Proton Pump Inhibitors and the Treatment of GERD, Dyspepsia, NSAID-associated Peptic Ulcer Disease
|
|
|
- Angelica Wright
- 6 years ago
- Views:
Transcription


1 Pharmacist Presentation Proton Pump Inhibitors and the Treatment of GERD, Dyspepsia, NSAID-associated Peptic Ulcer Disease Presenter Title Affiliation Date
2 Disclaimer The information in this presentation is not a substitute for clinical judgement in the care of a particular patient. CADTH is not liable for any damages arising from the use or misuse of any information contained in or implied by the information in this presentation. The statements, conclusions and views expressed herein do not necessarily represent the view of Health Canada or any Provincial or Territorial Government. Made possible through funding from Health Canada. Copyright 2007 CADTH
3 Statement of disclosure
4 Goals Assist you to identify potential clinical situations where proton pump inhibitor (PPI) prescribing may not be consistent with optimal drug therapy Identify key references and tools to assist in the optimal prescribing and use of PPIs Create an awareness of optimal drug therapy information from the Canadian Agency for Drugs and Technologies in Health (CADTH)
5 Objectives Review the use of Proton Pump Inhibitors (PPIs) in the treatment of: GERD Dyspepsia Peptic ulcer disease (NSAID induced & H.Pylori) Review evidence for following PPI issues: Efficacy of one PPI vs. another Double-dose PPI as initial therapy Role in asthma, laryngeal symptoms & chronic cough associated with GERD
6 Background Who is CADTH? What is COMPUS? How were the PPI evidence-based statements developed? Process for identifying evidence-based optimal therapy Why focus on PPIs?
7 Who is CADTH? Health Technology Assessment Common Drug Review COMPUS
8 What is COMPUS? Identify evidencebased optimal drug therapy Evaluate current use & identify gaps Provide strategies & tools Support & encourage informed decision making Build networks & partnerships
9 CADTH Stakeholders: Physicians, pharmacists, nurses, other allied health professionals Federal/Provincial/Territorial Governments Consumers Manufacturers Collaborators in Canada and internationally
10 Identifying the evidence Clinical Practice Guidelines (CPGs) & Consensus Documents (CDs) Extracted PPI related recommendations and statements Compiled a synopsis of existing statements and recommendations Evaluated all relevant cited references (AMSTAR SR, adapted SIGN 50 checklist observational ) RCT, cohort, Identified & evaluated relevant new evidence not yet incorporated in the CPGs
11 Identifying optimal drug therapy PPI Expert Review Panel reviewed results, decided on final wording, and voted on statements Stakeholder feedback/input (preliminary scientific report containing statements and evidence posted on web) Published scientific report March 2007 Developed tools/strategies to support implementation of Optimal Drug Therapy
12 PPI Expert Review Panel BC Dr. J. Rideout Family Physician AB Dr. S. van Zanten Gastroenterologist AB Dr. A. Thomson Gastroenterologist SK Dr. M. Caughlin Family Physician SK Dr. B. Schuster Pharmacist MB Dr. L. Targownik Gastroenterologist ON Dr. A. Holbrook Pharmacologist ON Dr. M. Brouwers Methodologist ON Ron Goeree Health Economist ON Dr. M. Man-Son-Hing Geriatrician ON Dr. J. Marshall Gastroenterologist NS Pam McLean-Veysey Pharmacist
13 Why focus on PPIs? Adoption of optimal therapy would have an impact on a large number of Canadians. Criteria included Over or under- use of prescription medications Size of patient population Potential impact on health outcomes Cost-effectiveness Potential to effect change Benefit to multiple jurisdictions Measurable outcomes
14 Why focus on PPIs? Commonly prescribed, potentially over-utilized Canada PPI prescriptions dispensed increased by 15% million million CADTH 2007
15 Background Estimated total PPI retail pharmacy sales in Canada: Millions of Dollars % increase Year Source: IMS HEALTH, CANADA. Reprinted with permission of IMS HEALTH, CANADA
16 CADTH 2007 Evidence for PPI Use in gastroesophageal reflux disease, dyspepsia and peptic ulcer disease
17 Canadian Dyspepsia Working Group Definition Dyspepsia is a symptom complex of epigastric pain or discomfort thought to originate in the upper gastrointestinal tract, and it may include any of the following symptoms: heartburn, acid regurgitation, excessive burping/belching, increased abdominal bloating, nausea, feeling of abnormal/slow digestion or early satiety. Van Zanten 2000
18 Five key decision points in the approach to patients with uninvestigated dyspepsia 1. Are there other possible causes for the symptoms? 2. Does patient have Alarm symptoms (VBAD) or >50years of age? 3. Is the patient using NSAIDs (including ASA)? 4. Is the dominant symptom heartburn, acid regurgitation, or both? 5. Is the patient infected with H. Pylori? Van Zanten 2000
19 Are there other possible causes for the symptoms? Cardiac Hepatobiliary Medication-induced Lifestyle Treat as appropriate Dietary indiscretion Van Zanten 2000
20 Example medications associated with dyspepsia/esophagitis NSAIDS/ASA/COX2 inhibitors acarbose (Glucobay ) alcohol alendronate (Fosamax ) corticosteroids metformin (Glucophage ) antibiotics (erythromycin) orlistat (Xenical ) potassium theophylline iron Thomson 2002 Bazaldua 1999
21 Herbs that may cause dyspepsia HERB Garlic Gingko Saw palmetto Feverfew White willow SIDE EFFECT Stomach burning, nausea Mild GI disturbances Upset stomach GI disturbances Possible ADR similar to salicylates Thomson 2002 Bazaldua 1999
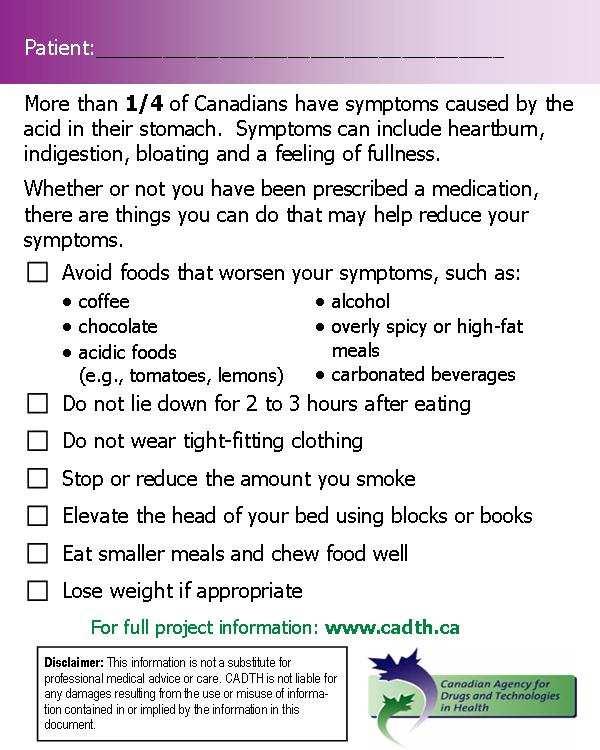
22 Lifestyle modifications to consider Thomson 2002 Kaltenbach 2006 Heidelbaugh 2003 Small frequent meals Elevate head of bed Avoid tight fitting clothes avoid laying down for 2-3 hours after eating stop/reduce smoking, alcohol & caffeine avoid irritating foods that precipitate event lose weight/maintain an ideal weight review medications stress reduction
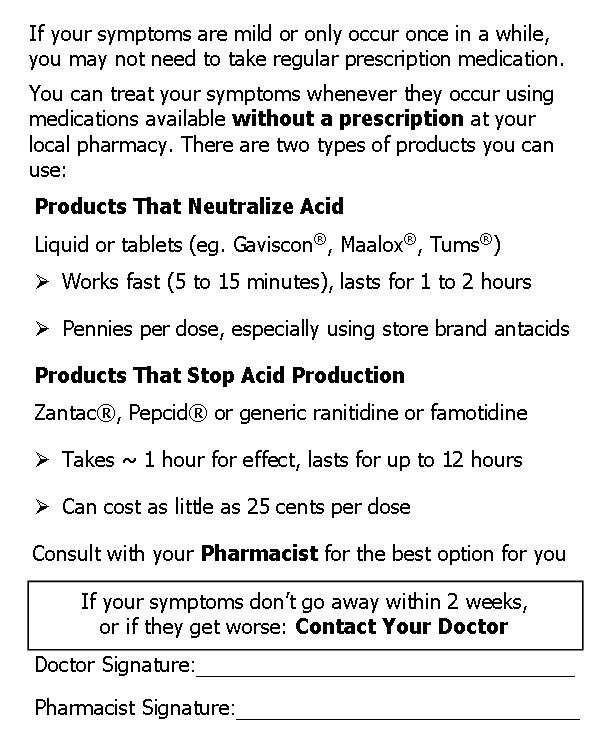
23 OTCs for dietary indiscretion, mildintermittent symptoms Antacids limited evidence Dose of antacids is based on acid-neutralizing capacity of individual products Works fast (5-15 minutes) Frequent dosing, volume of liquid and taste can be a challenge constipating=calcium, aluminum diarrhea =magnesium Mg/Al antacids eg.maalox, Mylanta preferred as constipating effect of Al +2 counterbalanced by laxative effect of Mg +2 Consider concurrent clinical conditions & convenience (e.g.renal failure & use of Mg and Al containing antacids) Thomson 2002
24 OTCs for dietary indiscretion, mildintermittent symptoms H2RAs (Famotidine Pepcid AC, Complete, ranitidine Zantac ) Symptom relief similar to antacids, but takes 1 hour for effect duration of effect is longer Famotidine 10mg -ranitidine 75mg 30 tablets $12 (generic <$10) Famotidine 10mg/Ca Carb/MgOH (Pepcid Complete ) 10 tabs $9 Famotidine 20mg, ranitidine 150mg pkg size 30 tabs *if on a regular H2RA or PPI, can use an OTC product for occasional symptoms related to dietary indiscretion Thomson 2002
25 Does patient have alarm symptoms (VBAD) or is patient >50yrs? Refer back to physician when... Age > 50 or alarm features Vomiting Bleeding/anemia Abdominal mass/unexplained weight loss Dysphagia Van Zanten 2000
26 Is the patient using NSAIDs (including ASA)? If on NSAID, STOP therapy If symptoms resolve & still need analgesic/ anti-inflammatory Avoid NSAID, if possible (acetaminophen) If NSAID must be used : lowest dose shortest duration Van Zanten 2000
27 Is the patient using NSAIDs (including ASA)? If NSAID must be continued For treatment of NSAID induced ulcer; standard dose PPI x 4-8 weeks provides higher healing rates than H2RAs & misoprostol 800mcg/day Overall success rate healed ulcer, <5 erosions, mild dyspepsia in study of omeprazole 20mg, 40mg, and ranitidine 300mg daily (n=541): Omeprazole 40mg: 79% Omeprazole 20mg: 80% Ranitidine: 63% Overall success rate healed ulcer, <5 erosions, mild dyspepsia in study of omeprazole 20mg, 40mg, and misoprostol 800mcg daily (n=935): Omeprazole 40mg: 75% Omeprazole 20mg: 76% Misoprostol: 71% NS p<0.001, NNT = 6 (95% CI: 4-13) NS NS CADTH 2007
28 Is the patient using NSAIDs (including ASA)? Do not need double dose PPI 2 RCTs n=1476 : double dose omeprazole was not superior to single dose, both doses more efficacious than H2RA and misoprostol Different PPIs produce similar healing rates for NSAID-associated ulcer. CADTH 2007 McDonagh systematic review: 3 RCTs allowed for indirect comparison of healing rates: Omeprazole: 84-93% Lansoprazole: 81-93%
29 NSAID ulcer prophylaxis Secondary prevention of gastric and duodenal ulcers: Standard-dose PPIs are more efficacious than standard-dose H2RA NNT GU =10 (95% CI: 8-17) NNT DU =27 (95% CI: ) Standard-dose PPIs have similar efficacy to misoprostol mcg/day No significant differences in terms of DU and GU relapse at 6 months CADTH 2007
30 Who should be considered for NSAID prophylaxis? Prior history of GI event (ulcer, hemorrhage) Age >60 years High NSAID dosage (>2x normal dose) Patients on warfarin and NSAID Patients on corticosteroid and NSAID All patients taking NSAIDS do not require prophylaxis. Lanza 1998


31 Is the dominant symptom heartburn or acid regurgitation? 0 A burning feeling rising from the stomach or lower chest towards the neck
32 GERD/Esophagitis definitions Uninvestigated GERD: dominant symptoms of heartburn and/or regurgitation which may be associated with other symptoms such as epigastric pain/discomfort and not investigated by endoscopy (or upper GI series) Erosive esophagitis: the presence of reflux symptoms and any length of mucosal break in the esophagus as a result of gastroesopageal reflux Endoscopy-negative reflux disease (ENRD): applies to individuals with GERD who have normal endoscopy results while off treatment Armstrong 2005 Vakil 2006 CADTH 2007
33 GERD treatment PPIs or H2RAs? Although H2RA therapy is effective in managing many patients, standard dose PPIs are superior to H2RAs in the initial & maintenance management of uninvestigated GERD and erosive esophagitis. PPIs have a similar adverse event rate (generally minor) as H2RAs. CADTH 2007
34 Uninvestigated GERD initial therapy Standard-dose PPIs, for up to four weeks, are more efficacious than H2RAs for improvement of reflux symptoms in uninvestigated GERD. 5 RCTS, N=1896 Patient pop n: most had at least moderate heartburn Outcomes: Heartburn relief Time to relief, regurgitation, epigastric pain Symptom relief with initial 4-8 weeks: PPIs 55-75% H2RAs 27-58%, p<0.001 NNT 4-6 (95% CI 4-8 weeks Higher healing 8 wks CADTH 2007
35 Uninvestigated GERD maintenance therapy PPI therapy in uninvestigated GERD is more efficacious than H2RAs for control of symptoms, for up to six months. 3 RCTs, duration 20 weeks to 1 year, N=3056 Patients with heartburn dominant symptoms 1-year study, pantoprazole 20 mg daily vs ranitidine 150 mg bid Complete symptom control at 6 months Pantoprazole 71% Ranitidine 56% NNT 7 (95% CI 4-23) Complete symptom control at 12 months Pantoprazole 77% Ranitidine 59% NNT 6 ( 95% CI 4-13) At 12 months: Proportion with sufficient symptom control and relapse rates in patients who were controlled at 8 weeks No difference between PPI and H2RA 2 shorter studies showed decreased relapse rate and better symptom control with PPIs. CADTH 2007
36 Alternates to daily PPI maintenance for GERD Continued PPI therapy is more efficacious than stepdown to H2RAs in uninvestigated GERD and erosive esophagitis Alternatives (PPI discontinuation, H2RAs, on demand dosing) to long-term regular use of standard dose PPIs for GERD may be appropriate in select patients 20% of uninvestigated GERD patients remain asymptomatic off therapy for up to 6 months after a successful initial course (4-8 wks treatment) with a PPI or H2RA CADTH 2007
37 Uninvestigated GERD step down to H2RA Patients who have completed an initial course of PPI, continued PPI is more efficacious than stepdown to H2RA for symptom relief. One RCT using lansoprazole 30 mg once daily and ranitidine 150 mg twice daily. Outcome: Heartburn relief at 20 weeks PPI: 82% PPI x 8 weeks, H2RA x 12 weeks: 67% NNT 7 (95%CI 4, 20) CADTH 2007
38 On demand PPI therapy? More efficacious than placebo (uninvestigated GERD, ENRD) More efficacious than continuous standard dose H2RA (uninvestigated GERD) Less efficacious than continuous PPI (uninvestigated GERD, EE) CADTH 2007
39 On demand PPI therapy? The two latter statements were supported by 1 RCT (n=2,156) that compared continuous std dose PPI, continuous std dose H2RA, and std dose PPI taken on-demand over 6 months in patients heartburn as predominant symptom: Proportion w/o heartburn at 6 months Continuous PPI: 72.2% On-demand PPI: 45.1% Continuous H2RA: 32.5% Proportion at least very satisfied at 6 months Continuous PPI: 82.2% On-demand PPI: 75.4% Continuous H2RA: 33.5% NNT (95% CI) = 4 (3, 5) NNT (95% CI) = 8 (6, 14) p<0.01 p< On-demand patients used 35% less drug on average than continuously-dosed patients CADTH 2007
40 Is the patient infected with Helicobacter Pylori? First-Line Triple Therapy : 1 week, 2 times a day, 3 drugs Currently approved 7 day regimens PPI + clarithromycin (Biaxin ) + amoxicillin or metronidazole First-Line Quadruple Regimens PPI twice daily + BMT four times daily (bismuth+metronidazole+tetracycline) Compliance is critical for HP eradication treatment success Van Zanten 2000
41 HP common questions Is follow-up acid suppression needed? Not generally indicated for uncomplicated duodenal ulcer Exceptions gastric ulcers patients that remain symptomatic complicated patients with large or refractory ulcers ensure ulcer healing & HP eradicated Maintenance anti-secretory therapy for patients at high risk for recurrence / bleeding e.g. high acid-secretory condition CADTH 2007 Gisbert 2005 Hunt 1998 Van Zanten 1997 Tytgat 1998
42 HP common questions Is follow-up testing to confirm eradication required? Repeat testing generally not recommended Exceptions: patients that remain symptomatic, bleeding/perforated ulcers, MALT lymphoma or gastric cancer Cannot use serology What approach for HP eradication treatment failure? Use a different first-line therapy other than one used initially or PPI + BMT 14 days Does drug therapy impact Urea Breath Test for HP results? H. pylori testing possible false negatives: discontinue abx/bismuth 4wks prior suppress discontinue acid suppression 1wk HP Van Zanten 2000 Hunt 1999 Hunt 1998
43 Objectives Review the use of Proton Pump Inhibitors (PPIs) in the treatment of GERD Dyspepsia Peptic ulcer disease (NSAID induced & H.Pylori) Review evidence for following PPI issues Efficacy of one PPI vs. another Double-dose PPI as initial therapy Role in asthma, laryngeal symptoms & chronic cough associated with GERD
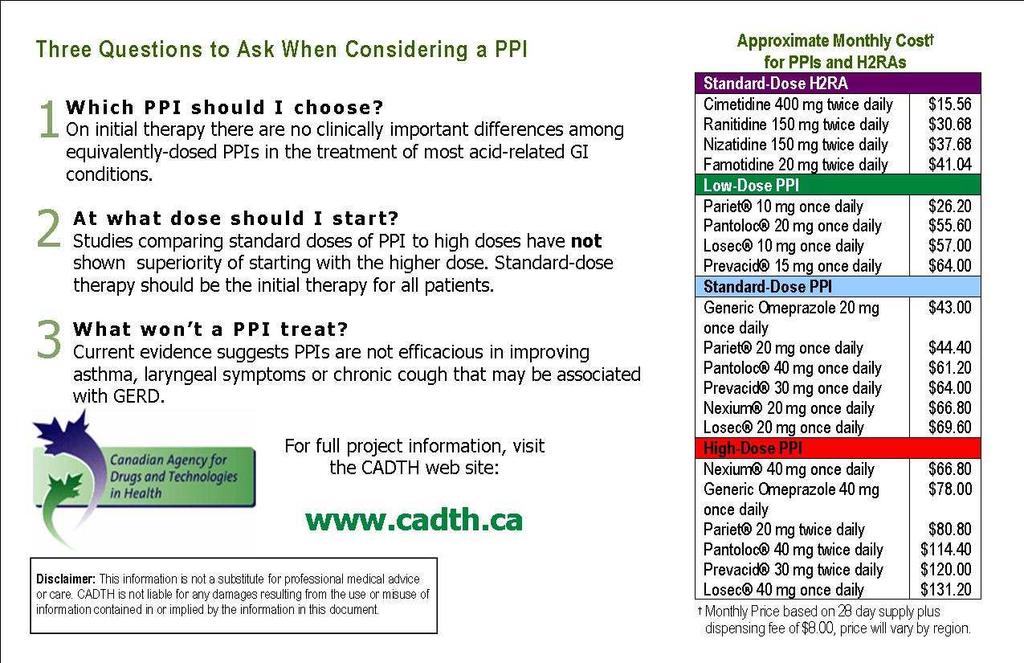
44 Which PPI should be used? All PPIs are equally efficacious Standard doses of PPIs may be used interchangeably when initiating therapy because there are no clinically important differences among the various PPIs in the treatment of most acid-related GI conditions. PPI Standard doses Omeprazole Rabeprazole Pantoprazole Lansoprazole Esomeprazole (Losec ) (Pariet ) (Pantoloc ) (Prevacid ) (Nexium ) 20mg daily 20mg daily 40mg daily 30 mg daily 20mg daily CADTH 2007
45 Evidence-based support All PPIs are equally efficacious GERD/ENRD/Esophagitis 6 good quality systematic reviews-no clinically important differences in standard doses PPIs Isolated exceptions, majority showed no differences Comparisons showing some degree of difference involved non-equivalent comparisons (e.g. high dose vs. standard dose) H.pylori Eradication 7 systematic reviews 5 good quality : PPIs have similar efficacy when used in triple therapy regimens CADTH 2007
46 Evidence-based Support All PPIs are equally efficacious NSAID Ulcer Prophylaxis 1 good quality systematic review 7 RCTs (indirect comparisons formal stat methods not employed ), and 1 RCT direct comparison : different PPIs reduce ulcer risk to a similar degree (the only direct comparison was of omeprazole vs pantoprazole) NSAID Ulcer Healing 1 good quality systematic review 3RCTs (indirect comparisons formal stat methods not employed ): similar healing rates for the PPIs that have been studied (omeprazole & lansoprazole) CADTH 2007
47 Evidence-based limitations All PPIs are equally efficacious Isolated studies may show superiority, balance against weight of evidence Caution for comparisons between non-equivalent doses of PPIs, e.g. omeprazole 20mg vs. esomeprazole 40mg No evidence regarding safety and efficacy of switching to a different PPI in patients successfully treated with a given PPI Not all comparisons have been made for all indications Official indications may be more limited in scope e.g. apoomeprazole not officially indicated for H. pylori eradication Balance evidence against need for patient individualization CADTH 2007
48 Bottom line All PPIs are equally efficacious There are no clinically important differences among standard doses, or equivalent doses of PPIs in the initial treatment of most acid related GI conditions In most circumstances the data suggests clinicians may interchange PPIs with confidence The equality of PPIs is supported by the majority of the available literature CADTH 2007
49 Implications to practice Cost savings to the patient/society Simplify prescribing by focusing on lowest cost PPI. Standard Dose PPIs Generic Omeprazole 20mg Daily Rabeprazole (Pariet ) 20mg Daily Pantoprazole (Pantoloc ) 40mg Daily Lansoprazole (Prevacid ) 30mg Daily Esomeprazole (Nexium ) 20mg Daily Omeprazole (Losec ) 20mg Daily Daily Price $1.25 $1.30 $1.90 $2.00 $2.10 $2.20 Approximate Monthly Price $43.00 $44.40 $61.20 $64.00 $66.80 $69.60 Generic omeprazole 20mg and rabeprazole (Pariet ) 20mg are the cheapest standard dose PPIs on the Canadian market. Using a PPI that costs $1.40/day vs. $2.20/day will save a patient almost $300 per year in drug costs. CADTH 2007
50 Potential yearly savings Society/Patients Canada million PPI prescriptions Imagine if 50% were changed from: $2.20/day regimen $1.25/day regimen 0.95 cents saved/day x 30 days x 6.2 million prescriptions: $176 million dollars/year
51 What dose of PPI? More may not always be better High or double-dose PPI, as initial therapy, is no better than standard daily dose therapy in the management of erosive esophagitis Research Gaps: double dose in GERD patients with severe symptoms or in patients who remain symptomatic after an initial course of standard dose therapy CADTH 2007
52 Evidence based support More may not always be better High or Double-dose PPIs for initial Rx Erosive Esophagitis 6 RCTs N=1388 : 2 RCTs very good quality, 1 good quality, 3 poor qualitygrade2-4 esophagitis Majority of evidence: no benefit for initial treatment Limitation: small number of trials, all of poor quality, specifically addressed Grade 2-4 esophagitis (more severe) Esomeprazole 40mg is approved dose for erosive esophagitis Some but not all trials of 40mg vs standard dose PPIs have shown benefit Clinical importance unclear. CADTH 2007 McDonagh 2005
53 Evidence based support More may not always be better Double-dose initial Rx NSAID-induced ulcer 2 RCTs n=1476 : double dose omeprazole was not superior to single dose both standard and double doses more effective than H2RA (NNT=4-9) and misoprostol (NNT=6-8) Do not need double-dose PPI. CADTH 2007
54 Bottom line Little evidence that more is better Doubling the standard daily dose of PPIs, as initial therapy, is no better than standard daily dose therapy. Standard dose should be the initial therapy.
55 Double-dose PPI therapy may be considered if: Standard doses are not effective (e.g. after 2-4 weeks) Lack of response to standard dose PPI warrants: Reassessment of diagnosis Ensure patient taking PPI properly In hypersecretory conditions (e.g. Zollinger-Ellison syndrome, H.pylori eradication regimens and select patients post-gi bleed (4 weeks) Double-dose PPI should be reassessed after 4-8 weeks Khan 2007
56 Implications to practice Cost savings Standard Dose PPIs Generic omeprazole 20mg Daily Rabeprazole (Pariet ) 20mg Daily Pantoprazole (Pantoloc ) 40mg Daily Lansoprazole (Prevacid ) 30mg Daily Esomeprazole (Nexium ) 20mg Daily Omeprazole (Losec ) 20mg Daily Daily Price $1.25 $1.30 $1.90 $2.00 $2.10 $2.20 Approximate Monthly Price High Dose PPIs $43.00 Esomeprazole 40mg Daily $44.40 $61.20 Generic Omeprazole 40mg Daily Rabeprazole 20mg Twice Daily $64.00 $66.80 $69.60 Pantoprazole 40mg Twice Daily Lansoprazole 30mg Twice Daily Omeprazole 20mg Daily Daily Price $2.10 $2.50 $2.60 $3.80 $4.00 $4.40 Approximate Monthly Price $66.80 $78.00 $80.80 $ $ $ CADTH 2007
57 PPIs: asthma, laryngeal symptoms & chronic cough use the right tool for the job PPIs are not efficacious in the treatment of asthma, chronic cough and laryngeal symptoms that may be associated with GERD. CADTH 2007
58 Evidence-based support Asthma with concomitant GERD One good quality systematic review (12 RCTs, n=432) PPI (omeprazole mg) or H2RA did not improve FEV1, PEF, airway responsiveness or use of inhalers 1 RCT (omeprazole 40 mg vs placebo) reported improvement in nocturnal symptom score CADTH 2007
59 Evidence-based support Laryngeal symptoms with Reflux One good quality systematic review (5 RCTs, n=247) No significant effect on laryngo-pharyngeal symptoms (e.g., cough, throat clearing, globus, hoarseness, sore throat) CADTH 2007
60 Evidence-based support Chronic cough with or without GERD One good quality systematic review Chronic cough 3 weeks without respiratory symptoms/signs or systemic illness Cough score at various times No benefit of PPI vs. placebo Limitations: Small pooled sample size: analysis likely underpowered Heterogeneity in study population CADTH 2007
61 Bottom line PPIs: asthma, laryngeal symptoms & chronic Cough PPI effective for treating GI disease Current evidence would suggest they are not efficacious in improving asthma, laryngeal symptoms or chronic cough that may be associated with GERD. The use of PPIs for this indication should be discouraged.
62 PPI Interventions & Tools Physician Educational Materials Alternate Prescription Pad Newsletter 3 Questions to Ask When Starting a PPI Self Audit Form Academic Detailing Interactive and Didactic Presentation Prescribing Aid Pharmacists Materials Interactive and Didactic Presentation Patient Education Materials Information Brochure / Alternate Prescription Pad
63 Alternate prescription pad

64 Optimal therapy newsletter Which PPI should I choose? What dose should I start At? What won t a PPI treat?

65 Quick reference prescribing aid
66 Role of pharmacist Referral to family physician (Remember Vbad) Identify drug and herbal causes of dyspepsia Treatment consistent with best practices Tailor drug therapy Medication information Monitor response/side effects & drug interactions Seamless care Ensure therapy reassessed
67 Summary Standard doses of PPIs may be used interchangeably for initial therapy because there are no clinically important differences among the PPIs in most acid-related GI conditions Standard doses are sufficient for initial therapy in most conditions (exceptions: HP regimens, upper GI bleed) PPIs are not efficacious in the treatment of asthma, chronic cough, and laryngeal symptoms that may be associated with GERD
68 Summary Although H2RA therapy is effective in managing many patients, standard-dose PPIs are superior to H2RAs for initial and maintenance therapy of uninvestigated GERD and erosive esophagitis and the initial treatment of ENRD Patients with uncomplicated duodenal ulcers don t require continuation of PPI therapy after HP eradication Standard-dose PPIs and misoprostol mcg/day have similar efficacy in the prevention of NSAIDassociated ulcers
69 Questions?
70 References 1. Canadian Agency for Drugs and Technologies in Health. Evidence for PPI use in gastroesophageal reflux disease, dyspepsia and peptic ulcer disease: scientific report. Optimal Therapy Report - COMPUS 2007;1(2). Available: (accessed 2007 Mar 28). 2. Canadian Agency for Drugs and Technologies in Health. Economic models and conclusions for the treatment of dyspepsia, gastroesophageal reflux disease-related heartburn and the prevention of non-steroidal antiinflammatory induced gastrointestinal complications. Optimal Therapy Report COMPUS 2007; 1(3). Available: (accessed 2007 Mar 28). 3. Armstrong D, Marshall JK, Chiba N, Enns R, Fallone CA, Fass R, et al. Canadian consensus conference on the management of gastroesophageal reflux disease in adults: update Can J Gastroenterol 2005;19(1): Berger ML, Bingefors K, Hedblom EC, Pashos CL, Torrance GW, editors. Health care cost, quality, and outcomes: ISPOR book of terms. Lawrenceville: International Society for Pharmacoeconomics and Outcomes Research; 2003.
71 References 5. Bazaldua OV, Schneider FD. Evaluation and management of dyspepsia. Am Fam Physician 1999;60(6): Available: (accessed 2005 Jul 18). 6. Gisbert JP, Pajares JM. Systematic review and meta-analysis: is 1- week proton pump inhibitor-based triple therapy sufficient to heal peptic ulcer? Aliment Pharmacol Ther 2005;21(7): Hawkey CJ, Karrasch JA, Szczepanski L, Walker DG, Barkun A, Swannell AJ, et al. Omeprazole compared with misoprostol for ulcers associated with nonsteroidal antiinflammatory drugs. Omeprazole versus Misoprostol for NSAID-induced Ulcer Management (OMNIUM) Study Group. N Engl J Med 1998;338(11): Heidelbaugh JJ, Nostrant TT, Kim C, Van Harrison R. Management of gastroesophageal reflux disease. Am Fam Physician 2003;68(7): Hunt R, Thomson AB. Canadian Helicobacter pylori consensus conference. Canadian Association of Gastroenterology. Can J Gastroenterol 1998;12(1): Hunt RH, Fallone CA, Thomson AB. Canadian Helicobacter pylori consensus conference update: infections in adults. Canadian Helicobacter Study Group. Can J Gastroenterol 1999;13(3):213-7.
72 References 11. Kaltenbach T, Crockett S, Gerson LB. Are lifestyle measures effective in patients with gastroesophageal reflux disease? An evidencebased approach. Arch Intern Med 2006;166(9): Khan M, Santana J, Donnellan C, Preston C, Moayyedi P. Medical treatments in the short term management of reflux oesophagitis. Cochrane Database Syst Rev 2007;(2):CD Lanza FL. A guideline for the treatment and prevention of NSAIDinduced ulcers. Members of the Ad Hoc Committee on Practice Parameters of the American College of Gastroenterology. Am J Gastroenterol 1998;93(11): Quality adjusted life year [definition]. Medicinenet.com. Available: Accessed: 13 Sept McDonagh MS, Carson S. Drug class review on proton pump inhibitors: final report update 3. Portland (OR): Oregon Health & Science University; Thomson P. Dyspepsia and GERD. In: Patient self-care: helping patients make therapeutic choices. 1st ed. Ottawa: Canadian Pharmacists Association; p
73 References 17. Tytgat GN. Treatment of peptic ulcer. Digestion 1998;59(5): Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol 2006;101(8): Van Zanten SJO, Sherman PM, Hunt RH,. Helicobacter pylori: new developments and treatments. CMAJ 1997;156(11): Available: (accessed 2006 Feb 3). 20. Van Zanten VSJ, Flook N, Chiba N, Armstrong D, Barkun A, Bradette M, et al. An evidence-based approach to the management of uninvestigated dyspepsia in the era of Helicobacter pylori. CMAJ 2000;162(12 Suppl):S3-S23. Available: (accessed 2007 Apr 9). 21. Yeomans ND, Tulassay Z, Juhász L, Rácz I, Howard JM, van Rensburg CJ, et al. A comparison of omeprazole with ranitidine for ulcers associated with nonsteroidal antiinflammatory drugs. N Engl J Med 1998;338(11):
74 References 22. Aalykke C, Lauritsen K. Epidemiology of NSAID-related gastroduodenal mucosal injury. Best Pract Res Clin Gastroenterol 2001;15(5): Chan FK, Graham DY. Review article: prevention of non-steroidal anti-inflammatory drug gastrointestinal complications--review and recommendations based on risk assessment. Aliment Pharmacol Ther 2004;19(10): Straus WL, Ofman JJ. Gastrointestinal toxicity associated with nonsteroidal anti-inflammatory drugs. Epidemiologic and economic issues. Gastroenterol Clin North Am 2001;30(4): Hirth RA, Chernew ME, Miller E, Fendrick AM, Weissert WG. Willingness to pay for a quality-adjusted life year: in search of a standard. Med Decis Making 2000;20(3):
75 Additional background slides
76 Factors influencing drug coverage There are many factors that influence decisions to include a drug on a formulary: Patient population Clinical efficacy Cost-effectiveness Resources available/budget Impact Choices: Full Benefit, Restricted Benefit, Not a benefit
77 The PPI economic component The economic component of the PPI project compared expected costs and outcomes of various primary care strategies for the following: Heartburn in patients with moderate-to-severe, uninvestigated GERD Patients with uninvestigated dyspepsia Prevention of GI complications in patients using NSAIDs
78 Economic terminology Quality Adjusted Life Year (QALY): Outcome measure that incorporates both quantity of life (mortality) and health-related quality of life (morbidity) Quantity how long person lives Quality factor that represents a preference for a health state one year of perfect health = one QALY one year less than perfect health < one QALY death = zero i.e., a person in perfect health (quality weight=1) for 10 years followed by 10 years in a health state with a quality weight of 0.50 would have achieved 15 QALYs (10 X X 0.5)* Berger 2003 Medicinenet.com
79 Economic terminology How much is a QALY worth? There is no simple answer The debate on appropriate value (i.e. $50,000) of a QALY continues* Resource allocation decisions must take this question into consideration * Hirth et al.,(2003) Medical Decision Making
80 Economic conclusions Prevention of GI complications associated with NSAID use Strategy Cost (C$) Incr Cost Effectiveness (QALY) Incr Eff Incr C/E (ICER)* NSAID alone NSAID+PPI ,835 NSAID+H2RA ,112,682 Incr=incremental; QALY=quality-adjusted life year; Incr Eff=incremental effectiveness CADTH Economic Models 2007
81 Economic conclusions Heartburn in patients with moderate to severe uninvestigated GERD Population - Uninvestigated GERD Strategy Expected 1yr cost per patient Expected QALYs Incremental cost per QALY 1 (Cdn$) A: PPI on-demand $ B: H2RA on demand $ Dominated by A C: PPI with step-down H2RA maintenance $ Extendedly dominated D: H2RA maintenance $ Dominated by C E: PPI maintenance $ $27,848 1 Relative to the next less costly non-dominated strategy CADTH Economic Models 2007
82 Economic conclusions Patients with non-heartburn predominant uninvestigated dyspepsia Strategy Empirical Antisecretory Therapy (omeprazole) Test and treat all (omeprazole) Prompt Endoscopy (H 2 RA) Prompt Endoscopy (PPI) Cost B) Without dominated options (simple or extended) Incremental Cost ICER 10, , ,990 H2RA=histamine-2 receptor antagonists; ICER=international cost-effectiveness ratio; PPI=proton pump inhibitor; SF=symptom free Incremental cost-effectiveness ratio (incremental cost per QALY) CADTH Economic Models 2007
83 ENRD Initial Therapy PPIs are more efficacious than H2RAs as initial therapy for improvement of heartburn symptoms at 4 weeks in patients with ENRD. However, PPIs are not superior to H2RAs in terms of improving quality of life. One SR included 4 RCTs (N=960) RR for heartburn persistence = 0.78 (95% CI: ) Pooled heartburn relief rates in the 4 trials: Standard dose PPIs: 53% H2RAs: 42% 2 RCTs measured QoL: No significant difference in reflux dimension or total score of Gastrointestinal Symptoms Rating Scale (GSRS) CADTH 2007
84 Economic conclusions Heartburn in patients with moderate to severe uninvestigated GERD Population - ENRD Strategy Expected 1yr cost per patient Expected QALYs Incremental cost per QALY 1 (Cdn$) A: H2RA on demand B: PPI on demand $2,505 C: PPI with step-down H2RA maintenance Extendedly Dominated D: H2RA maintenance Dominated by C E: PPI maintenance $26,986 1 Relative to the next less costly non-dominated strategy CADTH Economic Models 2007
85 Erosive esophagitis- initial therapy PPIs are more efficacious than H2RAs for improving symptoms and healing of erosive esophagitis. 2 SRs and 5 RCTs N= 4310 Outcomes: 1 week 6 months Healing of erosions H2RAs PPIs Symptom relief 4 weeks range of 26% - 54% 8 weeks or more range of: 35-76% 4 weeks 56 74% 8 weeks or more 71% - 90% Similar rates as for healing CADTH 2007
86 Erosive esophagitis - maintenance Long-term maintenance PPI therapy (i.e., up to 12 months) in erosive esophagitis is more efficacious than H2RAs for prevention of symptomatic and endoscopic relapse. Patients resistant to H2RAs: 1RCT N=98 Proportion with symptomatic and endoscopic remission at 12 months: Omeprazole 40 mg daily 67% Ranitidine 300 mg bid 10% (p<0.0001) CADTH 2007
87 Erosive esophagitis - maintenance Long-term PPI therapy is more efficacious than H2RAs for erosive esophagitis complicated by strictures. 3 RCTs, N=561, Duration 6 months- 1 year Outcomes: redilatation, dysphagia relief Results in 2 smaller studies: PPIs lower rates of redilatation and greater reduction in dysphagia but nonsignificant The larger study (n=366) found a significant reduction in redilatation and symptom relief however the rates were similar to other studies: dysphagia relief in 76% of PPI patients vs. 64% of H2RA patients, p<0.05 Consensus thought is that PPIs are better for this patient population CADTH 2007
88 Economic conclusions Heartburn in patients with moderate to severe uninvestigated GERD Population - erosive esophagitis Strategy Expected 1yr cost per patient Expected QALYs Incremental cost per QALY 1 (Cdn$) A: PPI on-demand B: H2RA on-demand Dominated by A C: PPI with step-down H2RA maintenance $33,692 D: H2RA maintenance Dominated by C E: PPI maintenance $44,168 1 Relative to the next less costly non-dominated strategy CADTH Economic Models 2007
89 Erosive esophagitis step-down In patients with erosive esophagitis who have completed an initial course of PPIs, half-dose PPI maintenance therapy is more efficacious than step-down to H2RAs for preventing relapse and providing improvement of symptoms. One systematic review of 4-6 trials. N= Proportion with relapse of esophagitis at weeks: PPI half dose 39% H2RA 66%; RR=0.57; (95% CI 0.47, 0.69) NNT (95% CI) 3 (2-5) Proportion with relapse of symptoms at weeks: PPI half dose 31% H2RA 44%; RR=0.55; (95% CI 0.47, 0.65) NNT (95% CI) 4 (3-5) CADTH 2007
90 The Evidence (ASTRONAUT Study): 541 patients with DU, GU, or >10 GI erosions receiving NSAIDs treated with omeprazole 20mg or 40mg, or ranitidine 300mg daily Results for omeprazole 20mg vs. ranitidine: Outcome (at 8 weeks) Tx failures (Ome vs. Ran) RR of failure (95% CI) NNT (95% CI) for success Treatment Failure 20% vs. 37% 0.55 ( ) 6 (4, 13) DU healing 8% vs. 19% 0.44 ( ) 9 (NNH 4, NNT 24) GU healing 16% vs. 36% 0.44 ( ) Results for double dose vs. standard dose omeprazole: 5 (3, 17) Treatment failure: 21% vs. 20%, p>0.05 (NS) DU persistence: 12% vs. 8%, p>0.05 (NS) GU persistence: 13% vs. 16%, p>0.05 (NS) Yeomans 1998
91 What about a COX2 vs a NSAID? There is no difference in ulcer reoccurance and bleeding rates between COX-2 selective NSAIDs and the combination PPI and conventional NSAIDs in patients with previous NSAIDassociated upper GI bleeding One RCT comparing 6 months of celecoxib 200 bid vs. diclofenac 75 mg bid plus omeprazole 20 mg qd in patients with previous GI hemorrhage on an NSAID no difference in risk of recurrent bleeding or endoscopic ulcer at 6months Second RCT- celecoxib 200 qd vs. lansoprazole 30 mg qd plus naproxen 250 tid for 24 weeks No difference in re-occurnace of ulcer complications CADTH 2007
Disclaimer. Statement of disclosure. Goals. Background. Objectives
 Pharmacist Presentation Disclaimer Proton Pump Inhibitors and the Treatment of GERD, Dyspepsia, NSAID-associated Peptic Ulcer Disease Presenter Title Affiliation Date The information in this presentation
Pharmacist Presentation Disclaimer Proton Pump Inhibitors and the Treatment of GERD, Dyspepsia, NSAID-associated Peptic Ulcer Disease Presenter Title Affiliation Date The information in this presentation
Five key decision points: uninvestigated dyspepsia
 Five key decision points: uninvestigated dyspepsia 1. Are there other possible causes for the 2. Does patient have Alarm symptoms (VBAD) or > 50 years of age? 3. Is the patient using NSAIDs (including
Five key decision points: uninvestigated dyspepsia 1. Are there other possible causes for the 2. Does patient have Alarm symptoms (VBAD) or > 50 years of age? 3. Is the patient using NSAIDs (including
Proton Pump Inhibitors and the Treatment of GERD, Dyspepsia, and NSAID-associated Peptic Ulcer Disease Presenter Title Affiliation Date
 Proton Pump Inhibitors and the Treatment of GERD, Dyspepsia, and NSAID-associated Peptic Ulcer Disease Presenter Title Affiliation Date Disclaimer The information in this presentation is not a substitute
Proton Pump Inhibitors and the Treatment of GERD, Dyspepsia, and NSAID-associated Peptic Ulcer Disease Presenter Title Affiliation Date Disclaimer The information in this presentation is not a substitute
Disclaimer. Statement of disclosure. Objectives. Background
 Physician Presentation Disclaimer Proton Pump Inhibitors and the Treatment of GERD, Dyspepsia, and NSAID-associated Peptic Ulcer Disease Presenter Title Affiliation Date The information in this presentation
Physician Presentation Disclaimer Proton Pump Inhibitors and the Treatment of GERD, Dyspepsia, and NSAID-associated Peptic Ulcer Disease Presenter Title Affiliation Date The information in this presentation
COMPUS OPTIMAL THERAPY REPORT. Supporting Informed Decisions. À l appui des décisions éclairées. Proton Pump Inhibitor Project Overview: Summaries
 OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 1 March 2007 Proton Pump Inhibitor Project Overview: Summaries Supporting Informed Decisions À l appui des décisions éclairées This Executive Summary is based
OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 1 March 2007 Proton Pump Inhibitor Project Overview: Summaries Supporting Informed Decisions À l appui des décisions éclairées This Executive Summary is based
COMPUS OPTIMAL THERAPY REPORT. Supporting Informed Decisions. À l appui des décisions éclairées
 OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 5 March 2007 Current Practice Analysis Report for the Prescribing and Use of Proton Pump Inhibitors (PPIs) Supporting Informed Decisions À l appui des décisions
OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 5 March 2007 Current Practice Analysis Report for the Prescribing and Use of Proton Pump Inhibitors (PPIs) Supporting Informed Decisions À l appui des décisions
COMPUS OPTIMAL THERAPY REPORT. Supporting Informed Decisions. À l appui des décisions éclairées
 OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 6 March 2007 Gap Analysis Report for the Prescribing and Use of Proton Pump Inhibitors (PPIs) Supporting Informed Decisions À l appui des décisions éclairées
OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 6 March 2007 Gap Analysis Report for the Prescribing and Use of Proton Pump Inhibitors (PPIs) Supporting Informed Decisions À l appui des décisions éclairées
Health Economics 101: PPI prescriptions in the Emergency Room
 : PPI prescriptions in the Emergency Room Canadian Optimal Medication Prescribing & Utilization Service (COMPUS) Presented by: Chris Cameron October 26, 2007 What is Health Economics? Health economics
: PPI prescriptions in the Emergency Room Canadian Optimal Medication Prescribing & Utilization Service (COMPUS) Presented by: Chris Cameron October 26, 2007 What is Health Economics? Health economics
Developing Evidence-Based Best Practices for the Prescribing and Use of Proton Pump Inhibitors in Canada
 Developing Evidence-Based Best Practices for the Prescribing and Use of Proton Pump Inhibitors in Canada Presented by: Sumeet R. Singh, COMPUS April 4, 2006 Background COMPUS Objective: To identify and
Developing Evidence-Based Best Practices for the Prescribing and Use of Proton Pump Inhibitors in Canada Presented by: Sumeet R. Singh, COMPUS April 4, 2006 Background COMPUS Objective: To identify and
COMPUS OPTIMAL THERAPY REPORT. Supporting Informed Decisions. À l appui des décisions éclairées. Proton Pump Inhibitor Project Overview: Summaries
 OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 1 March 2007 Proton Pump Inhibitor Project Overview: Summaries Supporting Informed Decisions À l appui des décisions éclairées This Executive Summary is based
OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 1 March 2007 Proton Pump Inhibitor Project Overview: Summaries Supporting Informed Decisions À l appui des décisions éclairées This Executive Summary is based
PLANNING COMMITTEE. Seek simplicity, and mistrust it. Alfred North Whitehead
 PLANNING COMMITTEE 1. Content Experts Clinical experts Desmond Leddin MB FRCPC, Head, Division of Gastroenterology, Dalhousie University Drug evaluation pharmacist Pam McLean-Veysey BScPharm, Drug Evaluation
PLANNING COMMITTEE 1. Content Experts Clinical experts Desmond Leddin MB FRCPC, Head, Division of Gastroenterology, Dalhousie University Drug evaluation pharmacist Pam McLean-Veysey BScPharm, Drug Evaluation
QUICK QUERIES. Topical Questions, Sound Answers
 QUICK QUERIES Topical Questions, Sound Answers Dyspepsia: An Evidence-Based Approach Alan B. R. Thomson, MD, PhD, FRCPC, FACP, FACG Presented at the University of Alberta s Medical Grand Rounds, University
QUICK QUERIES Topical Questions, Sound Answers Dyspepsia: An Evidence-Based Approach Alan B. R. Thomson, MD, PhD, FRCPC, FACP, FACG Presented at the University of Alberta s Medical Grand Rounds, University
Proton Pump Inhibitors Drug Class Prior Authorization Protocol
 Proton Pump Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review
Proton Pump Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review
MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD)
") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD) Routine endoscopic investigation of patients of any age, presenting with dyspepsia
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD) Routine endoscopic investigation of patients of any age, presenting with dyspepsia
Drug Class Monograph
 Drug Class Monograph Class: Proton Pump Inhibitors Drugs: Aciphex Sprinkle (rabeprazole), Dexilant (dexlansoprazole), Lansoprazole, Nexium (esomeprazole capsule, esomeprazole granules), Omeprazole, Pantoprazole,
Drug Class Monograph Class: Proton Pump Inhibitors Drugs: Aciphex Sprinkle (rabeprazole), Dexilant (dexlansoprazole), Lansoprazole, Nexium (esomeprazole capsule, esomeprazole granules), Omeprazole, Pantoprazole,
Management of dyspepsia and of Helicobacter pylori infection
 Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
Proton Pump Inhibitors (PPIs) (Sherwood Employer Group)
 (Sherwood Employer Group)") Proton Pump Inhibitors (PPIs) (Sherwood Employer Group) BCBSKS will review Prior Authorization requests Prior Authorization Form: https://www.bcbsks.com/customerservice/forms/pdf/priorauth-6058ks-st-ippi.pdf
Proton Pump Inhibitors (PPIs) (Sherwood Employer Group) BCBSKS will review Prior Authorization requests Prior Authorization Form: https://www.bcbsks.com/customerservice/forms/pdf/priorauth-6058ks-st-ippi.pdf
SASKATCHEWAN REGISTERED NURSES ASSOCIATION
 DEFINITION Reflux of gastric contents into the esophagus, which results in esophageal irritation or inflammation. IMMEDIATE CONSULTATION REQUIRED IN THE FOLLOWING SITUATIONS Dysphagia (solid food, progressive)
DEFINITION Reflux of gastric contents into the esophagus, which results in esophageal irritation or inflammation. IMMEDIATE CONSULTATION REQUIRED IN THE FOLLOWING SITUATIONS Dysphagia (solid food, progressive)
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA
 MANAGEMENT OF DYSPEPSIA") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA o Patients of any age with ALARM signs should be referred through the 2-week referral system o Routine endoscopic investigation
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA o Patients of any age with ALARM signs should be referred through the 2-week referral system o Routine endoscopic investigation
GASTROINTESTINAL AND ANTIEMETIC DRUGS. Submitted by: Shaema M. Ali
 GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
Management of Dyspepsia
 MPharm Programme Management of Dyspepsia Slide 1 of 28 Learning Objectives Understand the principles and wider implications underpinning evidence based therapeutics in the key clinical specialities Objectively
MPharm Programme Management of Dyspepsia Slide 1 of 28 Learning Objectives Understand the principles and wider implications underpinning evidence based therapeutics in the key clinical specialities Objectively
Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist
 Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist") Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist Disclosures I have no actual or potential conflicts of interest to report in relation to this
Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist Disclosures I have no actual or potential conflicts of interest to report in relation to this
11/19/2012. Comparison between PPIs G CELL. Risk ratio (95% CI) Patient subgroup. gastrin. S-form of omeprazole. Acid sensitive. coated.
 Patient subgroup. gastrin. S-form of omeprazole. Acid sensitive. coated.") REGULATION OF GASTRIC ACID SECRETION Comparison between PPIs Omeprazole Lansoprazole Rabeprazole Pantoprazole Esomeprazole gastrin G CELL + Acid sensitive Yes T1/2 30-60 minutes Main elimination Enteric
REGULATION OF GASTRIC ACID SECRETION Comparison between PPIs Omeprazole Lansoprazole Rabeprazole Pantoprazole Esomeprazole gastrin G CELL + Acid sensitive Yes T1/2 30-60 minutes Main elimination Enteric
A C A D E M I C D E TA I L I N G C H O O S I N G W I S E LY C O N F E R E N C E O C T 2 1, PA M M C L E A N - V E Y S E Y B S C P H A R M D R
 PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
Committee Approval Date: October 14, 2014 Next Review Date: October 2015
 Medication Policy Manual Topic: esomeprazole-containing medications: - Nexium - Vimovo - esomeprazole strontium Policy No: dru039 Date of Origin: May 2001 Committee Approval Date: October 14, 2014 Next
Medication Policy Manual Topic: esomeprazole-containing medications: - Nexium - Vimovo - esomeprazole strontium Policy No: dru039 Date of Origin: May 2001 Committee Approval Date: October 14, 2014 Next
Summary of Findings on the Prescribing and Use of Proton Pump Inhibitors. COMPUS Interim Report CCOHTA. March 6, 2006
 Summary of Findings on the Prescribing and Use of Proton Pump Inhibitors COMPUS Interim Report CCOHTA March 6, 2006 Note that the information presented in this document does not constitute recommendations
Summary of Findings on the Prescribing and Use of Proton Pump Inhibitors COMPUS Interim Report CCOHTA March 6, 2006 Note that the information presented in this document does not constitute recommendations
Proton Pump Inhibitors. Description. Section: Prescription Drugs Effective Date: July 1, 2014
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.09.01 Subject: Proton Pump Inhibitors Page: 1 of 7 Last Review Date: June 12, 2014 Proton Pump Inhibitors
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.09.01 Subject: Proton Pump Inhibitors Page: 1 of 7 Last Review Date: June 12, 2014 Proton Pump Inhibitors
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Reflux of gastric contents, particularly acid, into the esophagus
 Heartburn Reflux of gastric contents, particularly acid, into the esophagus Patient assessment with GERD 1-signs and symptoms The hallmark of typical symptom of GERD is heartburn (restrosternal),acid regurgitation,
Heartburn Reflux of gastric contents, particularly acid, into the esophagus Patient assessment with GERD 1-signs and symptoms The hallmark of typical symptom of GERD is heartburn (restrosternal),acid regurgitation,
You May Be at Risk. You are currently taking a proton pump inhibitor (PPI):
:") PPI You are currently taking a proton pump inhibitor (PPI): Dexlansoprazole (Dexilant ) Esomeprazole (Nexium ) Omeprazole (Losec, Olex ) Lansoprazole (Prevacid, Prevacid Fast Tab ) Pantoprazole sodium
PPI You are currently taking a proton pump inhibitor (PPI): Dexlansoprazole (Dexilant ) Esomeprazole (Nexium ) Omeprazole (Losec, Olex ) Lansoprazole (Prevacid, Prevacid Fast Tab ) Pantoprazole sodium
Guidelines for the Management of Dyspepsia and GORD. Gastroenterology/ Acute Adult Governance. Drugs and Therapeutics Committee
 Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
Rpts. GENERAL General Schedule (Code GE) Program Prescriber type: Dental Medical Practitioners Nurse practitioners Optometrists Midwives
 Program Prescriber type: Dental Medical Practitioners Nurse practitioners Optometrists Midwives") Esomeprazole 20mg Name, Restriction, Manner of esomeprazole 20 mg enteric tablet, 30 (8886Q) (029W) Gastric ulcer Peptic ulcer Treatment Phase: Initial treatment The therapy must be for initial treatment
Esomeprazole 20mg Name, Restriction, Manner of esomeprazole 20 mg enteric tablet, 30 (8886Q) (029W) Gastric ulcer Peptic ulcer Treatment Phase: Initial treatment The therapy must be for initial treatment
Nexium 24HR. Tools and information for you and your pharmacy team NOW OTC FOR FREQUENT HEARTBURN. Consumer Healthcare Pfizer Inc.
 NOW OTC FOR FREQUENT HEARTBURN w e N Nexium 24HR P H A R M A S S I S T K I T Tools and information for you and your pharmacy team 2014 Pfizer Inc. NXM041468 05/14 Q: What is the indication for Nexium 24HR
NOW OTC FOR FREQUENT HEARTBURN w e N Nexium 24HR P H A R M A S S I S T K I T Tools and information for you and your pharmacy team 2014 Pfizer Inc. NXM041468 05/14 Q: What is the indication for Nexium 24HR
PRESCRIBING SUPPORT TEAM AUDIT: PROTON PUMP INHIBITOR PRESCRIBING REVIEW
 PRESCRIBING SUPPORT TEAM AUDIT: PROTON PUMP INHIBITOR PRESCRIBING REVIEW DATE OF AUTHORISATION: AUTHORISING GP: PRESCRIBING SUPPORT TECHNICIAN: SUMMARY Dyspepsia refers to a broad range of symptoms related
PRESCRIBING SUPPORT TEAM AUDIT: PROTON PUMP INHIBITOR PRESCRIBING REVIEW DATE OF AUTHORISATION: AUTHORISING GP: PRESCRIBING SUPPORT TECHNICIAN: SUMMARY Dyspepsia refers to a broad range of symptoms related
SELECTED ABSTRACTS. Figure. Risk Stratification Matrix A CLINICIAN S GUIDE TO THE SELECTION OF NSAID THERAPY
 SELECTED ABSTRACTS A CLINICIAN S GUIDE TO THE SELECTION OF NSAID THERAPY The authors of this article present a 4-quadrant matrix based on 2 key clinical parameters: risk for adverse gastrointestinal (GI)
SELECTED ABSTRACTS A CLINICIAN S GUIDE TO THE SELECTION OF NSAID THERAPY The authors of this article present a 4-quadrant matrix based on 2 key clinical parameters: risk for adverse gastrointestinal (GI)
Setting The setting was primary care. The economic study was carried out in Canada.
 Economic evaluation of Helicobacter pylori eradication in the CADET-Hp randomized controlled trial of H-pylori-positive primary care patients with uninvestigated dyspepsia Chiba N, Van Zanten S J, Escobedo
Economic evaluation of Helicobacter pylori eradication in the CADET-Hp randomized controlled trial of H-pylori-positive primary care patients with uninvestigated dyspepsia Chiba N, Van Zanten S J, Escobedo
The PPI Doesn t Work, Now What? PPI Non-responsive Dyspepsia. Disclosures
 The PPI Doesn t Work, Now What? PPI Non-responsive Dyspepsia Lana Bistritz MD FRCPC Royal Alexandra Hospital GI Update 2016 Disclosures I have no relevant financial disclosures I will be discussing off
The PPI Doesn t Work, Now What? PPI Non-responsive Dyspepsia Lana Bistritz MD FRCPC Royal Alexandra Hospital GI Update 2016 Disclosures I have no relevant financial disclosures I will be discussing off
Proton Pump Inhibitors. Description
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.01 Subject: Proton Pump Inhibitors Page: 1 of 6 Last Review Date: June 24, 2015 Proton Pump Inhibitors
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.01 Subject: Proton Pump Inhibitors Page: 1 of 6 Last Review Date: June 24, 2015 Proton Pump Inhibitors
Helicobacter 2008;13:1-6. Am J Gastroent 2007;102: Am J of Med 2004;117:31-35.
 An Update on Helicobacter pylori and Its Treatment Trenika Mitchell, PharmD, BCPS Clinical Assistant Professor University of Kentucky College of Pharmacy October 18, 2008 Objectives Review the epidemiology
An Update on Helicobacter pylori and Its Treatment Trenika Mitchell, PharmD, BCPS Clinical Assistant Professor University of Kentucky College of Pharmacy October 18, 2008 Objectives Review the epidemiology
Mitigating GI Risks Associated with the Use of NSAIDs
 bs_bs_banner Pain Medicine 2013; 14: S18 S22 Wiley Periodicals, Inc. Mitigating GI Risks Associated with the Use of NSAIDs Mahnaz Momeni, MD,* and James D. Katz, MD Departments of *Rheumatology, Medicine,
bs_bs_banner Pain Medicine 2013; 14: S18 S22 Wiley Periodicals, Inc. Mitigating GI Risks Associated with the Use of NSAIDs Mahnaz Momeni, MD,* and James D. Katz, MD Departments of *Rheumatology, Medicine,
TECHNOLOGY OVERVIEW: PHARMACEUTICALS
 TECHNOLOGY OVERVIEW: PHARMACEUTICALS ISSUE 3.1 JUNE 1996 PHARMACEUTICAL MANAGEMENT OF PEPTIC ULCER DISEASE prepared by Ms. Christine Perras, BSc Phm Pharmaceutical Associate, CCOHTA and Dr. Nicolaas Otten,
TECHNOLOGY OVERVIEW: PHARMACEUTICALS ISSUE 3.1 JUNE 1996 PHARMACEUTICAL MANAGEMENT OF PEPTIC ULCER DISEASE prepared by Ms. Christine Perras, BSc Phm Pharmaceutical Associate, CCOHTA and Dr. Nicolaas Otten,
Management of dyspepsia in adults in primary care
 Dyspepsia Management of dyspepsia in adults in primary care June 2005. The recommendations on referral for endoscopy in this NICE guideline have been amended in line with the recommendation in the NICE
Dyspepsia Management of dyspepsia in adults in primary care June 2005. The recommendations on referral for endoscopy in this NICE guideline have been amended in line with the recommendation in the NICE
Gastroesophageal Reflux Disease (GERD)
") Gastroesophageal Reflux Disease (GERD) Information for patients UHN Read this handout to learn about: What gastroesohageal reflux (GERD) is Signs and symptoms How your doctor will know if you have it Tests
Gastroesophageal Reflux Disease (GERD) Information for patients UHN Read this handout to learn about: What gastroesohageal reflux (GERD) is Signs and symptoms How your doctor will know if you have it Tests
Omeprazole 10mg. Name, Restriction, Manner of administration and form OMEPRAZOLE omeprazole 10 mg enteric tablet, 30 (8332M) Max. Qty.
 Max. Qty.") Omeprazole 10mg Name, Restriction, Manner of administration and form omeprazole 10 mg enteric tablet, 30 (8332M) Gastro-oesophageal reflux disease Name, Restriction, Manner of administration and form omeprazole
Omeprazole 10mg Name, Restriction, Manner of administration and form omeprazole 10 mg enteric tablet, 30 (8332M) Gastro-oesophageal reflux disease Name, Restriction, Manner of administration and form omeprazole
Helicobacter pylori. Objectives. Upper Gastrointestinal Bleeding Peptic Ulcer Disease
 Upper Gastrointestinal Bleeding Peptic Ulcer Disease Pharmacotherapy Issues in Acute Management and Secondary Prevention Peter J. Zed, B.Sc., B.Sc.(Pharm), Pharm.D. Pharmacotherapeutic Specialist - Emergency
Upper Gastrointestinal Bleeding Peptic Ulcer Disease Pharmacotherapy Issues in Acute Management and Secondary Prevention Peter J. Zed, B.Sc., B.Sc.(Pharm), Pharm.D. Pharmacotherapeutic Specialist - Emergency
Treatment Options for GERD or Acid Reflux Disease A Review of the Research for Adults
 Treatment Options for GERD or Acid Reflux Disease A Review of the Research for Adults hur till återvinna från prostataoperation Is This Information Right for Me? Yes, if: A doctor said that you have gastroesophageal
Treatment Options for GERD or Acid Reflux Disease A Review of the Research for Adults hur till återvinna från prostataoperation Is This Information Right for Me? Yes, if: A doctor said that you have gastroesophageal
PPIs: Good or Bad? 1. Basics of PPIs. Gastric Acid Basics. Outline. Gastric Acid Basics. Proton Pump Inhibitors (PPI)
") Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
Drug Class Review on Proton Pump Inhibitors
 Drug Class Review on Proton Pump Inhibitors Final Report Update 4 July 2006 Original Report Date: November 2002 Update 1 Report Date: April 2003 Update 2 Report Date: April 2004 Update 3 Report Date: May
Drug Class Review on Proton Pump Inhibitors Final Report Update 4 July 2006 Original Report Date: November 2002 Update 1 Report Date: April 2003 Update 2 Report Date: April 2004 Update 3 Report Date: May
Setting The setting was primary care. The economic study was conducted in Canada.
 Treating Helicobacter pylori infection in primary care patients with uninvestigated dyspepsia: the Canadian adult dyspepsia empiric treatment - Helicobacter pylori positive (CADET-Hp) randomised controlled
Treating Helicobacter pylori infection in primary care patients with uninvestigated dyspepsia: the Canadian adult dyspepsia empiric treatment - Helicobacter pylori positive (CADET-Hp) randomised controlled
Proton Pump Inhibitor De-prescribing Guidance
 Amendment History Proton Pump Inhibitor De-prescribing Guidance VERSION DATE AMENDMENT HISTORY 1.0 2013 Previous version 2.0 September 2015 Comments Amendment to Flow chart and addition of Rationale page
Amendment History Proton Pump Inhibitor De-prescribing Guidance VERSION DATE AMENDMENT HISTORY 1.0 2013 Previous version 2.0 September 2015 Comments Amendment to Flow chart and addition of Rationale page
High use of maintenance therapy after triple therapy regimes in Ireland
 High use of maintenance therapy after triple therapy regimes in Ireland K Bennett, H O Connor, M Barry, C O Morain, J Feely Department of Pharmacology & Therapeutics Department of Gastroenterology Trinity
High use of maintenance therapy after triple therapy regimes in Ireland K Bennett, H O Connor, M Barry, C O Morain, J Feely Department of Pharmacology & Therapeutics Department of Gastroenterology Trinity
National Digestive Diseases Information Clearinghouse
 Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA
 GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA MANAGEMENT Dyspepsia refers to a spectrum of usually intermittent upper gastrointestinal symptoms, including epigastric pain and heartburn. For the majority
GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA MANAGEMENT Dyspepsia refers to a spectrum of usually intermittent upper gastrointestinal symptoms, including epigastric pain and heartburn. For the majority
Unmet Needs in the Management of Gastroesophageal Reflux Disease
 Unmet Needs in the Management of Gastroesophageal Reflux Disease Ronnie Fass MD Professor of Medicine Case Western Reserve University Chairman, Division of Gastroenterology and Hepatology Director, Esophageal
Unmet Needs in the Management of Gastroesophageal Reflux Disease Ronnie Fass MD Professor of Medicine Case Western Reserve University Chairman, Division of Gastroenterology and Hepatology Director, Esophageal
Non-Ulcer Dyspepsia: what is it? What can we do with these patients? Overview. Dyspepsia Definition. Functional Dyspepsia. Dyspepsia the Basics
 Non-Ulcer : what is it? What can we do with these patients? Temporal Changes and Geographic Variations in Developing Peptic Ulcer Disease Gastric Cancer 1900 Eamonn M M Quigley MD FACG Alimentary Pharmabiotic
Non-Ulcer : what is it? What can we do with these patients? Temporal Changes and Geographic Variations in Developing Peptic Ulcer Disease Gastric Cancer 1900 Eamonn M M Quigley MD FACG Alimentary Pharmabiotic
Gastroesophageal Reflux Disease (GERD)
") Gastroesophageal Reflux Disease (GERD) Acid Reflux Acid reflux occurs when acid from the stomach moves backwards into the esophagus. Heartburn Heartburn is a symptom of acid reflux and GERD. It may feel
Gastroesophageal Reflux Disease (GERD) Acid Reflux Acid reflux occurs when acid from the stomach moves backwards into the esophagus. Heartburn Heartburn is a symptom of acid reflux and GERD. It may feel
Gastro-oesophageal reflux disease and peptic ulcer disease. By: Dr. Singanamala Suman Assistant Professor Department of Pharm.D
 Gastro-oesophageal reflux disease and peptic ulcer disease By: Dr. Singanamala Suman Assistant Professor Department of Pharm.D Gastro-oesophageal reflux disease and peptic ulcer disease Learning objectives:
Gastro-oesophageal reflux disease and peptic ulcer disease By: Dr. Singanamala Suman Assistant Professor Department of Pharm.D Gastro-oesophageal reflux disease and peptic ulcer disease Learning objectives:
All Indiana Medicaid Prescribers and Pharmacy Providers
 P R O V I D E R B U L L E T I N BT200148 NOVEMBER 28, 2001 To: All Indiana Medicaid Prescribers and Pharmacy Providers Subject: Note: The information in this bulletin regarding prior authorization payment
P R O V I D E R B U L L E T I N BT200148 NOVEMBER 28, 2001 To: All Indiana Medicaid Prescribers and Pharmacy Providers Subject: Note: The information in this bulletin regarding prior authorization payment
Helicobacter Pylori Testing HELICOBACTER PYLORI TESTING HS-131. Policy Number: HS-131. Original Effective Date: 9/17/2009
 Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
PEPTIC ULCER DISEASE JOHN R SALTZMAN, MD. Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School
 PEPTIC ULCER DISEASE JOHN R SALTZMAN, MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School No disclosures Disclosures Overview Causes of peptic ulcer disease
PEPTIC ULCER DISEASE JOHN R SALTZMAN, MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School No disclosures Disclosures Overview Causes of peptic ulcer disease
Heartburn, also referred to acid reflux, happens when stomach acid flows back (refluxes) into your esophagus.
 into your esophagus.") WHILE almost everyone experiences mild heartburn from time to time and many individuals have some antacids or another medication on hand for its relief, talk to your doctor, if you have heartburn more
WHILE almost everyone experiences mild heartburn from time to time and many individuals have some antacids or another medication on hand for its relief, talk to your doctor, if you have heartburn more
Disclosures. Proton Pump Inhibitors Deprescribing? Deprescribing PPI Objectives. Deprescribing. Proton Pump Inhibitors (PPI) 5/28/2018.
 5/28/2018.") Proton Pump Inhibitors Deprescribing? None Disclosures Chad Burski, MD Assistant Professor of Medicine UAB Gastroenterology Deprescribing PPI Objectives AR Why? Who? How? The mechanism of action of Proton
Proton Pump Inhibitors Deprescribing? None Disclosures Chad Burski, MD Assistant Professor of Medicine UAB Gastroenterology Deprescribing PPI Objectives AR Why? Who? How? The mechanism of action of Proton
ACID REFLUX & GERD: The Unsettling Reality in Canada
 ACID REFLUX & GERD: The Unsettling Reality in Canada gerd fact 1 see page 8 Canadian Society of Intestinal Research On average, ARD patients wait over two years before seeking care 1. 1 gerd fact 2 see
ACID REFLUX & GERD: The Unsettling Reality in Canada gerd fact 1 see page 8 Canadian Society of Intestinal Research On average, ARD patients wait over two years before seeking care 1. 1 gerd fact 2 see
COMPARISON OF ONCE-A-DAY VERSUS TWICE-A-DAY CLARITHROMYCIN IN TRIPLE THERAPY FOR HELICOBACTER PYLORI ERADICATION
 Phil J Gastroenterol 2006; 2: 25-29 COMPARISON OF ONCE-A-DAY VERSUS TWICE-A-DAY CLARITHROMYCIN IN TRIPLE THERAPY FOR HELICOBACTER PYLORI ERADICATION Marianne P Collado, Ma Fatima P Calida, Peter P Sy,
Phil J Gastroenterol 2006; 2: 25-29 COMPARISON OF ONCE-A-DAY VERSUS TWICE-A-DAY CLARITHROMYCIN IN TRIPLE THERAPY FOR HELICOBACTER PYLORI ERADICATION Marianne P Collado, Ma Fatima P Calida, Peter P Sy,
June By: Reza Gholami
 ACG/CAG guideline on Management of Dyspepsia June 2017 By: Reza Gholami DEFINITION OF DYSPEPSIA AND SCOPE OF THE GUIDELINE Dyspepsia was originally defined as any symptoms referable to the upper gastrointestinal
ACG/CAG guideline on Management of Dyspepsia June 2017 By: Reza Gholami DEFINITION OF DYSPEPSIA AND SCOPE OF THE GUIDELINE Dyspepsia was originally defined as any symptoms referable to the upper gastrointestinal
Policy Evaluation: Proton Pump Inhibitors (PPIs)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Peptic Ulcer Disease Update
 Peptic Ulcer Disease Update Col Pat Storms RAM 2005 Disclosure Information 84th Annual AsMA Scientific Meeting Col Patrick Storms I have no financial relationships to disclose. I will discuss the following
Peptic Ulcer Disease Update Col Pat Storms RAM 2005 Disclosure Information 84th Annual AsMA Scientific Meeting Col Patrick Storms I have no financial relationships to disclose. I will discuss the following
Setting The setting was secondary care. The economic study was carried out in Hong Kong, China.
 Cost-effectiveness of Helicobacter pylori "test and treat" for patients with typical reflux symptoms in a population with a high prevalence of H. pylori infection: a Markov model analysis You J H, Wong
Cost-effectiveness of Helicobacter pylori "test and treat" for patients with typical reflux symptoms in a population with a high prevalence of H. pylori infection: a Markov model analysis You J H, Wong
PREVENTING NSAID INDUCED GI COMPLICATIONS: AN ECONOMIC EVALUATION OF ALTERNATIVE STRATEGIES IN CANADA. February 13, 2007
 PREVENTING NSAID INDUCED GI COMPLICATIONS: AN ECONOMIC EVALUATION OF ALTERNATIVE STRATEGIES IN CANADA February 13, 2007 Canadian Agency for Drugs and Technologies in Health (CADTH) TABLE OF CONTENTS 1.0
PREVENTING NSAID INDUCED GI COMPLICATIONS: AN ECONOMIC EVALUATION OF ALTERNATIVE STRATEGIES IN CANADA February 13, 2007 Canadian Agency for Drugs and Technologies in Health (CADTH) TABLE OF CONTENTS 1.0
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: CP.CPA.209 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: Reference Number: CP.CPA.209 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy for important
Copy right protected Page 1
 DRUGS USED IN ULCERS AND GIT DISORDERS A peptic ulcer, also known as PUD or peptic ulcer disease is an ulcer of an area of the gastrointestinal tract that is usually acidic and thus extremely painful.
DRUGS USED IN ULCERS AND GIT DISORDERS A peptic ulcer, also known as PUD or peptic ulcer disease is an ulcer of an area of the gastrointestinal tract that is usually acidic and thus extremely painful.
Effective Health Care
 Effective Health Care Comparative Effectiveness of Management Strategies for Gastroesophageal Reflux Disease Executive Summary Background Gastroesophageal reflux disease (GERD), defined as weekly heartburn
Effective Health Care Comparative Effectiveness of Management Strategies for Gastroesophageal Reflux Disease Executive Summary Background Gastroesophageal reflux disease (GERD), defined as weekly heartburn
KK College of Nursing Peptic Ulcer Badil D ass Dass, Lecturer 25th July, 2011
 KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
One-third of adults experience pain or discomfort in
 GASTROENTEROLOGY 2002;122:1270 1285 Dyspepsia Management in Primary Care: A Decision Analysis of Competing Strategies BRENNAN M. R. SPIEGEL,* NIMISH B. VAKIL, and JOSHUA J. OFMAN*, *Department of Medicine
GASTROENTEROLOGY 2002;122:1270 1285 Dyspepsia Management in Primary Care: A Decision Analysis of Competing Strategies BRENNAN M. R. SPIEGEL,* NIMISH B. VAKIL, and JOSHUA J. OFMAN*, *Department of Medicine
Scientific Report. Evidence for PPI use in Gastroesophageal Reflux Disease, Dyspepsia and Peptic Ulcer Disease (Draft) December 6, 2006
 December 6, 2006") Scientific Report Evidence for PPI use in Gastroesophageal Reflux Disease, Dyspepsia and Peptic Ulcer Disease (Draft) December 6, 2006 CADTH COMPUS Expert Review Panel on PPIs Melissa C Brouwers, PhD,
Scientific Report Evidence for PPI use in Gastroesophageal Reflux Disease, Dyspepsia and Peptic Ulcer Disease (Draft) December 6, 2006 CADTH COMPUS Expert Review Panel on PPIs Melissa C Brouwers, PhD,
 Page 1 of 5 Official reprint from UpToDate www.uptodate.com 2017 UpToDate Patient education: Acid reflux (gastroesophageal reflux disease) in adults (The Basics) Written by the doctors and editors at UpToDate
Page 1 of 5 Official reprint from UpToDate www.uptodate.com 2017 UpToDate Patient education: Acid reflux (gastroesophageal reflux disease) in adults (The Basics) Written by the doctors and editors at UpToDate
Rpts. GENERAL General Schedule (Code GE)
") Pantoprazole 20mg Name, Restriction, Manner of administration and form Pantoprazole 20mg enteric tablet, 30 (8399C) Gastro-oesophageal reflux disease Name, Restriction, Manner of administration and form
Pantoprazole 20mg Name, Restriction, Manner of administration and form Pantoprazole 20mg enteric tablet, 30 (8399C) Gastro-oesophageal reflux disease Name, Restriction, Manner of administration and form
ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease
 ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease Philip O. Katz MD 1, Lauren B. Gerson MD, MSc 2 and Marcelo F. Vela MD, MSCR 3 1 Division of Gastroenterology, Einstein
ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease Philip O. Katz MD 1, Lauren B. Gerson MD, MSc 2 and Marcelo F. Vela MD, MSCR 3 1 Division of Gastroenterology, Einstein
You May Be at Risk. You are currently taking a proton-pump inhibitor (PPI): Dexlansoprazole (Dexilant ) Pantoprazole (Pantoloc, Panto IV )
: Dexlansoprazole (Dexilant ) Pantoprazole (Pantoloc, Panto IV )") You May Be at Risk. You are currently taking a proton-pump inhibitor (PPI): Dexlansoprazole (Dexilant ) Esomeprazole (Nexium ) Omeprazole (Losec, Olex ) Pantoprazole (Pantoloc, Panto IV ) Pantoprazole
You May Be at Risk. You are currently taking a proton-pump inhibitor (PPI): Dexlansoprazole (Dexilant ) Esomeprazole (Nexium ) Omeprazole (Losec, Olex ) Pantoprazole (Pantoloc, Panto IV ) Pantoprazole
Zantac for stomach ulcers
 P ford residence southampton, ny Zantac for stomach ulcers Information on the drug ranitidine (Zantac) used in and duodenal ulcers, heartburn, esophagitis, and Zollinger Ellison Syndrome. Side. But with
P ford residence southampton, ny Zantac for stomach ulcers Information on the drug ranitidine (Zantac) used in and duodenal ulcers, heartburn, esophagitis, and Zollinger Ellison Syndrome. Side. But with
Review Article. NSAID Gastropathy: An Update on Prevention. Introduction. Risk Factors. Kam-Chuen Lai
 Review Article NSAID Gastropathy: An Update on Prevention Kam-Chuen Lai Abstract: Keywords: Adverse reactions to non-steroidal anti-inflammatory drugs (NSAIDs) are common. Upper gastrointestinal complications
Review Article NSAID Gastropathy: An Update on Prevention Kam-Chuen Lai Abstract: Keywords: Adverse reactions to non-steroidal anti-inflammatory drugs (NSAIDs) are common. Upper gastrointestinal complications
Hold the Wrap! There is so much more to be done!
 Hold the Wrap! There is so much more to be done! (Well, a few things that can be done.) (Well, not all that much, really ) (But Blair has never killed anyone with a PPI!) Nicholas Shaheen, MD, MPH Center
Hold the Wrap! There is so much more to be done! (Well, a few things that can be done.) (Well, not all that much, really ) (But Blair has never killed anyone with a PPI!) Nicholas Shaheen, MD, MPH Center
Epidemiology of Peptic Ulcer Disease
 Epidemiology of Peptic Ulcer Disease Introduction Peptic Ulcer Disease (PUD) is disruption of the mucosal integrity of the stomach and/or duodenum leading to a local defect or excavation due to active
Epidemiology of Peptic Ulcer Disease Introduction Peptic Ulcer Disease (PUD) is disruption of the mucosal integrity of the stomach and/or duodenum leading to a local defect or excavation due to active
CYP2C19-Proton Pump Inhibitors
 CYP2C19-Proton Pump Inhibitors Cameron Thomas, Pharm.D. PGY2 Clinical Pharmacogenetics Resident St. Jude Children s Research Hospital February 1, 2018 Objectives: CYP2C19-PPI Implementation Review the
CYP2C19-Proton Pump Inhibitors Cameron Thomas, Pharm.D. PGY2 Clinical Pharmacogenetics Resident St. Jude Children s Research Hospital February 1, 2018 Objectives: CYP2C19-PPI Implementation Review the
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 PROTON PUMP INHIBITORS, NON-PREFERRED FORMS: ACIPHEX (rabeprazole sodium EC) oral tablet ACIPHEX SPRINKLE (rabeprazole sodium DR) oral capsule ESOMEPRAZOLE STRONTIUM (esomeprazole strontium DR) oral capsule
PROTON PUMP INHIBITORS, NON-PREFERRED FORMS: ACIPHEX (rabeprazole sodium EC) oral tablet ACIPHEX SPRINKLE (rabeprazole sodium DR) oral capsule ESOMEPRAZOLE STRONTIUM (esomeprazole strontium DR) oral capsule
https://www.uptodate.com/contents/acid-reflux-gastroesophageal-reflux-disease-in-adults-...
 Page 1 of 10 Official reprint from UpToDate www.uptodate.com 2017 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment.
Page 1 of 10 Official reprint from UpToDate www.uptodate.com 2017 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment.
6/25/ % 20% 50% 19% Functional Dyspepsia Peptic Ulcer GERD Cancer Other
 Peptic Ulcer Disease and Dyspepsia John M. Inadomi, MD Professor of Medicine UCSF Chief, Clinical Gastroenterology San Francisco General Hospital Case History 49 y/o woman complains of several months of
Peptic Ulcer Disease and Dyspepsia John M. Inadomi, MD Professor of Medicine UCSF Chief, Clinical Gastroenterology San Francisco General Hospital Case History 49 y/o woman complains of several months of
Esomeprazole versus omeprazole for the eradication of Helicobacter pylori infection
 International Journal of Community Medicine and Public Health Ageeli R et al. Int J Community Med Public Health. 2018 Jul;5(7):2686-2691 http://www.ijcmph.com pissn 2394-6032 eissn 2394-6040 Original Research
International Journal of Community Medicine and Public Health Ageeli R et al. Int J Community Med Public Health. 2018 Jul;5(7):2686-2691 http://www.ijcmph.com pissn 2394-6032 eissn 2394-6040 Original Research
Study population The study population comprised hypothetical patients with gastric and duodenal ulcer.
 Evaluation of the cost-effectiveness of Helicobacter pylori eradication triple therapy vs. conventional therapy for ulcers in Japan Ikeda S, Tamamuro T, Hamashima C, Asaka M Record Status This is a critical
Evaluation of the cost-effectiveness of Helicobacter pylori eradication triple therapy vs. conventional therapy for ulcers in Japan Ikeda S, Tamamuro T, Hamashima C, Asaka M Record Status This is a critical
LONG -TERM USE OF PPIS: INDICATIONS, BENEFITS AND HARMS. Jihane Naous, M.D.
 LONG -TERM USE OF PPIS: INDICATIONS, BENEFITS AND HARMS Jihane Naous, M.D. Objectives Identify the conditions supported by AGA/ACG guidelines necessitating long-term use of daily PPIs, Recognize which
LONG -TERM USE OF PPIS: INDICATIONS, BENEFITS AND HARMS Jihane Naous, M.D. Objectives Identify the conditions supported by AGA/ACG guidelines necessitating long-term use of daily PPIs, Recognize which
Functional Heartburn and Dyspepsia
 Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
CHAPTER 18. PEPTIC ULCER DISEASE, SELF-ASSESSMENT QUESTIONS. 1. Which of the following is not a common cause of peptic ulcer disease (PUD)?
?") CHAPTER 18. PEPTIC ULCER DISEASE, SELF-ASSESSMENT QUESTIONS 1. Which of the following is not a common cause of peptic ulcer disease (PUD)? A. Chronic alcohol ingestion B. Nonsteroidal antiinflammatory
CHAPTER 18. PEPTIC ULCER DISEASE, SELF-ASSESSMENT QUESTIONS 1. Which of the following is not a common cause of peptic ulcer disease (PUD)? A. Chronic alcohol ingestion B. Nonsteroidal antiinflammatory
Heartburn Overview. Causes & Risk Factors
 Return to Web version Heartburn Overview What is heartburn? Despite its name, heartburn doesn't affect the heart. Heartburn is a burning feeling in the lower chest, along with a sour or bitter taste in
Return to Web version Heartburn Overview What is heartburn? Despite its name, heartburn doesn't affect the heart. Heartburn is a burning feeling in the lower chest, along with a sour or bitter taste in
Drug Class Literature Scan: Proton Pump Inhibitors and Histamine-2 Receptor Antagonists
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Update on the Management of Acid-Related Disorders: A Canadian Perspective
 A FREE CONTINUING EDUCATION LESSON OBJECTIVES This professional development activity shares the clinical experience of experts, demonstrates best clinical practices, and highlights new clinical trials
A FREE CONTINUING EDUCATION LESSON OBJECTIVES This professional development activity shares the clinical experience of experts, demonstrates best clinical practices, and highlights new clinical trials
GERD: 2014 Dilemmas and Solutions. Ronnie Fass MD, FACP Professor of Medicine Case Western Reserve University
 GERD: 2014 Dilemmas and Solutions Ronnie Fass MD, FACP Professor of Medicine Case Western Reserve University How to Maximize Your PPI Treatment? Improve compliance and adherance Fass R. Am J Gastroenterol.
GERD: 2014 Dilemmas and Solutions Ronnie Fass MD, FACP Professor of Medicine Case Western Reserve University How to Maximize Your PPI Treatment? Improve compliance and adherance Fass R. Am J Gastroenterol.
Class Update: Proton Pump Inhibitors and Histamine 2 Receptor Antagonists
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: helicobacter_pylori_testing 01/01/2019 N/A 01/01/2020 01/01/2019 Policy Effective April 1, 2019 Description
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: helicobacter_pylori_testing 01/01/2019 N/A 01/01/2020 01/01/2019 Policy Effective April 1, 2019 Description
Alginates Extended Abstract
 Alginates Extended Abstract III) Clinical practice guidelines: DeVault KR, Castell DO; American College of Gastroenterology. Updated guidelines for the diagnosis and treatment of gastroesophageal reflux
Alginates Extended Abstract III) Clinical practice guidelines: DeVault KR, Castell DO; American College of Gastroenterology. Updated guidelines for the diagnosis and treatment of gastroesophageal reflux
Gastroesophageal Reflux Disease, Paraesophageal Hernias &
 530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs