Anesthetic Management of a Patient with Traumatic Brain Injury
|
|
|
- Vernon Wells
- 6 years ago
- Views:
Transcription

1 Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S Hershey Medical Center Penn State University College of Medicine
2 The Following Slides, Questions and Recommendations are based on the Guidelines for the Management of Severe Traumatic Brain Injury 3 rd Edition Brain Trauma Foundation American Association of Neurological Surgeons AANS Congress of Neurological Surgeons CNS AANS/CNS Joint Section on Neurotrauma and Critical Care Journal of Neurotrauma Volume 24, Supplement 1, 2007 Permission for reproduction of all images and graphs in this presentation has been received.
3 Brain Trauma Foundation (BTF) Recommendations: BTF levels of Recommendations (I, II, III) are derived from Class of Evidence (I, II, III). Recommendations: Level I: high degree of clinical certainty Level II: moderate degree of clinical certainty Level III: degree clinical certainty not established
4 A Case of TBI History and Physical The patient sustained a closed head injury in a motorcycle accident one hour ago. He is booked for an emergency craniotomy. PMHx: Family history: Physical exam: Labs: X-Ray: NPO: Illnesses: previously healthy Surgeries: none Meds: none Habits: smokes with a 10 packyear history, drinks alcohol regularly Allergies: none No anesthetic complications Thin male, lethargic and somewhat combative, vomiting Wt : 75 Kg HR : 52 BP : 196/102 RR : 20 Airway: Receding mandible, severe overbite Lungs: clear to ausculation Heart: sinus bradycardia, hypertension Neuro: does not open his eyes to noise or pain, Pupils right 5/4, left 3/2, moans and groans, withdraws right arm and leg to painful stimuli, does not move left arm or leg. Normal Cervical fractures ruled out Consumed large burger and fries, and 6 beers one hour prior to injury.

5 CT Scan of our patient Principles of Neurological Surgery, 3 th Ed., online
6 Based on this patients exam, his intracranial pressure is likely to be? 1. High 2. Normal 3. Low
7 Sorry I disagree Try again
8 CORRECT!! Next slide
9 Symptoms of increased ICP Headache Nausea and Vomiting Pupillary changes Depressed Level of Consciousness Irregular Breathing Hypertension Cushing s Triad Bradycardia
10 What is the threshold to treat ICP? mmhg mmhg mmhg mmhg
11 Sorry I disagree Try again
12 CORRECT!! Next slide
13 Treatment of increased ICP increased ICP is defined as >15 mmhg Symptoms occur at mmhg ICP Herniation can occur at mmhg ICP Symptoms are dependent on CBF and CPP BTF: Level II Current data support mmhg as an upper threshold above which treatment to lower ICP should generally be initiated
14 Our patient has an increased ICP of 30 mmhg. What would be the lowest MAP that you could tolerate? mmhg mmhg mmhg mmhg mmhg
15 Sorry I disagree Try again
16 CORRECT!! Next slide
17 CPP Threshold for treatment Lower CPP limit: mmhg CPP = MAP ICP or CPP = MAP CVP (take the higher of ICP or CVP) CPP of 50 mmhg is considered the ischemic threshold for most patients and lower levels should be avoided BTF: Level III CPP of < 50 mmhg should be avoided
18 Autoregulation: CPP and CBF Cottrell and Young s neuroanesthesia, 5 th Ed., online Cerebral blood flow (CBF) autoregulation: For a cerebral perfusion pressure (CPP) value between 50 and 150 mm Hg, global CBF is maintained at 50mL/100g/min

19 What would be the maximum CPP you should aim for in our patient? mmhg mmhg mmhg mmhg mmhg
20 Sorry I disagree Try again
21 CORRECT!! Next slide
22 CPP Threshold Upper CPP limit: 70 mmhg CPP = MAP ICP or CVP (use the greater of ICP or CVP) BTF: Level II Aggressive attempts to maintain CPP above 70 mmhg with fluids and vasopressors should be avoided because of a higher risk to develop ARDS
23 What is the critical lower threshold for CBF? ml/100g/min ml/100g/min ml/100g/min ml/100g/min ml/100g/min
24 Sorry I disagree Try again
25 CORRECT!! Next slide
26 Regional Cerebral Blood Flow (rcbf) Edema Reversible injury Infarction ml/100g/min Overall cerebral blood of 50 ml/100mg/min is usually maintained for a CPP between mmhg ml/100mg/min = critical rcbf 15 ml/100mg/min = iso-electric EEG 10 ml/100mg/min = metabolic failure Penumbra (15-20ml/100mg/min): Semi-stable cells that can be saved for a full recovery with appropriate treatment, including optimal anesthetic management
27 What is the patient s GCS? < 8
28 Sorry I disagree Try again
29 CORRECT!! Next slide
30 GCS Glasgow Coma Scale Eye Opening None To Pain To Speech Spontaneous Motor Response None Extension Flexor Response Withdrawal Localizes Pain Obeys Commands Verbal Response None Incomprehensible Inappropriate Disoriented Oriented 1 = Even to supra-orbital pressure 2 = Pain from sternum/limb/supra-orbital pressure 3 = Non-specific response, not necessarily to command 4 = Eyes open, not necessarily aware 1 = To any pain; limbs remain flaccid 2 = Shoulder adducted and shoulder and forearm internally rotated 3 = Withdrawal response or assumption of hemiplegic posture 4 = Arm withdraws to pain, shoulder abducts/flexion 5 = Arm attempts to remove supra-orbital/chest pressure 6 = Follows simple commands 1 = No verbalization of any type 2 = Moans/groans, no speech 3 = Intelligible, no sustained sentences 4 = Converses but confused, disoriented 5 = Converses and oriented
31 Clinical Signs and GCS Glasgow coma scale is helpful to summarize clinical signs in patients with increased ICP. GCS is a useful measure for the severity of TBI. Severe TBI: GCS < 8 Moderate TBI: GCS 9-12 Minor TBI: GCS 13-15
32 Given our patients H+P, what is the likely side of the subdural hematoma? 1. Right side 2. Left side
33 Sorry I disagree Try again
34 CORRECT!! Next slide
35 TBI History and Physical The patient sustained a closed head injury in a motorcycle accident one hour ago. PMHx: Family history: Physical exam: Labs: X-Ray: NPO: Illnesses: previously healthy Surgeries: none Meds: none Habits: smokes with a 10 packyear history, drinks alcohol regularly Allergies: none No anesthetic complications Thin male, lethargic and somewhat combative, vomiting Wt : 75 Kg HR : 52 BP : 196/102 RR : 20 Airway: Receding mandible, severe overbite Lungs: clear to ausculation Heart: sinus bradycardia, hypertension Neuro: does not open his eyes to noise or pain, Pupils right 5/4, left 3/2, moans and groans, withdraws right arm and leg to painful stimuli, does not move left arm or leg. Normal Cervical fractures ruled out Consumed large burger and fries, and 6 beers one hour prior to injury.
36 CT Scan of our patient Principles of Neurological Surgery, 3 th Ed., online right sided subdural hematoma with midline shift and compression of left lateral ventricle
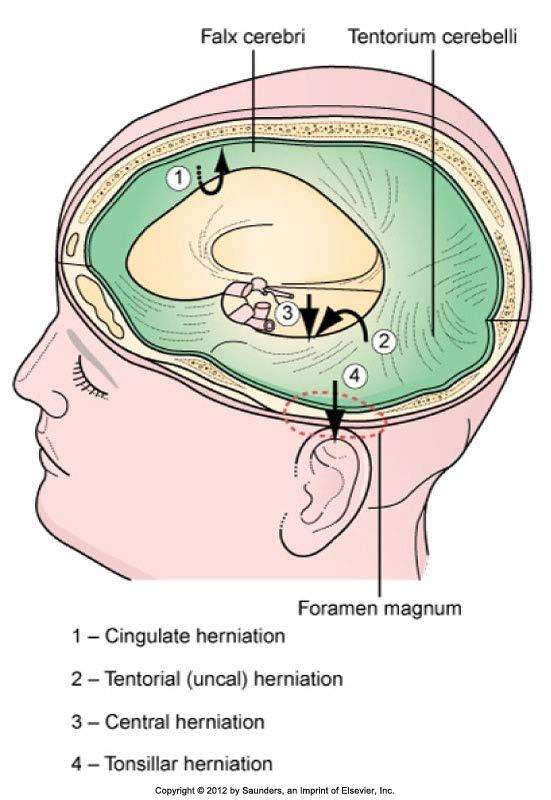
37 Herniation Sites
38 Herniation Symptoms Eye abnormalities Autonomic dysfunction Motor dysfunction Other (nausea, vomiting, level of consciousness )
39 Symptoms of Subfalcine Herniation Trapping of one or both anterior cerebral arteries, causing infarction of the paramedian cortex Leg paralysis Expansion of infarcted area Edema Increased intracranial pressure Increased risk of transtentorial herniation central herniation or both
40 Symptoms of Transtentorial Herniation Compression of ipsilateral 3rd cranial nerve Unilateral dilated, fixed pupil Oculomotor paresis Compression of the posterior cerebral artery Contralateral homonymous hemianopia Absence of blinking reflex Compression of the contralateral 3rd cranial nerve and cerebral peduncle Contralateral dilated pupil and oculomotor paresis Ipsiateral hemiparesis Compression of the ipsilateral cerebral peduncle Contralateral hemiparesis Compression of the upper brain stem and the area in and around the thalamus Impaired consciousness Abnormal breathing patterns Fixed, unequal pupils Further compromise of the brain stem Loss of oculocephalic reflex Loss of oculovestibular reflex Loss of corneal reflexes Decerebrate posturing
41 Symptoms of Central Herniation Both temporal lobes herniate because of bilateral mass effects or diffuse brain edema. Bilateral damage to the midbrain Pupils fixed in midposition Decerebrate posturing Same symptoms as transtentorial herniation Further compromise of the brain stem Loss of all brain stem reflexes Disappearance of decerebrate posturing Cessation of respirations Brain death
42 Symptoms Tonsillar Herniation Compression of the brain stem Obstruction of CSF flow Acute hydrocephalus Impaired consciousness Headache Vomiting Meningismus Dysconjugate eye movements Respiratory and cardiac arrest
43 A linear relationship between CBF exists for? 1. PaCO2 2. ICP 3. PaO2 4. CPP
44 Sorry I disagree Try again
45 CORRECT!! Next slide

46 CBF, Pressures and Blood Gases Modified from: Cottrell and Young s neuroanesthesia, 5 th Ed., online There is a linear relationship between PaCO2 and CBF for PaCO2 values between 20 and 80 mmhg
47 Level II or III recommendations for this patient include all of the following, except? 1. Avoid Hypoxia with SpO2 < 90% 2. Provide prophylactic Hyperventilation to 25 mmhg 3. Avoid Hypotension with SBP < 90 mmhg 4. Avoid Hypoxia with PaO2 < 60 mmhg
48 Sorry I disagree Try again
49 CORRECT!! Next slide
50 Blood Pressure and Oxygenation Avoid BOTH: HYPOTENSION and HYPOXIA Hypotension: avoid BP < 90 mmhg BTF: Level II Blood pressure should be monitored and hypotension (SPB < 90 mmhg) avoided Hypoxia: avoid SpO2 < 90%, pao2 < 60 mmhg BTF: Level III Oxygenation should be monitored and hypoxia (pao2 < 60 mmhg or O2 Sat. < 90 %) avoided

51 Treat Hypotension then ICP!! CBF is more affected by decrease in ABP than by increase in ICP. For the same CPP of 40 mmhg, an increase in ICP lead to a CBF of 90%, whereas hypotension decreased CBF to 60%.
52 What would be the least desirable iv fluid to restore hypovolemia in this patient? 1. Normal Saline 2. Lactated Ringers 3. PRBC with symptomatic anemia 4. Balanced E lyte solution (Plasmalyte)
53 Sorry I disagree Try again
54 CORRECT!! Next slide
55 i.v. fluids First choice: Normal Saline NS (308 mosmol/l) Balanced electrolyte solutions - Plasmalyte (312 mosmol/l) AVOID the following hypotonic solutions, that can increase ICP by increasing cerebral edema Hypotonic solutions Glucose containing solutions High Glc. is associated with bad outcome Glc. is metabolized, free water remains, hypotonic sloution is the result. Avoid Lactated Ringers (275 mosml/l, slightly hypotonic) Albumin is associated with increased mortality in TBI HES still under debate (FDA black box warning for increased mortality and severe renal injury, and additional warning on risk of bleeding)
56 Should this patient be hyperventilated? 1. Always until ICP normalizes 2. As needed for a brief period 3. Never
57 Sorry I disagree Try again
58 CORRECT!! Next slide

59 Hyperventilation and Rebound effect Return to baseline Rebound increase in CBF and ICP after discontinuation of Hyperventilation. Hyperventilation should only be a temporary measure to avoid herniation. Miller s Anesthesia, 7th edition, online Paco2, cerebral blood flow (CBF), and cerebrospinal fluid (CSF) ph changes with prolonged hyperventilation. Although the decreased arterial Paco2 (and the systemic alkalosis) persist for the duration of hyperventilation, the ph of the brain and CBF return toward normal over 8 to 12 hours.
60 Summary Avoid secondary injury Recognize signs and symptoms of increased ICP / brain herniation Glasgow Coma Scale useful in grading of severity of TBI Maintain Normotension Maintain Normovolemia (avoid hypoosmotic solutions) Maintain Oxygenation Avoid Hypercarbia but hyperventilate only as a temporary measure Hypotension and Hypoxemia associated with worse outcomes
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Neurocritical Care Basics. Tapan Kavi, MD Christina Fox, RN
 Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
CNS pathology Third year medical students,2019. Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
10/6/2017. Notice. Traumatic Brain Injury & Head Trauma
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
PEDIATRIC BRAIN CARE
 PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Patho-physiology of nervous System Talk 2 Syndromes in neurosciences. Petr Maršálek Dept pathological physiology 1.Med. F. CUNI
 Patho-physiology of nervous System Talk 2 Syndromes in neurosciences Petr Maršálek Dept pathological physiology 1.Med. F. CUNI Talks on NS Talk 1 - Pain and Motor disorders Talk 2 - This - Syndromes in
Patho-physiology of nervous System Talk 2 Syndromes in neurosciences Petr Maršálek Dept pathological physiology 1.Med. F. CUNI Talks on NS Talk 1 - Pain and Motor disorders Talk 2 - This - Syndromes in
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
BRAIN HERNIATION S54 (1) Brain Herniation
 Brain Herniation") BRAIN HERNIATION S54 (1) Brain Herniation Last updated: September 5, 2017 PATHOPHYSIOLOGY... 1 TYPES OF HERNIATION... 2 SUPRATENTORIAL MASSES... 2 Central (s. downward transtentorial) herniation... 2 Uncal
BRAIN HERNIATION S54 (1) Brain Herniation Last updated: September 5, 2017 PATHOPHYSIOLOGY... 1 TYPES OF HERNIATION... 2 SUPRATENTORIAL MASSES... 2 Central (s. downward transtentorial) herniation... 2 Uncal
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Evaluation & Management of Elevated Intracranial Pressure in Adults. Dr. Tawfiq Almezeiny
 Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Head Trauma Protocol
 Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
D is for Disability Altered Mental Status in Children
 D is for Disability Altered Mental Status in Children Joshua Ross, MD, FAAP Pediatric Emergency Medicine Emergency Care and Trauma Symposium June 22, 2015 Objectives Describe a basic approach to evaluating
D is for Disability Altered Mental Status in Children Joshua Ross, MD, FAAP Pediatric Emergency Medicine Emergency Care and Trauma Symposium June 22, 2015 Objectives Describe a basic approach to evaluating
PACT module. Traumatic Brain Injury. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
CHILD IN NON - TRAUMATIC COMA
 May / 2018 PELC / SLCP 1 CHILD IN NON - TRAUMATIC COMA PELS May / 2018 PELC / SLCP 2 Objectives Recognize depressed mental status Know the causes of depressed mental status in children Assessment and workup
May / 2018 PELC / SLCP 1 CHILD IN NON - TRAUMATIC COMA PELS May / 2018 PELC / SLCP 2 Objectives Recognize depressed mental status Know the causes of depressed mental status in children Assessment and workup
Head & Brain Trauma. Presented By: Steven Jones, NREMT-P
 Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
COMA & INTENSIVE CARE
 COMA & INTENSIVE CARE Jozef Firment, MD. PhD., Judita Capkova, MD. PhD. Department of Anaesthesiology & Intensive Care Medicine Šafárik University Faculty of Medicine, Košice Coma Is a state of unarousable
COMA & INTENSIVE CARE Jozef Firment, MD. PhD., Judita Capkova, MD. PhD. Department of Anaesthesiology & Intensive Care Medicine Šafárik University Faculty of Medicine, Košice Coma Is a state of unarousable
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Mild Traumatic Brain Injury
 Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Brain Death Determination: Outline. Definition. Brain Death Determination. Brain Death Determination. No conflict of interest
 No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency
 Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency Traumatic Brain Injury Causes Pathophysiology Neurologic assessment Therapeutic Approach Status
Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency Traumatic Brain Injury Causes Pathophysiology Neurologic assessment Therapeutic Approach Status
Conflict of Interest Disclosure J. Claude Hemphill III, MD,MAS. Difficult Diagnosis and Treatment: New Onset Obtundation
 Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
Experiences as a Donation Support Physician. Dead or not Dead? Are the following statements consistent with neurological
 Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
DRAFT: Cendoma, M. Sideline Identification of Intracranial Hematoma
 1. Orlando Regional Healthcare, Education and Development. Orlando Regional Health Care. [Online] 2004. [Cited: April 27, 2012.] http://www.orlandoregional.org/pdf%20folder/overview%20adult%20brain%20injury.pd
1. Orlando Regional Healthcare, Education and Development. Orlando Regional Health Care. [Online] 2004. [Cited: April 27, 2012.] http://www.orlandoregional.org/pdf%20folder/overview%20adult%20brain%20injury.pd
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Characteristic features of CNS pathology. By: Shifaa AlQa qa
 Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Assessment and Scoring Tools
 Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Neurological Determination of Death Adult
 Approved by: Vice President and Chief Medical Officer Neurological Determination of Death Adult Corporate Policy & Procedures Manual Number: VII-B-400 Date Approved June 9, 2015 Next Review (3 years from
Approved by: Vice President and Chief Medical Officer Neurological Determination of Death Adult Corporate Policy & Procedures Manual Number: VII-B-400 Date Approved June 9, 2015 Next Review (3 years from
Traumatic Brain Injury (1.2.3) Management of severe TBI ( ) Learning Objectives
 Management of severe TBI ( ) Learning Objectives") Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio
 Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Chapter 31. Objectives. Objectives 01/09/2013. Head Trauma
 Chapter 31 Head Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Chapter 31 Head Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Paediatric Neurosurgical Emergencies. Kate Parkins Consultant Paediatric Intensivist Alder Hey
 Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
It s All in Your Head: Neuro Assessment for Non- Neuro Folks
 It s All in Your Head: Neuro Assessment for Non- Neuro Folks Causes for Neuro Changes Stroke Head Injury Tumors Increased ICP Drugs Anoxia Altered Blood Glucose Toxins Alcohol Meningitis Poor Circulation
It s All in Your Head: Neuro Assessment for Non- Neuro Folks Causes for Neuro Changes Stroke Head Injury Tumors Increased ICP Drugs Anoxia Altered Blood Glucose Toxins Alcohol Meningitis Poor Circulation
COMA. DIAH MUSTIKA HW,SpS,KIC INTENSIVE CARE UNIT of EMERGENCY DEPARTMENT
 COMA DIAH MUSTIKA HW,SpS,KIC INTENSIVE CARE UNIT of EMERGENCY DEPARTMENT NAVAL HOSPITAL dr RAMELAN, SURABAYA DEFINITIONS Coma State of unresponsiveness to external or internal stimuli in which a patient
COMA DIAH MUSTIKA HW,SpS,KIC INTENSIVE CARE UNIT of EMERGENCY DEPARTMENT NAVAL HOSPITAL dr RAMELAN, SURABAYA DEFINITIONS Coma State of unresponsiveness to external or internal stimuli in which a patient
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
BATLS Battlefield Advanced Trauma Life Support
 J R Army Med Corps 2002; 148: 151-158 BATLS Battlefield Advanced Trauma Life Support CHAPTER 8 HEAD INJURIES Aim 0801. On successfully completing this topic you will be able to: Discuss general management
J R Army Med Corps 2002; 148: 151-158 BATLS Battlefield Advanced Trauma Life Support CHAPTER 8 HEAD INJURIES Aim 0801. On successfully completing this topic you will be able to: Discuss general management
Supplementary Online Content
 Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and
 1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
A GLANCE ON NEUROLOGICAL EMERGENCIES. Baystate Medical Center
 A GLANCE ON NEUROLOGICAL EMERGENCIES Baystate Medical Center Anthony Shamoun, MSN, RN, ACNP-BC, CCNS Clinical Nurse Specialist/Nurse Educator anthony.shamoun@bhs.org Outline I. Neurological Examination
A GLANCE ON NEUROLOGICAL EMERGENCIES Baystate Medical Center Anthony Shamoun, MSN, RN, ACNP-BC, CCNS Clinical Nurse Specialist/Nurse Educator anthony.shamoun@bhs.org Outline I. Neurological Examination
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Blood Brain Barrier (BBB)
") Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Neurosurgery Review. Mudit Sharma, MD May 16 th, 2008
 Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
VISUAL REFLEXES. B. The oculomotor nucleus, Edinger-Westphal nucleus, and oculomotor nerve at level of the superior colliculus.
 Neuroanatomy Suzanne Stensaas February 24, 2011, 10:00-12:00 p.m. Reading: Waxman Ch. 15 HyperBrain: Ch 7 with quizzes and or Lab 7 videotape http://www-medlib.med.utah.edu/kw/hyperbrain/anim/reflex.html
Neuroanatomy Suzanne Stensaas February 24, 2011, 10:00-12:00 p.m. Reading: Waxman Ch. 15 HyperBrain: Ch 7 with quizzes and or Lab 7 videotape http://www-medlib.med.utah.edu/kw/hyperbrain/anim/reflex.html
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Instructional Course #34. Review of Neuropharmacology in Pediatric Brain Injury. John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD
 Instructional Course #34 Review of Neuropharmacology in Pediatric Brain Injury John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD Outline of Course 1. Introduction John Pelegano MD 2. Neuropharmocologic
Instructional Course #34 Review of Neuropharmacology in Pediatric Brain Injury John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD Outline of Course 1. Introduction John Pelegano MD 2. Neuropharmocologic
CEREBROVASCULAR ACCIDENT (CVA)
") Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP5-002 Approval Date: 12/01/2017 Effective Date: 12/01/2017 Revision Due Date: 12/01/2018 CEREBROVASCULAR ACCIDENT (CVA) PURPOSE
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP5-002 Approval Date: 12/01/2017 Effective Date: 12/01/2017 Revision Due Date: 12/01/2018 CEREBROVASCULAR ACCIDENT (CVA) PURPOSE
Mechanical Ventilation
 Mechanical Ventilation Effects of Mechanical Ventilation Cardiovascular Effects PPV Q T HR 1. intrathoracic pressure 2. card. tamponade effect 3. loss of +/- press chg in lungs w/spont breathing normal
Mechanical Ventilation Effects of Mechanical Ventilation Cardiovascular Effects PPV Q T HR 1. intrathoracic pressure 2. card. tamponade effect 3. loss of +/- press chg in lungs w/spont breathing normal
Proceedings of the Southern European Veterinary Conference - SEVC -
 www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 29-Oct. 2, 2011, Barcelona, Spain Next SEVC Conference: Oct. 18-21, 2012 - Barcelona, Spain Reprinted in the IVIS website
www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 29-Oct. 2, 2011, Barcelona, Spain Next SEVC Conference: Oct. 18-21, 2012 - Barcelona, Spain Reprinted in the IVIS website
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8:
 Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Deceased donor. Solid organ transplantation
 Deceased donor Solid organ transplantation Deceased donor donation process 1. Potential donor detection 2. Brain death diagnosis 3. Donor management 4. Organ allocation 5. Organ retrieval Brain death Irreversible
Deceased donor Solid organ transplantation Deceased donor donation process 1. Potential donor detection 2. Brain death diagnosis 3. Donor management 4. Organ allocation 5. Organ retrieval Brain death Irreversible
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Stephanie Banfield. 1. Frontal Lobe Controls: Behaviour Emotions Organisation Personality Planning Problem solving Arteries: ACA, MCA. 5.
 1. Frontal Lobe Controls: Behaviour Emotions Organisation Personality Planning Problem solving Arteries: ACA, MCA 2. Parietal Lobe Controls: Judgement of shape,size,texture, and weight The sensation of
1. Frontal Lobe Controls: Behaviour Emotions Organisation Personality Planning Problem solving Arteries: ACA, MCA 2. Parietal Lobe Controls: Judgement of shape,size,texture, and weight The sensation of
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia
 Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia Reza Gorji, MD University Hospital September 2007 Topics Covered Today Intracranial Pressure Intracranial
Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia Reza Gorji, MD University Hospital September 2007 Topics Covered Today Intracranial Pressure Intracranial
BASIC CONCEPT ON PEDIATRIC NEUROANESTHESIA INASNACC
 BASIC CONCEPT ON PEDIATRIC NEUROANESTHESIA INASNACC Newborn period is the first 24 hours of life. Neonatal period is the first 30 days of life and includes the newborn period. Infant is less than 1 year
BASIC CONCEPT ON PEDIATRIC NEUROANESTHESIA INASNACC Newborn period is the first 24 hours of life. Neonatal period is the first 30 days of life and includes the newborn period. Infant is less than 1 year