Fundamental Clinical Brain MR Imaging Applications and Protocols
|
|
|
- Janis Glenn
- 6 years ago
- Views:
Transcription
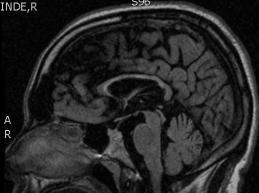
1 Continuing Education Seminar for Radiologic Technologists Fundamental Clinical Brain MR Imaging Applications and Protocols Darren P. O Neill, MD Indiana University Neuroradiology Objectives Review fundamental clinical cases that illustrate the wide array and utility of available brain MR imaging techniques / applications Gain insight into the rationale behind MR imaging protocols Develop a greater understanding of potential points of patient care impact Outline Review fundamental clinical cases that illustrate the wide array and utility of available brain MR imaging techniques: Gradient echo Diffusion FLAIR IR-SPGR / MP-RAGE MRA / MRV Spectroscopy Perfusion Review potential points of patient care impact: Additional patient history? Are the referring physician and/or neuroradiologist aware of the findings? Would an additional study(s) or different protocol be better? Would intravenous contrast be helpful? Brain Screen Indications Screen, Altered mental status, Dementia, Psychiatric disorder, Headaches Sequences 3 PL LOC Sag T1 SE Sag T2 FLAIR Ax T2 FLAIR Ax T1 SE Ax T2 TSE FS Ax DWI EPI Cor T2 TSE Comments Axial scans should be parallel to the AC-PC line 25 year-old pregnant female with mental status change Do we know more than mental status change? Onset of symptoms? Hypertension? Pregnancy? Steroids? Sequences to consider anticipating? MRI brain without contrast => evaluate for acute ischemia Avoid contrast with pregnancy! 1

 and bilateral cerebellar hemispheres Small amount of diffusion")
 Associated with a multitude of diverse")





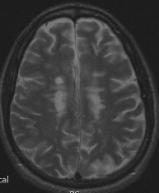
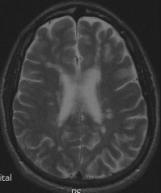
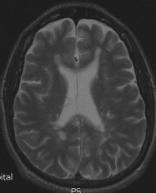
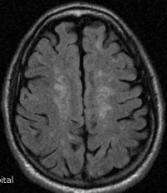
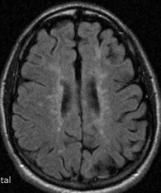
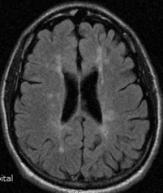
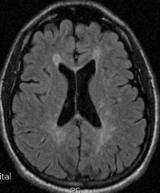
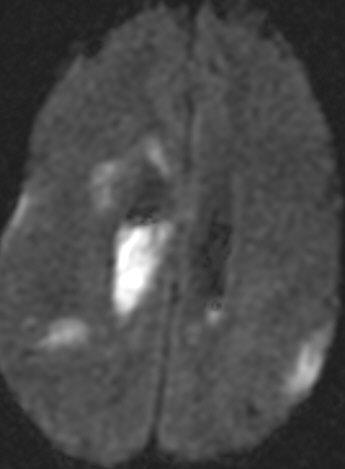
2 CT Head: Posterior > anterior cerebral hemispheric white matter hypodensity Bilateral cerebellar hypodensity MRI Brain: Abnormal T2 / FLAIR hyperintense signal within bilateral cerebral hemispheric white mater (parietooccipital > frontal) and bilateral cerebellar hemispheres Small amount of diffusion restriction within right cerebellar hemisphere Posterior Reversible Encephalopathy Syndrome (PRES) Associated with a multitude of diverse clinical entities: acute glomerulonephritis, preeclampsia / eclampsia, SLE, thrombotic thrombocytopenic purpura, and hemolytic-uremic syndrome, as well as drug toxicity (e.g. cyclosporine, tacrolimus, cisplatin, and erythropoietin) Most cases manifest with acute to subacute hypertension, and seizures are also frequent Two pathophysiologic mechanisms: Cerebral vasospasm and resulting ischemia within the involved territories Breakdown in cerebrovascular autoregulation with ensuing interstitial extravasation of fluid Diffusion MR imaging - used to discriminate Cytotoxic edema of cerebral ischemia demonstrates decreased water mobility Vasogenic edema due to cerebrovascular autoregulatory dysfunction results in increased water mobility Middle-aged female with new onset parasthesias 2


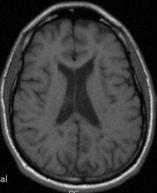

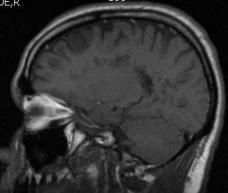


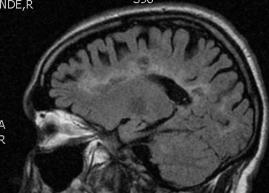
3 Axial T1 Do we know more than parasthesias? Onset of symptoms? Prior history? Neurologic deficits? Sequences to consider anticipating? Sagittal FLAIR imaging (eg. multiple sclerosis) Post-contrast images Axial T2 Axial FLAIR Sagittal T1 Sagittal FLAIR 3

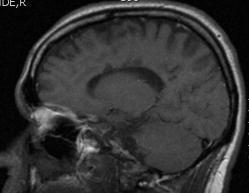
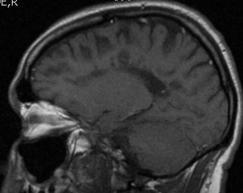
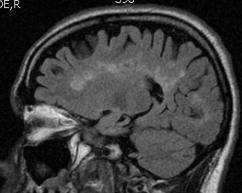
 that is generally considered to be autoimmune in nature White matter tracts")


4 Multiple Sclerosis MRI Brain: Hyperintense FLAIR signal scattered throughout the frontal-parietal white matter Involves corpus callosum, immediate pericallosal white matter, and callosal-septal junction on the sagittal FLAIR sequence Inflammatory demyelinating condition of the central nervous system (CNS) that is generally considered to be autoimmune in nature White matter tracts are affected, including those of the cerebral hemispheres, infratentorium, and spinal cord Clinical diagnosis supported by radiologic findings 3 month-old male with obtundation Do we know more than obtundation? Onset of symptoms? History of cardiopulmonary arrest? Are the referring physician and/or neuroradiologist aware? Other studies to consider anticipating? MRI => confirm suspected acute ischemia 4


 anoxia (hypoxic-ischemic injury) - not enough blood flow most common localized (such as")
 Headache Do we know more than headache? Onset of symptoms? Recent trauma? Neurologic deficits?")
5 Diffuse reversal of gray/white matter densities Decreased density of cerebral cortical gray matter Relatively increased density of thalami, brainstem, and cerebellum Relatively decompressed ventricles, with diffuse loss of sulcation and effaced suprasellar cistern Indicative of diffuse cerebral edema and early transtentorial herniation Diffuse hypoxic-ischemic cerebral injury Major cause of morbidity in children Clinical discrepancies should raise possibility of nonaccidental trauma Several possible reasons for anoxic injury: Anoxic anoxia - not enough oxygen uncommon Anemic anoxia - not enough blood or hemoglobin acute hemorrhage chronic anemia carbon monoxide poisoning Stagnant (ischemic) anoxia (hypoxic-ischemic injury) - not enough blood flow most common localized (such as ischemic strokes) generalized (circulatory collapse / arrhythmias / cardiac arrest) CT reversal sign (reversal of gray/white matter densities) Headache Do we know more than headache? Onset of symptoms? Recent trauma? Neurologic deficits? Are the referring physician and/or neuroradiologist aware? 5

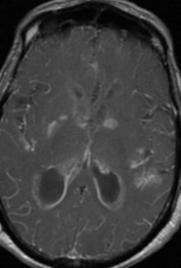
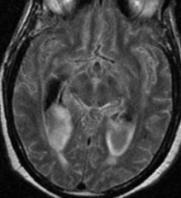
6 MRI Brain: Hyperintense FLAIR signal within scattered cerebral sulci Unremarkable on other sequences Patent basilar cisterns Subarachnoid hemorrhage Differential diagnosis of hyperintense FLAIR signal within subarachnoid space: Subarachnoid hemorrhage Meningitis / pus Carcinomatosis Supplemental oxygen Caution: Most sedated / general anesthesia patients will have this finding be careful not to overcall in this setting! Brain Tumor or Infection Indications Tumor, Infection, Meningitis Sequences 3PL LOC SAG T1 SE SAG T2 FLAIR AX T2 FLAIR AX T1 SE _Inject_ AX T2 TSE FS AX DW EPI SAG T1 IRSPGR 3D +C AX T1 IRSPGR 3D +C MPR COR T1 SE FS +C SAG T1 SE +C OPT AX T1 SE +C OPT Optional SPECT Single Voxel SPECT Multi Voxel Mental status change Do we know more than mental status change? Onset of symptoms? Neurologic deficits? Fever? Elevated WBC? Other studies to consider anticipating? MRI brain => include post-contrast images Include ADC map to assess diffusion restriction 6






7 Cerebral abscess MRI Brain: Left frontal lobe intra-axial lesion with fluidlike signal characteristics Bright T2, low FLAIR, low T1 Partial low T2 rim, peripheral enhancement Large area of central restricted diffusion Marked surrounding vasogenic edema Key characteristics: central diffusion restriction; rim enhancement; vasogenic edema Differential diagnosis: Non-Hodgkin s lymphoma Can have rim enhancement and restricted diffusion, but usually isoto low T2 signal GBM Usually more heterogeneous, without large fluid center or diffusion restriction Tumefactive MS Metastasis Resolving hematoma Infarct Mental status change Do we know more than mental status change? Onset of symptoms? Neurologic deficits? Fever? Elevated WBC? Other studies to consider anticipating? MRI brain => include post-contrast images, particularly if infectious process is suspected 7




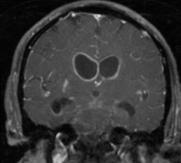
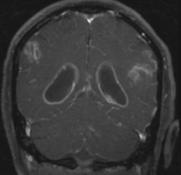

8 CT Head: Layering debris within dilated ventricles Gross pus on ventriculostomy MR Brain: Extensive leptomeningeal enhancement (including brainstem, cord) and ependymal enhancement Parenchymal enhancement along lenticulostriate distribution Scattered small infarcts Diffusion restriction within layering intraventricular pus Hydrocephalus 8






9 Meningitis / Ventriculitis Debris in ventricles with ependymal enhancement ventriculitis Can have ependymal enhancement with NHL, spread of GBM, etc. but usually more nodular/focal and w/o debris 45 year-old woman who presented with severe headache; recent lumbar puncture performed for suspected meningitis Often associated with abscess rupture or indwelling shunt catheter 40-80% mortality but often indolent Do we know more than severe headache? Any neurologic symptoms? Recent surgery? Other studies to consider anticipating? MRI brain WITH contrast concern for meningitis 9





10 MRI Brain without and with contrast: Diffuse thin pachymeningeal / dural enhancement Depressed appearance of brain and brainstem Small bilateral extra-axial fluid collections which are T1 isointense and T2 hyperintense (3 mm maximum diameter) Intracranial Hypotension Result of low CSF volume caused by: Head trauma Tear in spinal nerve root sheath, perineural cyst, or spinal arachnoid diverticulum Iatrogenic causes Lumbar puncture Overdraining ventricular or spinal shunts Spontaneous Results from rupture of spinal arachnoid membrane, which allows CSF passage into subdural or epidural space MR imaging: Diffuse, smooth dural / pachymeningeal enhancement Contrast material accumulates in engorged dural veins and in interstitium of dura Subdural fluid collections Mostly bilateral and without significant mass effect Brain descent Inferior displacement relative to incisural line Brain Trauma / Hemorrhage Indications Trauma, Hemorrhage Sequences 3 PL LOC Sag T1 SE Sag T2 FLAIR Ax T2 FLAIR Ax T1 SE Ax T2 TSE FS Ax DWI EPI Cor T2 TSE Ax GRE 7-month old male with scalp swelling Comments Axial GRE should have TE>25 10








11 Do we know more than scalp swelling? History of trauma or fall? Are the referring physician and/or neuroradiologist aware? Must exclude non-accidental trauma Other studies to consider anticipating? CT => characterize suspected fracture and evaluate for potential associated intracranial hemorrhage Soft tissue and bone algorithms MRI => assess for additional parenchymal injuries and potentially assist with injury / hemorrhage dating 11
, with relative effacement of adjacent sulci")




12 Skull radiographs: Suspected oblique right parietal skull fracture CT Head without contrast: Asymmetric mild right frontoparietal scalp soft tissue swelling, with suspected nondisplaced oblique right parietal skull fracture Heterogeneously hyperdense lenticular right parietal extra-axial fluid collection (2 cm maximum thickness), with relative effacement of adjacent sulci and right lateral ventricle MRI Brain without contrast: Heterogeneously lenticular right parietal extra-axial fluid collection (T1 hyperintense; T2/FLAIR mildly hyperintense), with relative effacement of adjacent sulci and right lateral ventricle Non-accidental trauma CT - recommended in initial evaluation of non-accidental trauma High sensitivity in detecting acute intracranial bleed, fractures, cerebral edema and hypoxic-ischemic injury Attenuation of subdural / epidural hematoma varies by chronicity: Acute - hyperdense Subacute isodense Chronic hypodense Various factors such as low hematocrit and active hemorrhage may affect overall density 80 year-old male with dementia that has progressed over the past 4 years MRI - essential second investigation Best performed 5-10 days after insult Can reliably differentiate between acute and chronic subdural hematoma Most sensitive modality for detecting early ischemic changes Clearly delineates anatomical locations that are difficult to image with CT posterior fossa, anterior part of middle cranial fossa, close to inner table of skull Figure 3a. Sensitivity of GRE imaging for hemosiderin in an 80-year-old man with dementia that has progressed over the past 4 years Do we know more than dementia? Previous CVA symptoms? Risk factors? Neurologic deficits? Other studies to consider anticipating? GRE imaging evaluate for previous hemorrhage associated with infarcts Chao C P et al. Radiographics 2006;26: by Radiological Society of North America 12



13 Figure 3b. Sensitivity of GRE imaging for hemosiderin in an 80-year-old man with dementia that has progressed over the past 4 years Figure 4a. Recurrent CAA-related ICH in a 65-year-old woman with progressive aphasia, right visual field deficits, and headache Chao C P et al. Radiographics 2006;26: Chao C P et al. Radiographics 2006;26: by Radiological Society of North America 2006 by Radiological Society of North America Figure 4b. Recurrent CAA-related ICH in a 65-year-old woman with progressive aphasia, right visual field deficits, and headache MRI Brain: Multiple foci of signal loss / blooming in cortical-subcortical locations Consistent with chronic microhemorrhages Chao C P et al. Radiographics 2006;26: by Radiological Society of North America Cerebral Amyloid Angiopathy Cerebrovascular disorder characterized by deposition of β-amyloid protein in the media and adventitia of small and medium-sized vessels Both sporadic and hereditary forms may occur Manifests radiologically as part or all of a constellation of findings including acute or chronic ICHs in a distinctive cortical-subcortical distribution, leukoencephalopathy, and atrophy Brain Seizure / Dysplasia Indications Seizure, Dysplasia, Mesial temporal sclerosis Sequences 3 PL LOC Sag T1 SE Ax T2 FLAIR Ax T1 SE Ax T2 TSE FS Ax DWI EPI Cor T2 TSE (angled perpendicular to temporal lobes) Cor FLAIR (angled perpendicular to temporal lobes) Ax IR-SPGR / MP-RAGE or Cor IR-SPGR / MP-RAGE Comments Coronal sequences should be thin section perpendicular to the long axis of the hippocampus 13

 Periventricular Nodular Heterotopia In a normal brain, much of the gray matter (consisting mostly of nerve cells) appears on the brain's surface, while white matter")
14 2 year-old female with seizures Do we know more than seizures? Onset of symptoms? Prior studies / previous surgery / trauma? Pulse sequences to consider anticipating? Axial IR-SPGR / MP-RAGE Coronal T2 and FLAIR through hippocampi MRI Brain: In a normal brain, white matter is in the interior, and gray matter is mostly on the surface In patients with periventricular nodular heterotopia, clumps of gray matter, called nodules, appear deep within the brain, instead of on the surface Image courtesy of Bernard Chang, MD, Beth Israel Deaconess Medical Center (via Internet for teaching) Periventricular Nodular Heterotopia In a normal brain, much of the gray matter (consisting mostly of nerve cells) appears on the brain's surface, while white matter (consisting mostly of nerve fibers, or "wiring" interconnecting areas of gray matter) runs deeper in the brain In PNH, a migrational abnormality occurs during development - portions of gray matter sit deep in the brain's core, in the white matter, having failed to migrate out to the surface May serve as elliptogenic foci 14








15 Brain Advanced Protocols Dural venous sinus thrombosis Cor 2D TOF SPGR Sag 2D TOF SPGR (slight oblique angle) Stroke, TIA, Vertebrobasilar infarct, Aneurysm Ax 3D TOF SPGR Ax Perfusion 30 year-old female with mental status changes Tumor, Metabolic abnormality Single voxel spectroscopy (short and long echo; eg. TE 35 and 144) on all new mass lesions Multi voxel spectroscopy - suspected gliomas Perfusion Gd ml/s Do we know more than mental status changes? Any neurologic symptoms? Recent surgery? Dehydration? Are the referring physician and/or neuroradiologist aware? Other studies to consider anticipating? CTV head + contrast; reconstructions / MIP images MRI brain evaluation for ischemia / hemorrhage 15










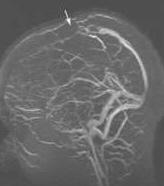
16 CT Head without contrast: Tubular hyperdensity within superior sagittal sinus, torcula, and left frontal cortical veins CT Venography with contrast: Extensive irregular filling defects within superior sagittal sinus extending to torcula, left transverse sinus, and left sigmoid sinus Irregular filling defects within left frontal cortical veins MRI Brain without contrast: Tubular T1 hyperintense signal and loss of normal flow void within superior sagittal sinus, torcula, left transverse sinus, and left frontal cortical veins 16

17 Dural Venous Thrombosis empty delta sign With CT venography, the thrombus does not enhance but dura enhances Triangular defect can be demonstrated within superior sagittal and transverse sinuses Seen in 25 75% of cases Because of volume averaging, may fail to demonstrate a hyperattenuating sinus or an empty delta sign in horizontal segment of superior sagittal sinus or transverse sinus Can disappear in chronic stages with enhancement of organized clot Dural Venous Thrombosis "dense triangle sign Hyperdense triangular shaped structure along posterior aspect of superior sagittal sinus cord sign Hyperdense tubular superficial cortical vein or dural venous sinus Represent intravascular acute blood clots Takes approximately 1 2 weeks to disappear Caution Similarly increased attenuation of cerebral venous sinuses may also represent polycythemia Nonmyelinated brain in neonates makes sinuses appear hyperattenuating Dural Venous Thrombosis MRI Main sign is lack of expected signal flow void on standard T1- and T2-weighted images Challenging diagnosis in acute stage Hypointense signal of acute thrombus mimics normal flow void on T2-weighted images Absence of flow void on T1-weighted images must be carefully sought because thrombus may be isointense / mildly hyperintense to brain tissue 69 year-old female with chronic headaches Do we know more than headaches? Any neurologic symptoms? Concern for cerebral aneurysm? Other studies to consider anticipating? CTA head - reconstructions / MIP images Cerebral angiogram if warranted 17



18 18


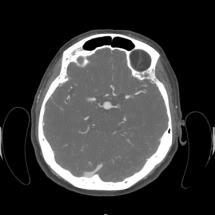
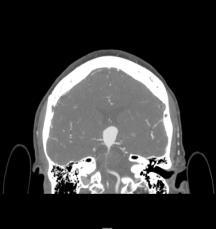
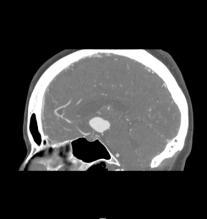
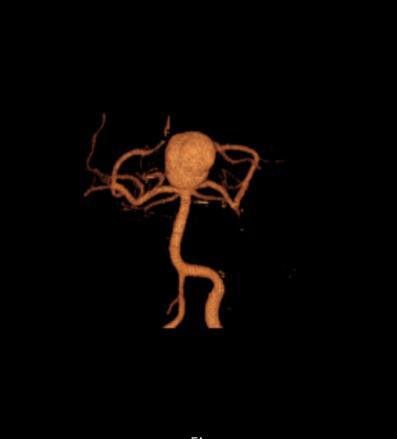
19 CT head angiography: Large aneurysm projects superiorly from basilar tip 20 mm CC, 13 mm transverse, and 23 mm AP Origins of both posterior cerebral arteries and superior cerebellar arteries appear incorporated into aneurysm neck Aneurysm projects superiorly into third ventricle and compresses foramen of Monroe Cerebral angiography: Large, lobulated aneurysm at basilar artery tip Left P1 segment arises from base of aneurysm Right P1 segment appears clear Basilar Tip Aneurysm Occurs at distal bifurcation of basilar artery, between origin of two posterior cerebral arteries Intracranial aneurysm distribution: 30-35% => anterior communicating artery 30-35% => posterior communicating artery origin 20% => middle cerebral artery bifurcation 5% => basilar artery bifurcation or tip 1-5% => other posterior fossa vessels Conventional angiography remains gold standard for detection and characterization of cerebral aneurysms CTA can detect more than 95% of aneurysms identified on conventional angiography 50 year-old male with brain tumor found on an outside hospital MRI study Do we know more than tumor? Previous surgery? Neurologic deficits? Outside images available for radiologist review? Other studies to consider anticipating? MR spectroscopy MR perfusion Post-contrast IR-SPGR (for radiation therapy) 19



20 MR Spectroscopy: Increased choline Decreased NAA Decreased creatine MR Spectroscopy Useful in tumor evaluation and surgical / biopsy planning Although water and fat contribute virtually all of the signal in proton MR imaging, it is possible to suppress these signals and assess the signal from other metabolites including choline, creatine, and NAA Altered in concentration in various disease processes, particularly tumors Middle-aged female with a brain tumor Metabolic mapping of spectra allows rapid assessment of spectral peaks and choline map also demonstrates the most malignant site to biopsy Elevated choline probably represents the cell membrane breakdown secondary to the tumor, while NAA is a metabolite of normal neuronal tissue Do we know more than tumor? Previous surgery and/or biopsy results? Neurologic deficits? Outside images available for radiologist review? Other studies to consider anticipating? MR spectroscopy MR perfusion Post-contrast IR-SPGR (for radiation therapy) 20
21 MR Brain: Large avidly enhancing mass centered within the left insula MR Perfusion: Significant patchy hyperperfusion increased CBF compared with surrounding cortex / juxtacortical white matter MR Perfusion Useful in brain tumor evaluation and surgical / biopsy planning Uses contrast which has slightly different magnetic characteristics from blood - causes a disturbance in the localized magnetic field Signals are analyzed mathematically and expressed as an image (e.g. CBF, CBV, MTT maps). By offsetting the changes in shape in the flow of the contrast bolus against time, it is possible to calculate how much blood is reaching the area of concern within the brain. THANK YOU! HAVE A GREAT DAY! 21
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
41 year old female with headache. Elena G. Violari MD and Leo Wolansky MD
 41 year old female with headache Elena G. Violari MD and Leo Wolansky MD ? Dural Venous Sinus Thrombosis with Hemorrhagic Venous Infarct Acute intraparenchymal hematoma measuring ~3 cm in diameter centered
41 year old female with headache Elena G. Violari MD and Leo Wolansky MD ? Dural Venous Sinus Thrombosis with Hemorrhagic Venous Infarct Acute intraparenchymal hematoma measuring ~3 cm in diameter centered
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Index. aneurysm, 92 carotid occlusion, 94 ICA stenosis, 95 intracranial, 92 MCA, 94
 A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
ISCHEMIC STROKE IMAGING
 ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT
 Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
Benign brain lesions
 Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
Non-Traumatic Neuro Emergencies
 Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Disclosure. + Outline. Case-based approach to neurological emergencies that might present to the ED
 Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Outline Case-based
Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Outline Case-based
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
Meninges and Ventricles
 Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
Intracranial spontaneous hemorrhage mechanisms, imaging and management
 Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Magnetic Resonance Imaging. Basics of MRI in practice. Generation of MR signal. Generation of MR signal. Spin echo imaging. Generation of MR signal
 Magnetic Resonance Imaging Protons aligned with B0 magnetic filed Longitudinal magnetization - T1 relaxation Transverse magnetization - T2 relaxation Signal measured in the transverse plane Basics of MRI
Magnetic Resonance Imaging Protons aligned with B0 magnetic filed Longitudinal magnetization - T1 relaxation Transverse magnetization - T2 relaxation Signal measured in the transverse plane Basics of MRI
NEURORADIOLOGY DIL part 3
 NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
CT and MR findings of systemic lupus erythematosus involving the brain: Differential diagnosis based on lesion distribution
 CT and MR findings of systemic lupus erythematosus involving the brain: Differential diagnosis based on lesion distribution Poster No.: C-2723 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro
CT and MR findings of systemic lupus erythematosus involving the brain: Differential diagnosis based on lesion distribution Poster No.: C-2723 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD
 Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
Imaging Acute Stroke and Cerebral Ischemia
 Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
CT - Brain Examination
 CT - Brain Examination Submitted by: Felemban 1 CT - Brain Examination The clinical indication of CT brain are: a) Chronic cases (e.g. headache - tumor - abscess) b) ER cases (e.g. trauma - RTA - child
CT - Brain Examination Submitted by: Felemban 1 CT - Brain Examination The clinical indication of CT brain are: a) Chronic cases (e.g. headache - tumor - abscess) b) ER cases (e.g. trauma - RTA - child
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Case Conference: Neuroradiology. Case 1: Tumor Case 1: 22yo F w/ HA and prior Seizures
 Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
Laura Tormoehlen, M.D. Neurology and EM-Toxicology Indiana University
 Laura Tormoehlen, M.D. Neurology and EM-Toxicology Indiana University Disclosures! No conflicts of interest to disclose Neuroimaging 101! Plain films! Computed tomography " Angiography " Perfusion! Magnetic
Laura Tormoehlen, M.D. Neurology and EM-Toxicology Indiana University Disclosures! No conflicts of interest to disclose Neuroimaging 101! Plain films! Computed tomography " Angiography " Perfusion! Magnetic
Cerebrovascular diseases-2
 Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Applicable Neuroradiology
 For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
STROKE - IMAGING. Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli.
 STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
An Introduction to Imaging the Brain. Dr Amy Davis
 An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
Neuroradiology: Imaging and Stroke
 Neuroradiology: Imaging and Stroke Stroke 2017 William Gallmann January 28, 2017 Stroke Arterial ischemia/infarct accounts for ~85% Cerebral venous occlusions - 0.5-1% Spontaneous intracranial hemorrhage
Neuroradiology: Imaging and Stroke Stroke 2017 William Gallmann January 28, 2017 Stroke Arterial ischemia/infarct accounts for ~85% Cerebral venous occlusions - 0.5-1% Spontaneous intracranial hemorrhage
SWI including phase and magnitude images
 On-line Table: MRI imaging recommendation and summary of key features Sequence Pathologies Visible Key Features T1 volumetric high-resolution whole-brain reformatted in axial, coronal, and sagittal planes
On-line Table: MRI imaging recommendation and summary of key features Sequence Pathologies Visible Key Features T1 volumetric high-resolution whole-brain reformatted in axial, coronal, and sagittal planes
Attenuation value in HU From -500 To HU From -10 To HU From 60 To 90 HU. From 200 HU and above
 Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
NEURORADIOLOGY Angela Lignelli, MD
 Neuroradiology NEURORADIOLOGY Angela Lignelli, MD Plain radiographs CT MRI Cerebral Angiogram Myelograms Neuroradiology Computerized Axial Tomography (CT) CT without and with contrast CTA CT angiogram
Neuroradiology NEURORADIOLOGY Angela Lignelli, MD Plain radiographs CT MRI Cerebral Angiogram Myelograms Neuroradiology Computerized Axial Tomography (CT) CT without and with contrast CTA CT angiogram
NEURORADIOLOGY Angela Lignelli, MD
 NEURORADIOLOGY Angela Lignelli, MD Neuroradiology Plain radiographs CT MRI Cerebral Angiogram Myelograms 1 Neuroradiology Computerized Axial Tomography (CT) CT without and with contrast CTA CT angiogram
NEURORADIOLOGY Angela Lignelli, MD Neuroradiology Plain radiographs CT MRI Cerebral Angiogram Myelograms 1 Neuroradiology Computerized Axial Tomography (CT) CT without and with contrast CTA CT angiogram
Imaging in a confused patient: Infections and Inflammation
 American Society of Neuroimaging Imaging in a confused patient: Infections and Inflammation January 21, 2017 Los Angeles, California Joshua P. Klein, MD, PhD, FANA, FAAN, FASN Chief, Division of Hospital
American Society of Neuroimaging Imaging in a confused patient: Infections and Inflammation January 21, 2017 Los Angeles, California Joshua P. Klein, MD, PhD, FANA, FAAN, FASN Chief, Division of Hospital
brain MRI for neuropsychiatrists: what do you need to know
 brain MRI for neuropsychiatrists: what do you need to know Christoforos Stoupis, MD, PhD Department of Radiology, Spital Maennedorf, Zurich & Inselspital, University of Bern, Switzerland c.stoupis@spitalmaennedorf.ch
brain MRI for neuropsychiatrists: what do you need to know Christoforos Stoupis, MD, PhD Department of Radiology, Spital Maennedorf, Zurich & Inselspital, University of Bern, Switzerland c.stoupis@spitalmaennedorf.ch
CEREBROVASCULAR DISEASES. By: Shifaa AlQa qa
 CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Neuroradiology MR Protocols
 Neuroradiology MR Protocols Brain protocols N 1: Brain MRI without contrast N 2: Pre- and post-contrast brain MRI N 3 is deleted N 4: Brain MRI without or pre-/post-contrast (seizure protocol) N 5: Pre-
Neuroradiology MR Protocols Brain protocols N 1: Brain MRI without contrast N 2: Pre- and post-contrast brain MRI N 3 is deleted N 4: Brain MRI without or pre-/post-contrast (seizure protocol) N 5: Pre-
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
RINGS N THINGS: Imaging Patterns in Differential Diagnosis. Anne G. Osborn, M.D.
 RINGS N THINGS: Imaging Patterns in Differential Diagnosis Anne G. Osborn, M.D. ExpDDxs: Intra-axial (Parenchymal) Lesions Ring-enhancing lesions, solitary 1 Ring-enhancing lesion crossing corpus callosum
RINGS N THINGS: Imaging Patterns in Differential Diagnosis Anne G. Osborn, M.D. ExpDDxs: Intra-axial (Parenchymal) Lesions Ring-enhancing lesions, solitary 1 Ring-enhancing lesion crossing corpus callosum
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
The dura is sensitive to stretching, which produces the sensation of headache.
 Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
What Are We Going to Do? Fourth Year Meds Clinical Neuroanatomy. Hydrocephalus and Effects of Interruption of CSF Flow. Tube Blockage Doctrine
 Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
NEURO PROTOCOLS MRI NEURO PROTOCOLS (SIEMENS SCANNERS)
") Page 1 NEURO PROTOCOLS Brain Stroke Brain Brain with contrast Brain for seizures Brain for MS Brain for Pineal gland Sella FAST Scan for hydrocephalus MRA/MRV Brain MRA carotids 8 th nerve Cranial nerves
Page 1 NEURO PROTOCOLS Brain Stroke Brain Brain with contrast Brain for seizures Brain for MS Brain for Pineal gland Sella FAST Scan for hydrocephalus MRA/MRV Brain MRA carotids 8 th nerve Cranial nerves
secondary effects and sequelae of head trauma.
 Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
RING ENCHANCING LESION BY M.S. HEMHNATH
 RING ENCHANCING LESION BY M.S. HEMHNATH A 21 YRS FEMALE CAME WITH H/O HEADACHE AND SEIZURE FOR THE PAST ONE MONTH. NO OTHER FOCAL NEUROLOGICAL DEFICIT. DIFFERENTIAL DIAGNOSIS For this case are Neurocysticerosis
RING ENCHANCING LESION BY M.S. HEMHNATH A 21 YRS FEMALE CAME WITH H/O HEADACHE AND SEIZURE FOR THE PAST ONE MONTH. NO OTHER FOCAL NEUROLOGICAL DEFICIT. DIFFERENTIAL DIAGNOSIS For this case are Neurocysticerosis
Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review
 Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review M B Moss, MD; L Lanier, MD; R Slater; C L Sistrom, MD; R G Quisling, MD; I M Schmalfuss, MD; and D Rajderkar, MD Contact:
Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review M B Moss, MD; L Lanier, MD; R Slater; C L Sistrom, MD; R G Quisling, MD; I M Schmalfuss, MD; and D Rajderkar, MD Contact:
NEURO IMAGING OF ACUTE STROKE
 1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
Structural and functional imaging for the characterization of CNS lymphomas
 Structural and functional imaging for the characterization of CNS lymphomas Cristina Besada Introduction A few decades ago, Primary Central Nervous System Lymphoma (PCNSL) was considered as an extremely
Structural and functional imaging for the characterization of CNS lymphomas Cristina Besada Introduction A few decades ago, Primary Central Nervous System Lymphoma (PCNSL) was considered as an extremely
NEURORADIOLOGY Part I
 NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED DISEASES OF CNS BRAIN Developmental anomalies Cerebrovascular disorders Tumours Inflammatory diseases Trauma DISEASES
NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED DISEASES OF CNS BRAIN Developmental anomalies Cerebrovascular disorders Tumours Inflammatory diseases Trauma DISEASES
What Is an Arteriovenous malformation (AVM)?
?") American Society of Neuroradiology What Is an Arteriovenous malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall
American Society of Neuroradiology What Is an Arteriovenous malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall
MRI and differential diagnosis in patients suspected of having MS
 Andrea Falini Italy MRI and differential diagnosis in patients suspected of having MS IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Outline of presentation - Diagnostic criteria
Andrea Falini Italy MRI and differential diagnosis in patients suspected of having MS IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Outline of presentation - Diagnostic criteria
Outline. Neuroradiology. Diffusion Imaging in. Clinical Applications of. Basics of Diffusion Imaging. Basics of Diffusion Imaging
 Clinical Applications of Diffusion Imaging in Neuroradiology No disclosures Stephen F. Kralik Assistant Professor of Radiology Indiana University School of Medicine Department of Radiology and Imaging
Clinical Applications of Diffusion Imaging in Neuroradiology No disclosures Stephen F. Kralik Assistant Professor of Radiology Indiana University School of Medicine Department of Radiology and Imaging
Department of Radiology University of California San Diego. MR Angiography. Techniques & Applications. John R. Hesselink, M.D.
 Department of Radiology University of California San Diego MR Angiography Techniques & Applications John R. Hesselink, M.D. Vascular Imaging Arterial flow void Flow enhancement Gadolinium enhancement Vascular
Department of Radiology University of California San Diego MR Angiography Techniques & Applications John R. Hesselink, M.D. Vascular Imaging Arterial flow void Flow enhancement Gadolinium enhancement Vascular
Case 9511 Hypertensive microangiopathy
 Case 9511 Hypertensive microangiopathy Schepers S, Barthels C Section: Neuroradiology Published: 2011, Nov. 3 Patient: 67 year(s), male Authors' Institution Department of Radiology, Jessa ziekenhuis campus
Case 9511 Hypertensive microangiopathy Schepers S, Barthels C Section: Neuroradiology Published: 2011, Nov. 3 Patient: 67 year(s), male Authors' Institution Department of Radiology, Jessa ziekenhuis campus
Neuroradiology. of Stroke and Headaches
 Neuroradiology of Stroke and Headaches Learning Objec:ves 1. Iden:fy T1 and T2 sequences 2. Recall the normal anatomy of the intracranial circula:on 3. Apply appropriate CT and MR imaging of the brain
Neuroradiology of Stroke and Headaches Learning Objec:ves 1. Iden:fy T1 and T2 sequences 2. Recall the normal anatomy of the intracranial circula:on 3. Apply appropriate CT and MR imaging of the brain
Ventricles, CSF & Meninges. Steven McLoon Department of Neuroscience University of Minnesota
 Ventricles, CSF & Meninges Steven McLoon Department of Neuroscience University of Minnesota 1 Coffee Hour Thursday (Sept 14) 8:30-9:30am Surdyk s Café in Northrop Auditorium Stop by for a minute or an
Ventricles, CSF & Meninges Steven McLoon Department of Neuroscience University of Minnesota 1 Coffee Hour Thursday (Sept 14) 8:30-9:30am Surdyk s Café in Northrop Auditorium Stop by for a minute or an
IV. Cerebrovascular diseases
 IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
Brain Meninges, Ventricles and CSF
 Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
L M Thornton, MD; L Lanier, MD; C L Sistrom, MD; D Rajderkar, MD; A Mancuso, MD; IM Schmalfuss, MD University of Florida, Gainesville Department of
 L M Thornton, MD; L Lanier, MD; C L Sistrom, MD; D Rajderkar, MD; A Mancuso, MD; IM Schmalfuss, MD University of Florida, Gainesville Department of Radiology RSNA Annual Meeting 2016 Trainee call readiness
L M Thornton, MD; L Lanier, MD; C L Sistrom, MD; D Rajderkar, MD; A Mancuso, MD; IM Schmalfuss, MD University of Florida, Gainesville Department of Radiology RSNA Annual Meeting 2016 Trainee call readiness
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases
 How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
Meningeal thickening in MRI: from signs to etiologies
 Meningeal thickening in MRI: from signs to etiologies Poster No.: C-1979 Congress: ECR 2016 Type: Educational Exhibit Authors: A. Hssine, N. Mallat, M. Limeme, H. Zaghouani, S. Majdoub, H. Amara, D. Bakir,
Meningeal thickening in MRI: from signs to etiologies Poster No.: C-1979 Congress: ECR 2016 Type: Educational Exhibit Authors: A. Hssine, N. Mallat, M. Limeme, H. Zaghouani, S. Majdoub, H. Amara, D. Bakir,
HYPERTENSIVE ENCEPHALOPATHY
 HYPERTENSIVE ENCEPHALOPATHY Reversible posterior leukoencephalopathy syndrome Cause Renal disease Pheochromocytoma Disseminated vasculitis Eclampsia Acute toxemia Medications & illicit drugs (cocaine)
HYPERTENSIVE ENCEPHALOPATHY Reversible posterior leukoencephalopathy syndrome Cause Renal disease Pheochromocytoma Disseminated vasculitis Eclampsia Acute toxemia Medications & illicit drugs (cocaine)
Dating Neurological Injury
 Dating Neurological Injury wwwwwwwww Jeff L. Creasy Dating Neurological Injury A Forensic Guide for Radiologists, Other Expert Medical Witnesses, and Attorneys Jeff L. Creasy Associate Professor of Neuroradiology
Dating Neurological Injury wwwwwwwww Jeff L. Creasy Dating Neurological Injury A Forensic Guide for Radiologists, Other Expert Medical Witnesses, and Attorneys Jeff L. Creasy Associate Professor of Neuroradiology
NEURORADIOLOGY Part I
 NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
M555 Medical Neuroscience Blood Flow in CNS Meninges Blood Brain Barrier CSF
 M555 Medical Neuroscience Blood Flow in CNS Meninges Blood Brain Barrier CSF Arterial Blood Flow to CNS approximately % of what goes wrong within the skull that produces neurological deficits is vascular
M555 Medical Neuroscience Blood Flow in CNS Meninges Blood Brain Barrier CSF Arterial Blood Flow to CNS approximately % of what goes wrong within the skull that produces neurological deficits is vascular
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Brain Pain Infections of the CNS
 FRIDAY, OCTOBER 28, 2016 Brain Pain Infections of the CNS Suyash Mohan MD, PDCC Assistant Professor of Radiology & Neurosurgery Division of Neuroradiology, Department of Radiology Perelman School of Medicine
FRIDAY, OCTOBER 28, 2016 Brain Pain Infections of the CNS Suyash Mohan MD, PDCC Assistant Professor of Radiology & Neurosurgery Division of Neuroradiology, Department of Radiology Perelman School of Medicine
Tutorials. By Dr Sharon Truter
 Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Medical Review Guidelines Magnetic Resonance Angiography
 Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Functional aspects of anatomical imaging techniques
 Functional aspects of anatomical imaging techniques Nilendu Purandare Associate Professor & Consultant Radiologist Tata Memorial Centre Functional/metabolic/molecular imaging (radioisotope scanning) PET
Functional aspects of anatomical imaging techniques Nilendu Purandare Associate Professor & Consultant Radiologist Tata Memorial Centre Functional/metabolic/molecular imaging (radioisotope scanning) PET
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
NEURORADIOLOGY DIL part 4
 NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Transverse Dural Sinus Thrombosis Joseph Junewick, MD FACR
 Transverse Dural Sinus Thrombosis Joseph Junewick, MD FACR 03/19/2010 History Child with headache and otomastoiditis. Diagnosis Dural venous thrombosis secondary to mastoiditis Discussion The cerebral
Transverse Dural Sinus Thrombosis Joseph Junewick, MD FACR 03/19/2010 History Child with headache and otomastoiditis. Diagnosis Dural venous thrombosis secondary to mastoiditis Discussion The cerebral
Masses of the Corpus Callosum
 Masses of the Corpus Callosum Kesav Raghavan, HMS Year III Dr. Agenda Corpus Callosum Development and Anatomy Our Patient: Clinical Presentation Differential Diagnosis of Masses in the Corpus Callosum
Masses of the Corpus Callosum Kesav Raghavan, HMS Year III Dr. Agenda Corpus Callosum Development and Anatomy Our Patient: Clinical Presentation Differential Diagnosis of Masses in the Corpus Callosum
Pediatric CNS Tumors. Disclosures. Acknowledgements. Introduction. Introduction. Posterior Fossa Tumors. Whitney Finke, MD
 Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
Insults to the Term Brain
 Insults to the Term Brain Monica Epelman, MD mepelman@nemours.org Literature comparing US and MR has deficiencies Retrospective studies Long time interval between US and MR exams in the same patient
Insults to the Term Brain Monica Epelman, MD mepelman@nemours.org Literature comparing US and MR has deficiencies Retrospective studies Long time interval between US and MR exams in the same patient
MRI and CT of the CNS
 MRI and CT of the CNS Dr.Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Computed Tomography CT is used for the detection of intracranial lesions. CT relies
MRI and CT of the CNS Dr.Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Computed Tomography CT is used for the detection of intracranial lesions. CT relies
RADIOLOGY TEACHING CONFERENCE
 RADIOLOGY TEACHING CONFERENCE John Athas, MD Monica Tadros, MD Columbia University, College of Physicians & Surgeons Department of Otolaryngology- Head & Neck Surgery September 27, 2007 CT SCAN IMAGING
RADIOLOGY TEACHING CONFERENCE John Athas, MD Monica Tadros, MD Columbia University, College of Physicians & Surgeons Department of Otolaryngology- Head & Neck Surgery September 27, 2007 CT SCAN IMAGING
Anoxic brain injury CT and MRI patterns - quick pictoral quide for junior radiologists.
 Anoxic brain injury CT and MRI patterns - quick pictoral quide for junior radiologists. Poster No.: C-1844 Congress: ECR 2017 Type: Educational Exhibit Authors: A. Kecler - Pietrzyk, W. Torreggiani ; Dublin/IE,
Anoxic brain injury CT and MRI patterns - quick pictoral quide for junior radiologists. Poster No.: C-1844 Congress: ECR 2017 Type: Educational Exhibit Authors: A. Kecler - Pietrzyk, W. Torreggiani ; Dublin/IE,
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Magnetic Resonance Imaging for Neurological Conditions. Lawrance Yip Department of Radiology Queen Mary Hospital
 Magnetic Resonance Imaging for Neurological Conditions Lawrance Yip Department of Radiology Queen Mary Hospital Outline Strength and limitations of MRI for neurological conditions MR Imaging techniques
Magnetic Resonance Imaging for Neurological Conditions Lawrance Yip Department of Radiology Queen Mary Hospital Outline Strength and limitations of MRI for neurological conditions MR Imaging techniques
Disorders of the Nervous System. Disorders of the Neurological System. General Endpoints of CNS Disease. General Endpoints of CNS Disease
 HD in Nursing-Pathophysiology Disorders of the Nervous System What are some disorders of the nervous system? Disorders of the Neurological System Dr. C.H. Lai The nervous system is vulnerable to various
HD in Nursing-Pathophysiology Disorders of the Nervous System What are some disorders of the nervous system? Disorders of the Neurological System Dr. C.H. Lai The nervous system is vulnerable to various
Neurology Clerkship Learning Objectives
 Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
On Call Guide to CT Perfusion. Updated: March 2011
 On Call Guide to CT Perfusion Updated: March 2011 CT Stroke Protocol 1. Non contrast CT brain 2. CT perfusion: contrast 40cc bolus dynamic imaging at 8 slice levels ~ 60 sec creates perfusion color maps
On Call Guide to CT Perfusion Updated: March 2011 CT Stroke Protocol 1. Non contrast CT brain 2. CT perfusion: contrast 40cc bolus dynamic imaging at 8 slice levels ~ 60 sec creates perfusion color maps
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
Characteristic features of CNS pathology. By: Shifaa AlQa qa
 Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Vascular Malformations
 Vascular Malformations LTC Robert Shih Chief of Neuroradiology Walter Reed Medical Center Special thanks to LTC Alice Smith (retired) Disclosures: None. This presentation reflects the personal views of
Vascular Malformations LTC Robert Shih Chief of Neuroradiology Walter Reed Medical Center Special thanks to LTC Alice Smith (retired) Disclosures: None. This presentation reflects the personal views of
POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME: MAGNETIC RESONANCE IMAGING AND DIFFUSION-WEIGHTED IMAGING IN 12 CASES
 Posterior reversible encephalopathy syndrome POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME: MAGNETIC RESONANCE IMAGING AND DIFFUSION-WEIGHTED IMAGING IN 12 CASES Mei-Chun Chou, Ping-Hong Lai, Lee-Ren Yeh,
Posterior reversible encephalopathy syndrome POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME: MAGNETIC RESONANCE IMAGING AND DIFFUSION-WEIGHTED IMAGING IN 12 CASES Mei-Chun Chou, Ping-Hong Lai, Lee-Ren Yeh,