UNION MINE HIGH SCHOOL
|
|
|
- Gabriella Henry
- 6 years ago
- Views:
Transcription
 Principal: Paul Neville Athletic Director: Jay Aliff FALL WINTER SPRING August 7, 2017 November 6, 2017 February 5, 2017 Cross Country - Co-Ed Basketball Boys (F/JV/V) Baseball")
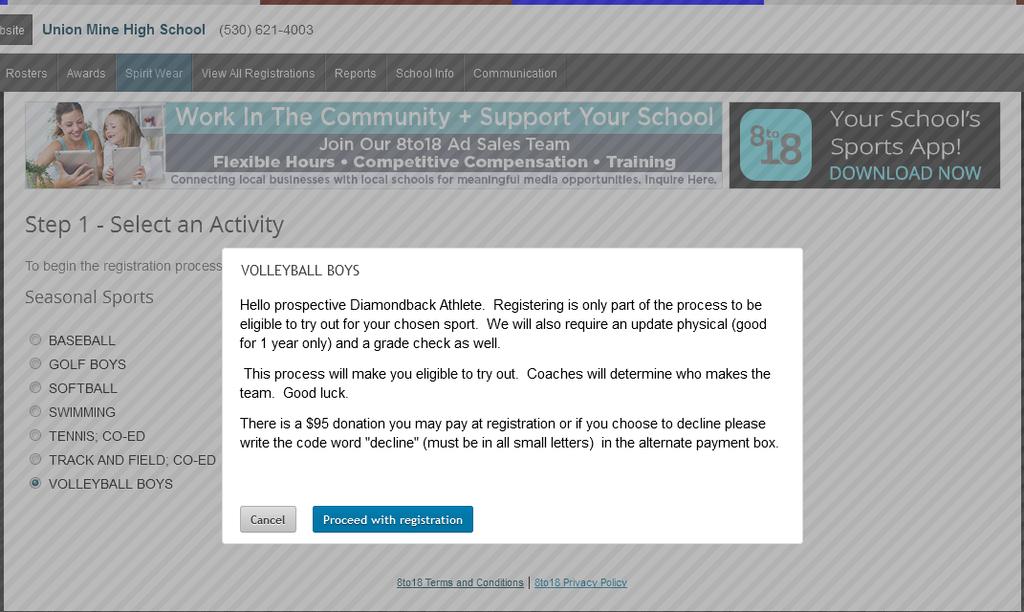
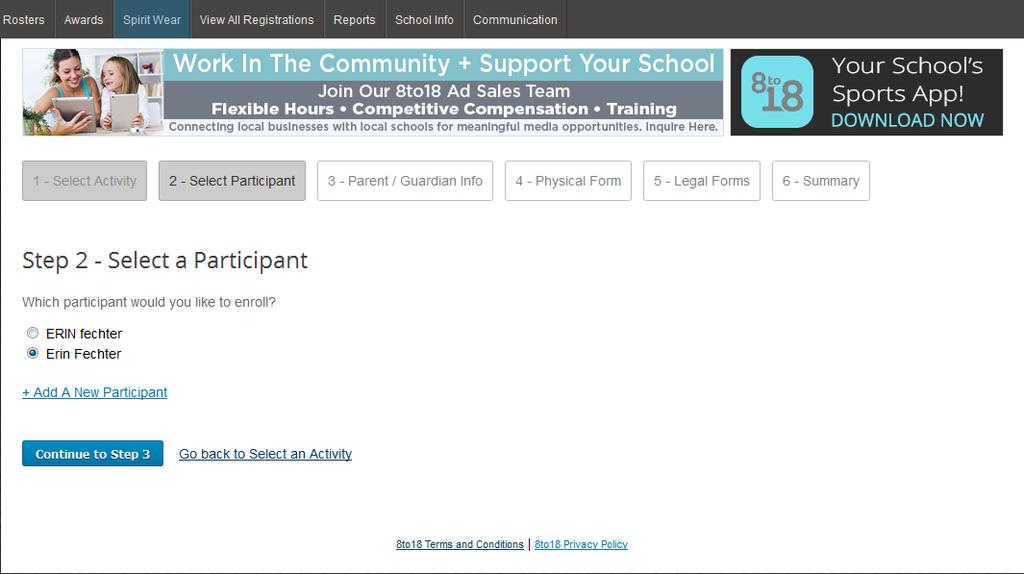
1 UNION MINE HIGH SCHOOL Home of the DIAMONDBACKS umhs.eduhsd.k12.ca.us (select Athletics) Principal: Paul Neville Athletic Director: Jay Aliff FALL WINTER SPRING August 7, 2017 November 6, 2017 February 5, 2017 Cross Country - Co-Ed Basketball Boys (F/JV/V) Baseball (JV/V) Golf Girls Basketball Girls (JV/V) Golf -Boys Football (JV/V) Ski/Snowboard Co-Ed Softball (JV/V) Volleyball Girls (F/JV/V) Soccer Boys (JV/V) Swimming - Co-Ed Soccer Girls (JV/V) Wrestling (JV/V) Tennis - Co-Ed Track & Field - Co-Ed Volleyball Boys (JV/V) 1. REGISTER ONLINE The online registration must be completed by the parent/legal guardian of the student. o (no o Click Create an Account and enter your own address and create a password. Please remember this password as you will use this each year for your child/children for sports registration. o Click Begin Registration o Select Activity (select all the sports your child is interested in participating in) o Select Participant Add a New Participant (or choose your child if you have already done this step) Fill out all information fields and continue to the next step o Physical Form Blank copy of the physical form is available for you to print, if needed. Remember every student athlete must have a current physical in order to begin tryouts/practice. o Legal Form Click to open and read each legal form. These forms are legal, binding documents. By clicking on the boxes you are agreeing and consenting to all information provided. Please note, if the form has a parent/guardian AND a student check box then both boxes must be checked in order to proceed forward. You do not need to turn in these forms as they are submitted electronically. o Summary At this time you will see what you have registered for. If you would like to contribute the VOLUNTARY $95 to the Athletic Program, you may either pay by credit card or check. If you would like to DECLINE the contribution, select the Alternate Payment (CODE) and type in decline in lowercase letters. Also add decline into the comment field. o Click Finish to complete the online registration process. These forms are submitted electronically to the UMHS Athletic office. 2. GET A PHYSICAL for the student athlete from a medical doctor. (See blank physical form) 3. TURN IN THE PHYSICAL to the UM Front Office/Athletic Secretary. GRADES AND FINES will be checked by the athletic office prior to each season to complete eligibility requirements. Students & coaches will be notified when athletes are cleared. Any questions please contact the Athletic Secretary, Anne Kling at (530) x4125 or akling@eduhsd.net

2
3

4 Please open and scroll to the bottom of each form. Some forms require both the parent/guardian as well as the participant acknowledgement. You do NOT need to print the forms off and return them. Please check the boxes to approve and acknowledge. Once all forms are approved and acknowledged, please continue to step six. The donation requested is completely VOLUNTARY. In no way does a donation influence the student s participation status on the team. If you would like to decline the voluntary donation, please select the Alternate Payment (CODE) box.
5 The word decline (lower case only) needs to be typed here. Comment may be brief and simple. Please don t feel that you have to explain your reasons for declining. Once again, VOLUNTARY donation has no weight on team participation or status.
6 [PLEASE PRINT] EL DORADO UNION HIGH SCHOOL DISTRICT Sports Participation Health Record This form must be completed every academic year NAME AGE SEX (CIRCLE) M F GRADUATION YEAR ADDRESS CITY ZIP PHONE Baseball Cheerleading Football Lacrosse Soccer Swimming/Diving Track Water Polo Basketball Cross-country Golf Skiing/ Snowboarding Softball Tennis Volleyball Wrestling Yes No PART A 1. Have you ever had an illness or injury that: a. Required you to stay in the hospital, explain: b. Lasted longer than a week, explain: HEALTH HISTORY c. Is related to allergies, e.g., hay fever, hives, bee sting, explain: d. Required an operation, explain: e. Is chronic, e.g., asthma, diabetes, seizures*, explain: 2. Do you take medications or pills, specify: 3. Have any members of your family under age 50 had a heart attack or died unexpectedly, explain: 4. Have you ever been: a. Dizzy or passed out during or after exercise, explain: b. Unconscious or had a concussion, explain: 5. Does running the 1/2-mile give you difficulty, explain: 6. Do you wear glasses or contacts, explain: 7. Do you have dental bridges, plates, or braces, explain: 8. Have you ever had a heart murmur, high blood pressure, or a heart abnormality, explain: 9. Do you have any allergies to medicines, explain: 10. Are you missing a kidney, lung, eye, or testicle, explain: 11. Have you ever had severe arm or neck pain, explain: 12. Have you sprained, strained, dislocated, or broken any of the following: *A swim seizure form is required for swim activities Ankle Elbow Hip Neck Other, explain: Back Foot Humerus Pelvis Chest/Ribs Forearm Knee Shoulder Collarbone Hand Leg Wrist I, hereby, state the answers on form are correct to the best of my knowledge. I have also read and agree to the contents of the athletic handbook. X Signature of Student Athlete Date I agree with the health history and give my permission for an examination. I have also read and agree to the contents of the athletic handbook. X Signature of Parent / Guardian Date PAGE 1 OF 2 F5141.3A REV 3/17/16
7 PART B PHYSICAL EXAMINATION RECORD (TO BE COMPLETED BY A LICENSED MEDICAL DOCTOR) Height (inches) Blood Pressure / Vision (Right) Weight (pounds) Pulse Vision (Left) CORE EXAMINATION NORMAL ABNORMAL FINDINGS INITIALS a. Eyes b. Ears, Nose, Throat c. Mouth, Teeth d. Neck e. Cardiovascular f. Chest, Lungs g. Abdomen h. Skin i. Genitalia, Hernia ORTHOPEDIC EXAMINATION NORMAL ABNORMAL FINDINGS INITIALS a. Neck b. Spine c. Shoulders d. Arms, Elbows e. Forearms, Wrists, Hands f. Hips g. Knees, Legs h. Ankles, Feet i. Flexibility j. Neuromuscular Abnormalities found in the health history and/or physical examination that needs assessment: RECOMMENDATIONS: Approved for full participation Needs to have the above abnormalities cleared before participation. Disqualified or limited in the following sports: X Licensed Medical Doctor's Signature Date: Licensed Medical Doctor's Printed Name Licensed Medical Doctor's Address PAGE 2 OF 2 F5141.3A REV 3/17/6
ATHLETIC PARTICIPATION FEE
 Dear Celtics, Welcome to Trinity Catholic High School. We are looking forward to a great year. The following athletic activities will be offered in the upcoming school year. Fall Sports Season Winter Sports
Dear Celtics, Welcome to Trinity Catholic High School. We are looking forward to a great year. The following athletic activities will be offered in the upcoming school year. Fall Sports Season Winter Sports
MARINA HS SPORTS PHYSICALS
 MARINA HS SPORTS PHYSICALS WHEN May 30 th, 2018 @ 4pm8pm WHERE Marina Gymnasium COST $30 cash or check WHAT TO BRING Peach PHYSICAL FORM (with front side filled out) $30 CASH or CHECK made out to Marina
MARINA HS SPORTS PHYSICALS WHEN May 30 th, 2018 @ 4pm8pm WHERE Marina Gymnasium COST $30 cash or check WHAT TO BRING Peach PHYSICAL FORM (with front side filled out) $30 CASH or CHECK made out to Marina
PIAA COMPREHENSIVE INITIAL PRE-PARTICIPATION PHYSICAL EVALUATION
 PIAA COMPREHENSIVE INITIAL PRE-PARTICIPATION PHYSICAL EVALUATION INITIAL EVALUATION: Prior to any student participating in Practices, Inter-School Practices, Scrimmages, and/or Contests, at any PIAA member
PIAA COMPREHENSIVE INITIAL PRE-PARTICIPATION PHYSICAL EVALUATION INITIAL EVALUATION: Prior to any student participating in Practices, Inter-School Practices, Scrimmages, and/or Contests, at any PIAA member
The New Mexico Activities Association physical form provides schools, parents and providers with a recommended form.
 The New Mexico Activities Association physical form provides schools, parents and providers with a recommended form. If the NMAA recommended Physical Form is to be used, please ensure that your child s
The New Mexico Activities Association physical form provides schools, parents and providers with a recommended form. If the NMAA recommended Physical Form is to be used, please ensure that your child s
Student s Name Male Female Date of Birth Grade. Parent s/guardian s Name Date Phone # Family Physician Phone #
 IOWA ATHLETIC PRE-PARTICIPATION PHYSICAL EXAMINATION ARTICLE VII 36.14(1) PHYSICAL EXAMINATION. Every year each student (grades 7-12) shall present to the student s superintendent a certificate signed
IOWA ATHLETIC PRE-PARTICIPATION PHYSICAL EXAMINATION ARTICLE VII 36.14(1) PHYSICAL EXAMINATION. Every year each student (grades 7-12) shall present to the student s superintendent a certificate signed
East Stroudsburg University Athletic Training Medical Forms Information and Directions
 East Stroudsburg University Athletic Training Medical Forms Information and Directions 2013 2014 All student athletes must complete all medical information forms on the ATS Webportal by July 27 th, 2013.
East Stroudsburg University Athletic Training Medical Forms Information and Directions 2013 2014 All student athletes must complete all medical information forms on the ATS Webportal by July 27 th, 2013.
NORTH CAROLINA HIGH SCHOOL ATHLETIC ASSOCIATION SPORT PREPARTICIPATION EXAMINATION FORM
 NORTH CAROLINA HIGH SCHOOL ATHLETIC ASSOCIATION SPORT PREPARTICIPATION EXAMINATION FORM Patient s Name: Age: This is a screening examination for participation in sports. This does not substitute for a
NORTH CAROLINA HIGH SCHOOL ATHLETIC ASSOCIATION SPORT PREPARTICIPATION EXAMINATION FORM Patient s Name: Age: This is a screening examination for participation in sports. This does not substitute for a
Durham Public Schools Assumptions of Risk/Medical Treatment Release
 Durham Public Schools Assumptions of Risk/Medical Treatment Release Student Athlete Name School Sport(s) Date The Durham Public Schools system makes every effort to prevent injuries, but injuries do occur
Durham Public Schools Assumptions of Risk/Medical Treatment Release Student Athlete Name School Sport(s) Date The Durham Public Schools system makes every effort to prevent injuries, but injuries do occur
DELAWARE INTERSCHOLASTIC ATHLETIC ASSOCIATION
 DELAWARE INTERSCHOLASTIC ATHLETIC ASSOCIATION Parents/Guardian: The DIAA pre-participation physical evaluation and consents form is a five page document. Pages one, two and four require your signature
DELAWARE INTERSCHOLASTIC ATHLETIC ASSOCIATION Parents/Guardian: The DIAA pre-participation physical evaluation and consents form is a five page document. Pages one, two and four require your signature
Celebration Lutheran School
 Celebration Lutheran School Wisconsin Interscholastic Athletic Association Athletic History and Physical Examination Approval for TWO YEARS of Competition All students participating in interscholastic
Celebration Lutheran School Wisconsin Interscholastic Athletic Association Athletic History and Physical Examination Approval for TWO YEARS of Competition All students participating in interscholastic
Huntsville High School Swim and Dive Check List. Name:
 Huntsville High School Swim and Dive Check List Name: Code of Conduct Physical Signed by Doctor Athletics Permission Form Liability Release Form 7 th Period Release Form Travel Form Medical Form Copy of
Huntsville High School Swim and Dive Check List Name: Code of Conduct Physical Signed by Doctor Athletics Permission Form Liability Release Form 7 th Period Release Form Travel Form Medical Form Copy of
Mount Mystics MSVU Athletics & Recreation
 Mount Mystics 2015-2016 MSVU Athletics & Recreation Student Athlete Medical History Card Please complete the first 3 pages and bring to entire document to the doctor s office. Athlete Information Sport:
Mount Mystics 2015-2016 MSVU Athletics & Recreation Student Athlete Medical History Card Please complete the first 3 pages and bring to entire document to the doctor s office. Athlete Information Sport:
The New Mexico Activities Association physical form provides schools, parents and providers with a recommended form.
 The New Mexico Activities Association physical form provides schools, parents and providers with a recommended form. If the NMAA recommended Physical Form is to be used, please ensure that your child s
The New Mexico Activities Association physical form provides schools, parents and providers with a recommended form. If the NMAA recommended Physical Form is to be used, please ensure that your child s
S Student Date of Birth (MM/DD/YYYY) Academic School Year Graduating Class
 Academic School Year Graduating Class") Student Last Name Student First Name Middle Initial 2018-2019 S Student Date of Birth (MM/DD/YYYY) Academic School Year Graduating Class Student ID Number Sport(s) of Interest (please list all) Athletic
Student Last Name Student First Name Middle Initial 2018-2019 S Student Date of Birth (MM/DD/YYYY) Academic School Year Graduating Class Student ID Number Sport(s) of Interest (please list all) Athletic
Regards, ext ext. 1160
 FOR: FROM: RE: Current/Prospective Medina Valley ISD Student-Athletes and Parents Randy Neuman, ATC, LAT, & Monica Valdez LAT, M. Ed. Athletic Physicals for the 2018-2019 school year Dear Athletes and
FOR: FROM: RE: Current/Prospective Medina Valley ISD Student-Athletes and Parents Randy Neuman, ATC, LAT, & Monica Valdez LAT, M. Ed. Athletic Physicals for the 2018-2019 school year Dear Athletes and
Oxford Golden Bears Comprehensive Initial Pre-Participation Physical Evaluation
 2018 Comprehensive Initial Pre-Participation Physical Evaluation SECTION 1: PERSONAL AND EMERGENCY INFORMATION ATHLETE S PERSONAL INFORMATION Name Male/Female (circle one) Date of Birth / / Age on Last
2018 Comprehensive Initial Pre-Participation Physical Evaluation SECTION 1: PERSONAL AND EMERGENCY INFORMATION ATHLETE S PERSONAL INFORMATION Name Male/Female (circle one) Date of Birth / / Age on Last
Pre-participation Physical Evaluation
 Pre-participation Physical Evaluation HISTORY FORM Date of Exam: Name Sex Age Date of Birth Grade School Sport(s) Address Phone Personal Physician In case of emergency, contact: Relationship Phone (H)
Pre-participation Physical Evaluation HISTORY FORM Date of Exam: Name Sex Age Date of Birth Grade School Sport(s) Address Phone Personal Physician In case of emergency, contact: Relationship Phone (H)
NORTH CAROLINA HIGH SCHOOL ATHLETIC ASSOCIATION SPORT PREPARTICIPATION EXAMINATION FORM
 NORTH CAROLINA HIGH SCHOOL ATHLETIC ASSOCIATION SPORT PREPARTICIPATION EXAMINATION FORM Patient s Name: Age: Sex: This is a screening examination for participation in sports. This does not substitute for
NORTH CAROLINA HIGH SCHOOL ATHLETIC ASSOCIATION SPORT PREPARTICIPATION EXAMINATION FORM Patient s Name: Age: Sex: This is a screening examination for participation in sports. This does not substitute for
Spring Hill College Athletic Training Department NCAA Division II Tryout
 Dear Parent/Guardian: Spring Hill College Athletic Training Department NCAA Division II Tryout I want to first welcome you to Spring Hill College and its athletic department; this is an exciting time for
Dear Parent/Guardian: Spring Hill College Athletic Training Department NCAA Division II Tryout I want to first welcome you to Spring Hill College and its athletic department; this is an exciting time for
have completed a physical exam on Print Physicians Name on. Name of Patient
 This form must be filled out by the physician that completed the physical and returned to the ATP Director by the patient. This form will be kept on record in the students permanent program file. Please
This form must be filled out by the physician that completed the physical and returned to the ATP Director by the patient. This form will be kept on record in the students permanent program file. Please
School Year
 2017-2018 School Year Dear Parents/Guardians, This letter is to inform you of our sports participation fee. The fee will be $140 per athlete, per sport. This fee will cover uniforms, transportation and
2017-2018 School Year Dear Parents/Guardians, This letter is to inform you of our sports participation fee. The fee will be $140 per athlete, per sport. This fee will cover uniforms, transportation and
OLD TAPPAN BOARD OF EDUCATION FILE CODE: / Old Tappan, NJ INTRAMURAL/INTERASCHOLASTIC COMPETITION
 OLD TAPPAN BOARD OF EDUCATION FILE CODE: 6145.1/ 6145.2 Old Tappan, NJ 07675 INTRAMURAL/INTERASCHOLASTIC COMPETITION New Jersey Department of Education ATHLETIC PRE-PARTICIPATION PHYSICAL EXAMINATION FORM
OLD TAPPAN BOARD OF EDUCATION FILE CODE: 6145.1/ 6145.2 Old Tappan, NJ 07675 INTRAMURAL/INTERASCHOLASTIC COMPETITION New Jersey Department of Education ATHLETIC PRE-PARTICIPATION PHYSICAL EXAMINATION FORM
Dear Parent or Legal Guardian: (NCSAA FORM A)
") Dear Parent or Legal Guardian: (NCSAA FORM A) Enclosed is the Nevada Choice Schools Activities Association ( NCSAA ) information packet for your child s sport s history and physical examination. The purpose
Dear Parent or Legal Guardian: (NCSAA FORM A) Enclosed is the Nevada Choice Schools Activities Association ( NCSAA ) information packet for your child s sport s history and physical examination. The purpose
AVORS MEDICAL GROUP Antelope Valley Orthopaedic & Rehabilitation Specialists
 Sports Physical Patient Forms Packet -- Page 1 of 7 AVORS MEDICAL GROUP Antelope Valley Orthopaedic & Rehabilitation Specialists Alon Antebi, DO Thomas S. Nasser, DO Ajay K. Masih, MD Justin Heller, MD
Sports Physical Patient Forms Packet -- Page 1 of 7 AVORS MEDICAL GROUP Antelope Valley Orthopaedic & Rehabilitation Specialists Alon Antebi, DO Thomas S. Nasser, DO Ajay K. Masih, MD Justin Heller, MD
University of Nebraska Omaha Athletic Performance Pre-Participation Medical History & Physical Examination Form TEAM TRYOUTS
 Name (Last, First, MI) University of Nebraska Omaha Athletic Performance Pre-Participation Medical History & Physical Examination Form TEAM TRYOUTS of Birth Address Sex M / F Sport Phone City State Zip
Name (Last, First, MI) University of Nebraska Omaha Athletic Performance Pre-Participation Medical History & Physical Examination Form TEAM TRYOUTS of Birth Address Sex M / F Sport Phone City State Zip
AVORS MEDICAL GROUP Antelope Valley Orthopaedic & Rehabilitation Specialists
 Work Physical Patient Forms Packet -- Page 1 of 6 AVORS MEDICAL GROUP Antelope Valley Orthopaedic & Rehabilitation Specialists Alon Antebi, DO Thomas S. Nasser, DO Ajay K. Masih, MD Justin Heller, MD Justin
Work Physical Patient Forms Packet -- Page 1 of 6 AVORS MEDICAL GROUP Antelope Valley Orthopaedic & Rehabilitation Specialists Alon Antebi, DO Thomas S. Nasser, DO Ajay K. Masih, MD Justin Heller, MD Justin
Sports Registration Check List
 Sports Registration Check List The following completed paperwork will need to be turned into the ATHLETIC OFFICE during registration dates for participation in a sport and 1 st day of practice. Physical
Sports Registration Check List The following completed paperwork will need to be turned into the ATHLETIC OFFICE during registration dates for participation in a sport and 1 st day of practice. Physical
ATHLETIC CONTRACT. I will strive to give my best to the team in every practice and every game.
 ATHLETIC CONTRACT Please initial each statement below to acknowledge your agreement to this contract. Then, sign the form at the bottom and return to the Athletic Director to be eligible for participation.
ATHLETIC CONTRACT Please initial each statement below to acknowledge your agreement to this contract. Then, sign the form at the bottom and return to the Athletic Director to be eligible for participation.
Jones Co. Jr. College Sports Medicine Medical History Questionairre
 Jones Co. Jr. College Sports Medicine Medical History Questionairre DEMOGRAPHIC INFORMATION Full Name: Social Security #: - - Date of Birth: Sport: Year in School: Home Phone #: Cell Phone #: Parent/Guardian
Jones Co. Jr. College Sports Medicine Medical History Questionairre DEMOGRAPHIC INFORMATION Full Name: Social Security #: - - Date of Birth: Sport: Year in School: Home Phone #: Cell Phone #: Parent/Guardian
ICSA Sports Physical Examination
 Learning and Leading in a Collaborative Culture ICSA Sports Physical Examination (Circle One) MALE FEMALE What Sport do you plan to play? Student s Name: Date of Birth: M D Y Age: Grade / Class Address:
Learning and Leading in a Collaborative Culture ICSA Sports Physical Examination (Circle One) MALE FEMALE What Sport do you plan to play? Student s Name: Date of Birth: M D Y Age: Grade / Class Address:
ALABAMA INDEPENDENT SCHOOL ASSOCIATION PHYSICAL EXAMINATION FORM
 ALABAMA INDEPENDENT SCHOOL ASSOCIATION PHYSICAL EXAMINATION FORM (Completed by Physician) HEIGHT WEIGHT BLOOD PRESSURE PULSE (SYSTOLIC/DIASTOLIC) (BEATS/MIN) VISION: RIGHT 20/ LEFT 20/ CORRECTED UNCORRECTED
ALABAMA INDEPENDENT SCHOOL ASSOCIATION PHYSICAL EXAMINATION FORM (Completed by Physician) HEIGHT WEIGHT BLOOD PRESSURE PULSE (SYSTOLIC/DIASTOLIC) (BEATS/MIN) VISION: RIGHT 20/ LEFT 20/ CORRECTED UNCORRECTED
STUDENT/ATHLETE Medical Release Form. Alabama Independent School Association
 STUDENT/ATHLETE Medical Release Form 1500 East Fairview Avenue Huntingdon College Montgomery, AL 36106 (334) 833-4080 Fax (334) 833-4086 www.aisaonline.org Alabama Independent School Association Federal
STUDENT/ATHLETE Medical Release Form 1500 East Fairview Avenue Huntingdon College Montgomery, AL 36106 (334) 833-4080 Fax (334) 833-4086 www.aisaonline.org Alabama Independent School Association Federal
ATHLETIC TRAINING INFORMATION AND PROCEDURES. Jaime Dickerson, MA, ATC Athletic Trainer
 ATHLETIC TRAINING INFORMATION AND PROCEDURES Jaime Dickerson, MA, ATC Athletic Trainer 973-661-8995 jdickerson@nutleyschools.org PHYSICAL INSTRUCTIONS ALL FORMS MUST BE TURNED IN TOGETHER!! All incoming
ATHLETIC TRAINING INFORMATION AND PROCEDURES Jaime Dickerson, MA, ATC Athletic Trainer 973-661-8995 jdickerson@nutleyschools.org PHYSICAL INSTRUCTIONS ALL FORMS MUST BE TURNED IN TOGETHER!! All incoming
Illinois State University. Athletic Training Education Program
 Illinois State University Athletic Training Education Program Procedures for Determining that the Health Status of an Athletic Training Student will permit him or her to meet the Established Technical
Illinois State University Athletic Training Education Program Procedures for Determining that the Health Status of an Athletic Training Student will permit him or her to meet the Established Technical
Sports Merit Badge Workbook
 Merit Badge Workbook This workbook can help you but you still need to read the merit badge pamphlet. This Workbook can help you organize your thoughts as you prepare to meet with your merit badge counselor.
Merit Badge Workbook This workbook can help you but you still need to read the merit badge pamphlet. This Workbook can help you organize your thoughts as you prepare to meet with your merit badge counselor.
FRESHMEN/TRANSFER STUDENT CHECKLIST
 FRESHMEN/TRANSFER STUDENT CHECKLIST Pre Participation Questionnaire Medical Consent Form Insurance Form Please include a copy of the FRONT and BACK of your insurance card. Pre Participation Physical Form
FRESHMEN/TRANSFER STUDENT CHECKLIST Pre Participation Questionnaire Medical Consent Form Insurance Form Please include a copy of the FRONT and BACK of your insurance card. Pre Participation Physical Form
Sudden Cardiac Death in Young Athletes
 Sudden Cardiac Death in Young Athletes Information for student-athletes and parents/legal custodians What is sudden cardiac death in the young athlete? Sudden cardiac death is the result of an unexpected
Sudden Cardiac Death in Young Athletes Information for student-athletes and parents/legal custodians What is sudden cardiac death in the young athlete? Sudden cardiac death is the result of an unexpected
Following this letter are health forms for parents or legal guardians to complete and sign. Please note that:
 Summer Pre-College Programs Dear Summer Pre-College Student and Family, Welcome to Marist College! Please review the attached Health Forms. Students will be informed of health and emergency information
Summer Pre-College Programs Dear Summer Pre-College Student and Family, Welcome to Marist College! Please review the attached Health Forms. Students will be informed of health and emergency information
Archery Climbing Fasmode Hip Hop Dance Tennis Triathlon Baseball Boxing Brazilian Jiu Jitsu Cheer Cycling Ice Hockey M/W Basketball
 New Participants Congratulations on becoming a part of the Sport Clubs Program at California State University, Northridge. At Sport Clubs your health and welfare is extremely important to us. To ensure
New Participants Congratulations on becoming a part of the Sport Clubs Program at California State University, Northridge. At Sport Clubs your health and welfare is extremely important to us. To ensure
CONTENTS ALL PARTS OF THIS PACKET ARE IMPORTANT, AND IT MUST BE COMPLETED IN ITS ENTIRETY!
 2017-18 Point Park University Athletics Medical Packet Enclosed you will find many of the necessary forms needed to compete in intercollegiate athletics during the 2017-18 year. Please return all completed
2017-18 Point Park University Athletics Medical Packet Enclosed you will find many of the necessary forms needed to compete in intercollegiate athletics during the 2017-18 year. Please return all completed
FORMS 1) PAR Q & YOU:
 PAR Q & YOU:") Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
INITIAL MEDICAL PACKET
 P a g e 1 INITIAL MEDICAL PACKET Name: Sport: Date: Last First Middle SSN: - - DOB: / / Age: Cell Phone: ( ) - Home Phone: ( ) - Family Physician: Phone: ( ) - Emergency contact: Name: Phone: ( ) - Relationship:
P a g e 1 INITIAL MEDICAL PACKET Name: Sport: Date: Last First Middle SSN: - - DOB: / / Age: Cell Phone: ( ) - Home Phone: ( ) - Family Physician: Phone: ( ) - Emergency contact: Name: Phone: ( ) - Relationship:
PIAA COMPREHENSIVE INITIAL PRE-PARTICIPATION PHYSICAL EVALUATION
 PIAA COMPREHENSIVE INITIAL PRE-PARTICIPATION PHYSICAL EVALUATION INITIAL EVALUATION: Prior to any student participating in Practices, Inter-School Practices, Scrimmages, and/or Contests, at any PIAA member
PIAA COMPREHENSIVE INITIAL PRE-PARTICIPATION PHYSICAL EVALUATION INITIAL EVALUATION: Prior to any student participating in Practices, Inter-School Practices, Scrimmages, and/or Contests, at any PIAA member
Print or Type. Emergency Information Student s Name Grade Date of Birth Home Address
 Athlete s Health Records Pre-participation Physical Exam The Shelby County Interscholastic Athletic Association requires every student-athlete to receive a pre-participation physical exam, including a
Athlete s Health Records Pre-participation Physical Exam The Shelby County Interscholastic Athletic Association requires every student-athlete to receive a pre-participation physical exam, including a
Piedmont High School Athletic Department Athletic Eligibility Requirements
 2017-2018 Piedmont High School Athletic Department Athletic Eligibility Requirements 1. Cover Page 2. Proof of Online Registration and Insurance (Must be notarized) 3. NCHSAA Pre-Participation Form (only
2017-2018 Piedmont High School Athletic Department Athletic Eligibility Requirements 1. Cover Page 2. Proof of Online Registration and Insurance (Must be notarized) 3. NCHSAA Pre-Participation Form (only
UWSP Medical History Form
 UWSP Medical History Form 2017-2018 Student: Please complete the first 6 pages prior to your appointment with your medical provider. The medical provider must sign off on the medical history form. Student
UWSP Medical History Form 2017-2018 Student: Please complete the first 6 pages prior to your appointment with your medical provider. The medical provider must sign off on the medical history form. Student
Pre-participation Physical Examinations
 Pre-participation Physical Examinations www.acsm.org Past Medical History History of any of the following should be made available to the healthcare provider: allergy allergies to medications asthma birth
Pre-participation Physical Examinations www.acsm.org Past Medical History History of any of the following should be made available to the healthcare provider: allergy allergies to medications asthma birth
LIST RESTRICTED ACTIVITY: CURRENT ACTIVITY LEVEL USUAL ACTIVITY LEVEL
 Whom may we thank for referring you to this office Today s Date: PATIENT DEMOGRAPHICS? HRN: Name: Birth Date: Age: Male Female Address: City: State: Zip: E mail Address: Home Phone: Mobile Phone: Marital
Whom may we thank for referring you to this office Today s Date: PATIENT DEMOGRAPHICS? HRN: Name: Birth Date: Age: Male Female Address: City: State: Zip: E mail Address: Home Phone: Mobile Phone: Marital
ETSU Athletic Training Jerry Robertson BucSports Athletic Medicine Center
 To: Potential ETSU Student Athlete From: Nathan Barger, MA, ATC Assistant Athletic Trainer for Football Re: Athletic Training Room Physical Paperwork Thank you for your interest in East Tennessee State
To: Potential ETSU Student Athlete From: Nathan Barger, MA, ATC Assistant Athletic Trainer for Football Re: Athletic Training Room Physical Paperwork Thank you for your interest in East Tennessee State
Health Services & Sports Medicine Entrance / Pre-Participation Physical Exam
 Full Name (First, Middle, Last): Health Services & Sports Medicine Entrance / Pre-Participation Physical Exam Sport (if athlete): Date of Birth: Social Security #: Home Address: Gender: Year in Sport:
Full Name (First, Middle, Last): Health Services & Sports Medicine Entrance / Pre-Participation Physical Exam Sport (if athlete): Date of Birth: Social Security #: Home Address: Gender: Year in Sport:
REDDY & ASSOCIATES LLC D/B/A Reddy Medical Group D/B/A Reddy Urgent Care. Reddy Urgent Care Pre-Employment Physical Form
 REDDY & ASSOCIATES LLC D/B/A Reddy Medical Group D/B/A Reddy Urgent Care 132 Franklin Springs St. 1061 Dowdy Road STE 100 280 General Daniels Ave. Royston, GA 30662 Athens, GA 30606 Danielsville, GA 30633
REDDY & ASSOCIATES LLC D/B/A Reddy Medical Group D/B/A Reddy Urgent Care 132 Franklin Springs St. 1061 Dowdy Road STE 100 280 General Daniels Ave. Royston, GA 30662 Athens, GA 30606 Danielsville, GA 30633
Immunization Packet for Incoming Students
 Health Occupations Division (707) 256-7600 Immunization Packet for Incoming Students Congratulations on being accepted into a Napa Valley College Health Occupations Program. This packet has been designed
Health Occupations Division (707) 256-7600 Immunization Packet for Incoming Students Congratulations on being accepted into a Napa Valley College Health Occupations Program. This packet has been designed
FORMS 1) PAR Q & YOU:
 PAR Q & YOU:") Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
East Coweta High School Practice Procedures for High Heat and Humidity
 East Coweta High School Practice Procedures for High Heat and Humidity The Coweta County School System and East Coweta High School are concerned about the health and safety of all student athletes. In
East Coweta High School Practice Procedures for High Heat and Humidity The Coweta County School System and East Coweta High School are concerned about the health and safety of all student athletes. In
Role of the Athletic Trainers:
 Role of the Athletic Trainers: Athletic trainers (ATC s) are members of the allied health community who work to prevent and treat athletic related injuries. They are certified by the National Athletic
Role of the Athletic Trainers: Athletic trainers (ATC s) are members of the allied health community who work to prevent and treat athletic related injuries. They are certified by the National Athletic
PART I - ATHLETIC PARTICIPATION (To be filled in and signed by the student)
") HRLax High School League Athletic Participation/Parental Consent/Medical Release Form Separate signed form is required for each school year May 1 of the current year through June 30 of the succeeding year.
HRLax High School League Athletic Participation/Parental Consent/Medical Release Form Separate signed form is required for each school year May 1 of the current year through June 30 of the succeeding year.
Titan Athletics Information for the School Year
 Titan Athletics Information for the 2018-2019 School Year -Physicals for athletes participating in athletics for the 2018-2019 school year must be completed and dated AFTER May 1st, 2018. Katy ISD sponsored
Titan Athletics Information for the 2018-2019 School Year -Physicals for athletes participating in athletics for the 2018-2019 school year must be completed and dated AFTER May 1st, 2018. Katy ISD sponsored
CONCUSSION. Thinking/Remembering Physical Emotional/Mood Sleep. Feeling sick to your stomach/queasy
 CONCUSSION INFORMATION FOR STUDENT-ATHLETES & PARENTS/LEGAL CUSTODIANS What is a concussion? A concussion is an injury to the brain caused by a direct or indirect blow to the head. It results in your brain
CONCUSSION INFORMATION FOR STUDENT-ATHLETES & PARENTS/LEGAL CUSTODIANS What is a concussion? A concussion is an injury to the brain caused by a direct or indirect blow to the head. It results in your brain
Checklist for Participation in Athletics
 Checklist for Participation in Athletics Dear Parent(s)/ Guardian(s), Enclosed you will find the documentation required in order for your child to participate in athletics at HPCA. Please read ALL information
Checklist for Participation in Athletics Dear Parent(s)/ Guardian(s), Enclosed you will find the documentation required in order for your child to participate in athletics at HPCA. Please read ALL information
Sports Clearance Process for Cornell Student Athletes
 Cornell Health Sports Medicine 110 Ho Plaza Ithaca, New York 14853-3101 t. 607.255.5155 f. 607.255.0269 www.health.cornell.edu Sports Clearance Process for Cornell Student Athletes The Sports Medicine
Cornell Health Sports Medicine 110 Ho Plaza Ithaca, New York 14853-3101 t. 607.255.5155 f. 607.255.0269 www.health.cornell.edu Sports Clearance Process for Cornell Student Athletes The Sports Medicine
Pre-Participation Medical Questionnaire Team Canada Volleyball Centralized Training
 Pre-Participation Medical Questionnaire Team Canada Volleyball Centralized Training This form should be completed by the athlete and presented to the physician during his/her medical exam. Player I.D.
Pre-Participation Medical Questionnaire Team Canada Volleyball Centralized Training This form should be completed by the athlete and presented to the physician during his/her medical exam. Player I.D.
PATIENT FEE SCHEDULE As of January 1, 2017
 TERMS OF ACCEPTANCE When a patient seeks chiropractic care and we accept such a patient for care, it is essential for both to be working towards the same objective. Chiropractic has only one goal. It is
TERMS OF ACCEPTANCE When a patient seeks chiropractic care and we accept such a patient for care, it is essential for both to be working towards the same objective. Chiropractic has only one goal. It is
Name (First, MI, Last) Date of Birth Age Male Female. Primary Care Physician. Referring Physician
 Date of Birth Age Male Female. Primary Care Physician. Referring Physician") Current Problem Date Name (First, MI, Last) Date of Birth Age Male Female Primary Care Physician Referring Physician Height (feet/inches) Weight (lbs.) Right Handed Left Handed Both Current Problem: Right
Current Problem Date Name (First, MI, Last) Date of Birth Age Male Female Primary Care Physician Referring Physician Height (feet/inches) Weight (lbs.) Right Handed Left Handed Both Current Problem: Right
Notto Chiropractic Health Center Patient Information
 Notto Chiropractic Health Center Patient Information Acct #: Name: Preferred Name: Address: City: State: Zip: Home Phone: ( ) - _. Work Phone: ( ) -. Who Referred You? In Case of Emergency: Phone Number:
Notto Chiropractic Health Center Patient Information Acct #: Name: Preferred Name: Address: City: State: Zip: Home Phone: ( ) - _. Work Phone: ( ) -. Who Referred You? In Case of Emergency: Phone Number:
T1D Camper s Name: Birth date: Gender: F M School Grade: Date Diagnosed: Insulin Type(s):
:") REGISTRATION FORM- T1D Camper + Optional Sibling/Friend Sam Fuld s USF Diabetes Sports Camp 2019 February 2-3, 2019 University of South Florida Athletic Fields Tampa, Florida Open to Campers Ages 8-17.
REGISTRATION FORM- T1D Camper + Optional Sibling/Friend Sam Fuld s USF Diabetes Sports Camp 2019 February 2-3, 2019 University of South Florida Athletic Fields Tampa, Florida Open to Campers Ages 8-17.
(Please assign a numerical value from 1-6 to each goal in order of importance) Improve Energy Weight Loss Improve Physical Stamina/Endurance
 Improve Energy Weight Loss Improve Physical Stamina/Endurance") Through our desire to provide you with the most focused and personalized healthcare experience, we would like to understand the primary reasons that have brought you to the clinic today. Please take a
Through our desire to provide you with the most focused and personalized healthcare experience, we would like to understand the primary reasons that have brought you to the clinic today. Please take a
Korebalance Concussion Management Program
 Korebalance Concussion Management Program The comprehensive program that combines baseline assessment, proven strengthening regimen, and post injury assessment including both cerebrum (cognitive) and cerebellum
Korebalance Concussion Management Program The comprehensive program that combines baseline assessment, proven strengthening regimen, and post injury assessment including both cerebrum (cognitive) and cerebellum
Did you complete the Sports Ware Online required information (
 Dear New VSU Student Athlete and Parent/Guardian, Welcome to Virginia State University. It is important that a safe and knowledgeable environment is maintained for you, the student-athlete, the athletic
Dear New VSU Student Athlete and Parent/Guardian, Welcome to Virginia State University. It is important that a safe and knowledgeable environment is maintained for you, the student-athlete, the athletic
KEY TO LIFE CHIROPRACTIC
 KEY TO LIFE CHIROPRACTIC REGISTRATION FORM Date Home Phone Cell Phone Email Last Name First Name Middle Initial Street Address City State Zip Sex M F Birth Date Occupation How did you hear about this office?
KEY TO LIFE CHIROPRACTIC REGISTRATION FORM Date Home Phone Cell Phone Email Last Name First Name Middle Initial Street Address City State Zip Sex M F Birth Date Occupation How did you hear about this office?
Please everything to the address below: ITEMS TO MAIL. 1. Copy of the athletes immunization record
 In order to participate in the Syracuse Indoor Showcase each player will need to EMAIL all the items below upon completion of their online registration. Your registration/spot in the showcase is not complete
In order to participate in the Syracuse Indoor Showcase each player will need to EMAIL all the items below upon completion of their online registration. Your registration/spot in the showcase is not complete
3. Have you had any serious illness, operation, or been hospitalized in the past five years? Venereal disease (STD s), Sickle cell disease medication
, Sickle cell disease medication") MEDICAL HISTORY Patient's Name: Birth Date: 1. Has there been any change in your general health within the past year? 2. Are you now under the care of a physician or health care professional? Physician's
MEDICAL HISTORY Patient's Name: Birth Date: 1. Has there been any change in your general health within the past year? 2. Are you now under the care of a physician or health care professional? Physician's
WELLNESS CENTER Student Health Services (434) FAX (434)
 FAX (434)") Page 1 WELLNESS CENTER Student Health Services (434) 223-6167 FAX (434) 223-7071 New Student Health Form The staff at Student Health are dedicated to providing you with high-quality health care designed
Page 1 WELLNESS CENTER Student Health Services (434) 223-6167 FAX (434) 223-7071 New Student Health Form The staff at Student Health are dedicated to providing you with high-quality health care designed
Form and Protocol for Sports Physical Examinations
 581-021-0041 Form and Protocol for Sports Physical Examinations The State Board of Education adopts by reference the form entitled "School Sports Pre-Participation Examination May 2010" that must be used
581-021-0041 Form and Protocol for Sports Physical Examinations The State Board of Education adopts by reference the form entitled "School Sports Pre-Participation Examination May 2010" that must be used
,
 , o o o : : Girl Scouts, Hornets Nest Council 2018 Summer Camp Health/Permission Form SECTION ONE (must be completed every year for ALL campers) CAMPER INFORMATION Camp Session Name and Date: Camper Name
, o o o : : Girl Scouts, Hornets Nest Council 2018 Summer Camp Health/Permission Form SECTION ONE (must be completed every year for ALL campers) CAMPER INFORMATION Camp Session Name and Date: Camper Name
MEDICAL INFORMATION: Physician s Name: Phone #: When was your last physical examination?:
 PERSONAL INFORMATION: HEALTH STATUS QUESTIONNAIRE Name: Phone (hm): (bus): Address: City: State: Zip: Occupation: Male/Female: Age: Height: Weight: Lbs.: Emergency Contact: Phone: Relationship: MEDICAL
PERSONAL INFORMATION: HEALTH STATUS QUESTIONNAIRE Name: Phone (hm): (bus): Address: City: State: Zip: Occupation: Male/Female: Age: Height: Weight: Lbs.: Emergency Contact: Phone: Relationship: MEDICAL
UNIVERSITY HOSPITALS CASE MEDICAL CENTER CONSENT FOR INVESTIGATIONAL STUDIES (v )
") UNIVERSITY HOSPITALS CASE MEDICAL CENTER CONSENT FOR INVESTIGATIONAL STUDIES (v. 11.2012) Project Title: The Impact of Achilles Tightness on Lower Etremity Injuries in Adolescent Athletes Principal Investigator:
UNIVERSITY HOSPITALS CASE MEDICAL CENTER CONSENT FOR INVESTIGATIONAL STUDIES (v. 11.2012) Project Title: The Impact of Achilles Tightness on Lower Etremity Injuries in Adolescent Athletes Principal Investigator:
MOUNT VERNON CITY SCHOOL DISTRICT ATHLETICS and HEALTH SERVICES
 STUDENT NAME SPORT DATE GRADE LEVEL COACH PARENT/GUARDIAN ATHLETIC PARTICIPATION CONSENT FORM *PLEASE RETURN THIS FORM ON THE DAY THE ATHLETE HAS HIS/HER PHYSICAL/CONFERENCE* Dear Parent or Guardian: Your
STUDENT NAME SPORT DATE GRADE LEVEL COACH PARENT/GUARDIAN ATHLETIC PARTICIPATION CONSENT FORM *PLEASE RETURN THIS FORM ON THE DAY THE ATHLETE HAS HIS/HER PHYSICAL/CONFERENCE* Dear Parent or Guardian: Your
TRYOUT REQUEST COVERSHEET FOR PROSPECTIVE STUDENT
 TRYOUT REQUEST COVERSHEET FOR PROSPECTIVE STUDENT To be completed by Student prior to tryout Name Date Date of Birth Sport School Currently Attending Registered with NCAA Eligibility Center o Yes o No
TRYOUT REQUEST COVERSHEET FOR PROSPECTIVE STUDENT To be completed by Student prior to tryout Name Date Date of Birth Sport School Currently Attending Registered with NCAA Eligibility Center o Yes o No
POLICY AND PROCEDURE FOR MANAGEMENT OF HEAD INJURIES AND CONCUSSIONS IN EXTRACURRICULAR ATHLETIC ACTIVITIES
 File: JJIF POLICY AND PROCEDURE FOR MANAGEMENT OF HEAD INJURIES AND CONCUSSIONS IN EXTRACURRICULAR ATHLETIC ACTIVITIES This policy is aligned with the Commonwealth of Massachusetts Regulation (CMR 201.000)
File: JJIF POLICY AND PROCEDURE FOR MANAGEMENT OF HEAD INJURIES AND CONCUSSIONS IN EXTRACURRICULAR ATHLETIC ACTIVITIES This policy is aligned with the Commonwealth of Massachusetts Regulation (CMR 201.000)
Dartmouth College HANOVER NEW HAMPSHIRE 03755
 Dartmouth College HANOVER NEW HAMPSHIRE 03755 Health Service, Dick Hall s House, 7 Rope Ferry Road, HB 6143 TELEPHONE 603/646.9400 Dear Dartmouth Student-Athlete, 2016-2017 Academic Year It is a requirement
Dartmouth College HANOVER NEW HAMPSHIRE 03755 Health Service, Dick Hall s House, 7 Rope Ferry Road, HB 6143 TELEPHONE 603/646.9400 Dear Dartmouth Student-Athlete, 2016-2017 Academic Year It is a requirement
Name (First, MI, Last) Date of Birth Age Male Female. Primary Care Physician. Referring Physician
 Date of Birth Age Male Female. Primary Care Physician. Referring Physician") Current Problem Date Name (First, MI, Last) Date of Birth Age Male Female Primary Care Physician Referring Physician Height (feet/inches) Weight (lbs.) Right Handed Left Handed Both Current Problem: Right
Current Problem Date Name (First, MI, Last) Date of Birth Age Male Female Primary Care Physician Referring Physician Height (feet/inches) Weight (lbs.) Right Handed Left Handed Both Current Problem: Right
KEY TO LIFE CHIROPRACTIC
 KEY TO LIFE CHIROPRACTIC REGISTRATION FORM Date Home Phone Cell Phone Email Last Name First Name Middle Initial Street Address City State Zip Sex M F Birth Date Occupation How did you hear about this office?
KEY TO LIFE CHIROPRACTIC REGISTRATION FORM Date Home Phone Cell Phone Email Last Name First Name Middle Initial Street Address City State Zip Sex M F Birth Date Occupation How did you hear about this office?
Dear Incoming Student:
 Dear Incoming Student: As the Director of Wellness Services, I want to welcome you to Nyack College! Our Staff is dedicated to providing you with quality health care. Our philosophy is based on the wellness
Dear Incoming Student: As the Director of Wellness Services, I want to welcome you to Nyack College! Our Staff is dedicated to providing you with quality health care. Our philosophy is based on the wellness
Dartmouth College HANOVER NEW HAMPSHIRE 03755
 Dartmouth College HANOVER NEW HAMPSHIRE 03755 Health Service, Dick Hall s House, 7 Rope Ferry Road, HB 6143 TELEPHONE 603/646.9400 Dear Dartmouth Student-Athlete, 2017-2018 Academic Year It is a requirement
Dartmouth College HANOVER NEW HAMPSHIRE 03755 Health Service, Dick Hall s House, 7 Rope Ferry Road, HB 6143 TELEPHONE 603/646.9400 Dear Dartmouth Student-Athlete, 2017-2018 Academic Year It is a requirement
Prevention and Care of Activity Related Injuries KIN
 Instructor: Sherry Ann Miller, ATC, LAT Term: Spring 2019 Prevention and Care of Activity Related Injuries KIN 3360-030 Office: Center of Human Performance (CHP) 104; 942-2173(Kinesiology)/486-6171(Direct)
Instructor: Sherry Ann Miller, ATC, LAT Term: Spring 2019 Prevention and Care of Activity Related Injuries KIN 3360-030 Office: Center of Human Performance (CHP) 104; 942-2173(Kinesiology)/486-6171(Direct)
RAINIER VALLEY CHIROPRACTIC P.S th Avenue S. Seattle, WA 98118
 Patient Health History Full Name Date Street Address City & State Zip Phone Number Gender Date of Birth Age SSN How did you hear about our office? Marital Status # of Children? Currently Pregnant? / How
Patient Health History Full Name Date Street Address City & State Zip Phone Number Gender Date of Birth Age SSN How did you hear about our office? Marital Status # of Children? Currently Pregnant? / How
4. ADD/ADHD Medical Documentation Athlete is responsible for reading, completing, and providing required documentation.
 LAST NAME FIRST SPORT Returning Student-Athlete Health Information ONLY complete this booklet if you play varsity men s or women s soccer, women s volleyball, men s golf, men s or women s swimming, men
LAST NAME FIRST SPORT Returning Student-Athlete Health Information ONLY complete this booklet if you play varsity men s or women s soccer, women s volleyball, men s golf, men s or women s swimming, men
STRENGTH & CONDITIONING INFORMATION AND PRE-ACTIVITY SCREENING
 STRENGTH & CONDITIONING INFORMATION AND PRE-ACTIVITY SCREENING Please take the time to read through all the information and ensure all relevant forms are completed. The following questionnaire and waivers
STRENGTH & CONDITIONING INFORMATION AND PRE-ACTIVITY SCREENING Please take the time to read through all the information and ensure all relevant forms are completed. The following questionnaire and waivers
CASE HISTORY. Address: City: State: Zip: Date of Birth: Age: address: Occupation: Employer: Spouse's Employer: Referred by:
 CASE HISTORY Account #: Please complete this form using your keyboard, then print it using the print function of your browser. You can then sign the form and bring it with you to your first appointment.
CASE HISTORY Account #: Please complete this form using your keyboard, then print it using the print function of your browser. You can then sign the form and bring it with you to your first appointment.
Name: Date: Address: City: State: Zip: Birthday: / /
 PERSONAL TRAINING Name: Date: Address: City: State: Zip: Birthday: / / Sex: Male Female Name of Gym: Occupation: Phone (home): Phone (work): Body Weight: Body Fat: Height: Personal Goals 1. Primary Training
PERSONAL TRAINING Name: Date: Address: City: State: Zip: Birthday: / / Sex: Male Female Name of Gym: Occupation: Phone (home): Phone (work): Body Weight: Body Fat: Height: Personal Goals 1. Primary Training
PART ONE Stretching Fundamentals
 Contents Preface vii Acknowledgments xiii Reviewers xv PART ONE Stretching Fundamentals CHAPTER 1 Introduction to Stretching 3 WHY STRETCH: THE BENEFITS OF STRETCHING 3 Maintains and Improves Range of
Contents Preface vii Acknowledgments xiii Reviewers xv PART ONE Stretching Fundamentals CHAPTER 1 Introduction to Stretching 3 WHY STRETCH: THE BENEFITS OF STRETCHING 3 Maintains and Improves Range of
NEW PATIENT PAPERWORK
 NEW PATIENT PAPERWORK Welcome! Please fill out the necessary paperwork provided. It is our pleasure to serve you and your family. How did you find out about us? If It was a friend or doctor, please list
NEW PATIENT PAPERWORK Welcome! Please fill out the necessary paperwork provided. It is our pleasure to serve you and your family. How did you find out about us? If It was a friend or doctor, please list
Patient Name: First MI Last Preferred Name. DOB: Sex: MALE FEMALE SSN: Address: City: State: Zip Code:
 PATIENT DEMOGRAPHICS: Patient Name: First MI Last Preferred Name DOB: Sex: MALE FEMALE SSN: Address: City: State: Zip Code: Home Phone: _( ) Marital Status: Married Single Divorced Widowed Cell Phone:
PATIENT DEMOGRAPHICS: Patient Name: First MI Last Preferred Name DOB: Sex: MALE FEMALE SSN: Address: City: State: Zip Code: Home Phone: _( ) Marital Status: Married Single Divorced Widowed Cell Phone:
INTERCOLLEGIATE ATHLETICS RETURNING STUDENT-ATHLETE MEDICAL FORMS CHECKLIST
 RETURNING STUDENT-ATHLETE MEDICAL FORMS CHECKLIST Dear PC Student-Athletes, Welcome back to Aberdeen. We are excited to see you return to continue your pursuit of athletic excellence and academic success.
RETURNING STUDENT-ATHLETE MEDICAL FORMS CHECKLIST Dear PC Student-Athletes, Welcome back to Aberdeen. We are excited to see you return to continue your pursuit of athletic excellence and academic success.
INFORMATION/APPLICATION FOR CARE
 INFORMATION/APPLICATION FOR CARE The following information is needed in order to better serve you. Please complete all questions. If you need help please ask. Name Home Phone Work Phone Cell Phone E-Mail
INFORMATION/APPLICATION FOR CARE The following information is needed in order to better serve you. Please complete all questions. If you need help please ask. Name Home Phone Work Phone Cell Phone E-Mail
Socorro ISD Physical Packet Student Athlete Information Sheet (Clearly Print all information in Black or Blue Ink only.)
") Socorro ISD Physical Packet Student Athlete Information Sheet (Clearly Print all information in Black or Blue Ink only.) School ID #: Grade: Graduation Date: Name: M ( ) F ( ) Date of Birth: Age: Home
Socorro ISD Physical Packet Student Athlete Information Sheet (Clearly Print all information in Black or Blue Ink only.) School ID #: Grade: Graduation Date: Name: M ( ) F ( ) Date of Birth: Age: Home
SMITH CHIROPRACTIC HEALTH PROFILE Today s Date:
 SMITH CHIROPRACTIC HEALTH PROFILE Today s Date: Name: Age: Male/Female DOB: Address: City: State: Zip: Home Phone:_ Cell: Cell Phone Provider: SSN#: Email Address: Single/Married/Divorced/Widowed Spouse
SMITH CHIROPRACTIC HEALTH PROFILE Today s Date: Name: Age: Male/Female DOB: Address: City: State: Zip: Home Phone:_ Cell: Cell Phone Provider: SSN#: Email Address: Single/Married/Divorced/Widowed Spouse
Student Full Name: Date of Birth:
 Student Medical Form This form is to be completed for new students upon admission, and returning students prior to starting grades 3, 6, and 9. Students participating in athletics must complete form every
Student Medical Form This form is to be completed for new students upon admission, and returning students prior to starting grades 3, 6, and 9. Students participating in athletics must complete form every
Academic Year
 HEALTH SERVICE Sport s M edicine 7 Rope Ferr y Rd. 603-646-9419 2019-2020 Academic Year Dear Dartmouth Student-Athlete, It is a requirement under NCAA Bylaw 17.1.5 for all student-athletes beginning their
HEALTH SERVICE Sport s M edicine 7 Rope Ferr y Rd. 603-646-9419 2019-2020 Academic Year Dear Dartmouth Student-Athlete, It is a requirement under NCAA Bylaw 17.1.5 for all student-athletes beginning their
(emergency room pain)
") Welcome to Moving Body Chiropractic! We re glad you re here. Whether you re looking to work on a specific problem or just feel great, this form is the start to your wellness journey! Please take the time
Welcome to Moving Body Chiropractic! We re glad you re here. Whether you re looking to work on a specific problem or just feel great, this form is the start to your wellness journey! Please take the time