Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
|
|
|
- Hugo Garrison
- 5 years ago
- Views:
Transcription

1
2 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2
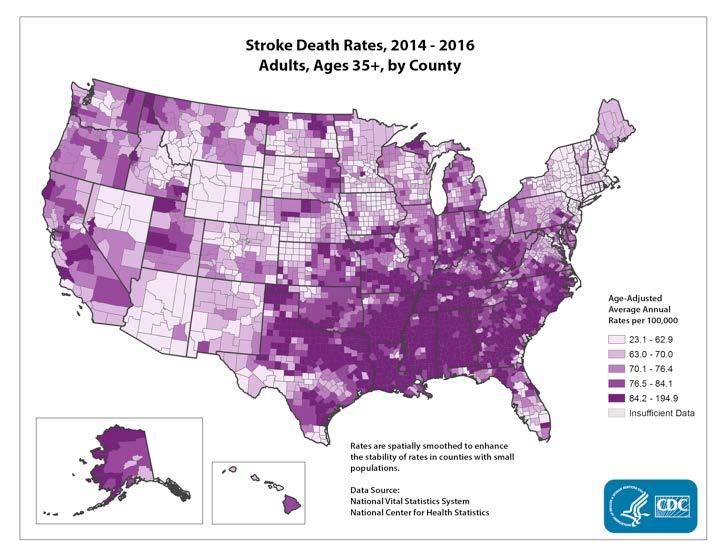
3 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in the entire country On average, one American dies from stroke every 4 minutes Every year, more than 795,000 people in the United States have a stroke. About 87% of all strokes are ischemic strokes, when blood flow to the brain is blocked Estimated $36.5 billion each year in costs Leading cause of serious long-term disability
4 4
5 Stroke Ischemic atherosclerotic cardiogenic Hemorrhagic Hypertensive Vascular aneurysmal AVM, cavernoma 5

6 Stroke To Cut or Not to Cut? 6
7 To Cut or Not to Cut? 7
8 To Cut or Not to Cut? 8
9 To Cut or Not to Cut? 9


10 To Cut or Not to Cut? 10


11 To Cut or Not to Cut? 11

12

13

14 14
15 Who, What, When and Why? Factors: Location, location, location Age comorbidity Timing (early vs late) ethics cost 15
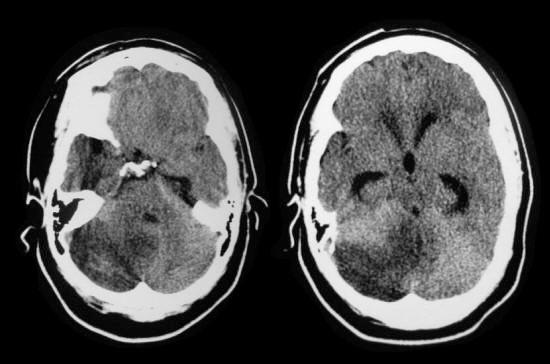
16 What? Malignant MCA territory infarction 10% of strokes rapid progressive deterioration 48 hours or less Mortality ~80% Cerebral edema herniation 16
17 What? Malignant MCA territory infarction Mortality risk factors: early obtundation dense hemiplegia age early parenchymal hypodenisty involving >50% of MCA territory Midline shift: 8-10mm Hyperdense MCA sign 17
18 Treatment: supportive BP for perfusion intubation glycemic control ICP management ICP monitor CSF Diversion Hyperosmolar therapies Mannitol Hypertonic Saline Surgery Guidelines 18

19 Hemicraniectomy Surgery 19
20 Guidelines Age < 70? nondominant vs dominant hemisphere ethical question evidence for large territorial infarction or signs of impending herniation on imaging Post admission neurologic deterioration 20
21 Mortality Hemicraniectomy May reduce mortality to as low as 32% in nondominant hemisphere strokes as low as 39% in all comers Alexander, Paul et al. Hemicraniectomy versus medical treatment with large MCA infarct: a review and meta-analysis BMJ open vol. 6,11 e Nov. 2016, doi: /bmjopen
22 Morbidity Hemicraniectomy Modified Rankin score 0-3: No symptoms - moderate disability (able to walk) 43% (surgical group) vs 21% (medical group) Park, Jaechan and Jeong-Hyun Hwang. Where are We Now with Decompressive Hemicraniectomy for Malignant Middle Cerebral Artery Infarction? Journal of cerebrovascular and endovascular neurosurgery vol. 15,2 (2013): Hofmeijer J, Kappelle LJ, Algra A, Amelink GJ, van Gijn J, van der Worp HB HAMLET investigators. Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery Infarction with Lifethreatening Edema Trial [HAMLET]): a multicentre, open, randomized trial. Lancet Neurol Apr;8(4):
23 When? Within 48 hours Vahedi K, Hofmeijer J, Juettler E, Vicaut E, George B, Algra A, et al. DECIMAL, DESTINY and HAMLET investigators. Early decompressive surgery in malignant infarction of the middle cerebral artery: a pooled analysis of three randomised controlled trials. Lancet Neurol Mar;6(3): No evidence for improvement in functional outcome with decompression > 96 hours after stroke 23
24 WHO? Age ish Major current randomized trials included age ranges from or 60 only DESTINY II trial: only 7% of pts > 60 were able to walk none were independent Infarct volume >145 cc on diffusion-weightedimages (DWI), One analysis found a high specificity of 98% for the development of MMCAI if the DWI lesion was >82 cc 24
25 Cerebellar Stroke Location PICA SCA AICA Complications Hydrocephalus brain stem compression 25
26 Cerebellar Stroke 26

27 Cerebellar Stroke Relatively Rare 1/5 of ischemic strokes PICA stroke: inferior vermis and tonsils SCA: superior hemisphere or vermis 27
28 Cerebellar Stroke Early findings: dizziness/vertigo nausea/vomiting loss of balance headache signs: ataxia/nystagmus/dysarthria Late findings: obtundation brainstem compression: typically findings associated with lower pons (loss lateral gaze, facial paralysis, small pupils) coma, posturing, ataxic respirations and respiratory failure 28
29 Cerebellar Stroke Indications for surgery: Hydrocephalus progressive brainstem compression must distinguish between Lateral Medullary Syndrome related to stroke. LMS not accompanied with altered sensorium 80% fatal without intervention Surgery: External ventriculostomy drain with caution Suboccipital craniectomy w/ foramen magnum enlargement and debridement of infarcted brain 29
30 Cerebellar Stroke Outcomes of surgery: German-Austrian Space-Occupying Cerebellar Infarction Study (GASCIS) Series of 84 patients with massive cerebellar infarction: 40% required surgical craniotomies 17% were managed with ventricular drainage In this series, 74% of patients had very good outcomes. 30
31 Intracerebral Hemorrhage 31
32 Locations: ICH Putaminal (most common) Thalamoperforators paramedian branches of Basilar artery Pontine ICH Lobar (underlying structural lesion likely) Cerebellar 32
33 ICH STICH (International Surgical Trial in Intracerebral Hemorrhage) 1033 patients enrolled BG or lobar ICH Surgery within 24 hours with possible surgery after 24 hours if deterioration despite medical management 33
34 STICH Outcome: Only 26% favorable outcome vs 24 % in medical management Subgroup analysis: 1cm or less from the cortical surface 34
35 STICH II 600 patients ICH volume ml No IVH Evacuation within 12 hours plus medical treatment vs medical management alone with option for later surgical intervention for deterioration 35
36 STICH II Outcome: Mortality 18% vs 24 % Surgery group had no vegetative survivors Trend to better GOS Subgroup Analysis Pts with GCS 9-12 have more favorable outcome with surgery GCS 13-15: no survival advantage with early surgery option for delayed surgery with deterioration 36
37 ICH Guidelines Non-Surgical Minimal symptoms -small volume < 30 cc Situational: -High ICH score -extensive ICH Large volume > 60cc -dominant hemisphere age >75 severe coagulopathy deep putaminal/bf ICH Surgical ICH w/ mass effect and symptoms related to increased ICP rapid deterioration Moderate volume =30-60 cc location - lobar - cerebellar Young patient < 60 37

38 Intraventricular Hemorrhage 38
39 IVH Mortality ~80% Associated with hydrocephalus Current guidelines for surgical intervention directed at HCP management with CSF diversion 39
40 IVH CLEAR trials I-III EVD with rtpa administration rtpa 1mg Q8 hours up to 12 doses or until ventricles cleared Early results showed improved clearance of blood from ventricles Inclusion criteria required casting of 3rd and 4th ventricles with small volume (<30cc) ICH. Deemed safe in selected patients 19% death rate vs 29% with saline 49% adverse events vs 62% Only 3% difference in disability score 40
41 Thank You! 41
42 42
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
National Collaborating Centre for Chronic Conditions at the Royal College of Physicians
 13. Surgery for acute stroke 13.2 Surgical referral for decompressive hemicraniectomy Reference Gupta R, Connolly ES, Mayer S et al. Hemicraniectomy for massive middle cerebral artery territory infarction:
13. Surgery for acute stroke 13.2 Surgical referral for decompressive hemicraniectomy Reference Gupta R, Connolly ES, Mayer S et al. Hemicraniectomy for massive middle cerebral artery territory infarction:
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD.
 Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Decompressive Hemicraniectomy in Acute Neurological Diseases
 Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS
 CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Early Management of Patients Considered for Hemicraniectomy Update 2015 Casaubon LK, Boulanger JM (Writing Group Chairs) on Behalf of the Stroke Hyperacute
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Early Management of Patients Considered for Hemicraniectomy Update 2015 Casaubon LK, Boulanger JM (Writing Group Chairs) on Behalf of the Stroke Hyperacute
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Intensive Medical Therapy with Therapeutic Hypothermia for Malignant Middle Cerebral Artery Infarction
 Intensive Medical Therapy with Therapeutic Hypothermia for Malignant Middle Cerebral Artery Infarction Kyu sun Lee 1, Sung Eun Lee, 1 Jin Soo Lee 1, Ji Man Hong 1 1 Department of Neurology, Ajou University
Intensive Medical Therapy with Therapeutic Hypothermia for Malignant Middle Cerebral Artery Infarction Kyu sun Lee 1, Sung Eun Lee, 1 Jin Soo Lee 1, Ji Man Hong 1 1 Department of Neurology, Ajou University
Surgical Management of an Unusual Case of Malignant Middle Cerebral Artery Infarction
 Elmer Press Case Report Surgical Management of an Unusual Case of Malignant Middle Cerebral Artery Infarction Jon Durrani a, c, Mohammed Rahman b, Phillip Porcelli a, Keith Kattner a Abstract Decompressive
Elmer Press Case Report Surgical Management of an Unusual Case of Malignant Middle Cerebral Artery Infarction Jon Durrani a, c, Mohammed Rahman b, Phillip Porcelli a, Keith Kattner a Abstract Decompressive
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
Case Series. Abstract. Introduction. Patients and Methods
 Case Series Salvage decompressive craniectomy in malignant MCA infarcts results of local experience at Shifa International Hospital, Islamabad, Pakistan Ismail A. Khatri, Maimoona Siddiqui, Inayatullah
Case Series Salvage decompressive craniectomy in malignant MCA infarcts results of local experience at Shifa International Hospital, Islamabad, Pakistan Ismail A. Khatri, Maimoona Siddiqui, Inayatullah
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Decompressive Hemicraniectomy for Malignant Middle Cerebral Artery Infarct
 DOI: 10.5137/1019-5149.JTN.13241-14.1 Received: 27.10.2014 / Accepted: 08.01.2015 Published Online: 24.02.2016 Original Investigation Decompressive Hemicraniectomy for Malignant Middle Cerebral Artery
DOI: 10.5137/1019-5149.JTN.13241-14.1 Received: 27.10.2014 / Accepted: 08.01.2015 Published Online: 24.02.2016 Original Investigation Decompressive Hemicraniectomy for Malignant Middle Cerebral Artery
7/22/2016. Navaz Karanjia, MD. FINANCIAL DISCLOSURE: none. UNLABELED/UNAPPROVED USE DISCLOSURE: none
 Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
Original Article CT grouping and microsurgical treatment strategies of hypertensive cerebellar hemorrhage
 Int J Clin Exp Med 2016;9(8):15921-15927 www.ijcem.com /ISSN:1940-5901/IJCEM0022273 Original Article CT grouping and microsurgical treatment strategies of hypertensive cerebellar hemorrhage Xielin Tang
Int J Clin Exp Med 2016;9(8):15921-15927 www.ijcem.com /ISSN:1940-5901/IJCEM0022273 Original Article CT grouping and microsurgical treatment strategies of hypertensive cerebellar hemorrhage Xielin Tang
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Large ischemic strokes presenting as malignant cerebral
 Neurosurg Focus 30 (6):E18, 2011 Decompressive hemicraniectomy after malignant middle cerebral artery infarction: rationale and controversies Omar M. Arnaout, M.D., Salah G. Aoun, M.D., H. Hunt Batjer,
Neurosurg Focus 30 (6):E18, 2011 Decompressive hemicraniectomy after malignant middle cerebral artery infarction: rationale and controversies Omar M. Arnaout, M.D., Salah G. Aoun, M.D., H. Hunt Batjer,
The management of ICH when to operate when not to?
 The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
ISCHEMIC STROKE IMAGING
 ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Outcomes of 33 patients from the wars in Iraq and Afghanistan undergoing bilateral or bicompartmental craniectomy
 J Neurosurg 115:124 129, 2011 Outcomes of 33 patients from the wars in Iraq and Afghanistan undergoing bilateral or bicompartmental craniectomy Clinical article Robert D. Ecker, M.D., LCDR, USN, 1 Lisa
J Neurosurg 115:124 129, 2011 Outcomes of 33 patients from the wars in Iraq and Afghanistan undergoing bilateral or bicompartmental craniectomy Clinical article Robert D. Ecker, M.D., LCDR, USN, 1 Lisa
Malignant Cerebral Infarction
 Malignant Cerebral Infarction Dr. Ahmed Reshi Neurocritical Care Operations Director Neurocritical Care Fellowship Director University of Minnesota Dr. Christopher Streib Stroke Operations Director Stroke
Malignant Cerebral Infarction Dr. Ahmed Reshi Neurocritical Care Operations Director Neurocritical Care Fellowship Director University of Minnesota Dr. Christopher Streib Stroke Operations Director Stroke
9/18/16. Management of Ischemic Stroke in the Intensive Care Unit. Outline. Introduction. Kyle B Walsh MD. Phases of Stroke Diagnosis and Treatment
 Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Surgical Treatment of Malignant Cerebral Infarction
 Case Report imedpub Journals www.imedpub.com Journal of Universal Surgery DOI: 10.21767/2254-6758.100088 Abstract Surgical Treatment of Malignant Cerebral Infarction Cerebrovascular disease (CVD) is the
Case Report imedpub Journals www.imedpub.com Journal of Universal Surgery DOI: 10.21767/2254-6758.100088 Abstract Surgical Treatment of Malignant Cerebral Infarction Cerebrovascular disease (CVD) is the
Intracerebral Hemorrhage
 Update on Intracerebral Hemorrhage November 8, 2013 Anne E. O Duffy, MD Assistant Professor of Neurology Stroke Division Intracerebral Hemorrhage Traumatic Spontaneous Primary (80-88%): due to spontaneous
Update on Intracerebral Hemorrhage November 8, 2013 Anne E. O Duffy, MD Assistant Professor of Neurology Stroke Division Intracerebral Hemorrhage Traumatic Spontaneous Primary (80-88%): due to spontaneous
Malignant Infarction Of The Middle Cerebral Artery In Elderly: A Point Of Controversy For Decompressive Surgery: A Case Report
 IPUB.COM The Internet Journal of Neurosurgery Volume 9 Number 1 Malignant Infarction Of The Middle Cerebral Artery In Elderly: A Point Of Controversy For Decompressive urgery: A Case Report L C Meguins,
IPUB.COM The Internet Journal of Neurosurgery Volume 9 Number 1 Malignant Infarction Of The Middle Cerebral Artery In Elderly: A Point Of Controversy For Decompressive urgery: A Case Report L C Meguins,
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke is the most prevalent disease involving the
 Treatment of Cerebellar Infarction by Decompressive Suboccipital Craniectomy Han-Jung Chen, MD; Tao-Chen Lee, MD; and Chi-Peng Wei, MD Background and Purpose: We present an anecdotal series of 11 patients
Treatment of Cerebellar Infarction by Decompressive Suboccipital Craniectomy Han-Jung Chen, MD; Tao-Chen Lee, MD; and Chi-Peng Wei, MD Background and Purpose: We present an anecdotal series of 11 patients
Stereotactic Burr Hole Aspiration Surgery for Spontaneous Hypertensive Cerebellar Hemorrhage
 Journal of Cerebrovascular and Endovascular Neurosurgery ISSN 2234-8565, EISSN 2287-3139, http://dx.doi.org/10.7461/jcen.2012.14.3.170 Original Article Stereotactic Burr Hole Aspiration Surgery for Spontaneous
Journal of Cerebrovascular and Endovascular Neurosurgery ISSN 2234-8565, EISSN 2287-3139, http://dx.doi.org/10.7461/jcen.2012.14.3.170 Original Article Stereotactic Burr Hole Aspiration Surgery for Spontaneous
Lothian Audit of the Treatment of Cerebral Haemorrhage (LATCH)
") 1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Tyler Carson D.O., Vladamir Cortez D.O., Dan E. Miulli D.O.
 Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Microsurgery for ruptured cerebellar arteriovenous malformations
 European Review for Medical and Pharmacological Sciences Microsurgery for ruptured cerebellar arteriovenous malformations S.-F. GONG 1,2, X.-B. WANG 1,3, Y.-Q. LIAO 1,2, T.-P. JIANG 1,2, J.-B. HE 1,2,
European Review for Medical and Pharmacological Sciences Microsurgery for ruptured cerebellar arteriovenous malformations S.-F. GONG 1,2, X.-B. WANG 1,3, Y.-Q. LIAO 1,2, T.-P. JIANG 1,2, J.-B. HE 1,2,
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Intracerebral Hemorrhage
 Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
Byung Rhae Yoo, Chan Jong Yoo, Myeong Jin Kim, Woo-Kyung Kim, Dae Han Choi
 Journal of Cerebrovascular and Endovascular Neurosurgery pissn 2234-8565, eissn 2287-3139, http://dx.doi.org/10.7461/jcen.2016.18.3.175 Original Article Analysis of the Outcome and Prognostic Factors of
Journal of Cerebrovascular and Endovascular Neurosurgery pissn 2234-8565, eissn 2287-3139, http://dx.doi.org/10.7461/jcen.2016.18.3.175 Original Article Analysis of the Outcome and Prognostic Factors of
Chapter 10. Long-term cognitive outcome after decompressive surgery for space-occupying hemispheric infarction
 Cognitive outcome after decompressive surgery Chapter 10 Long-term cognitive outcome after decompressive surgery for space-occupying hemispheric infarction Jeannette Hofmeijer, H. Bart van der Worp, G.
Cognitive outcome after decompressive surgery Chapter 10 Long-term cognitive outcome after decompressive surgery for space-occupying hemispheric infarction Jeannette Hofmeijer, H. Bart van der Worp, G.
Journal of Clinical Neuroscience
 Journal of Clinical Neuroscience 19 (2012) 1222 1227 Contents lists available at SciVerse ScienceDirect Journal of Clinical Neuroscience journal homepage: www.elsevier.com/locate/jocn Clinical Study Craniectomy-Associated
Journal of Clinical Neuroscience 19 (2012) 1222 1227 Contents lists available at SciVerse ScienceDirect Journal of Clinical Neuroscience journal homepage: www.elsevier.com/locate/jocn Clinical Study Craniectomy-Associated
Outlook for intracerebral haemorrhage after a MISTIE spell
 Outlook for intracerebral haemorrhage after a MISTIE spell David J Werring PhD FRCP Stroke Research Centre, Department of Brain Repair and Rehabilitation, UCL Institute of Neurology, National Hospital
Outlook for intracerebral haemorrhage after a MISTIE spell David J Werring PhD FRCP Stroke Research Centre, Department of Brain Repair and Rehabilitation, UCL Institute of Neurology, National Hospital
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
The management of ICH when to operate when not to?
 The management of ICH when to operate when not to? ICH is a Bad Disease High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
The management of ICH when to operate when not to? ICH is a Bad Disease High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Ventriculostomy and Risk of Upward Herniation in Patients with Obstructive Hydrocephalus from Posterior Fossa Mass Lesions
 https://doi.org/10.1007/s12028-017-0487-3 ORIGINAL ARTICLE Ventriculostomy and Risk of Upward Herniation in Patients with Obstructive Hydrocephalus from Posterior Fossa Mass Lesions Sherri A. Braksick
https://doi.org/10.1007/s12028-017-0487-3 ORIGINAL ARTICLE Ventriculostomy and Risk of Upward Herniation in Patients with Obstructive Hydrocephalus from Posterior Fossa Mass Lesions Sherri A. Braksick
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Feeling the Pressure
 Feeling the Pressure (as in Intracranial Pressure.) Liz Kim, MSN, ACNS-BC, FAHA Advanced Practice Provider Neurocritical Care Stanford Health Care May 15, 2017 World Live Neurovascular Conference Disclosures
Feeling the Pressure (as in Intracranial Pressure.) Liz Kim, MSN, ACNS-BC, FAHA Advanced Practice Provider Neurocritical Care Stanford Health Care May 15, 2017 World Live Neurovascular Conference Disclosures
Retrospective Comparison of Decompressive Hemicraniectomy and Hematoma Evacuation for Spontaneous Supratentorial Intracerebral Hematoma
 ORIGINAL ARTICLE Retrospective Comparison of Decompressive Hemicraniectomy and Hematoma Evacuation for Spontaneous Supratentorial Intracerebral Hematoma Joarder MA 1, Karim AKMB 2, Kamal T 3, Sujon SI
ORIGINAL ARTICLE Retrospective Comparison of Decompressive Hemicraniectomy and Hematoma Evacuation for Spontaneous Supratentorial Intracerebral Hematoma Joarder MA 1, Karim AKMB 2, Kamal T 3, Sujon SI
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
A few Neurosurgical Emergencies. Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015
 A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
Standard NICE (CG ) RCP (2016)
 RCP (2016)") Standard NICE (CG68 2008) RCP (2016) Stroke Unit Adults presenting at an A&E department with suspected stroke are admitted to a specialist stroke unit within 4 hours direct admission of patients with acute
Standard NICE (CG68 2008) RCP (2016) Stroke Unit Adults presenting at an A&E department with suspected stroke are admitted to a specialist stroke unit within 4 hours direct admission of patients with acute
The Worst Headache of My Life Hemorrhagic Stroke
 The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
Intracranial spontaneous hemorrhage mechanisms, imaging and management
 Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
NEURO IMAGING OF ACUTE STROKE
 1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER
 CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
Patients with cerebellar infarction should not be neglected
 Preventive Suboccipital Decompressive Craniectomy for Cerebellar Infarction A Retrospective-Matched Case Control Study Myeong Jin Kim, MD; Sang Kyu Park, MD; Jihye Song, MD; Se-yang Oh, MD; Yong Cheol
Preventive Suboccipital Decompressive Craniectomy for Cerebellar Infarction A Retrospective-Matched Case Control Study Myeong Jin Kim, MD; Sang Kyu Park, MD; Jihye Song, MD; Se-yang Oh, MD; Yong Cheol
Chapter 8: Cerebral protection Stephen Lo
 Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Acute cerebellar infarction or hemorrhage may initially manifest in a clinically indolent
 NEUROLOGICAL REVIEW SECTION EDITOR: DAVID E. PLEASURE, MD Management of Acute Cerebellar Stroke Matt B. Jensen, MD; Erik K. St. Louis, MD Acute cerebellar infarction or hemorrhage may initially manifest
NEUROLOGICAL REVIEW SECTION EDITOR: DAVID E. PLEASURE, MD Management of Acute Cerebellar Stroke Matt B. Jensen, MD; Erik K. St. Louis, MD Acute cerebellar infarction or hemorrhage may initially manifest
Outcome and Prognostic Factors of Decompressive Hemicraniectomy in Malignant Middle Cerebral Artery Infarction
 ORIGINAL ARTICLE Outcome and Prognostic Factors of Decompressive Hemicraniectomy in Malignant Middle Cerebral Artery Infarction Chun-Chung Chen, Der-Yang Cho*, Shu-Chiu Tsai Department of Neurosurgery,
ORIGINAL ARTICLE Outcome and Prognostic Factors of Decompressive Hemicraniectomy in Malignant Middle Cerebral Artery Infarction Chun-Chung Chen, Der-Yang Cho*, Shu-Chiu Tsai Department of Neurosurgery,
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
Emergency Management of Acute Ischemic Stroke in Incapacitated Patients Who Have No Surrogate Decision Makers Fred Rincon, MD, MSc
 Ethical Perspectives Emergency Management of Acute Ischemic Stroke in Incapacitated Patients Who Have No Surrogate Decision Makers Fred Rincon, MD, MSc Address correspondence to Dr Fred Rincon, Department
Ethical Perspectives Emergency Management of Acute Ischemic Stroke in Incapacitated Patients Who Have No Surrogate Decision Makers Fred Rincon, MD, MSc Address correspondence to Dr Fred Rincon, Department
Management of Intracerebral Haemorrhage
 Management of Intracerebral Haemorrhage It s the worst type of stroke. Least treatable form of stroke Evidence-base limited most Overall mortality 35-50% Half of these would die within first 24 hours
Management of Intracerebral Haemorrhage It s the worst type of stroke. Least treatable form of stroke Evidence-base limited most Overall mortality 35-50% Half of these would die within first 24 hours
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH
 SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
BRAIN HERNIATION S54 (1) Brain Herniation
 Brain Herniation") BRAIN HERNIATION S54 (1) Brain Herniation Last updated: September 5, 2017 PATHOPHYSIOLOGY... 1 TYPES OF HERNIATION... 2 SUPRATENTORIAL MASSES... 2 Central (s. downward transtentorial) herniation... 2 Uncal
BRAIN HERNIATION S54 (1) Brain Herniation Last updated: September 5, 2017 PATHOPHYSIOLOGY... 1 TYPES OF HERNIATION... 2 SUPRATENTORIAL MASSES... 2 Central (s. downward transtentorial) herniation... 2 Uncal
WHITE PAPER: A GUIDE TO UNDERSTANDING LARGE HEMISPHERIC INFARCTION
 WHITE PAPER: A GUIDE TO UNDERSTANDING LARGE HEMISPHERIC INFARCTION Large Hemispheric Infarction (LHI) represents a minority of strokes, yet is responsible for a disproportionately large share of stroke-related
WHITE PAPER: A GUIDE TO UNDERSTANDING LARGE HEMISPHERIC INFARCTION Large Hemispheric Infarction (LHI) represents a minority of strokes, yet is responsible for a disproportionately large share of stroke-related
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
Jan 5, Coma 8 years. Jan 11, 2014
 Jan 5, 2006 Coma 8 years Jan 11, 2014 CT Scan of Head showing large right frontal ICH The Intracerebral Hemorrhage: Team Approach Rodney Leacock MD Introduction Intracerebral hemorrhage (ICH) is a very
Jan 5, 2006 Coma 8 years Jan 11, 2014 CT Scan of Head showing large right frontal ICH The Intracerebral Hemorrhage: Team Approach Rodney Leacock MD Introduction Intracerebral hemorrhage (ICH) is a very
Vascular Malformations of the Brain: A Review of Imaging Features and Risks
 Vascular Malformations of the Brain: A Review of Imaging Features and Risks Comprehensive Neuroradiology: Best Practices October 27-30, 2016 Sudhakar R. Satti, MD Associate Director Neurointerventional
Vascular Malformations of the Brain: A Review of Imaging Features and Risks Comprehensive Neuroradiology: Best Practices October 27-30, 2016 Sudhakar R. Satti, MD Associate Director Neurointerventional
HHS Public Access Author manuscript Am J Emerg Med. Author manuscript; available in PMC 2016 April 01.
 The excess cost of inter-island transfer of intracerebral hemorrhage patients Kazuma Nakagawa, MD 1,2, Alexandra Galati, BA 2, and Deborah Taira Juarez, ScD 3 1 Neuroscience Institute, The Queen s Medical
The excess cost of inter-island transfer of intracerebral hemorrhage patients Kazuma Nakagawa, MD 1,2, Alexandra Galati, BA 2, and Deborah Taira Juarez, ScD 3 1 Neuroscience Institute, The Queen s Medical
Brain under pressure Managing ICP. Giuseppe
 Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Spontaneous ICH: the issue of perihemmorhagic edema
 4 rd Congress of the European Academy of Neurology Lisbon, Portugal, June 16-19, 2018 Teaching Course 13 New concepts in critical care of stroke patients - Level 3 Spontaneous ICH: the issue of perihemmorhagic
4 rd Congress of the European Academy of Neurology Lisbon, Portugal, June 16-19, 2018 Teaching Course 13 New concepts in critical care of stroke patients - Level 3 Spontaneous ICH: the issue of perihemmorhagic
The Role of Neuroimaging in Acute Stroke. Bradley Molyneaux, HMS IV
 The Role of Neuroimaging in Acute Stroke Bradley Molyneaux, HMS IV Patient CR 62 yo F w/ 2 wk h/o altered mental status Presents to ED w/ confusion following a fall 1 day prior New onset left facial droop
The Role of Neuroimaging in Acute Stroke Bradley Molyneaux, HMS IV Patient CR 62 yo F w/ 2 wk h/o altered mental status Presents to ED w/ confusion following a fall 1 day prior New onset left facial droop
Classification of Stroke. CNA Neuroscience Nursing Course: Cerebrovascular Disorders. Stroke in Canada
 CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
Case Report Intraoperative Visualization of Bilateral Thrombosis in the Posterior Inferior Cerebellar Artery Apparent in the Telovelomedullary Segment
 Case Reports in Neurological Medicine, Article ID 247652, 4 pages http://dx.doi.org/10.1155/2014/247652 Case Report Intraoperative Visualization of Bilateral Thrombosis in the Posterior Inferior Cerebellar
Case Reports in Neurological Medicine, Article ID 247652, 4 pages http://dx.doi.org/10.1155/2014/247652 Case Report Intraoperative Visualization of Bilateral Thrombosis in the Posterior Inferior Cerebellar
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ABSTRACT. n engl j med 370;12 nejm.org march 20,
 The new england journal of medicine established in 1812 march 20, 2014 vol. 370 no. 12 in Older Patients with Extensive Middle-Cerebral-Artery Stroke Eric Jüttler, M.D., Ph.D., Andreas Unterberg, M.D.,
The new england journal of medicine established in 1812 march 20, 2014 vol. 370 no. 12 in Older Patients with Extensive Middle-Cerebral-Artery Stroke Eric Jüttler, M.D., Ph.D., Andreas Unterberg, M.D.,
The surgical strategy of hypertensive thalamus hemorrhage. Lu Ma, Chao You Dept. of Neurosurgery, West China Hospital
 The surgical strategy of hypertensive thalamus hemorrhage Lu Ma, Chao You Dept. of Neurosurgery, West China Hospital Preface Spontaneous Intracranial hemorrhage (SICH) Spontaneous thalamus hemorrhage---hypertensive
The surgical strategy of hypertensive thalamus hemorrhage Lu Ma, Chao You Dept. of Neurosurgery, West China Hospital Preface Spontaneous Intracranial hemorrhage (SICH) Spontaneous thalamus hemorrhage---hypertensive
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Update in Management of Acute Spontaneous Intracerebral Haemorrhage
 Update in Management of Acute Spontaneous Intracerebral Haemorrhage Aldy S. Rambe Neurology Department, School of Medicine EPIDEMIOLOGY Although ICH represents only about 9% of all stroke, it accounts
Update in Management of Acute Spontaneous Intracerebral Haemorrhage Aldy S. Rambe Neurology Department, School of Medicine EPIDEMIOLOGY Although ICH represents only about 9% of all stroke, it accounts