Hypertension Clinical Pearls: We re treating more than a number
|
|
|
- Mavis Bates
- 6 years ago
- Views:
Transcription



1 Hypertension Clinical Pearls: We re treating more than a number Emily Ashjian, PharmD, BCPS, BCACP February 2017
2 Learning Objectives Review blood pressure goals and differences between treatment guidelines Discuss treatment strategies for patients with resistant hypertension Develop appropriate treatment regimens for hypertension based on patient specific factors and co-morbidities
3 Meet JS 67 year old male referred to the ambulatory care clinical pharmacist for management of resistant hypertension. Previously presented as a new patient 3 weeks ago after seeking care in the ED for a gout flare which has since resolved. PMH: HTN, T2DM, HFrEF (EF 36%), AF, STEMI (3/2015), gout, migraines, Stage 3 CKD Social hx: -EtOH: 2-3 drinks per night -Tobacco: ½ ppd (recently decreased from 1ppd) Allergies: ACE-Is tried several in the past (cough) Vitals: BP: 164/94 mmhg, HR 82 Weight: 170 lbs BMI: 32.5
4 Meet JS Medications: allopurinol 100 mg daily atenolol 25 mg daily aspirin 81 mg daily atorvastatin 40 mg daily apixaban 5 mg twice daily hydrochlorothiazide12.5 mg daily clonidine 0.1 mg daily furosemide 20 mg daily glipizide XL 10 mg daily ibuprofen 400 mg twice daily as needed losartan 25 mg daily metformin 1000 mg twice daily potassium chloride 20 meq daily tramadol 50 mg twice daily as needed Labs 2/2/17 Na 135 meq/l K 4.2 meq/l BUN 29 mg/dl SCr 1.4 g/dl Glucose 179 mg/dl Total Cholesterol 211 mg/dl HDL 42 mg/dl TG 250 mg/dl LDL-C 119 mg/dl Urine microal/cr 19 mg/g egfr HbA1c 8.2% Uric acid 6.7 CrCl 59 ml/min/1.73 m2 ~56 ml/min
5 What is Hypertension (HTN)? 2 or more blood pressure readings 140/90 mmhg 2 or more clinical encounters Systolic blood pressure 140 mmhg Diastolic blood pressure 90 mmhg Taking antihypertensive medications

6 Resistant HTN BP 140/90 mmhg while using optimally dosed medications from 3 different classes including a diuretic Taking 4 or more antihypertensives regardless of BP Circulation 2008;117:e510-e526.
7 Etiology Primary Hypertension (90-95%) Idiopathic Secondary Hypertension (5-10%) Chronic kidney disease Cushing s syndrome or excess glucocorticoid states Drug-induced or drug-related Obstructive uropathy Pheochromocytoma Primary aldosteronism or other mineralocorticoid excess Renovascular disease Sleep apnea Thyroid or parathyroid disease Circulation 2008;117:e510-e526.

8 Set blood pressure goal JAMA. 2014;311:

9 Comparison of Blood Pressure Goals HTN: Hypertension. CV: Cardiovascular. ASH/ISH: American Society of Hypertension/International Society of Hypertension. CHEP: Canadian Hypertension Education Program. ESH/ESC: European Society of Hypertension/European Society of Cardiology. ADA: American Diabetes Association. ACC/AHA: American College of Cardiology/American Heart Association. KDIGO: Kidney Disease: Improving Global Outcomes. Adapted from: ACCP Pharmacotherapy Self-Assessment Program See last slide for complete citations.
10 ACCORD N Engl J Med 2010;362:

11 Lifestyle changes Hypertension. 2008;51: Hypertension. 2003;42:

12 Select Medications JAMA. 2014;311:
13 Back to JS Medications: allopurinol 100 mg daily atenolol 25 mg daily aspirin 81 mg daily atorvastatin 40 mg daily apixaban 5 mg twice daily hydrochlorothiazide 12.5 mg daily clonidine 0.1 mg daily furosemide 20 mg daily glipizide XL 10 mg daily ibuprofen 400 mg twice daily as needed losartan 25 mg daily metformin 1000 mg twice daily potassium chloride 20 meq daily tramadol 50 mg twice daily as needed Problem List: HTN T2DM HF AF STEMI (3/2015) Gout Migraines Stage 3 CKD
14 Back to JS Medications by indication: HTN: atenolol 25 mg daily, hydrochlorothiazide 12.5 mg daily, clonidine 0.1 mg daily, furosemide 20 mg daily, losartan 25 mg daily HFrEF: atenolol 25 mg daily, furosemide 20 mg daily, losartan 25 mg daily STEMI: atenolol 25 mg daily, aspirin 81 mg daily, atorvastatin 40 mg daily, losartan 25 mg daily AF: apixaban 5 mg twice daily, atenolol 25 mg daily T2DM: metformin 1000 mg twice daily, glipizide XL 10 mg daily Gout: allopurinol 100 mg daily Migraines: tramadol 50 mg twice daily as needed No listed problem: ibuprofen 400 mg twice daily as needed, potassium chloride 20 meq daily
15 Cardiovascular Conditions Condition Angina History of Myocardial Infarction Heart Failure with reduced Ejection Fraction (HFrEF) Disease Specific Medication Beta blocker ACE-I if LV dysfunction Beta blocker ACE-I Beta blocker ACE-I Aldosterone antagonist Relatively Contraindicated Non-DHP CCB if reduced LVEF Non-DHP calcium channel blocker Alpha blocker Notes -ARB if ACE-I not tolerated -Beta blockers should be used in low dosage and slowly titrated -Hydralazine + isosorbide dinitrate if ACE-I/ARB not tolerated Adapted from: UMHS FGP Guideline: Essential Hypertension 2014.
16 Post-Myocardial Infarction Beta blocker Oral beta blockers should be continued during and after hospitalization for all patients with STEMI and no contraindications to their use Start and continue for 3 years for all patients with history of MI or ACS (reasonable to continue as chronic therapy after 3 years) Consider as chronic therapy for all other patients with coronary or vascular disease ACE-I Initiate within 24 hours of anterior wall STEMI, in patients presenting with s/sxs of HF, and those with LVEF 40% unless contraindicated Continue indefinitely in those with LVEF 40%, HTN, DM, or CKD ARB Alternative in those unable to tolerate ACE-I Aldosterone Antagonists For those already receiving an ACE-I + beta blocker with LVEF 40% and either symptomatic HF or DM Circulation. 2013;127:
17 Heart Failure HFrEF EF 40% ACE-I Evidence based beta-blocker (carvedilol, metoprolol succinate, bisoprolol) Class II-IV + LVEF < 35%: spironolactone HFrEF (symptomatic) + LVEF < 40% after acute MI: spironolactone HFpEF EF 50% Blood pressure control Circulation 2013;133:e
18 HFrEF: ACE-I Recommended in all patients with symptomatic HFrEF (reduce mortality and heart failure hospitalization) Generic Brand Initial dose Target dose Captopril Capoten 6.25 mg TID 50 mg TID Enalapril Vasotec 2.5 mg BID mg BID Fosinopril Monopril 5-10 mg daily 40 mg daily Lisinopril Zestril, Prinivil mg daily mg daily Perindopril Aceon 2 mg daily 8-16 mg daily Quinapril Accupril 5 mg BID 20 mg BID Ramipril Altace mg daily 10 mg daily Trandolapril Mavik 1 mg daily 4 mg daily Circulation 2013;133:e
19 HFrEF: ARBs Recommended in patients with symptomatic HFrEF unable to tolerate an ACE-I (reduce mortality and heart failure hospitalization) Generic Brand Initial dose Target dose Candesartan Atacand 4-8 mg daily 32 mg daily Losartan Cozaar mg daily mg daily Valsartan Diovan mg BID 160 mg BID Avoid combining an ACE-I + ARB Circulation 2013;133:e
20 HFrEF: Beta blockers Recommended in patients with symptomatic HFrEF (reduce mortality and heart failure hospitalizations) Generic Brand Initial dose Target dose Bisoprolol Zebeta 1.25 mg daily 10 mg daily Carvedilol Coreg mg BID mg BID Carvedilol Coreg CR 10 mg daily 80 mg daily Metoprolol succinate Toprol XL mg daily 200 mg daily Circulation 2013;133:e
21 HFrEF: Mineralocorticoid antagonists Recommended in patients with symptomatic HFrEF (reduce mortality and heart failure hospitalizations) Generic Brand Initial dose Target dose Spironolactone Aldactone mg daily 25 mg daily Eplerenone Inspra 25 mg daily 50 mg daily Dosing and titration based on renal function: Estimated CrCl ml/min 50 ml/min Eplerenone Spironolactone Eplerenone Spironolactone Initial dose (K<5) Maintenance (K<5) 25 mg every other day 12.5 mg daily or every other day 25 mg daily mg daily 25 mg daily mg daily 50 mg daily 25 mg daily or BID Circulation 2013;133:e
22 HFrEF: Other vasodilators Recommended in patients with symptomatic HFrEF (reduce HF hospitalizations) Generic Brand Initial dose Target dose Hydralazine/ isosorbide dinitrate BiDil 37.5/20 mg TID 75/40 mg TID Hydralazine Apresoline mg TID 100 mg TID Isosorbide dinitrate Isordil mg TID 40 mg TID Circulation 2013;133:e
23 HFrEF: Loop Diuretics Generic Brand Initial dose Furosemide Lasix mg daily or twice daily Torsemide Demadex mg daily Bumetanide Bumex mg daily or twice daily Conversion (oral): 40 mg furosemide: 20 mg torsemide: 1 mg bumetanide Circulation 2013;133:e

24 Diuretics: Sites of action
25 Thiazide/Thiazide-type Diuretics Formulations & Dosing Generic Brand Dosing (mg) Frequency Chlorthalidone Hygroton Once daily Hydrochlorothiazide Microzide Once daily Indapamide Lozol Once daily Metolazone Zaroxolyn Once daily
26 Cardiovascular Conditions Condition Supraventricular tachycardia (Atrial Fibrillation) Bradycardia Heart block Disease Specific Medication Beta blocker Non-DHP CCB Relatively Contraindicated -- Beta blocker Non-DHP CCB α2-agonist Adapted from: UMHS FGP Guideline: Essential Hypertension 2014.
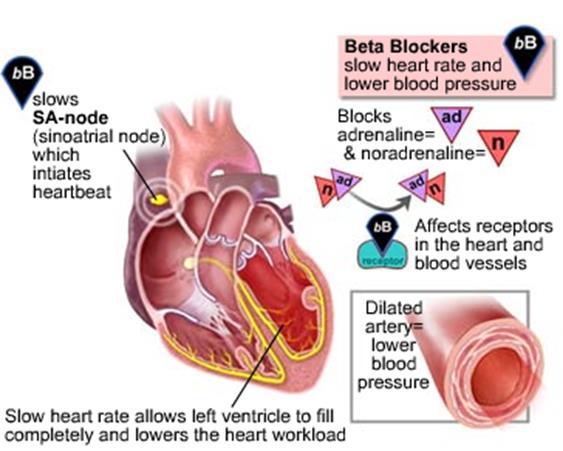
27 β-blockers Mechanism of Action
28 β-blockers Cardioselective atenolol betaxolol bisoprolol metoprolol tartrate metoprolol succinate Tenormin Kerlone Zebeta Lopressor Toprol Mixed (α and non-selective β effects) carvedilol labetalol Coreg Trandate Intrinsic sympathomimetic activity acebutolol carteolol penbutolol pindolol nadolol propranolol propranolol long-acting Sectral Cartrol Levatol Visken Non-selective timolol Corgard Inderal Inderal LA blocadren
29 Calcium Channel Blockers Dihydropyridines amlodipine Norvasc felodipine Plendil isradipine DynaCirc CR nicardipine Cardene nifedipine Procardia nisoldipine Sular Non-dihydropyridines diltiazem verapamil Cardizem, Dilacor, Taztia, Tiazac Calan, Isoptin, Verelan
30 Calcium Channel Blockers Mechanism of Action Calcium Channel Blocker Dihydropyridine Calcium channels on vascular smooth muscle Site of inhibition Calcium channels of cardiac conduction system Non-dihydropyridine
31 Back to JS Medications by indication: HTN: atenolol 25 mg daily, hydrochlorothiazide12.5 mg daily, clonidine 0.1 mg daily, furosemide 20 mg daily, losartan 25 mg daily HFrEF: atenolol 25 mg daily, furosemide 20 mg daily, losartan 25 mg daily STEMI: atenolol 25 mg daily, aspirin 81 mg daily, atorvastatin 40 mg daily, losartan 25 mg daily AF: apixaban 5 mg twice daily, atenolol 25 mg daily T2DM: metformin 1000 mg twice daily, glipizide XL 10 mg daily Gout: allopurinol 100 mg daily Migraines: sumatriptan 100 mg as needed No listed problem: ibuprofen 400 mg twice daily as needed, potassium chloride 20 meq daily
32 Endocrine/Renal Condition Disease Specific Medication Relatively Contraindicated Notes Diabetes Mellitus ACE-I or ARB DHP CCBs, thiazides may be used if uma/cr WNL Chronic Kidney Disease Gout ACE-I DHP CCB (alone) -ARB if ACE-I not tolerated -Consider spironolactone or eplerenone if proteinuria -Loop diuretic if egfr < 30 Losartan (uricosuric) -Thiazides may contribute to gout Adapted from: UMHS FGP Guideline: Essential Hypertension 2014.
33 Central Nervous System/Psychiatric Condition Disease Specific Medication Relatively Contraindicated Notes Headaches Beta blocker Non-DHP CCB -Propranolol, timolol for migraine prophylaxis -Verapamil for cluster headache prophylaxis Essential tremor Beta blocker Concurrent lithium use Beta blocker Non-DHP CCB DHP CCB Diuretic ACEI ARB -Thiazides may increase lithium level by 25-40%; ACE- Is, ARBs may also increase lithium concentrations -Potassium sparing diuretics have minor effects PTSD Alpha blocker (prazosin) Crosses blood brain barrier PTSD associated nightmares Adapted from: UMHS FGP Guideline: Essential Hypertension 2014.
34 Genitourinary Conditions Condition Disease Specific Medication Relatively Contraindicated Notes Bilateral renal artery stenosis Beta blocker DHP CCB ACE-I ARB Impotence ACE-I or ARB DHP CCB Avoid beta blockers Adapted from: UMHS FGP Guideline: Essential Hypertension 2014.
35 Special Populations/Other Condition Disease Specific Medication Relatively Contraindicated Notes Pregnancy Methyldopa (preferred) Labetalol, hydralazine, CCB, beta blockers (except atenolol, propranolol) Atenolol Propranolol ACE-I, ARB are absolutely contraindicated Patients taking cyclosporine DHP CCB Beta blocker Reactive Airway Diseases If beta blockers used, start low and slowly titrate Adapted from: UMHS FGP Guideline: Essential Hypertension 2014.
36 Back to JS Medications by indication: HTN: carvedilol 12.5 mg twice daily, furosemide 20 mg daily, losartan 50 mg twice daily, spironolactone 12.5 mg daily HFrEF: carvedilol 12.5 mg twice daily, furosemide 20 mg daily, losartan 50 mg twice daily, spironolactone 12.5 mg daily STEMI: carvedilol 12.5 mg twice daily, aspirin 81 mg daily, atorvastatin 40 mg daily, losartan 50 mg twice daily, spironolactone 12.5 mg daily AF: apixaban 5 mg twice daily, carvedilol 12.5 mg twice daily T2DM: metformin 1000 mg twice daily, glipizide XL 10 mg daily Gout: allopurinol 100 mg daily Migraines: tramadol 50 mg twice daily as needed
37 How low is too low? SBP is a stronger predictor of cardiovascular disease than DBP in adults age > 50 Pulse pressure = SBP-DBP Increased pulse pressure reflects degree of artherosclerotic disease in elderly; measure of increased arterial stiffness Caution with diastolic blood pressure less than 60 mmhg Lancet. 2002;360:

38 24 hour blood pressures N Engl J Med 2006;354:
39 Bedtime Dosing of BP Medication(s) Blood pressure follows a circadian rhythm Non-dippers have a higher risk of cardiovascular events Evidence that moving at least one BP med to bedtime improves BP control, reduces the prevalence of non-dipping, and lowers cardiovascular morbidity and mortality Considerations: Impact on patient adherence Diuretics at bedtime nocturia Diabetes Care 2011; 34: J Clin Hypertension 2014;16:
40 Medication Class ACE-I, ARB Indications to use first line Contraindications Clinical Pearls DM CKD HF or LV dysfunction with LVEF 40% Coronary artery disease Recurrent stroke prevention Bilateral renal artery stenosis Pregnancy Angioedema -SCr increase up to 30% above baseline is acceptable -Monitor for hyperkalemia, dry cough (ACE-I > ARB), angioedema -Avoid in women during childbearing years -Consider lower initial dose in elderly, renal impairment or concomitant diuretic use
41 Medication Class Beta Blockers Indications to use first line Contraindications Clinical Pearls HF or LV systolic dysfunction with LVEF 40% (bisoprolol, carvedilol, metoprolol succinate first line with ACE-I) Post-MI SA or AV node dysfunction Decompensated HF Severe bronchospasm Adjust doses for symptomatic bradycardia May cause exercise intolerance, sexual dysfunction, fatigue Monitor HR regularly
42 Medication Class Thiazide diuretics Potassium sparing diuretics Loop diuretics Indications to use first line Contraindications Clinical Pearls Hypertension Anuria -First line or in combination with an ACE-I, ARB, or CCB -Monitor Na, K, SCr -May cause hyperuricemia -- Anuria Hyperkalemia Severe renal or hepatic disease -Usually used in combination with thiazide diuretic for potassium balance -Monitor K, SCr HF, CKD Anuria -Monitor Na, K, SCr -Ethacrynic acid mg daily may be used if sulfa allergy
43 Medication Class Indications to use first line Contraindications Clinical Pearls Dihydropyridine calcium channel blockers Hypertension Angina -Monitor for peripheral edema Nondiphydropyridine calcium channel blockers Atrial fibrillation Stable angina Heart block LV systolic dysfunction (EF < 40%) -Monitor heart rate -CYP450 inhibitor -Constipation with verapamil
44 Medication Class Indications to use first line Contraindications Clinical Pearls Aldosterone antagonists Resistant HTN HF Anuria Avoid if CrCl < 30 ml/min or K > 5 meq/l Monitor K, SCr at 3 days, 7 days, and monthly x first 3 months after initiation or titration -Gynecomastia with spironolactone Alpha-1 blockers (terazosin, doxazosin, prazosin) BPH PTSD -First dose hypotension start low dose, take at bedtime -4 th or 5 th line
45 Medication Class Indications to use first line Contraindications Clinical Pearls Central alpha-2 agonists (clonidine, methyldopa, guanfacine) Resistant HTN Hypertensive urgency Pregnancy Avoid in HF -De-escalate dose slowly rebound HTN, especially if taking a beta blocker -Dry mouth, orthostatic hypotension Vasodilators (hydralazine, minoxidil) Resistant HTN HTN + HF (hydralazine) -Hydralazine: drug induced lupus, tachycardia (use w/ beta-blocker) -Minoxidil: fluid retention (use with diuretic), hirsutism
46 Guidelines for Reference JNC 8: James PA, Oparil S, Carter BL, et al. JAMA 2014;311: KDIGO: Kidney Int 2013;5: ASH/ISH: Weber MA, Schiffrin EL, White WB, et al. J Clin Hypertens 2014;16: AHA/ACC/ASH: Rosendorff C, Lackland DT, Allison M, et al. Circulation 2015;131:e CHEP: Hackam DG, Quin RR, Ravani P, et al. Can J Cardiol 2013;29: ESH/ESC: Mancia G, Fagard R,Narkiewicz K, et al. J Hypertens 2013;31:
47 Hypertension Clinical Pearls: We re treating more than a number Emily Ashjian, PharmD, BCPS, BCACP February 2017
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
12.5mg, 25mg, 50mg. 25mg, 50mg. 2.5mg, 5mg, 10mg. 5mg, 10mg, 20mg, 100mg. 25mg. -- $2.81 Acetazolamide (IR, 125mg, 250mg, 500mg (ER)
") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Blood Pressure P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular Disorders REVIEW HISTORY: 9/15, 2/13, 2/08, 5/07 LOB
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Blood Pressure P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular Disorders REVIEW HISTORY: 9/15, 2/13, 2/08, 5/07 LOB
Cardiac Medications At A Glance
 Cardiac Medications At A Glance 1) Anticoagulants (Also known as Blood Thinners.) Dalteparin (Fragmin), Danaparoid (Orgaran) Enoxaparin (Lovenox) Heparin (various) Tinzaparin (Innohep) Warfarin (Coumadin)
Cardiac Medications At A Glance 1) Anticoagulants (Also known as Blood Thinners.) Dalteparin (Fragmin), Danaparoid (Orgaran) Enoxaparin (Lovenox) Heparin (various) Tinzaparin (Innohep) Warfarin (Coumadin)
Antihypertensive Agents
 Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
12.5mg, 25mg, 50mg. 25mg, 50mg. 250mg, 500mg, 250mg/5ml. 2.5mg, 5mg, 10mg. 5mg, 10mg, 20mg, 100mg. 25mg
 MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Blood Pressure P&T DATE: 9/11/2018 THERAPEUTIC CLASS: Cardiovascular Disorders REVIEW HISTORY: 5/17, 9/15, 2/13, 2/08, LOB
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Blood Pressure P&T DATE: 9/11/2018 THERAPEUTIC CLASS: Cardiovascular Disorders REVIEW HISTORY: 5/17, 9/15, 2/13, 2/08, LOB
8/19/2016. No Conflicts. I struggled with everything cardiac in nursing school.
 Cindy Weston, DNP, RN, CCRN, CNS CC, FNP BC Assistant Professor, Texas A&M Health Science Center College of Nursing Describe and define epidemiology and pathophysiology of hypertension Differentiate JNC8
Cindy Weston, DNP, RN, CCRN, CNS CC, FNP BC Assistant Professor, Texas A&M Health Science Center College of Nursing Describe and define epidemiology and pathophysiology of hypertension Differentiate JNC8
Preventing and Managing High Blood Pressure
 MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Preventing and Managing High Blood Pressure About This Kit Fortunately, high blood pressure is easily detected and
MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Preventing and Managing High Blood Pressure About This Kit Fortunately, high blood pressure is easily detected and
What in the World is Functional Medicine?
 What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Cardiovascular Clinical Practice Guideline Pilot Implementation
 Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Hypertension is also an important risk factor in the development of chronic kidney disease and heart failure.
 Hypertension Hypertension Hypertension is defined as either a sustained systolic blood pressure of greater than 140 mm Hg or a sustained diastolic blood pressure of greater than 90 mm Hg. Hypertension
Hypertension Hypertension Hypertension is defined as either a sustained systolic blood pressure of greater than 140 mm Hg or a sustained diastolic blood pressure of greater than 90 mm Hg. Hypertension
Adapted d from Federation of Health Regulatory Colleges of Ontario Template Last Updated September 18, 2017
 Insert Logo or Org Name Here Primary Care Medical Directive for Hypertension Management Adapted d from Federation of Health Regulatory Colleges of Ontario Template Last Updated September 18, 2017 Title:
Insert Logo or Org Name Here Primary Care Medical Directive for Hypertension Management Adapted d from Federation of Health Regulatory Colleges of Ontario Template Last Updated September 18, 2017 Title:
Adult Blood Pressure Clinician Guide June 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Hypertension Management - Summary
 Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Diabetes and a Healthy Heart. Meeting 6. Welcome! Glucose. Balance Makes a Difference! Medicine Helps with. Glucose. Balance!
 6-1 Welcome! Welcome to the lesson! It s good to see you again! Before we visit with Uncle Tommy and Kaipo, let s take a few minutes to review the last five meetings. Glucose Balance Makes a Difference!
6-1 Welcome! Welcome to the lesson! It s good to see you again! Before we visit with Uncle Tommy and Kaipo, let s take a few minutes to review the last five meetings. Glucose Balance Makes a Difference!
New Hypertension Guidelines: How Lower Blood Pressure Targets Affect Medication Safety
 New Hypertension Guidelines: How Lower Blood Pressure Targets Affect Medication Safety Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Andrew Straw, PharmD, BC-ADM
New Hypertension Guidelines: How Lower Blood Pressure Targets Affect Medication Safety Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Andrew Straw, PharmD, BC-ADM
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
LESSON ASSIGNMENT. After completing this lesson you will be able to:
 LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 7 Therapeutics III. Antihypertensive Agents. LESSON ASSIGNMENT Paragraphs 7-1--7-12. LESSON OBJECTIVES After completing this lesson you will be able to: 7-1. From
LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 7 Therapeutics III. Antihypertensive Agents. LESSON ASSIGNMENT Paragraphs 7-1--7-12. LESSON OBJECTIVES After completing this lesson you will be able to: 7-1. From
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%
 with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%") Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Hypertension: Update
 Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC
 DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC Pharmacotherapy of HTN Rationale for reducing arterial pressure Reduce cardiac output Reduce heart rate Reduce stroke
DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC Pharmacotherapy of HTN Rationale for reducing arterial pressure Reduce cardiac output Reduce heart rate Reduce stroke
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Network Hypertension Algorithm
 Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
Physician/Clinic Collaborative Practice Agreement
 Physician/Clinic Collaborative Practice Agreement Effective October 1, 2010, Connecticut Senate Bill 428 (PA 10-117) extends to all settings and medical conditions the opportunity for licensed pharmacists
Physician/Clinic Collaborative Practice Agreement Effective October 1, 2010, Connecticut Senate Bill 428 (PA 10-117) extends to all settings and medical conditions the opportunity for licensed pharmacists
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood:
 Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Contemporary Management of Heart Failure. Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium
 Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Medications and Falls Part 1
 Medications and Falls Part 1 Introduction with General Principles and Risk Evaluation for Cardiovascular Medications Dennis J Chapron Medication Safety Pharmacist Saint Francis Hospital and Medical Center
Medications and Falls Part 1 Introduction with General Principles and Risk Evaluation for Cardiovascular Medications Dennis J Chapron Medication Safety Pharmacist Saint Francis Hospital and Medical Center
Some Facts. Medications and Falls Part 1. Centers for Disease Control (CDC) Falls Statistics for Older Adults ( 65yrs) 11/27/2018
 Falls Statistics for Older Adults ( 65yrs) 11/27/2018") Medications and Falls Part 1 Introduction with General Principles and Risk Evaluation for Cardiovascular Medications Dennis J Chapron reports no real or potential conflicts of interest relevant to this
Medications and Falls Part 1 Introduction with General Principles and Risk Evaluation for Cardiovascular Medications Dennis J Chapron reports no real or potential conflicts of interest relevant to this
PassAssured's Pharmacy Technician Training Systems. Medication Review. Cardiovascular Drugs. Pharmacy Technician Training Systems Passassured, LLC
 Medication Review Cardiovascular Drugs Pharmacy Technician Training Systems Passassured, LLC p1 Medication Review, Cardiovascular Drugs Click Here for Glossary Index! Click Here to Print Topic Help File
Medication Review Cardiovascular Drugs Pharmacy Technician Training Systems Passassured, LLC p1 Medication Review, Cardiovascular Drugs Click Here for Glossary Index! Click Here to Print Topic Help File
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Case 1. Case 2. What do you think about reducing or discontinuing some of the above now that his LVEF has normalized?
 Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Value-Based Drug List for ABCs of Diabetes
 Effective January 1, 2019 Value-Based Drug List for ABCs of Diabetes PCPS provides a Value-Based Benefit Design (VBD) to qualified participants in the ABCs of Diabetes. This means you will have lower out-of-pocket
Effective January 1, 2019 Value-Based Drug List for ABCs of Diabetes PCPS provides a Value-Based Benefit Design (VBD) to qualified participants in the ABCs of Diabetes. This means you will have lower out-of-pocket
MEDICATION FACT SHEET
 ACE Inhibitors Names of ACE Inhibitors: quinapril (Accupril ), enalapril (Vasotec ), ramipril (Altace ), captopril (Capoten ), fosinopril (Monopril ), benazepril (Lotensin ), lisinopril (Zestril, Prinivil
ACE Inhibitors Names of ACE Inhibitors: quinapril (Accupril ), enalapril (Vasotec ), ramipril (Altace ), captopril (Capoten ), fosinopril (Monopril ), benazepril (Lotensin ), lisinopril (Zestril, Prinivil
8/20/2018. Objectives. What is hypertension? cont. What is hypertension? Epidemiology cont. Epidemiology
 Objectives Hypertension (high blood pressure): Clinical Pearls for the Pharmacy Technician Tanya Schmidt PharmD, RPh Director of Central Operations at Thrifty White Pharmacy North Dakota Board of Pharmacy
Objectives Hypertension (high blood pressure): Clinical Pearls for the Pharmacy Technician Tanya Schmidt PharmD, RPh Director of Central Operations at Thrifty White Pharmacy North Dakota Board of Pharmacy
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
ACEBUTOLOL HCL 100MG TABLET GENERIC BETA BLOCKERS ALISKIREN 150MG TABLET RASILAZ RENIN INHIBITOR
 S/N ME OF MEDICATIONS BRANDED/GENERIC DRUG CLASS * UNIT PRICE RANGE (SGD$) 1 ACEBUTOLOL HCL 100MG CAPSULE SECTRAL BETA BLOCKERS 0.50 2 ACEBUTOLOL HCL 100MG TABLET GENERIC BETA BLOCKERS 0.33 3 ALISKIREN
S/N ME OF MEDICATIONS BRANDED/GENERIC DRUG CLASS * UNIT PRICE RANGE (SGD$) 1 ACEBUTOLOL HCL 100MG CAPSULE SECTRAL BETA BLOCKERS 0.50 2 ACEBUTOLOL HCL 100MG TABLET GENERIC BETA BLOCKERS 0.33 3 ALISKIREN
Top 200 Section 4. Cardiovascular Drugs
 Top 200 Section 4 Cardiovascular Drugs Objectives After finishing this presentation the audience should be able to: Describe conditions/disease states that would make a person a candidate for drug therapy.
Top 200 Section 4 Cardiovascular Drugs Objectives After finishing this presentation the audience should be able to: Describe conditions/disease states that would make a person a candidate for drug therapy.
Codes for a Medicare claims-based model to predict LVEF class- User Guide
 Description and citation: This guide accompanies our manuscript [Desai RJ, Lin KJ, Patorno E, et al. Development and Preliminary Validation of a Medicare Claims Based Model to Predict Left Ventricular
Description and citation: This guide accompanies our manuscript [Desai RJ, Lin KJ, Patorno E, et al. Development and Preliminary Validation of a Medicare Claims Based Model to Predict Left Ventricular
Guide to the New Hypertension Guidelines
 Guide to the New Hypertension Guidelines LCDR J. Garrett Sims, PharmD, BCPS Advanced Practice Pharmacist Crow/Northern Cheyenne Hospital Hypertension St Disclosures None Objectives Describe the new hypertension
Guide to the New Hypertension Guidelines LCDR J. Garrett Sims, PharmD, BCPS Advanced Practice Pharmacist Crow/Northern Cheyenne Hospital Hypertension St Disclosures None Objectives Describe the new hypertension
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Hypertension Management: Making Sense of Guidelines and Therapy Options for the Elderly
 Butler University Digital Commons @ Butler University Scholarship and Professional Work COPHS College of Pharmacy & Health Sciences 2015 Hypertension Management: Making Sense of Guidelines and Therapy
Butler University Digital Commons @ Butler University Scholarship and Professional Work COPHS College of Pharmacy & Health Sciences 2015 Hypertension Management: Making Sense of Guidelines and Therapy
ANTIHYPERTENSIVES. Assoc. Prof. Bilgen Başgut
 ANTIHYPERTENSIVES Assoc. Prof. Bilgen Başgut Hypertension Hypertension is a condition in which the blood pressure is persistently higher than normal Hypertension > 140 mmhg > 90 mmhg Systolic Blood Pressure
ANTIHYPERTENSIVES Assoc. Prof. Bilgen Başgut Hypertension Hypertension is a condition in which the blood pressure is persistently higher than normal Hypertension > 140 mmhg > 90 mmhg Systolic Blood Pressure
2014 HYPERTENSION GUIDELINES
 2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
8/20/2017. No Conflicts. I struggled with everything cardiac in nursing school. Review background and definitions of hypertension with
 Cindy Weston, DNP, RN, CCRN, CNS CC, FNP BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Review background and definitions of hypertension with appropriate ICD 10 Discuss
Cindy Weston, DNP, RN, CCRN, CNS CC, FNP BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Review background and definitions of hypertension with appropriate ICD 10 Discuss
Guide to the New Hypertension Guidelines. LCDR J. Garrett Sims, PharmD, BCPS Crow/Northern Cheyenne Hospital
 Guide to the New Hypertension Guidelines LCDR J. Garrett Sims, PharmD, BCPS Crow/Northern Cheyenne Hospital Disclosures None Objectives Describe the new hypertension staging and blood pressure goals and
Guide to the New Hypertension Guidelines LCDR J. Garrett Sims, PharmD, BCPS Crow/Northern Cheyenne Hospital Disclosures None Objectives Describe the new hypertension staging and blood pressure goals and
Hypertension Controversies: SPRINTing to New Goals
 Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Balanced information for better care. Heart failure: Managing risk and improving patient outcomes
 Balanced information for better care Heart failure: Managing risk and improving patient outcomes Heart failure increases hospitalization Heart failure is the most common medical reason for hospitalization
Balanced information for better care Heart failure: Managing risk and improving patient outcomes Heart failure increases hospitalization Heart failure is the most common medical reason for hospitalization
Annual Review of Antihypertensives - Fiscal Year 2009
 Annual Review of Antihypertensives - Fiscal Year 2009 Oklahoma HealthCare Authority April 2010 Current Prior Authorization Criteria There are 7 categories of antihypertensive medications currently included
Annual Review of Antihypertensives - Fiscal Year 2009 Oklahoma HealthCare Authority April 2010 Current Prior Authorization Criteria There are 7 categories of antihypertensive medications currently included
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
4/3/2014 OBJECTIVES BLOOD PRESSURE BASICS. Discuss the new blood pressure guidelines (JNC 8) and recognize the changes from JNC 7
 and recognize the changes from JNC 7") 1 OBJECTIVES Discuss the new blood pressure guidelines (JNC 8) and recognize the changes from JNC 7 Review mechanisms for the main drug classes used to treat hypertension Describe the dosing strategies
1 OBJECTIVES Discuss the new blood pressure guidelines (JNC 8) and recognize the changes from JNC 7 Review mechanisms for the main drug classes used to treat hypertension Describe the dosing strategies
New classification of HT Systolic Diastolic Normal <120 <80 Prehypertension Stage1HT Stage 2 HT >160 or >100
 Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Heart Disease and Prevention PRESENTED BY: DOTTIE CRAIG NP- C, JANE ARCHER NP-C, KATHY DAPPER RN, NICCI FRAVEL RN
 Heart Disease and Prevention PRESENTED BY: DOTTIE CRAIG NP- C, JANE ARCHER NP-C, KATHY DAPPER RN, NICCI FRAVEL RN Objectives Identify Normal Systolic and Diastolic Blood pressures Recognize common Antihypertensive
Heart Disease and Prevention PRESENTED BY: DOTTIE CRAIG NP- C, JANE ARCHER NP-C, KATHY DAPPER RN, NICCI FRAVEL RN Objectives Identify Normal Systolic and Diastolic Blood pressures Recognize common Antihypertensive
TREATMENT OF HYPERTENSION
 TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Medications. Your prescriptions can be filled by your home pharmacy or by the Michigan Medicine Taubman Center outpatient pharmacy.
 Medications Your prescriptions can be filled by your home pharmacy or by the Michigan Medicine Taubman Center outpatient pharmacy. What do I need to know about medications after my heart attack? When you
Medications Your prescriptions can be filled by your home pharmacy or by the Michigan Medicine Taubman Center outpatient pharmacy. What do I need to know about medications after my heart attack? When you
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Living with Congestive Heart Failure: A Guide to a Healthy Heart
 Living with Congestive Heart Failure: A Guide to a Healthy Heart Things to Know, Before You Go Dear Patient/Caregiver These are the things you NEED TO KNOW, BEFORE YOU GO. It is very important that you
Living with Congestive Heart Failure: A Guide to a Healthy Heart Things to Know, Before You Go Dear Patient/Caregiver These are the things you NEED TO KNOW, BEFORE YOU GO. It is very important that you
Cardiovascular Risk Reduction in Diabetic Mellitus. Presenter: Dr. Martin N. Wanyoike MB.CHB., M. Med.(internal med) Physician / Cardiologist
 Physician / Cardiologist") Cardiovascular Risk Reduction in Diabetic Mellitus Presenter: Dr. Martin N. Wanyoike MB.CHB., M. Med.(internal med) Physician / Cardiologist Cardiovascular Risk Reduction in Diabetic Mellitus Disclosures
Cardiovascular Risk Reduction in Diabetic Mellitus Presenter: Dr. Martin N. Wanyoike MB.CHB., M. Med.(internal med) Physician / Cardiologist Cardiovascular Risk Reduction in Diabetic Mellitus Disclosures
Disclosures. This speaker has indicated there are no relevant financial relationships to be disclosed.
 Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Clinical Teach-Back Cards
 Clinical Teach-Back Cards The Medicare Quality Improvement Organization for Texas TMF Health Quality Institute focuses on improving lives by improving the quality of health care through contracts with
Clinical Teach-Back Cards The Medicare Quality Improvement Organization for Texas TMF Health Quality Institute focuses on improving lives by improving the quality of health care through contracts with
sympatholytics sympatholytics sympatholytics
 sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults
 DETAILED SUMMARY FROM THE 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults A REPORT OF THE American College of Cardiology/ American Heart Association
DETAILED SUMMARY FROM THE 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults A REPORT OF THE American College of Cardiology/ American Heart Association
What s at the Heart of the Matter?
 What s at the Heart of the Matter? Inpatient Pharmacy Services for Heart Failure Patients Jason Williamson, PharmD, BCPS Clinical Pharmacy Manager, PGY1 Pharmacy Residency Director Genesys Regional Medical
What s at the Heart of the Matter? Inpatient Pharmacy Services for Heart Failure Patients Jason Williamson, PharmD, BCPS Clinical Pharmacy Manager, PGY1 Pharmacy Residency Director Genesys Regional Medical
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups. Lisa Ivy APRN
 Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Hypertension (HTN) Lecture Note
 Lecture Note") Hypertension (HTN) Lecture Note October, 2009 Chuang-Ye Hong, MD, PhD, FACP Wan-Fang Hospital Taipei Medical University Outline Definition Epidemiology Measurement of BP Secondary cause Target organ damage
Hypertension (HTN) Lecture Note October, 2009 Chuang-Ye Hong, MD, PhD, FACP Wan-Fang Hospital Taipei Medical University Outline Definition Epidemiology Measurement of BP Secondary cause Target organ damage
HEART FAILURE KEEPING YOUR PATIENT AT HOME
 HEART FAILURE KEEPING YOUR PATIENT AT HOME SUZANNE FRAZIER MS, CRNP, NP-C, CHFN HEART FAILURE DISEASE MANAGEMENT COORDINATOR PENN STATE HERSHEY HEART & VASCULAR INSTITUTE IMPACT OF HEART FAILURE In 2010,
HEART FAILURE KEEPING YOUR PATIENT AT HOME SUZANNE FRAZIER MS, CRNP, NP-C, CHFN HEART FAILURE DISEASE MANAGEMENT COORDINATOR PENN STATE HERSHEY HEART & VASCULAR INSTITUTE IMPACT OF HEART FAILURE In 2010,
CONCORD INTERNAL & PULMONARY MEDICINE CONGESTIVE HEART FAILURE PROTOCOL. Douglas G. Kelling, Jr., MD & C. Gismondi-Eagan, MD, FACP
 CONCORD INTERNAL & PULMONARY MEDICINE CONGESTIVE HEART FAILURE PROTOCOL Douglas G. Kelling, Jr., MD & C. Gismondi-Eagan, MD, FACP Revised August 14, 2009 Page 1 Congestive Heart Failure Protocol Patients
CONCORD INTERNAL & PULMONARY MEDICINE CONGESTIVE HEART FAILURE PROTOCOL Douglas G. Kelling, Jr., MD & C. Gismondi-Eagan, MD, FACP Revised August 14, 2009 Page 1 Congestive Heart Failure Protocol Patients
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Factors Involved in Poor Control of Risk Factors
 Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Which antihypertensives are more effective in reducing diastolic hypertension versus systolic hypertension? May 24, 2017
 Which antihypertensives are more effective in reducing diastolic hypertension versus systolic hypertension? May 24, 2017 The most important reason for treating hypertension in primary care is to prevent
Which antihypertensives are more effective in reducing diastolic hypertension versus systolic hypertension? May 24, 2017 The most important reason for treating hypertension in primary care is to prevent
Beta-blockers. Atenolol. Propranolol. Bisoprolol. Metoprolol. Labetalol. Carvedilol.
 Drugs of CVS Beta-blockers Atenolol. Propranolol. Bisoprolol. Metoprolol. Labetalol. Carvedilol. Atenolol.cardioselective Propranolol, nonselective Bisoprolol, cardioselective Metoprolol Carvedilol, alpha
Drugs of CVS Beta-blockers Atenolol. Propranolol. Bisoprolol. Metoprolol. Labetalol. Carvedilol. Atenolol.cardioselective Propranolol, nonselective Bisoprolol, cardioselective Metoprolol Carvedilol, alpha
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
α 1 receptor smooth muscle activation
 Drugs in Hypertension Dr. Yuri Clement Pharmacology Unit, FMS Objectives Revision of physiological control of BP. What is hypertension? Associated risks of uncontrolled hypertension ANTIHYPERTENSIVE DRUGS:
Drugs in Hypertension Dr. Yuri Clement Pharmacology Unit, FMS Objectives Revision of physiological control of BP. What is hypertension? Associated risks of uncontrolled hypertension ANTIHYPERTENSIVE DRUGS:
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Comparison of Oral Beta-Blockers
 This Clinical Resource gives subscribers additional insight related to the Recommendations published in March 2017 ~ Resource #330356 Comparison of Oral Beta-Blockers Noncardioselective s (beta-1 and beta-2
This Clinical Resource gives subscribers additional insight related to the Recommendations published in March 2017 ~ Resource #330356 Comparison of Oral Beta-Blockers Noncardioselective s (beta-1 and beta-2
Treatment of Hypertension
 This Clinical Resource gives subscribers additional insight related to the Recommendations published in January 2018 ~ Resource #340101 Treatment of Hypertension In 2013, the JNC 8 panel released recommendations
This Clinical Resource gives subscribers additional insight related to the Recommendations published in January 2018 ~ Resource #340101 Treatment of Hypertension In 2013, the JNC 8 panel released recommendations
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
CARDIAC IMAGING QUESTIONNAIRE
 Date of test: / / Month day year Last name First name Middle initial Street address City State Zip code Home phone ( ) - Work phone ( ) - Cell Phone ( ) - Email: Age: Demographics: What is your ethnicity?
Date of test: / / Month day year Last name First name Middle initial Street address City State Zip code Home phone ( ) - Work phone ( ) - Cell Phone ( ) - Email: Age: Demographics: What is your ethnicity?
Treatment of Essential Hypertension
 2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology