Hypoxic-Ischemic Encephalopathy. TW de Witt University of Pretoria Department of Paediatrics Neonatology
|
|
|
- Rosanna Bradford
- 5 years ago
- Views:
Transcription
1 Hypoxic-Ischemic Encephalopathy TW de Witt University of Pretoria Department of Paediatrics Neonatology
2 Background HIE remains a serious condition that causes significant mortality and longterm morbidity.


3 Physiology / Pathology Fetal response to asphyxia illustrating the initial redistribution of blood flow to vital organs. With prolonged asphyxia insult and failure of compensatory mechanisms, cerebral blood flow falls, leading to ischemic brain injury.


4 Patho-physiology (cont.)
5 Frequency HIE is the most important reason why term babies die in South Africa
6 Mortality/Morbidity Grade 3 HIE 80% DIED 20% SEVERE DISABILITIES Data: Pretoria Academic Hospital 2004
7 Guidelines for the diagnosis of HIE. Profound metabolic or mixed acidemia (ph <7) in an umbilical artery blood sample. Persistence of an Apgar score of 0-3 for longer than 5 minutes Neonatal neurologic sequelae (eg, seizures, coma, hypotonia) Multiple organ involvement (eg, kidney, lungs, liver, heart, intestines) However, infants may have experienced asphyxia or brain hypoxia remote from the time of delivery and may have exhibited the signs and symptoms of hypoxic encephalopathy prior to the time of birth and, therefore, may not meet all of the criteria set forth by the AAP and ACOG at birth.
8 Clinical manifestations and course vary depending on hypoxic-ischemic encephalopathy severity.
9 Mild hypoxic-ischemic encephalopathy Muscle tone - slightly increased Deep tendon reflexes - brisk Behavioral abnormalities- poor feeding Irritability excessive crying sleepiness. By 3-4 days of life, the CNS examination become normal.
10 Moderately severe hypoxicischemic encephalopathy Lethargic, hypotonia and diminished deep tendon reflexes. Primitive reflexes sluggish or absent Moro, grasping sucking reflexes Periods of apnea. Seizures within the first 24 hours of life. Full recovery within 1-2 weeks is possible and is associated with a better long-term outcome. An initial period of well-being or mild hypoxic-ischemic encephalopathy may be followed by sudden deterioration, suggesting ongoing brain cell dysfunction, injury, and death; during this period, seizure intensity might increase.
11 Severe hypoxic-ischemic encephalopathy Stupor or coma. No response to any physical stimulus. Breathing irregular, (gasping) and the infant often requires ventilatory support Generalized hypotonia and depressed deep tendon reflexes Neonatal reflexes (eg, sucking, swallowing, grasping, Moro) are absent. Disturbances of ocular motion, such as a skewed deviation of the eyes, nystagmus, bobbing, and loss of "doll's eye" Pupils dilated, fixed, or poorly reactive to light.
12 Severe hypoxic-ischemic encephalopathy (cont.) Seizures - early frequency may increase during the hours after onset. As the injury progresses, seizures subside and the EEG becomes isoelectric or shows a burst suppression pattern. Fontanelle bulge- increasing cerebral edema. Irregularities of heart rate and blood pressure (BP)
13 Infants who survive The level of alertness improves by days 4-5 of life Hypotonia and feeding difficulties persist, requiring tube feeding for weeks to months. Severe CP
14 Multi-organ dysfunction Heart (43-78%): Lungs (71-86%): Renal (46-72%):. Liver (80-85%): GI dysfunction: Hematologic (32-54%): Severely depressed respiratory and cardiac functions and signs of brainstem compression suggest a lifethreatening rupture of the vein of Galen (ie, great cerebral vein) with a hematoma in the posterior cranial fossa.
15 SARNAT CLASSIFICATION or SHANKARAN
16 CAUSES HIE South Africa high incidence of intra-partum asphyxia
17 Diagnosis No specific test can always confirm or exclude a diagnosis of hypoxic-ischemic encephalopathy (HIE) because the diagnosis is made based on the history and physical and neurological examinations. Many of the tests are performed to assess the severity of brain injury and to monitor the functional status of systemic organs. As always, the results of the tests should be interpreted in conjunction with the clinical history and the findings from physical examination.
18 WORK-UP Serum electrolytes Acute tubular necrosis. Polyuria Renal function studies: Serum creatinine levels, and urea. Coagulation system evaluation: prothrombin time, partial thromboplastin time, and fibrinogen levels. ABG: acid-base status hyperoxia and hypoxia as well as hypercapnia and hypocapnia. Cardiac and liver enzymes: degree of hypoxic-ischemic injury
19 Imaging studies MRI is the imaging modality of choice for the diagnosis and follow-up of infants diagnosed with moderate-tosevere hypoxic-ischemic encephalopathy. Not regularly available NICU / SBAH
20 Imaging Studies Cranial ultrasonography: Findings in hypoxic-ischemic encephalopathy may be imprecise. It can reveal intracerebral or intraventricular hemorrhage. Cerebral edema may be evident in the form of decreased ventricular size or indistinct sulci and gyral patterns. Gross structural abnormalities
21 Amplitude-integrated electroencephalography (aeeg) Single-channel a-eeg Discontinuous tracing Burst suppression pattern Continuous low voltage Inactive pattern with no detectable cortical activity Seizures, abrupt rise in both the lower and upper margins
22 Standard EEG Generalized depression varying degrees of superimposed seizures Burst suppression and iso-electric EEG patterns are particularly ominous. Note that large doses of anticonvulsant therapy may alter the EEG findings. Serial EEGs to assess seizure control and evolution of background abnormalities. Repeat EEGs obtained just prior to discharge can be helpful in establishing prognosis. Improvement in the EEG findings over the first week, in conjunction with improvement in the clinical condition, may help predict a better long-term outcome.
23 Special sensory evaluation: Hearing test increased incidence of deafness Retinal and ophthalmic examination for developmental abnormalities of the brain.

24 Bilateral acute infarctions of the frontal lobe

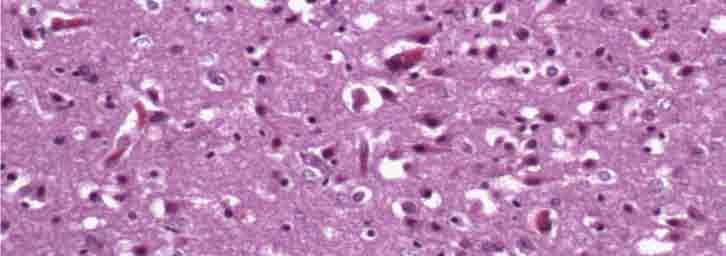
25 Severe acute hypoxicischemic neuronal change

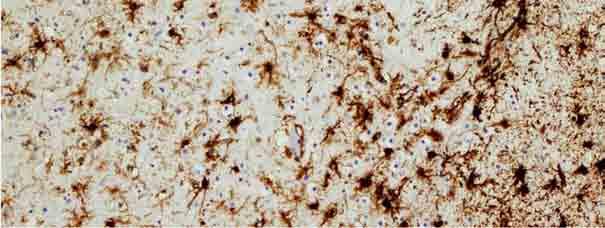
26 Gliosis secondary to the hypoxicischemic event
27 Treatment: Medical Care PREVENTION Obstetric and Neonatal resussitation Supportive care Maintain adequate ventilation Maintain the blood gases and acid-base status in the physiological ranges Maintain adequate perfusion. Maintain the mean blood pressure (BP) above mm Hg (for term infants). Dopamine or dobutamine can be used to maintain adequate cardiac output.
28 Treatment: Medical Care Maintain adequate metabolic status. Fluid and glucose homeostasis Because of the concern for acute tubular necrosis (ATN) insensible water loss (40-60 ml/kg/d in term infant). Avoid hyperthermia.
29 Treatment of seizures Seizures should be treated early and be well controlled because even asymptomatic seizures (ie, seen only on EEG) may continue to injure the brain. Seizures should be treated with phenobarbital or lorazepam; phenytoin may be added if either of these medications fails to control the seizures.
30 Hypothermia treatment Extensive experimental data suggest that mild hypothermia (3-4 C below the baseline temperature) applied within a few hours (no later than 6 h) of hypoxia-ischemia injury is neuro-protective. Therapeutic hypothermia is now the standard of care in neonates with moderate-to-severe hypoxic-ischemic encephalopathy.
31 Hypothermia treatment Near-term infants born at 36 weeks' gestation or less with birth weight of g or less, younger than 6 hours at admission Evidence of acute event around the time of birth Apgar score of 5 or less at 10 minutes after birth (In the study by Shankaran et al, this needed to be in conjunction with either evidence of acute perinatal event or need for assisted ventilation for at least 10 min.13 ) Severe acidosis, defined as ph level of less than 7 or base deficit of 16 mmol/l or less (cord blood or any blood gas obtained within 1 h of birth) Continued need for resuscitation at 10 minutes after birth Evidence of moderate to severe encephalopathy at birth Clinically determined (at least 2) Lethargy, stupor, or coma Abnormal tone or posture Abnormal reflexes (suck, grasp, Moro, gag, stretch reflexes) Decrease or absent spontaneous activity Autonomic dysfunction (including bradycardia, abnormal pupils, apneas) Clinical evidence of seizures Moderately or severely abnormal aeeg background or seizures
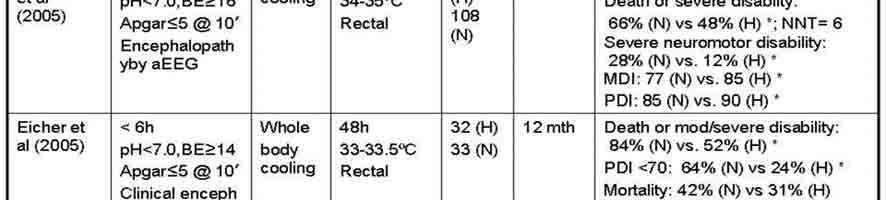

32 Hypothermia studies

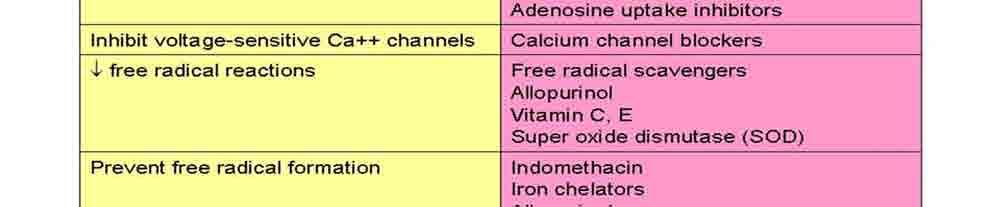

33 Neuro-protective strategies
34 Surgical Care Posterior cranial fossa hematoma- surgical drainage Diet Trophic feeding with expressed breast milk about 5 ml every 3-4 hours if bowel sounds audible. Individualize increments in feeding volume and composition
35 Anticonvulsants These agents are used to control seizures. Phenobarbital Clinical or EEG seizures - continued on the basis of both EEG findings and clinical status. Weaned and stopped during the first month of life if no further convulsions. EEG and clinical status should guide decision.
36 Follow-up Physical therapy and developmental evaluation are needed before discharge. Further Outpatient Care Severely disabled children may need to be monitored in multi-discipility clinics and by a developmental neurologist.
37 Experimental treatment. None has shown consistent efficacy in infants. Alloperinol High dosis Phenobarb
38 Prognosis Accurate prediction of the severity of long-term complications is difficult, although the following pointers may be used: Lack of spontaneous respiratory effort within minutes birth almost always associated with death. of The presence of seizures is an ominous sign. The risk of poor neurological outcome is distinctly greater in such infants, Abnormal clinical neurological findings persisting beyond the first 7-10 days of life usually indicate poor prognosis. Among these, abnormalities of muscle tone and posture (hypotonia, rigidity, weakness) should be carefully noted.
39 Prognosis ( cont.) An EEG done at about 7 days that has normal background activity is a good prognostic sign. Persistent feeding difficulties, which generally are due to abnormal tone of the muscles of sucking and swallowing, also suggest significant CNS damage. Poor head growth during the postnatal period and the first year of life is a sensitive finding predicting higher frequency of neurologic deficits.
40 Medico-legal pitfalls Birth asphyxia, birth injury, and perinatal asphyxia are terms often used incorrectly to describe hypoxic-ischemic encephalopathy (HIE). It is recommend using hypoxic-ischemic encephalopathy because this term accurately describes the clinical condition, encephalopathy from asphyxia, without implying the time of brain injury. Counseling the parents with realistic explanations about their infant's clinical status and prognosis is always recommended. Always document and sign the counseling session.
41 References: American Academy of Pediatrics. Relation between perinatal factors and neurological outcome. In: Guidelines for Perinatal Care. 3rd ed. Elk Grove Village, Ill: American Academy of Pediatrics; 1992: Committee on fetus and newborn, American Academy of Pediatrics and Committee on obstetric practice, American College of Obstetrics and Gynecology. Use and abuse of the APGAR score. Pediatr. 1996;98: [Medline]. Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress: A clinical and electroencphalographic study. Archives of Neur. 1976;33: Badawi N, Kurinczuk JJ, Keogh JM, et al. Antepartum risk factors for newborn encephalopathy: the Western Australian case-control study. British Medical Journal. 1998;317: [Medline]. Gluckman PD, Wyatt JS, Azzopardi D, et al. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicenter randomised trial. Lancet. 2005;365: [Medline]. [Best Evidence] Jacobs S, Hunt R, Tarnow-Mordi W, Inder T, Davis P. Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Rev. 2007;4:CD [Medline]. de Vries LS, Toet MC. Amplitude integrated electroencephalography in the full-term newborn. Clin Perinatol. 2006;33: [Medline].
Birth Asphyxia. Perinatal Depression. Birth Asphyxia. Risk Factors maternal. Risk Factors fetal. Risk Factors Intrapartum 2/12/2011
 Birth Asphyxia Perinatal Depression Sara Brown, ARNP Children s Hospital and Regional Medical Center May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood
Birth Asphyxia Perinatal Depression Sara Brown, ARNP Children s Hospital and Regional Medical Center May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Objectives. Birth Depression Management. Birth Depression Terms
 Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Birth Asphyxia - Summary of the previous meeting and protocol overview
 Birth Asphyxia - Summary of the previous meeting and protocol overview Dr Ornella Lincetto, WHO Geneve Milano, 11June 2007 Vilka är Personality egenskaper med den astrologiska Tvillingarna? Objective of
Birth Asphyxia - Summary of the previous meeting and protocol overview Dr Ornella Lincetto, WHO Geneve Milano, 11June 2007 Vilka är Personality egenskaper med den astrologiska Tvillingarna? Objective of
Perinatal Depression. Lauren Sacco DNP, ARNP Seattle Children s
 Perinatal Depression Lauren Sacco DNP, ARNP Seattle Children s Birth Asphyxia May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood gas exchange that leads
Perinatal Depression Lauren Sacco DNP, ARNP Seattle Children s Birth Asphyxia May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood gas exchange that leads
Running head: THERAPEUTIC HYPOTHERMIA AND TRANSPORT 1
 Running head: THERAPEUTIC HYPOTHERMIA AND TRANSPORT 1 Therapeutic Hypothermia for Neonatal Encephalopathy: Preparation for Transport to Cooling Center Teresa Z. Baker, DNP-S Annie L. Addison, FNP-S NURS
Running head: THERAPEUTIC HYPOTHERMIA AND TRANSPORT 1 Therapeutic Hypothermia for Neonatal Encephalopathy: Preparation for Transport to Cooling Center Teresa Z. Baker, DNP-S Annie L. Addison, FNP-S NURS
Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia. Lauren Sacco DNP, ARNP, NNP-BC
 Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia Lauren Sacco DNP, ARNP, NNP-BC Pathophysiology of HIE Occurs in two energy failure phases: First phase happens during the initial insult
Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia Lauren Sacco DNP, ARNP, NNP-BC Pathophysiology of HIE Occurs in two energy failure phases: First phase happens during the initial insult
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara
 Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
TLC March 27, Shawn Hollinger-Neonatal Fellow CHEO
 TLC March 27, 2013 Presented/Prepared by: Shawn Hollinger, PGY5 Neonatal-Perinatal Medicine Resident - University of Ottawa With slides/images from Dr. Brigitte Lemyre Associate Professor of Pediatrics
TLC March 27, 2013 Presented/Prepared by: Shawn Hollinger, PGY5 Neonatal-Perinatal Medicine Resident - University of Ottawa With slides/images from Dr. Brigitte Lemyre Associate Professor of Pediatrics
Queen Charlotte Hospital
 Queen Charlotte Hospital Neuroprotection for neonatal encephalopathy Neonatal encephalopathy accounts for 1 million deaths worldwide and even greater numbers of disabled survivors In countries with
Queen Charlotte Hospital Neuroprotection for neonatal encephalopathy Neonatal encephalopathy accounts for 1 million deaths worldwide and even greater numbers of disabled survivors In countries with
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on Needed to be resuscitated at birth
 No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
Disclosures. Objectives. Definition: HIE. HIE: Incidence. Impact 9/10/2018. Hypoxic Ischemic Encephalopathy in the Neonate
 Disclosures Hypoxic Ischemic Encephalopathy in the Neonate No relevant financial relationships or conflicts of interest to disclose Franscesca Miquel-Verges MD 2018 Review therapies currently under research
Disclosures Hypoxic Ischemic Encephalopathy in the Neonate No relevant financial relationships or conflicts of interest to disclose Franscesca Miquel-Verges MD 2018 Review therapies currently under research
Wales Neonatal Network Guideline Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling.
 Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
TREATMENT OF HYPOXIC ISCHEMIC ENCEPHALOPATHY WITH COOLING Children s Hospital & Research Center Oakland Guideline Revised by P.
 TREATMENT OF HYPOXIC ISCHEMIC ENCEPHALOPATHY WITH COOLING Children s Hospital & Research Center Oakland Guideline Revised 05-13-13 by P. Joe SCREENING FOR POTENTIAL COOLING PATIENTS Patients who are >
TREATMENT OF HYPOXIC ISCHEMIC ENCEPHALOPATHY WITH COOLING Children s Hospital & Research Center Oakland Guideline Revised 05-13-13 by P. Joe SCREENING FOR POTENTIAL COOLING PATIENTS Patients who are >
This lecture will provide an overview of the neurologic exam of a neonate in the context of clinical cases.
 A11a Neuro Nuggets from the Trenches Michael D. Weiss, MD Associate Professor Department of Pediatrics, Division of Neonatology University of Florida, Gainesville, FL The speaker has signed a disclosure
A11a Neuro Nuggets from the Trenches Michael D. Weiss, MD Associate Professor Department of Pediatrics, Division of Neonatology University of Florida, Gainesville, FL The speaker has signed a disclosure
Inclusion criteria for cooling: Babies should be assessed for 3 criteria: A, B and C. See Appendix 1 for a decision making flowchart.
 Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Neonatal Therapeutic Hypothermia. A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi
 Neonatal Therapeutic Hypothermia A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi Definition of Perinatal Asphyxia *No agreed universal definition ACOG/AAP
Neonatal Therapeutic Hypothermia A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi Definition of Perinatal Asphyxia *No agreed universal definition ACOG/AAP
Therapeutic Hypothermia for infants > 35 wks with moderate or severe Hypoxic Ischaemic Encephalopathy (HIE) Clinical Guideline Reference Number:
 Clinical Guideline Reference Number:") This is an official Northern Trust policy and should not be edited in any way Therapeutic Hypothermia for infants > 35 wks with moderate or severe Hypoxic Ischaemic Encephalopathy (HIE) Clinical Guideline
This is an official Northern Trust policy and should not be edited in any way Therapeutic Hypothermia for infants > 35 wks with moderate or severe Hypoxic Ischaemic Encephalopathy (HIE) Clinical Guideline
State of Florida Systemic Supportive Care Guidelines. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
These signs should lead to the administration of high concentrations of
 Hypoxic-ischemic encephalopathy (HIE); (cont.) Clinical manifestations; *Intrauterine; growth restriction and increased vascular resistances may be the st manifestation of fetal hypoxia. *During labor;
Hypoxic-ischemic encephalopathy (HIE); (cont.) Clinical manifestations; *Intrauterine; growth restriction and increased vascular resistances may be the st manifestation of fetal hypoxia. *During labor;
Case Presentations. Anamika B. Mukherjee, MD September 13, 2017
 Case Presentations Anamika B. Mukherjee, MD September 13, 2017 Nothing to disclose Disclosures Learning Objectives Use the CPQCC Toolkit for therapeutic hypothermia to apply the guidelines for screening
Case Presentations Anamika B. Mukherjee, MD September 13, 2017 Nothing to disclose Disclosures Learning Objectives Use the CPQCC Toolkit for therapeutic hypothermia to apply the guidelines for screening
NEONATAL SEIZURE. IAP UG Teaching slides
 NEONATAL SEIZURE 1 INTRODUCTION One of the important neonatal neurological emergencies requiring immediate medical care. Contribute to significant morbidity and mortality Incidence is around 0.5 to 0.8%
NEONATAL SEIZURE 1 INTRODUCTION One of the important neonatal neurological emergencies requiring immediate medical care. Contribute to significant morbidity and mortality Incidence is around 0.5 to 0.8%
COOLING FOR HYPOXIC ISCHEMIC ENCEPHALOPATHY
 COOLING FOR HYPOXIC ISCHEMIC ENCEPHALOPATHY Roger F. Soll H. Wallace Professor of Neonatology University of Vermont 19 th International Symposium on Neonatology Sao Paulo, Brazil DISCLOSURE Roger F. Soll
COOLING FOR HYPOXIC ISCHEMIC ENCEPHALOPATHY Roger F. Soll H. Wallace Professor of Neonatology University of Vermont 19 th International Symposium on Neonatology Sao Paulo, Brazil DISCLOSURE Roger F. Soll
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Hypoxic Ischemic Encephalopathy. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Hypoxic Ischemic Encephalopathy. These podcasts are designed to give medical students an overview of key topics in pediatrics.
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY
 ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
7 Simple Steps to Assess & Document any Neonatal aeeg
 7 Simple Steps to Assess & Document any Neonatal aeeg Created for you by: www.aeegcoach.com How to use the Seven Simple Steps Checklist Hi! It s Kathi Randall here Your aeeg coach. I m so excited to share
7 Simple Steps to Assess & Document any Neonatal aeeg Created for you by: www.aeegcoach.com How to use the Seven Simple Steps Checklist Hi! It s Kathi Randall here Your aeeg coach. I m so excited to share
PEDIATRIC BRAIN CARE
 PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
State of Florida Hypothermia Protocol. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy
 Original article: Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy *Dr Harshad Bhagat, ** Dr Ravindra Kawade, ***Dr Y.P.Sachdev *Junior Resident, Department Of Radiodiagnosis,
Original article: Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy *Dr Harshad Bhagat, ** Dr Ravindra Kawade, ***Dr Y.P.Sachdev *Junior Resident, Department Of Radiodiagnosis,
GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA
 GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA The newborn is not an adult, nor a child. In people of all ages, death can occur from a failure of breathing and / or circulation. The interventions required to aid
GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA The newborn is not an adult, nor a child. In people of all ages, death can occur from a failure of breathing and / or circulation. The interventions required to aid
Too or Too Cold. Too Cold...Too Hot...Just Right. Temperature Control in Newborns. Temperature Balance in Newborns. Basics in the Delivery Room
 Too or Too Cold Neonatology Rediscovers Temperature Control Advances and Controversies in Clinical Pediatrics May 31, 2007 Terri A. Slagle Neonatology, CPMC Too Cold...Too Hot...Just Right Too Cold = Issues
Too or Too Cold Neonatology Rediscovers Temperature Control Advances and Controversies in Clinical Pediatrics May 31, 2007 Terri A. Slagle Neonatology, CPMC Too Cold...Too Hot...Just Right Too Cold = Issues
Original article: Evaluation of hypoxic-ischaemic events in preterm neonates using trans cranial ultrasound
 Original article: Evaluation of hypoxic-ischaemic events in preterm neonates using trans cranial ultrasound Priyanka Upadhyay *, Ketki U Patil 1, Rajesh Kuber 2, Vilas Kulkarni 3, Amarjit Singh 4 * Chief
Original article: Evaluation of hypoxic-ischaemic events in preterm neonates using trans cranial ultrasound Priyanka Upadhyay *, Ketki U Patil 1, Rajesh Kuber 2, Vilas Kulkarni 3, Amarjit Singh 4 * Chief
Study of renal functions in neonatal asphyxia
 Original article: Study of renal functions in neonatal asphyxia *Dr. D.Y.Shrikhande, **Dr. Vivek Singh, **Dr. Amit Garg *Professor and Head, **Senior Resident Department of Pediatrics, Pravara Institute
Original article: Study of renal functions in neonatal asphyxia *Dr. D.Y.Shrikhande, **Dr. Vivek Singh, **Dr. Amit Garg *Professor and Head, **Senior Resident Department of Pediatrics, Pravara Institute
Serum creatine kinase and lactic dehydrogenase levels as useful markers of immediate and long-term outcome of perinatal asphyxia
 Serum creatine kinase and lactic dehydrogenase levels as useful markers of immediate and long-term outcome of perinatal asphyxia D H Karunatilaka 1, G W D S Amaratunga 2, K D N I Perera 3, V Caldera 4
Serum creatine kinase and lactic dehydrogenase levels as useful markers of immediate and long-term outcome of perinatal asphyxia D H Karunatilaka 1, G W D S Amaratunga 2, K D N I Perera 3, V Caldera 4
Pathophysiology Review. Hypoxic-Ischemic Encephalopathy & Therapeutic Hypothermia. Objectives. What is Hypoxic-Ischemic Encephalopathy?
 Hypoxic-Ischemic Encephalopathy & Therapeutic Hypothermia Nancy Couto Nurse Practitioner, NICU London Health Sciences Centre, Children s Hospital nancy.couto@lhsc.on.ca 2014 12 17 Objectives Review Pathophysiology
Hypoxic-Ischemic Encephalopathy & Therapeutic Hypothermia Nancy Couto Nurse Practitioner, NICU London Health Sciences Centre, Children s Hospital nancy.couto@lhsc.on.ca 2014 12 17 Objectives Review Pathophysiology
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO
 TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
Predicting Outcomes in HIE. Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016
 Predicting Outcomes in HIE Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016 Interactive please! Case 1 Term, 3.5 kg Antenatal: Breech Labour/Delivery: Em CS failure to progress, mec
Predicting Outcomes in HIE Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016 Interactive please! Case 1 Term, 3.5 kg Antenatal: Breech Labour/Delivery: Em CS failure to progress, mec
Fetal Heart Rate Monitoring Myths and Misperceptions s: Electronic Fetal Heart Rate Monitoring (EFM): Baseline Assumptions.
: Baseline Assumptions.") Can FHR Monitoring Prevent Hypoxic-Ischemic Encephalopathy in the Newborn? Fetal Heart Rate Monitoring Myths and Misperceptions 1. Yes 2. No 72% Tekoa L. King CNM, MPH June 6, 2008 28% Yes No Objectives
Can FHR Monitoring Prevent Hypoxic-Ischemic Encephalopathy in the Newborn? Fetal Heart Rate Monitoring Myths and Misperceptions 1. Yes 2. No 72% Tekoa L. King CNM, MPH June 6, 2008 28% Yes No Objectives
Cerebral function monitoring in term or near term neonates at MDH: preliminary experience and proposal of a guideline
 Original Article Cerebral function monitoring in term or near term neonates at MDH: preliminary experience and proposal of a guideline Stephen Attard, Doriette Soler, Paul Soler Introduction: Cerebral
Original Article Cerebral function monitoring in term or near term neonates at MDH: preliminary experience and proposal of a guideline Stephen Attard, Doriette Soler, Paul Soler Introduction: Cerebral
Perinatal asphyxia: Pathophysiology and therapy
 Perinatal asphyxia: Pathophysiology and therapy Peter Davis Melbourne Australia With thanks to Dr Sue Jacobs Moderate or severe HIE Complicates ~1/1000 term live births: Mortality: >25% Major neurological
Perinatal asphyxia: Pathophysiology and therapy Peter Davis Melbourne Australia With thanks to Dr Sue Jacobs Moderate or severe HIE Complicates ~1/1000 term live births: Mortality: >25% Major neurological
Therapeutic hypothermia for hypoxic ischemic encephalopathy using low-technology methods: A systematic review and meta-analysis
 Therapeutic hypothermia for hypoxic ischemic encephalopathy using low-technology methods: A systematic review and meta-analysis Rossouw G 1, Irlam J 2, Horn AR 1 1)Division of Neonatal Medicine, Department
Therapeutic hypothermia for hypoxic ischemic encephalopathy using low-technology methods: A systematic review and meta-analysis Rossouw G 1, Irlam J 2, Horn AR 1 1)Division of Neonatal Medicine, Department
Safety of 6% hydroxyethylstarch 130/0.42 in term neonates with severe HIE
 Safety of 6% hydroxyethylstarch 130/0.42 in term neonates with severe HIE D. Surkov Department of NICU, Regional Children s Hospital, Dnepropetrovsk, Ukraine Corresponding author: D. Surkov, Department
Safety of 6% hydroxyethylstarch 130/0.42 in term neonates with severe HIE D. Surkov Department of NICU, Regional Children s Hospital, Dnepropetrovsk, Ukraine Corresponding author: D. Surkov, Department
CEREBRAL FUNCTION MONITORING
 CEREBRAL FUNCTION MONITORING Introduction and Definitions The term amplitude integrated electroencephalography (aeeg) is used to denote a method for electro-cortical monitoring whereas cerebral function
CEREBRAL FUNCTION MONITORING Introduction and Definitions The term amplitude integrated electroencephalography (aeeg) is used to denote a method for electro-cortical monitoring whereas cerebral function
Infection. Risk factor for infection ACoRN alerting sign with * Clinical deterioration. Problem List. Respiratory. Cardiovascular
 The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
Retrospectıve analysıs for newborn ınfants wıth hypoxıc-ıschemıc encephalopathy
 Basic Research Journal of Medicine and Clinical Sciences ISSN 2315-6864 Vol. 1(2) pp. 19-24 September 2012 Available online http//www.basicresearchjournals.org Copyright 2012 Basic Research Journal Full
Basic Research Journal of Medicine and Clinical Sciences ISSN 2315-6864 Vol. 1(2) pp. 19-24 September 2012 Available online http//www.basicresearchjournals.org Copyright 2012 Basic Research Journal Full
Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants
 Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants Ajou University School of Medicine Department of Pediatrics Moon Sung Park M.D. Hee Cheol Jo, M.D., Jang Hoon Lee,
Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants Ajou University School of Medicine Department of Pediatrics Moon Sung Park M.D. Hee Cheol Jo, M.D., Jang Hoon Lee,
Neonatal Seizure. Dr.Nawar Yahya. Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan. Supervised by:
 Neonatal Seizure Supervised by: Dr.Nawar Yahya Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan Objectives: What is neonatal seizure Etiology Clinical presentation Differential diagnosis
Neonatal Seizure Supervised by: Dr.Nawar Yahya Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan Objectives: What is neonatal seizure Etiology Clinical presentation Differential diagnosis
Severity of Hypoxic Ischaemic Encephalopathy in Neonates with Birth Asphyxia
 Journal of Rawalpindi Medical College (JRMC); 2007; (): 8-22 Severity of Hypoxic Ischaemic Encephalopathy in Neonates with Birth Asphyxia Rubina Zulfiqar, Samiya Naeemullah Department of Paediatrics, Holy
Journal of Rawalpindi Medical College (JRMC); 2007; (): 8-22 Severity of Hypoxic Ischaemic Encephalopathy in Neonates with Birth Asphyxia Rubina Zulfiqar, Samiya Naeemullah Department of Paediatrics, Holy
SWISS SOCIETY OF NEONATOLOGY. Neonatal cerebral infarction
 SWISS SOCIETY OF NEONATOLOGY Neonatal cerebral infarction May 2002 2 Mann C, Neonatal and Pediatric Intensive Care Unit, Landeskrankenhaus und Akademisches Lehrkrankenhaus Feldkirch, Austria Swiss Society
SWISS SOCIETY OF NEONATOLOGY Neonatal cerebral infarction May 2002 2 Mann C, Neonatal and Pediatric Intensive Care Unit, Landeskrankenhaus und Akademisches Lehrkrankenhaus Feldkirch, Austria Swiss Society
Resuscitating neonatal and infant organs and preserving function. GI Tract and Kidneys
 Resuscitating neonatal and infant organs and preserving function GI Tract and Kidneys Australian and New Zealand Resuscitation Council Joint Guidelines Outline Emphasis on the infant - PICU Kidney Gastrointestinal
Resuscitating neonatal and infant organs and preserving function GI Tract and Kidneys Australian and New Zealand Resuscitation Council Joint Guidelines Outline Emphasis on the infant - PICU Kidney Gastrointestinal
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Subhairline EEG Part II - Encephalopathy
 Subhairline EEG Part II - Encephalopathy Teneille Gofton September 2013 Objectives To review the subhairline EEG changes seen with encephalopathy To discuss specific EEG findings in encephalopathy To outline
Subhairline EEG Part II - Encephalopathy Teneille Gofton September 2013 Objectives To review the subhairline EEG changes seen with encephalopathy To discuss specific EEG findings in encephalopathy To outline
Hypoglycaemia of the neonate. Dr. L.G. Lloyd Dept. Paediatrics
 Hypoglycaemia of the neonate Dr. L.G. Lloyd Dept. Paediatrics Why is glucose important? It provides 60-70% of energy needs Utilization obligatory by red blood cells, brain and kidney as major source of
Hypoglycaemia of the neonate Dr. L.G. Lloyd Dept. Paediatrics Why is glucose important? It provides 60-70% of energy needs Utilization obligatory by red blood cells, brain and kidney as major source of
SWISS SOCIETY OF NEONATOLOGY. Severe apnea and bradycardia in a term infant
 SWISS SOCIETY OF NEONATOLOGY Severe apnea and bradycardia in a term infant October 2014 2 Walker JH, Arlettaz Mieth R, Däster C, Division of Neonatology, University Hospital Zurich, Switzerland Swiss Society
SWISS SOCIETY OF NEONATOLOGY Severe apnea and bradycardia in a term infant October 2014 2 Walker JH, Arlettaz Mieth R, Däster C, Division of Neonatology, University Hospital Zurich, Switzerland Swiss Society
Temperature Correction of Blood Gas Measurements during Therapeutic Hypothermia: Is it Time to Chill Out?
 Temperature Correction of Blood Gas Measurements during Therapeutic Hypothermia: Is it Time to Chill Out? Dr. Elizabeth Zorn Dr. Gwenyth Fischer Dr. Martha Lyon Disclosures (ML) Speaking Honoraria Radiometer
Temperature Correction of Blood Gas Measurements during Therapeutic Hypothermia: Is it Time to Chill Out? Dr. Elizabeth Zorn Dr. Gwenyth Fischer Dr. Martha Lyon Disclosures (ML) Speaking Honoraria Radiometer
Hypothermia: Neuroprotective Treatment of Hypoxic-Ischemic Encephalopathy. Serious perinatal asphyxia. Therapeutic hypothermia
 Therapeutic hypothermia Hypothermia: Neuroprotective Treatment of Hypoxic-Ischemic Encephalopathy Background of hypothermia Clinical application Floris Groenendaal Department of Neonatology Complications
Therapeutic hypothermia Hypothermia: Neuroprotective Treatment of Hypoxic-Ischemic Encephalopathy Background of hypothermia Clinical application Floris Groenendaal Department of Neonatology Complications
1/29/2014. Kimberly Johnson Hatchett, MD PGY-4 11/15/13
 Kimberly Johnson Hatchett, MD PGY-4 11/15/13 History of Present Illness 14 month old previously healthy infant boy presented via EMS after being found by his mother to be breathing loudly and non-responsive.
Kimberly Johnson Hatchett, MD PGY-4 11/15/13 History of Present Illness 14 month old previously healthy infant boy presented via EMS after being found by his mother to be breathing loudly and non-responsive.
The Clinical Spectrum and Prediction of Outcome in Hypoxic-Ischemic Encephalopathy
 Article neurology The Clinical Spectrum and Prediction of Outcome in Hypoxic-Ischemic Encephalopathy Walter C. Allan, MD* Objectives After completing this article, readers should be able to: 1. List the
Article neurology The Clinical Spectrum and Prediction of Outcome in Hypoxic-Ischemic Encephalopathy Walter C. Allan, MD* Objectives After completing this article, readers should be able to: 1. List the
COOLING FOR NEONATAL HYPOXIC ISCHAEMIC ENCEPHALOPATHY (HIE) - GUIDELINE
 - GUIDELINE") Background Objective Equipment Indications Contraindications When to initiate cooling in NPICU Procedure for therapeutic cooling NETS Transfer Issues Follow-up References Acknowledgements Related Documents
Background Objective Equipment Indications Contraindications When to initiate cooling in NPICU Procedure for therapeutic cooling NETS Transfer Issues Follow-up References Acknowledgements Related Documents
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article A Study on Serum Calcium Level in Birth Asphyxia Amrita Vamne 1*, Ramesh Chandra Thanna 2*,
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article A Study on Serum Calcium Level in Birth Asphyxia Amrita Vamne 1*, Ramesh Chandra Thanna 2*,
NEONATOLOGY Healthy newborn. Neonatal sequelaes
 NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
NEONATAL SEIZURES-PGPYREXIA REVIEW
 NEONATAL SEIZURES-PGPYREXIA REVIEW This is a very important Postgraduate topics will few Q asked in undergraduation also. Lets see them in detail. References: 1.Volpe s Neurology of newborn 2.Nelson s
NEONATAL SEIZURES-PGPYREXIA REVIEW This is a very important Postgraduate topics will few Q asked in undergraduation also. Lets see them in detail. References: 1.Volpe s Neurology of newborn 2.Nelson s
When? Incidence of neonatal seizures in a NICU population The incidence of seizures is higher in the neonatal period than in any other age group.
 Incidence of neonatal seizures in a NICU population The incidence of seizures is higher in the neonatal period than in any other age group. Standard EEG 2,3% 8.6% Standard EEG + aeeg Scher MS et al; Pediatrics
Incidence of neonatal seizures in a NICU population The incidence of seizures is higher in the neonatal period than in any other age group. Standard EEG 2,3% 8.6% Standard EEG + aeeg Scher MS et al; Pediatrics
Newborn Hypoxic Ischemic Brain Injury. Hisham Dahmoush, MBBCh FRCR Lucile Packard Children s Hospital at Stanford
 Newborn Hypoxic Ischemic Brain Injury Hisham Dahmoush, MBBCh FRCR Lucile Packard Children s Hospital at Stanford NO DISCLOSURES INTRODUCTION Neonatal hypoxic-ischemic encephalopathy (HIE) is a major cause
Newborn Hypoxic Ischemic Brain Injury Hisham Dahmoush, MBBCh FRCR Lucile Packard Children s Hospital at Stanford NO DISCLOSURES INTRODUCTION Neonatal hypoxic-ischemic encephalopathy (HIE) is a major cause
Kimberly M. Thornton, 1,2 Hongying Dai, 3 Seth Septer, 2,4 and Joshua E. Petrikin 1,2. 1. Introduction
 International Pediatrics, Article ID 643689, 7 pages http://dx.doi.org/10.1155/2014/643689 Research Article Effects of Whole Body Therapeutic Hypothermia on Gastrointestinal Morbidity and Feeding Tolerance
International Pediatrics, Article ID 643689, 7 pages http://dx.doi.org/10.1155/2014/643689 Research Article Effects of Whole Body Therapeutic Hypothermia on Gastrointestinal Morbidity and Feeding Tolerance
Current Management of the Infant Who Presents with Neonatal Encephalopathy
 Current Management of the Infant Who Presents with Neonatal Encephalopathy Elena V. Wachtel, MD, MPH, FAAP, and Karen D. Hendricks-Muñoz, MD, MPH, FAAP Neonatal encephalopathy after perinatal hypoxic-ischemic
Current Management of the Infant Who Presents with Neonatal Encephalopathy Elena V. Wachtel, MD, MPH, FAAP, and Karen D. Hendricks-Muñoz, MD, MPH, FAAP Neonatal encephalopathy after perinatal hypoxic-ischemic
Epilepsy CASE 1 Localization Differential Diagnosis
 2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
Running head: CASE STUDY NEONATAL HEAD COOLING 1
 Running head: CASE STUDY NEONATAL HEAD COOLING 1 Case Study 1: Head Cooling as Treatment for Neonatal Encephalopathy NURS 6035 Practicum I Teresa Z. Baker Texas Woman s University CASE STUDY NEONATAL HEAD
Running head: CASE STUDY NEONATAL HEAD COOLING 1 Case Study 1: Head Cooling as Treatment for Neonatal Encephalopathy NURS 6035 Practicum I Teresa Z. Baker Texas Woman s University CASE STUDY NEONATAL HEAD
Neonatal Hypotonia. Encephalopathy acute No encephalopathy. Neurology Chapter of IAP
 The floppy infant assumes a frog legged position. On ventral suspension, the baby can not maintain limb posture against gravity and assumes the position of a rag doll. Encephalopathy acute No encephalopathy
The floppy infant assumes a frog legged position. On ventral suspension, the baby can not maintain limb posture against gravity and assumes the position of a rag doll. Encephalopathy acute No encephalopathy
CEREBRAL OXIMETRY IN INFANTS WITH HIE DAPHNA YASOVA BARBEAU, MD FN3 MEETING 2018
 CEREBRAL OXIMETRY IN INFANTS WITH HIE DAPHNA YASOVA BARBEAU, MD FN3 MEETING 2018 OBJECTIVES 1. Understand how cerebral oximetry works 2. Understand how cerebral oximetry may guide intervention 3. Learn
CEREBRAL OXIMETRY IN INFANTS WITH HIE DAPHNA YASOVA BARBEAU, MD FN3 MEETING 2018 OBJECTIVES 1. Understand how cerebral oximetry works 2. Understand how cerebral oximetry may guide intervention 3. Learn
Neonatal Hypoxic-Ischemic Injury: Ultrasound and Dynamic Color Doppler Sonography perfusion of the Brain and Abdomen with pathologic correlation.
 Neonatal Hypoxic-Ischemic Injury: Ultrasound and Dynamic Color Doppler Sonography perfusion of the Brain and Abdomen with pathologic correlation. Ricardo Faingold,MD Montreal Children s Hospital Medical
Neonatal Hypoxic-Ischemic Injury: Ultrasound and Dynamic Color Doppler Sonography perfusion of the Brain and Abdomen with pathologic correlation. Ricardo Faingold,MD Montreal Children s Hospital Medical
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of therapeutic hypothermia with intracorporeal temperature monitoring for hypoxic
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of therapeutic hypothermia with intracorporeal temperature monitoring for hypoxic
Figure removed due to copyright restrictions.
 Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz IN SUMMARY HST 071 An Example of a Fetal Heart Rate Tracing Figure removed
Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz IN SUMMARY HST 071 An Example of a Fetal Heart Rate Tracing Figure removed
Medical Follow-up of the High-Risk NICU Graduate
 Medical Follow-up of the High-Risk NICU Graduate Silvia Fajardo-Hiriart, M.D. Medical Director High-Risk Infant Follow-Up/Early Intervention Program University of Miami Miller School of Medicine Department
Medical Follow-up of the High-Risk NICU Graduate Silvia Fajardo-Hiriart, M.D. Medical Director High-Risk Infant Follow-Up/Early Intervention Program University of Miami Miller School of Medicine Department
ACoRN Workbook 2012 Update
 ACoRN Neonatal Society Société néonatale ACoRN www.acornprogram.net A Canadian non-profit Society Vancouver, British Columbia ACoRN Workbook 2012 Update Name: The ACoRN Process The Resuscitation Sequence
ACoRN Neonatal Society Société néonatale ACoRN www.acornprogram.net A Canadian non-profit Society Vancouver, British Columbia ACoRN Workbook 2012 Update Name: The ACoRN Process The Resuscitation Sequence
05/14/2012. I have been a paid speaker for Natus
 I have been a paid speaker for Natus Robert White, MD Medical Director, Pediatrix Medical Group Memorial Hospital, South Bend, IN For diagnosis/prognosis following HIE For seizure detection and monitoring
I have been a paid speaker for Natus Robert White, MD Medical Director, Pediatrix Medical Group Memorial Hospital, South Bend, IN For diagnosis/prognosis following HIE For seizure detection and monitoring
Neurodevelopmental Follow Up After Therapeutic Hypothermia for Perinatal Asphyxia
 ORIGINAL PAPER doi: 10.5455/medarh.2015.69.362-366 Med Arh. 2015 Dec; 69(6): 362-366 Received: August 25th 2015 Accepted: November 05th 2015 2015 Smail Zubcevic, Suada Heljic, Feriha Catibusic, Sajra Uzicanin,
ORIGINAL PAPER doi: 10.5455/medarh.2015.69.362-366 Med Arh. 2015 Dec; 69(6): 362-366 Received: August 25th 2015 Accepted: November 05th 2015 2015 Smail Zubcevic, Suada Heljic, Feriha Catibusic, Sajra Uzicanin,
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Difficulties at Birth: Long Term Developmental Outcomes
 Difficulties at Birth: Long Term Developmental Outcomes Alan D. Bedrick MD Division of Neonatology and Developmental Biology Department of Pediatrics University of Arizona Tucson, Arizona DISCLOSURE I
Difficulties at Birth: Long Term Developmental Outcomes Alan D. Bedrick MD Division of Neonatology and Developmental Biology Department of Pediatrics University of Arizona Tucson, Arizona DISCLOSURE I
Imaging findings in neonates with hypoxic-ischaemic encephalopathy and terapeutic hypothermia.
 Imaging findings in neonates with hypoxic-ischaemic encephalopathy and terapeutic hypothermia. Poster No.: C-1577 Congress: ECR 2014 Type: Scientific Exhibit Authors: S. Manso Garcia, M. J. Velasco Marcos,
Imaging findings in neonates with hypoxic-ischaemic encephalopathy and terapeutic hypothermia. Poster No.: C-1577 Congress: ECR 2014 Type: Scientific Exhibit Authors: S. Manso Garcia, M. J. Velasco Marcos,
Hypoxic-ischemic encephalopathy has an incidence of
 Original Article Amplitude-Integrated EEG Is Useful in Predicting Neurodevelopmental Outcome in Full-Term Infants With Hypoxic-Ischemic Encephalopathy: A Meta-Analysis Journal of Child Neurology Volume
Original Article Amplitude-Integrated EEG Is Useful in Predicting Neurodevelopmental Outcome in Full-Term Infants With Hypoxic-Ischemic Encephalopathy: A Meta-Analysis Journal of Child Neurology Volume
PRACTICE GUIDELINES WOMEN S HEALTH PROGRAM
 C Title: NEWBORN: HYPOGLYCEMIA IN NEONATES BORN AT 35+0 WEEKS GESTATION AND GREATER: DIAGNOSIS AND MANAGEMENT IN THE FIRST 72 HOURS Authorization Section Head, Neonatology, Program Director, Women s Health
C Title: NEWBORN: HYPOGLYCEMIA IN NEONATES BORN AT 35+0 WEEKS GESTATION AND GREATER: DIAGNOSIS AND MANAGEMENT IN THE FIRST 72 HOURS Authorization Section Head, Neonatology, Program Director, Women s Health
11/9/2012. Group B Streptococcal Infections: Consensus and Controversies. Prevention of Early-Onset GBS Disease in the USA.
 Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Neurological outcome after perinatal asphyxia at term
 Section 1 Chapter 1 Scientific background Neurological outcome after perinatal asphyxia at term David Odd and Andrew Whitelaw Introduction It was nearly 150 years ago that an association between perinatal
Section 1 Chapter 1 Scientific background Neurological outcome after perinatal asphyxia at term David Odd and Andrew Whitelaw Introduction It was nearly 150 years ago that an association between perinatal
RESEARCH BRIEF. Prognostic Value of Resistive Index in Neonates with Hypoxic Ischemic
 RESEARCH BRIEF Prognostic Value of Resistive Index in Neonates with Hypoxic Ischemic A Senthil Kumar, Aparna Chandrasekaran, Rajamannar Asokan and *Kathirvelu Gopinathan From the Department of Neonatology,
RESEARCH BRIEF Prognostic Value of Resistive Index in Neonates with Hypoxic Ischemic A Senthil Kumar, Aparna Chandrasekaran, Rajamannar Asokan and *Kathirvelu Gopinathan From the Department of Neonatology,
Swings... Page 15 BTLG Newsletter July 2015
 Page 15 BTLG Newsletter July 2015 Swings... By James P. Fitzgerald, John M. Daly, Randy B. Nassau, and Margaret Johnson-Pertet, Yonkers, New York Introduction In March 2014, the American College of Obstetrics
Page 15 BTLG Newsletter July 2015 Swings... By James P. Fitzgerald, John M. Daly, Randy B. Nassau, and Margaret Johnson-Pertet, Yonkers, New York Introduction In March 2014, the American College of Obstetrics
Summary of Changes: References/content updated to reflect most current standards of practice.
 Alaska Native Medical Center: Mother Baby Unit Guideline: Neonatal Hypoglycemia Subject: Neonatal Hypoglycemia REVISION DATE: Jan 2015,12/2011, 02/2009, 11, 2007, 07/2007,04/2001, 04/1999 REPLACES: NSY:
Alaska Native Medical Center: Mother Baby Unit Guideline: Neonatal Hypoglycemia Subject: Neonatal Hypoglycemia REVISION DATE: Jan 2015,12/2011, 02/2009, 11, 2007, 07/2007,04/2001, 04/1999 REPLACES: NSY:
Prognosis in. Encephalopathy. Hypoxic-Ischemic. Özge Aydemİr MD
 Prognosis in Hypoxic-Ischemic Encephalopathy Özge Aydemİr MD Major problems we have to face while caring infants with HIE are; Øto provide families with reliable information about outcome. Øto decide how
Prognosis in Hypoxic-Ischemic Encephalopathy Özge Aydemİr MD Major problems we have to face while caring infants with HIE are; Øto provide families with reliable information about outcome. Øto decide how
Medically Fragile Children (Chapter 2)
") Medically Fragile Children (Chapter 2) Birth to three programs classify children with delays as those who have either established risk or are at risk Established risk infants are those with Genetic disorders
Medically Fragile Children (Chapter 2) Birth to three programs classify children with delays as those who have either established risk or are at risk Established risk infants are those with Genetic disorders
The Child with Alterations in Cerebral Function
 The Child with Alterations in Cerebral Function Neurologic Assessment VS HR, BP, Respirations, Temperature LOC Orientation Pediatric Glasgow Coma Scale Eyes Pupillary response and movement, extraoccular
The Child with Alterations in Cerebral Function Neurologic Assessment VS HR, BP, Respirations, Temperature LOC Orientation Pediatric Glasgow Coma Scale Eyes Pupillary response and movement, extraoccular
Predictive Value of Multimodality Evoked Potentials in Asphyxiated Term Newborns
 Ann Ali Abdel Kader et al. Predictive Value of Multimodality Evoked Potentials in Asphyxiated Term Newborns Ann Ali Abdel Kader 1, Saly El-Kholy 1, Dahlia El-Sebaie 2, Shahira Mostafa 1, Amira El-Gohary
Ann Ali Abdel Kader et al. Predictive Value of Multimodality Evoked Potentials in Asphyxiated Term Newborns Ann Ali Abdel Kader 1, Saly El-Kholy 1, Dahlia El-Sebaie 2, Shahira Mostafa 1, Amira El-Gohary
Advancing Neurologic Care in the Intensive Care Nursery
 Article neurology Advancing Neurologic Care in the Intensive Care Nursery Hannah C. Glass, MDCM* AUTHOR DISCLOSURE Dr Glass has disclosed that she is supported by grant K23NS066137 from the National Institute
Article neurology Advancing Neurologic Care in the Intensive Care Nursery Hannah C. Glass, MDCM* AUTHOR DISCLOSURE Dr Glass has disclosed that she is supported by grant K23NS066137 from the National Institute
Dysphagia in Encephalopathic Neonates Treated with Hypothermia
 Dysphagia in Encephalopathic Neonates Treated with Hypothermia A thesis submitted to the University of Arizona College of Medicine -- Phoenix in partial fulfillment of the requirements for the degree of
Dysphagia in Encephalopathic Neonates Treated with Hypothermia A thesis submitted to the University of Arizona College of Medicine -- Phoenix in partial fulfillment of the requirements for the degree of
ACoRN Workbook 2010 Update
 ACoRN Neonatal Society Société néonatale ACoRN A Canadian non-profit Society Vancouver, British Columbia www.acornprogram.net ACoRN Workbook 2010 Update Name: ACoRN Acute Care of at-risk Newborns The ACoRN
ACoRN Neonatal Society Société néonatale ACoRN A Canadian non-profit Society Vancouver, British Columbia www.acornprogram.net ACoRN Workbook 2010 Update Name: ACoRN Acute Care of at-risk Newborns The ACoRN
Brain injury and Resuscitation! Turning Back the Clock!
 Brain injury and Resuscitation! Turning Back the Clock! Dec 2008 Patrick J McNamara Learning Objectives Understand the benefits of Hypothermia and how it works? Identify patients who may benefit from treatment.
Brain injury and Resuscitation! Turning Back the Clock! Dec 2008 Patrick J McNamara Learning Objectives Understand the benefits of Hypothermia and how it works? Identify patients who may benefit from treatment.
University of Bristol - Explore Bristol Research
 Elstad, M., Liu, X., & Thoresen, M. (2016). Heart rate response to therapeutic hypothermia in infants with hypoxic-ischaemic encephalopathy. Resuscitation, 106, 53-57. DOI: 10.1016/j.resuscitation.2016.06.023
Elstad, M., Liu, X., & Thoresen, M. (2016). Heart rate response to therapeutic hypothermia in infants with hypoxic-ischaemic encephalopathy. Resuscitation, 106, 53-57. DOI: 10.1016/j.resuscitation.2016.06.023
Cooling guidance for babies presenting with moderate to severe hypoxic ischaemic encephalopathy within the North West London Perinatal Network
 Cooling guidance for babies presenting with moderate to severe hypoxic ischaemic encephalopathy within the North West London Perinatal Network 1. INTRODUCTION Perinatal asphyxia severe enough to cause
Cooling guidance for babies presenting with moderate to severe hypoxic ischaemic encephalopathy within the North West London Perinatal Network 1. INTRODUCTION Perinatal asphyxia severe enough to cause
HIE (Hypoxic Ischaemic Encephalopathy)
") HIE (Hypoxic Ischaemic Encephalopathy) Document Title and Reference : HIE (Hypoxic Ischaemic Encephalopathy Main Auth (s) Kiran Yajamanyam Consultant LWH Ratified by: CM NSG Date Ratified: May 2017 Review
HIE (Hypoxic Ischaemic Encephalopathy) Document Title and Reference : HIE (Hypoxic Ischaemic Encephalopathy Main Auth (s) Kiran Yajamanyam Consultant LWH Ratified by: CM NSG Date Ratified: May 2017 Review
AMERICAN ACADEMY OF PEDIATRICS
 AMERICAN ACADEMY OF PEDIATRICS The Role of the Primary Care Pediatrician in the Management of High-risk Newborn Infants ABSTRACT. Quality care for high-risk newborns can best be provided by coordinating
AMERICAN ACADEMY OF PEDIATRICS The Role of the Primary Care Pediatrician in the Management of High-risk Newborn Infants ABSTRACT. Quality care for high-risk newborns can best be provided by coordinating