JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
|
|
|
- Cora Rice
- 5 years ago
- Views:
Transcription
1 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
2 THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated injuries (abdominal and others) High complication rate WWII - series of 118 cases of duodenal injuries with 57% mortality. Largest military series.

3 RELATIONSHIPS TO ADJACENT STRUCTURES ANATOMY duodenum digitorum - space of 12 digits. 30 cm D1 - pylorus to CBD and GDA D2 - CBD to ampulla of Vater D3 - Ampulla - SMA/SMV D4 - SMA/SMV - jejunum

4 ANATOMIC CONSIDERATIONS ADJACENT STRUCTURES Over aorta and IVC; spine SMV joins splenic vein to form portal vein Anterior to right kidney Inferior to gallbladder and liver Distal pancreas intimate with spleen Multiple variations in vascular anatomy
5 PHYSIOLOGIC CONSIDERATIONS PANCREATIC FUNCTION Approximately 10 L of fluid from stomach, biliary tract, and pancreas pass through duodenum each day. Normally, small bowel absorbs 80% of this If hole, leak, fistula - significant impact on fluid and electrolyte homeostasis. Endocrine (insulin, glucagon, gastrin) and Exocrine (amylase, proteases and lipases)
6 IMAGING, LABS DIAGNOSIS History - blow to epigastric area Labs (amylase, lipase) - can be helpful but unreliable Imaging - CT scan - good (80-90%) at detecting injury, but not very good at determining ductal injury ERCP - can be diagnostic and therapeutic (stent) MRCP - non-invasive. Not very helpful
7 INTRA-OPERATIVE STRATEGIES DIAGNOSIS OF INJURY INTRA-OPERATIVELY Laparotomy - bile staining, retroperitoneal hematoma, fat necrosis, supra-mesocolic edema. Kocher maneuver - head of pancreas and duodenum Lesser sack/ gastrocolic ligament - body and tail of pancreas In rare cases, need to divide pancreas - smv/pv bleeding
8 COMBINED PANCREATICODUODENAL INJURIES PRINCIPLES OF TREATMENT Adequate debridement and drainage Duodenal diversion Nutritional support

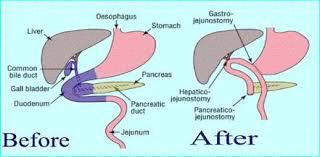
9 THERAPEUTIC OPTIONS TREATMENT Grade 1/2 - non-operative tx or simple drainage Grade 3 - Distal pancreatectomy +/- splenectomy vs wide drainage Grade 4 - wide drainage, ERCP/stent Grade 5 - Damage control laparotomy; Wide drainage and debridement,?staged Whipple - if devitalized duodenum or pancreatic head

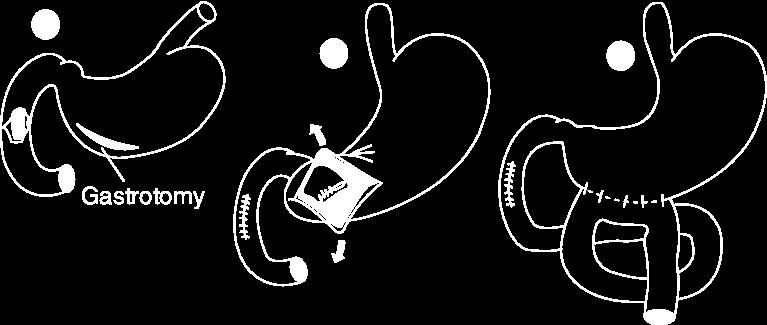
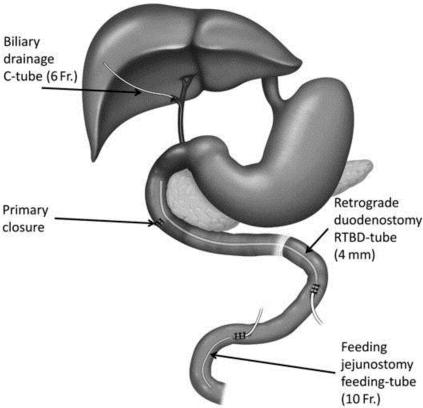
10 SEVERAL OPTIONS USUALLY MEANS NO BEST SOLUTION TREATMENT OF DUODENAL INJURIES Grade 1 - observe Grade 2 - +/- evacuate hematoma; primary repair (single layer monofilament) Grade 3 - Primary repair, duodenoduodenostomy, duodenojejunostomy, pyloric exclusion +/- feeding jejunostomy, triple tube therapy Grade 4/5 - damage control;? delayed whipple
11 MORE OPTIONS DUODENAL MANAGEMENT - CONTINUED Duodenal diverticulization (Berne et al, 1968) - antrectomy, vagotomy, tube douodenostomy, and gastrojejunostomy. Time consuming, resecting normal stomach, largely abandoned. Pyloric exclusion - Close pylorus, gastrojejunostomy. Ben Taub experience (Vaughn et al). More recent data worse results (Dubose JJ, Inaba K, Teixeira, et al) - more complications and no survival benefit.


12
13 DO BEST OPTION FIRST MORE DUODENAL TRICKS Duodenostomy - for decompression after primary repair Serosal patches Both show no benefit (Ivatury, et al) Duodenojejunostomy with Roux-en-Y reconstruction may be safest option if cannot repair primarily (Weigelt, et al)
14 MORBIDITY AND MORTALITY COMPLICATIONS Hemorrhage - most common cause of early death; delayed Pancreatic fistula - low/high output. Drainage, ERCP/stent, operative tx. Somatostatin, Distal feeding. Adds avg 27 days and $191K. Duodenal fistula and stricture - pyloric exclusion with gastroenterostomy - decreases output of fistula and facilitates drainage of GI tract if stricture
15 MORBIDITY CONTINUES COMPLICATIONS Abdominal abscess - Image guided drainage can usually effectively manage Pancreatic pseudocyst - endoscopic, percutaneous and surgical options Pancreatitis - usually self limiting. Pancreatic necrosis requires debridement at times. Pancreatic insufficiency - Usually if > 80% removed or underlying pathology. Replace endocrine/exocrine fun
16 HERE S THE DEAL SUMMARY Complex pancreaticoduodenal injuries are challenging In acute setting, stop bleeding, identify injuries, close holes, and drain Avoid Whipple (definitely the reconstruction) in initial operation, but do it soon if necessary Bile, gastric contents and pancreatic enzymes leaking into abdominal cavity and/or retroperitoneum worse than results of good Whipple Good Luck!
Complex pancreatico- duodenal injuries. Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University
 Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Surgical Management of CBD Injury Jin Seok Heo
 Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY 2013/12/21
 THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
Multilevel Duodenal Injury after Blunt Trauma
 J Korean Surg Soc 2009;77:282-286 DOI: 10.4174/jkss.2009.77.4.282 증 례 Multilevel Duodenal Injury after Blunt Trauma Department of Surgery, College of Medicine, Hallym University, Chuncheon, Korea Jeong
J Korean Surg Soc 2009;77:282-286 DOI: 10.4174/jkss.2009.77.4.282 증 례 Multilevel Duodenal Injury after Blunt Trauma Department of Surgery, College of Medicine, Hallym University, Chuncheon, Korea Jeong
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Duodenum retroperitoneal
 Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Anatomy of the SMALL INTESTINE. Dr. Noman Ullah Wazir PMC
 Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
Nasogastric tube. Stomach. Pylorus. Duodenum 1. Duodenum 2. Duodenum 3. Duodenum 4
 Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Dr. Zahiri. In the name of God
 Dr. Zahiri In the name of God small intestine = small bowel is the part of the gastrointestinal tract Boundaries: Pylorus Ileosecal junction Function: digestion and absorption of food It receives bile
Dr. Zahiri In the name of God small intestine = small bowel is the part of the gastrointestinal tract Boundaries: Pylorus Ileosecal junction Function: digestion and absorption of food It receives bile
Pancreas & Biliary System. Dr. Vohra & Dr. Jamila
 Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT
 BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT By: Amy Cisyk Home for the Summer Program July, 2016 Brandon, Manitoba Supervisor: Dr. Marvin Goossen Whipple s Procedure Audit
BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT By: Amy Cisyk Home for the Summer Program July, 2016 Brandon, Manitoba Supervisor: Dr. Marvin Goossen Whipple s Procedure Audit
د. عصام طارق. Objectives:
 GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
Penetrating Injuries to the Stomach, Duodenum, and Small Bowel
 Curr Trauma Rep (2015) 1:107 112 DOI 10.1007/s40719-015-0010-2 PENETRATING INJURIES TO HOLLOW ABDOMINAL VISCERA (K INABA, SECTION EDITOR) Penetrating Injuries to the Stomach, Duodenum, and Small Bowel
Curr Trauma Rep (2015) 1:107 112 DOI 10.1007/s40719-015-0010-2 PENETRATING INJURIES TO HOLLOW ABDOMINAL VISCERA (K INABA, SECTION EDITOR) Penetrating Injuries to the Stomach, Duodenum, and Small Bowel
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
1 Right & left Hepatic ducts Gastric Impression of spleen
 Pancreatic Model 1 Right & left Hepatic ducts 14 Gastric Impression of spleen 2 Common hepatic duct 15 Renal Impression of spleen 3 Cystic Duct 16 Colic Impression of spleen 4 Common Bile Duct 17 Splenic
Pancreatic Model 1 Right & left Hepatic ducts 14 Gastric Impression of spleen 2 Common hepatic duct 15 Renal Impression of spleen 3 Cystic Duct 16 Colic Impression of spleen 4 Common Bile Duct 17 Splenic
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
Anatomy: Know Your Abdomen
 Anatomy: Know Your Abdomen Glossary Abdomen - part of the body below the thorax (chest cavity); separated by the diaphragm. Anterior - towards the front of the body. For example, the umbilicus is anterior
Anatomy: Know Your Abdomen Glossary Abdomen - part of the body below the thorax (chest cavity); separated by the diaphragm. Anterior - towards the front of the body. For example, the umbilicus is anterior
USMLE Step 1 Problem Drill 17: Gastrointestinal System
 USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Complication of Laparoscopic Cholecystectomy
 Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
To describe the liver. To list main structures in porta hepatis.
 GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
BILIARY TRACT & PANCREAS, PART II
 CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
Pylorus Preserving Pancreaticoduodenectomy
 REVIEW Pylorus Preserving Pancreaticoduodenectomy Jacqueline M. Garonzik-Wang, M. B. Majella Doyle Pancreaticoduodenectomy (PD) has become the standard of care for resectable pancreatic cancer and premalignant
REVIEW Pylorus Preserving Pancreaticoduodenectomy Jacqueline M. Garonzik-Wang, M. B. Majella Doyle Pancreaticoduodenectomy (PD) has become the standard of care for resectable pancreatic cancer and premalignant
Prevention Of Pancreaticojejunal Fistula After Whipple Procedure
 ISPUB.COM The Internet Journal of Surgery Volume 4 Number 2 Prevention Of Pancreaticojejunal Fistula After Whipple Procedure N Barbetakis, K Setsiz Citation N Barbetakis, K Setsiz. Prevention Of Pancreaticojejunal
ISPUB.COM The Internet Journal of Surgery Volume 4 Number 2 Prevention Of Pancreaticojejunal Fistula After Whipple Procedure N Barbetakis, K Setsiz Citation N Barbetakis, K Setsiz. Prevention Of Pancreaticojejunal
GASTROINTESTINAL SYSTEM
 GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
PANCREAS DUCTAL ADENOCARCINOMA PDAC
 CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
The gastroduodenal artery: Radiological anatomy, imaging and endovascular intervention
 The gastroduodenal artery: Radiological anatomy, imaging and endovascular intervention Poster No.: C-2049 Congress: ECR 2010 Type: Educational Exhibit Topic: Interventional Radiology Authors: R. D. White,
The gastroduodenal artery: Radiological anatomy, imaging and endovascular intervention Poster No.: C-2049 Congress: ECR 2010 Type: Educational Exhibit Topic: Interventional Radiology Authors: R. D. White,
Gastrointestinal Complications of Hepatic Transplantation
 Gastrointestinal Complications of Hepatic Transplantation L. J. Koep, T. E. Starzl, and R. Weil III I N THE largest series of orthotopic liver transplants, now numbering 150 patients, the largest number
Gastrointestinal Complications of Hepatic Transplantation L. J. Koep, T. E. Starzl, and R. Weil III I N THE largest series of orthotopic liver transplants, now numbering 150 patients, the largest number
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE. PRESENTED BY: Susan DePasquale, CGRN, MSN
 PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
Treatment of chronic calcific pancreatitis endoscopy versus surgery
 Treatment of chronic calcific pancreatitis endoscopy versus surgery 35 - year old ladypresented to LPC Mumbai with intermittent abdominal pain. Pain was intermittent, colicky, more in epigastrium and periumbilical
Treatment of chronic calcific pancreatitis endoscopy versus surgery 35 - year old ladypresented to LPC Mumbai with intermittent abdominal pain. Pain was intermittent, colicky, more in epigastrium and periumbilical
Pancreas (non-endocrine) (see also: biliary/pancreatic folios => pancreas)
 (see also: biliary/pancreatic folios => pancreas)") Pancreas (non-endocrine) (see also: biliary/pancreatic folios => pancreas) Physiology ductal system produces bicarb, high carbonic anhydrase secretin primary stimulus duodenal enterokinase activates trypsin
Pancreas (non-endocrine) (see also: biliary/pancreatic folios => pancreas) Physiology ductal system produces bicarb, high carbonic anhydrase secretin primary stimulus duodenal enterokinase activates trypsin
ABDOMEN - GI. Duodenum
 TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
-12. -Renad Habahbeh. -Dr Mohammad mohtasib
 -12 -Renad Habahbeh - -Dr Mohammad mohtasib The Gallbladder -The gallbladder has a body, a fundus (a rounded end), a neck, Hartmann s pouch before the neck and a cystic duct that meets the common hepatic
-12 -Renad Habahbeh - -Dr Mohammad mohtasib The Gallbladder -The gallbladder has a body, a fundus (a rounded end), a neck, Hartmann s pouch before the neck and a cystic duct that meets the common hepatic
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Common Bile Duct (CBD)
") Liver Last time we talked about the liver and the doctor started by revising some information about it: It has five surfaces. It reaches the 5 th intercostal space ; some books write that it reaches the
Liver Last time we talked about the liver and the doctor started by revising some information about it: It has five surfaces. It reaches the 5 th intercostal space ; some books write that it reaches the
Surgical Workload, Outcome and Research Database: V1.1
 Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Pancreas and Biliary System
 Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Pediatric Pancreatic Lesions
 Pediatric Pancreatic Lesions Pediatric Surgery Grand Rounds 9 October 2013 Tim Weatherall, PGY2 The University of Tennessee Health Science Center Memphis, TN Disclosures No financial interests to disclose
Pediatric Pancreatic Lesions Pediatric Surgery Grand Rounds 9 October 2013 Tim Weatherall, PGY2 The University of Tennessee Health Science Center Memphis, TN Disclosures No financial interests to disclose
4/9/2018 OBJECTIVES PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS
 PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
Pancreatic Lesions. Valerie Jefford Pediatric Surgery Rounds June 6, 2003
 Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Reinterventions belong to complications
 Reinterventions belong to complications Pancreatic surgery is the archetypus of complex abdominal surgery Mortality (1-4%) and morbidity (7-60%) rates are relevant even at high volume centres Reinterventions
Reinterventions belong to complications Pancreatic surgery is the archetypus of complex abdominal surgery Mortality (1-4%) and morbidity (7-60%) rates are relevant even at high volume centres Reinterventions
Anatomical and Functional MRI of the Pancreas
 Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
Chronic Pancreatitis. Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture
 Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
Index (SIRS), 158, 173
, 158, 173") Index A Acute pancreatitis surgery abdominal compartment syndrome, 188 adjuvant treatment, 194 anterior approach, 175 antibiotic prophylaxis, 166 167, 197 Atlanta classification, 181 classification of
Index A Acute pancreatitis surgery abdominal compartment syndrome, 188 adjuvant treatment, 194 anterior approach, 175 antibiotic prophylaxis, 166 167, 197 Atlanta classification, 181 classification of
I patients with nonendocrine pancreas carcinoma
 LYMPH NODE INVOLVEMENT IN CARCINOMA OF THE HEAD OF THE PANCREAS AREA ANTONIO L. CUBILLA, MD,* JOSEPH FORTNER, MD,+~ AND PATRICK J. FITZGERALD, MD*~ A prospective study to determine the lymph node involvement
LYMPH NODE INVOLVEMENT IN CARCINOMA OF THE HEAD OF THE PANCREAS AREA ANTONIO L. CUBILLA, MD,* JOSEPH FORTNER, MD,+~ AND PATRICK J. FITZGERALD, MD*~ A prospective study to determine the lymph node involvement
Surgery for pancreatic cancer
 Surgery for pancreatic cancer Andrew Smith 12 September 2018 Leeds Regional Study Day North & West Yorkshire Pancreas Department Pancreatic Surgery Range of pancreatic surgery Pre-op preparation Post op
Surgery for pancreatic cancer Andrew Smith 12 September 2018 Leeds Regional Study Day North & West Yorkshire Pancreas Department Pancreatic Surgery Range of pancreatic surgery Pre-op preparation Post op
Appendix 9: Endoscopic Ultrasound in Gastroenterology
 Appendix 9: Endoscopic Ultrasound in Gastroenterology This curriculum is intended for clinicians who perform endoscopic ultrasonography (EUS) in gastroenterology. It includes standards for theoretical
Appendix 9: Endoscopic Ultrasound in Gastroenterology This curriculum is intended for clinicians who perform endoscopic ultrasonography (EUS) in gastroenterology. It includes standards for theoretical
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist. Alireza Sedarat, MD UCLA Division of Digestive Diseases
 Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
DIGESTIVE. CHAPTER 17 Lecture: Part 1 Part 2 BIO 212: ANATOMY & PHYSIOLOGY II
 BIO 212: ANATOMY & PHYSIOLOGY II CHAPTER 17 Lecture: DIGESTIVE Part 1 Part 2 Dr. Lawrence G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill. SMALL INTESTINE DUODENUM > JEJUNUM
BIO 212: ANATOMY & PHYSIOLOGY II CHAPTER 17 Lecture: DIGESTIVE Part 1 Part 2 Dr. Lawrence G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill. SMALL INTESTINE DUODENUM > JEJUNUM
Lesions of the pancreaticoduodenal groove, a pictorial review
 Lesions of the pancreaticoduodenal groove, a pictorial review Poster No.: C-2131 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Ni Mhurchu, L. Lavelle, I. Murphy, S. Skehan ; IE, Dublin/ IE Keywords:
Lesions of the pancreaticoduodenal groove, a pictorial review Poster No.: C-2131 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Ni Mhurchu, L. Lavelle, I. Murphy, S. Skehan ; IE, Dublin/ IE Keywords:
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Preview from Notesale.co.uk Page 1 of 34
 Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
Severe necrotizing pancreatitis. ICU Fellowship Training Radboudumc
 Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER
 1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
TRAUMATIC DUODENAL RUPTURE AND AVULSION
 HPB Surgery, 1994, Vol. 7, pp. 225-229 Reprints available directly from the publisher Photocopying permitted by license only (C) 1994 Harwood Academic Publishers GmbH Printed in the United States of America
HPB Surgery, 1994, Vol. 7, pp. 225-229 Reprints available directly from the publisher Photocopying permitted by license only (C) 1994 Harwood Academic Publishers GmbH Printed in the United States of America
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer
 What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
General Surgery PURPLE SERVICE MUHC-RVH Site
 Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Chronic Pancreatitis: Surgical Options. W. Charles Conway MD, FACS Upper GI/HPB Surgical Oncology Ochsner Medical Center New Orleans, LA
 Chronic Pancreatitis: Surgical Options W. Charles Conway MD, FACS Upper GI/HPB Surgical Oncology Ochsner Medical Center New Orleans, LA Chronic Pancreatitis Recurrent, debilitating abdominal pain with
Chronic Pancreatitis: Surgical Options W. Charles Conway MD, FACS Upper GI/HPB Surgical Oncology Ochsner Medical Center New Orleans, LA Chronic Pancreatitis Recurrent, debilitating abdominal pain with
Gastric Contrac,le Ac,vity. Regula,on of Gastric Emptying
 Gastric Contrac,le Ac,vity Figure 23.18 Regula,on of Gastric Emptying Gastric emptying is regulated by: Neural enterogastric reflex Hormonal (enterogastrone) mechanisms In the presence of gastric gastrin
Gastric Contrac,le Ac,vity Figure 23.18 Regula,on of Gastric Emptying Gastric emptying is regulated by: Neural enterogastric reflex Hormonal (enterogastrone) mechanisms In the presence of gastric gastrin
Postpancreatectomy Hemorrhage: Imaging and Interventional Radiological Treatment
 Postpancreatectomy Hemorrhage: Imaging and Interventional Radiological Treatment Poster No.: C-1422 Congress: ECR 2014 Type: Educational Exhibit Authors: T. Matsuura, K. Takase, T. Hasegawa, H. Ota, K.
Postpancreatectomy Hemorrhage: Imaging and Interventional Radiological Treatment Poster No.: C-1422 Congress: ECR 2014 Type: Educational Exhibit Authors: T. Matsuura, K. Takase, T. Hasegawa, H. Ota, K.
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil
 Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
EFSUMB EUROPEAN FEDERATION OF SOCIETIES FOR ULTRASOUND IN MEDICINE AND BIOLOGY Building a European Ultrasound Community
 MINIMUM TRAINING REQUIREMENTS FOR THE PRACTICE OF MEDICAL ULTRASOUND IN EUROPE Appendix 9: Endoscopic Ultrasound in Gastroenterology This curriculum is intended for clinicians who perform endoscopic ultrasonography
MINIMUM TRAINING REQUIREMENTS FOR THE PRACTICE OF MEDICAL ULTRASOUND IN EUROPE Appendix 9: Endoscopic Ultrasound in Gastroenterology This curriculum is intended for clinicians who perform endoscopic ultrasonography
Development of the Liver and Pancreas
 Development of the Liver and Pancreas Professor Alfred Cuschieri Department of Anatomy University of Malta Three glandular buds arise from the distal end of the foregut during the fourth week Day 22 -The
Development of the Liver and Pancreas Professor Alfred Cuschieri Department of Anatomy University of Malta Three glandular buds arise from the distal end of the foregut during the fourth week Day 22 -The
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I
 IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
Safety of Repair for Severe Duodenal Injuries
 World J Surg (2008) 32:7 12 DOI 10.1007/s00268-007-9255-4 Safety of Repair for Severe Duodenal Injuries George C. Velmahos Æ Constantinos Constantinou Æ George Kasotakis Published online: 22 October 2007
World J Surg (2008) 32:7 12 DOI 10.1007/s00268-007-9255-4 Safety of Repair for Severe Duodenal Injuries George C. Velmahos Æ Constantinos Constantinou Æ George Kasotakis Published online: 22 October 2007
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options
 Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
Biology Human Anatomy Abdominal and Pelvic Cavities
 Biology 351 - Human Anatomy Abdominal and Pelvic Cavities Please place your name and I.D. number on the back of the last page of this exam. You must answer all questions on this exam. Because statistics
Biology 351 - Human Anatomy Abdominal and Pelvic Cavities Please place your name and I.D. number on the back of the last page of this exam. You must answer all questions on this exam. Because statistics
Cattell-Braasch maneuver combined with superior mesenteric artery first approach for resection of borderline resectable pancreatic cancer
 Masters of Surgery Page 1 of 5 Cattell-Braasch maneuver combined with superior mesenteric artery first approach for resection of borderline resectable pancreatic cancer Tingsong Yang 1, Fairweather Mark
Masters of Surgery Page 1 of 5 Cattell-Braasch maneuver combined with superior mesenteric artery first approach for resection of borderline resectable pancreatic cancer Tingsong Yang 1, Fairweather Mark
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
Diagnosis of chronic Pancreatitis. Christoph Beglinger, University Hospital Basel, Switzerland
 Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
(A) Diarrhea. (B) Stomach cramps. (C) Dehydration due to excess fluid loss. (D) A, B, and C are correct. (E) Only answer B is correct.
 Diarrhea. (B) Stomach cramps. (C) Dehydration due to excess fluid loss. (D) A, B, and C are correct. (E) Only answer B is correct.") Human Anatomy - Problem Drill 21: The Digestive System Question No. 1 of 10 1. A 26-year-old male is treated in the emergency department for severe gastrointestinal disturbance. Which of the following
Human Anatomy - Problem Drill 21: The Digestive System Question No. 1 of 10 1. A 26-year-old male is treated in the emergency department for severe gastrointestinal disturbance. Which of the following
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE
 PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
NUTRIENT DIGESTION & ABSORPTION
 NUTRIENT DIGESTION & ABSORPTION NUTR 2050: Nutrition for Nursing Professionals Mrs. Deborah A. Hutcheon, MS, RD, LD Lesson Objectives At the end of the lesson, the student will be able to: 1. Differentiate
NUTRIENT DIGESTION & ABSORPTION NUTR 2050: Nutrition for Nursing Professionals Mrs. Deborah A. Hutcheon, MS, RD, LD Lesson Objectives At the end of the lesson, the student will be able to: 1. Differentiate
Adipocytes, Obesity, Bariatric Surgery and its Complications
 Adipocytes, Obesity, Bariatric Surgery and its Complications Daniel C. Morris, MD, FACEP, FAHA Senior Staff Physician Department of Emergency Medicine Objectives Basic science of adipocyte Adipocyte tissue
Adipocytes, Obesity, Bariatric Surgery and its Complications Daniel C. Morris, MD, FACEP, FAHA Senior Staff Physician Department of Emergency Medicine Objectives Basic science of adipocyte Adipocyte tissue
5/17/2013. Pancreatic Cancer. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Case presentation. Differential diagnosis
 Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Small Plicae Circularis. Short Closely packed together. Sparse, completely absent at distal part Lymphoid Nodule
 Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Citation Hepato-Gastroenterology, 55(86-87),
,") NAOSITE: Nagasaki University's Ac Title Author(s) Combined pancreatic resection and p multiple lesions of the pancreas: i of the pancreas concomitant with du Kuroki, Tamotsu; Tajima, Yoshitsugu Tomohiko;
NAOSITE: Nagasaki University's Ac Title Author(s) Combined pancreatic resection and p multiple lesions of the pancreas: i of the pancreas concomitant with du Kuroki, Tamotsu; Tajima, Yoshitsugu Tomohiko;
Laparoscopic & Robotic Surgery in Pancreas Disease
 2007 년도대한췌담도학회추계학술대회 Session IV: Recent Updates in Pancreatobiliary Diseases Laparoscopic & Robotic Surgery in Pancreas Disease Department of Surgery, Yonsei University College of Medicine, Korea Woo-Jung
2007 년도대한췌담도학회추계학술대회 Session IV: Recent Updates in Pancreatobiliary Diseases Laparoscopic & Robotic Surgery in Pancreas Disease Department of Surgery, Yonsei University College of Medicine, Korea Woo-Jung
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
This lab activity is aligned with Visible Body s Human Anatomy Atlas app. Learn more at visiblebody.com/professors
 1 This lab activity is aligned with Visible Body s Human Anatomy Atlas app. Learn more at visiblebody.com/professors 2 A. Digestive System Overview To Start: Go to the Views menu and scroll down to the
1 This lab activity is aligned with Visible Body s Human Anatomy Atlas app. Learn more at visiblebody.com/professors 2 A. Digestive System Overview To Start: Go to the Views menu and scroll down to the
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Surgical Treatment for Periampullary Carcinoma A Study of 129 Patients*)
") Hiroshima Journal of Medical Sciences Vol. 33, No. 2, 179,...183, June, 1984 HJM 33-24 179 Surgical Treatment for Periampullary Carcinoma A Study of 129 Patients*) Tsuneo TAN AKA, Motomu KODAMA, Rokuro
Hiroshima Journal of Medical Sciences Vol. 33, No. 2, 179,...183, June, 1984 HJM 33-24 179 Surgical Treatment for Periampullary Carcinoma A Study of 129 Patients*) Tsuneo TAN AKA, Motomu KODAMA, Rokuro