Updates in Coagulation Thrombophilia testing and direct oral anticoagulants. Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017
|
|
|
- Timothy Walker
- 6 years ago
- Views:
Transcription
1 Updates in Coagulation Thrombophilia testing and direct oral anticoagulants Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017
2 No conflicts of interest
3 Introduction to thrombosis
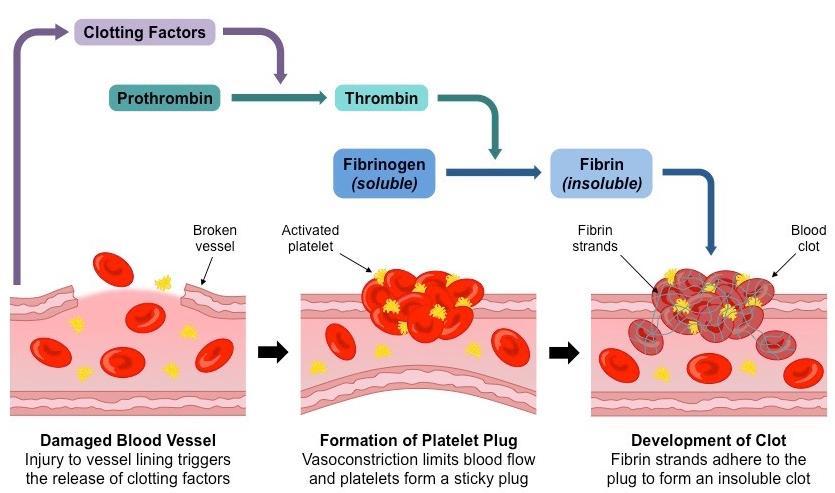
4 Hemostasis
5 Coagulation cascade

6 Virchow s triad
7 Overview of Acute Venous Thromboembolism Annual incidence in U.S. = 1-2/1000 general population Incidence increases dramatically with age >60 Standard therapy (3 or more months of anticoagulation) Decreases the short-term recurrence rate from ~25% to ~3% Associated with major bleeding (~1-2%/year of treatment with warfarin) Recurrence after stopping anticoagulation 1 year 5years Provoked by surgery ~1% ~3% Provoked by non-surgical reversible risk factors ~5% ~15% (e.g., estrogen, pregnancy, leg injury, flight >8 hours) Unprovoked ~10% ~30% Active cancer ~15%/year
8 American College of Chest Physicians 2016 Guidelines for Treatment of VTE Kearon C et al., Chest 2012; 141(2 Suppl): e419s-494s (9 th Edition) Kearon C et al., Chest 2016 Feb; 149(2): (10 th Edition) Graded recommendations for: Proximal lower extremity DVT and PE PE with hypotension Distal lower extremity DVT Superficial venous thrombosis Upper extremity DVT Post-thrombotic syndrome Catheter-associated thrombosis Splanchnic and hepatic vein thrombosis Chronic thromboembolic pulmonary hypertension Recommendations Strong (Grade 1) Weak (Grade 2) Evidence High-quality (Grade A) Moderate-quality (Grade B) Low-quality (Grade C)
9 Acute Proximal DVT or PE Initial Treatment For initial treatment with heparin, suggest LMWH or fondaparinux over IV unfractionated heparin (IV UFH preferred in patients with severe renal failure or those undergoing thrombolysis) If using warfarin, initiate therapy on day 1 Continue parenteral AC for 5 days and until the INR 2.0 for 24 h IVC filter Use only in patients with a contraindication to anticoagulation Begin a conventional course of AC if the risk of bleeding resolves (A permanent IVC filter is no longer considered to be an indication for extended AC) Grade 2B/2C 1B 1B 2B
10 Acute Proximal DVT or PE Choice of Anticoagulant VTE and no cancer Suggest a DOAC over warfarin * In patients not treated with a DOAC, suggest warfarin over LMWH (target INR for all treatment durations) VTE and active cancer Suggest LMWH over warfarin or a DOAC * VTE and pregnancy Suggest LMWH over UFH (warfarin is teratogenic, esp. 1 st TM) Discontinue 24 h prior to induction or C-section Grade 2B 2C 2C 1B 1B * new in 2016 guidelines * new in 2016 guidelines
11 Duration of Treatment for Acute VTE Depends on estimation of: (1) Risk of recurrence ~1%/y ~15%/y (2) Risk of bleeding Provoked by surgery Provoked by non-surgical reversible risk (e.g., estrogen, pregnancy, leg injury, flight >8 hours) First unprovoked VTE Active cancer/ Second unprovoked VTE
12 Estimation of Bleeding Risk (not validated prospectively) Risk factors Age >65 Age >75 Previous bleeding Cancer Metastatic cancer Renal failure Liver failure Thrombocytopenia Previous stroke Diabetes Anemia Antiplatelet therapy Poor anticoagulant control Comorbidity and reduced functional capacity Recent surgery Frequent falls Alcohol abuse NSAID use (added in 2016) Bleeding Risk Low factors 0 risk Moderate 1 risk factor High factors 2 risk
13 Estimation of Bleeding Risk Major Bleeding After VTE (most studies assessed risk on warfarin therapy) Initial 3 Months (%) Extended >3 Months (%/y)
14 Acute Proximal DVT or PE Duration of Treatment (symptomatic=incidental) VTE provoked by Surgery Non-surgical transient risk factor 1st unprovoked VTE Low/moderate bleeding risk High bleeding risk 2nd unprovoked VTE Low/moderate bleeding risk High bleeding risk VTE and active cancer Low/moderate bleeding risk High bleeding risk VTE during pregnancy 3 months 3 months Indefinite 3 months Indefinite 3 months Indefinite Indefinite Continue until 6 wk postpartum (3 mo minimum) Grade 1B 1B 2B 1B 1B/2B 2B 1B 2B 2C
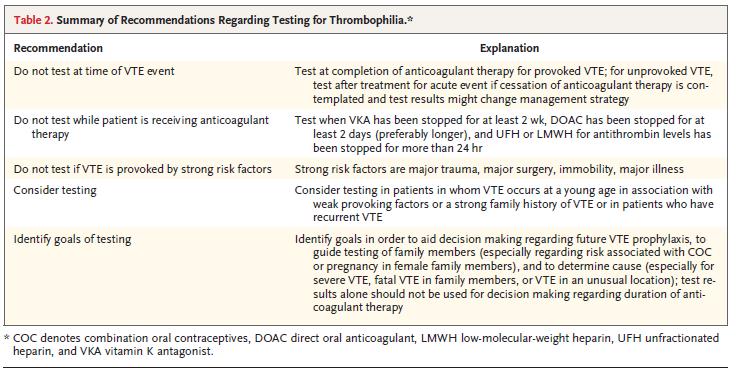
15 Hypercoagulable work up Although inherited and acquired thrombophilias are acknowledged to increase the risk of VTE, the majority of patients should not be tested for thrombophilia. Some arguing that these tests should never be performed. NEJM, Connors, 2017
16 570 patients with first VTE followed prospectively 85% had thrombophilia testing (after anticoagulation stopped) Recurrence rate 11% Recurrence rate not related to inherited thrombophilia status: Hazard ratio 1.5 ( )

17 Case control study of 197 patients who had recurrence after first VTE and 324 control patients Primary endpoint: Odds ratio of recurrent thrombosis based on those tested and those not tested J Thromb Haemost 2008;6:1474
18 What are the issues with testing? No data supporting benefit of testing to guide secondary or primary prophylaxis Results may not alter management Negative testing does not equate low risk Current tests are insufficient Accuracy of some testing is dependent on timing
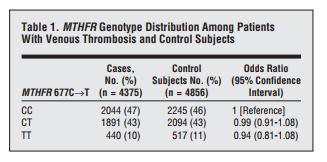
 PAI-1 promoter polymorphism MTHFR polymorphism (677C- >T, 1298A->C) NEJM, Connors,")
19 Other testing: MPN testing (JAK2, CALR, MPL, BCR-ABL) PNH testing (FLAER) Elevated Factor VIII Elevated Factor IX Elevated Factor XI Elevated plasminogen activator inhibitor -1 (PAI-1) PAI-1 promoter polymorphism MTHFR polymorphism (677C- >T, 1298A->C) NEJM, Connors, 2017
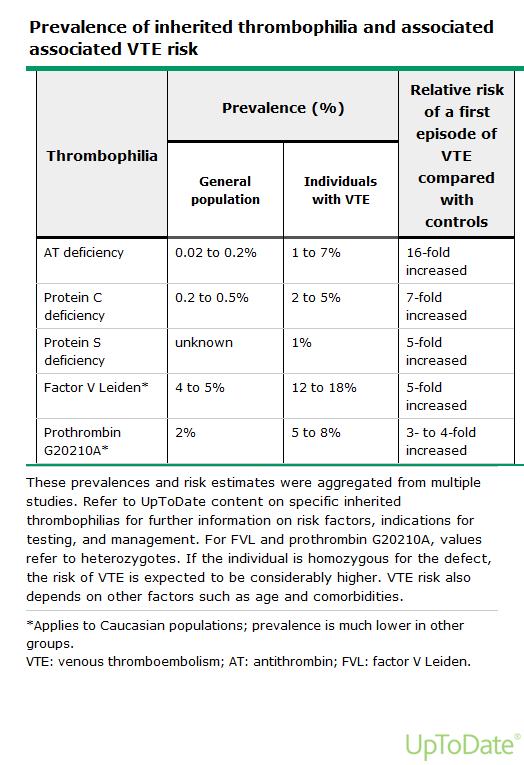
20 Inherited thrombophila

21 Clinical characteristics NEJM, Connors, 2017
22

23 Antiphospholipid antibody syndrome NEJM, Connors, 2017

24 Inherited thrombophila and pregnancy
25 Recommendations
26 Clinical scenarios A 33 year old male with no medical problems suffers a fractured femur playing football. He has surgery, but 1 week later develops calf swelling and is found to have a DVT. His 65 year old mother was recently found to have PE and was diagnosed with breast cancer.
27 Clinical scenarios A 23 year old with 2 younger sisters develops a DVT while 28 weeks pregnant. Her mother had a spontaneous PE when she was in her 30s.
28 Clinical scenarios A 36 year old female in her usual state of health is admitted into the ICU and found to have bilateral PE. She has a depressed EF and is given thrombolytics. Her aunt also had DVTs in her thirties
29 Algorithm for testing


30 854 patients randomized to limited cancer screening vs limited cancer screening with body CT Cancer detection: 3.2% vs 4.5% Cancers missed: 4 vs 5 Time to cancer diagnosis: 4.2mos vs 4.0mos Cancer related mortality: 1.4% vs 0.9%
 - A: Age < 50 (+1) - S: Male (+1) - H: Hormone use (-2) Annual risk of recurrence 1 or less: 2.")
31 1818 patient with unprovoked DVT treated with coumadin Cox regression to determine factors for recurrence DASH SCORE - D: post-anticoagulation D-Dimer (+2) - A: Age < 50 (+1) - S: Male (+1) - H: Hormone use (-2) Annual risk of recurrence 1 or less: 2.1% 2: 6.4% 3+: 12.3%

32 3365 patients with VTE and had completed 6-12 months of treatment randomized to 20mg rivaroxaban, 10mg rivaroxaban, 100mg ASA Primary outcome recurrent VTE, safety outcome of major bleeding
33 Recurrent VTE - 20mg (1.5%) - 10mg (1.2%) - ASA (4.4%) Major Bleeding - 20mg (0.5%) - 10mg (0.4%) - ASA (0.3%) Non major bleeding - 20mg (2.7%) - 10mg (2.0%) - ASA (1.8%)
34 Take home points Thrombophilia testing is often not indicated May be clinically relevant in select patients (especially APLAB) Testing should not be done at time of acute event Clinical factors more relevant for duration of anti-coagulation Consider age appropriate cancer screening Long term low dose anticoagulation may be an option for intermediate risk patients
35 Direct oral anticoagulants If these novel breakthrough oral anticoagulant drugs prove to be effective across the broad spectrum of patients in routine care and are conscientiously priced, the worldwide impact will be huge. NEJM, Hylek, 2010

36 Betrixaban FDA approved 2017
37 Direct Oral Anticoagulants Bind reversibly to the catalytic sites of their target proteases Thrombin Factor Xa In vivo Rivaroxaban Apixaba n Dabigatran etexilate (prodrug) Dabigatran (active drug) Edoxaban

38 Coagulation cascade Anthrombin mediated inhibitor of Xa, Iia - UFH - LMWH - Fondaparinaux Vitamin K Antagonist - Warfarin Direct thrombin inhibitor - Argatroban - Bivalrudin - Dabigatran Factor Xa inhibitor - Rivaroxaban - Apixaban - Edoxaban - Betrixiban
39
40 Direct Oral Anticoagulants Dabigatran (Pradaxa) Rivaroxaban (Xarelto) Apixaban (Eliquis) Edoxaban (Savaysa) Target Thrombin Xa Xa Xa Bioavailability 7% 80% (with food) 60% 60% Peak action hours 2-4 hours 1-3 hours 1-2 hours Half-life hours 7-12 hours 8-15 hours hours Renal clearance Interactions Dosing Initial parenteral anticoagulation 80% 33% 25% 50% P-gp Twice daily 5-10 days of heparin/lmwh P-gp CYP3A4 Twice then once daily None P-gp CYP3A4 Twice daily None P-gp Once daily 5-10 days of heparin/lmwh Monitoring None None None None
41 Dabigatran Dose Stroke prevention in A fib: mg bid 110 mg dose not available in US For patients with CrCl 15-30: 75 mg bid Not recommended for CrCl < 15 or dialysis dependent Postop VTE prophylaxis*: mg once daily VTE treatment/prevention of recurrent VTE: 150 mg bid (following LMWH or heparin Rx) Less than 10% absorbed; relatively high rate of GI side effects Crosses the placenta do not use during pregnancy Drug may degrade over time after exposure to air must be kept in original packaging
42 Rivaroxaban Dose: Stroke prevention in nonvalvular Afib: mg once daily Post op VTE prophylaxis: 10 mg once daily Acute VTE treatment: 15 mg twice daily Secondary prevention of VTE: 20 mg once daily or 10mg daily after 6 months Acute coronary syndrome*: mg twice daily Use with caution in moderate renal impairment (CrCL 30-49); 15 mg/day dose recommended Avoid use if CrCl < 30 (not dialyzable) Avoid use in severe liver disease
43 Apixaban Dose: Stroke prevention in nonvalvular Afib: 5 mg bid 2.5 mg bid if age >80, weight < 60 kg, or serum creatinine > 1.5 Post op VTE prophylaxis: 2.5 mg bid Treatment of acute VTE: 10 mg bid x 7 days, then 5 mg bid Secondary prevention of VTE: 2.5 mg bid after 6 months Lowest dependence on renal excretion of new agents Avoid use in severe liver disease (75% biliary excretion)
44 Edoxaban Dose: Stroke prevention in Afib: 60 mg/d 30 mg/d if CrCl or body wt 60 kg Post op VTE prophylaxis*: 30 mg/d Treatment of acute VTE: 60 mg/d (following LMWH or heparin Rx) Avoid use if CrCl > 95 ml/min (excessive excretion decreases efficacy)
45 Betrixaban Dose: VTE (prophylaxis): Oral: 160 mg as a single dose on day 1, followed by 80 mg once daily for 35 to 42 days Reduce betrixaban dose (initial and maintenance) by 50% for patients receiving or starting P- glycoprotein inhibitors (eg, amiodarone, azithromycin, clarithromycin, ketoconazole, verapamil). Severe renal impairment: avoid use

46 Efficacy of DOACs for treatment of acute VTE J Thromb Haemost 2014;12:320

47 Safety of DOACs for treatment of acute VTE J Thromb Haemost 2014;12:320
48 DOACS in atrial fibrillation Dabigatran 150 mg bid Rivaroxaban 20 mg qd Apixaban 5 mg bid Edoxaban 60 mg qd Combined Ruff et al, Lancet 2013

49 DOACs in VTE prophylaxis after total hip arthroplasty Symptomatic VTE Total VTE + All-cause mortality Major bleeding J Thromb Haemost 2014;12:107
50 Non-valvular a fib stroke prophylaxis FDA-approved Indications Dabigatran (Pradaxa) Rivaroxaban (Xarelto) Apixaban (Eliquis) Edoxaban (Savaysa) Betrixaban (Bevyxxa) Initial DVT/PE treatment after 5-10 d heparin Extended-duration DVT/PE treatment Knee replacement VTE prophylaxis Hip replacement VTE prophylaxis Hip fracture VTE prophylaxis after 5-10 d heparin Medical VTE prophylaxis Acute coronary syndrome Heparin-induced thrombocytopenia
51 Drug effects on coagulation tests PT/INR and PTT are relatively insensitive to the effects of DOACs Reagent-dependent results will vary among labs Normal PT and PTT do not rule out significant blood level of DOAC If PT or PTT elevated assume significant blood levels of DOAC Thrombin time very sensitive to dabigatran effect normal TT implies no drug on board Direct Xa inhibitors do not affect TT
52 Monitoring Dabigatran: Modified thrombin time assay (Hemoclot ) Rivaroxaban, apixaban, edoxaban: Anti-Xa activity (similar to LMWH assay) Neither assay FDA-approved or widely available now When to consider measuring drug level: Detect/quantify overdose Screen for drug accumulation (eg, impaired renal or liver function) Assure low drug level prior to surgery Limited usefulness for assessing compliance due to short drug half-lives


53 Reversal agents
54 Data from 12 RCTs of DOACs involving 102,607 patients Risk Ratios Comparing DOACs to Warfarin RR 0.72 [ ] RR 0.53 [ ] RR 0.43 [ ] RR 0.94 [ ] Major bleeding Fatal bleeding Intracranial bleeding Major GI bleeding Blood 2014;124(15):
55 Reversal of Direct Oral Anticoagulants Kaatz et al. Am J Hematol 2012; 87: S141-5 (<2 h) (?) (?)
56 Reversal of Rivaroxaban by 4-factor PCC (50 IU/kg) in Healthy Volunteers Rivaroxaban PT Dabigatran aptt Dabigatran Thrombin time placebo PCC Eerenberg et al. Circulation 2011; 124(14):
57 Idarucizumab (Praxbind) for Dabigatran Reversal Pollack et al., N Engl J Med 2015 Aug 6;373(6): Idarucizumab (Praxbind ) is a monoclonal antibody fragment that binds to dabigatran with high affinity (350x that of thrombin) 5 mg of idarucizumab (2 x 2.5 mg vials) completely reverses the anticoagulant effect of dabigatran when the drug is taken at usual recommended doses This effect occurs within minutes of drug administration and restores normal hemostasis (NEJM 2015; 373:511) Idarucizumab approved by FDA in October 2015
58 503 patients enrolled, 301 uncontrolled bleeding, 202 required urgent procedure Primary end point reversal measure by dilute thrombin time Median maximum percentage reversal was 100% Median time to cessation of bleeding 2.5 hours, median time to procedure 1.6 hours
59 Idarucizumab (Praxbind) for Dabigatran Reversal

 Figures from Nature Medicine 19,")
60 Andexanet alfa for Reversal of Xa Inhibitors Recombinant factor Xa variant Lacks the γ-carboxyglutamic acid domain required for phospholipid binding Alanine substituted for serine in the active site (catalytically inactive) Figures from Nature Medicine 19, (2013)
61 Andexanet alfa for Reversal of Xa Inhibitors Siegal et al., N Engl J Med 2015 Dec 17;373(25): Study Design Healthy volunteers (50-75 years old) housed at a study site for 8 days Apixaban study: 5 mg PO BID x 3.5 days, then Andexanet 400 mg IV bolus +/- 4 mg/min continuous IV infusion for 2 h OR placebo Rivaroxaban study: 20 mg PO QD x 4 days, then Andexanet 800 mg IV bolus +/- 8 mg/min continuous IV infusion for 2 h OR placebo Primary outcome: percent change in anti-factor Xa activity
62 Andexanet alfa for Reversal of Xa Inhibitors Siegal et al., N Engl J Med 2015 Dec 17;373(25): Bolus plus infusion
63 Andexanet alfa for Reversal of Xa Inhibitors Siegal et al., N Engl J Med 2015 Dec 17;373(25): Conclusions Andexanet reversed the anticoagulant activity of apixaban and rivaroxaban within minutes Rapid onset and offset of action (provides flexibility of treatment?) No serious adverse events (1 patient with hives) No antibodies against factor X or Xa detected at 43 days
 39% and 30% (4 hours after infusion complete) Good/excellent clinical hemostasis 12")
64 67 patients with acute major bleeding within 18 hours of receiving anti Xa inhibitor Mean time from ED arrival to rx: 4.8 hours Decrease in antixa activity: 89% and 93% (after bolus, during 2hour infusion) 39% and 30% (4 hours after infusion complete) Good/excellent clinical hemostasis 12 hours after: 79% Thrombotic event rate: 18% at 30 days
65 Transition to DOAC Unfractionated heparin to DOAC: Start DOAC when UFH infusion stopped LMWH to DOAC: Start DOAC 2 h before next scheduled sq dose of LMWH Warfarin to DOAC: When INR < 2.0
66 Transition from DOAC DOAC to parenteral anticoagulant: CrCl >30: start 12 hours after last NOAC dose CrCl <30: start 24 hours after last NOAC dose DOAC to warfarin: CrCl >50: start warfarin 3 days before NOAC stopped CrCl 31-50: start warfarin 2 days before NOAC stopped CrCl 15-30: start warfarin 1 day before NOAC stopped Remember that NOACs can prolong PT/INR
67 Perioperative management Stop DOAC at least 3 drug half-lives prior to surgery Dabigatran: h Rivaroxaban: h Apixaban: h Allow more time if: Age > 75 Impaired renal or liver function High bleeding risk
68 Recurrent VTE While on Anticoagulation Approach to Treatment If recurrence on warfarin or a DOAC Evaluate for true recurrence, compliance, or malignancy Switch to LMWH for at least 1 month * Grade 2C If recurrence on long-term LMWH and patient is compliant Increase dose of LMWH by 25% to 33% * 2C * new in 2016 guidelines
69 Cost per month Rivaroxaban (20 mg/day) : $290 Dabigatran (150 mg bid): $290 Apixaban (5 mg bid): $147 Warfarin (7.5 mg/day): $31
70 Patients selection for DOAC Patients who have unstable INR on warfarin not due to poor compliance Adequate renal & hepatic function No mechanical valve Not pregnant (drugs cross placenta) Not at extremes of weight (can t adjust dose) Not at high risk of lower GI bleeding
Update on Oral Anticoagulants. Dr. Miten R. Patel Cancer Specialists of North Florida Cell
 Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism
 Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DOAC for VTE. Direct Oral Anticoagulants Clint Shedd DNP, FNP-BC Emory University
 DOAC for VTE Direct Oral Anticoagulants Clint Shedd DNP, FNP-BC Emory University No disclosures Direct Oral Anticoagulants Understand VTE and the ACCP s position on it List the DOACs available in the US
DOAC for VTE Direct Oral Anticoagulants Clint Shedd DNP, FNP-BC Emory University No disclosures Direct Oral Anticoagulants Understand VTE and the ACCP s position on it List the DOACs available in the US
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Challenges in Coagulation
 Challenges in Coagulation Michael H. Rosove, MD Clinical Professor of Medicine UCLA Division of Hematology-Oncology April 30, 2016 Vitamin K Deficiency Vitamin K1 source from diet Vitamin K2 source from
Challenges in Coagulation Michael H. Rosove, MD Clinical Professor of Medicine UCLA Division of Hematology-Oncology April 30, 2016 Vitamin K Deficiency Vitamin K1 source from diet Vitamin K2 source from
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015
 Clinical Practice Guideline August 2015") Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
New Anticoagulants Therapies
 New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
New Antithrombotic Agents DISCLOSURE
 New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Direct Oral Anticoagulants
 Direct Oral Anticoagulants Holly Jahn, PharmD, CACP Objectives Identify the FDA approved indications for use, appropriate dosing, and monitoring parameters for each direct oral anticoagulant. Distinguish
Direct Oral Anticoagulants Holly Jahn, PharmD, CACP Objectives Identify the FDA approved indications for use, appropriate dosing, and monitoring parameters for each direct oral anticoagulant. Distinguish
UPDATE ON TREATMENT OF ACUTE VENOUS THROMBOSIS
 UPDATE ON TREATMENT OF ACUTE VENOUS THROMBOSIS Armando Mansilha MD, PhD, FEBVS 16 th National Congress of the Italian Society of Vascular and Endovascular Surgery Bologna, 2017 Disclosure I have the following
UPDATE ON TREATMENT OF ACUTE VENOUS THROMBOSIS Armando Mansilha MD, PhD, FEBVS 16 th National Congress of the Italian Society of Vascular and Endovascular Surgery Bologna, 2017 Disclosure I have the following
Do s and Don t of DOACs DISCLOSURE
 Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Clinical issues which drug for which patient
 Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Clinical Guideline for Anticoagulation in VTE
 Clinical Guideline for Anticoagulation in VTE These clinical guidelines are intended to provide evidence-based recommendations regarding the anticoagulation in patients with DVT and PE. Please note that
Clinical Guideline for Anticoagulation in VTE These clinical guidelines are intended to provide evidence-based recommendations regarding the anticoagulation in patients with DVT and PE. Please note that
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS
 NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
Anticoagulation Task Force
 Anticoagulation Task Force Newest Recommendations Donald Zabriskie, BPharm, MBA, RPh Pharmacy Patient Care Services Cleveland Clinic- Fairview Hospital THE DRUGS THE PERFECT ANTICOAGULANT Oral administration
Anticoagulation Task Force Newest Recommendations Donald Zabriskie, BPharm, MBA, RPh Pharmacy Patient Care Services Cleveland Clinic- Fairview Hospital THE DRUGS THE PERFECT ANTICOAGULANT Oral administration
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY
 ASWAN UNIVERSITY") New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
Oral Anticoagulants Update. Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation
 Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
The DOACs. Update on Anticoagulation 10/20/2017. Dabigatran (Pradaxa ) Rivaroxaban (Xarelto ) Apixaban (Eliquis ) Edoxaban (Savaysa ) Objectives
 Rivaroxaban (Xarelto ) Apixaban (Eliquis ) Edoxaban (Savaysa ) Objectives") Objectives Update on Anticoagulation JEFF REIST PHARMD, BCPS CLINICAL ASSOCIATE PROFESSOR UNIVERSITY OF IOWA COLLEGE OF PHARMACY At the conclusion of this program, the participant should be able to: List
Objectives Update on Anticoagulation JEFF REIST PHARMD, BCPS CLINICAL ASSOCIATE PROFESSOR UNIVERSITY OF IOWA COLLEGE OF PHARMACY At the conclusion of this program, the participant should be able to: List
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS
: COMPARISON AND FREQUENTLY ASKED QUESTIONS") NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
New and old anticoagulants. Anticoagulation Focus on Direct Oral Anticoagulants
 Anticoagulation Focus on Direct Oral Anticoagulants Tzu-Fei Wang, MD Assistant Professor Department of Internal Medicine Division of Hematology The Ohio State University Wexner Medical Center Objectives
Anticoagulation Focus on Direct Oral Anticoagulants Tzu-Fei Wang, MD Assistant Professor Department of Internal Medicine Division of Hematology The Ohio State University Wexner Medical Center Objectives
Reversal Agents for Anticoagulants Understanding the Options. Katisha Vance, MD, FACP Alabama Oncology January 28, 2017
 Reversal Agents for Anticoagulants Understanding the Options Katisha Vance, MD, FACP Alabama Oncology January 28, 2017 Objectives Appropriately recommend reversal agents for Vitamin K antagonists Appropriately
Reversal Agents for Anticoagulants Understanding the Options Katisha Vance, MD, FACP Alabama Oncology January 28, 2017 Objectives Appropriately recommend reversal agents for Vitamin K antagonists Appropriately
10 Key Things the Vascular Community Should Know about the DOACs Heather Gornik, MD, RVT, RPVI
 10 Key Things the Vascular Community Should Know about the DOACs Heather Gornik, MD, RVT, RPVI Cleveland Clinic Heart and Vascular Institute Heather L. Gornik, MD has the following relationships to disclose:
10 Key Things the Vascular Community Should Know about the DOACs Heather Gornik, MD, RVT, RPVI Cleveland Clinic Heart and Vascular Institute Heather L. Gornik, MD has the following relationships to disclose:
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Anticoagulants: Agents, Pharmacology and Reversal
 Anticoagulants: Agents, Pharmacology and Reversal Lori B Heller, M.D. Cardiac Anesthesiology Swedish Heart and Vascular Institute Medical Director, Swedish Blood Management Clinical Instructor, University
Anticoagulants: Agents, Pharmacology and Reversal Lori B Heller, M.D. Cardiac Anesthesiology Swedish Heart and Vascular Institute Medical Director, Swedish Blood Management Clinical Instructor, University
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Reversal of Novel Oral Anticoagulants. Angelina The, MD March 22, 2016
 Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
New Oral Anticoagulants
 New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
Novel Oral An,coagulants: Prac,cal Aspects. Caroline Berube, MD Clinical Associate Professor Division of Hematology November 2015
 Novel Oral An,coagulants: Prac,cal Aspects Caroline Berube, MD Clinical Associate Professor Division of Hematology November 2015 The New Oral An,coagulants (NOACs) The Non VKA Oral An,coagulants (NOACs)
Novel Oral An,coagulants: Prac,cal Aspects Caroline Berube, MD Clinical Associate Professor Division of Hematology November 2015 The New Oral An,coagulants (NOACs) The Non VKA Oral An,coagulants (NOACs)
Professional Practice Minutes December 7, 2016
 Professional Practice Minutes December 7, 2016 **New Opportunity for Patient Education** We can now request the educational videos we want our patients to watch after our visit. Video topics include colon
Professional Practice Minutes December 7, 2016 **New Opportunity for Patient Education** We can now request the educational videos we want our patients to watch after our visit. Video topics include colon
Idarucizumab for Dabigatran Reversal Pollack CV, Reilly PA, Eikelboom J, et al. N Engl J Med 2015; 373(6):
:") Idarucizumab for Dabigatran Reversal Pollack CV, Reilly PA, Eikelboom J, et al. N Engl J Med 2015; 373(6):511-520. Objective: To measure the safety of idarucizumab to reverse dabigatran anticoagulant effects
Idarucizumab for Dabigatran Reversal Pollack CV, Reilly PA, Eikelboom J, et al. N Engl J Med 2015; 373(6):511-520. Objective: To measure the safety of idarucizumab to reverse dabigatran anticoagulant effects
Acute Care: Understanding Direct Oral Anticoagulants (DOACs)
") Acute Care: Understanding Direct Oral Anticoagulants (DOACs) National Conference for Nurse Practitioners (NCNP) October 11, 2017 John Togami, PharmD, PhC Pharmacist Clinician - Outpatient Anticoagulation
Acute Care: Understanding Direct Oral Anticoagulants (DOACs) National Conference for Nurse Practitioners (NCNP) October 11, 2017 John Togami, PharmD, PhC Pharmacist Clinician - Outpatient Anticoagulation
Updates in Management of Venous Thromboembolic Disease
 Updates in Management of Venous Thromboembolic Disease November 7 th 2018 UHN Emergency Conference Susan Jenkins RN(EC) NP-Adult Thrombosis and Hemostasis Program University Health Network Disclosures
Updates in Management of Venous Thromboembolic Disease November 7 th 2018 UHN Emergency Conference Susan Jenkins RN(EC) NP-Adult Thrombosis and Hemostasis Program University Health Network Disclosures
Managing Bleeding in the Patient on DOACs
 Managing Bleeding in the Patient on DOACs Spring 2016 Jean M. Connors, MD Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine, HMS Conflicts
Managing Bleeding in the Patient on DOACs Spring 2016 Jean M. Connors, MD Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine, HMS Conflicts
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT
. Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT") Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Choosing and Managing Direct Oral Anticoagulants (DOACs)
") Choosing and Managing Direct Oral Anticoagulants (DOACs) Ana G. Antun, MD, MSc Assistant Professor, Department of Hematology and Medical Oncology Winship Cancer Institute of Emory University 1 Outline
Choosing and Managing Direct Oral Anticoagulants (DOACs) Ana G. Antun, MD, MSc Assistant Professor, Department of Hematology and Medical Oncology Winship Cancer Institute of Emory University 1 Outline
Treatment Options and How They Work
 Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
The Direct Oral Anticoagulants: Practical Considerations. David Garcia, MD University of Washington Seattle Cancer Care Alliance September 2015
 The Direct Oral Anticoagulants: Practical Considerations David Garcia, MD University of Washington Seattle Cancer Care Alliance September 2015 Disclosure Occasional consultant to : BMS, Pfizer, Daiichi
The Direct Oral Anticoagulants: Practical Considerations David Garcia, MD University of Washington Seattle Cancer Care Alliance September 2015 Disclosure Occasional consultant to : BMS, Pfizer, Daiichi
Warfarin for Long-Term Anticoagulation. Disadvantages of Warfarin. Narrow Therapeutic Window. Warfarin vs. NOACs. Challenges Monitoring Warfarin
 1 2:15 pm The Era of : Selecting the Best Approach to Treatment SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza,
1 2:15 pm The Era of : Selecting the Best Approach to Treatment SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza,
Challenging Anticoagulation Case Studies. Earl J. Hope, M.D. Tower Health Cardiology
 Challenging Anticoagulation Case Studies Earl J. Hope, M.D. Tower Health Cardiology Financial Disclosures Nothing to disclose Objectives: 1. Understand indications for heparin bridging. 2. Recognize the
Challenging Anticoagulation Case Studies Earl J. Hope, M.D. Tower Health Cardiology Financial Disclosures Nothing to disclose Objectives: 1. Understand indications for heparin bridging. 2. Recognize the
Nibal R. Chamoun, Pharm.D., BCPS Clinical Assistant Professor of Pharmacy Practice at the Lebanese American University Clinical Pharmacy Coordinator
 Nibal R. Chamoun, Pharm.D., BCPS Clinical Assistant Professor of Pharmacy Practice at the Lebanese American University Clinical Pharmacy Coordinator at LAUMCRH Review the mechanism of action, indications
Nibal R. Chamoun, Pharm.D., BCPS Clinical Assistant Professor of Pharmacy Practice at the Lebanese American University Clinical Pharmacy Coordinator at LAUMCRH Review the mechanism of action, indications
Tim Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Akron General Medical Center for Family Medicine Professor, Northeast Ohio
 Tim Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Akron General Medical Center for Family Medicine Professor, Northeast Ohio Medical University Objectives 1. 2. 3. 4. Review and discuss
Tim Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Akron General Medical Center for Family Medicine Professor, Northeast Ohio Medical University Objectives 1. 2. 3. 4. Review and discuss
NOACS/DOACS*: COAGULATION TESTS
 NOACS/DOACS*: COAGULATION TESTS OBJECTIVES: To describe the effect of the newer direct oral anticoagulants (DOACs) on laboratory coagulation tests which are widely available: prothrombin time (PT), international
NOACS/DOACS*: COAGULATION TESTS OBJECTIVES: To describe the effect of the newer direct oral anticoagulants (DOACs) on laboratory coagulation tests which are widely available: prothrombin time (PT), international
Drug Use Criteria: Direct Oral Anticoagulants
 Texas Vendor Drug Program Drug Use Criteria: Oral Anticoagulants Publication History 1. Developed March 2017. 2. Revised February 2018. Notes: Information on indications for use or diagnosis is assumed
Texas Vendor Drug Program Drug Use Criteria: Oral Anticoagulants Publication History 1. Developed March 2017. 2. Revised February 2018. Notes: Information on indications for use or diagnosis is assumed
A VENOUS THROMBOEMBOLISM (VTE) TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention
 TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention") A VENOUS THROMBOEMBOLISM (VTE) TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention This handout is a supplemental resource to an educational video activity released on Medscape
A VENOUS THROMBOEMBOLISM (VTE) TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention This handout is a supplemental resource to an educational video activity released on Medscape
Direct Oral Anticoagulants An Update
 Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
New Antithrombotic Agents
 New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
Reversal of direct oral anticoagulants in the patient with GI bleeding. Marc Carrier
 Reversal of direct oral anticoagulants in the patient with GI bleeding Marc Carrier Disclosure Faculty: Dr. Marc Carrier Relationships with commercial interests: Grants/Research Support: Leo Pharma, Bristol
Reversal of direct oral anticoagulants in the patient with GI bleeding Marc Carrier Disclosure Faculty: Dr. Marc Carrier Relationships with commercial interests: Grants/Research Support: Leo Pharma, Bristol
Perioperative Management of the Anticoagulated Patient
 Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Hemostasis and Thrombosis for Primary Care Providers: An Update. Andrew D. Leavitt, MD. May 21, Topic Outline. Direct Oral Anti-Coagulants DOACs
 Hemostasis and Thrombosis for Primary Care Providers: An Update 43 nd Annual Advances in Internal Medicine Andrew D. Leavitt, MD May 21, 2015 Topic Outline Direct Oral Anti-Coagulants DOACs Update and
Hemostasis and Thrombosis for Primary Care Providers: An Update 43 nd Annual Advances in Internal Medicine Andrew D. Leavitt, MD May 21, 2015 Topic Outline Direct Oral Anti-Coagulants DOACs Update and
Appendix IV - Prescribing Guidance for Apixaban
 Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
ASH 2011: Clinically Relevant Highlights Regarding Venous Thromboembolism and Anticoagulation
 ASH 2011: Clinically Relevant Highlights Regarding Venous Thromboembolism and Anticoagulation Stephan Moll Department of Medicine, Division of Hematology-Oncology, University of North Carolina School of
ASH 2011: Clinically Relevant Highlights Regarding Venous Thromboembolism and Anticoagulation Stephan Moll Department of Medicine, Division of Hematology-Oncology, University of North Carolina School of
New Age Anticoagulants: Bleeding Considerations
 Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging
 and advances in peri-procedural interruption of anticoagulation-- Bridging") Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
A place for new oral anticoagulants in medicine: a fast evolving story
 A place for new oral anticoagulants in medicine: a fast evolving story Prof Beverley Hunt MB ChB, FRCP, FRCPath, MD Chair of Thrombosis & Haemostasis, King s College, London Medical Director of Lifeblood:
A place for new oral anticoagulants in medicine: a fast evolving story Prof Beverley Hunt MB ChB, FRCP, FRCPath, MD Chair of Thrombosis & Haemostasis, King s College, London Medical Director of Lifeblood:
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA
 INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
Spontaneous Atrial Fibrillation and Noacs and Reversal agents
 Spontaneous Atrial Fibrillation and Noacs and Reversal agents Laurent Lewkowiez, MD Regional Service Chief, Hospital Cardiology CPMG Cardiac Electrophysiology Educational Goals relationship between atrial
Spontaneous Atrial Fibrillation and Noacs and Reversal agents Laurent Lewkowiez, MD Regional Service Chief, Hospital Cardiology CPMG Cardiac Electrophysiology Educational Goals relationship between atrial
Managing Perioperative Anticoagulation. Edie Shen MD
 Managing Perioperative Anticoagulation Edie Shen MD Anticoagulation VKA Warfarin (Coumadin) DOACs Direct Thrombin Inhibitor Dabigatran (Pradaxa) Factor Xa Inhibitor Rivaroxaban(Xarelto) Apixaban(Eliquis)
Managing Perioperative Anticoagulation Edie Shen MD Anticoagulation VKA Warfarin (Coumadin) DOACs Direct Thrombin Inhibitor Dabigatran (Pradaxa) Factor Xa Inhibitor Rivaroxaban(Xarelto) Apixaban(Eliquis)
New Oral Anticoagulant Drugs in the Prevention of DVT
 New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
Reversal of DOACs Breakthroughs and Their Aftermath
 Reversal of DOACs Breakthroughs and Their Aftermath Geno J Merli, MD, MACP, FSVM, FHM Professor Medicine & Surgery Co-Director Jefferson Vascular Center Sidney Kimmel Medical College Thomas Jefferson University
Reversal of DOACs Breakthroughs and Their Aftermath Geno J Merli, MD, MACP, FSVM, FHM Professor Medicine & Surgery Co-Director Jefferson Vascular Center Sidney Kimmel Medical College Thomas Jefferson University
Obesity, renal failure, HIT: which anticoagulant to use?
 Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
3/25/2016. Objectives for Pharmacists. Stop the Bleeding! New Reversal Agents. Objectives for Pharmacy Technicians. Assessment Pre-test
 Objectives for Pharmacists Stop the Bleeding! New Reversal Agents Gary D Peksa, Pharm.D., BCPS Clinical Pharmacy Specialist, Emergency Medicine Rush University Medical Center Review current strategies
Objectives for Pharmacists Stop the Bleeding! New Reversal Agents Gary D Peksa, Pharm.D., BCPS Clinical Pharmacy Specialist, Emergency Medicine Rush University Medical Center Review current strategies
Thrombosis. Tom DeLoughery, MD FACP. Oregon Health and Sciences University
 Thrombosis Tom DeLoughery, MD FACP Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant Amgen, Alexion What I am Talking About New Anticoagulants
Thrombosis Tom DeLoughery, MD FACP Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant Amgen, Alexion What I am Talking About New Anticoagulants
Oral Anticoagulation Drug Class Prior Authorization Protocol
 Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING
 DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Novel Anticoagulant Drugs. by: Dr. M. Kamandi Fellowship of hematology and Oncology
 Novel Anticoagulant Drugs by: Dr. M. Kamandi Fellowship of hematology and Oncology A-Novel Oral Anticoagulants A drug that is: safe and effective has predictable pharmacology has few drug drug and drug
Novel Anticoagulant Drugs by: Dr. M. Kamandi Fellowship of hematology and Oncology A-Novel Oral Anticoagulants A drug that is: safe and effective has predictable pharmacology has few drug drug and drug
Ischemic and hemorrhagic strokes in the context of the direct acting oral anticoagulants
 Ischemic and hemorrhagic strokes in the context of the direct acting oral anticoagulants Van Hellerslia, PharmD, BCPS, CACP Clinical Assistant Professor Temple University School of Pharmacy Over 4 million
Ischemic and hemorrhagic strokes in the context of the direct acting oral anticoagulants Van Hellerslia, PharmD, BCPS, CACP Clinical Assistant Professor Temple University School of Pharmacy Over 4 million
Duration of Anticoagulant Therapy. Linda R. Kelly PharmD, PhC, CACP September 17, 2016
 Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
Top 5 (or so) Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE
 Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE") Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Oral Anticoagulants Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Oral Anticoagulant - Bevyxxa (betrixaban), Eliquis (apixaban), Pradaxa (dabigatran),
Oral Anticoagulants Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Oral Anticoagulant - Bevyxxa (betrixaban), Eliquis (apixaban), Pradaxa (dabigatran),
Comparison of novel oral anticoagulants (NOACs)
") Comparison of novel oral anticoagulants (NOACs) For guidance for full information refer to individual SPCs available at www.medicines.org.uk Licensed indications for NOACs Prevention of stroke and systemic
Comparison of novel oral anticoagulants (NOACs) For guidance for full information refer to individual SPCs available at www.medicines.org.uk Licensed indications for NOACs Prevention of stroke and systemic
Update on the Management of Cancer Associated VTE
 Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
Nanik Hatsakorzian Pharm.D/MPH
 Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Drug Class Review Newer Oral Anticoagulant Drugs
 Drug Class Review Newer Oral Anticoagulant Drugs Final Original Report May 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
Drug Class Review Newer Oral Anticoagulant Drugs Final Original Report May 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
ADMINISTRATIVE CLINICAL Page 1 of 6
 ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
Reversal of Direct Oral Anticoagulants. Why are we now seeing so many patients on DOACs? Objectives. DOAC: Recurrent VTE. DOAC: Intracranial Bleeding
 Reversal of Direct Oral Anticoagulants Cameron D Griffiths, MD, FRCPC Clinical Assistant Professor Division of Hematology UBC Objectives Review efficacy and safety data for Direct Oral Anticoagulants (DOACs)
Reversal of Direct Oral Anticoagulants Cameron D Griffiths, MD, FRCPC Clinical Assistant Professor Division of Hematology UBC Objectives Review efficacy and safety data for Direct Oral Anticoagulants (DOACs)
The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for
: Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for") The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for Anticoagulation Services Sanford USD Medical Center Sioux Falls,
The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for Anticoagulation Services Sanford USD Medical Center Sioux Falls,
A Cascade of Updates: Hot Topics in Anticoagulation
 A Cascade of Updates: Hot Topics in Anticoagulation Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Golden L. Peters, PharmD, BCPS Associate
A Cascade of Updates: Hot Topics in Anticoagulation Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Golden L. Peters, PharmD, BCPS Associate
Managing Hemorrhagic Complications of Non-Vitamin K Antagonist Oral Anticoagulants
 Managing Hemorrhagic Complications of Non-Vitamin K Antagonist Oral Anticoagulants MICHAEL E. MULLINS MD FAACT FACEP Washington University School Of Medicine Chair, BJH Anticoagulation Subcommittee Chair,
Managing Hemorrhagic Complications of Non-Vitamin K Antagonist Oral Anticoagulants MICHAEL E. MULLINS MD FAACT FACEP Washington University School Of Medicine Chair, BJH Anticoagulation Subcommittee Chair,
Changing the Ambulatory Training Paradigm: The Design and Implementation of an Outpatient Pulmonology Fellowship Curriculum
 Online Data Supplement Changing the Ambulatory Training Paradigm: The Design and Implementation of an Outpatient Pulmonology Fellowship Curriculum Stacey M. Kassutto, C. Jessica Dine, Maryl Kreider, Rupal
Online Data Supplement Changing the Ambulatory Training Paradigm: The Design and Implementation of an Outpatient Pulmonology Fellowship Curriculum Stacey M. Kassutto, C. Jessica Dine, Maryl Kreider, Rupal
BLOOD DISEASE RESEARCH FOUNDATION
 BLOOD DISEASE RESEARCH FOUNDATION BLOOD DISEASE RESEARCH FOUNDATION The mission of Blood Disease Research Foundation is to support hematological research, e.g. by donating grants for thesis work and abstract
BLOOD DISEASE RESEARCH FOUNDATION BLOOD DISEASE RESEARCH FOUNDATION The mission of Blood Disease Research Foundation is to support hematological research, e.g. by donating grants for thesis work and abstract
Emergency Management of Patients on Direct Oral Anticoagulants (DOACs)
") Emergency Management of Patients on Direct Oral Anticoagulants (DOACs) Dr Tina Biss Consultant Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust NE RTC Annual Education Symposium 11 th October
Emergency Management of Patients on Direct Oral Anticoagulants (DOACs) Dr Tina Biss Consultant Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust NE RTC Annual Education Symposium 11 th October
Anticoagulation Overview Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita
 Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Leading the Charge in Anticoagulation Reversal: Benefits, Risks, and Key Factors in Application to the Traumatically Injured Patient
 Leading the Charge in Anticoagulation Reversal: Benefits, Risks, and Key Factors in Application to the Traumatically Injured Patient Emily Hutchison, PharmD BCPS Clinical Pharmacy Specialist, Trauma/Adult
Leading the Charge in Anticoagulation Reversal: Benefits, Risks, and Key Factors in Application to the Traumatically Injured Patient Emily Hutchison, PharmD BCPS Clinical Pharmacy Specialist, Trauma/Adult
A Review of Direct-Acting Oral Anticoagulants (DOACs) and Their Use in Special Populations
 and Their Use in Special Populations") A Review of Direct-Acting Oral Anticoagulants (DOACs) and Their Use in Special Populations Allison Bernard, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics October 25 th,
A Review of Direct-Acting Oral Anticoagulants (DOACs) and Their Use in Special Populations Allison Bernard, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics October 25 th,
Emergent Anticoagulation Reversal
 U N C M E D I C A L C E N T E R G U I D E L I N E Emergent Anticoagulation Reversal I. PURPOSE: The purpose of these instructions is to provide guidelines for the reversal of or management of bleeding
U N C M E D I C A L C E N T E R G U I D E L I N E Emergent Anticoagulation Reversal I. PURPOSE: The purpose of these instructions is to provide guidelines for the reversal of or management of bleeding
Rapid Fire-Top Articles You Need to Know
 Rapid Fire-Top Articles You Need to Know TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Rapid Fire-Top Articles You Need to Know TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Reversal Agents for NOACs (Novel Oral Anticoagulants)
") Reversal Agents for NOACs (Novel Oral Anticoagulants) Current status and future challenges Paul A Reilly, PhD Clinical Research, Boehringer Ingelheim, Inc CSRC Symposium Washington DC Oct 18, 2016 Atrial
Reversal Agents for NOACs (Novel Oral Anticoagulants) Current status and future challenges Paul A Reilly, PhD Clinical Research, Boehringer Ingelheim, Inc CSRC Symposium Washington DC Oct 18, 2016 Atrial
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Heparin-Induced Thrombocytopenia (HIT)
") Heparin-Induced Thrombocytopenia (HIT) Joshua Ononuju, Pharm. D. Owensboro Medical Health Systems Objectives Overview Pathogenesis Risk factors Clinical Presentation and Diagnosis Treatment goals and options
Heparin-Induced Thrombocytopenia (HIT) Joshua Ononuju, Pharm. D. Owensboro Medical Health Systems Objectives Overview Pathogenesis Risk factors Clinical Presentation and Diagnosis Treatment goals and options