Cough and gastroesophageal reflux: from the gastroenterologist end
|
|
|
- Myles Merritt
- 6 years ago
- Views:
Transcription
, pp.135. <10.1016/j.pupt.2008.11.007>.")

1 Cough and gastroesophageal reflux: from the gastroenterologist end Ans Pauwels, Kathleen Blondeau, Lieven Dupont, Daniel Sifrim To cite this version: Ans Pauwels, Kathleen Blondeau, Lieven Dupont, Daniel Sifrim. Cough and gastroesophageal reflux: from the gastroenterologist end. Pulmonary Pharmacology & Therapeutics, 2009, 22 (2), pp.135. < /j.pupt >. <hal > HAL Id: hal Submitted on 11 Sep 2010 HAL is a multi-disciplinary open access archive for the deposit and dissemination of scientific research documents, whether they are published or not. The documents may come from teaching and research institutions in France or abroad, or from public or private research centers. L archive ouverte pluridisciplinaire HAL, est destinée au dépôt et à la diffusion de documents scientifiques de niveau recherche, publiés ou non, émanant des établissements d enseignement et de recherche français ou étrangers, des laboratoires publics ou privés.

2 Accepted Manuscript Title: Cough and gastroesophageal reflux: from the gastroenterologist end Authors: Ans Pauwels, Kathleen Blondeau, Lieven Dupont, Daniel Sifrim PII: S (08) DOI: /j.pupt Reference: YPUPT 883 To appear in: Pulmonary Pharmacology & Therapeutics Received Date: 13 October 2008 Revised Date: 3 November 2008 Accepted Date: 15 November 2008 Please cite this article as: Pauwels A, Blondeau K, Dupont L, Sifrim D. Cough and gastroesophageal reflux: from the gastroenterologist end, Pulmonary Pharmacology & Therapeutics (2008), doi: /j.pupt This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
3 COUGH AND GASTROESOPHAGEAL REFLUX: FROM THE GASTROENTEROLOGIST END Ans Pauwels, Kathleen Blondeau, Lieven Dupont and Daniel Sifrim Centre for Gastroenterological Research KULeuven and Department of Pneumology, Gasthuisberg University Hospital, KULeuven, Belgium Short title: Gastroesophageal reflux and chronic cough All correspondence to: Daniel Sifrim M.D., Ph.D Faculty of Medicine K.U.Leuven Lab G-I Physiopathology O&N Gasthuisberg, 7th floor Herestraat 49, 3000, Leuven, Belgium. Tel: Fax:
4 Abstract Gastroesophageal reflux (GER) is one of the three most common causes of chronic unexplained cough. Diagnosing GER related cough is challenging since many patients do not have esophagitis or an increased esophageal acid exposure during 24h esophageal ph-metry. A significant time association between acid reflux and cough can be demonstrated in a subgroup of patients, even if the total esophageal acid exposure is normal. Establishing an exact time relationship between reflux and cough requires objective measurements of both cough and reflux episodes. A variety of techniques for cough assessment are available, including sound recordings and continuous measurement of gastroesophageal pressures. The Symptom Association Probability (SAP) has been suggested as the most reliable algorithm to establish the non-chance association between GER and cough. Although the relationship between acid reflux and cough is generally accepted, the response rate of patients with chronic unexplained cough to proton pump inhibitor treatment (PPI) is poorer compared to that in patients with typical GERD symptoms. Combined impedance-ph recordings, a new technique for the measurement of all types of reflux, have recently shown that not only acid but also weakly acidic GER may be associated with cough. Moreover, measurements in patients on PPI therapy demonstrated that weakly acidic reflux may persist during PPI treatment and may be associated with cough. Aspiration of gastric contents into the lungs and a vagally mediated reflex arc, originating from the distal esophagus, have been proposed as pathophysiological mechanisms in GER-related cough. More recently, reflux induced bronchial hypersensitivity has been proposed as a third underlying mechanism. Treatment of GER related cough remains challenging. So far, long term PPI treatments produce unsatisfactory results. In patients not responding to PPI, weakly acidic GER might still be the cause of cough. In these patients other therapeutic strategies i.e. abolishing all types of GER might need to be considered. Antireflux surgery has been performed successfully in a group of patients with GER related cough. However, controlled, prospective outcome studies are necessary to confirm the role of antireflux treatments in the management of GER related cough. 2
5 Introduction Gastroesophageal reflux (GER) can result into typical symptoms such as regurgitation and heartburn with or without esophagitis. [1] Gastroesophageal reflux disease (GERD) can also be associated with extraesophageal symptoms, such as chronic cough, asthma and laryngitis. [2] Gastroenterologists often come across with patients having heartburn and/or regurgitation who also experience cough. On the other hand, pulmonologists are confronted with patients having chronic cough and heartburn. Increased GER is the third most common cause of chronic cough [3] and according to Jaspersen et al. cough is common either in erosive (30.5 %) and non-erosive (34.9 %) reflux disease. [4] To better understand the relationship between reflux and cough and provide a rationale therapy, both gastroenterologists and pulmonologists should 1) optimize their selection of patients with suspicion of reflux-related cough, 2) use the most sensitive methods for reflux detection, 3) use an objective method of cough detection and 4) use a good statistical algorithm that excludes a chance association between reflux in cough in each individual patient. Patient selection Before considering increased GER as a cause of cough, gastroenterologists need to make sure that other causes of chronic cough like allergies, smoking, ACE inhibitors, cancer or asthma are thoroughly excluded. Likewise, pulmonologists should not consider or exclude the diagnosis of increased GER, in a patient with cough, only based on a symptom questionnaire. It is known that a high proportion of patients with GER-related chronic cough do not have heartburn or regurgitation. [5-8] Detection of gastroesophageal reflux Endoscopy will detect esophagitis in 30-50% of patients with typical GER symptoms. [9] Patients with chronic cough without heartburn are unlikely to have esophagitis. [10] Twenty-four hour ph monitoring is considered the gold standard for diagnosis of GERD. Reflux episodes are defined as a ph drop below 4 for more than 10 seconds. Ph- 3
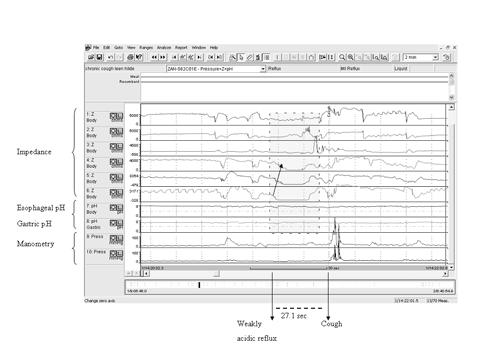
6 monitoring is considered pathological if total esophageal acid exposure is higher than 4.5 % of the 24h monitoring. Esophageal ph monitoring is limited to detection of acid reflux. More recently, a more sensitive ambulatory technique i.e. impedance-ph monitoring, has been introduced to measure both acid and non-acid reflux. [11] Our group first reported a possible involvement of non-acid reflux in the pathogenesis of chronic cough. [12;13] Detection of cough To understand the association between cough and reflux, it is necessary to record cough episodes during reflux monitoring. Several methods are currently used. The most frequently used is a diary card where the patient writes the exact timing of significant cough bursts. The patient also can push an event marker in the reflux monitoring data logger. This is a simple method that identifies the daytime cough episodes that were significant for the patient. However, many cough events are not recorded, and also nocturnal cough is missed. Other methods have been developed for objective cough recording, including microphone based sound recording using computer algorithm for automatic cough recognition. So far this method has not been used during reflux monitoring. [14] Finally, a manometric technique has been suggested by Paterson et al. [15] This technique consists of adding to the reflux monitoring catheter, a second thin catheter containing pressure sensors located in the abdomen and thorax. Coughing provokes a typical pressure pattern artifact that is recognized in the simultaneous refluxpressure monitoring. In this way, cough episodes are identified objectively and the presence of reflux before the cough can easily be recognized during the preceding time window. (Figure 1) Using this technique, our group has analyzed the relationship between cough and reflux in 100 patients with unexplained chronic cough. [12;13] Statistical algorithm that excludes a chance association between reflux and cough During a 24h ambulatory monitoring, many reflux and cough episodes may occur close together in time. Because of the large number of reflux and cough episodes, this might be due only by chance. If we want to address a possible causal association, we need first to identify cough episodes preceded by reflux. In order to exclude the chance association, 4
7 between reflux and other symptoms like heartburn or chest pain, several mathematical algorithms were designed. [16] The symptom index (SI) has been defined as the percentage of reflux associated symptom episodes and is considered positive if 50%. The disadvantage of the SI is that it does not take into account the total number of reflux episodes that occur. This means that patients with a large number of reflux events and a small number of symptoms may have a positive SI by chance. The symptom association probability (SAP) calculates the statistical relationship between symptoms and reflux episodes using the Fischer s exact test, taking into account the number of associated reflux-symptom episodes as well as the total number of reflux and symptom events. [17] For this the total twenty-four hour monitoring will be divided into frames of two minutes. A 2 minute period in which a reflux episode is detected, will be addressed as R+. In the next step, we will determine for every symptom if it was preceded by reflux in a 2 minute frame (R+S+). The Fisher s exact test will calculate the probability (p value) that the observed distribution could have occurred by chance. The SAP is calculated as (1-p)*100% and is considered positive when higher than 95%. [16] It is important to acknowledge that a time window of 2 minutes was chosen as optimal to assess the association between heartburn/chest pain and GER. [18] The optimal time window to calculate the SAP between reflux and cough is still unknown. In recent studies we used impedance-ph monitoring for reflux detection and continuous manometry for objective cough detection in 100 patients with unexplained chronic cough. We calculated the SAP with a time window of 2 minutes and found that 36% of the patients had a non-chance time association between their reflux and cough. Pathophysiology of reflux-related cough Aspiration of gastric juices containing acid, pepsin, bile acids and duodenal pancreatic enzymes, is considered to be an important mechanism in the etiology of reflux-related cough. Pharyngeal ph recording that demonstrated micro-aspiration of gastric contents into the pharynx favor this hypothesis. [19] In the past, detection of lipid-laden macrophages in bronchoalveolar lavage fluid (BALF) or sputum has been used as possible a marker for aspiration. Studies show that lipid-laden 5
8 alveolar macrophages are present in 85% of children with chronic respiratory tract disorders and GER. [20;21] This method has low specificity and little is known on its prevalence in adult patients with chronic unexplained cough. [22;23] BALF is tested on the presence of pepsin and/or bile acids to establish aspiration. Pepsin is found in BALF of almost all lung transplant patients and bile acids in half of the lung transplant patients. [24] It is not yet known which component of the refluxate is the most harmful to bronchial epithelial damage. A vagal reflex arc originating from the distal esophagus after either exposure to acid or esophageal distention can cause cough. [25-27] Lidocaine, a topical anesthetic, blocks cough induction by distal esophageal acidification. [25] Furthermore, acidification of the esophagus can activate local axonal reflexes which can cause inflammation in the airway. A study of Patterson et al. showed that the presence of acid in the esophagus in asthma and chronic cough patients releases tachykinins such as substance P and neurokinin A into the lungs where they will cause bronchoconstriction and airway micro vascular leakage. [27] Patients with GER and cough have higher cough sensitivity after perfusion of an acid solution into the distal esophagus compared to patients with GER without cough. [28] If gastroesophageal reflux induces cough, why not all patients with increased GER have cough? Is there a specific difference in the refluxate or rather a hypersensitivity pattern in those patients with reflux-related cough? We studied 100 patients with chronic unexplained cough. [13] A minority of these patients had an increased number of reflux episodes compared with asymptomatic controls. We studied in detail the characteristics of acid and weakly acidic reflux episodes temporally related to cough. A symptomatic reflux was defined as a reflux episode followed by cough in a two minute time window. Reflux episodes that occurred from 1 hour before to 1 hour after a symptomatic episode were considered as asymptomatic reflux controls. Symptomatic reflux episodes had a higher nadir ph (3.7) compared to asymptomatic reflux events (2.9). Furthermore, patients with a positive SAP between reflux and cough had more reflux episodes reaching the more proximal esophagus. [29] 6
9 A positive SAP between reflux and cough was found in 36 of 100 patients (9 SAP+ for acid reflux, 23 SAP+ for weakly acidic reflux and 4 SAP+ for both acid and weakly acidic reflux). These results imply that in a number of patients weakly acidic reflux can be the potential mechanism for chronic cough. Because most of these patients did not have an elevated number of reflux events, we believe that hypersensitivity to one or more components (non acid) of the refluxate might play a role in the etiology of cough. Previous studies revealed a higher prevalence of acid GER in patients with cystic fibrosis (CF). Moreover, CF patients with GER have a slightly poorer lung function than those without GER. [30] As in patients with chronic cough, we performed combined 24h impedance-phmanometry studies in a group of 23 CF adult patients. We found increased GER in a majority of the patients, mostly acid GER but with a subgroup having increased weakly acidic reflux. In these patients we found a significant correlation between esophageal acid exposure and the number of coughs/24h. We also found that reflux is a primary event in CF, and not a consequence of coughing. Only a small portion of the esophageal acid exposure and volume exposure was caused by cough. [31] Treatment of reflux related cough If increased GER can provoke chronic cough, treatment of GER should reduce cough. However, results of antireflux therapy in patients with cough are somehow disappointing. Kiljander et al. showed improvement of cough in 72 % of the patients in a placebo controlled study with PPI s. [32] On the contrary, other studies have shown a less good response rate. [33;34] In many of these studies, patients were asked to fill in a questionnaire about their symptoms, without using objective measurement for cough. Since it has been established that weakly acidic reflux could be a possible cause of chronic cough, treatment of cough-related weakly acidic reflux should be considered. The main mechanism for weakly acidic reflux are transient lower esophageal sphincter (LES) relaxations. Baclofen is a γ-aminobutyric acid agonist (GABA B -agonist) that reduces the number of reflux episodes by reducing the number of transient LES relaxations. Baclofen reduces weakly acidic reflux [35] and has also an antitussive effect. However, baclofen 7
10 has side effects like nausea and sedation and it is not well tolerated by several patients. New GABA B -agonists with less neurological side effects are under development. Azithromycin (AZI) belongs to the group of macrolide antibiotics, which are known to have prokinetic effects, and is often used in lung transplant patients (LTx). Lung transplantation has become an effective therapeutic option for end-stage pulmonary diseases, improving quality of life and prolongating survival. [36] An important factor in the long term outcome of these patients is the development of chronic allograft rejection (bronchiolitis obliterans syndrome, BOS), which is identified as a persistent drop in FEV 1 after transplantation. [36] Since GER has been implicated as a potential factor in the etiology of BOS, many studies have been done trying to clarify their relationship. In LTx, standard esophageal ph-monitoring revealed an increased acid exposure in 70 % of the patients. [37;38] We studied the effect of AZI on gastroesophageal reflux in LTx and found that AZI reduced esophageal acid and volume exposure as well as the number of proximal reflux events. [39] Furthermore, AZI reduced the concentration of bile acids found in BALF in these patients suggesting that GER and the risk of aspiration decreases on AZI. [40] In patients with clearly demonstrated association between reflux and cough but no response to full treatment with PPI s, antireflux surgery has been proposed. The rationale, being the persistence of non-acid reflux in spite of PPI s. So far, uncontrolled studies are encouraging [41-43], and there is a need for new outcome controlled studies with objective cough measurements before and after surgery to consolidate the recommendation for antireflux surgery in patients with chronic cough not responding to PPI s. 8
11 Figure Legend: Figure 1: Tracing of esophageal impedance-ph combined with manometry: example of a weakly acidic reflux followed by a cough burst. Impedance tracing shows a retrograde movement of a liquid bolus, with a drop in esophageal ph of more than 1 ph unit but remaining above 4 (weakly acidic reflux). A cough burst is shown manometrically as phasic, short duration, rapid pressure rises occurring simultaneously and with the same pressure configuration at all manometric recording sites. Cough occurred 25.4 seconds after the onset of a weakly acidic reflux event. 9
12 Reference List [1] Vakil N, Van Zanten SV, Kahrilas P et al. [The Montreal definition and classification of gastroesophageal reflux disease: a global, evidence-based consensus paper]. Z Gastroenterol 2007;45(11): [2] Richter JE. Review article: extraoesophageal manifestations of gastrooesophageal reflux disease. Aliment Pharmacol Ther 2005;22 Suppl 1: [3] Irwin RS, Corrao WM, Pratter MR. Chronic persistent cough in the adult: the spectrum and frequency of causes and successful outcome of specific therapy. Am Rev Respir Dis 1981;123(4 Pt 1): [4] Jaspersen D, Kulig M, Labenz J et al. Prevalence of extra-oesophageal manifestations in gastro-oesophageal reflux disease: an analysis based on the ProGERD Study. Aliment Pharmacol Ther 2003;17(12): [5] Irwin RS, Curley FJ. Is the anatomic, diagnostic work-up of chronic cough not all that it is hacked up to be? Chest 1989;95(4): [6] Irwin RS, Curley FJ, French CL. Chronic cough. The spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Am Rev Respir Dis 1990;141(3): [7] Irwin RS. Chronic cough due to gastroesophageal reflux disease: ACCP evidencebased clinical practice guidelines. Chest 2006;129(1): 80S-94S [8] Waring JP, Lacayo L, Hunter J et al. Chronic cough and hoarseness in patients with severe gastroesophageal reflux disease. Diagnosis and response to therapy. Dig Dis Sci 1995;40(5): [9] Fass R. Erosive esophagitis and nonerosive reflux disease (NERD): comparison of epidemiologic, physiologic, and therapeutic characteristics. J Clin Gastroenterol 2007;41(2):
13 [10] Jaspersen D. Extra-esophageal disorders in gastroesophageal reflux disease. Dig Dis 2004;22(2): [11] Silny, J. Intraluminal multiple electric impedance procedure for meaurement of gastrointestinal motility. 3, Ref Type: Generic [12] Sifrim D, Dupont L, Blondeau K et al. Weakly acidic reflux in patients with chronic unexplained cough during 24 hour pressure, ph, and impedance monitoring. Gut 2005;54(4): [13] Blondeau K, Dupont LJ, Mertens V et al. Improved diagnosis of gastrooesophageal reflux in patients with unexplained chronic cough. Aliment Pharmacol Ther 2007;25(6): [14] Coyle MA, Keenan DB, Henderson LS et al. Evaluation of an ambulatory system for the quantification of cough frequency in patients with chronic obstructive pulmonary disease. Cough 2005;1:3. [15] Paterson WG, Murat BW. Combined ambulatory esophageal manometry and dual-probe ph-metry in evaluation of patients with chronic unexplained cough. Dig Dis Sci 1994;39(5): [16] Bredenoord AJ, Weusten BL, Smout AJ. Symptom association analysis in ambulatory gastro-oesophageal reflux monitoring. Gut 2005;54(12): [17] Weusten BL, Roelofs JM, Akkermans LM et al. The symptom-association probability: an improved method for symptom analysis of 24-hour esophageal ph data. Gastroenterology 1994;107(6): [18] Lam HG, Breumelhof R, Roelofs JM et al. What is the optimal time window in symptom analysis of 24-hour esophageal pressure and ph data? Dig Dis Sci 1994;39(2):
14 [19] Oelschlager BK, Quiroga E, Isch JA et al. Gastroesophageal and pharyngeal reflux detection using impedance and 24-hour ph monitoring in asymptomatic subjects: defining the normal environment. J Gastrointest Surg 2006;10(1): [20] Ahrens P, Noll C, Kitz R et al. Lipid-laden alveolar macrophages (LLAM): a useful marker of silent aspiration in children. Pediatr Pulmonol 1999;28(2):83-8. [21] Parameswaran K, Anvari M, Efthimiadis A et al. Lipid-laden macrophages in induced sputum are a marker of oropharyngeal reflux and possible gastric aspiration. Eur Respir J 2000;16(6): [22] Koksal D, Ozkan B, Simsek C et al. Lipid-laden alveolar macrophage index in sputum is not useful in the differential diagnosis of pulmonary symptoms secondary to gastroesophageal reflux. Arch Med Res 2005;36(5): [23] Krishnan U, Mitchell JD, Tobias V et al. Fat laden macrophages in tracheal aspirates as a marker of reflux aspiration: a negative report. J Pediatr Gastroenterol Nutr 2002;35(3): [24] Blondeau K, Mertens V, Vanaudenaerde BA et al. Acid, non-acid GER and gastric aspiration in lung transplant patients with or without chronic rejection. Eur Respir J [25] Ing AJ, Ngu MC, Breslin AB. Pathogenesis of chronic persistent cough associated with gastroesophageal reflux. Am J Respir Crit Care Med 1994;149(1): [26] Irwin RS, Zawacki JK, Curley FJ et al. Chronic cough as the sole presenting manifestation of gastroesophageal reflux. Am Rev Respir Dis 1989;140(5): [27] Patterson RN, Johnston BT, Ardill JE et al. Increased tachykinin levels in induced sputum from asthmatic and cough patients with acid reflux. Thorax 2007;62(6):
15 [28] Javorkova N, Varechova S, Pecova R et al. Acidification of the oesophagus acutely increases the cough sensitivity in patients with gastro-oesophageal reflux and chronic cough. Neurogastroenterol Motil 2008;20(2): [29] Blondeau K, Mertens V, Dupont L et al. Characteristics of acid and weakly acidic reflux temporally related to cough. Gastroenterology 2006;130(4):A634. [30] Stringer DA, Sprigg A, Juodis E et al. The association of cystic fibrosis, gastroesophageal reflux, and reduced pulmonary function. Can Assoc Radiol J 1988;39(2): [31] Blondeau K, Dupont L, Mertens V et al. Gastroesophageal reflux and aspiration of gastric contents in adult patients with cystic fibrosis. Gut [32] Kiljander TO, Salomaa ER, Hietanen EK et al. Chronic cough and gastrooesophageal reflux: a double-blind placebo-controlled study with omeprazole. Eur Respir J 2000;16(4): [33] Ours TM, Kavuru MS, Schilz RJ et al. A prospective evaluation of esophageal testing and a double-blind, randomized study of omeprazole in a diagnostic and therapeutic algorithm for chronic cough. Am J Gastroenterol 1999;94(11): [34] Poe RH, Harder RV, Israel RH et al. Chronic persistent cough. Experience in diagnosis and outcome using an anatomic diagnostic protocol. Chest 1989;95(4): [35] Vela MF, Tutuian R, Katz PO et al. Baclofen decreases acid and non-acid postprandial gastro-oesophageal reflux measured by combined multichannel intraluminal impedance and ph. Aliment Pharmacol Ther 2003;17(2): [36] Trulock EP, Edwards LB, Taylor DO et al. Registry of the International Society for Heart and Lung Transplantation: twenty-third official adult lung and heartlung transplantation report J Heart Lung Transplant 2006;25(8):
16 [37] Benden C, Aurora P, Curry J et al. High prevalence of gastroesophageal reflux in children after lung transplantation. Pediatr Pulmonol 2005;40(1): [38] D'Ovidio F, Mura M, Ridsdale R et al. The effect of reflux and bile acid aspiration on the lung allograft and its surfactant and innate immunity molecules SP-A and SP-D. Am J Transplant 2006;6(8): [39] Blondeau K, Mertens V, Vanaudenaerde B et al. The macrolide antibiotic azithromycin reduces gastroesophageal reflux in lung transplant patients. Gastroenterology 2007;132(4):A594. [40] Mertens V, Blondeau K, Vanaudenaerde BM et al. Azithromycin red uces bile acid aspiration in lung transplant recipients. Journal of Heart and Lung Transplantation 2008;27(2):S124. [41] Mainie I, Tutuian R, Agrawal A et al. Fundoplication eliminates chronic cough due to non-acid reflux identified by impedance ph monitoring. Thorax 2005;60(6): [42] Mainie I, Tutuian R, Agrawal A et al. Combined multichannel intraluminal impedance-ph monitoring to select patients with persistent gastro-oesophageal reflux for laparoscopic Nissen fundoplication. Br J Surg 2006;93(12): [43] Tutuian R, Mainie I, Agrawal A et al. Nonacid reflux in patients with chronic cough on acid-suppressive therapy. Chest 2006;130(2):
17
P ersistent cough for more than eight weeks is a common
 449 GASTRO-OESOPHAGEAL REFLUX Weakly acidic in patients with chronic unexplained cough during 24 hour pressure, ph, and impedance monitoring D Sifrim, L Dupont, K Blondeau, X Zhang, J Tack, J Janssens...
449 GASTRO-OESOPHAGEAL REFLUX Weakly acidic in patients with chronic unexplained cough during 24 hour pressure, ph, and impedance monitoring D Sifrim, L Dupont, K Blondeau, X Zhang, J Tack, J Janssens...
The relationship between gastroesophageal reflux and cough in children with chronic unexplained cough using combined impedance-ph-manometry recordings
 The relationship between gastroesophageal reflux and cough in children with chronic unexplained cough using combined impedance-ph-manometry recordings Kathleen Blondeau, Veerle Mertens, Lieven Dupont,
The relationship between gastroesophageal reflux and cough in children with chronic unexplained cough using combined impedance-ph-manometry recordings Kathleen Blondeau, Veerle Mertens, Lieven Dupont,
Characteristics of gastroesophageal reflux in patients with and without excessive gastroesophageal acid exposure
 13 Characteristics of gastroesophageal reflux in patients with and without excessive gastroesophageal acid exposure A.J. Bredenoord B.L.A.M. Weusten R. Timmer A.J.P.M. Smout Dept. of Gastroenterology,
13 Characteristics of gastroesophageal reflux in patients with and without excessive gastroesophageal acid exposure A.J. Bredenoord B.L.A.M. Weusten R. Timmer A.J.P.M. Smout Dept. of Gastroenterology,
Review article: the measurement of non-acid gastro-oesophageal reflux
 Alimentary Pharmacology & Therapeutics Review article: the measurement of non-acid gastro-oesophageal reflux A. J. P. M. SMOUT Department of Gastroenterology, University Medical Center Utrecht, Utrecht,
Alimentary Pharmacology & Therapeutics Review article: the measurement of non-acid gastro-oesophageal reflux A. J. P. M. SMOUT Department of Gastroenterology, University Medical Center Utrecht, Utrecht,
Reproducibility of multichannel intraluminal electrical impedance monitoring of gastroesophageal reflux
 3 Reproducibility of multichannel intraluminal electrical impedance monitoring of gastroesophageal reflux A.J. Bredenoord B.L.A.M. Weusten R. Timmer A.J.P.M. Smout Dept. of Gastroenterology, St. Antonius
3 Reproducibility of multichannel intraluminal electrical impedance monitoring of gastroesophageal reflux A.J. Bredenoord B.L.A.M. Weusten R. Timmer A.J.P.M. Smout Dept. of Gastroenterology, St. Antonius
Chronic cough and gastro-oesophageal reflux: a double-blind placebo-controlled study with omeprazole
 Eur Respir J 2000; 16: 633±638 Printed in UK ± all rights reserved Copyright #ERS Journals Ltd 2000 European Respiratory Journal ISSN 0903-1936 Chronic cough and gastro-oesophageal reflux: a double-blind
Eur Respir J 2000; 16: 633±638 Printed in UK ± all rights reserved Copyright #ERS Journals Ltd 2000 European Respiratory Journal ISSN 0903-1936 Chronic cough and gastro-oesophageal reflux: a double-blind
Minimum sample frequency for multichannel intraluminal impedance measurement of the oesophagus
 Neurogastroenterol Motil (2004) 16, 713 719 doi: 10.1111/j.1365-2982.2004.00575.x Minimum sample frequency for multichannel intraluminal impedance measurement of the oesophagus A. J. BREDENOORD,* B. L.
Neurogastroenterol Motil (2004) 16, 713 719 doi: 10.1111/j.1365-2982.2004.00575.x Minimum sample frequency for multichannel intraluminal impedance measurement of the oesophagus A. J. BREDENOORD,* B. L.
127 Chapter 1 Chapter 2 Chapter 3
 CHAPTER 8 Summary Summary 127 In Chapter 1, a general introduction on the principles and applications of intraluminal impedance monitoring in esophageal disorders is provided. Intra-esophageal impedance
CHAPTER 8 Summary Summary 127 In Chapter 1, a general introduction on the principles and applications of intraluminal impedance monitoring in esophageal disorders is provided. Intra-esophageal impedance
Refractory GERD: What s a Gastroenterologist To Do?
 Refractory GERD: What s a Gastroenterologist To Do? Philip O. Katz, MD, FACG Chairman, Division of Gastroenterology Einstein Medical Center Clinical Professor of Medicine Jefferson Medical College Philadelphia,
Refractory GERD: What s a Gastroenterologist To Do? Philip O. Katz, MD, FACG Chairman, Division of Gastroenterology Einstein Medical Center Clinical Professor of Medicine Jefferson Medical College Philadelphia,
ORIGINAL ARTICLES ALIMENTARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:379 384 ORIGINAL ARTICLES ALIMENTARY TRACT Baclofen Improves Symptoms and Reduces Postprandial Flow Events in Patients With Rumination and Supragastric
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:379 384 ORIGINAL ARTICLES ALIMENTARY TRACT Baclofen Improves Symptoms and Reduces Postprandial Flow Events in Patients With Rumination and Supragastric
Baclofen decreases acid and non-acid post-prandial gastro-oesophageal reflux measured by combined multichannel intraluminal impedance and ph
 Aliment Pharmacol Ther 23; 17: 243 21. doi: 1.146/j.136-236.23.1394.x decreases acid and non-acid post-prandial gastro-oesophageal reflux measured by combined multichannel intraluminal impedance and ph
Aliment Pharmacol Ther 23; 17: 243 21. doi: 1.146/j.136-236.23.1394.x decreases acid and non-acid post-prandial gastro-oesophageal reflux measured by combined multichannel intraluminal impedance and ph
Findings of impedance ph-monitoring in patients with atypical gastroesophageal reflux symptoms
 Gastroenterology and Hepatology From Bed to Bench. 2013 RIGLD, Research Institute for Gastroenterology and Liver Diseases ORIGINAL ARTICLE Findings of impedance ph-monitoring in patients with atypical
Gastroenterology and Hepatology From Bed to Bench. 2013 RIGLD, Research Institute for Gastroenterology and Liver Diseases ORIGINAL ARTICLE Findings of impedance ph-monitoring in patients with atypical
J Neurogastroenterol Motil, Vol. 16 No. 3 July, 2010 DOI: /jnm Journal of Neurogastroenterology and Motility
 ㅋ JNM J Neurogastroenterol Motil, Vol. 16 No. 3 July, 2010 DOI: 10.5056/jnm.2010.16.3.258 Journal of Neurogastroenterology and Motility Review The Role of Weakly Acidic Reflux in Proton Pump Inhibitor
ㅋ JNM J Neurogastroenterol Motil, Vol. 16 No. 3 July, 2010 DOI: 10.5056/jnm.2010.16.3.258 Journal of Neurogastroenterology and Motility Review The Role of Weakly Acidic Reflux in Proton Pump Inhibitor
Refractory GERD : case presentation and discussion
 Refractory GERD : case presentation and discussion Ping-Huei Tseng National Taiwan University Hospital May 19, 2018 How effective is PPI based on EGD? With GERD symptom 75% erosive 25% NERD Endoscopy 81%
Refractory GERD : case presentation and discussion Ping-Huei Tseng National Taiwan University Hospital May 19, 2018 How effective is PPI based on EGD? With GERD symptom 75% erosive 25% NERD Endoscopy 81%
Gastroesophageal Reflux Disease in Infants and Children
 Gastroesophageal Reflux Disease in Infants and Children 4 Marzo 2017 Drssa Chiara Leoni Drssa Valentina Giorgio pediatriagastro@gmail.com valentinagiorgio1@gmail.com Definitions: GER GER is the passage
Gastroesophageal Reflux Disease in Infants and Children 4 Marzo 2017 Drssa Chiara Leoni Drssa Valentina Giorgio pediatriagastro@gmail.com valentinagiorgio1@gmail.com Definitions: GER GER is the passage
Maximizing Outcome of Extraesophageal Reflux Disease. (GERD) is often accompanied
 is often accompanied") ...PRESENTATIONS... Maximizing Outcome of Extraesophageal Reflux Disease Based on a presentation by Peter J. Kahrilas, MD Presentation Summary Gastroesophageal reflux disease (GERD) accompanied by regurgitation
...PRESENTATIONS... Maximizing Outcome of Extraesophageal Reflux Disease Based on a presentation by Peter J. Kahrilas, MD Presentation Summary Gastroesophageal reflux disease (GERD) accompanied by regurgitation
Bile Acids Aspiration Reduces Survival in Lung Transplant Recipients with BOS Despite Azithromycin
 American Journal of Transplantation 2011; 11: 329 335 Wiley Periodicals Inc. C 2011 The Authors Journal compilation C 2011 The American Society of Transplantation and the American Society of Transplant
American Journal of Transplantation 2011; 11: 329 335 Wiley Periodicals Inc. C 2011 The Authors Journal compilation C 2011 The American Society of Transplantation and the American Society of Transplant
The Role of Microaspiration in the Pathogenesis of Gastroesophageal Reflux-related Chronic Cough
 JNM J Neurogastroenterol Motil, Vol. 23 No. 1 January, 2017 pissn: 2093-0879 eissn: 2093-0887 https://doi.org/10.5056/jnm16057 Original Article The Role of Microaspiration in the Pathogenesis of Gastroesophageal
JNM J Neurogastroenterol Motil, Vol. 23 No. 1 January, 2017 pissn: 2093-0879 eissn: 2093-0887 https://doi.org/10.5056/jnm16057 Original Article The Role of Microaspiration in the Pathogenesis of Gastroesophageal
Gastroesophageal reflux disease (GERD) is a common chronic
 is a common chronic") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:743 748 Efficacy of Esophageal Impedance/pH Monitoring in Patients With Refractory Gastroesophageal Reflux Disease, on and off Therapy JASON M. PRITCHETT,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:743 748 Efficacy of Esophageal Impedance/pH Monitoring in Patients With Refractory Gastroesophageal Reflux Disease, on and off Therapy JASON M. PRITCHETT,*
Systematic review: role of acid, weakly acidic and weakly alkaline reflux in gastroesophageal reflux disease
 Systematic review: role of acid, weakly acidic and weakly alkaline reflux in gastroesophageal reflux disease Guy E Boeckxstaens, Smout J Smout To cite this version: Guy E Boeckxstaens, Smout J Smout. Systematic
Systematic review: role of acid, weakly acidic and weakly alkaline reflux in gastroesophageal reflux disease Guy E Boeckxstaens, Smout J Smout To cite this version: Guy E Boeckxstaens, Smout J Smout. Systematic
Rhinosinusitis, Laryngopharyngeal Reflux and Cough: an ENT Viewpoint
 Rhinosinusitis, Laryngopharyngeal Reflux and Cough: an ENT Viewpoint Hesham Saleh To cite this version: Hesham Saleh. Rhinosinusitis, Laryngopharyngeal Reflux and Cough: an ENT Viewpoint. Pulmonary Pharmacology
Rhinosinusitis, Laryngopharyngeal Reflux and Cough: an ENT Viewpoint Hesham Saleh To cite this version: Hesham Saleh. Rhinosinusitis, Laryngopharyngeal Reflux and Cough: an ENT Viewpoint. Pulmonary Pharmacology
GERD: A linical Clinical Clinical Update Objectives
 GERD: A Clinical Update Jeff Gilbert, M.D. University i of Kentucky Gastroenterology 11/6/08 Objectives To review the basic pathophysiology underlying gastroesophageal reflux disease To highlight current
GERD: A Clinical Update Jeff Gilbert, M.D. University i of Kentucky Gastroenterology 11/6/08 Objectives To review the basic pathophysiology underlying gastroesophageal reflux disease To highlight current
The most widely accepted tool for the diagnosis of
 Evaluation of Gastroesophageal Reflux Events in Children Using Multichannel Intraluminal Electrical Impedance Tobias G. Wenzl, MD The majority of gastroesophageal reflux (GER) episodes in infants and children
Evaluation of Gastroesophageal Reflux Events in Children Using Multichannel Intraluminal Electrical Impedance Tobias G. Wenzl, MD The majority of gastroesophageal reflux (GER) episodes in infants and children
GERD is a condition which develops when the reflux of stomach contents causes troublesome symptoms and/or complications
 GERD is a condition which develops when the reflux of stomach contents causes troublesome symptoms and/or complications Esophageal Syndromes Extra - esophageal Syndromes Symptomatic Syndromes Typical reflux
GERD is a condition which develops when the reflux of stomach contents causes troublesome symptoms and/or complications Esophageal Syndromes Extra - esophageal Syndromes Symptomatic Syndromes Typical reflux
Successful resolution of refractory chronic cough induced by gastroesophageal reflux with treatment of baclofen
 Xu et al. Cough, 8:8 Cough CASE REPORT Open Access Successful resolution of refractory chronic cough induced by gastroesophageal reflux with treatment of baclofen Xianghuai Xu, Qiang Chen, Siwei Liang,
Xu et al. Cough, 8:8 Cough CASE REPORT Open Access Successful resolution of refractory chronic cough induced by gastroesophageal reflux with treatment of baclofen Xianghuai Xu, Qiang Chen, Siwei Liang,
GERD DIAGNOSIS & TREATMENT DISCLOSURES 4/18/2018
 GERD DIAGNOSIS & TREATMENT Subhash Chandra MBBS Assistant Professor CHI Health Clinic Gastroenterology Creighton University, School of Medicine April 28, 2018 DISCLOSURES None 1 OBJECTIVES Review update
GERD DIAGNOSIS & TREATMENT Subhash Chandra MBBS Assistant Professor CHI Health Clinic Gastroenterology Creighton University, School of Medicine April 28, 2018 DISCLOSURES None 1 OBJECTIVES Review update
Cough regardless of etiology and duration is the
 GASTROENTEROLOGY 2010;139:754 762 CLINICAL Acoustic Cough Reflux Associations in Chronic Cough: Potential Triggers and Mechanisms JACLYN A. SMITH,* SAMANTHA DECALMER,* ANGELA KELSALL,*, KEVIN McGUINNESS,*,
GASTROENTEROLOGY 2010;139:754 762 CLINICAL Acoustic Cough Reflux Associations in Chronic Cough: Potential Triggers and Mechanisms JACLYN A. SMITH,* SAMANTHA DECALMER,* ANGELA KELSALL,*, KEVIN McGUINNESS,*,
A model for calculation of growth and feed intake in broiler chickens on the basis of feed composition and genetic features of broilers
 A model for calculation of growth and feed intake in broiler chickens on the basis of feed composition and genetic features of broilers Bernard Carré To cite this version: Bernard Carré. A model for calculation
A model for calculation of growth and feed intake in broiler chickens on the basis of feed composition and genetic features of broilers Bernard Carré To cite this version: Bernard Carré. A model for calculation
Prevalence and Clinical Characteristics of Refractoriness to Optimal Proton Pump Inhibitor Therapy in Non-erosive Reflux Disease
 www.medscape.com Prevalence and Clinical Characteristics of Refractoriness to Optimal Proton Pump Inhibitor Therapy in Non-erosive Reflux Disease Mentore Ribolsi; Michele Cicala; Patrizia Zentilin; Matteo
www.medscape.com Prevalence and Clinical Characteristics of Refractoriness to Optimal Proton Pump Inhibitor Therapy in Non-erosive Reflux Disease Mentore Ribolsi; Michele Cicala; Patrizia Zentilin; Matteo
Four-Day Bravo ph Capsule Monitoring With and Without Proton Pump Inhibitor Therapy
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1083 1088 Four-Day Bravo ph Capsule Monitoring With and Without Proton Pump Inhibitor Therapy IKUO HIRANO, QING ZHANG, JOHN E. PANDOLFINO, and PETER J. KAHRILAS
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1083 1088 Four-Day Bravo ph Capsule Monitoring With and Without Proton Pump Inhibitor Therapy IKUO HIRANO, QING ZHANG, JOHN E. PANDOLFINO, and PETER J. KAHRILAS
A stepwise protocol for the treatment of refractory gastroesophageal reflux-induced chronic cough
 Original Article A stepwise protocol for the treatment of refractory gastroesophageal reflux-induced chronic cough Xianghuai Xu*, Hanjing Lv*, Li Yu, Qiang Chen, Siwei Liang, Zhongmin Qiu Department of
Original Article A stepwise protocol for the treatment of refractory gastroesophageal reflux-induced chronic cough Xianghuai Xu*, Hanjing Lv*, Li Yu, Qiang Chen, Siwei Liang, Zhongmin Qiu Department of
ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease
 ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease Philip O. Katz MD 1, Lauren B. Gerson MD, MSc 2 and Marcelo F. Vela MD, MSCR 3 1 Division of Gastroenterology, Einstein
ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease Philip O. Katz MD 1, Lauren B. Gerson MD, MSc 2 and Marcelo F. Vela MD, MSCR 3 1 Division of Gastroenterology, Einstein
Achalasia is a rare disease with an annual incidence estimated REVIEWS. Erroneous Diagnosis of Gastroesophageal Reflux Disease in Achalasia
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:1020 1024 REVIEWS Erroneous Diagnosis of Gastroesophageal Reflux Disease in Achalasia BOUDEWIJN F. KESSING, ALBERT J. BREDENOORD, and ANDRÉ J. P. M. SMOUT
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:1020 1024 REVIEWS Erroneous Diagnosis of Gastroesophageal Reflux Disease in Achalasia BOUDEWIJN F. KESSING, ALBERT J. BREDENOORD, and ANDRÉ J. P. M. SMOUT
Gastroesophageal Reflux Evaluation in Patients Affected by Chronic Cough: Restech Versus Multichannel Intraluminal Impedance/pH Metry
 The Laryngoscope VC 2012 The American Laryngological, Rhinological and Otological Society, Inc. Gastroesophageal Reflux Evaluation in Patients Affected by Chronic Cough: Restech Versus Multichannel Intraluminal
The Laryngoscope VC 2012 The American Laryngological, Rhinological and Otological Society, Inc. Gastroesophageal Reflux Evaluation in Patients Affected by Chronic Cough: Restech Versus Multichannel Intraluminal
Acidic and Non-Acidic Reflux During Sleep Under Conditions of Powerful Acid Suppression*
 Original Research SLEEP MEDICINE Acidic and Non-Acidic Reflux During Sleep Under Conditions of Powerful Acid Suppression* William C. Orr, PhD; Andrea Craddock, PhD; and Suanne Goodrich, PhD Background:
Original Research SLEEP MEDICINE Acidic and Non-Acidic Reflux During Sleep Under Conditions of Powerful Acid Suppression* William C. Orr, PhD; Andrea Craddock, PhD; and Suanne Goodrich, PhD Background:
ACID REFLUX & GERD: The Unsettling Reality in Canada
 ACID REFLUX & GERD: The Unsettling Reality in Canada gerd fact 1 see page 8 Canadian Society of Intestinal Research On average, ARD patients wait over two years before seeking care 1. 1 gerd fact 2 see
ACID REFLUX & GERD: The Unsettling Reality in Canada gerd fact 1 see page 8 Canadian Society of Intestinal Research On average, ARD patients wait over two years before seeking care 1. 1 gerd fact 2 see
Patients with refractory gastroesophageal reflux disease: diagnostic tools
 INVITED REVIEW Annals of Gastroenterology (2012) 25, 1-6 Patients with refractory gastroesophageal reflux disease: diagnostic tools Georgios P. Karamanolis a, Daniel Sifrim b Aretaieion Hospital, Athens
INVITED REVIEW Annals of Gastroenterology (2012) 25, 1-6 Patients with refractory gastroesophageal reflux disease: diagnostic tools Georgios P. Karamanolis a, Daniel Sifrim b Aretaieion Hospital, Athens
EFFECT OF ITOPRIDE ON ESOPHAGEAL MOTILITY AND LOWER ESOPHAGEAL SPHINCTER FUNCTION IN MAN
 EFFECT OF ITOPRIDE ON ESOPHAGEAL MOTILITY AND LOWER ESOPHAGEAL SPHINCTER FUNCTION IN MAN Emidio Scarpellini, Rita Vos, Kathleen Blondeau, Veerle Boecxstaens, Ricard Farre, Antonio Gasbarrini, Jan Tack
EFFECT OF ITOPRIDE ON ESOPHAGEAL MOTILITY AND LOWER ESOPHAGEAL SPHINCTER FUNCTION IN MAN Emidio Scarpellini, Rita Vos, Kathleen Blondeau, Veerle Boecxstaens, Ricard Farre, Antonio Gasbarrini, Jan Tack
The Frequency of Gastroesophageal Reflux Disease in Nutcracker Esophagus and the Effect of Acid-Reduction Therapy on the Motor Abnormality
 Bahrain Medical Bulletin, Vol.22, No.4, December 2000 The Frequency of Gastroesophageal Reflux Disease in Nutcracker Esophagus and the Effect of Acid-Reduction Therapy on the Motor Abnormality Saleh Mohsen
Bahrain Medical Bulletin, Vol.22, No.4, December 2000 The Frequency of Gastroesophageal Reflux Disease in Nutcracker Esophagus and the Effect of Acid-Reduction Therapy on the Motor Abnormality Saleh Mohsen
Original Policy Date 12:2013
 MP 2.01.17 Esophageal ph Monitoring Medical Policy Section Medicine Issue 12:2013 Subsection Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature search/12:2013 Return to Medical
MP 2.01.17 Esophageal ph Monitoring Medical Policy Section Medicine Issue 12:2013 Subsection Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature search/12:2013 Return to Medical
Pharmacokinetics of caspofungin in a critically ill patient with liver cirrhosis
 Pharmacokinetics of caspofungin in a critically ill patient with liver cirrhosis Isabel Spriet, Wouter Meersseman, Pieter Annaert, Jan Hoon, Ludo Willems To cite this version: Isabel Spriet, Wouter Meersseman,
Pharmacokinetics of caspofungin in a critically ill patient with liver cirrhosis Isabel Spriet, Wouter Meersseman, Pieter Annaert, Jan Hoon, Ludo Willems To cite this version: Isabel Spriet, Wouter Meersseman,
pissn: eissn: Journal of Neurogastroenterology and Motility
 JNM J Neurogastroenterol Motil, Vol. 21 No. 3 July, 2015 pissn: 2093-0879 eissn: 2093-0887 http://dx.doi.org/10.5056/jnm15002 Journal of Neurogastroenterology and Motility Original Article Supragastric
JNM J Neurogastroenterol Motil, Vol. 21 No. 3 July, 2015 pissn: 2093-0879 eissn: 2093-0887 http://dx.doi.org/10.5056/jnm15002 Journal of Neurogastroenterology and Motility Original Article Supragastric
The association of and -related gastroduodenal diseases
 The association of and -related gastroduodenal diseases N. R. Hussein To cite this version: N. R. Hussein. The association of and -related gastroduodenal diseases. European Journal of Clinical Microbiology
The association of and -related gastroduodenal diseases N. R. Hussein To cite this version: N. R. Hussein. The association of and -related gastroduodenal diseases. European Journal of Clinical Microbiology
Obesity Is Associated With Increased Transient Lower Esophageal Sphincter Relaxation. Introduction. Predisposing factor. Introduction.
 Obesity Is Associated With Increased Transient Lower Esophageal Sphincter Relaxation Gastro Esophageal Reflux Disease (GERD) JUSTIN CHE-YUEN WU, et. al. The Chinese University of Hong Kong Gastroenterology,
Obesity Is Associated With Increased Transient Lower Esophageal Sphincter Relaxation Gastro Esophageal Reflux Disease (GERD) JUSTIN CHE-YUEN WU, et. al. The Chinese University of Hong Kong Gastroenterology,
Gastro-oesophageal reflux related cough and its response to laparoscopic fundoplication
 Thorax 1998;53:963 968 963 Departments of Medicine and Surgery, McMaster University, St Joseph s Hospital, Hamilton, Ontario, Canada L8N 4A6 C J Allen M Anvari Correspondence to: Dr C Allen. Received 10
Thorax 1998;53:963 968 963 Departments of Medicine and Surgery, McMaster University, St Joseph s Hospital, Hamilton, Ontario, Canada L8N 4A6 C J Allen M Anvari Correspondence to: Dr C Allen. Received 10
Esophageal Impedance: Role in the Evaluation of Esophageal Motility
 TZ CHI MED J June 2009 Vol 21 No 2 available at http://ajws.elsevier.com/tcmj Tzu Chi Medical Journal Review Article Esophageal Impedance: Role in the Evaluation of Esophageal Motility Chien-Lin Chen*
TZ CHI MED J June 2009 Vol 21 No 2 available at http://ajws.elsevier.com/tcmj Tzu Chi Medical Journal Review Article Esophageal Impedance: Role in the Evaluation of Esophageal Motility Chien-Lin Chen*
Virtual imaging for teaching cardiac embryology.
 Virtual imaging for teaching cardiac embryology. Jean-Marc Schleich, Jean-Louis Dillenseger To cite this version: Jean-Marc Schleich, Jean-Louis Dillenseger. Virtual imaging for teaching cardiac embryology..
Virtual imaging for teaching cardiac embryology. Jean-Marc Schleich, Jean-Louis Dillenseger To cite this version: Jean-Marc Schleich, Jean-Louis Dillenseger. Virtual imaging for teaching cardiac embryology..
La tasca acida nella MRGE: aspetti patogenetici e terapeutici
 La tasca acida nella MRGE: aspetti patogenetici e terapeutici Prof. VINCENZO SAVARINO Professore Ordinario di Gastroenterologia, Università degli Studi di Genova Direttore della Clinica Gastroenterologica
La tasca acida nella MRGE: aspetti patogenetici e terapeutici Prof. VINCENZO SAVARINO Professore Ordinario di Gastroenterologia, Università degli Studi di Genova Direttore della Clinica Gastroenterologica
Bilateral anterior uveitis secondary to erlotinib
 Bilateral anterior uveitis secondary to erlotinib Lik Thai Lim, Robert Alexander Blum, Chee Peng Cheng, Abdul Hanifudin To cite this version: Lik Thai Lim, Robert Alexander Blum, Chee Peng Cheng, Abdul
Bilateral anterior uveitis secondary to erlotinib Lik Thai Lim, Robert Alexander Blum, Chee Peng Cheng, Abdul Hanifudin To cite this version: Lik Thai Lim, Robert Alexander Blum, Chee Peng Cheng, Abdul
INTER-OBSERVER AND INTRA-OBSERVER AGREEMENT IN THE ANALYSIS OF
 UNIVERSITÀ DEGLI STUDI DI MILANO FACOLTA DI MEDICINA E CHIRURGIA DIPARTIMENTO DI FISIOPATOLOGIA MEDICO-CHIRURGICA E DEI TRAPIANTI CORSO DI DOTTORATO IN GASTROENTEROLOGIA CICLO XXV INTER-OBSERVER AND INTRA-OBSERVER
UNIVERSITÀ DEGLI STUDI DI MILANO FACOLTA DI MEDICINA E CHIRURGIA DIPARTIMENTO DI FISIOPATOLOGIA MEDICO-CHIRURGICA E DEI TRAPIANTI CORSO DI DOTTORATO IN GASTROENTEROLOGIA CICLO XXV INTER-OBSERVER AND INTRA-OBSERVER
CMEARTICLE. WHAT CAN I DO IN MY PRACTICE? History. Daphne Ang 1, MBBS, FRCP (Edin), Choon How How 2, MMed, FCFP, Tiing Leong Ang 1, MBBS, FRCP (Edin)
, Choon How How 2, MMed, FCFP, Tiing Leong Ang 1, MBBS, FRCP (Edin)") Singapore Med J 2016; 57(10): 546-551 10.11622/smedj.2016167 CMEARTICLE Persistent gastro-oesophageal reflux symptoms despite proton pump inhibitor therapy Daphne Ang 1, MBBS, FRCP (Edin), Choon How How
Singapore Med J 2016; 57(10): 546-551 10.11622/smedj.2016167 CMEARTICLE Persistent gastro-oesophageal reflux symptoms despite proton pump inhibitor therapy Daphne Ang 1, MBBS, FRCP (Edin), Choon How How
Simultaneous Intraesophageal Impedance and ph Measurement of Acid and Nonacid Gastroesophageal Reflux: Effect of Omeprazole
 GASTROENTEROLOGY 2001;120:1599 1606 Simultaneous Intraesophageal Impedance and ph Measurement of Acid and Nonacid Gastroesophageal Reflux: Effect of Omeprazole MARCELO F. VELA, LUCIANA CAMACHO LOBATO,
GASTROENTEROLOGY 2001;120:1599 1606 Simultaneous Intraesophageal Impedance and ph Measurement of Acid and Nonacid Gastroesophageal Reflux: Effect of Omeprazole MARCELO F. VELA, LUCIANA CAMACHO LOBATO,
Aerophagia, gastric, and supragastric belching: a study using intraluminal electrical impedance monitoring
 14 Aerophagia, gastric, and supragastric belching: a study using intraluminal electrical impedance monitoring A.J. Bredenoord B.L.A.M. Weusten D. Sifrim R. Timmer A.J.P.M. Smout Dept. of Gastroenterology,
14 Aerophagia, gastric, and supragastric belching: a study using intraluminal electrical impedance monitoring A.J. Bredenoord B.L.A.M. Weusten D. Sifrim R. Timmer A.J.P.M. Smout Dept. of Gastroenterology,
CHAPTER 3. J.M. Conchillo 1, N.Q. Nguyen 2, M. Samsom 1, R.H. Holloway 2, A.J.P.M. Smout 1
 CHAPTER 3 Multichannel ntraluminal impedance monitoring in the evaluation of patients with non-obstructive dysphagia J.M. Conchillo 1, N.Q. Nguyen 2, M. Samsom 1, R.H. Holloway 2, A.J.P.M. Smout 1 1 Department
CHAPTER 3 Multichannel ntraluminal impedance monitoring in the evaluation of patients with non-obstructive dysphagia J.M. Conchillo 1, N.Q. Nguyen 2, M. Samsom 1, R.H. Holloway 2, A.J.P.M. Smout 1 1 Department
TLESR, transient lower esophageal sphincter relaxation.
 GASTROENTEROLOGY 2010;139:409 417 CLINICAL Effects of Lesogaberan on Reflux and Lower Esophageal Sphincter Function in Patients With Gastroesophageal Reflux Disease GUY E. BOECKXSTAENS,*, HANNEKE BEAUMONT,*
GASTROENTEROLOGY 2010;139:409 417 CLINICAL Effects of Lesogaberan on Reflux and Lower Esophageal Sphincter Function in Patients With Gastroesophageal Reflux Disease GUY E. BOECKXSTAENS,*, HANNEKE BEAUMONT,*
Intraesophageal Impedance Monitoring Clinical Studies. J.M. Conchillo
 Intraesophageal Impedance Monitoring Clinical Studies J.M. Conchillo Intraesophageal Impedance Monitoring: Clinical Studies Conchillo Armendáriz, José Maria Thesis, University Utrecht, with summary in
Intraesophageal Impedance Monitoring Clinical Studies J.M. Conchillo Intraesophageal Impedance Monitoring: Clinical Studies Conchillo Armendáriz, José Maria Thesis, University Utrecht, with summary in
What can you expect from the lab?
 Role of the GI Motility Lab in the Diagnosis and Treatment of Esophageal Disorders Kenneth R. DeVault MD, FACG, FACP Professor and Chair Department of Medicine Mayo Clinic Florida What can you expect from
Role of the GI Motility Lab in the Diagnosis and Treatment of Esophageal Disorders Kenneth R. DeVault MD, FACG, FACP Professor and Chair Department of Medicine Mayo Clinic Florida What can you expect from
Survey of findings in patients having persistent heartburn on proton pump inhibitor therapy
 Diseases of the Esophagus (2014) (2016), 29, 27 33 DOI: 10.1111/dote.12293 Original article Survey of findings in patients having persistent heartburn on proton pump inhibitor therapy R. Mandaliya, 1 A.
Diseases of the Esophagus (2014) (2016), 29, 27 33 DOI: 10.1111/dote.12293 Original article Survey of findings in patients having persistent heartburn on proton pump inhibitor therapy R. Mandaliya, 1 A.
An Alternate, Egg-Free Radiolabeled Meal Formulation for Gastric-Emptying Scintigraphy
 An Alternate, Egg-Free Radiolabeled Meal Formulation for Gastric-Emptying Scintigraphy Philippe Garrigue, Aurore Bodin-Hullin, Sandra Gonzalez, Quentin Sala, Benjamin Guillet To cite this version: Philippe
An Alternate, Egg-Free Radiolabeled Meal Formulation for Gastric-Emptying Scintigraphy Philippe Garrigue, Aurore Bodin-Hullin, Sandra Gonzalez, Quentin Sala, Benjamin Guillet To cite this version: Philippe
Functional heartburn has more in common with functional dyspepsia than with non-erosive reflux disease
 1 Division of Gastroenterology, Department of Internal Medicine, University of Genoa, Genoa, Italy; 2 Division of Gastroenterology and Hepatology, Department of Internal Medicine, University Hospital Zurich,
1 Division of Gastroenterology, Department of Internal Medicine, University of Genoa, Genoa, Italy; 2 Division of Gastroenterology and Hepatology, Department of Internal Medicine, University Hospital Zurich,
GERD: How to. Failures
 GERD: How to Manage Treatment Failures John Fang MD University of Utah Introduction GERD: condition of reflux of stomach contents causes troublesome symptoms and/complications Refractory GERD: poor response
GERD: How to Manage Treatment Failures John Fang MD University of Utah Introduction GERD: condition of reflux of stomach contents causes troublesome symptoms and/complications Refractory GERD: poor response
Review article: identifying the causes of reflux events and symptoms new approaches
 Review article: identifying the causes of reflux events and symptoms new approaches M. Fox Nottingham Digestive Diseases Centre and Biomedical Research Unit, Queen s Medical Centre, University Hospital,
Review article: identifying the causes of reflux events and symptoms new approaches M. Fox Nottingham Digestive Diseases Centre and Biomedical Research Unit, Queen s Medical Centre, University Hospital,
Extraesophageal Manifestations of GERD in Children
 Extraesophageal Manifestations of GERD in Children Jose Luis Martinez, M.D. Associate Professor University of California San Francisco Director Endoscopy Unit Children s Hospital Central California Overview
Extraesophageal Manifestations of GERD in Children Jose Luis Martinez, M.D. Associate Professor University of California San Francisco Director Endoscopy Unit Children s Hospital Central California Overview
Enrichment culture of CSF is of limited value in the diagnosis of neonatal meningitis
 Enrichment culture of CSF is of limited value in the diagnosis of neonatal S. H. Chaudhry, D. Wagstaff, Anupam Gupta, I. C. Bowler, D. P. Webster To cite this version: S. H. Chaudhry, D. Wagstaff, Anupam
Enrichment culture of CSF is of limited value in the diagnosis of neonatal S. H. Chaudhry, D. Wagstaff, Anupam Gupta, I. C. Bowler, D. P. Webster To cite this version: S. H. Chaudhry, D. Wagstaff, Anupam
Esophageal ph Monitoring
 Esophageal ph Monitoring Policy Number: 2.01.20 Last Review: 11/2017 Origination: 11/2003 Next Review: 11/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for esophageal
Esophageal ph Monitoring Policy Number: 2.01.20 Last Review: 11/2017 Origination: 11/2003 Next Review: 11/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for esophageal
Unmet Needs in the Management of Gastroesophageal Reflux Disease
 Unmet Needs in the Management of Gastroesophageal Reflux Disease Ronnie Fass MD Professor of Medicine Case Western Reserve University Chairman, Division of Gastroenterology and Hepatology Director, Esophageal
Unmet Needs in the Management of Gastroesophageal Reflux Disease Ronnie Fass MD Professor of Medicine Case Western Reserve University Chairman, Division of Gastroenterology and Hepatology Director, Esophageal
Combined multichannel intraluminal impedance and. Characteristics of Consecutive Esophageal Motility Diagnoses After a Decade of Change
 ORIGINAL ARTICLE Characteristics of Consecutive Esophageal Motility Diagnoses After a Decade of Change Katherine Boland, BS,* Mustafa Abdul-Hussein, MD,* Radu Tutuian, MD,w and Donald O. Castell, MD* Background
ORIGINAL ARTICLE Characteristics of Consecutive Esophageal Motility Diagnoses After a Decade of Change Katherine Boland, BS,* Mustafa Abdul-Hussein, MD,* Radu Tutuian, MD,w and Donald O. Castell, MD* Background
Bile Acids in Sputum and Increased Airway Inflammation in Patients With Cystic Fibrosis
 CHEST Bile Acids in Sputum and Increased Airway Inflammation in Patients With Cystic Fibrosis Original Research Ans Pauwels, MSc ; Ann Decraene, PhD ; Kathleen Blondeau, PhD ; Veerle Mertens, PhD ; Ricard
CHEST Bile Acids in Sputum and Increased Airway Inflammation in Patients With Cystic Fibrosis Original Research Ans Pauwels, MSc ; Ann Decraene, PhD ; Kathleen Blondeau, PhD ; Veerle Mertens, PhD ; Ricard
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: esophageal_ph_monitoring 4/2011 5/2017 5/2018 5/2017 Description of Procedure or Service Acid reflux is the
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: esophageal_ph_monitoring 4/2011 5/2017 5/2018 5/2017 Description of Procedure or Service Acid reflux is the
Relationships between air swallowing, intragastric air, belching and gastro-oesophageal reflux
 16 Relationships between air swallowing, intragastric air, belching and gastro-oesophageal reflux A.J. Bredenoord B.L.A.M. Weusten R. Timmer L.M.A. Akkermans A.J.P.M. Smout Dept. of Gastroenterology, St.
16 Relationships between air swallowing, intragastric air, belching and gastro-oesophageal reflux A.J. Bredenoord B.L.A.M. Weusten R. Timmer L.M.A. Akkermans A.J.P.M. Smout Dept. of Gastroenterology, St.
Normal Values of Pharyngeal and Esophageal 24-Hour ph Impedance in Individuals on and off Therapy and Interobserver Reproducibility
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2013;11:366 372 ALIMENTARY TRACT Normal Values of Pharyngeal and Esophageal 24-Hour ph Impedance in Individuals on and off Therapy and Interobserver Reproducibility
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2013;11:366 372 ALIMENTARY TRACT Normal Values of Pharyngeal and Esophageal 24-Hour ph Impedance in Individuals on and off Therapy and Interobserver Reproducibility
Chronic persistent cough and gastro-oesophageal
 Thorax 1991;46:479-483 Department of Thoracic Medicine A J Ing A B X Breslin Department of Gastroenterology M C Ngu Concord Hospital, Sydney, NSW 2139, Australia Reprint requests to: Dr Ing Accepted 17
Thorax 1991;46:479-483 Department of Thoracic Medicine A J Ing A B X Breslin Department of Gastroenterology M C Ngu Concord Hospital, Sydney, NSW 2139, Australia Reprint requests to: Dr Ing Accepted 17
Determinants of reflux-induced chronic cough
 1/5 This site uses cookies. More info Home / Online First Article Text Article menu Neurogastroenterology Original article Determinants of reflux-induced chronic cough PDF Thomas V K Herregods 1, Ans Pauwels
1/5 This site uses cookies. More info Home / Online First Article Text Article menu Neurogastroenterology Original article Determinants of reflux-induced chronic cough PDF Thomas V K Herregods 1, Ans Pauwels
Sleeve sensor versus high-resolution manometry for the detection of transient lower esophageal sphincter relaxations
 6 Sleeve sensor versus high-resolution manometry for the detection of transient lower esophageal sphincter relaxations A.J. Bredenoord B.L.A.M. Weusten R. Timmer A.J.P.M. Smout Dept. of Gastroenterology,
6 Sleeve sensor versus high-resolution manometry for the detection of transient lower esophageal sphincter relaxations A.J. Bredenoord B.L.A.M. Weusten R. Timmer A.J.P.M. Smout Dept. of Gastroenterology,
Policy #: 138 Latest Review Date: November 2016
 Name of Policy: Ambulatory Esophageal ph Monitoring Policy #: 138 Latest Review Date: November 2016 Category: Medical Policy Grade: B Background/Definitions: As a general rule, benefits are payable under
Name of Policy: Ambulatory Esophageal ph Monitoring Policy #: 138 Latest Review Date: November 2016 Category: Medical Policy Grade: B Background/Definitions: As a general rule, benefits are payable under
Gastroesophageal reflux disease (GERD) is a frequent presentation
 is a frequent presentation") Insight Into the Relationship Between Gastroesophageal Reflux Disease and Asthma Fehmi Ates, MD, and Michael F. Vaezi, MD, PhD, MSc (Epi) Dr Ates is an associate professor of medicine at Mersin University
Insight Into the Relationship Between Gastroesophageal Reflux Disease and Asthma Fehmi Ates, MD, and Michael F. Vaezi, MD, PhD, MSc (Epi) Dr Ates is an associate professor of medicine at Mersin University
4/24/2015. History of Reflux Surgery. Recent Innovations in the Surgical Treatment of Reflux
 Recent Innovations in the Surgical Treatment of Reflux Scott Carpenter, DO, FACOS, FACS Mercy Hospital Ardmore Ardmore, OK History of Reflux Surgery - 18 th century- first use of term heartburn - 1934-
Recent Innovations in the Surgical Treatment of Reflux Scott Carpenter, DO, FACOS, FACS Mercy Hospital Ardmore Ardmore, OK History of Reflux Surgery - 18 th century- first use of term heartburn - 1934-
Review article: gastric acidity ) comparison of esomeprazole with other proton pump inhibitors
 comparison of esomeprazole with other proton pump inhibitors") Aliment Pharmacol Ther 2003; 17 (Suppl. 1): 10 15. Review article: gastric acidity ) comparison of esomeprazole with other proton pump inhibitors J. G. HATLEBAKK Department of Medicine, Haukeland Sykehus,
Aliment Pharmacol Ther 2003; 17 (Suppl. 1): 10 15. Review article: gastric acidity ) comparison of esomeprazole with other proton pump inhibitors J. G. HATLEBAKK Department of Medicine, Haukeland Sykehus,
Review article: extraoesophageal manifestations of gastro-oesophageal reflux disease
 Aliment Pharmacol Ther 2005; 22 (Suppl. 1): 70 80. Review article: extraoesophageal manifestations of gastro-oesophageal reflux disease J. E. RICHTER Department of Medicine, Temple University School of
Aliment Pharmacol Ther 2005; 22 (Suppl. 1): 70 80. Review article: extraoesophageal manifestations of gastro-oesophageal reflux disease J. E. RICHTER Department of Medicine, Temple University School of
Surgical Evaluation for Benign Esophageal Disease. Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018
 Surgical Evaluation for Benign Esophageal Disease Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018 Disclosures No disclosures relevant to this presentation. Objectives (for CME purposes)
Surgical Evaluation for Benign Esophageal Disease Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018 Disclosures No disclosures relevant to this presentation. Objectives (for CME purposes)
Gastroesophageal and extraesophageal symptoms in patients with gastroesophageal reflux disease: An endoscopy-based study in Albania
 ORIGINAL RESEARCH Gastroesophageal and extraesophageal symptoms in patients with gastroesophageal reflux disease: An endoscopy-based study in Albania Indrit Kellici 1,2, Bledar Kraja 1,3,4, Rozana Aleksi
ORIGINAL RESEARCH Gastroesophageal and extraesophageal symptoms in patients with gastroesophageal reflux disease: An endoscopy-based study in Albania Indrit Kellici 1,2, Bledar Kraja 1,3,4, Rozana Aleksi
Archived at the Flinders Academic Commons:
 Archived at the Flinders Academic Commons: http://dspace.flinders.edu.au/dspace/ This is the peer reviewed version of the following article: Fox M, Omari T, Rommel N. Supraesophageal Reflux Disease: Solving
Archived at the Flinders Academic Commons: http://dspace.flinders.edu.au/dspace/ This is the peer reviewed version of the following article: Fox M, Omari T, Rommel N. Supraesophageal Reflux Disease: Solving
Effects of anti-reflux surgery on chronic cough and asthma in patients with gastro-oesophageal reflux disease
 RESPIRATORY MEDICINE (2000) 94, 1166 1170 doi:10.1053/rmed.2000.0944, available online at http://www.idealibrary.com on Effects of anti-reflux surgery on chronic cough and asthma in patients with gastro-oesophageal
RESPIRATORY MEDICINE (2000) 94, 1166 1170 doi:10.1053/rmed.2000.0944, available online at http://www.idealibrary.com on Effects of anti-reflux surgery on chronic cough and asthma in patients with gastro-oesophageal
Putting Chronic Heartburn On Ice
 Putting Chronic Heartburn On Ice Over the years, gastroesophageal reflux disease has proven to be one of the most common complaints facing family physicians. With quicker diagnosis, this pesky ailment
Putting Chronic Heartburn On Ice Over the years, gastroesophageal reflux disease has proven to be one of the most common complaints facing family physicians. With quicker diagnosis, this pesky ailment
In vitro study of the effects of cadmium on the activation of the estrogen response element using the YES screen
 In vitro study of the effects of cadmium on the activation of the estrogen response element using the YES screen Xavier Denier, Jérome Couteau, Magalie Baudrimont, Elisabeth M. Hill, Jeanette Rotchell,
In vitro study of the effects of cadmium on the activation of the estrogen response element using the YES screen Xavier Denier, Jérome Couteau, Magalie Baudrimont, Elisabeth M. Hill, Jeanette Rotchell,
Related Policies None
 Medical Policy MP 2.01.20 BCBSA Ref. Policy: 2.01.20 Last Review: 11/30/2017 Effective Date: 11/30/2017 Section: Medicine Related Policies None DISCLAIMER Our medical policies are designed for informational
Medical Policy MP 2.01.20 BCBSA Ref. Policy: 2.01.20 Last Review: 11/30/2017 Effective Date: 11/30/2017 Section: Medicine Related Policies None DISCLAIMER Our medical policies are designed for informational
JNM Journal of Neurogastroenterology and Motility
 JNM Journal of Neurogastroenterology and Motility J Neurogastroenterol Motil, Vol. 18 No. 2 April, 2012 pissn: 2093-0879 eissn: 2093-0887 http://dx.doi.org/10.5056/jnm.2012.18.2.169 Original Article Bravo
JNM Journal of Neurogastroenterology and Motility J Neurogastroenterol Motil, Vol. 18 No. 2 April, 2012 pissn: 2093-0879 eissn: 2093-0887 http://dx.doi.org/10.5056/jnm.2012.18.2.169 Original Article Bravo
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Achalasia, barium esophagography for, 57 58 Acid pocket, 18 19 Acid-sensing ion, 20 Acupuncture, 128 Adiponectin, in obesity, 166 ADX10059 metabotropic
Note: Page numbers of article titles are in boldface type. A Achalasia, barium esophagography for, 57 58 Acid pocket, 18 19 Acid-sensing ion, 20 Acupuncture, 128 Adiponectin, in obesity, 166 ADX10059 metabotropic
ORIGINAL ARTICLE. Proximal Reflux as a Cause of Adult-Onset Asthma
 ORIGINAL ARTICLE Proximal Reflux as a Cause of Adult-Onset Asthma The Case for Hypopharyngeal Impedance Testing to Improve the Sensitivity of Diagnosis Yoshihiro Komatsu, MD; Toshitaka Hoppo, MD, PhD;
ORIGINAL ARTICLE Proximal Reflux as a Cause of Adult-Onset Asthma The Case for Hypopharyngeal Impedance Testing to Improve the Sensitivity of Diagnosis Yoshihiro Komatsu, MD; Toshitaka Hoppo, MD, PhD;
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Afferent nerves, interactions of, in cough, 20 21 Airway, eosinophilic inflammation of, 124 narrowing of, in asthma, 126 protection of, terms
Note: Page numbers of article titles are in boldface type. A Afferent nerves, interactions of, in cough, 20 21 Airway, eosinophilic inflammation of, 124 narrowing of, in asthma, 126 protection of, terms
From universal postoperative pain recommendations to procedure-specific pain management
 From universal postoperative pain recommendations to procedure-specific pain management Hélène Beloeil, Francis Bonnet To cite this version: Hélène Beloeil, Francis Bonnet. From universal postoperative
From universal postoperative pain recommendations to procedure-specific pain management Hélène Beloeil, Francis Bonnet To cite this version: Hélène Beloeil, Francis Bonnet. From universal postoperative
Iodide mumps: Sonographic appearance
 Iodide mumps: Sonographic appearance Salvatore Greco, Riccardo Centenaro, Giuseppe Lavecchia, Francesco Rossi To cite this version: Salvatore Greco, Riccardo Centenaro, Giuseppe Lavecchia, Francesco Rossi.
Iodide mumps: Sonographic appearance Salvatore Greco, Riccardo Centenaro, Giuseppe Lavecchia, Francesco Rossi To cite this version: Salvatore Greco, Riccardo Centenaro, Giuseppe Lavecchia, Francesco Rossi.
Effectiveness of Antireflux Surgery for the Cure of Chronic Cough Associated with Gastroesophageal Reflux Disease
 DOI 10.1007/s00268-014-2769-7 ORIGINAL SCIENTIFIC REPORT Effectiveness of Antireflux Surgery for the Cure of Chronic Cough Associated with Gastroesophageal Reflux Disease Marialuisa Lugaresi Beatrice Aramini
DOI 10.1007/s00268-014-2769-7 ORIGINAL SCIENTIFIC REPORT Effectiveness of Antireflux Surgery for the Cure of Chronic Cough Associated with Gastroesophageal Reflux Disease Marialuisa Lugaresi Beatrice Aramini
Medical Policy An independent licensee of the Blue Cross Blue Shield Association.
 Esophageal ph Monitoring Page 1 of 13 Medical Policy An independent licensee of the Blue Cross Blue Shield Association. Title: Esophageal ph Monitoring Professional Institutional Original Effective Date:
Esophageal ph Monitoring Page 1 of 13 Medical Policy An independent licensee of the Blue Cross Blue Shield Association. Title: Esophageal ph Monitoring Professional Institutional Original Effective Date:
Clinical Policy Title: Esophageal ph monitoring
 Clinical Policy Title: Esophageal ph monitoring Clinical Policy Number: CCP.1381 Effective Date: August 1, 2018 Initial Review Date: June 5, 2018 Most Recent Review Date: July 3, 2018 Next Review Date:
Clinical Policy Title: Esophageal ph monitoring Clinical Policy Number: CCP.1381 Effective Date: August 1, 2018 Initial Review Date: June 5, 2018 Most Recent Review Date: July 3, 2018 Next Review Date:
Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University
 Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University Asthma-related Comorbidities Comorbid conditions of the upper airways Rhinitis and Sinusitis
Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University Asthma-related Comorbidities Comorbid conditions of the upper airways Rhinitis and Sinusitis
Eosinophilic Esophagitis: Extraesophageal Manifestations
 Eosinophilic Esophagitis: Extraesophageal Manifestations Karen B. Zur, MD Director, Pediatric Voice Program Associate Director, Center for Pediatric Airway Disorders The Children s Hospital of Philadelphia
Eosinophilic Esophagitis: Extraesophageal Manifestations Karen B. Zur, MD Director, Pediatric Voice Program Associate Director, Center for Pediatric Airway Disorders The Children s Hospital of Philadelphia
Extraesophageal presentations of gastroesophageal reflux disease: the case for aggressive diagnosis and treatment
 JOEL E. RICHTER, MD Dr. Richter is chairman of the Department of Gastroenterology at the Cleveland Clinic Foundation, specializing in esophageal diseases with particular interest in GERD, achalasia, and
JOEL E. RICHTER, MD Dr. Richter is chairman of the Department of Gastroenterology at the Cleveland Clinic Foundation, specializing in esophageal diseases with particular interest in GERD, achalasia, and
Gastroesophageal Reflux Disease, Paraesophageal Hernias &
 530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
Mathieu Hatt, Dimitris Visvikis. To cite this version: HAL Id: inserm
 Defining radiotherapy target volumes using 18F-fluoro-deoxy-glucose positron emission tomography/computed tomography: still a Pandora s box?: in regard to Devic et al. (Int J Radiat Oncol Biol Phys 2010).
Defining radiotherapy target volumes using 18F-fluoro-deoxy-glucose positron emission tomography/computed tomography: still a Pandora s box?: in regard to Devic et al. (Int J Radiat Oncol Biol Phys 2010).