Pancreatobiliary Frozen Section Nightmares
|
|
|
- Damon Gilbert
- 5 years ago
- Views:
Transcription
1 Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology Objectives Briefly give an overview or perspective of pancreatic cancer. Review the appropriate margins to be taken for frozen section from pancreatobiliary specimens. Examine the histopathology of pancreatobiliary margins on frozen section. Discuss some of the difficulties ( gray areas ) in assessing pancreatobiliary margins. 4th Leading cause of cancer deaths in the United States. 1st Mortality rate among all major cancers. LAST 40 YEARS Pancreatic Breast Leukemia Cancer 5-Year 5-Year Survival Survival Rate Rate Rate Trend Trend 90.2 % 75.1 % 58.1 % 34.4 % 2 % 6% 1973 Of Breast the 10 Clinical cancer most survival trials lethal have cancers, rates helped have pancreatic turn increased the cancer odds significantly. in remains 2013 Breakthroughs the only favor one in early with of those a detection single-digit with leukemia. deserve survival much rate. credit. Adapted from 1

2 4th Leading cause of cancer deaths in the United States. 1st Mortality rate among all major cancers. 94% 74% 55% 0 Die within 5 years of being diagnosed. Die within the first year of diagnosis. Increase in new pancreatic cancer cases projected over the next 2 decades. Early detection methods and successful treatment options have been discovered. Adapted from 20% Surgically resectable and considered the only chance for a cure. Adapted from 2



3 Vascular groove Uncinate process Adapted from Vascular groove Uncinate process Adapted from 3
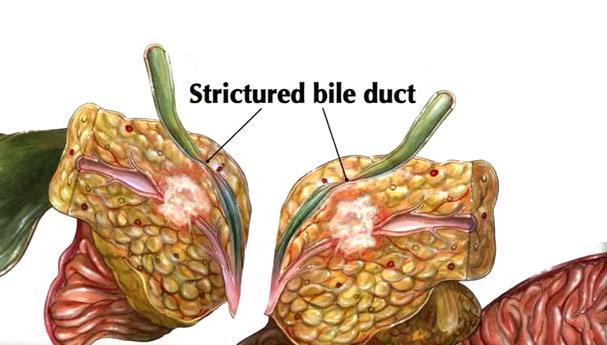
4 Bile Duct Margin Pancreatic Neck Margin Adapted from Pancreatic Neck Margin Adapted from Bile Duct Margin Bbb Pancreatic Neck Margin Adapted from 4


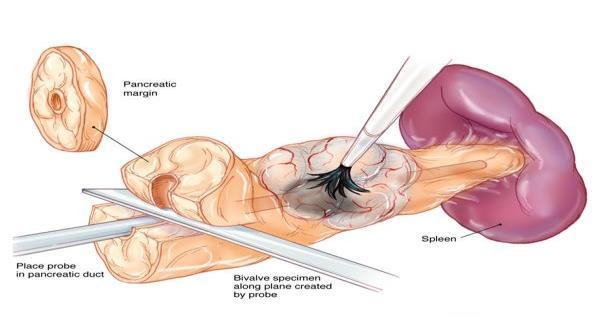
5 Bile Duct Margin Pancreatic Neck Margin Proximal Duodenal Margin Adapted from Adapted from Adapted from 5

6 Adapted from Adapted from Adapted from 6

7 Adapted from Adapted from Adapted from 7


8 Adapted from Pancreatic Neck Margins - Artifacts FFPE Pancreatic Neck Margins - Artifacts 8
 Pancreatic Neck")
 Over staining (eosin) Pancreatic Neck")
9 Pancreatic Neck Margins - Artifacts Tissue folding Tissue folding Over staining (hematoxylin) Pancreatic Neck Margins - Artifacts Tissue folding Over staining (hematoxylin) Over staining (eosin) Pancreatic Neck Margins - Artifacts 9
10 Pancreatic Neck Margins - Artifacts Tissue folding Over staining (hematoxylin) Over staining (eosin) Cauterization Tissue folding Over staining (hematoxylin) Over staining (eosin) Cauterization Drying Pancreatic Neck Margins - Artifacts Tissue folding Over staining (hematoxylin) Over staining (eosin) Cauterization Drying Thick sections Pancreatic Neck Margins - Artifacts 10
 Over staining (eosin)")


11 Pancreatic Neck Margins - Artifacts Tissue folding Over staining (hematoxylin) Over staining (eosin) Cauterization Drying Thick sections Air bubbles Normal Pancreas Pancreatic Neck Margins Normal Pancreas Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules 11
 Interlobular fibrosis (absence of")
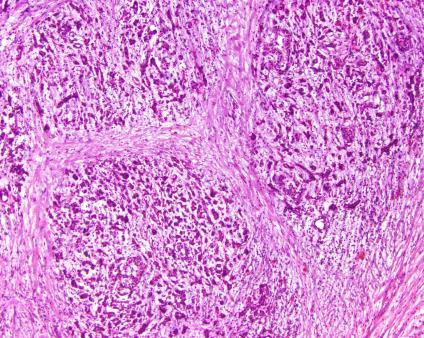
12 Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss 12
 Acinar loss (absence of glands) Acinar loss Ductal changes (absence of glands) Acinar loss Ductal")
13 Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss Ductal changes Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss Ductal changes - Reactive 13

14 Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss Ductal changes - Reactive - Open lumen - Absence of luminal debris Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss Ductal changes - Reactive - Open lumen - Absence of luminal debris - Remains within the lobule Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss Ductal changes - Reactive - Open lumen - Absence of luminal debris - Remains within the lobule 14


15 Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss Ductal changes - Reactive - Open lumen - Absence of luminal debris - Remains within the lobule - Squamous metaplasia - Intraluminal concretions Pancreatic Neck Margins Normal Pancreas Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss Ductal changes Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss Ductal changes Islets of Langerhans - Aggregation 15
 Acinar loss Ductal changes Islets of Langerhans - Aggregation - Fusion fibrosis")
 Acinar loss Ductal changes Islets of Langerhans - Aggregation - Fusion - Myxoid change -")
16 Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss Ductal changes Islets of Langerhans - Aggregation - Fusion Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss Ductal changes Islets of Langerhans - Aggregation - Fusion - Myxoid change Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss Ductal changes Islets of Langerhans - Aggregation - Fusion - Myxoid change - Pseudoglandular appearance 16



17 Pancreatic Neck Margins Chronic Pancreatitis Normal Pancreas Chronic Pancreatitis Variable lobules Interlobular fibrosis (absence of glands) Acinar loss Ductal changes Islets of Langerhans - Aggregation - Fusion - Myxoid change - Pseudoglandular appearance - Persistence of reticular architecture 17


18 Glands in interlobular septa Glands in interlobular septa FFPE Glands in interlobular septa 18


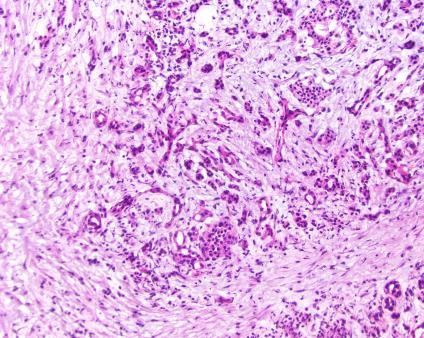
19 Glands in interlobular septa Growth near muscular vessels Glands in interlobular septa Growth near muscular vessels Growth near nerves Glands in interlobular septa Growth near muscular vessels Growth near nerves 19

20 Glands in interlobular septa Growth near muscular vessels Growth near nerves Lymphovascular and perineural invasion Glands in interlobular septa Growth near muscular vessels Growth near nerves Lymphovascular and perineural invasion FFPE Glands in interlobular septa Growth near muscular vessels Growth near nerves Lymphovascular and perineural invasion 20


21 Glands in interlobular septa Growth near muscular vessels Growth near nerves Lymphovascular and perineural invasion FFPE Glands in interlobular septa Growth near muscular vessels Growth near nerves Perineural invasion Glands in interlobular septa Growth near muscular vessels Growth near nerves Lymphovascular and perineural invasion Luminal necrosis or debris 21

22 Glands in interlobular septa Growth near muscular vessels Growth near nerves Lymphovascular and perineural invasion Luminal necrosis or debris Incomplete glands Glands in interlobular septa Growth near muscular vessels Growth near nerves Lymphovascular and perineural invasion Luminal necrosis or debris Incomplete glands 4:1 nuclear variability Glands in interlobular septa Growth near muscular vessels Growth near nerves Lymphovascular and perineural invasion Luminal necrosis or debris Incomplete glands 4:1 nuclear variability 22


23 Glands in interlobular septa Growth near muscular vessels Growth near nerves Lymphovascular and perineural invasion Luminal necrosis or debris Incomplete glands 4:1 nuclear variability Glands in interlobular septa Growth near muscular vessels Growth near nerves Lymphovascular and perineural invasion Luminal necrosis or debris Incomplete glands 4:1 nuclear variability FFPE Normal Bile Duct Bile Duct Margins - Normal 23

 Cauterization Drying")

24 Bile Duct Margins - Artifact Tissue folding Over staining (hematoxylin) Over staining (eosin) Cauterization Drying Thick sections Air bubbles Bile Duct Margins - Normal Bile Duct Margins - Normal 24


25 Bile Duct Margins - Adenocarcinoma Perineural invasion Perineural invasion Bile Duct Margins - Adenocarcinoma Perineural invasion Involvement of periductular soft tissue Bile Duct Margins - Adenocarcinoma 25


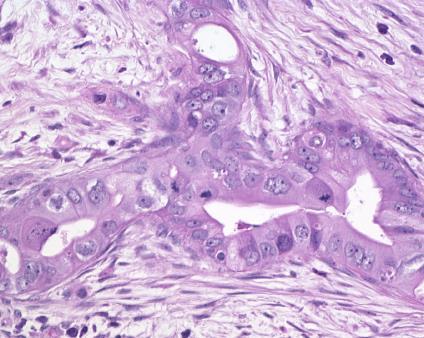
26 Proximal Duodenal Resection Margins - Normal Proximal Duodenal Resection Margins - Adenocarcinoma Lymphovascular invasion Proper appreciation of normal anatomy, histology and non-neoplastic pathology Features supporting a diagnosis of adenocarcinoma - pattern - Glands within interlobular septa - Growth of glands near muscular vessels and nerves - Lymphovascular and perineural invasion - Incomplete glands - Necrotic glandular debris - Nuclear variation, 4:1 26
 at the pancreatic neck margin")

 Pancreatic")
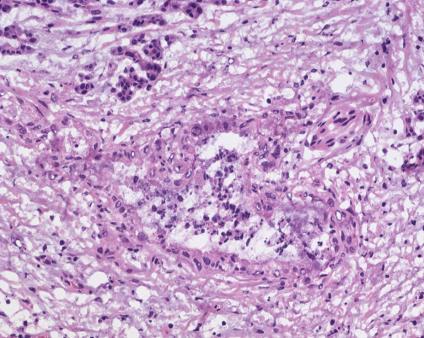
27 Challenging Issues The presence of pancreatic intraepithelial neoplasia (PanIN) and intraductal papillary mucinous neoplasms (IPMN) at the pancreatic neck margin Dysplasia at the bile duct margin Acellular mucin present within the pancreatic parenchymal margin Adenocarcinoma within a lymph node at a margin Lymphovascular or perineural invasion within the peripancreatic soft tissue at the pancreatic neck margin Incidentalomas Pancreatic Intraepithelial Neoplasia (PanIN) Pancreatic Intraepithelial Neoplasia (PanIN) 27
 Neoplasia")
 28")
28 Pancreatic Intraepithelial Neoplasia (PanIN) Pancreatic Intraepithelial Neoplasia (PanIN) Intraductal Papillary Mucinous Neoplasm (IPMN) 28

 29")

29 Intraductal Papillary Mucinous Neoplasm (IPMN) Intraductal Papillary Mucinous Neoplasm (IPMN) Intraductal Papillary Mucinous Neoplasm (IPMN) 29



30 Intraductal Papillary Mucinous Neoplasm (IPMN) Intraductal Papillary Mucinous Neoplasm (IPMN) Biliary Dysplasia at the Bile Duct Margin 30


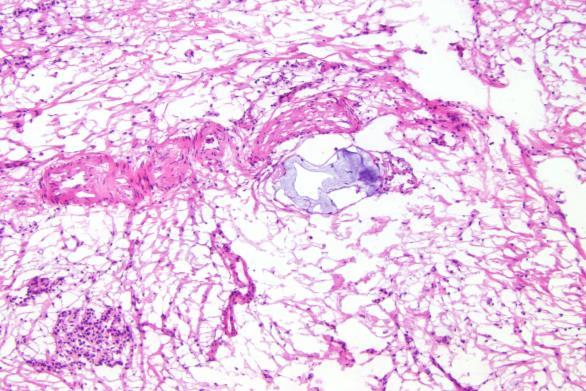
31 Biliary Dysplasia at the Bile Duct Margin Biliary Dysplasia at the Bile Duct Margin Frozen FFPE The Presence of Acellular Mucin 31


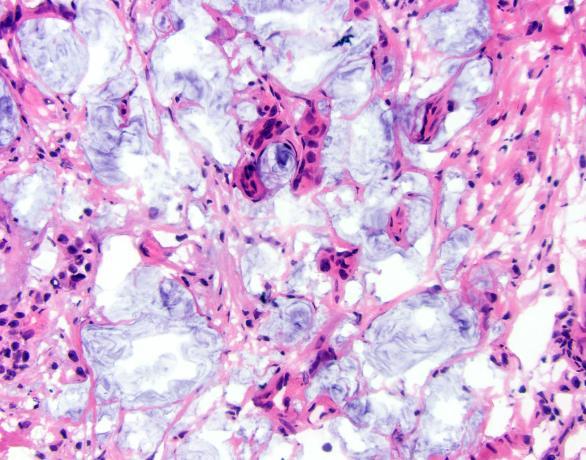
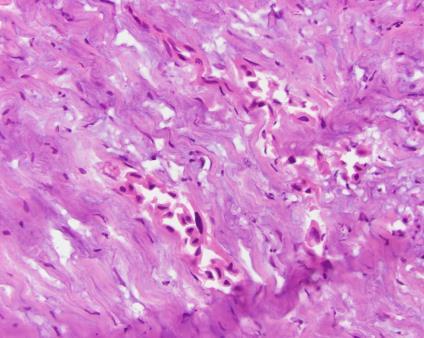
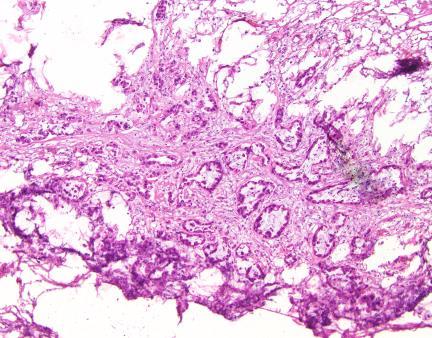
32 The Presence of Acellular Mucin The Presence of Acellular Mucin Colloid Carcinoma The Presence of Acellular Mucin Colloid Carcinoma 32

33 The Presence of Acellular Mucin Neoadjuvant Chemotherapy FFPE The Presence of Acellular Mucin Neoadjuvant Chemotherapy FFPE Adenocarcinoma within a Lymph Node at a Margin 33


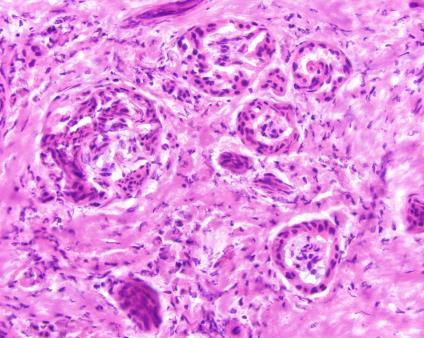
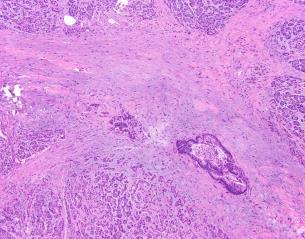
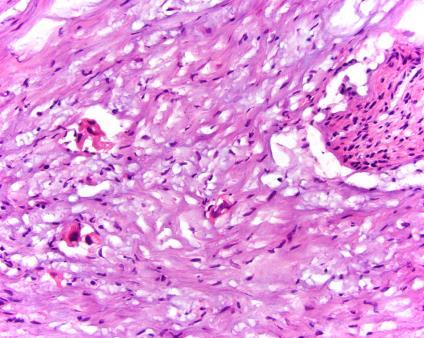
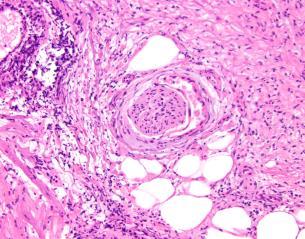
34 Adenocarcinoma within a Lymph Node at a Margin Intraneural or Perineural Invasion within the Peripancreatic Soft Tissue Intraneural or Perineural Invasion within the Peripancreatic Soft Tissue 34



35 Intraneural or Perineural Invasion within the Peripancreatic Soft Tissue Frozen FFPE Incidental Lesions Incidental Lesions 35
36 Objectives Briefly give an overview or perspective of pancreatic cancer. Review the appropriate margins to be taken for frozen section from pancreatobiliary specimens. Examine the histopathology of pancreatobiliary margins on frozen section. Discuss some of the difficulties ( gray areas ) in assessing pancreatobiliary margins. Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu 36
Objectives. Intraoperative Consultation of the Whipple Resection Specimen. Pancreas Anatomy. Pancreatic ductal carcinoma 11/10/2014
 Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD
 CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas.
 Protocol applies to all carcinomas of the exocrine pancreas.") Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines
 Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreatic Cancer: The ABCs of the AJCC and WHO
 Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget
 Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
Pancreatico-biliary cytology: a practical approach to diagnosis. Corina Cotoi
 Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Pancreatic intraepithelial
 Pancreatic intraepithelial neoplasia (PanIN) Markéta Hermanová St. Anne s University Hospital Brno Faculty of Medicine, Masaryk University Precursor lesions of invasive pancreatic cancer Pancreatic intraepithelial
Pancreatic intraepithelial neoplasia (PanIN) Markéta Hermanová St. Anne s University Hospital Brno Faculty of Medicine, Masaryk University Precursor lesions of invasive pancreatic cancer Pancreatic intraepithelial
p53 expression in invasive pancreatic adenocarcinoma and precursor lesions
 Malaysian J Pathol 2011; 33(2) : 89 94 ORIGINAL ARTICLE p53 expression in invasive pancreatic adenocarcinoma and precursor lesions NORFADZILAH MY MBBCH,* Jayalakshmi PAILOOR MPath, FRCPath,* RETNESWARI
Malaysian J Pathol 2011; 33(2) : 89 94 ORIGINAL ARTICLE p53 expression in invasive pancreatic adenocarcinoma and precursor lesions NORFADZILAH MY MBBCH,* Jayalakshmi PAILOOR MPath, FRCPath,* RETNESWARI
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues
- Test slide, Breast cancer tissues with corresponding normal tissues") A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
A 60-year old Man with Left Jaw Mass. Simon Chiosea, MD University of Pittsburgh medical Center 3/15/2016
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
S1.04 Principal clinician. G1.01 Comments. G2.01 *Specimen dimensions (prostate) S2.02 *Seminal vesicles
 S2.02 *Seminal vesicles") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies. Agenda
 Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017
 Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Case 1. Case 1: EUS Report 5/1/2017. Interesting Cases of Pancreatic Masses
 Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Adenocarcinoma of the pancreas
 Adenocarcinoma of the pancreas SEMINARS IN DIAGNOSTIC PATHOLOGY 31 (2014) 443 451 Ralph H.Hruban, MD, David S. Klimstra, MD Paola Parente Anatomia Patologica Casa Sollievo della Sofferenza San Giovanni
Adenocarcinoma of the pancreas SEMINARS IN DIAGNOSTIC PATHOLOGY 31 (2014) 443 451 Ralph H.Hruban, MD, David S. Klimstra, MD Paola Parente Anatomia Patologica Casa Sollievo della Sofferenza San Giovanni
7th Annual Symposium on Gastrointestinal Cancers " St. Louis, Mo, 9/20/08
 Molecular markers to aid in early diagnosis of pancreatic cancer Michael Goggins, MD Professor of Pathology, Medicine and Oncology Johns Hopkins Medical Institutions, Baltimore, MD 7th Annual Symposium
Molecular markers to aid in early diagnosis of pancreatic cancer Michael Goggins, MD Professor of Pathology, Medicine and Oncology Johns Hopkins Medical Institutions, Baltimore, MD 7th Annual Symposium
The pathology of pancreas
 5. Practice The pathology of pancreas 2017/2018. 2nd semester MACROSCOPY- MICROSCOPY THE STRUCTURE OF PANCREAS Exocrine: 80-85% Enzymes in the zymogenic granules of acinar cells: trypsin, chymotrypsin,
5. Practice The pathology of pancreas 2017/2018. 2nd semester MACROSCOPY- MICROSCOPY THE STRUCTURE OF PANCREAS Exocrine: 80-85% Enzymes in the zymogenic granules of acinar cells: trypsin, chymotrypsin,
Contemporary Imaging of Biliary Malignancy and Preoperative Evaluation
 Contemporary Imaging of Biliary Malignancy and Preoperative Evaluation Linda Pantongrag-Brown, MD Advanced Diagnostic Imaging, Ramathibodi Hospital, Bangkok, Thailand Malignancy of biliary tract Cholangiocarcinoma
Contemporary Imaging of Biliary Malignancy and Preoperative Evaluation Linda Pantongrag-Brown, MD Advanced Diagnostic Imaging, Ramathibodi Hospital, Bangkok, Thailand Malignancy of biliary tract Cholangiocarcinoma
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012
 Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
Protocol for the Examination of Specimens From Patients With Carcinoma of the Pancreas
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Pancreas Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For
Protocol for the Examination of Specimens From Patients With Carcinoma of the Pancreas Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For
3/28/2017. Disclosure of Relevant Financial Relationships. GU Evening Subspecialty Case Conference. Differential Diagnosis:
 GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
A712(18)- Test slide, Breast cancer tissues with corresponding normal tissues
- Test slide, Breast cancer tissues with corresponding normal tissues") A712(18)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
A712(18)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
Dr. Heba Kalbouneh. Dr. Heba Kalbouneh. Dr. Heba Kalbouneh
 Dr. Heba Kalbouneh Dr. Heba Kalbouneh Dr. Heba Kalbouneh Basement membrane: What is the basement membrane? - It is a layer of ECM separating the epithelial cells from the underlying connective tissue Basement
Dr. Heba Kalbouneh Dr. Heba Kalbouneh Dr. Heba Kalbouneh Basement membrane: What is the basement membrane? - It is a layer of ECM separating the epithelial cells from the underlying connective tissue Basement
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
ICD-O-3 UPDATES - PENDING
 ICD-O-3 UPDATES - PENDING FCDS Annual Meeting July 26, 2013 Sunrise, Florida Steven Peace, CTR ICD-O-3 Work Group ICD-O-3 WORK GROUP Name April Fritz, CTR Lynn Ries, MS Lois Dickie, CTR Linda Mulvihill,
ICD-O-3 UPDATES - PENDING FCDS Annual Meeting July 26, 2013 Sunrise, Florida Steven Peace, CTR ICD-O-3 Work Group ICD-O-3 WORK GROUP Name April Fritz, CTR Lynn Ries, MS Lois Dickie, CTR Linda Mulvihill,
ICD-O-3 UPDATES - PENDING
 ICD-O-3 UPDATES - PENDING FCDS Annual Meeting July 26, 2013 Sunrise, Florida Steven Peace, CTR ICD-O-3 Work Group ICD-O-3 WORK GROUP Name April Fritz, CTR Lynn Ries, MS Lois Dickie, CTR Linda Mulvihill,
ICD-O-3 UPDATES - PENDING FCDS Annual Meeting July 26, 2013 Sunrise, Florida Steven Peace, CTR ICD-O-3 Work Group ICD-O-3 WORK GROUP Name April Fritz, CTR Lynn Ries, MS Lois Dickie, CTR Linda Mulvihill,
DIAGNOSTIC CHALLENGES Pancreas FNAB. Dr. M. Weir Oct 2017
 DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
Intraductal papillary neoplasms in the bile ducts
 Intraductal papillary neoplasms in the bile ducts Seok Hwa Youn Myunghee Yoon Dong Hoon Shin Kosin University Gospel Hospital Department of general surgery Hepato-biliary-pancreatic division Introduction
Intraductal papillary neoplasms in the bile ducts Seok Hwa Youn Myunghee Yoon Dong Hoon Shin Kosin University Gospel Hospital Department of general surgery Hepato-biliary-pancreatic division Introduction
Patient History. A 58 year old man presents with a 16 mm cyst in the pancreatic tail. The cyst is unilocular with a thick wall and no mural nodule.
 Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
(formalin fixed) 6 non-neoplastic spots (6 spots) Corresponding normal tissues with cancers: Yes Diameter: 1. 0 mm
 6 non-neoplastic spots (6 spots) Corresponding normal tissues with cancers: Yes Diameter: 1. 0 mm") CBA729-Test slide, Head and neck cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 6 Tissue type: Test slide, Head and neck cancer tissues No. of spots: 6 spots from each
CBA729-Test slide, Head and neck cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 6 Tissue type: Test slide, Head and neck cancer tissues No. of spots: 6 spots from each
NEOPLASIA-I CANCER. Nam Deuk Kim, Ph.D.
 NEOPLASIA-I CANCER Nam Deuk Kim, Ph.D. 1 2 Tumor in the hieroglyphics of the Edwin Smith papyrus (1,600 B.C., Breasted s translation 1930) 3 War on Cancer (National Cancer Act, 1971) 4 Cancer Acts in Korea
NEOPLASIA-I CANCER Nam Deuk Kim, Ph.D. 1 2 Tumor in the hieroglyphics of the Edwin Smith papyrus (1,600 B.C., Breasted s translation 1930) 3 War on Cancer (National Cancer Act, 1971) 4 Cancer Acts in Korea
Cholangiocarcinoma. Judy Wyatt Dundee November 2010
 Cholangiocarcinoma Judy Wyatt Dundee November 2010 Making sense of cholangiocarcinoma Difficulties with diagnostic criteria How many entities within cholangiocarcinoma? Rapidly evolving Intrahepatic cholangiocarcinoma
Cholangiocarcinoma Judy Wyatt Dundee November 2010 Making sense of cholangiocarcinoma Difficulties with diagnostic criteria How many entities within cholangiocarcinoma? Rapidly evolving Intrahepatic cholangiocarcinoma
3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours
 60 3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours Compilation and editing and of this volume: Prof. Chandu de Silva (Consultant Histopathologist) List of contributors Consultant
60 3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours Compilation and editing and of this volume: Prof. Chandu de Silva (Consultant Histopathologist) List of contributors Consultant
Icd 10 pancreatic mass
 Icd 10 pancreatic mass 24-2-2018 islet cell tumor (of pancreas ) ( ICD - 10 -CM Diagnosis Code D13.7.. ICD - 10 - CM Diagnosis Code K90.3. Pancreatic steatorrhea. 2016 2017 2018 Billable. Abdominal wall
Icd 10 pancreatic mass 24-2-2018 islet cell tumor (of pancreas ) ( ICD - 10 -CM Diagnosis Code D13.7.. ICD - 10 - CM Diagnosis Code K90.3. Pancreatic steatorrhea. 2016 2017 2018 Billable. Abdominal wall
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
Bladder Case 1 SURGICAL PATHOLOGY REPORT. Procedure: Cystoscopy, transurethral resection of bladder tumor (TURBT)
") Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Video Microscopy Tutorial 19
 Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Overview. Disclosure. PRE INVASIVE NEOPLASIA OF BILIARY TREE New Perspectives on Old Themes. N. Volkan Adsay, MD
 PRE INVASIVE NEOPLASIA OF BILIARY TREE New Perspectives on Old Themes N. Volkan Adsay, MD Professor and Vice-Chair Director of Anatomic Pathology Emory University and Emory Winship Cancer Institute Atlanta,
PRE INVASIVE NEOPLASIA OF BILIARY TREE New Perspectives on Old Themes N. Volkan Adsay, MD Professor and Vice-Chair Director of Anatomic Pathology Emory University and Emory Winship Cancer Institute Atlanta,
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node
 Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
O Farrell Legacy UPDATE ON WHO NOMENCLATURE. World Health Organization, 2010 DISCLOSURES WITH EMPHASIS ON PROBLEM HEPATOCELLULAR TUMORS
 O Farrell Legacy UPDATE ON WHO NOMENCLATURE WITH EMPHASIS ON PROBLEM HEPATOCELLULAR TUMORS Linda Ferrell, MD University of California San Francisco Vice Chair, Director of Surgical Pathology World Health
O Farrell Legacy UPDATE ON WHO NOMENCLATURE WITH EMPHASIS ON PROBLEM HEPATOCELLULAR TUMORS Linda Ferrell, MD University of California San Francisco Vice Chair, Director of Surgical Pathology World Health
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
CLINICAL SIGNIFICANCE OF BENIGN EPITHELIAL CHANGES
 Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Protocol for the Examination of Specimens from Patients With Carcinoma of the Distal Extrahepatic Bile Ducts
 Protocol for the Examination of Specimens from Patients With Carcinoma of the Distal Extrahepatic Bile Ducts Version: DistalExtrahepaticBileDucts 4.0.0.1 Protocol Posting Date: June 2017 Includes ptnm
Protocol for the Examination of Specimens from Patients With Carcinoma of the Distal Extrahepatic Bile Ducts Version: DistalExtrahepaticBileDucts 4.0.0.1 Protocol Posting Date: June 2017 Includes ptnm
Biliary Tract Neoplasia: A Cyto-histologic Review. Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital
 Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
Management A Guideline Based Approach to the Incidental Pancreatic Cysts. Common Cystic Pancreatic Neoplasms.
 Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Intro to Gallbladder & Pancreas Pathology
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
Standardization of Nomenclature
 Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Index (SIRS), 158, 173
, 158, 173") Index A Acute pancreatitis surgery abdominal compartment syndrome, 188 adjuvant treatment, 194 anterior approach, 175 antibiotic prophylaxis, 166 167, 197 Atlanta classification, 181 classification of
Index A Acute pancreatitis surgery abdominal compartment syndrome, 188 adjuvant treatment, 194 anterior approach, 175 antibiotic prophylaxis, 166 167, 197 Atlanta classification, 181 classification of
Measure Specifications Measure Description
 CMS ID/CMS QCDR ID: CAP 25 Title: Time for Pancreas Specifications Description Percentage of all eligible pancreatic exocrine carcinoma (including small cell and large cell (poorly differentiated) neuroendocrine
CMS ID/CMS QCDR ID: CAP 25 Title: Time for Pancreas Specifications Description Percentage of all eligible pancreatic exocrine carcinoma (including small cell and large cell (poorly differentiated) neuroendocrine
A Minute Pancreatic Ductal Adenocarcinoma with Lipomatous Pseudohypertrophy of the Pancreas
 CASE REPORT A Minute Pancreatic Ductal Adenocarcinoma with Lipomatous Pseudohypertrophy of the Pancreas Sadanobu Izumi 1, Satoko Nakamura 2, Masaki Tokumo 1, Shohei Mano 2 Departments of 1 Surgery and
CASE REPORT A Minute Pancreatic Ductal Adenocarcinoma with Lipomatous Pseudohypertrophy of the Pancreas Sadanobu Izumi 1, Satoko Nakamura 2, Masaki Tokumo 1, Shohei Mano 2 Departments of 1 Surgery and
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
An investigation of pancreatic volume by disease using pancreatic volumetry
 Yamagata Med J (ISSN 0288-030X)2015;33(2):71-76 DOI 10.15022/00003469 An investigation of pancreatic volume by disease using pancreatic volumetry Tsuyoshi Fukumoto, Toshihiro Watanabe, Koji Tezuka, Akiko
Yamagata Med J (ISSN 0288-030X)2015;33(2):71-76 DOI 10.15022/00003469 An investigation of pancreatic volume by disease using pancreatic volumetry Tsuyoshi Fukumoto, Toshihiro Watanabe, Koji Tezuka, Akiko
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
PLEOMORPHIC ADENOMA ( BENIGN MIXED TUMOR )
") ( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
Cystic Pancreatic Lesions: Approach to Diagnosis
 Cystic Pancreatic Lesions: Approach to Diagnosis Poster No.: R-0130 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: A. AGARWAL, R. M. Mendelson; Perth/AU Keywords: Cysts, Biopsy, Endoscopy,
Cystic Pancreatic Lesions: Approach to Diagnosis Poster No.: R-0130 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: A. AGARWAL, R. M. Mendelson; Perth/AU Keywords: Cysts, Biopsy, Endoscopy,
PAPER. Experience With 208 Resections for Intraductal Papillary Mucinous Neoplasm of the Pancreas
 PAPER Experience With 0 Resections for Intraductal Papillary Mucinous Neoplasm of the Pancreas Thomas Schnelldorfer, MD; Michael G. Sarr, MD; David M. Nagorney, MD; Lizhi Zhang, MD; Thomas C. Smyrk, MD;
PAPER Experience With 0 Resections for Intraductal Papillary Mucinous Neoplasm of the Pancreas Thomas Schnelldorfer, MD; Michael G. Sarr, MD; David M. Nagorney, MD; Lizhi Zhang, MD; Thomas C. Smyrk, MD;
They Do Look Alike : Mimics of Prostate Cancer in Biopsy Samples
 They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
Intro to Gallbladder & Pancreas Pathology
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis i acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Dept. of Pathology
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis i acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Dept. of Pathology
Matthew McCollough, M.D. April 9, 2009 University of Louisville
 Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT
 CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
Triple Negative Breast Cancer
 Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Other Sites. Table 2 Continued. MPH Rules 11/8/07. NAACCR Webinar Series 1
 MPH s 11/8/07 Other s 1 Table 2 Continued Use this two-page table to select combination histology codes. Compare the terms in the diagnosis to the terms in Columns 1 and 2. If the terms match, code the
MPH s 11/8/07 Other s 1 Table 2 Continued Use this two-page table to select combination histology codes. Compare the terms in the diagnosis to the terms in Columns 1 and 2. If the terms match, code the
Anatomy of the liver and pancreas
 Anatomy of the liver and pancreas Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk abdulameerh@yahoo.com Liver Aorta Pulm. Trunk Rt. At, Duct. Art. Lt. Ven. Rt. Ven. Internal Posterior
Anatomy of the liver and pancreas Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk abdulameerh@yahoo.com Liver Aorta Pulm. Trunk Rt. At, Duct. Art. Lt. Ven. Rt. Ven. Internal Posterior
Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes
 Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes Evan A. Alston, MD 1 ; Sejong Bae, PhD 2 ; and Isam A. Eltoum, MD, MBA 1 BACKGROUND:
Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes Evan A. Alston, MD 1 ; Sejong Bae, PhD 2 ; and Isam A. Eltoum, MD, MBA 1 BACKGROUND:
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Section 8 Liver and Gallbladder
 General and Systemic Histopathology C601 and C602 Section 8 As we will see in this unit, the liver is subject to many types of injury. Additionally, many systemic diseases have a liver component and sometimes
General and Systemic Histopathology C601 and C602 Section 8 As we will see in this unit, the liver is subject to many types of injury. Additionally, many systemic diseases have a liver component and sometimes
VULVAR CARCINOMA. Page 1 of 5
 VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Outline. Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines
 Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines") Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification
Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification
Three Cases of Concomitant Intraductal Papillary Mucinous Neoplasm and Pancreatic Neuroendocrine Tumour
 CASE SERIES Three Cases of Concomitant Intraductal Papillary Mucinous Neoplasm and Pancreatic Neuroendocrine Tumour Nilanjana Tewari 1, Abed M Zaitoun 2, Daniel Lindsay 2, Areeg Abbas 2, Mohammad Ilyas
CASE SERIES Three Cases of Concomitant Intraductal Papillary Mucinous Neoplasm and Pancreatic Neuroendocrine Tumour Nilanjana Tewari 1, Abed M Zaitoun 2, Daniel Lindsay 2, Areeg Abbas 2, Mohammad Ilyas
Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors
 AJCP / REPORTING RECOMMENDATIONS FOR PANCREATIC SPECIMENS CONTAINING MALIGNANT TUMORS Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors Jorge AlboresSaavedra, David
AJCP / REPORTING RECOMMENDATIONS FOR PANCREATIC SPECIMENS CONTAINING MALIGNANT TUMORS Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors Jorge AlboresSaavedra, David
Genetics of Pancreatic Cancer. October 6, If you experience technical difficulty during the presentation:
 Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Breast Pathology. Breast Development
 Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment
 Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment Andrew W. Bowman, MD PhD Assistant Professor of Radiology Mayo Clinic Florida SCBT-MR Annual Meeting Nashville,
Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment Andrew W. Bowman, MD PhD Assistant Professor of Radiology Mayo Clinic Florida SCBT-MR Annual Meeting Nashville,
Pancreas & Biliary System. Dr. Vohra & Dr. Jamila
 Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist