nasogastric suction may be unnecessary after a pancreatic resection William E. Fisher, Sally E. Hodges, Guillermina Cruz, Avo Artinyan,
DOI:10.1111/j.1477-2574.2011.00359.x HPB ORIGINAL ARTICLE Routine nasogastric suction may be unnecessary after a pancreatic resection William E. Fisher, Sally E. Hodges, Guillermina Cruz, Avo Artinyan,
1. Epidemiology of Esophageal Cancer 2. Operative Strategies 3. Minimally Invasive Esophagectomy 4. Video
 Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Managing Complications of Bariatric Surgery. Objectives
 Managing Complications of Bariatric Surgery John J. Vargo, II, MD, MPH, FACG Chair, Department of Gastroenterology and Hepatology Digestive Disease and Surgery Institute Cleveland Clinic Cleveland, OH
Managing Complications of Bariatric Surgery John J. Vargo, II, MD, MPH, FACG Chair, Department of Gastroenterology and Hepatology Digestive Disease and Surgery Institute Cleveland Clinic Cleveland, OH
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Causes of pancreatic insufficiency. Eugen Dumitru
 Causes of pancreatic insufficiency Eugen Dumitru Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes 3. The Consequences Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes
Causes of pancreatic insufficiency Eugen Dumitru Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes 3. The Consequences Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes
Information Technology Solutions
 2016 2014 CPT Esophagoscopy Changes - Gastroenterology CPT Changes Information Technology Solutions ASGE LOGO AND INFO Esophagogastroduodenoscopy CPT Codes 43235-43270 The American Society for Gastrointestinal
2016 2014 CPT Esophagoscopy Changes - Gastroenterology CPT Changes Information Technology Solutions ASGE LOGO AND INFO Esophagogastroduodenoscopy CPT Codes 43235-43270 The American Society for Gastrointestinal
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options
 Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
Citation Hepato-Gastroenterology, 55(86-87),
,") NAOSITE: Nagasaki University's Ac Title Author(s) Combined pancreatic resection and p multiple lesions of the pancreas: i of the pancreas concomitant with du Kuroki, Tamotsu; Tajima, Yoshitsugu Tomohiko;
NAOSITE: Nagasaki University's Ac Title Author(s) Combined pancreatic resection and p multiple lesions of the pancreas: i of the pancreas concomitant with du Kuroki, Tamotsu; Tajima, Yoshitsugu Tomohiko;
INFORMATION ON PANCREATIC HEAD AND PERIAMPULLARY CANCER
 INFORMATION ON PANCREATIC HEAD AND PERIAMPULLARY CANCER What is Pancreas? The pancreas is a gland located in the back of your abdomen behind the stomach. pancreas is divided into four parts: the head,
INFORMATION ON PANCREATIC HEAD AND PERIAMPULLARY CANCER What is Pancreas? The pancreas is a gland located in the back of your abdomen behind the stomach. pancreas is divided into four parts: the head,
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
Safety of pancreatic resection in the elderly: a retrospective analysis of 556 patients
 ORIGINAL ARTICLE Annals of Gastroenterology (2016) 29, 1-5 Safety of pancreatic resection in the elderly: a retrospective analysis of 556 patients Daniel Ansari, Linus Aronsson, Joakim Fredriksson, Bodil
ORIGINAL ARTICLE Annals of Gastroenterology (2016) 29, 1-5 Safety of pancreatic resection in the elderly: a retrospective analysis of 556 patients Daniel Ansari, Linus Aronsson, Joakim Fredriksson, Bodil
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Case discussion. Anastomotic leakage. intern superviser
 Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
A Simple, Secure and Universal
 HPB Surgery, 1997, Vol. 10, pp. 305-310 Reprints available directly from the publisher Photocopying permitted by license only (C) 1997 OPA (Overseas Publishers Association) Amsterdam B.V. Published in
HPB Surgery, 1997, Vol. 10, pp. 305-310 Reprints available directly from the publisher Photocopying permitted by license only (C) 1997 OPA (Overseas Publishers Association) Amsterdam B.V. Published in
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
Update in abdominal Surgery in cirrhotic patients
 Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
Percutaneous Transarterial Embolization of Pseudoaneurysm Secondary to Pancreatitis: a case report
 Chin J Radiol 2003; 28: 347-351 347 Percutaneous Transarterial Embolization of Pseudoaneurysm Secondary to Pancreatitis: a case report HSIN-YI LAI YUNG-FANG CHEN HSEIN-JAR CHIANG WU-CHUNG SHEN Department
Chin J Radiol 2003; 28: 347-351 347 Percutaneous Transarterial Embolization of Pseudoaneurysm Secondary to Pancreatitis: a case report HSIN-YI LAI YUNG-FANG CHEN HSEIN-JAR CHIANG WU-CHUNG SHEN Department
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Computed Tomography (CT) imaging following Whipple procedure: A pictorial essay of normal postoperative findings and complications
 imaging following Whipple procedure: A pictorial essay of normal postoperative findings and complications") Computed Tomography (CT) imaging following Whipple procedure: A pictorial essay of normal postoperative findings and complications Poster No.: R-0200 Congress: 2014 CSM Type: Scientific Exhibit Authors:
Computed Tomography (CT) imaging following Whipple procedure: A pictorial essay of normal postoperative findings and complications Poster No.: R-0200 Congress: 2014 CSM Type: Scientific Exhibit Authors:
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
LONG TERM OUTCOME OF ELECTIVE SURGERY
 LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
Overview. Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco
 GASTROINTESTINAL COMPLICATIONS AFTER BARIATRIC SURGERY Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco UCSF DEPARTMENT OF SURGERY Original Article
GASTROINTESTINAL COMPLICATIONS AFTER BARIATRIC SURGERY Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco UCSF DEPARTMENT OF SURGERY Original Article
Malignant Obstructive Jaundice has dismal
 Proceeding S.Z.P.G.M.L vol: 22(2}: pp. 79-83, 2008. Anatomic Level of Biliary Obstruction and Outcome of Pre-Operative Biliary Stenting in Malignant Obstructive Jaundice -A Shaikh Zayed Hospital Experience
Proceeding S.Z.P.G.M.L vol: 22(2}: pp. 79-83, 2008. Anatomic Level of Biliary Obstruction and Outcome of Pre-Operative Biliary Stenting in Malignant Obstructive Jaundice -A Shaikh Zayed Hospital Experience
Pancreatic Lesions. Valerie Jefford Pediatric Surgery Rounds June 6, 2003
 Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Complication of Laparoscopic Cholecystectomy
 Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Definitive Surgical Treatment When Endoscopy Fails. Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept.
 Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
1 Year Result Of Stent Graft For Carotid Artery Pseudo- Aneurysm In Behcet s Disease Patients
 1 Year Result Of Stent Graft For Carotid Artery Pseudo- Aneurysm In Behcet s Disease Patients H Lotfy, W Shaalan, A Elemam, A Naga Prof Dr Hassan Lotfy Vascular and Endovascular Consultant Alexandria University
1 Year Result Of Stent Graft For Carotid Artery Pseudo- Aneurysm In Behcet s Disease Patients H Lotfy, W Shaalan, A Elemam, A Naga Prof Dr Hassan Lotfy Vascular and Endovascular Consultant Alexandria University
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
General Surgery PURPLE SERVICE MUHC-RVH Site
 Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
MATERIALS AND METHODS Patients
 Yonago Acta medica 216;59:232 236 Original Article Usefulness of T-Shaped Gauze for Precise Dissection of Supra-Pancreatic Lymph Nodes and for Reduced Postoperative Pancreatic Fistula in Patients Undergoing
Yonago Acta medica 216;59:232 236 Original Article Usefulness of T-Shaped Gauze for Precise Dissection of Supra-Pancreatic Lymph Nodes and for Reduced Postoperative Pancreatic Fistula in Patients Undergoing
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Minimally Invasive Esophagectomy- Valuable. Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006
 Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
ERCP in altered anatomy. Lars Aabakken Oslo University Hospital - Rikshospitalet Oslo, Norway
 ERCP in altered anatomy Lars Aabakken Oslo University Hospital - Rikshospitalet Oslo, Norway CO2 as insufflation gas Reduces post-procedure pain Reduces in-procedure bowel distension Improves the intubation
ERCP in altered anatomy Lars Aabakken Oslo University Hospital - Rikshospitalet Oslo, Norway CO2 as insufflation gas Reduces post-procedure pain Reduces in-procedure bowel distension Improves the intubation
Endoscopic management of postoperative bile duct injuries: a single center experience.
 1- Endoscopic management of postoperative bile duct injuries: a single center experience. BACKGROUND/AIM: Biliary endoscopic procedures may be less invasive than surgery for management of postoperative
1- Endoscopic management of postoperative bile duct injuries: a single center experience. BACKGROUND/AIM: Biliary endoscopic procedures may be less invasive than surgery for management of postoperative
NEUROENDOCRINE CARCINOID TUMORS PANCREATIC NEUROENDOCRINE TUMORS
 University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
EGD Data Collection Form
 Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Classification and Management of Leaks after Gastric Bypass for Patients with Morbid Obesity: A Prospective Study of 60 Patients
 OBES SURG (2012) 22:855 862 DOI 10.1007/s11695-011-0519-6 CLINICAL REPORT Classification and Management of Leaks after Gastric Bypass for Patients with Morbid Obesity: A Prospective Study of 60 Patients
OBES SURG (2012) 22:855 862 DOI 10.1007/s11695-011-0519-6 CLINICAL REPORT Classification and Management of Leaks after Gastric Bypass for Patients with Morbid Obesity: A Prospective Study of 60 Patients
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist. Alireza Sedarat, MD UCLA Division of Digestive Diseases
 Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Cuneyt Kayaalp, Murat Sait Dogan, and Veysel Ersan. Department of Surgery, Inonu University, Malatya, Turkey
 Ann Hepatobiliary Pancreat Surg 2017;21:101-105 https://doi.org/10.14701/ahbps.2017.21.2.101 Case Report Surgery for intractable pain in a patient with chronic pancreatitis complicated with biliary obstruction,
Ann Hepatobiliary Pancreat Surg 2017;21:101-105 https://doi.org/10.14701/ahbps.2017.21.2.101 Case Report Surgery for intractable pain in a patient with chronic pancreatitis complicated with biliary obstruction,
Department of Hepatobiliary and Pancreatic Surgery About Pancreatic Surgery A guide for patients and relatives
 Department of Hepatobiliary and Pancreatic Surgery About Pancreatic Surgery A guide for patients and relatives page 2 This booklet has been written to provide information about the surgical procedures
Department of Hepatobiliary and Pancreatic Surgery About Pancreatic Surgery A guide for patients and relatives page 2 This booklet has been written to provide information about the surgical procedures
Case Presentation. PMH: HTN, BPH, strabismus PSH: appendectomy Medications: norvasc, tamsulosin NKDA SH/FH: negative
 Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
PANCREAS DUCTAL ADENOCARCINOMA PDAC
 CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
Patient characteristics Intervention Comparison Length of follow-up. Endoscopic treatment. Endoscopic transampullary drainage of the pancreatic duct
 1) In patients with alcohol-related, what is the safety and efficacy of a) coeliac access block vs medical management b) thoracoscopic splanchnicectomy vs medical management c) coeliac access block vs
1) In patients with alcohol-related, what is the safety and efficacy of a) coeliac access block vs medical management b) thoracoscopic splanchnicectomy vs medical management c) coeliac access block vs
Shuichi Fujioka 1*, Fumitake Suzuki 1, Naotake Funamizu 1, Tomoyoshi Okamoto 1, Koji Munakata 2, Hirokazu Ashida 2 and Katsuhiko Yanaga 3
 Fujioka et al. Surgical Case Reports (2015) 1:60 DOI 10.1186/s40792-015-0060-2 CSE REPORT Stent graft placement and balloon dilation for pseudoaneurysm complicated by distal arterial stenosis of the hepatic
Fujioka et al. Surgical Case Reports (2015) 1:60 DOI 10.1186/s40792-015-0060-2 CSE REPORT Stent graft placement and balloon dilation for pseudoaneurysm complicated by distal arterial stenosis of the hepatic