Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines. John Potter Professor Ageing & Stroke Medicine University of East Anglia
|
|
|
- Amie Copeland
- 5 years ago
- Views:
Transcription
1 Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia

2 Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines People operate with beliefs and biases. To the extent you can eliminate both and replace them with data, you gain a clear advantage. - Michael Lewis, Moneyball: The Art of Winning an Unfair Game Human nature being what it is, we tend to say we are following Guidelines when in reality we re not - Rita Marker

3 Leading Causes of Death by Age and Cause UK years years 85+ years All Ages

4 Deaths/year/ 100,000 Deaths/year/ 100,000 Deaths/year/ 100,000 Deaths/year/ 100,000 UK Deaths from CVD Years 70+Years 2010 Deaths Male 29% 43% < % < Deaths Male 33% 46% < % <1955 Female 18% 45%< % <1955 Female 28% 48%< % <1955 UK Deaths from Stroke Deaths Male 4% 42% < % < Deaths Male 7% 44% < % <1955 Female 4% 44%< % <1955 Female 8% 44%< % <1955
5
6 Incidence 1000 patient years Prevalence 1000 patient years Changes in UK Stroke Incidence & Prevalence Incidence Prevalence Men 2.4% Women 2.2% Lee BMJ 2011
7 Primary CVD Prevention - GP Research Database BHS 3 QOF JBS2 Lee BMJ 2011
8 Stroke Primary Prevention The Untreatables - Age, Sex, Ethnicity, low Birthweight, Migraine, Genetic The Unattainables Lifestyle Mods - Obesity, Diet, Exercise, Smoking, Alcohol Medications - Oral contraceptive/hrt, Drugs, Infections - CMV Surgical - Asymptomatic Carotid Stenosis, IC Aneurysm screening
9 What s new in the Guidelines for Hypertension Management? Criteria for the measurement (Office, Home or Ambulatory) and diagnosis of hypertension What levels to start treatment especially the Old Old and those with TOD New Anti-hypertensive treatment regimens
10 The evidence that Diagnosis or Treatment changes based on ABPM v Office values improves BP control or Outcomes for Young or Old?

11 Masked Hypertension? Stage 1 CBP /90-99 ABPM 135/85 Stage 2 CBP / ABPM 150/95 Use Daytime ABPM (or Self BPM over 1 week) for Diagnosis Potential not to treat ABPM levels up to 149/94 mmhg
12 JBS3/NICE / BHS Threshold & Treatment BP Levels for Hypertension by Different Methods of Measurement Setting Clinic BP (>80 yrs) Aims! Diabetes/Stroke (JBS3 2014) SBP mmhg > 140 (160) 140 and/or DBP mmhg > 90 (100) 90 Target SBP mmhg <140 (<150) <140 (130) Target DBP mmhg <90 (<90) <90 (80) Home/Self (>80 yrs) Diabetes/Stroke (JBS3 2014) > 135 > 85 <135 (<150) 125 < 85 (<85) 75 Daytime ABPM (>80 yrs) BHS 2004 Diabetes/Stroke (JBS3 2014) > 135 (150) (>130) >85 (95) (>85) <135 (<145) < <85 (<85) < hour ABPM (JBS32014) Night >125 >120 >80 >75 Values in parenthesis for 80+ age group
 for older HT s as BP")
13 First and Second line Treatment changes The Shrinking Alphabet? Removal since 2004 Guidelines Diuretic - Thiazide changed to Non-Thiazide Plus Lifestyle changes NICE - 1 st line agent CCB (not Diuretic) for older HT s as BP variability, Diabetes, Cost effectiveness & better outcome combined with ACEI (Contrast to AHA 2013!)
14 The important recent changes in Hypertension Management Use of ABPM (SBPM) for Diagnosis of HT Stage 1 - Start drug treatment dependent on CV Risk level (?20% over 10 years) or presence of CVD/Diabetes Stage 2 Start drug treatment Target BP same for those with TOD and no TOD, office BP<140/90 mmhg, 80+ age group <150/90 mmhg Offer 80+age group same treatment as those years CCB as 1 st line agent in 55+ age group If Diuretic added use low-dose Thiazide-like e.g. Chlortalidone, Indapamide not Thiazide Single pill combinations preferred
15 What s new in the Guidelines for Lipid Management? Changes from previous Guidelines? Treat at 20% CV risk. Which lipid fractions best predict risk ie Total Cholesterol & Non-HDL-c (TC HDL-c) v LDL-c v Apo s. What levels to start treatment and benefits, especially the Old Old and those with TOD. What to use and what dose? Treatment Goals Treat to Target, Lower the Better, Give and Forget?
 - Statins for Primary Prevention if 10 year CV risk 10% for those aged 40-74 (85+) years (No target TC/HDL, was<4/2 mmol/l) AHA (2013) - Primary Prevention if 10 year CV risk 7.")
16 Lipid Management - What do we/others do now? NICE (2014) - Statins for Primary Prevention if 10 year CV risk 10% for those aged (85+) years (No target TC/HDL, was<4/2 mmol/l) AHA (2013) - Primary Prevention if 10 year CV risk 7.5% for those aged years or LDL-C >4.9 mmol/l LDL-C 4.9 mmol/l 4.9 mmol/l.9 mmol/l High Intensity Statins eg Atorvastatin 80 mg 50% LDL Moderate Intensity Statins eg Atorvastatin 20 mg = 30-50% LDL Target No Recommendations LDL-C mmol/l?
17 Lipid Management JBS3 (NICE) All 40+ should have lipids checked, no upper age limit set (individualise >75 years, 85 +) Use non-fasting samples for TC & HDL-C (Non-HDL-C will replace LDL-C), treatment benefits from LDL <2mmol/l Lifestyle support Cholesterol lowering drugs (Statins) for: High 10 year risk (NICE to decide level, level) High lifetime risk (to include younger people), upper age limit? High risk conditions eg Diabetes, CKD stage 3-5, FH +ve Established CVD Primary Prevention - Atorvastatin 20mg Secondary Prevention - Atorvastatin 80mg?Targets (40% reduction Non-HDL-C or <2.5 mmol/l LDL-C <1.8 mmol/l)
18 Statins in 1 o Prevention Statins Compared to Control/Placebo: Stroke 22% (NNT for 5 years 155) but small increase in Cerebral Haemorrhage Fatal/Non-Fatal CHD 27% (NNT 88) Total CVD Events 25% (NNT 49) All deaths 14% (NNT 138) Type 2 Diabetes 18% (NNH 99) Other potential benefits - Dementia & MCI (26%) Adverse events overall No difference including Cancer risk
19 What s new in the Guidelines for Anti-platelet and Anti-coagulant therapy?
20 Aspirin in Primary Prevention BHS 4 (2004). primary prevention in people with hypertension over the age of 50 years who have a 10-year CVD risk 20% and in whom BP is controlled to the audit standard (A). JBS2 (2005) -. evidence supports daily doses of aspirin in the range of mg for the long term prevention of serious vascular events in high risk people.. Benefits - Outcome Odds Ratio (95% CI) 1 0 Prevention Trials (5) All CHD Events 0.72 ( ) CHD death 0.87 ( ) Total stroke 1.02 ( ) All-cause mortality 0.93 ( ) Harms Haemorrhagic stroke 1.4 ( ) Major gastrointestinal bleeding event 1.7 ( ) Outcome Estimated 10-Year Risk for 1000 treated patients CHD Events at Baseline 2% 6% 10% Effect on all-cause mortality No change No change No change CHD events avoided, n 3 (1 4) 8 (4 12) 14 (6 20) Ischaemic strokes avoided, n Haemorrhagic strokes precipitated, n 1 (0 2) 1 (0 2) 1 (0 2) Major gastrointestinal bleeding events n 3 (2 4) 3 (2 4) 3 (2 4)
21 Aspirin and Primary Prevention Risks v Benefits Old Studies Prior Stroke/TIA 2000 n = 100,000 F/U 6 years 4000 events Meta-Analysis Odds Ratio Major CV Events 0.87 ( ) Major CHD events 0.85 ( ) Any Stroke 0.92 ( ) Vascular Death 0.96 ( ) Any Death 0.93 ( )
22 Aspirin and Primary Prevention Benefits v Risks Cancers years >5 Major Vascular Events years >5 Major Extracranial Bleeds years >5 GI Bleeding Risk NNH = Number Needed to Harm Odds Ratio Major Bleed 1.6 ( ) with low dose Aspirin Men Moderate CV risk Benefit 1-3/1000/yr v 1-2/1000/yr Major Bleeds Benefit of Aspirin v Other Measures? NO Aspirin in Primary Prevention
23 New Anticoagulants v Warfarin for Event/Risk Factor Stroke/Systemic Embolic events <75 years 75 years Atrial Fibrillation RR (95% CI) 0.81 ( ) 0.85 ( ) 0.78 ( ) Cerebral Infarct (High Dose) 0.92 ( ) Cerebral Infarct (Low Dose) 1.28 ( ) PICH 0.49 ( ) Cranial Bleeding (SAH, PICH, Sub-dural etc) 0.48 ( ) All Cause Mortality 0.90 ( ) GI Bleed 1.25 ( ) Major Bleed (High Dose) 0.86 ( ) Ruff Lancet 2014
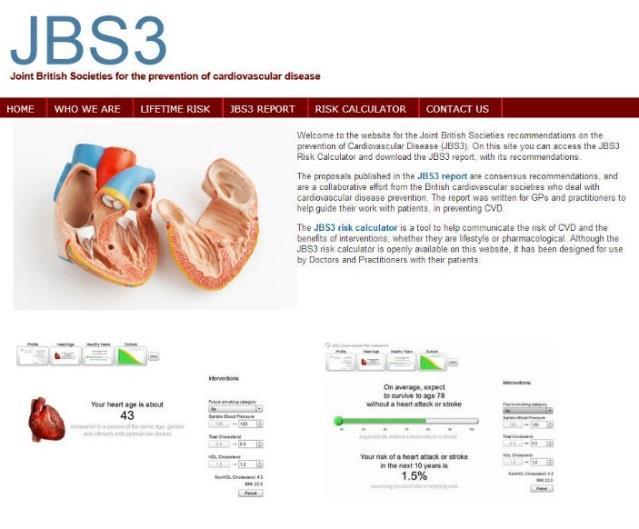
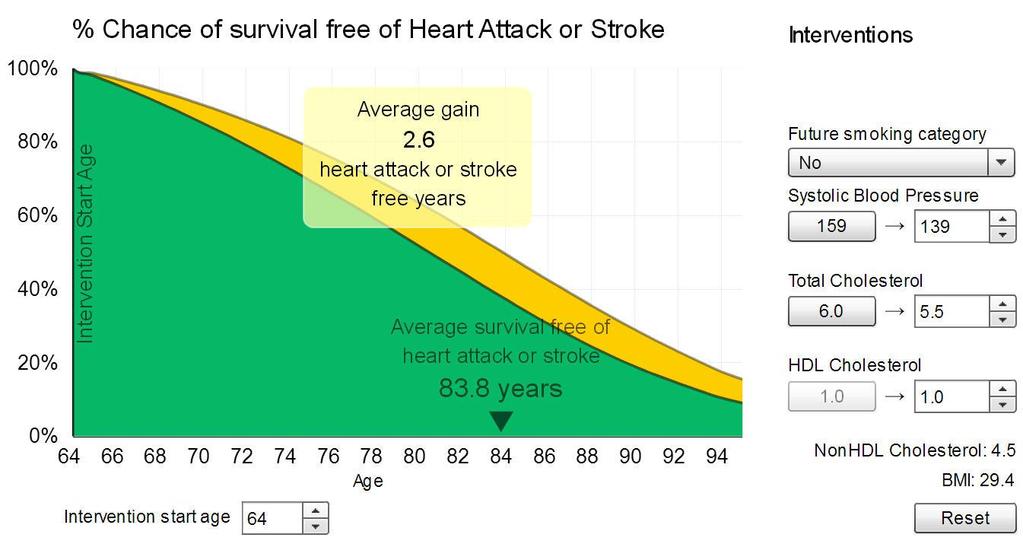
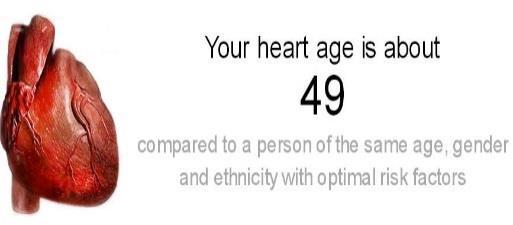
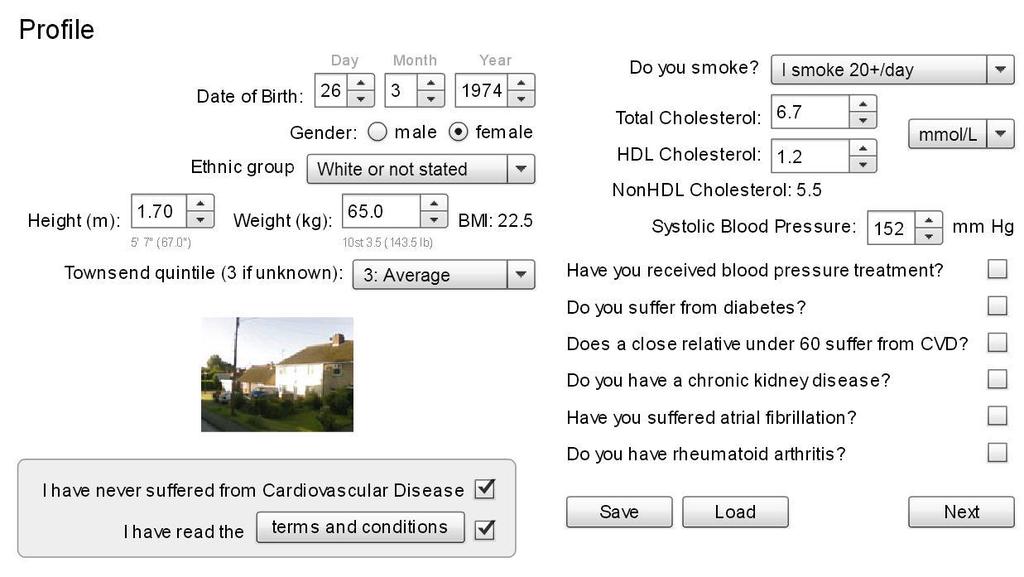
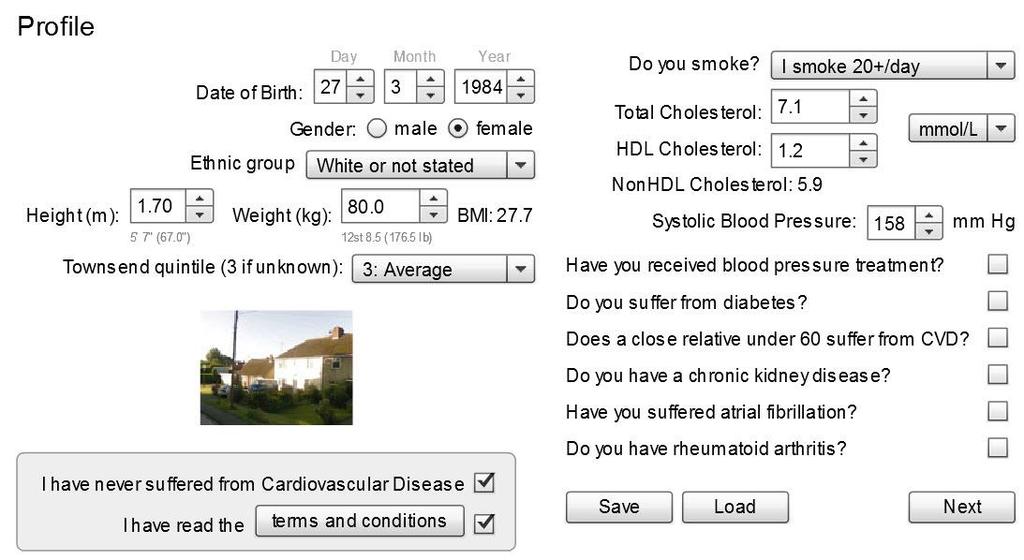
24 JBS3 Risk Calculator - 10 Year & Lifetime CV Risk Framingham based Framingham score, JBS2/BHS, New Zealand, Framingham General CV Risk Score Non-Framingham - ASSIGN, Heart Score, QRISK2, UKPDS Risks factors included- Age, Sex, BP, Lipids, Smoking? + FH, Diabetes, Rh Arthritis, LVH, Post Code, Race Only UKPDS suitable for Diabetics Most Risk Calculators only allowed 5-10 year risk assessment Good for Population Risk,? Individual Risk Prediction JBS3 Risk Calculator Intervention Assumptions BP 20mmHg reduction = 50% CVD reduction LDL-c 1 mmol/l reduction = 22% CVD reduction Smoking Weight? effect


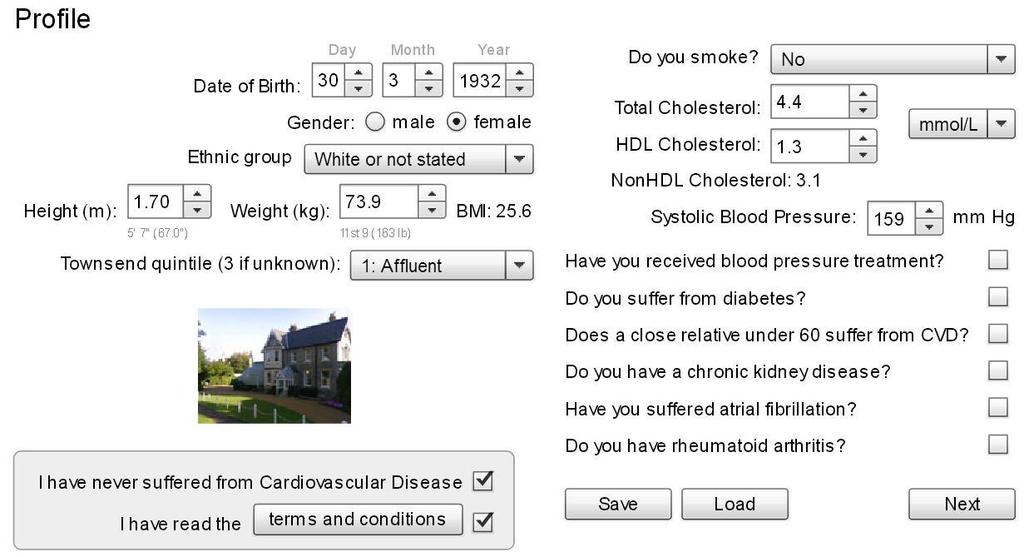
25 JBS3 Risk Calculator - 10 Year & Lifetime CV Risk
26 JBS2/BHS 26%
27
28
29

30 Not to be used in TIA patients
31 Take Home Messages Cardiovascular disease is still a major cause of morbidity and mortality in UK, prevention remains key. Many new and important Guideline based changes in CV management are being introduced. Need for intensive risk factor modification in those at high risk. Hypertension - new initiatives in diagnosis, treatment & targets. Lipids Non-fasting, LDL levels not needed, consider higher strength statins at 10% CV risk in all ages, use statins for 1 0 & 2 0 prevention, target 40% reduction. Aspirin -No for Primary prevention. Oral Anti-Coagulants - new OAC should be routinely considered. CV Risk Calculators - Differ in level of Risk assessment. JBS3 gives 10 year and Lifetime risk level. Potential different risk levels for BP and Lipid drug intervention. Guidelines are for Guidance, not a substitute for informed clinical judgement and pragmatic reasoning.
Stroke secondary prevention. Gill Cluckie Stroke Nurse Consultant St. George s Hospital
 Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Primary Prevention of Stroke
 Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
well-targeted primary prevention of cardiovascular disease: an underused high-value intervention?
 well-targeted primary prevention of cardiovascular disease: an underused high-value intervention? Rod Jackson University of Auckland, New Zealand October 2015 Lancet 1999; 353: 1547-57 Findings: Contribution
well-targeted primary prevention of cardiovascular disease: an underused high-value intervention? Rod Jackson University of Auckland, New Zealand October 2015 Lancet 1999; 353: 1547-57 Findings: Contribution
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Strokes, Falls, Forgetfulness and Frailty Managing the Very Elderly Hypertensive
 Strokes, Falls, Forgetfulness and Frailty Managing the Very Elderly Hypertensive John Potter Professor Ageing and Stroke Medicine University of East Anglia Oh God who knowest us to be set midst great dangers,
Strokes, Falls, Forgetfulness and Frailty Managing the Very Elderly Hypertensive John Potter Professor Ageing and Stroke Medicine University of East Anglia Oh God who knowest us to be set midst great dangers,
Should we base treatment decisions on short-term or lifetime CVD risk? Rod Jackson University of Auckland New Zealand
 Should we base treatment decisions on short-term or lifetime CVD risk? Rod Jackson University of Auckland New Zealand Presentation outline Strengths & weaknesses of short-term risk approach Strengths &
Should we base treatment decisions on short-term or lifetime CVD risk? Rod Jackson University of Auckland New Zealand Presentation outline Strengths & weaknesses of short-term risk approach Strengths &
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Key causes of preventable deaths in New Zealand In a population of 10,000 New Zealanders, every year there will be about:
 Preventive care - Chronic Disease Management in primary care: a population perspective Rod Jackson University of Auckland New Zealand (22/11/8) Key causes of preventable deaths in New Zealand In a population
Preventive care - Chronic Disease Management in primary care: a population perspective Rod Jackson University of Auckland New Zealand (22/11/8) Key causes of preventable deaths in New Zealand In a population
Overview. NOT A REPETION OF LOCAL GUIDELINE Dr Diviash Thakrar
 Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
Update in Cardiology Pharmacologic Management of Cardiovascular Risk. Christopher C. Roe, MSN, ACNP
 Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Best Medical Therapy for asymptomatic carotid disease
 Best Medical Therapy for asymptomatic carotid disease Richard Bulbulia Consultant Vascular Surgeon and Co-PI ACST-2 MRC Population Health Research Unit CTSU, Nuffield Department of Population Health University
Best Medical Therapy for asymptomatic carotid disease Richard Bulbulia Consultant Vascular Surgeon and Co-PI ACST-2 MRC Population Health Research Unit CTSU, Nuffield Department of Population Health University
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden
 Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Primary prevention of CVD Potential output:
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Primary prevention of CVD Potential output:
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Professor DA Fitzmaurice Primary Care Clinical Sciences University of Birmingham
 New Guidelines for SPAF Professor DA Fitzmaurice Primary Care Clinical Sciences University of Birmingham Stroke prevention and atrial fibrillation Epidemiology of atrial fibrillation How common is it?
New Guidelines for SPAF Professor DA Fitzmaurice Primary Care Clinical Sciences University of Birmingham Stroke prevention and atrial fibrillation Epidemiology of atrial fibrillation How common is it?
Understanding new international guidelines to tackle CV Risk: A practical model John Deanfield, MD UCL, London United Kingdom s
 Understanding new international guidelines to tackle CV Risk: A practical model John Deanfield, MD UCL, London United Kingdom s Ho Chi Minh City, Vietnam August 7, 2014 JBS 2 Risk Guidelines (2005) Based
Understanding new international guidelines to tackle CV Risk: A practical model John Deanfield, MD UCL, London United Kingdom s Ho Chi Minh City, Vietnam August 7, 2014 JBS 2 Risk Guidelines (2005) Based
Improve the Adherence, Save the Life
 Improve the Adherence, Save the Life Park, Chang Gyu Korea University Guro Hospital Cardiovascular Center Seoul, Korea Modifiable CVD Risk Factors Obesity BMI Hypertension Cholesterol LDL HDL Diabetes
Improve the Adherence, Save the Life Park, Chang Gyu Korea University Guro Hospital Cardiovascular Center Seoul, Korea Modifiable CVD Risk Factors Obesity BMI Hypertension Cholesterol LDL HDL Diabetes
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu Indicator area: Pulse rhythm assessment for AF Indicator: NM146 Date: June 2017 Introduction There is evidence
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu Indicator area: Pulse rhythm assessment for AF Indicator: NM146 Date: June 2017 Introduction There is evidence
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Managing Hypertension in 2018
 MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
surtout qui n est PAS à risque?
 3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center
 Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
What s the evidence, why do guidelines differ, and what should the GP do?
 What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
SESSION 3 11 AM 12:30 PM
 SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
Cardiovascular Risk Assessment and Management Making a Difference
 Cardiovascular Risk Assessment and Management Making a Difference Norman Sharpe March 2014 Numbers and age-standardised mortality rates from all causes, by sex, 1950 2010 Death rates halved Life expectancy
Cardiovascular Risk Assessment and Management Making a Difference Norman Sharpe March 2014 Numbers and age-standardised mortality rates from all causes, by sex, 1950 2010 Death rates halved Life expectancy
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
NICE BHS Hypertension guidelines 2011 update
 NICE BHS Hypertension guidelines 2011 update Review for clinicians Sept 2011 Mark Thomas West Midlands Hypertension Centre Heart of England NHS Trust www.wmhc.co.uk mark.thomas@heartofengland.nhs.uk Full
NICE BHS Hypertension guidelines 2011 update Review for clinicians Sept 2011 Mark Thomas West Midlands Hypertension Centre Heart of England NHS Trust www.wmhc.co.uk mark.thomas@heartofengland.nhs.uk Full
Reducing CVD globally through combination approaches to prevention: the polypill. Salim Yusuf
 Reducing CVD globally through combination approaches to prevention: the polypill. Salim Yusuf Disclosure None Polypill & CVD Prevention 1. Why do we need a polypill? 2. What components in the polypill?
Reducing CVD globally through combination approaches to prevention: the polypill. Salim Yusuf Disclosure None Polypill & CVD Prevention 1. Why do we need a polypill? 2. What components in the polypill?
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Four Years of NHS Health Checks in Barnsley - Outcomes and Inequalities
 Four Years of NHS Health Checks in Barnsley - Outcomes and Inequalities Summary After four years of NHS Health Checks, Barnsley has access to aggregated data on over 47,000 people. This data was analysed
Four Years of NHS Health Checks in Barnsley - Outcomes and Inequalities Summary After four years of NHS Health Checks, Barnsley has access to aggregated data on over 47,000 people. This data was analysed
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Randomized Design of ALLHAT BP Trial
 Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
CVD Risk Assessment. Michal Vrablík Charles University, Prague Czech Republic
 CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Kathryn M. Rexrode, MD, MPH. Assistant Professor. Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School
 Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
New indicators to be added to the NICE menu for the QOF and amendments to existing indicators
 New indicators to be added to the for the QOF and amendments to existing indicators 1 st September 2015 Version 1.1 This document was originally published on 3 rd August 2015, it has since been updated.
New indicators to be added to the for the QOF and amendments to existing indicators 1 st September 2015 Version 1.1 This document was originally published on 3 rd August 2015, it has since been updated.
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
SECONDARY PREVENTION OF CORONARY HEART DISEASE AND ISCHAEMIC STROKE/TIA
 PRIMARY PREVENTION OF CHD AND STROKE IN HIGH RISK PATIENTS Random non fasting test for total cholesterol, HDL cholesterol (TC:HDL ratio) and LFTs If cholesterol > 7.5 mmol/l or LDL C 5mmol/l exclude secondary
PRIMARY PREVENTION OF CHD AND STROKE IN HIGH RISK PATIENTS Random non fasting test for total cholesterol, HDL cholesterol (TC:HDL ratio) and LFTs If cholesterol > 7.5 mmol/l or LDL C 5mmol/l exclude secondary
Talking about blood pressure
 Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Review current guideline recommendations for lipid-lowering therapy
 Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
SESSION 5 2:20 3:35 PM
 SESSION 5 2:20 3:35 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
SESSION 5 2:20 3:35 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
Management of Hypertension for Stroke Prevention in New Zealand: Can We Do Better? Walter van der Merwe Nephrologist Waitemata DHB
 Management of Hypertension for Stroke Prevention in New Zealand: Can We Do Better? Walter van der Merwe Nephrologist Waitemata DHB Increasing stroke numbers in New Zealand an 'epidemic' says leading AUT
Management of Hypertension for Stroke Prevention in New Zealand: Can We Do Better? Walter van der Merwe Nephrologist Waitemata DHB Increasing stroke numbers in New Zealand an 'epidemic' says leading AUT
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Peripheral arterial disease Potential output:
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Peripheral arterial disease Potential output:
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
WPCCS May2013. Mr Ian Williams Consultant Vascular Surgeon UHW. Consultant Cardiologist UHW
 Peripheral Vascular Disease WPCCS May2013 Mr Ian Williams Consultant Vascular Surgeon UHW Prof Julian Halcox Prof Julian Halcox Consultant Cardiologist UHW Case 1? Ischaemic Legs History 85 years lady?varicose
Peripheral Vascular Disease WPCCS May2013 Mr Ian Williams Consultant Vascular Surgeon UHW Prof Julian Halcox Prof Julian Halcox Consultant Cardiologist UHW Case 1? Ischaemic Legs History 85 years lady?varicose
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
CHALLENGES OF HYPERTENSION IN THE COALFACE
 CHALLENGES OF HYPERTENSION IN THE COALFACE Y VERIAVA CENTRE FOR RURAL HEALTH SCHOOL OF CLINICAL MEDICINE FACULTY OF HEALTH SCIENCES UNIVERSITY OF WITWATERSRAND SYSTOLIC AND DIASTOLIC BLOOD PRESSURES (BP)
CHALLENGES OF HYPERTENSION IN THE COALFACE Y VERIAVA CENTRE FOR RURAL HEALTH SCHOOL OF CLINICAL MEDICINE FACULTY OF HEALTH SCIENCES UNIVERSITY OF WITWATERSRAND SYSTOLIC AND DIASTOLIC BLOOD PRESSURES (BP)
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Cardiovascular risk reduction in diabetes Lipids (NICE CG181)
") Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors
Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors
POTENTIAL LINKAGES BETWEEN THE QUALITY AND OUTCOMES FRAMEWORK (QOF) AND THE NHS HEALTH CHECK
 AND THE NHS HEALTH CHECK") POTENTIAL LINKAGES BETWEEN THE QUALITY AND OUTCOMES FRAMEWORK (QOF) AND THE NHS HEALTH CHECK Author: CHARLOTTE SIMPSON, SPECIALTY REGISTAR PUBLIC HEALTH (ST3), CHESHIRE EAST COUNCIL/MERSEY DEANERY SUMMARY
POTENTIAL LINKAGES BETWEEN THE QUALITY AND OUTCOMES FRAMEWORK (QOF) AND THE NHS HEALTH CHECK Author: CHARLOTTE SIMPSON, SPECIALTY REGISTAR PUBLIC HEALTH (ST3), CHESHIRE EAST COUNCIL/MERSEY DEANERY SUMMARY
Complications of Diabetes: Screening and Prevention
 Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
NICE Indicator Programme. Consultation on proposed amendments to current QOF indicators
 NICE Indicator Programme Consultation on proposed amendments to current QOF s Consultation dates: 18 July to 1 August 2018 This document outlines proposed amendments to a small number of QOF s in the diabetes
NICE Indicator Programme Consultation on proposed amendments to current QOF s Consultation dates: 18 July to 1 August 2018 This document outlines proposed amendments to a small number of QOF s in the diabetes
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
New Antihypertensive Strategies to Improve Blood Pressure Control
 New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Getting serious about preventing cardiovascular disease
 Getting serious about preventing cardiovascular disease Southwark s Experience Professor Kevin Fenton Director of Health and Wellbeing, London Borough of Southwark February 2018 Twitter: @ProfKevinFenton
Getting serious about preventing cardiovascular disease Southwark s Experience Professor Kevin Fenton Director of Health and Wellbeing, London Borough of Southwark February 2018 Twitter: @ProfKevinFenton
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
2/10/2014. Hypertension: Highlights of Hypertension Guidelines: Making the Most of Limited Evidence. Issues with contemporary guidelines
 Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Dyslipidaemia. Is there any new information? Dr. A.R.M. Saifuddin Ekram
 Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
ESC/EAS Guidelines for the Management of Dyslipidaemias
 ESC/EAS Guidelines for the Management of Dyslipidaemias Professor Željko Reiner, MD, PhD, FRCP(Lond), FESC, FACC University Hospital Center Zagreb School of Medicine, University of Zagreb, Croatia Declaration
ESC/EAS Guidelines for the Management of Dyslipidaemias Professor Željko Reiner, MD, PhD, FRCP(Lond), FESC, FACC University Hospital Center Zagreb School of Medicine, University of Zagreb, Croatia Declaration
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Controversies in Preventative Cardiology
 Controversies in Preventative Cardiology Francisco Lopez-Jimenez, M.D., M.Sc, FACC, FAHA Professor of Medicine, Mayo Medical School Chair, Division of Preventive Cardiology Co-Director, Artificial Intelligence
Controversies in Preventative Cardiology Francisco Lopez-Jimenez, M.D., M.Sc, FACC, FAHA Professor of Medicine, Mayo Medical School Chair, Division of Preventive Cardiology Co-Director, Artificial Intelligence
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventive Cardiology Scientific evidence
 Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Beyond Framingham. Prediction of cardiovascular risk. Niels van Pelt Cardiologist, Middlemore Hospital
 Beyond Framingham Prediction of cardiovascular risk Niels van Pelt Cardiologist, Middlemore Hospital Niels Bohr (Danish Physicist)1885-1962 Prediction is very difficult, especially if it's about the future
Beyond Framingham Prediction of cardiovascular risk Niels van Pelt Cardiologist, Middlemore Hospital Niels Bohr (Danish Physicist)1885-1962 Prediction is very difficult, especially if it's about the future
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification