What the Referring Physician Needs to Know About Magnetoencephalography (MEG)
|
|
|
- Irene Benson
- 5 years ago
- Views:
Transcription

1 What the Referring Physician Needs to Know About Magnetoencephalography (MEG) Richard C. Burgess, MD, PhD Director, Magnetoencephalography Laboratory Cleveland Clinic Epilepsy Center An American Clinical MEG Society Educational Webinar November 21, 2013
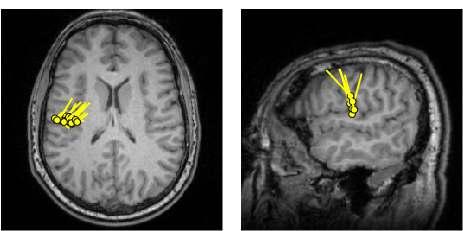
2 What is MEG? Green dots = Subdural electrode positions. Green cylinders = Depth electrode positions. Blue lollipops = MEG dipoles, where sphere is locaton and stem is orientation. Coregistration of MEG dipole sources and invasive electrodes
3 What is MEG? Neurophysiological Principles Based on recording of incredibly small magnetic fields (10-12 T). Easy acquisition of very high density ( channels), wideband (DC 2000 hz) recordings of currents within the brain. Magnetic fields, as opposed to electrical currents, suffer minimum attenuation and distortion from the different tissues that they have to cross to reach the scalp surface.
4 What is MEG? MEG is a localization tool. Based on solid theoretical reasons, MEG has localization accuracy better than the scalp EEG. Greater number of sensors typically employed Simpler source modeling and calculation Anatomical co-registration with 3D-MRI MEG is a neurophysiological technique, not an imaging method.
5 What do we know about MEG? MEG provides additional localizing information. (Wheless et al, 1999; Stefan et al, 2003; Pataraia et al, 2004) MEG results change the electrode coverage decisions for intracranial EEG. (Knowlton et al, 2009) The yield of MEG is higher than scalp EEG. (Yoshinaga et al, 2002; Iwasaki et al, 2005)
6 MEG is a valuable component of the presurgical epilepsy evaluation Evaluation goals in potential epilepsy surgery candidates: Locate the epileptogenic zone. Assess whether it can be resected to achieve seizure freedom. Multi-modality investigative tools: Video-EEG monitoring +/- sphenoidals MRI PET/SPECT Neuropsychology Wada/fMRI MEG source localization Invasive Monitoring
7 What Are the Main Questions from Epileptologists? 1. What should the referring physician expect from a MEG study? 2. What are the basic MEG modalities, clinical indications, and capabilities? 3. For patients with epilepsy, how can MEG help? 4. What can epileptologists expect from MEG in the future?
8 Some polling questions for the audience 1) Where do you send patients for clinical diagnostic MEG studies? a) MEG lab in my own institution. b) MEG lab at another institution. c) I do not have convenient access to any MEG lab for my patients. d) I do not currently request MEG testing. 2) What clinical indications do you currently use MEG for, or would you like to use MEG for? a) Epileptogenic zone localization. b) Sensory and/or motor evoked fields. c) Language assessment. d) Both epilepsy localization and eloquent cortex mapping. 3) What has been the greatest limitation of MEG testing in your patients? a) Results have been negative or provide no new information. b) Results are discordant with the rest of the clinical picture. c) Contents of the reports are confusing or not clinically relevant. d) I have generally been satisfied with the results of clinical MEG testing and the reports that I receive.
9 What is the MEG signal? Genesis of EEG and MEG Signals: A current dipole creates a magnetic field


 in the brain can adequately model surface")
10 Dipolar representation of brain currents The signals picked up by scalp electrodes or MEG sensors are generated by synchronized activity from many neurons Postsynaptic potentials produce intracellular laminar currents Neocortical pyramidal neurons arranged in a palisade structure Typically seen as a current dipole perpendicular to the cortical surface Dipolar models are based on the assumption that a small number of current sources (multiple dipoles) in the brain can adequately model surface measurements.
11 EEG and MEG Waveforms EEG MEG
12 Electric fields and magnetic fields generated by a current dipole


13 How is MEG recorded? MEG Instrumentation SQUID Flux transformers Shielded room Head position indicator
14 SQUID and Flux Transformer

15 How is MEG recorded? MEG Procedures Patient Preparation System / Patient Setup Data Recording Data Analysis HPI measurement Fiducial measurement Cloud of scalp points
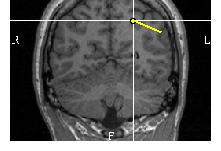
16 Careful Attention to Postion of Fiducials, Landmarks, HPI Coils Use of HPI (head position indicator) coils: Number: 5 Positions: Widely spaced over scalp but well inside array Alignment of scalp with MRI and MEG array: Three fiducials (LPA, RPA, Naison) Digitize additional scalp points for coregistration with MRI 16

17 MEG Procedures Patient Preparation System / Patient Setup Data Recording Data Analysis Simultaneous EEG and video monitoring with MEG On-line marker entry Feedback noise compensation Continuous head-position monitoring
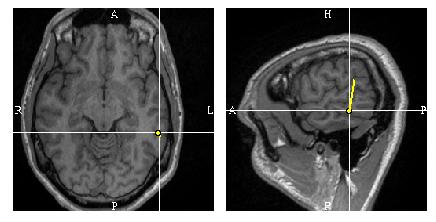
18 Alignment of Subject in MEG Array Generation of alignment image in real-time to insure good position Location of HPI coils monitored continuously.

19 MEG Procedures Patient Preparation System / Patient Setup Data Recording Data Analysis Review of markers Review of video Visual / manual analysis of every channel of MEG and EEG Montages Single ECD analysis at core
20 What are the Advantages of MEG? Why use MEG in epilepsy patients? 1. Inherently higher source resolution. 2. Direct connection to patient (i.e. pasting electrodes on) is not required. 3. Reference free. 4. Signals not attenuated or distorted by bone and scalp, or other inhomogeneities that exist between brain and surface. 5. Therefore for source analysis, the head modelling problem is significantly simpler. 6. Easy to obtain multichannel, whole-head, high spatial-density recordings. 7. No exposure to radiation, magnetic field, or other active device.
21 High temporal and spatial resolution Patient with parietal lobe seizures Scalp video-eeg localization unclear

22 Polyspikes Originating from Left parietal



23 Propagation of Polyspike Activity to Left Parietal Left basal temporo-occpital 37 msec Left inferior parietal 161 msec Left middle temporal
24 Representative interictal dipoles LEFT LEFT
25 High temporal and spatial resolution Patient with non-localizable, non-lateralizable scalp video-eeg

26 EEG: Polyspikes, Vertex #1 #2 Run I EEG

27 MEG: Polyspikes, Left > Right parietal sensors #1 #2 Left parietal sensors Right parietal sensors


28 All interictal dipoles: Left frontal CS LEFT CS
29 Why does MEG have a higher yield than EEG? EEG and MEG are complementary. MEG not only sees some different source, but sees more sources. Geography: MEG is more sensitive to tangential sources, while EEG is more sensitive to radial sources. Approximately 2/3 of cortex lies in sulci, i.e. more tangential sources. Resolution: MEG has an inherently higher resolution. Requires only ~4 cm 2 vs 6 cm 2 of synchronized discharging cortex. (Oishi M, Otsubo H et al. Epileptic spikes: Magnetoencephalography vs simultaneous electrocorticography. Epilepsia 43: ; 2002.) (Agirre-Arrizubieta Z et al. Brain 132, ; 2009)
30 Differences and Similarities: EEG and MEG Similarities Record the same phenomenon Same time-resolution Spontaneous activities (epileptic spikes, non-epileptiform physiological), evoked responses (SEP, VEP, AEP) Sensitivity to brain volume and depth
31 Differences and Similarities: EEG and MEG Similarities Record the same phenomenon Same time-resolution Spontaneous activities (epileptic spikes, non-epileptiform physiological), evoked responses (SEP, VEP, AEP) Sensitivity to brain volume and depth Differences Sensitivity to the current dipole orientation Sensitivity to the current dipole orientation Tangential or vertical to the scalp surface Complexity of the forward model Feasibility of the computerized source estimation Analysis MEG is reference-free Number of sensors Duration of the recording Different sensitivity to external noises Cost Established knowledge
32 Primary Clinical Applications Sensory Mapping Usually in relation to a lesion Mapping often done prior to resection Epileptic Spike Localization
33 What are the Indications for MEG in Epilepsy? Localization tool for interictal spikes Planning of intracranial investigations: grid placement, seeg, etc. Normal MRI or discordance between other non-invasive studies Pre-existing cranial defects (reoperations) Extensive lesions Multiple lesions Functional mapping Bilateral synchrony Normal EEG


34 Correlation of MEG Localization of Interictal Discharges to ICEEEG Ictal Activity ICEEG: Seizure Onset MEG: Interictal Dipoles
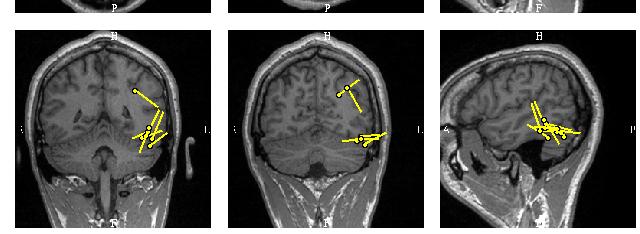
35 Patient Examples MEG localization is especially useful in patients with previous neurosurgery or other skull defects. Head shape, deformities, or position in the sensor array do not interfere.
36 Patient #1: MRI and EEG negative History 34 year old male Right-handed One febrile seizure at age 2.5 Onset: 10 years old Current seizures, up to 30/day, consist of a spasm in the neck and throat, sometimes accompanied by head turning to left, eye closure and facial grimacing Most recent GTC seizure was 15 years ago.
37 Patient #1 EEG and VEEG evaluations 1987 VEEG monitoring: 16 episodes recorded, none with any EEG change 1988 VEEG monitoring: 1 seizure lateralized to right 1989 Threee multihour EEG: No epileptiform abnormalities 1993 Routine EEG: Normal 1995 Routine EEG: Normal 2002 Routine EEG: Normal 2011 Routine EEG: Normal 2011 (February) 6 day VEEG monitoring: Many seizures with no EEG change, Two seizures with EEG patterns at the vertex, slightly higher on left 2011 (March) MEG


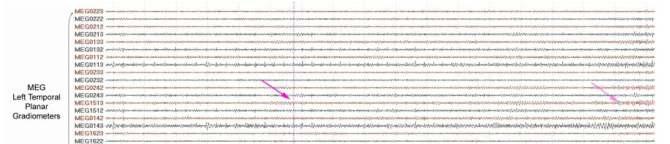
38 Spike, regional right temporal (Unique to MEG, not seen on EEG) Run I: Double banana bipolar EEG


39 Spike, regional right temporal on MEG MEG Left temporal sensors MEG Right temporal sensors


40 Right temporal spike dipole source localization L R L R RLeft
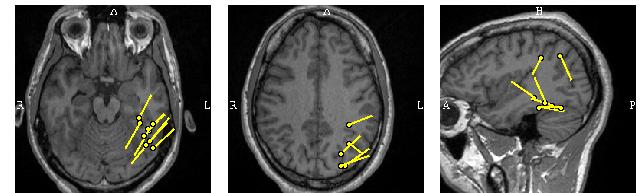
41 Representative spike dipoles R L Right side
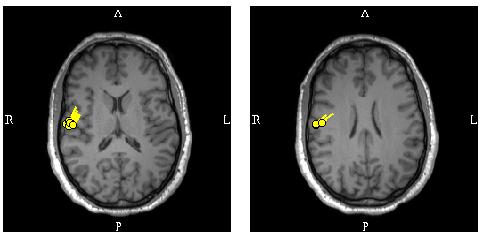
42 Patient #2: Scalp EEG Negative Case Example History: 55 year old, right handed male with onset of epilepsy at age 25. Mostly nocturnal seizures, sometimes in clusters, consisting of asymmetrical tonic posturing. Previous EEGs have been negative. MRI negative. Ictal SPECT showed bilateral frontal activation. VEEG monitoring showed extremely rare bifrontal spikes and non-localizable seizures. (MR# )


43 EEG: Intermittent slow, FP1/F3 1 sec 100 uv Run I EEG (Bipolar double bananna)
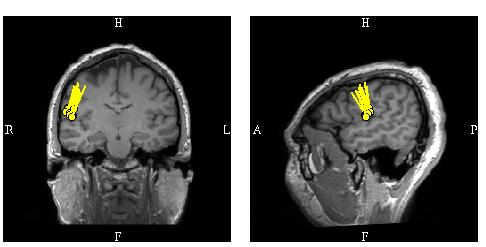
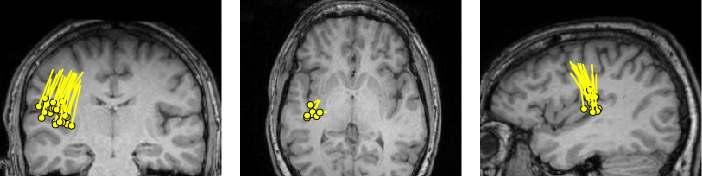
44 MEG: Run of sharp waves, Left frontal sensors (consistent localization) 1 sec 500 ft/cm Left frontal sensors Right frontal sensors




45 MEG Sources: Left middle frontal gyrus and superior frontal sulcus LEFT LEFT LEFT LEFT
 11 Spontaneous seizures")

46 Ictal Onset ( ) & CS seizure ( ) 11 Spontaneous seizures captured with onset at X 10,11,12 X 10 X 12 X 11 X 12 X 11
47 MEG in EEG-Negative Patients Routine MEGs: 358 Patients, 375 Studies Feb 2008 Jan 2012 Previous Routine EEG: 145 Patients (40.5%) No Epileptic Activity: 58 Patients (40%) MEG Results: Localizable dipoles: 38 Patients (65.5%) MEG-Unique Information: 12 Pt (31.6%) ( Ito et al. American Epilepsy Society Meeting, 2012 )
48 MEG in Non-Focal VEEG Patients Routine MEG 358 Patients, 375 Studies Previous EMU Evaluation 336 Patients (93.4%) Only generalized, no regional Activity: 83 Patients (24.7%) MEG Results: Localizable dipoles: 48 Patients (57.8%) MEG-Unique Information: 5 Pt (10.4%) ( Ito et al. American Epilepsy Society Meeting, 2012 )
49 Patient #3: MEG prompts re-review of a previously negative PET, identifying a subtle hypometabolism History: 42 yo right handed male Sz triggered by music with lyrics (or just thinking about the lyrics) that he knows Sz Classification: Auditory aura Dialeptic Right versive GTC
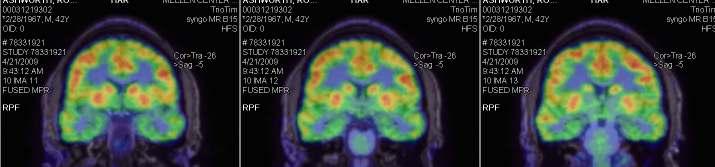
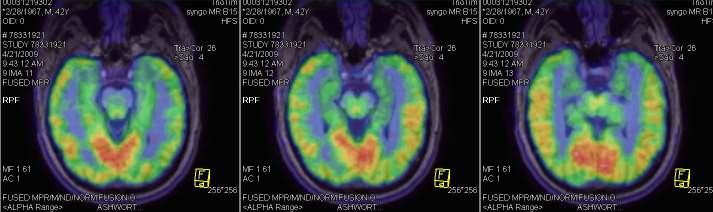
50 PET: Nonspecific



51 Simultaneous Multi-Modality Review: PET and MEG MEG highlights a subtle hypometabolism on a previously negative PET
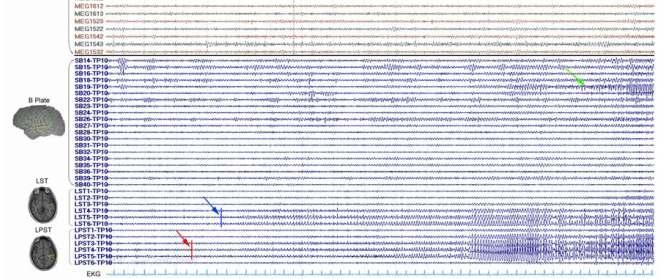
52 Simultaneous MEG and Subdural Grid Recording


53 Multimodality integration (Wang et al 2012, J of Neurology)
54 Some Myths and Realities about MEG Myth #1: MEG is too sensitive to artifacts and noise Myth #2: MEG only records interictal activity


55 Myth #1: MEG is too sensitive to noise and artifact.
56 Relative Field Strength Brain sources: Evoked cortical fields: 10 ft Alpha rhythm: 1000 ft Noise sources: Earth s magnetic field: ~50 µt Field from home appliances and wiring: <10 µt Urban environmental noise: 10 8 ft (ft = femto Tesla or Tesla)


57 MEG s Immunity to EMG Artifact EEG
58 Same Time Epoch as EEG on Previous Slide MEG
59 Patient with multiple implants 20 y.o. RH female with seizure onset age 13 Three seizure types: Dialeptic right version right arm tonic GTC Bilateral limb myoclonus Generalized myoclonic with eye blinking and shoulder shrugging S / P VNS implantation 2 yrs ago with no benefit Scalp VEEG: Interictal and ictal discharges generalized Multiple body piercings, three of which were unremoveable (one in left ear)


60 EEG: Run I: Double banana bipolar EEG


61 MEG without tsss (temporal signal space separation) Left temporal sensors Right temporal sensors


62 MEG with tsss (same time segment with same amplitude scale) Left temporal sensors Right temporal sensors




63 Effect of tsss Noise Cancellation in a Patient with a Left Temporal Spike and a VNS no SSS SSS tsss (Taulu and Simola 2006: Jin, Burgess et al 2012)
64 Myth #2: MEG only records interictal epileptic activity While MEG has been found most suitable for evaluation of interictal activity, as noted above, ictal MEG recordings have been made --- frequently serendipitously. Despite the obliteration of the MEG signal by movement artifact during an ictus, a sizable proportion of focal seizures are manifest by EEG/MEG activity for many seconds (typically 5-20) prior to any clinical movements, or even without any movements (patients with frequent auras). These recordings of ictal onset by MEG can yield precise localization of the epileptogenic zone.


65 Ictal MEG Recording Left temporal gradiometers
66 Ictal MEG studies at Cleveland Clinic All epilepsy patients- Between February 2008 January 2012 Who underwent VEEG and Who also had MEG studies within 6 months 309 total MEGs, 139 inpatients (45%), 170 outpatients 228 positive interictal MEGs 106/139 (76%) inpatients, 122/170 (72%) outpatients I.e. Similar proportion (p = n.s.) 39 ictal MEGs (12.6%) 26 (67%) inpatients and (33%) in outpatients Significantly higher in inpatients 26/139 (19%) than in outpatients 13/170 (8%) p <0.01 Of the 39 ictal MEGs, 25 (64%) localized using SECD Approximately half of which (14 or 56%) were not localizable by VEEG. ( Ito et al. 30 th International Epilepsy Congress, 2013 )
67 What should the referring physician expect from a MEG study? The publication of Clinical Practice Guidelines* has helped to establish referring physicians expectations for a high level of quality in the interpretation and for practical utility from the results. Centers with MEGs are striving to practice according to these guidelines. *Bagic, Knowlton, Rose, Ebersole. CPG #1. J Clin Neurophysiol, Burgess, Funke, Bowyer, Lewine, Kirsch, Bagic. CPG #2. J Clin Neurophysiol, Bagic, Knowlton, Rose, Ebersole. CPG #3. J Clin Neurophysiol, Bagic, Barkley, Rose, Ebersole. CPG #4. J Clin Neurophysiol, 2011.
68 What Can Epileptologists Expect From MEG? A routine and standardized procedure. ACMEGS Clinical Practice Guidelines CPG # 1: Recording and Analysis of Spontaneous Cerebral Activity ACMEGS Clinical Practice Guidelines CPG # 2: Presurgical Functional Brain Mapping Using Magnetic Evoked Fields
69 What Can Epileptologists Expect From MEG? A clear and helpful report. An answer to the clinical question posed. ACMEGS Clinical Practice Guidelines CPG # 3: MEG-EEG Reporting
70 How does MEG help to fill in the gaps in our clinical understanding? MEG is a complementary technique with different sensitivity, i.e. it adds new and unique information. MEG prompts focused re-review of other structural and functional tests. MEG s whole-head coverage fills in the gaps left by other techniques. MEG helps to explain results of other tests when they are surprising and to understand discordant results.
71 Beyond the basics: What might we expect in the future? Noise cancellation Movement compensation Streamlined software Multimodality integration and neuronavigation Analysis of connectivity and other quantitative assessments Replacement for intracranial VEEG monitoring
72 Dipole Sources Coregistered with Surface-Reconstructed MRI MEG dipole sources (blue) Subdural grids (green) Stereotactic EEG electrodes (green) Previous Resection (orange)
73 For Further Information Regarding: MEG Clinical Practice Guidelines Conferences, Courses & Symposia Scientific Information Regarding: Evaluation of Epilepsy Clinical Consultation MEG Testing American Clinical MEG Society Phone: Web: Cleveland Clinic Epilepsy Center Phone: Web: neurological_institute/epilepsy
74
75 Additional slides for Q & A period
76 How is MEG analyzed and interpreted (1) First identify important waveforms (e.g. spikes) By time correlation with EEG? Blindly? From spike detector? Spike!
77 Analysis of MEG Signals (2) Field determination requires computerized calculation Iso-magnetic field map 200fT/step Top view Lt lateral view Rt lateral view
 for search = + Measurement Model Residual (x,y,z)=45.2, 31.7, 8.")
78 Analysis of MEG Signals (3) Source localization dipole modeling Single or multiple dipole modeling most common Iteratively search dipole parameters (location, orientation, current strength) for best fit to the actual field distribution Requires a starting point (initial guess) for search = + Measurement Model Residual (x,y,z)=45.2, 31.7, 8.8 mm Modeled dipole parameters (Q)= 373 nam Goodness of fit = 84.5%
79 Spike Source Estimation (4) --- Solving the Inverse Problem Recording spontaneous MEG activity --- trace mode Typical MEG waveforms from sensors overlying the right central region; an epileptiform spike is outlined.
80 Spike Source Estimation (4) --- Solving the Inverse Problem Topographic view of MEG activity during the bracketed epoch Expanded view of MEG activity at maximally active sensor


81 Analysis of MEG Signals (5) Co-registration to Anatomy Requires 3-dimensional coordinate digitization of surface landmarks Import 3-D MRI
82
83 Ictal MEG Analysis MEG s strength: Time dimension! Example case: Six seizures during MEG recording, 1 clinical seizure and 5 with no clinical signs (NCS).


84 NCS Seizure. MEG: Spike and wave complex, Right parietal sensors Left temporal Right temporal Onset, #5 (MR# )

85 Dipole of #5 (Onset): Right posterior middle frontal gyrus (stable) L CS

86 Clinical Seizure. EEG: Onset, Right centro-parietal, Somatosensory Aura #1 EEG Onset #2 #3 #4 Run I EEG (MR# )


87 Clinical Seizure. MEG: Attenuation -> beta, polyspikes, Right parietal sensors Left temporal Right #1 EEG Onset #2 #3 #4 (MR# )

88 Dipole of #1-1 (early component): Right posterior middle frontal gyrus L CS
89 Dipole of #1-2 (late component): Right precentral gyrus L CS
: Right precentral &")
90 Dipole of #2 (3.3 sec after onset): Right precentral & parietal (unstable) L CS
91 Dipole of #3 (3.9 sec after): Right postcentral (hand and face) (stable) L CS
92 Dipole of #4 (5.2 sec after): Right postcentral (hand and face) (stable) L CS


93 All ICTAL dipoles CS RIGHT Clinical Sz 1 recorded NCS Sz Awake sec 5 recorded (2 dipoles ea The likely reason that one out of the six seizures had clinical manifestations is because of propagation of that seizure from the posterior middle frontal gyrus to the post central gyrus.
94 Subdural Grids and Depth Electrodes
95 Dipoles of NCS Seizures
96 Dipoles of Clinical Seizures
97
98 Does MEG See It All? Study of MEG ability to detect and localize spikes recorded on SEEG 3 simultaneous MEG / SEEG recordings Both TLE and ETLE 30 MEG patients who underwent intracranial recordings after MEG All extratemporal To assess factors which determine concordance between MEG and ICEEG Depth of contacts / sources Amplitude of spikes on intracranial electrodes Tightness of clusters on MEG Dipole orientation Jin, Burgess et al., JES 2010

 Number of Contacts >200 uv: 1 contact (30 SPKs) 2")
99 Simultaneous MEG and SEEG (Case 1) SEEG S1 S2 S3 S4 S5 S6 S7 S1 Depth of contact: Approx. 39 mm Max. Amplitude: ± uv ( ) Number of Contacts >200 uv: 1 contact (30 SPKs) 2 contacts (7 SPKs)
 Magnetometer")
100 Simultaneous MEG and SEEG (Case 1) Magnetometer Gradiometer
 SEEG M1")

101 Simultaneous MEG and SEEG (Case 3) SEEG M1 M2 M3 M4 M5 M6 M7 M8 M9 Q1 Q2 Q3 Q4 Q5 Q6 M9

102 Simultaneous MEG and SEEG (Case 3)
103 Simultaneous MEG and SEEG (Case 3)
104 Summary of 3 Cases CASE Depth of Contact (mm) Average of Max. Amplitude (uv) Number of Contacts >200 uv Detectability (%)
105
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 Modified Combinatorial Nomenclature Montage, Review, and Analysis of High Density EEG Terrence D. Lagerlund, M.D., Ph.D. CP1208045-16 Disclosure Relevant financial relationships None Off-label/investigational
Modified Combinatorial Nomenclature Montage, Review, and Analysis of High Density EEG Terrence D. Lagerlund, M.D., Ph.D. CP1208045-16 Disclosure Relevant financial relationships None Off-label/investigational
Sensitivity of scalp EEG and magnetoencephalography
 Original article Epileptic Disord 0; 5 (): 7- Sensitivity of scalp 0-0 EEG and magnetoencephalography Yosuke Kakisaka,, afeed Alkawadri, Zhong I Wang, ei Enatsu, John C Mosher, Anne-Sophie Dubarry, Andreas
Original article Epileptic Disord 0; 5 (): 7- Sensitivity of scalp 0-0 EEG and magnetoencephalography Yosuke Kakisaka,, afeed Alkawadri, Zhong I Wang, ei Enatsu, John C Mosher, Anne-Sophie Dubarry, Andreas
EMG, EEG, and Neurophysiology in Clinical Practice
 Mayo School of Continuous Professional Development EMG, EEG, and Neurophysiology in Clinical Practice Matthew T. Hoerth, M.D. Ritz-Carlton, Amelia Island, Florida January 29-February 4, 2017 2016 MFMER
Mayo School of Continuous Professional Development EMG, EEG, and Neurophysiology in Clinical Practice Matthew T. Hoerth, M.D. Ritz-Carlton, Amelia Island, Florida January 29-February 4, 2017 2016 MFMER
Est-ce que l'eeg a toujours sa place en 2019?
 Est-ce que l'eeg a toujours sa place en 2019? Thomas Bast Epilepsy Center Kork, Germany Does EEG still play a role in 2019? What a question 7T-MRI, fmri, DTI, MEG, SISCOM, Of ieeg course! /HFO, Genetics
Est-ce que l'eeg a toujours sa place en 2019? Thomas Bast Epilepsy Center Kork, Germany Does EEG still play a role in 2019? What a question 7T-MRI, fmri, DTI, MEG, SISCOM, Of ieeg course! /HFO, Genetics
The Sonification of Human EEG and other Biomedical Data. Part 3
 The Sonification of Human EEG and other Biomedical Data Part 3 The Human EEG A data source for the sonification of cerebral dynamics The Human EEG - Outline Electric brain signals Continuous recording
The Sonification of Human EEG and other Biomedical Data Part 3 The Human EEG A data source for the sonification of cerebral dynamics The Human EEG - Outline Electric brain signals Continuous recording
Benefit of Simultaneous Recording of EEG and MEG in Dipole Localization
 Epilepsia, 43(8):924 928, 2002 Blackwell Publishing, Inc. International League Against Epilepsy Benefit of Simultaneous Recording of EEG and MEG in Dipole Localization *Harumi Yoshinaga, *Tomoyuki Nakahori,
Epilepsia, 43(8):924 928, 2002 Blackwell Publishing, Inc. International League Against Epilepsy Benefit of Simultaneous Recording of EEG and MEG in Dipole Localization *Harumi Yoshinaga, *Tomoyuki Nakahori,
What s the difference between EEG and MEG in practice?
 International Workshop on Advanced Epilepsy Treatment March 28-30, 2009, Kitakyushu, Japan (Invited Talk #2) What s the difference between EEG and MEG in practice? Nobukazu Nakasato, MD, PhD Department
International Workshop on Advanced Epilepsy Treatment March 28-30, 2009, Kitakyushu, Japan (Invited Talk #2) What s the difference between EEG and MEG in practice? Nobukazu Nakasato, MD, PhD Department
EEG source Localization (ESL): What do we know now?
: What do we know now?") EEG source Localization (ESL): What do we know now? Talk overview Theoretical background Fundamental of ESL (forward and inverse problems) Voltage topography of temporal spikes Improving source localization
EEG source Localization (ESL): What do we know now? Talk overview Theoretical background Fundamental of ESL (forward and inverse problems) Voltage topography of temporal spikes Improving source localization
Diagnosing Complicated Epilepsy: Mapping of the Epileptic Circuitry. Michael R. Sperling, M.D. Thomas Jefferson University Philadelphia, PA
 Diagnosing Complicated Epilepsy: Mapping of the Epileptic Circuitry Michael R. Sperling, M.D. Thomas Jefferson University Philadelphia, PA Overview Definition of epileptic circuitry Methods of mapping
Diagnosing Complicated Epilepsy: Mapping of the Epileptic Circuitry Michael R. Sperling, M.D. Thomas Jefferson University Philadelphia, PA Overview Definition of epileptic circuitry Methods of mapping
The American Approach to Depth Electrode Insertion December 4, 2012
 The American Approach to Depth Electrode Insertion December 4, 2012 Jonathan Miller, MD Director, Epilepsy Surgery University Hospitals Case Medical Center/Case Western Reserve University Cleveland, Ohio
The American Approach to Depth Electrode Insertion December 4, 2012 Jonathan Miller, MD Director, Epilepsy Surgery University Hospitals Case Medical Center/Case Western Reserve University Cleveland, Ohio
Subject: Magnetoencephalography/Magnetic Source Imaging
 01-95805-16 Original Effective Date: 09/01/01 Reviewed: 07/26/18 Revised: 08/15/18 Subject: Magnetoencephalography/Magnetic Source Imaging THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION,
01-95805-16 Original Effective Date: 09/01/01 Reviewed: 07/26/18 Revised: 08/15/18 Subject: Magnetoencephalography/Magnetic Source Imaging THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION,
ChosingPhase 2 Electrodes
 ChosingPhase 2 Electrodes ACNS Course ECoG/Invasive EEG Houston, February 4 th, 2015 Stephan Schuele, MD, MPH Comprehensive Epilepsy Center Northwestern Memorial Hospital Northwestern University, Feinberg
ChosingPhase 2 Electrodes ACNS Course ECoG/Invasive EEG Houston, February 4 th, 2015 Stephan Schuele, MD, MPH Comprehensive Epilepsy Center Northwestern Memorial Hospital Northwestern University, Feinberg
Source Imaging in Mapping Eloquent Cortex December 6 th 2011
 Source Imaging in Mapping Eloquent Cortex December 6 th 2011 Samden Lhatoo, MD FRCP University Hospitals Case Medical Center American Epilepsy Society Annual Meeting Disclosure Name of Commercial Interest
Source Imaging in Mapping Eloquent Cortex December 6 th 2011 Samden Lhatoo, MD FRCP University Hospitals Case Medical Center American Epilepsy Society Annual Meeting Disclosure Name of Commercial Interest
Case reports functional imaging in epilepsy
 Seizure 2001; 10: 157 161 doi:10.1053/seiz.2001.0552, available online at http://www.idealibrary.com on Case reports functional imaging in epilepsy MARK P. RICHARDSON Medical Research Council Fellow, Institute
Seizure 2001; 10: 157 161 doi:10.1053/seiz.2001.0552, available online at http://www.idealibrary.com on Case reports functional imaging in epilepsy MARK P. RICHARDSON Medical Research Council Fellow, Institute
Interictal High Frequency Oscillations as Neurophysiologic Biomarkers of Epileptogenicity
 Interictal High Frequency Oscillations as Neurophysiologic Biomarkers of Epileptogenicity December 10, 2013 Joyce Y. Wu, MD Associate Professor Division of Pediatric Neurology David Geffen School of Medicine
Interictal High Frequency Oscillations as Neurophysiologic Biomarkers of Epileptogenicity December 10, 2013 Joyce Y. Wu, MD Associate Professor Division of Pediatric Neurology David Geffen School of Medicine
Toward a more accurate delimitation of the epileptic focus from a surgical perspective
 Toward a more accurate delimitation of the epileptic focus from a surgical perspective Margitta Seeck Department of Clinical Neurosciences EEG & Epilepsy Unit University Hospital of Geneva Geneva, Switzerland
Toward a more accurate delimitation of the epileptic focus from a surgical perspective Margitta Seeck Department of Clinical Neurosciences EEG & Epilepsy Unit University Hospital of Geneva Geneva, Switzerland
9/30/2016. Advances in Epilepsy Surgery. Epidemiology. Epidemiology
 Advances in Epilepsy Surgery George Jallo, M.D. Director, Institute for Brain Protection Sciences Johns Hopkins All Children s Hospital St Petersburg, Florida Epidemiology WHO lists it as the second most
Advances in Epilepsy Surgery George Jallo, M.D. Director, Institute for Brain Protection Sciences Johns Hopkins All Children s Hospital St Petersburg, Florida Epidemiology WHO lists it as the second most
Physiological and Physical Basis of Functional Brain Imaging 6. EEG/MEG. Kâmil Uludağ, 20. November 2007
 Physiological and Physical Basis of Functional Brain Imaging 6. EEG/MEG Kâmil Uludağ, 20. November 2007 Course schedule 1. Overview 2. fmri (Spin dynamics, Image formation) 3. fmri (physiology) 4. fmri
Physiological and Physical Basis of Functional Brain Imaging 6. EEG/MEG Kâmil Uludağ, 20. November 2007 Course schedule 1. Overview 2. fmri (Spin dynamics, Image formation) 3. fmri (physiology) 4. fmri
PRESURGICAL EVALUATION. ISLAND OF COS Hippocrates: On the Sacred Disease. Disclosure Research-Educational Grants. Patients with seizure disorders
 PRESURGICAL EVALUATION Patients with seizure disorders Gregory D. Cascino, MD Mayo Clinic Disclosure Research-Educational Grants Mayo Foundation Neuro Pace, Inc. American Epilepsy Society American Academy
PRESURGICAL EVALUATION Patients with seizure disorders Gregory D. Cascino, MD Mayo Clinic Disclosure Research-Educational Grants Mayo Foundation Neuro Pace, Inc. American Epilepsy Society American Academy
Faculty/Presenter Disclosure. Intracranial EEG Recording. Objectives. General Themes. Why invasive recordings? 6/27/2018
 CFPC CoI Templates: Slide 1 used in Faculty presentation only. Faculty/Presenter Disclosure Intracranial EEG Recording Faculty: Dr Richard S McLachlan Relationships with financial sponsors: None currently
CFPC CoI Templates: Slide 1 used in Faculty presentation only. Faculty/Presenter Disclosure Intracranial EEG Recording Faculty: Dr Richard S McLachlan Relationships with financial sponsors: None currently
EEG Instrumentation, Montage, Polarity, and Localization
 EEG Instrumentation, Montage, Polarity, and Localization 2 Krikor Tufenkjian The Source of EEG The source of the EEG potentials recorded from the scalp is the excitatory and inhibitory postsynaptic potentials
EEG Instrumentation, Montage, Polarity, and Localization 2 Krikor Tufenkjian The Source of EEG The source of the EEG potentials recorded from the scalp is the excitatory and inhibitory postsynaptic potentials
Diffusion Tensor Imaging 12/06/2013
 12/06/2013 Beate Diehl, MD PhD FRCP University College London National Hospital for Neurology and Neurosurgery Queen Square London, UK American Epilepsy Society Annual Meeting Disclosure None Learning
12/06/2013 Beate Diehl, MD PhD FRCP University College London National Hospital for Neurology and Neurosurgery Queen Square London, UK American Epilepsy Society Annual Meeting Disclosure None Learning
Multimodal Imaging in Extratemporal Epilepsy Surgery
 Open Access Case Report DOI: 10.7759/cureus.2338 Multimodal Imaging in Extratemporal Epilepsy Surgery Christian Vollmar 1, Aurelia Peraud 2, Soheyl Noachtar 1 1. Epilepsy Center, Dept. of Neurology, University
Open Access Case Report DOI: 10.7759/cureus.2338 Multimodal Imaging in Extratemporal Epilepsy Surgery Christian Vollmar 1, Aurelia Peraud 2, Soheyl Noachtar 1 1. Epilepsy Center, Dept. of Neurology, University
Surgery for Medically Refractory Focal Epilepsy
 Surgery for Medically Refractory Focal Epilepsy Seth F Oliveria, MD PhD The Oregon Clinic Neurosurgery Director of Functional Neurosurgery: Providence Brain and Spine Institute Portland, OR Providence
Surgery for Medically Refractory Focal Epilepsy Seth F Oliveria, MD PhD The Oregon Clinic Neurosurgery Director of Functional Neurosurgery: Providence Brain and Spine Institute Portland, OR Providence
Spatial localisation of EEG dipoles in MRI using the International System anatomical references
 Proc. of First Int'l Workshop on Image and Signal Processing and Analysis Spatial localisation of EEG dipoles in MRI using the 10-20 International System anatomical references J. Pascau a,b, M. Desco a,
Proc. of First Int'l Workshop on Image and Signal Processing and Analysis Spatial localisation of EEG dipoles in MRI using the 10-20 International System anatomical references J. Pascau a,b, M. Desco a,
Accepted Manuscript. Editorial. Responsive neurostimulation for epilepsy: more than stimulation. Jayant N. Acharya
 Accepted Manuscript Editorial Responsive neurostimulation for epilepsy: more than stimulation Jayant N. Acharya PII: S2467-981X(18)30022-2 DOI: https://doi.org/10.1016/j.cnp.2018.06.002 Reference: CNP
Accepted Manuscript Editorial Responsive neurostimulation for epilepsy: more than stimulation Jayant N. Acharya PII: S2467-981X(18)30022-2 DOI: https://doi.org/10.1016/j.cnp.2018.06.002 Reference: CNP
Epilepsy: diagnosis and treatment. Sergiusz Jóźwiak Klinika Neurologii Dziecięcej WUM
 Epilepsy: diagnosis and treatment Sergiusz Jóźwiak Klinika Neurologii Dziecięcej WUM Definition: the clinical manifestation of an excessive excitation of a population of cortical neurons Neurotransmitters:
Epilepsy: diagnosis and treatment Sergiusz Jóźwiak Klinika Neurologii Dziecięcej WUM Definition: the clinical manifestation of an excessive excitation of a population of cortical neurons Neurotransmitters:
EEG Source Imaging in Epilepsy Evaluations
 EEG Source Imaging in Epilepsy Evaluations December 6, 2011 Thomas Bast, MD Head of the Department of Children and Adolescents Epilepsy Centre Kork Germany American Epilepsy Society Annual Meeting Disclosure
EEG Source Imaging in Epilepsy Evaluations December 6, 2011 Thomas Bast, MD Head of the Department of Children and Adolescents Epilepsy Centre Kork Germany American Epilepsy Society Annual Meeting Disclosure
Invasive Evaluation for Epilepsy Surgery Lesional Cases NO DISCLOSURES. Mr. Johnson. Seizures at 29 Years of Age. Dileep Nair, MD Juan Bulacio, MD
 Invasive Evaluation for Epilepsy Surgery Lesional Cases NO DISCLOSURES Dileep Nair, MD Juan Bulacio, MD Mr. Johnson Seizures at 29 Years of Age Onset of seizures at 16 years of age bed wetting episodes
Invasive Evaluation for Epilepsy Surgery Lesional Cases NO DISCLOSURES Dileep Nair, MD Juan Bulacio, MD Mr. Johnson Seizures at 29 Years of Age Onset of seizures at 16 years of age bed wetting episodes
Depth/Surface Relationships: Confronting noninvasive measures to intracerebral EEG
 Depth/Surface Relationships: Confronting noninvasive measures to intracerebral EEG Christian G Bénar Institut de Neurosciences des Systèmes; INSERM, Aix-Marseille Université christian.benar@univ-amu.fr
Depth/Surface Relationships: Confronting noninvasive measures to intracerebral EEG Christian G Bénar Institut de Neurosciences des Systèmes; INSERM, Aix-Marseille Université christian.benar@univ-amu.fr
Epilepsy Surgery, Imaging, and Intraoperative Neuromonitoring: Surgical Perspective
 Epilepsy Surgery, Imaging, and Intraoperative Neuromonitoring: Surgical Perspective AC Duhaime, M.D. Director, Pediatric Neurosurgery, Massachusetts General Hospital Professor, Neurosurgery, Harvard Medical
Epilepsy Surgery, Imaging, and Intraoperative Neuromonitoring: Surgical Perspective AC Duhaime, M.D. Director, Pediatric Neurosurgery, Massachusetts General Hospital Professor, Neurosurgery, Harvard Medical
Neurophysiology & EEG
 Neurophysiology & EEG PG4 Core Curriculum Ian A. Cook, M.D. Associate Director, Laboratory of Brain, Behavior, & Pharmacology UCLA Department of Psychiatry & Biobehavioral Sciences Semel Institute for
Neurophysiology & EEG PG4 Core Curriculum Ian A. Cook, M.D. Associate Director, Laboratory of Brain, Behavior, & Pharmacology UCLA Department of Psychiatry & Biobehavioral Sciences Semel Institute for
Early seizure propagation from the occipital lobe to medial temporal structures and its surgical implication
 Original article Epileptic Disord 2008; 10 (4): 260-5 Early seizure propagation from the occipital lobe to medial temporal structures and its surgical implication Naotaka Usui, Tadahiro Mihara, Koichi
Original article Epileptic Disord 2008; 10 (4): 260-5 Early seizure propagation from the occipital lobe to medial temporal structures and its surgical implication Naotaka Usui, Tadahiro Mihara, Koichi
Depth/surface relationships: Confronting noninvasive measures to intracerebral EEG
 Depth/surface relationships: Confronting noninvasive measures to intracerebral EEG Christian G Bénar Institut de Neurosciences des Systèmes; INSERM, Aix-Marseille Université christian.benar@univ-amu.fr
Depth/surface relationships: Confronting noninvasive measures to intracerebral EEG Christian G Bénar Institut de Neurosciences des Systèmes; INSERM, Aix-Marseille Université christian.benar@univ-amu.fr
Magnetoencephalography/Magnetic Source Imaging
 6.01.21 Magnetoencephalography/Magnetic Source Imaging Section 6.0 Radiology Subsection Effective Date February 27, 2015 Original Policy Date June 1, 2004 Next Review Date February 2016 Description Magnetoencephalography
6.01.21 Magnetoencephalography/Magnetic Source Imaging Section 6.0 Radiology Subsection Effective Date February 27, 2015 Original Policy Date June 1, 2004 Next Review Date February 2016 Description Magnetoencephalography
The EEG in focal epilepsy. Bassel Abou-Khalil, M.D. Vanderbilt University Medical Center
 The EEG in focal epilepsy Bassel Abou-Khalil, M.D. Vanderbilt University Medical Center I have no financial relationships to disclose that are relative to the content of my presentation Learning Objectives
The EEG in focal epilepsy Bassel Abou-Khalil, M.D. Vanderbilt University Medical Center I have no financial relationships to disclose that are relative to the content of my presentation Learning Objectives
Stereotactic Electroencephalography (seeg) in the Pre-surgical Investigation of Refractory Focal Epilepsy December 4, 2012
 in the Pre-surgical Investigation of Refractory Focal Epilepsy December 4, 2012") Stereotactic Electroencephalography (seeg) in the Pre-surgical Investigation of Refractory Focal Epilepsy December 4, 2012 Case Hans O. Lűders Epilepsy Center Medical Center, University Hospitals, Cleveland
Stereotactic Electroencephalography (seeg) in the Pre-surgical Investigation of Refractory Focal Epilepsy December 4, 2012 Case Hans O. Lűders Epilepsy Center Medical Center, University Hospitals, Cleveland
Introduction to EEG del Campo. Introduction to EEG. J.C. Martin del Campo, MD, FRCP University Health Network Toronto, Canada
 Introduction to EEG J.C. Martin, MD, FRCP University Health Network Toronto, Canada What is EEG? A graphic representation of the difference in voltage between two different cerebral locations plotted over
Introduction to EEG J.C. Martin, MD, FRCP University Health Network Toronto, Canada What is EEG? A graphic representation of the difference in voltage between two different cerebral locations plotted over
Common Ictal Patterns in Patients with Documented Epileptic Seizures
 THE ICTAL IRAQI PATTERNS POSTGRADUATE IN EPILEPTIC MEDICAL JOURNAL PATIENTS Common Ictal Patterns in Documented Epileptic Seizures Ghaieb Bashar ALJandeel, Gonzalo Alarcon ABSTRACT: BACKGROUND: The ictal
THE ICTAL IRAQI PATTERNS POSTGRADUATE IN EPILEPTIC MEDICAL JOURNAL PATIENTS Common Ictal Patterns in Documented Epileptic Seizures Ghaieb Bashar ALJandeel, Gonzalo Alarcon ABSTRACT: BACKGROUND: The ictal
High Resolution Ictal SPECT: Enhanced Epileptic Source Targeting?
 High Resolution Ictal SPECT: Enhanced Epileptic Source Targeting? Marvin A Rossi MD, PhD RUSH Epilepsy Center Research Lab http://www.synapticom.net Chicago, IL USA Medically-Refractory Epilepsy 500,000-800,000
High Resolution Ictal SPECT: Enhanced Epileptic Source Targeting? Marvin A Rossi MD, PhD RUSH Epilepsy Center Research Lab http://www.synapticom.net Chicago, IL USA Medically-Refractory Epilepsy 500,000-800,000
Intracranial Studies Of Human Epilepsy In A Surgical Setting
 Intracranial Studies Of Human Epilepsy In A Surgical Setting Department of Neurology David Geffen School of Medicine at UCLA Presentation Goals Epilepsy and seizures Basics of the electroencephalogram
Intracranial Studies Of Human Epilepsy In A Surgical Setting Department of Neurology David Geffen School of Medicine at UCLA Presentation Goals Epilepsy and seizures Basics of the electroencephalogram
EPILEPSY SURGERY EVALUATION IN ADULTS WITH SCALP VIDEO-EEG MONITORING. Meriem Bensalem-Owen, MD University of Kentucky
 EPILEPSY SURGERY EVALUATION IN ADULTS WITH SCALP VIDEO-EEG MONITORING Meriem Bensalem-Owen, MD University of Kentucky DISCLOSURES Received grants for sponsored research as investigator from: UCB Eisai
EPILEPSY SURGERY EVALUATION IN ADULTS WITH SCALP VIDEO-EEG MONITORING Meriem Bensalem-Owen, MD University of Kentucky DISCLOSURES Received grants for sponsored research as investigator from: UCB Eisai
Advanced Imaging Techniques MRI, PET, SPECT, ESI-MSI, DTI December 8, 2013
 Advanced Imaging Techniques MRI, PET, SPECT, ESI-MSI, DTI December 8, 2013 Robert C. Knowlton, MD, MSPH University of California San Francisco Seizure Disorders Surgical Program American Epilepsy Society
Advanced Imaging Techniques MRI, PET, SPECT, ESI-MSI, DTI December 8, 2013 Robert C. Knowlton, MD, MSPH University of California San Francisco Seizure Disorders Surgical Program American Epilepsy Society
Spike voltage topography in temporal lobe epilepsy
 Thomas Jefferson University Jefferson Digital Commons Department of Neurology Faculty Papers Department of Neurology 5-17-2016 Spike voltage topography in temporal lobe epilepsy Ali Akbar Asadi-Pooya Thomas
Thomas Jefferson University Jefferson Digital Commons Department of Neurology Faculty Papers Department of Neurology 5-17-2016 Spike voltage topography in temporal lobe epilepsy Ali Akbar Asadi-Pooya Thomas
(Electric) Source Analysis Kanjana Unnwongse, MD
 Source Analysis Kanjana Unnwongse, MD") (Electric) Source Analysis Kanjana Unnwongse, MD Ruhr Epileptologie, Universtitätsklinikum Knappschaftskrankenhaus Bochum 1 What is source analysis? Source analysis or electric and magnetic source imaging
(Electric) Source Analysis Kanjana Unnwongse, MD Ruhr Epileptologie, Universtitätsklinikum Knappschaftskrankenhaus Bochum 1 What is source analysis? Source analysis or electric and magnetic source imaging
Automated detection of abnormal changes in cortical thickness: A tool to help diagnosis in neocortical focal epilepsy
 Automated detection of abnormal changes in cortical thickness: A tool to help diagnosis in neocortical focal epilepsy 1. Introduction Epilepsy is a common neurological disorder, which affects about 1 %
Automated detection of abnormal changes in cortical thickness: A tool to help diagnosis in neocortical focal epilepsy 1. Introduction Epilepsy is a common neurological disorder, which affects about 1 %
AMERICAN BOARD OF CLINICAL NEUROPHYSIOLOGY
 AMERICAN BOARD OF CLINICAL NEUROPHYSIOLOGY Part I Content Outline I. Physiology and Instrumentation 30% A. Physiology 1. Anatomy of neural generation 2. Mechanisms of EEG and evoked potential generation
AMERICAN BOARD OF CLINICAL NEUROPHYSIOLOGY Part I Content Outline I. Physiology and Instrumentation 30% A. Physiology 1. Anatomy of neural generation 2. Mechanisms of EEG and evoked potential generation
Elekta Neuromag TRIUX State-of-the-art Magnetoencephalography. The next level in functional mapping
 Elekta Neuromag TRIUX State-of-the-art Magnetoencephalography The next level in functional mapping The Path to the Future of MEG Starts Here As the leader in MEG technology, Elekta is pleased to introduce
Elekta Neuromag TRIUX State-of-the-art Magnetoencephalography The next level in functional mapping The Path to the Future of MEG Starts Here As the leader in MEG technology, Elekta is pleased to introduce
Clinical Policy: Digital EEG Spike Analysis
 Clinical Policy: Reference Number: CP.MP.105 Last Review Date: 01/18 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory and legal information. Description
Clinical Policy: Reference Number: CP.MP.105 Last Review Date: 01/18 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory and legal information. Description
A reappraisal of secondary bilateral synchrony
 Neurology Asia 2007; 12 : 29 35 A reappraisal of secondary bilateral synchrony Liri JIN MD, PhD Department of Neurology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing,
Neurology Asia 2007; 12 : 29 35 A reappraisal of secondary bilateral synchrony Liri JIN MD, PhD Department of Neurology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing,
Electroencephalography
 The electroencephalogram (EEG) is a measure of brain waves. It is a readily available test that provides evidence of how the brain functions over time. The EEG is used in the evaluation of brain disorders.
The electroencephalogram (EEG) is a measure of brain waves. It is a readily available test that provides evidence of how the brain functions over time. The EEG is used in the evaluation of brain disorders.
The neurolinguistic toolbox Jonathan R. Brennan. Introduction to Neurolinguistics, LSA2017 1
 The neurolinguistic toolbox Jonathan R. Brennan Introduction to Neurolinguistics, LSA2017 1 Psycholinguistics / Neurolinguistics Happy Hour!!! Tuesdays 7/11, 7/18, 7/25 5:30-6:30 PM @ the Boone Center
The neurolinguistic toolbox Jonathan R. Brennan Introduction to Neurolinguistics, LSA2017 1 Psycholinguistics / Neurolinguistics Happy Hour!!! Tuesdays 7/11, 7/18, 7/25 5:30-6:30 PM @ the Boone Center
PET and SPECT in Epilepsy
 PET and SPECT in Epilepsy 12.6.2013 William H Theodore MD Chief, Clinical Epilepsy Section NINDS NIH Bethesda MD American Epilepsy Society Annual Meeting Disclosures Entity DIR NINDS NIH Elsevier Individual
PET and SPECT in Epilepsy 12.6.2013 William H Theodore MD Chief, Clinical Epilepsy Section NINDS NIH Bethesda MD American Epilepsy Society Annual Meeting Disclosures Entity DIR NINDS NIH Elsevier Individual
EPILEPSY 2018: UPDATE ON MODERN SURGICAL MANAGEMENT. Robert Kellogg, MD Advocate Children s Hospital Park Ridge, IL April 20, 2018
 EPILEPSY 2018: UPDATE ON MODERN SURGICAL MANAGEMENT Robert Kellogg, MD Advocate Children s Hospital Park Ridge, IL April 20, 2018 No disclosures OBJECTIVES Brief history of epilepsy surgery Pre-operative
EPILEPSY 2018: UPDATE ON MODERN SURGICAL MANAGEMENT Robert Kellogg, MD Advocate Children s Hospital Park Ridge, IL April 20, 2018 No disclosures OBJECTIVES Brief history of epilepsy surgery Pre-operative
Research Perspectives in Clinical Neurophysiology
 Research Perspectives in Clinical Neurophysiology A position paper of the EC-IFCN (European Chapter of the International Federation of Clinical Neurophysiology) representing ~ 8000 Clinical Neurophysiologists
Research Perspectives in Clinical Neurophysiology A position paper of the EC-IFCN (European Chapter of the International Federation of Clinical Neurophysiology) representing ~ 8000 Clinical Neurophysiologists
Intracranial EEG Substrates of Scalp EEG Interictal Spikes
 Epilepsia, 46(5):669 676, 2005 Blackwell Publishing, Inc. C 2005 International League Against Epilepsy Intracranial EEG Substrates of Scalp EEG Interictal Spikes James X. Tao, Amit Ray, Susan Hawes-Ebersole,
Epilepsia, 46(5):669 676, 2005 Blackwell Publishing, Inc. C 2005 International League Against Epilepsy Intracranial EEG Substrates of Scalp EEG Interictal Spikes James X. Tao, Amit Ray, Susan Hawes-Ebersole,
Non-lesional Medically-intractable Localization-related Epilepsy Case Presentation December 8, 2013
 Non-lesional Medically-intractable Localization-related Epilepsy Case Presentation December 8, 2013 Jennifer L. DeWolfe, DO Associate Professor of Neurology University of Alabama at Birmingham American
Non-lesional Medically-intractable Localization-related Epilepsy Case Presentation December 8, 2013 Jennifer L. DeWolfe, DO Associate Professor of Neurology University of Alabama at Birmingham American
Latero-Orbital and Anterior-Temporal Electrodes "Their Usefulness in Diagnosing Complex Partial Seizures"
 Mona T. ElGhoneimy et al. LateroOrbital and AnteriorTemporal Electrodes "Their Usefulness in Diagnosing Complex Partial Seizures" Mona T. ElGhoneimy 1, Hanan Hosny 2, Faisal Abdel Wahab 3, Abdel Naser
Mona T. ElGhoneimy et al. LateroOrbital and AnteriorTemporal Electrodes "Their Usefulness in Diagnosing Complex Partial Seizures" Mona T. ElGhoneimy 1, Hanan Hosny 2, Faisal Abdel Wahab 3, Abdel Naser
Dipole Localization for Identification of Neuronal Generators in Independent Neighboring Interictal EEG Spike Foci
 Epilepsia, 42(4):483 490, 2001 Blackwell Science, Inc. International League Against Epilepsy Clinical Research Dipole Localization for Identification of Neuronal Generators in Independent Neighboring Interictal
Epilepsia, 42(4):483 490, 2001 Blackwell Science, Inc. International League Against Epilepsy Clinical Research Dipole Localization for Identification of Neuronal Generators in Independent Neighboring Interictal
Spatial and Temporal Analysis of Interictal Activity in the Epileptic Brain
 Spatial and Temporal Analysis of Interictal Activity in the Epileptic Brain Paul McCall, Mercedes Cabrerizo, Malek Adjouadi Florida International University Department of ECE Miami, FL, USA Email: {pmcca,
Spatial and Temporal Analysis of Interictal Activity in the Epileptic Brain Paul McCall, Mercedes Cabrerizo, Malek Adjouadi Florida International University Department of ECE Miami, FL, USA Email: {pmcca,
ESI and fmri of interictal and ictal epileptic discharges
 ESI and fmri of interictal and ictal epileptic discharges Simon Vogrin a,b, Stephan Lau a,b,c, Mark Cook a,b, Jens Haueisen c a Centre for Clinical Neurosciences and Neurological Research, St. Vincent
ESI and fmri of interictal and ictal epileptic discharges Simon Vogrin a,b, Stephan Lau a,b,c, Mark Cook a,b, Jens Haueisen c a Centre for Clinical Neurosciences and Neurological Research, St. Vincent
Connectivity in epilepsy: Characterization of pathological networks on EEG, MEG and intracerebral EEG
 Connectivity in epilepsy: Characterization of pathological networks on EEG, MEG and intracerebral EEG Christian-G. Bénar Institut de Neurosciences des Systèmes, Marseille christian.benar@univ-amu.fr OHBM
Connectivity in epilepsy: Characterization of pathological networks on EEG, MEG and intracerebral EEG Christian-G. Bénar Institut de Neurosciences des Systèmes, Marseille christian.benar@univ-amu.fr OHBM
HST 583 fmri DATA ANALYSIS AND ACQUISITION
 HST 583 fmri DATA ANALYSIS AND ACQUISITION Neural Signal Processing for Functional Neuroimaging Neuroscience Statistics Research Laboratory Massachusetts General Hospital Harvard Medical School/MIT Division
HST 583 fmri DATA ANALYSIS AND ACQUISITION Neural Signal Processing for Functional Neuroimaging Neuroscience Statistics Research Laboratory Massachusetts General Hospital Harvard Medical School/MIT Division
AdvAnced TMS. Research with PowerMAG Products and Application Booklet
 AdvAnced TMS Research with PowerMAG Products and Application Booklet Table of ConTenTs Introduction p. 04 Legend p. 06 Applications» navigated TMS p. 08» clinical Research p. 10» Multi-Modal TMS p. 12»
AdvAnced TMS Research with PowerMAG Products and Application Booklet Table of ConTenTs Introduction p. 04 Legend p. 06 Applications» navigated TMS p. 08» clinical Research p. 10» Multi-Modal TMS p. 12»
Extratemporal Nonlesional Epilepsy: Grids and Strips 11/30/2012
 Extratemporal Nonlesional Epilepsy: Grids and Strips 11/30/2012 Ashesh D. Mehta, M.D., Ph.D. Department of Neurosurgery Hofstra North Shore LIJ School of Medicine American Epilepsy Society Annual Meeting
Extratemporal Nonlesional Epilepsy: Grids and Strips 11/30/2012 Ashesh D. Mehta, M.D., Ph.D. Department of Neurosurgery Hofstra North Shore LIJ School of Medicine American Epilepsy Society Annual Meeting
The Changing Surgical Landscape in Kids
 The Changing Surgical Landscape in Kids December 7, 2013 Howard L. Weiner, MD NYU Langone Medical Center American Epilepsy Society Annual Meeting Disclosure none American Epilepsy Society 2013 Annual Meeting
The Changing Surgical Landscape in Kids December 7, 2013 Howard L. Weiner, MD NYU Langone Medical Center American Epilepsy Society Annual Meeting Disclosure none American Epilepsy Society 2013 Annual Meeting
From Spikes to Ripples: The Evolving and Expanding Role of Electroencephalography in the Diagnosis and Treatment of Epilepsy
 From Spikes to Ripples: The Evolving and Expanding Role of Electroencephalography in the Diagnosis and Treatment of Epilepsy December 3, 2011 Gregory K. Bergey, M.D. Johns Hopkins University School of
From Spikes to Ripples: The Evolving and Expanding Role of Electroencephalography in the Diagnosis and Treatment of Epilepsy December 3, 2011 Gregory K. Bergey, M.D. Johns Hopkins University School of
5/22/2009. Pediatric Neurosurgery Pediatric Neurology Neuroradiology Neurophysiology Neuropathology Neuropsychology
 Current Surgical Treatment Strategies for the Management of Pediatric Epilepsy University of California, San Francisco Department of Neurological Surgery San Francisco, California Kurtis Ian Auguste, M.D.
Current Surgical Treatment Strategies for the Management of Pediatric Epilepsy University of California, San Francisco Department of Neurological Surgery San Francisco, California Kurtis Ian Auguste, M.D.
Practical 3 Nervous System Physiology 2 nd year English Module. Dept. of Physiology, Carol Davila University of Medicine and Pharmacy
 Electroencephalography l h (EEG) Practical 3 Nervous System Physiology 2 nd year English Module Dept. of Physiology, Carol Davila University of Medicine and Pharmacy What is EEG EEG noninvasively records
Electroencephalography l h (EEG) Practical 3 Nervous System Physiology 2 nd year English Module Dept. of Physiology, Carol Davila University of Medicine and Pharmacy What is EEG EEG noninvasively records
EEG workshop. Epileptiform abnormalities. Definitions. Dr. Suthida Yenjun
 EEG workshop Epileptiform abnormalities Paroxysmal EEG activities ( focal or generalized) are often termed epileptiform activities EEG hallmark of epilepsy Dr. Suthida Yenjun Epileptiform abnormalities
EEG workshop Epileptiform abnormalities Paroxysmal EEG activities ( focal or generalized) are often termed epileptiform activities EEG hallmark of epilepsy Dr. Suthida Yenjun Epileptiform abnormalities
Seizure onset can be difficult to asses in scalp EEG. However, some tools can be used to increase the seizure onset activity over the EEG background:
 This presentation was given during the Dianalund Summer School on EEG and Epilepsy, July 24, 2012. The main purpose of this introductory talk is to show the possibilities of improved seizure onset analysis
This presentation was given during the Dianalund Summer School on EEG and Epilepsy, July 24, 2012. The main purpose of this introductory talk is to show the possibilities of improved seizure onset analysis
EEG in the ICU: Part I
 EEG in the ICU: Part I Teneille E. Gofton July 2012 Objectives To outline the importance of EEG monitoring in the ICU To briefly review the neurophysiological basis of EEG To introduce formal EEG and subhairline
EEG in the ICU: Part I Teneille E. Gofton July 2012 Objectives To outline the importance of EEG monitoring in the ICU To briefly review the neurophysiological basis of EEG To introduce formal EEG and subhairline
Outline of Talk. Introduction to EEG and Event Related Potentials. Key points. My path to EEG
 Outline of Talk Introduction to EEG and Event Related Potentials Shafali Spurling Jeste Assistant Professor in Psychiatry and Neurology UCLA Center for Autism Research and Treatment Basic definitions and
Outline of Talk Introduction to EEG and Event Related Potentials Shafali Spurling Jeste Assistant Professor in Psychiatry and Neurology UCLA Center for Autism Research and Treatment Basic definitions and
EEG History. Where and why is EEG used? 8/2/2010
 EEG History Hans Berger 1873-1941 Edgar Douglas Adrian, an English physician, was one of the first scientists to record a single nerve fiber potential Although Adrian is credited with the discovery of
EEG History Hans Berger 1873-1941 Edgar Douglas Adrian, an English physician, was one of the first scientists to record a single nerve fiber potential Although Adrian is credited with the discovery of
Difficult-to-Localize Intractable Focal Epilepsy: An In-Depth Look
 Current Literature In Clinical Science Difficult-to-Localize Intractable Focal Epilepsy: An In-Depth Look Stereoelectroencephalography in the Difficult to Localize Refractory Focal Epilepsy: Early Experience
Current Literature In Clinical Science Difficult-to-Localize Intractable Focal Epilepsy: An In-Depth Look Stereoelectroencephalography in the Difficult to Localize Refractory Focal Epilepsy: Early Experience
Epilepsy. Hyunmi Choi, M.D., M.S. Columbia Comprehensive Epilepsy Center The Neurological Institute. Seizure
 Epilepsy Hyunmi Choi, M.D., M.S. Columbia Comprehensive Epilepsy Center The Neurological Institute Seizure Symptom Transient event Paroxysmal Temporary physiologic dysfunction Caused by self-limited, abnormal,
Epilepsy Hyunmi Choi, M.D., M.S. Columbia Comprehensive Epilepsy Center The Neurological Institute Seizure Symptom Transient event Paroxysmal Temporary physiologic dysfunction Caused by self-limited, abnormal,
EEG in Medical Practice
 EEG in Medical Practice Dr. Md. Mahmudur Rahman Siddiqui MBBS, FCPS, FACP, FCCP Associate Professor, Dept. of Medicine Anwer Khan Modern Medical College What is the EEG? The brain normally produces tiny
EEG in Medical Practice Dr. Md. Mahmudur Rahman Siddiqui MBBS, FCPS, FACP, FCCP Associate Professor, Dept. of Medicine Anwer Khan Modern Medical College What is the EEG? The brain normally produces tiny
Clinical Policy Title: Magnetoencephalography and magnetic source imaging
 Clinical Policy Title: Magnetoencephalography and magnetic source imaging Clinical Policy Number: 09.01.07 Effective Date: January 1, 2015 Initial Review Date: July 16, 2014 Most Recent Review Date: July
Clinical Policy Title: Magnetoencephalography and magnetic source imaging Clinical Policy Number: 09.01.07 Effective Date: January 1, 2015 Initial Review Date: July 16, 2014 Most Recent Review Date: July
Case report. Epileptic Disord 2005; 7 (1): 37-41
: 37-41") Case report Epileptic Disord 2005; 7 (1): 37-41 Periodic lateralized epileptiform discharges (PLEDs) as the sole electrographic correlate of a complex partial seizure Gagandeep Singh, Mary-Anne Wright,
Case report Epileptic Disord 2005; 7 (1): 37-41 Periodic lateralized epileptiform discharges (PLEDs) as the sole electrographic correlate of a complex partial seizure Gagandeep Singh, Mary-Anne Wright,
True Epileptiform Patterns (and some others)
") True Epileptiform Patterns (and some others) a) What is epileptiform b) Some possible surprises c) Classification of generalized epileptiform patterns An epileptiform pattern Interpretative term based
True Epileptiform Patterns (and some others) a) What is epileptiform b) Some possible surprises c) Classification of generalized epileptiform patterns An epileptiform pattern Interpretative term based
Beyond the Basics in EEG Interpretation: Throughout the Life Stages
 Beyond the Basics in EEG Interpretation: Throughout the Life Stages Steve S. Chung, MD, FAAN Chairman, Neuroscience Institute Director, Epilepsy Program Banner University Medical Center University of Arizona
Beyond the Basics in EEG Interpretation: Throughout the Life Stages Steve S. Chung, MD, FAAN Chairman, Neuroscience Institute Director, Epilepsy Program Banner University Medical Center University of Arizona
CHAPTER 6 INTERFERENCE CANCELLATION IN EEG SIGNAL
 116 CHAPTER 6 INTERFERENCE CANCELLATION IN EEG SIGNAL 6.1 INTRODUCTION Electrical impulses generated by nerve firings in the brain pass through the head and represent the electroencephalogram (EEG). Electrical
116 CHAPTER 6 INTERFERENCE CANCELLATION IN EEG SIGNAL 6.1 INTRODUCTION Electrical impulses generated by nerve firings in the brain pass through the head and represent the electroencephalogram (EEG). Electrical
Audit and Compliance Department 1
 Introduction to Intraoperative Neuromonitoring An intro to those squiggly lines Kunal Patel MS, CNIM None Disclosures Learning Objectives History of Intraoperative Monitoring What is Intraoperative Monitoring
Introduction to Intraoperative Neuromonitoring An intro to those squiggly lines Kunal Patel MS, CNIM None Disclosures Learning Objectives History of Intraoperative Monitoring What is Intraoperative Monitoring
Approximately 70% of childhood SURGICAL TREATMENTS FOR PEDIATRIC EPILEPSY PROCEEDINGS. Ronald P. Lesser, MD KEY POINTS
 ASIM May p153-158 5/14/01 9:19 AM Page 153 SURGICAL TREATMENTS FOR PEDIATRIC EPILEPSY Ronald P. Lesser, MD KEY POINTS Most children with epilepsy refractory to drugs can improve with surgery Temporal lobe
ASIM May p153-158 5/14/01 9:19 AM Page 153 SURGICAL TREATMENTS FOR PEDIATRIC EPILEPSY Ronald P. Lesser, MD KEY POINTS Most children with epilepsy refractory to drugs can improve with surgery Temporal lobe
Magnetoencephalography
 Scan for mobile link. Magnetoencephalography Magnetoencephalography (MEG) is a non-invasive medical test that measures the magnetic fields produced by your brain s electrical currents. It is performed
Scan for mobile link. Magnetoencephalography Magnetoencephalography (MEG) is a non-invasive medical test that measures the magnetic fields produced by your brain s electrical currents. It is performed
Hamartomas and epilepsy: clinical and imaging characteristics
 Seizure 2003; 12: 307 311 doi:10.1016/s1059 1311(02)00272-8 Hamartomas and epilepsy: clinical and imaging characteristics B. DIEHL, R. PRAYSON, I. NAJM & P. RUGGIERI Departments of Neurology, Pathology
Seizure 2003; 12: 307 311 doi:10.1016/s1059 1311(02)00272-8 Hamartomas and epilepsy: clinical and imaging characteristics B. DIEHL, R. PRAYSON, I. NAJM & P. RUGGIERI Departments of Neurology, Pathology
Scalp EEG Findings in Temporal Lobe Epilepsy
 Scalp EEG Findings in Temporal Lobe Epilepsy Seyed M Mirsattari M.D., Ph.D., F.R.C.P.(C) Assistant Professor Depts. of CNS, Medical Biophysics, Medical Imaging, and Psychology University of Western Ontario
Scalp EEG Findings in Temporal Lobe Epilepsy Seyed M Mirsattari M.D., Ph.D., F.R.C.P.(C) Assistant Professor Depts. of CNS, Medical Biophysics, Medical Imaging, and Psychology University of Western Ontario
COGNITIVE SCIENCE 17. Peeking Inside The Head. Part 1. Jaime A. Pineda, Ph.D.
 COGNITIVE SCIENCE 17 Peeking Inside The Head Part 1 Jaime A. Pineda, Ph.D. Imaging The Living Brain! Computed Tomography (CT)! Magnetic Resonance Imaging (MRI)! Positron Emission Tomography (PET)! Functional
COGNITIVE SCIENCE 17 Peeking Inside The Head Part 1 Jaime A. Pineda, Ph.D. Imaging The Living Brain! Computed Tomography (CT)! Magnetic Resonance Imaging (MRI)! Positron Emission Tomography (PET)! Functional
Supplementary Figure 2. Inter discharge intervals are consistent across electrophysiological scales and are related to seizure stage.
 Supplementary Figure 1. Progression of seizure activity recorded from a microelectrode array that was not recruited into the ictal core. (a) Raw LFP traces recorded from a single microelectrode during
Supplementary Figure 1. Progression of seizure activity recorded from a microelectrode array that was not recruited into the ictal core. (a) Raw LFP traces recorded from a single microelectrode during
Magnetoencephalography/Magnetic Source Imaging
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
EEG Wave of the Future: The Video-EEG and fmri Suite?
 Current Literature In Clinical Science EEG Wave of the Future: The Video-EEG and fmri Suite? Mapping Preictal and Ictal Haemodynamic Networks Using Video-Electroencephalography and Functional Imaging.
Current Literature In Clinical Science EEG Wave of the Future: The Video-EEG and fmri Suite? Mapping Preictal and Ictal Haemodynamic Networks Using Video-Electroencephalography and Functional Imaging.
Pediatric Epilepsy Surgery. W. Donald Shields, MD Emeritus Professor of Neurology and Pediatrics David Geffen School of Medicine at UCLA
 Pediatric Epilepsy Surgery W. Donald Shields, MD Emeritus Professor of Neurology and Pediatrics David Geffen School of Medicine at UCLA PEDIATRIC EPILEPSY SURGERY A THING OF BEAUTY IF DONE RIGHT PEDIATRIC
Pediatric Epilepsy Surgery W. Donald Shields, MD Emeritus Professor of Neurology and Pediatrics David Geffen School of Medicine at UCLA PEDIATRIC EPILEPSY SURGERY A THING OF BEAUTY IF DONE RIGHT PEDIATRIC
Northeast Center for Special Care Grant Avenue Lake Katrine, NY
 300 Grant Avenue Lake Katrine, NY 12449 845-336-3500 Information Bulletin What is Brain Mapping? By Victor Zelek, Ph.D., Director of Neuropsychological Services Diplomate, National Registry of Neurofeedback
300 Grant Avenue Lake Katrine, NY 12449 845-336-3500 Information Bulletin What is Brain Mapping? By Victor Zelek, Ph.D., Director of Neuropsychological Services Diplomate, National Registry of Neurofeedback
Clinical Study Integrating Dense Array EEG in the Presurgical Evaluation of Temporal Lobe Epilepsy
 International Scholarly Research Network ISRN Neurology Volume 2012, Article ID 924081, 9 pages doi:10.5402/2012/924081 Clinical Study Integrating Dense Array EEG in the Presurgical Evaluation of Temporal
International Scholarly Research Network ISRN Neurology Volume 2012, Article ID 924081, 9 pages doi:10.5402/2012/924081 Clinical Study Integrating Dense Array EEG in the Presurgical Evaluation of Temporal
Intracranial video-eeg and surgery for focal atonic seizures
 Clinical commentary with video sequences Epileptic Disord 2013; 15 (1): 62-6 Intracranial video-eeg and surgery for focal atonic seizures Martín Donadío, Gabriela Ugarnes, Mónica Segalovich, Naomi rakaki,
Clinical commentary with video sequences Epileptic Disord 2013; 15 (1): 62-6 Intracranial video-eeg and surgery for focal atonic seizures Martín Donadío, Gabriela Ugarnes, Mónica Segalovich, Naomi rakaki,
RIGHT HEMISPHERE LANGUAGE MAPPING USING ELECTROCORTICAL STIMULATION IN PATIENTS WITH BILATERAL LANGUAGE
 RIGHT HEMISPHERE LANGUAGE MAPPING USING ELECTROCORTICAL STIMULATION IN PATIENTS WITH BILATERAL LANGUAGE Rosette A. Jabbour, MD Gail L. Risse, PhD Patricia E. Penovich, MD Frank J. Ritter, MD John R. Gates,
RIGHT HEMISPHERE LANGUAGE MAPPING USING ELECTROCORTICAL STIMULATION IN PATIENTS WITH BILATERAL LANGUAGE Rosette A. Jabbour, MD Gail L. Risse, PhD Patricia E. Penovich, MD Frank J. Ritter, MD John R. Gates,
Seizure Semiology CHARCRIN NABANGCHANG, M.D. PHRAMONGKUTKLAO COLLEGE OF MEDICINE
 Seizure Semiology CHARCRIN NABANGCHANG, M.D. PHRAMONGKUTKLAO COLLEGE OF MEDICINE Seizure Semiology Differentiate between epileptic and nonepileptic seizures Classification of epileptic syndrome Presurgical
Seizure Semiology CHARCRIN NABANGCHANG, M.D. PHRAMONGKUTKLAO COLLEGE OF MEDICINE Seizure Semiology Differentiate between epileptic and nonepileptic seizures Classification of epileptic syndrome Presurgical
Multiple Choice Questions for Part I
 Multiple Choice Questions for Part I 1. Neurons in the cerebral cortex are organized in: A. Three horizontal layers B. Four horizontal layers C. Six horizontal layers with layer IV receiving inputs from
Multiple Choice Questions for Part I 1. Neurons in the cerebral cortex are organized in: A. Three horizontal layers B. Four horizontal layers C. Six horizontal layers with layer IV receiving inputs from
Surgical Management of Post- Traumatic Epilepsy Complexities-Adhesions and Multifocality
 Surgical Management of Post- Traumatic Epilepsy Complexities-Adhesions and Multifocality December 2, 2012 Jeffrey P. Blount MD Division of Neurosurgery University of Alabama at Birmingham Children s of
Surgical Management of Post- Traumatic Epilepsy Complexities-Adhesions and Multifocality December 2, 2012 Jeffrey P. Blount MD Division of Neurosurgery University of Alabama at Birmingham Children s of
The relevance of somatosensory auras in refractory temporal lobe epilepsies
 BRIEF COMMUNICATION The relevance of somatosensory auras in refractory temporal lobe epilepsies Ghazala Perven, Ruta Yardi, Juan Bulacio, Imad Najm, William Bingaman, Jorge Gonzalez-Martinez, and Lara
BRIEF COMMUNICATION The relevance of somatosensory auras in refractory temporal lobe epilepsies Ghazala Perven, Ruta Yardi, Juan Bulacio, Imad Najm, William Bingaman, Jorge Gonzalez-Martinez, and Lara