Acute Ischemic Stroke Mechanism, Diagnosis, Treatment
|
|
|
- Nicholas Walsh
- 6 years ago
- Views:
Transcription
1 Acute Ischemic Stroke Mechanism, Diagnosis, Treatment IM Resident Lecture December 2016 Mohammad Shafie, MD PhD MEng Department of Neurology UC Irvine
2 Objectives Better understanding of stroke mechanisms contributing to stroke etiology Develop a systematic diagnostic approach that will facilitate expeditious identification of patients eligible for acute therapies. Familiarity with current selection criteria for acute stroke reperfusion therapies
3 Mechanism of Brain Tissue Injury in Stroke Stroke: Acute injury to brain by an abnormality of blood supply Ischemic Stroke ~ 80% Lack of or diminished blood flow Hemorrhagic Stroke ~20% Release of blood into the brain & extravascular spaces within the cranium or skull
4 Acute Reperfusion Therapy Treatment intended to emergently restoring blood flow in the acutely occluded cerebral artery. Pharmacologic IV tpa, and/or Mechanical Endovascular mechanical thrombectomy
5 The Numbers Nationally ~800,000 new annual stroke cases with ~600,000 first-time strokes Fifth cause of death with ~130,000 stroke-related deaths per year On average, every 40 seconds, someone has a stroke every 4 minutes,, someone died of a stroke Women have a higher lifetime risk of stroke than men Affects 3 times as many women as breast CA and receives much less public attention Stroke morbidity and mortality disproportionately affects minority populations Between 2012 and 2030 the total direct medical stroke-related costs are projected to triple, from $71.6 to $184.1 billion Globally In 2013, second-leading cause of death (after heart disease) In 2010, 33 million strokes with 16.9 million as a first stroke Burden of stroke now disproportionately affects those living in lower-income countries Both globally and nationally A leading cause of disability Mozzafarrian et al. 2016

6 Cerebrovascular Arterial Circulation


7 Cerebrovascular Arterial Circulation: Large Vessels Anterior Circulation Posterior Circulation
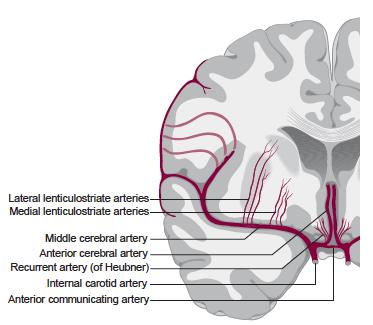
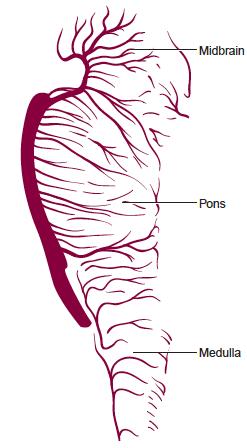
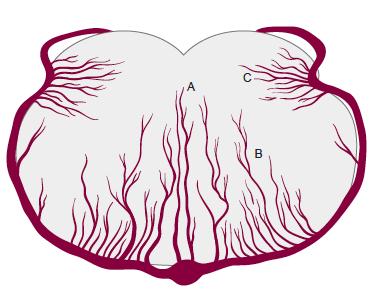
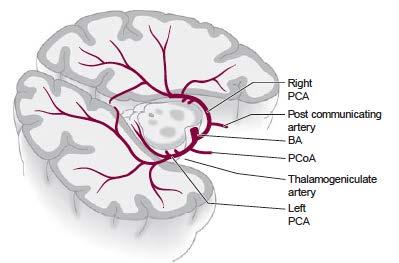
8 Cerebrovascular Arterial Circulation: Small Vessels Penetrators/Perforators Anterior Circulation Posterior Circulation
9 Ischemic Stroke Mechanisms A heterogeneous disease Classification is not always straight-forward Potential for combination of mechanisms Thrombosis Embolism Hypoperfusion


10 Ischemic Stroke Mechanisms Thrombosis Localized obstruction of blood flow due to an occlusive process with one or more blood vessels Atherosclerosis, most common vascular pathology Larger extra- and intra-cranial arteries Areas of turbulent flow and low shear stress, i.e. arterial bifurcations Hypertension Hypertrophy of media Lipohyalinosis Small intracranial penetrating and perforating arteries Dissection Primary hematologic conditions Arteritis/Vasculitis
, air, fibrocartilagenous tissue, amniotic fluid, tumor")
11 Ischemic Stroke Mechanisms Embolism Material formed elsewhere, typically from a proximal donor source, within the vascular system lodges in a recipient artery and blocks blood flow Cardiac source, most common Major arteries - artery-to-artery embolism Paradoxical embolism from systemic veins Through venous to arterial shunts, i.e. PFO, ASD Cholesterol (post-fracture), air, fibrocartilagenous tissue, amniotic fluid, tumor

12 Ischemic Stroke Mechanisms Hypoperfusion systemic perfusion = cerebral perfusion watershed regions most susceptible at periphery of major vascular supply territory Cardiac, most common Blood loss, Hypovolemia
13 Ischemic Stroke Subtypes TOAST classification of subtypes of acute ischemic stroke (Adams et al. 1993) Classification scheme for ischemic stroke widely used with good inter-observer agreement Attempts to classify based on the major mechanisms recognized as the cause of most ischemic strokes Five subtypes Large artery disease (20%) highest recurrence Small vessel disease (25%) best outcomes, survival, recurrence Lacunar: Cardioembolic (20%) worst outcomes, highest mortality Stroke of other determined etiology (5%) Cryptogenic (30%)
14 Transient Ischemic Attack (TIA) A brief episode of neurological dysfunction caused by focal brain or retinal ischemia, with clinical symptoms typically lasting less than an hour, and without evidence of acute infarction. Transient reduction of blood flow to a region in brain in the absence of infarction on brain imaging Most TIAs last only a few minutes and the great majority less than an hour. Those lasting longer than an hour often associated with brain infarction on MRI DWI
15 Transient Ischemic Attack (TIA) Mechanisms for TIA are similar to ischemic stroke Reconstitution of flow to the hypoperfused region results in the resolution of symptoms Significance of TIAs is increased risk of ischemic stroke after a TIA specifically early on after a TIA Prompt evaluation of mechanism and appropriate treatment
16 ABCD 2 Score Risk Factor Points Age 60 years Blood Pressure Systolic BP 140 mmhg OR Diastolic BP 90 mmhg Clinical features of TIA Unilateral weakness w/ or w/o speech impairment OR Speech impairment w/o unilateral weakness Duration 60 minutes minutes Diabetes 1 Total ABCD 2 score 0-7 Total Score 0-3: 1.0% 2-day stroke risk 4-5: 4.1% 2-day stroke risk 6-7: 8.1% 2-day stroke risk
17 Approach To Guide Acute Reperfusion Therapy Goal: Expeditious identification of eligible patients Bedside history and exam Neuroimaging Ancillary Testing
18 History Time Symptom onset-time available Use of cues Last well-known time (LKWT) Awaken with symptoms Reset after TIA Nature of symptom onset Sudden and maximal : embolic Gradual and progressive : thrombotic Other significant medical history
19 History History of the present illness Time of symptom onset Evolution of symptoms Convulsion or loss of consciousness at onset Headache Chest pain at onset Medical history Prior intracerebral hemorrhage Recent stroke Recent head trauma or loss of consciousness Recent myocardial infarction Surgical History Recent surgical procedures Arterial puncture Review of systems Gastrointestinal or genitourinary bleeding Medications Anticoagulant therapy
20 Common Ischemic Stroke Syndromes Vascular Territory L MCA distribution R MCA distribution L PCA distribution R PCA distribution Vertebrobasilar distribution (A) Internal capsule/corona radiata (B) Ventral pons Signs and Symptoms Aphasia, R hemiparesis/hemisensory disturbance, R homonymous hemianopsia, L head and gaze preference L hemispatial neglect, L hemiparesis/hemisensory disturbance, L homonymous hemianopsia, R head and gaze preference, anosognosia R visual field defect, impaired reading with intact writing (alexia without agraphia), poor color naming, R hemisensory disturbance L visual field defect, visual neglect, L hemisensory disturbance Dizziness, vertigo, nausea, diplopia, quadriparesis, crossed motor or sensory findings, truncal or limb ataxia, visual loss/dimming, impaired consciousness Penetrating artery distribution (ie, lacunar syndromes) (A, B) Contralateral hemiparesis alone (pure motor stroke) OR contralateral hemiparesis + ataxia out of proportion to weakness (ataxic-hemiparesis); no cortical signs (C) Thalamus (C) Contralateral sensory loss alone (pure sensory stroke); no cortical sign
21 Neurologic Examination: The NIH Stroke Scale (NIHSS) Category Scale Definition Category Scale Definition Category Scale Definition 1a. LOC 0 = Alert 1 = Not alert, arousable 2 = Not alert, obtunded 3 = Unresponsive 1b. Questions 0 = Answers both correctly 1=Answers one correctly 2=Answers neither correctly 1c. Commands 0=Performs both tasks correctly 1=Performs one task correctly 2=Performs neither task 2. Gaze 0=Normal 1=Partial gaze palsy 2=Total gaze palsy 3. Visual fields 0=No visual loss 1=Partial gaze palsy 2=Total gaze palsy 4. Facial Palsy 0=Normal 1=Minor paralysis 2=Partial paralysis 3=Complete paralysis 5a. L motor arm 0=No drift 1=Drift before 10 seconds 2=Falls before 10 seconds 3=No effort against gravity 4=No movement 5b. R motor arm 0=No drift 1=Drift before 10 seconds 2=Falls before 10 seconds 3=No effort against gravity 4=No movement 6a. L motor leg 0=No drift 1=Drift before 10 seconds 2=Falls before 10 seconds 3=No effort against gravity 4=No movement 6b. R motor leg 0=No drift 1=Drift before 10 seconds 2=Falls before 10 seconds 3=No effort against gravity 4=No movement 7. Ataxia 0=Absent 1=One limb 2=Two limbs 8. Sensory 0=Normal 1=Mild loss 2=Severe loss 9. Language 0=Normal 1=Mild aphasia 2=Severe aphasia 3=Mute or global aphasia 10.Dysarthria 11. Extinction/inat tention 0=Normal 1=Mild 2=Severe 0=Normal 1=Mild 2=Severe
22 Neurologic Examination: The NIH Stroke Scale (NIHSS) Limitation of NIHSS Does not include a detailed assessment of CNs Milder deficits may escape detection Higher stroke severity in dominant vs non-dominant hemispheres NIHSS should not take the place of a focused and thorough neurologic evaluation
23 Differential Diagnosis Intracerebral hemorrhage vs Stroke mimics Diagnosis Seizure (Post-ictal) Hypoglycemia Migraine Mass lesions/tumor Subarachnoid hemorrhage Encephalopathy Peripheral vestibulopathy Reactivation of prior deficits Conversion reaction Comments Focal deficits. Spontaneous resolution over hours (may last up to 48 hours) Aphasia or hemiplegia. Variable drowsiness or obtundation. Blood glucose usually <45 mg/dl. Resolution of symptoms (immediate to hours) with IV glucose. Symptoms begin in one region and gradually spread to involve other areas. Duration of symptoms. Associated symptoms. Headache, thunderclap headache. Hypertensive, hyperosmolar hyperglycemia, hyponatremia, hepatic. Associated with altered LOC, poor attention, or disorientation Vertigo, nystagmus on exam, nausea, emesis. Imaging evidence or history of remove stroke. Previous deficits may have resolved completely. Diagnosis of exclusion. Comorbid psychiatric problems are common. Paresis, paralysis, and movement disorders are common.

24 Acute Stroke Neuroimaging Initial imaging of brain parenchyma Exclude hemorrhagic stroke: CT or MRI Ischemia Hemorrhage
 is equal to that of CT.")
25 Acute Stroke Neuroimaging For acute hemorrhage accuracy of MRI (GRE sequences) is equal to that of CT. (Kidwell et al, 2004) CT Hemorrhage MRI GRE
26 Acute Stroke Neuroimaging CT vs MRI CT Advantages: Fast acquisition time, widely available, sensitive to hemorrhage Disadvantages: Limited sensitivity to infarct size, location of early ischemia MRI (DWI sequence) Advantage: Sensitive to early ischemia, fast acquisition time, high conspicuity of lesion Disadvantage: Lack of availability, patient contraindication (eg, metals, claustrophobia), long acquisition time
 Specificity: 86-100% Sensitivity:")
27 Acute Stroke Neuroimaging Imaging of the early ischemic changes: CT or MRI Non-contrast CT (within 6-8 hour) Specificity: % Sensitivity: 20-75% Worse in posterior fossa ischemia MRI DWI sequence (within <6 hours) Specificity: % Sensitivity: %
28 Multimodal Neuroimaging Potential to improve patient selection criteria to guide therapy Noninvasive multimodal CT and MR Angiography (A): vessel imaging (CTA, MRA) Perfusion (P): tissue viability, cerebral perfusion (CTP, MRP) Multimodal MRI parenchymal sequences Diffusion-weighted imaging (DWI) Apparent diffusion coefficient (ADC) Fluid-attenuated inversion recovery (FLAIR) Gradient recoiled echo (GRE) Susceptibility-weighted imaging (SWI) No standardized imaging protocols for acute stroke exist Advanced neuroimaging should not delay the administration of IV rtpa
29 Ancillary Testing Blood glucose (Finger stick is acceptable) The only lab result needed for administration of IV tpa Administration of IV tpa should NOT be delayed while awaiting results of the following lab results: Complete blood count (CBC) Unless clinical suspicion of a bleeding abnormality or thrombocytopenia < 3/1000 will have unsuspected thrombocytopenia (Cucchiara et al, 2007) Coagulation panel (PT/INR/PTT) Patient has received heparin or warfarin, Patient has received other anticoagulants <4/1000 will have an unsuspected INR>1.7 (Rost et al, 2009) Chemistry panel (Chem7) Cardiac enzymes CXR 12-lead ECG
30 Acute Ischemic Stroke Therapy Neuroprotectants Over 1,000 agents in clinical trials None has proved successful Acute reperfusion therapy IV rtpa (tissue plasminogen activator) Endovascular thrombectomy/embolectomy Combination of above Treatment is time-dependent Time is Brain!!
31 Recombinant Tissue Plasminogen Activator (rtpa) The only FDA-approved thrombolytic agent Up to 3 hours from symptom onset time Recommended by AHA/ASA Up to 4.5 hours from symptom onset time Selected patient population NOT FDA-approved Other agents available as experimental in the context of clinical trials Desmoteplase, Tenecteplase
 RCTs of rtpa for Acute Ischemic")
32 Recombinant Tissue Plasminogen Activator (rtpa) RCTs of rtpa for Acute Ischemic Stroke
33 NINDS Stroke Study Clinical question: In patients with ischemic stroke presenting within 3 hours of symptom onset does the administration of rtpa reduce morbidity and mortality? Multicenter, double-blinded, randomized, placebo-controlled trial N=624 Exclusion mostly based on risk of bleeding No exclusion based on severity of stroke or maximum age
34 NINDS continued Divided in 2 parts Part 1: Improvement by >4 points on NIHSS or complete resolution at 24 hours 47% vs 39% (RR 1.2; 95% CI ; p=0.21 Part 2: Proportion after stroke with favorable outcomes at 90 days Barthel Index: 50% vs 38% (OR 1.6; 95% CI , p=0.026) Modified Rankin Scale: 39% vs 26% (OR 1.7; 95% CI , p=0.019) Glasgow outcome scale: 44% vs 32% (OR 1.6; 95% CI , p=0.025) NIHSS: 31% vs 20% (OR 1.7; 95% CI ; p=0.033) 90-day Mortality: 17% vs 21% (p=0.30) Adverse Events: ICH within 36 hours of stroke treatment 6.4% vs 0.6% (p<0.001), of which 45% were fatal NNT to prevent significant disability: 8
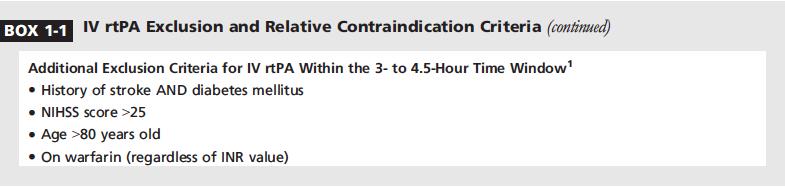
35 ECASS III Clinical question: In patients with ischemic stroke presenting up to 4.5 hours of symptom onset does the administration of rtpa reduce disability? Multicenter, double-blinded, randomized, placebocontrolled trial N=821; follow up of 3 months Exclusion mostly based on risk of bleeding Exclusion of patients > 80 yo NIHSS score > 25 Prior stroke AND diabetes Warfarin (regardless of INR)
36 ECASS III continued Primary Outcome: 90-day disability (mrs of 0 or 1) 52.4% vs 45.2% (OR 1.34; 95% CI ; p=0.04) Secondary Outcome: Global outcome Favoring rtpa: (OR 1.28; 95% CI , p<0.05) Barthel Index: 63.4% vs 58.6% (OR 1.23; 95% CI , p=0.16) Glasgow outcome scale: 51.0% vs 45.4% (OR 1.25; 95% CI , p=0.11) NIHSS: 50.2% vs 43.2% (OR 1.33; 95% CI ; p=0.04) NNT for a favorable outcome: 13.8 Adverse Events Any ICH: 27.0% vs 17.6% Symptomatic ICH: ECASS III definition: 2.4% vs 0.2% (OR 9.85; 95% CI ; p=0.008; NNH=45) NINDS definition: 7.9% vs 3.5% (OR 2.38; 95% CI ; p=0.006; NNH=23) 90-day Mortality 7.7% vs 8.4% (OR 0.80; 95% CI ; p=0.68)
 of axonal fibers. Each hour in which treatment fails to occur, the brain loses as many neuron as it does in almost 3.")
37 Time is Brain Every minute in which a large vessel ischemic stroke is untreated, the average patient loses 1.9 million neurons, 13.8 billion synapses, 12 km (7 miles) of axonal fibers. Each hour in which treatment fails to occur, the brain loses as many neuron as it does in almost 3.6 years of normal aging.
38 Time is Brain Faster Treatment=Better Outcomes The greatest population benefit would occur by treating more patients early. Lees et al. Lancet 2010

39 Time is Brain Faster Treatment=Better Outcomes Saver et al. JAMA 2013
40
41
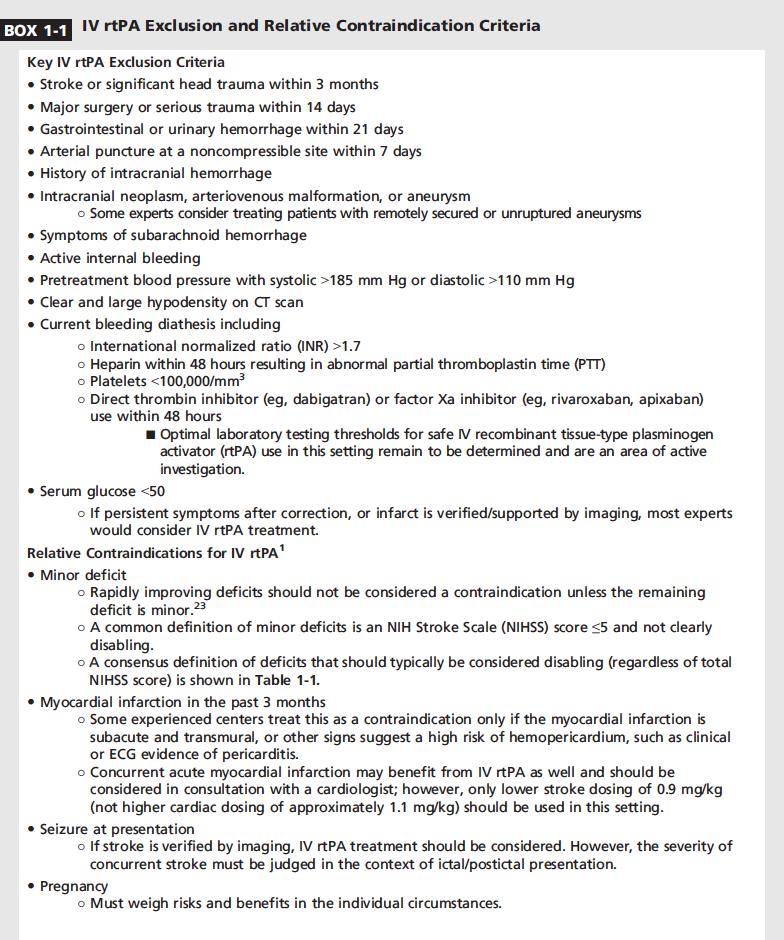
42 Criterion AHA/ASA Acute Stroke Management Guideline 2013 Old Alteplase (Activase) PI (Updated 2009) New Alteplase (Activase) PI (February 2015) Prior stroke Exclusion: prior stroke within 3 mo Contraindication: recent (within 3 mo) previous stroke Removed entirely Seizure at onset Relative exclusion: seizure at onset with postictal neurological impairments Contraindication: seizure at the onset of stroke Removed entirely Bleeding diathesis/oacs Exclusion: Platelet count < /mm3Heparin Contraindication: known bleeding diathesis including Bleeding diathesis remains a contraindication, but all laboratory values and
43 Treatment Timeline Goals IV tpa within 60 minutes of arrival to an ED Evaluation by ED physician (10 minutes) Evaluation by stroke/neurologist (15 minutes) Non-contrast CT scan is completed (25 minutes) CT is interpreted (45 minutes) Faster treatment = Better outcomes
44 Post-Reperfusion Therapy Standard post-tpa management for the first 24 hours: Admission to Stroke Unit ICU level of care NPO until dysphagia screening to avoid aspiration PNA Isotonic IV fluids (not dextrose containing because of risk of hyperglycemia) BP and neurologic monitoring Q15min x 2 hrs, then Q30min x 6 hrs, then Q60min x 16 hrs Aggressive BP treatment If SBP>180 mmhg or DBP >105 mmhg Emergent CT scan if neurologic decline, acute increase in BP, N/V, new HA Repeat brain imaging at 24 hours to assess for asymptomatic hemorrhage

45 Endovascular Therapies Five positive endovascular RCTs for treatment of acute ischemic
46
47 Endovascular Interventions Patients eligible for intravenous r-tpa should receive intravenous r-tpa even if endovascular treatments are being considered (Class I; Level of Evidence A). Patients should receive endovascular therapy with a stent retriever if they meet all the following criteria (Class I; Level of Evidence A). (New recommendation): Prestroke mrs score 0 to 1, Acute ischemic stroke receiving intravenous r-tpa within 4.5 hours of onset according to guidelines from professional medical societies, Causative occlusion of the ICA or proximal MCA (M1), Age 18 years, NIHSS score of 6, ASPECTS of 6, and Treatment can be initiated (groin puncture) within 6 hours of symptom onset In carefully selected patients with anterior circulation occlusion who have contraindications to intravenous r-tpa, endovascular therapy with stent retrievers completed within 6 hours of stroke onset is reasonable (class iia; level of evidence C). (New recommendation)
48 Imaging Emergency imaging of the brain is recommended before any specific treatment for acute stroke is initiated (Class I; Level of Evidence A). In most instances, nonenhanced CT will provide the necessary information to make decisions about emergency management. If endovascular therapy is contemplated, a noninvasive intracranial vascular study is strongly recommended during the initial imaging evaluation of the acute stroke patient but should not delay intravenous r-tpa if indicated. For patients who qualify for intravenous r-tpa according to guidelines from professional medical societies, initiating intravenous r-tpa before noninvasive vascular imaging is recommended for patients who have not had noninvasive vascular imaging as part of their initial imaging assessment for stroke. Noninvasive intracranial vascular imaging should then be obtained as quickly as possible (Class I; Level of Evidence A). (New recommendation) The benefits of additional imaging beyond CT and CTA or MRI and MRA such as CT perfusion or diffusion- and perfusion-weighted imaging for selecting patients for endovascular therapy are unknown (Class IIb; Level of Evidence C). (New recommendation)
49 Summary A leading cause of disability and death both in the US and globally Acute stroke treatment requires emergent and streamlined evaluation in a certified stroke center IV tpa is considered standard of care Endovascular treatment with mechanical thrombectomy has also become a standard of care for selected patients
50 Questions??
51 Category INSERT NIHSS Neurologic Examination: The NIH Stroke Scale (NIHSS) Scale Definition 1a. LOC 0 = Alert 1 = Not alert, arousable 2 = Not alert, obtunded 3 = Unresponsive 1b. Questions 0 = Answers both correctly 1=Answers one correctly 2=Answers neither correctly 1c. Commands 0=Performs both tasks correctly 1=Performs one task correctly 2=Performs neither task 2. Gaze 0=Normal 1=Partial gaze palsy 2=Total gaze palsy 3. Visual fields 0=No visual loss 1=Partial gaze palsy 2=Total gaze palsy 4. Facial Palsy 0=Normal 1=Minor paralysis 2=Partial paralysis
 previous stroke Removed entirely Seizure at onset Relative exclusion: seizure at onset with postictal neurological impairments Contraindication: seizure at the")
52 Criterion AHA/ASA Acute Stroke Management Guideline 2013 Old Alteplase (Activase) PI (Updated 2009) New Alteplase (Activase) PI (February 2015) Prior stroke Exclusion: prior stroke within 3 mo Contraindication: recent (within 3 mo) previous stroke Removed entirely Seizure at onset Relative exclusion: seizure at onset with postictal neurological impairments Contraindication: seizure at the onset of stroke Removed entirely
53 Criterion AHA/ASA Acute Stroke Management Guideline 2013 Old Alteplase (Activase) PI (Updated 2009) New Alteplase (Activase) PI (February 2015) Bleeding diathesis/oacs Exclusion: Platelet count < /mm3Heparin received within 48 h, resulting in abnormally elevated apttcurrent use of anticoagulant with INR >1.7 or PT >15 scurrent use of direct thrombin inhibitors or direct factor Xa inhibitors with elevated sensitive laboratory tests Contraindication: known bleeding diathesis including but not limited to:current use of OACs (eg, warfarin sodium), an INR >I.7, or a PT >15 sadministration of heparin within 48 h preceding the onset of stroke with an elevated aptt at presentationplatel et count < /mm3Warning for all indications: patients currently taking OACs Bleeding diathesis remains a contraindication, but all laboratory values and specific examples removed
54 Criterion AHA/ASA Acute Stroke Management Guideline 2013 Old Alteplase (Activase) PI (Updated 2009) New Alteplase (Activase) PI (February 2015) ICH Exclusion: history of previous ICH Contraindication: history of ICH Contraindication removed Warning added for recent ICH BP Exclusion: Elevated BP (systolic >85 mm Hg or diastolic >10 mm Hg) Contraindication: uncontrolled hypertension at the time of treatment (eg, >185 mm Hg systolic or >110 mm Hg diastolic) Contraindication: current severe uncontrolled hypertension remains, specific BP values removed Warning for BP >175/110 mm Hg remains for all alteplase indications
55 Criterion AHA/ASA Acute Stroke Management Guideline 2013 Old Alteplase (Activase) PI (Updated 2009) New Alteplase (Activase) PI (February 2015) Blood glucose Exclusion: blood glucose <50 mg/dl Warning: because of the increased risk for misdiagnosis of acute ischemic stroke, special diligence is required in making this diagnosis in patients whose blood glucose values are 50 or >400 mg/dl Removed entirely
56 Criterion AHA/ASA Acute Stroke Management Guideline 2013 Old Alteplase (Activase) PI (Updated 2009) Severe stroke Not listed Warning: patients with severe neurological deficit (NIHSS score >22) at presentation; there is an increased risk of ICH in these patients New Alteplase (Activase) PI (February 2015) Removed entirely
57 Criterion AHA/ASA Acute Stroke Management Guideline 2013 Old Alteplase (Activase) PI (Updated 2009) New Alteplase (Activase) PI (February 2015) Mild stroke Relative exclusion: only minor or rapidly improving stroke symptoms (clearing spontaneously) Warning: safety and efficacy in patients with minor neurological deficit or with rapidly improving symptoms have not been evaluated; therefore, treatment of patients with minor neurological deficit or with rapidly improving symptoms is not recommended Warning: safety and efficacy in patients with minor neurological deficit or with rapidly improving symptoms have not been evaluated; therefore, treatment of patients with minor neurological deficit or with rapidly improving symptoms is not recommended
58 Criterion AHA/ASA Acute Stroke Management Guideline 2013 Old Alteplase (Activase) PI (Updated 2009) New Alteplase (Activase) PI (February 2015) Neuroimaging findings Exclusion: CT demonstrates multilobar infarction (hypodensity >1/3 cerebral hemisphere) Warning: Major early infarct sign (substantial edema, mass effect, or midline shift on CT) Removed entirely SAH Exclusion: symptoms suggest SAH Contraindication: Suspicion of SAH on pretreatment evaluation Contraindication: subarachnoid hemorrhage
59 Criterion AHA/ASA Acute Stroke Management Guideline 2013 Old Alteplase (Activase) PI (Updated 2009) Use in specific populations Pregnancy Relative exclusion Warning: pregnancy Category C New Alteplase (Activase) PI (February 2015) No change Nursing mothers Not listed Not mentioned Unknown risk Children Inclusion: 18 y of age Indicated for adults Elderly Not listed Warning for all indications: advanced age (eg, >75 y) may increase risks Gastrointestinal or genitourinary bleeding Warning: gastrointestinal or genitourinary bleeding within the past 21 d Warning: gastrointestinal or genitourinary bleeding within the past 21 d Pediatric use not established Warning added: age >77 y was 1 of several interrelated baseline characteristics associated with an increased risk of ICH; efficacy results suggest a reduced but still favorable clinical outcome Warning: gastrointestinal or genitourinary bleeding
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
ENDOVASCULAR THERAPIES FOR ACUTE STROKE
 ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Pathophysiology of stroke
 A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke
 and Small Vessel Occlusion (SVO) in Stroke") Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Stroke in the Emergency Room: What do we need to know?
 Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Code Stroke in real life. Disclosures. Parkland Memorial Hospital. I have no disclosures. Has 1 million patient visits annually. Level 1 Trauma Center
 Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Acute Stroke Care: the Nuts and Bolts of it. ECASS I and II ATLANTIS. Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center
 Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Disclosure. + Outline. What is a stroke? Role of imaging in stroke Ischemic stroke Venous infarct Current topics
 + Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 + Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Thank you
+ Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 + Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Thank you
Carotid Embolectomy and Endarterectomy for Symptomatic Complete Occlusion of the Carotid Artery as a Rescue Therapy in Acute Ischemic Stroke
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Updated tpa Guidelines: Expanding the opportunity for good outcomes. Benjamin Morrow, MSN RN UPMC Stroke Institute
 Updated tpa Guidelines: Expanding the opportunity for good outcomes Benjamin Morrow, MSN RN UPMC Stroke Institute 1 Outline History Current State Review Exclusions: Minor stroke symptoms Severe strokes
Updated tpa Guidelines: Expanding the opportunity for good outcomes Benjamin Morrow, MSN RN UPMC Stroke Institute 1 Outline History Current State Review Exclusions: Minor stroke symptoms Severe strokes
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Page 1 of 7. Intraparenchymal hemorrhage or subarachnoid hemorrhage. Consult neurosurgery
 Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Brain Attacks and Acute Stroke Management
 Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Standard NICE (CG ) RCP (2016)
 RCP (2016)") Standard NICE (CG68 2008) RCP (2016) Stroke Unit Adults presenting at an A&E department with suspected stroke are admitted to a specialist stroke unit within 4 hours direct admission of patients with acute
Standard NICE (CG68 2008) RCP (2016) Stroke Unit Adults presenting at an A&E department with suspected stroke are admitted to a specialist stroke unit within 4 hours direct admission of patients with acute
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
AGWS Stroke Thrombolysis Clinical Profoma
 AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center
 Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Parameter Optimized Treatment for Acute Ischemic Stroke
 Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Background. Recommendations for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association
 for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association An Scientific Statement from the Stroke Council, American Heart Association and American Stroke Association
for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association An Scientific Statement from the Stroke Council, American Heart Association and American Stroke Association
Thrombolysis Assessment
 Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
Disclosures. Anesthesia for Endovascular Treatment of Acute Ischemic Stroke. Acute Ischemic Stroke. Acute Stroke = Medical Emergency!
 Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
RBWH ICU Journal Club February 2018 Adam Simpson
 RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1,
 I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
IDPH EMS Region Five. Stroke Education
 IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical