Update sulle lesioni emorragiche posttraumatiche
|
|
|
- Madison Johnston
- 6 years ago
- Views:
Transcription


1 Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia

2 LAW UPDATING
3 This document provides recommendations only when there is evidence to support them These recommendations do not constitute a complete protocol for clinical use
4 These recommendations be used by others to develop treatment protocols, which necessarily need to incorporate consensus and clinical judgment in areas where current evidence is lacking or insufficient.

5 asdh Present in up to 1/3 of patients with severe TBI Historically associated with a high mortality rate (between 40-60%) and functional recovery which ranges from 19 to 45% Approximately 2/3 of patients with TBI undergoing emergency cranial surgery have an ASDH evacuated LACK OF EVIDENCES Decompressive Craniectomy
6 Use of primary DC in >50% of ASDH cases p<0.001 It cannot be explained by differences in trauma care systems or epidemiology It probably reflects the lack of high quality evidence



7 CLEAR RADIOLOGICAL FINDINGS OF MASS EFFECT Hernia + Shift + Volume HIGH PROBABILITY FOR DC UP TO INTRAOPERATIVE FINDINGS



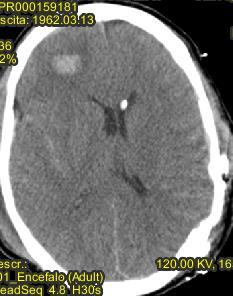
8 VOLUME > Shift Certainty for Surgery on asdh BUT PRIMARY DC? 65 y, rural job accident, GCS 12 on scene GCS 9 after CT No shift No basal cistern effacement

9 SHIFT> volume Certainty for Surgery on asdh BUT PRIMARY DC? 24 y Bicycle fall GCS 14 on scene GCS 11 after CT
 DC - 0.75 (95 % CI: 0.51 1.")
10 Cambridge experience (n=91) Although the confidence intervals overlapped, this study suggests that primary DC could be more effective than craniotomy for patients with ASDH Standardised morbidity ratio was lower in individuals who received DC CR (95 % CI: ) DC (95 % CI: )
 with a primary")

11 Hypothesis: the ability to control ICP (brain swelling) with a primary DC may improve outcome Italian recruitment: iaccarino.corrado@gmail.com
12 STEP 1 STEP 2 STEP 3 IN THEATRE
13 BRAIN CONTUSION LACK OF EVIDENCES Prediction of progression Surgical Indication
14 MONITORING CLINICAL parameters NEURORADIOLOGICAL parameters NEUROPHYSIOLOGICAL parameters (ICP) THESE PARAMETERS DO NOT HAVE THE SAME EVOLUTIVE BEHAVIOR
15 The aim of this retrospective, multi-center study was to identify predictors of unfavourable outcome, analyze the evolution of brain contusions and evaluate specific indications for surgery From January 2008 to December 2011 All patients with TBI + cerebral contusion (CT scan) treated in the Hospitals of the northwestern Emilia Inclusion criteria: Brain contusion > 1 ml 3 CT scan acquired Hospitalization 1 st day of TBI All clinical data available 352 Patients (277 excluded)
16 Patient demographics & Radiological parameters on CT admission
17 RADIOLOGICAL AND CLINICAL PROGRESSION 111 cases of clinical deterioration (31.5%) First 12 hours post-trauma: Clinical parameters CT parameters 22 cases of clinical improvement (6.3%) 219 cases of neurological stability (62.2%) 103 cases of no changing in lesion volume (29,2%) 43 cases of diminution of lesion volume (12,2%) 206 cases of radiological evolution (58,5%)

18 Multivariate analysis: At FOLLOW-UP CT Scan midline shift and/or basal cisterns effacement predictor for onset of clinical deterioration
19 ASSOCIATION BETWEEN CLINICAL AND RADIOLOGICAL PARAMETERS AND NEED FOR SURGERY AFTER 2 ND CT SCAN
20
21 OUTCOME
22
23
24

25 .dramatically similar results.
26
27 BIAS SELECTION?




28 Languages: english Species: humans From 01/01/1990 Title/abstract: «contusion/s», «lesion/s», «h(a)emorrhage/s», «intracranial mass/es», «h(a)ematoma/s» AND «icp» «intracranial pressure»



29

30 I CT Scan

31 I CT Scan NO ICP Monitoring
32 I CT Scan NO ICP Monitoring II CT Scan
33 I CT Scan II CT Scan Unchanged NO ICP Monitoring



34 I CT Scan II CT Scan Unchanged NO ICP Monitoring Petechiae progression &/or High ICP signs Midline Shift > 5mm Effacement of Basal Cisterns ICP Monitoring Disappearing cortical sulci Indistinguished gray /white matter Diffuse hypodensity
35 ICP CONSENSUS 2014 Sedation interruption is dangerous for : Rx signs high ICP and/or Respiratory failure and/or Ongoing emergency extracranial surgery GCS is not completely reliable for : SCI and/or Severe maxillofacial trauma Large bifrontal brain contusions Brain Contusions close to brainstem
36 ICP RULES ICU Monitoring Surgical indications Outcome Mismatched with neuroradiological and clinical data















37 MCA 54y,Trafic accident GCS 15 on scene GCS 13 in ER Mild effacement Temporal Contusion: risk of uncal herniation Frontal contusion Subdural effusion Mild shift 3 Vault fracture EVS ICU Admission Elevated ICP trend 6h control CT scan Better effacement Volume contusion progression WHICH PRIORITY? NO subdural progression Mild shift 5 New epidural mass Epidural evacuation Stable effacement Stable temporal contusion Frontal progression Mild shift 5








38 Secondary decompressive craniectomy + temporal toilette contusion 24h postop: Stable effacement,volume,shift mild R oedema progression h postop: rising ICP trend min max 0 I day II day a.m II day p.m








39 9 d post-dc: Open Box!! & Amyne for hypotension, volume expanders, E. Cloacae pneumonia, Ventricular enlargement & Brain bulging EVD 17d postdc: GCS E3M6Vt, left paresis- 7d EVD spontaneous remotion 1m post DC in NS: Awake, collaborating, left paresis (3/5)...OVERTREATMENT?...HARD TO SAY...





40 36d post DC in NS Awake, collaborating, left upper monoparesis (4/5) No pneumonie No sepsis - Rectal Klebsiella colonization Stable ventricular enlargement Mild Frontal syndrome AUTOLOGOUS CRANIOPLASTY CRANIOPLASTY AS SOON AS POSSIBLE POSSIBLE= No oedema, No Brain swelling, No sepsis






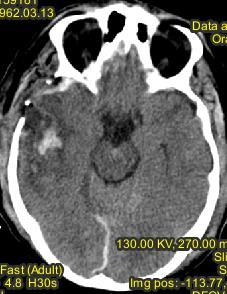
41 MB, 54 y, Fall GCS 7 on scene, OTI standard sedation in ER Fractures: Frontal, L parietal, orbit, ethmoid, sphenoid, dorsum sellae, R maxillar, L zygomus, L occipital, ESAt, IVH. Frontal hypodensity D4, D5 Fractures


 ICP")

42 ICU management Bedside posterior nasal packing No cough reflex GCS 3 (Short halflife sedation >1h) ICP 60 mmhg Sedation level CT scan Clinical signs






43 II CT scan = Clinical signs Volume progression Diencephalic and brainstem involvement GCS 3 No Cough reflex ICP 50 mmhg WITHDRAWAL NS NI decision NO CBF after 72h
44 UPDATE ABOUT SURGICAL DECISION ON BRAIN CONTUSION?

45

 - Leave the controlateral preop insertion via a bolt device (when")
46 SPECULATIVE CONSIDERATIONS -The question is not how high the ICP is but why is it happening -Targeting the number may prevent death from herniation but will not affect the fate of injured neurons RESEARCH CONSIDERATIONS The extent, severity, and time-course of HICP following decompressive surgery are unclear, deserve further research: - To assess effectiveness PRACTICAL CONSIDERATIONS If an intraparenchymal ICP probe is used: - To guide further therapy - insertion under direct vision intra-operatively and tunnelled under the scalp (suggested choice) - Leave the controlateral preop insertion via a bolt device (when available)
47
48
 Suggesting a revision of DC s diameter (1 pts) Early recognition and management ofpostoperative hematoma (3")
49 After primary decompressive craniectomy the ICP monitoring was useful for: Guiding osmotherapies (34 pts) Guiding barbiturate coma (7 pts) Indicating an EVD placement (4 pts) Suggesting a revision of DC s diameter (1 pts) Early recognition and management ofpostoperative hematoma (3 pts)
50 Avoid to transform survival in disability Mismatch clinical, neuroradiological and neuromonitoring data An awake patient and a comatous patient could have no benefit from a surgical evacuation of a brain contusion If you believe in the removal of bone flap after asdh evacuation, please partecipate to the asdh Rescue trial If you do not believe in the removal of bone flap after asdh evacuation, please partecipate to the asdh Rescue trial Preoperative ICP monitoring is indicated when there is a serious concern for the risk of herniation Postoperative ICP monitoring is indicate to drive medical and surgical decisions and to collect speculative data THE LACK OF EVIDENCE IS DUE NOT TO LACK OF EFFECTIVE THERAPIES BUT TO REDUCED PROSPECTIVE LARGE SERIES STUDIES


51 We think it is important to have evidence-based recommendations to clarify what aspects of practice currently can and cannot be supported by evidence, to encourage Use of evidence-based treatments that exist Creativity in treatment and research in areas where evidence does not exist
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD.
 Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
INDEX&NEUROTRAUMA&(INCLUDING&SPINAL&CORD&INJURIES)&!!
&!!") 1 INDEX&NEUROTRAUMA&(INCLUDING&SPINAL&CORD&INJURIES)& Prehospital,care,in,patients,with,severe,traumatic,brain,injury:,does,the,level,of,prehospital, care,influence,mortality?,...,3 Contralateral,extraaxial,hematomas,after,urgent,neurosurgery,of,a,mass,lesion,in,patients,
1 INDEX&NEUROTRAUMA&(INCLUDING&SPINAL&CORD&INJURIES)& Prehospital,care,in,patients,with,severe,traumatic,brain,injury:,does,the,level,of,prehospital, care,influence,mortality?,...,3 Contralateral,extraaxial,hematomas,after,urgent,neurosurgery,of,a,mass,lesion,in,patients,
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN
 Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature
 Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature Anand Sharma 1, Arti Sharma 2, Yashbir Dewan 1 1 Artemis
Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature Anand Sharma 1, Arti Sharma 2, Yashbir Dewan 1 1 Artemis
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Comparison of Burr Holes and Decompressive Craniotomy in the Surgical Treatment of Traumatic Acute Subdural Hematoma
 Med. J. Cairo Univ., Vol. 83, No. 1, March: 259-266, 2015 www.medicaljournalofcairouniversity.net Comparison of Burr Holes and Decompressive Craniotomy in the Surgical Treatment of Traumatic Acute Subdural
Med. J. Cairo Univ., Vol. 83, No. 1, March: 259-266, 2015 www.medicaljournalofcairouniversity.net Comparison of Burr Holes and Decompressive Craniotomy in the Surgical Treatment of Traumatic Acute Subdural
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Only 30% to 40% of acute subdural hematoma (SDH)
") Contralateral Acute Epidural Hematoma After Decompressive Surgery of Acute Subdural Hematoma: Clinical Features and Outcome Thung-Ming Su, MD, Tsung-Han Lee, MD, Wu-Fu Chen, MD, Tao-Chen Lee, MD, and Ching-Hsiao
Contralateral Acute Epidural Hematoma After Decompressive Surgery of Acute Subdural Hematoma: Clinical Features and Outcome Thung-Ming Su, MD, Tsung-Han Lee, MD, Wu-Fu Chen, MD, Tao-Chen Lee, MD, and Ching-Hsiao
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
CASE 1. Female 21 years old DOL: November 28, 2016
 CASE 1 Female 21 years old DOL: November 28, 2016 Injuries and Sequelae: GCS: 4 / 15 and coma for 3 weeks Multifocal intracranial hemorrhage at right thalamus and left frontal and temporal lobe Diffuse
CASE 1 Female 21 years old DOL: November 28, 2016 Injuries and Sequelae: GCS: 4 / 15 and coma for 3 weeks Multifocal intracranial hemorrhage at right thalamus and left frontal and temporal lobe Diffuse
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report
 214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Efficacy of neuroendoscopic evacuation of traumatic intracerebral or intracerebellar hematoma
 Original Contribution Kitasato Med J 2017; 47: 141-147 Efficacy of neuroendoscopic evacuation of traumatic intracerebral or intracerebellar hematoma Hiroyuki Koizumi, 1,2 Daisuke Yamamoto, 1 Yasushi Asari,
Original Contribution Kitasato Med J 2017; 47: 141-147 Efficacy of neuroendoscopic evacuation of traumatic intracerebral or intracerebellar hematoma Hiroyuki Koizumi, 1,2 Daisuke Yamamoto, 1 Yasushi Asari,
Decompressive craniectomy following traumatic brain injury
 Decompressive craniectomy following traumatic brain injury Peter Hutchinson Division of Academic Neurosurgery University of Cambridge Escalating cycle of brain swelling Primary insult Brain swelling Secondary
Decompressive craniectomy following traumatic brain injury Peter Hutchinson Division of Academic Neurosurgery University of Cambridge Escalating cycle of brain swelling Primary insult Brain swelling Secondary
Acute Ischaemic Stroke
 Acute Ischaemic Stroke CT or MR SCA READIG FORM SCA ID: DATE OF READIG: SCA QUALIT: Good Moderate Poor Comment: READER ID: TPE OF SCA: CT: Without contrast: With contrast: MR: Diffusion: Perfusion ote
Acute Ischaemic Stroke CT or MR SCA READIG FORM SCA ID: DATE OF READIG: SCA QUALIT: Good Moderate Poor Comment: READER ID: TPE OF SCA: CT: Without contrast: With contrast: MR: Diffusion: Perfusion ote
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
A Comprehensive Study on Post Traumatic Temporal Contusion in Adults
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/318 A Comprehensive Study on Post Traumatic Temporal Contusion in Adults R Renganathan 1, P John Paul 2, Heber Anandan
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/318 A Comprehensive Study on Post Traumatic Temporal Contusion in Adults R Renganathan 1, P John Paul 2, Heber Anandan
Anton-Babinski syndrome as a rare complication of chronic bilateral subdural hematomas
 DOI: 10.2478/romneu-2018-0050 Article Anton-Babinski syndrome as a rare complication of chronic bilateral subdural hematomas D. Adam, D. Iftimie, Cristiana Moisescu, Gina Burduşa ROMANIA Romanian Neurosurgery
DOI: 10.2478/romneu-2018-0050 Article Anton-Babinski syndrome as a rare complication of chronic bilateral subdural hematomas D. Adam, D. Iftimie, Cristiana Moisescu, Gina Burduşa ROMANIA Romanian Neurosurgery
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Use of CT in minor traumatic brain injury. Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD
 Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Case Report Neuroendoscopic Removal of Acute Subdural Hematoma with Contusion: Advantages for Elderly Patients
 Case Reports in Neurological Medicine Volume 2016, Article ID 2056190, 5 pages http://dx.doi.org/10.1155/2016/2056190 Case Report Neuroendoscopic Removal of Acute Subdural Hematoma with Contusion: Advantages
Case Reports in Neurological Medicine Volume 2016, Article ID 2056190, 5 pages http://dx.doi.org/10.1155/2016/2056190 Case Report Neuroendoscopic Removal of Acute Subdural Hematoma with Contusion: Advantages
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience
 80 Original Article THIEME Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience V. Velho 1 Hrushikesh U. Kharosekar 1 Jasmeet S. Thukral 1 Shonali Valsangkar
80 Original Article THIEME Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience V. Velho 1 Hrushikesh U. Kharosekar 1 Jasmeet S. Thukral 1 Shonali Valsangkar
Efficacy of Decompressive Craniectomy in Acute Subdural Hematoma in Head Injury Patients, Madurai Medical College, Madurai
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/107 Efficacy of Decompressive Craniectomy in Acute Subdural Hematoma in Head Injury Patients, Madurai Medical College,
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/107 Efficacy of Decompressive Craniectomy in Acute Subdural Hematoma in Head Injury Patients, Madurai Medical College,
Supplementary Online Content
 Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Head injuries in children. Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead
 Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
APP Placement of ICP Monitors. Sanjay Patra, MD
 APP Placement of ICP Monitors Sanjay Patra, MD Can midlevel providers place external ventricular drains safely and accurately? Sanjay Patra MD MSc Director Epilepsy Surgery Director Brain Trauma Spectrum
APP Placement of ICP Monitors Sanjay Patra, MD Can midlevel providers place external ventricular drains safely and accurately? Sanjay Patra MD MSc Director Epilepsy Surgery Director Brain Trauma Spectrum
Surgical Management & Clinical Outcome of Severe Brain Trauma due to Acute Subdural Hematoma.
 International Journal of Sciences: Basic and Applied Research (IJSBAR) ISSN 2307-4531 (Print & Online) http://gssrr.org/index.php?journal=journalofbasicandapplied ----------------------------------------------------------------------------------------------------------------
International Journal of Sciences: Basic and Applied Research (IJSBAR) ISSN 2307-4531 (Print & Online) http://gssrr.org/index.php?journal=journalofbasicandapplied ----------------------------------------------------------------------------------------------------------------
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Evaluation of Craniocerebral Trauma Using Computed Tomography
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 57-62 Evaluation of Craniocerebral Trauma Using Computed Tomography
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 57-62 Evaluation of Craniocerebral Trauma Using Computed Tomography
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases
 How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Extradural hematoma (EDH) accounts for 2% of all head injuries (1). In
 accounts for 2% of all head injuries (1). In") CASE REPORT Conservative management of extradural hematoma: A report of sixty-two cases A. Rahim H. Zwayed 1, Brandon Lucke-Wold 2 Zwayed ARH, Lucke-wold B. Conservative management of extradural hematoma:
CASE REPORT Conservative management of extradural hematoma: A report of sixty-two cases A. Rahim H. Zwayed 1, Brandon Lucke-Wold 2 Zwayed ARH, Lucke-wold B. Conservative management of extradural hematoma:
Predicting the need for operation in the patient with an occult traumatic intracranial hematoma
 J Neurosurg 55:75-81, 1981 Predicting the need for operation in the patient with an occult traumatic intracranial hematoma SAM GALBRAITH, M.D., F.R.C.S., AND GRAHAM TEASDALE, M.R.C.P., F.R.C.S. Department
J Neurosurg 55:75-81, 1981 Predicting the need for operation in the patient with an occult traumatic intracranial hematoma SAM GALBRAITH, M.D., F.R.C.S., AND GRAHAM TEASDALE, M.R.C.P., F.R.C.S. Department
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
Neurotrauma: The Place for Cooling
 Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
To date, head injury remains the leading cause of. Outcome in patients with blunt head trauma and a Glasgow Coma Scale score of 3 at presentation
 J Neurosurg 111:683 687, 2009 Outcome in patients with blunt head trauma and a Glasgow Coma Scale score of 3 at presentation Clinical article Ro u k o z B. Ch a m o u n, M.D., Cl a u d i a S. Ro b e r
J Neurosurg 111:683 687, 2009 Outcome in patients with blunt head trauma and a Glasgow Coma Scale score of 3 at presentation Clinical article Ro u k o z B. Ch a m o u n, M.D., Cl a u d i a S. Ro b e r
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Outcome Evaluation of Chronic Subdural Hematoma Using Glasgow Outcome Score
 Outcome Evaluation of Chronic Subdural Hematoma Using Glasgow Outcome Score Mehdi Abouzari, Marjan Asadollahi, Hamideh Aleali Amir-Alam Hospital, Medical Sciences/University of Tehran, Tehran, Iran Introduction
Outcome Evaluation of Chronic Subdural Hematoma Using Glasgow Outcome Score Mehdi Abouzari, Marjan Asadollahi, Hamideh Aleali Amir-Alam Hospital, Medical Sciences/University of Tehran, Tehran, Iran Introduction
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
Index. Note: Page numbers of article titles are in bold face type.
 Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Bone flap preservation in abdominal wall after decompressive craniectomy in head injury: A single institute experience
 DOI: 10.2478/romneu-2018-0063 Article Bone flap preservation in abdominal wall after decompressive craniectomy in head injury: A single institute experience Pavan Kumar, Ashok Kumar, Gaurav Jaiswal, Tarun
DOI: 10.2478/romneu-2018-0063 Article Bone flap preservation in abdominal wall after decompressive craniectomy in head injury: A single institute experience Pavan Kumar, Ashok Kumar, Gaurav Jaiswal, Tarun
Improving TBI outcome
 Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
NEURORADIOLOGY DIL part 3
 NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Correspondence should be addressed to Sorayouth Chumnanvej;
 Neurology Research International Volume 2016, Article ID 2737028, 7 pages http://dx.doi.org/10.1155/2016/2737028 Research Article Assessment and Predicting Factors of Repeated Brain Computed Tomography
Neurology Research International Volume 2016, Article ID 2737028, 7 pages http://dx.doi.org/10.1155/2016/2737028 Research Article Assessment and Predicting Factors of Repeated Brain Computed Tomography
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
INTRACRANIAL ARACHNOID CYSTS: CLASSIFICATION AND MANAGEMENT. G. Tamburrini, Rome
 INTRACRANIAL ARACHNOID CYSTS: CLASSIFICATION AND MANAGEMENT G. Tamburrini, Rome Incidence 2% of occasional neuroradiological findings From clinical studies (1960 s): 0.4-1% of intracranial space occupying
INTRACRANIAL ARACHNOID CYSTS: CLASSIFICATION AND MANAGEMENT G. Tamburrini, Rome Incidence 2% of occasional neuroradiological findings From clinical studies (1960 s): 0.4-1% of intracranial space occupying
CT - Brain Examination
 CT - Brain Examination Submitted by: Felemban 1 CT - Brain Examination The clinical indication of CT brain are: a) Chronic cases (e.g. headache - tumor - abscess) b) ER cases (e.g. trauma - RTA - child
CT - Brain Examination Submitted by: Felemban 1 CT - Brain Examination The clinical indication of CT brain are: a) Chronic cases (e.g. headache - tumor - abscess) b) ER cases (e.g. trauma - RTA - child
secondary effects and sequelae of head trauma.
 Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Trauma is the leading cause of death in the first four decades of life, with head injury being
 Correspondence to: Mr PJ Hutchinson, Academic Department of Neurosurgery, University of Cambridge, Box 167, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK: p.hutch@which.net ACUTE HEAD INJURY FOR THE NEUROLOGIST
Correspondence to: Mr PJ Hutchinson, Academic Department of Neurosurgery, University of Cambridge, Box 167, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK: p.hutch@which.net ACUTE HEAD INJURY FOR THE NEUROLOGIST
Abstract. The first surgeon promoting DC in post traumatic brain swelling was Kocher in 1901 [9].
![Abstract. The first surgeon promoting DC in post traumatic brain swelling was Kocher in 1901 [9].](/thumbs/74/69632405.jpg "Abstract. The first surgeon promoting DC in post traumatic brain swelling was Kocher in 1901 [9].") Med. J. Cairo Univ., Vol. 80, No. 2, March: 143-149, 2012 www.medicaljournalofcairouniversity.com Unilateral Decompressive Craniectomy in Traumatic Brain Injury Patients with Poor Glasgow Coma Scale as
Med. J. Cairo Univ., Vol. 80, No. 2, March: 143-149, 2012 www.medicaljournalofcairouniversity.com Unilateral Decompressive Craniectomy in Traumatic Brain Injury Patients with Poor Glasgow Coma Scale as
The postoperative cranium, normal findings and complications
 The postoperative cranium, normal findings and complications Poster No.: C-1330 Congress: ECR 2013 Type: Authors: Keywords: DOI: Scientific Exhibit P. M. Hernandez Guilabert 1, I. Herrera 2, M. D. P. SANCHEZ-
The postoperative cranium, normal findings and complications Poster No.: C-1330 Congress: ECR 2013 Type: Authors: Keywords: DOI: Scientific Exhibit P. M. Hernandez Guilabert 1, I. Herrera 2, M. D. P. SANCHEZ-
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Where is the contre-coup? Atypical localization of occipital brain contusion
 Romanian Neurosurgery Volume XXXII Number 1 2018 January-March Article Where is the contre-coup? Atypical localization of occipital brain contusion A.I. Cucu, Claudia Florida Costea, R.A. Sascau, B. Dobrovat,
Romanian Neurosurgery Volume XXXII Number 1 2018 January-March Article Where is the contre-coup? Atypical localization of occipital brain contusion A.I. Cucu, Claudia Florida Costea, R.A. Sascau, B. Dobrovat,
Lumbar puncture. Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: ml Replenished: 4-6 h Routine LP (3-5 ml): <1h
: <1h") Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Head Injury: Classification Most Severe to Least Severe
 Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Ruhong Wu, Jia Shi, Jiachao Cao, Yumin Mao and Bo Dong *
 Wu et al. BMC Surgery (2017) 17:123 DOI 10.1186/s12893-017-0303-1 CASE REPORT Open Access Two occurrences of delayed epidural hematoma in different areas following decompressive craniectomy for acute subdural
Wu et al. BMC Surgery (2017) 17:123 DOI 10.1186/s12893-017-0303-1 CASE REPORT Open Access Two occurrences of delayed epidural hematoma in different areas following decompressive craniectomy for acute subdural
ISCHEMIC STROKE IMAGING
 ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
Traumatic brain injury (TBI) is the most disabling
 is the most disabling") J Neurosurg 120:908 918, 2014 AANS, 2014 Patients with brain contusions: predictors of outcome and relationship between radiological and clinical evolution Clinical article Corrado Iaccarino, M.D., 1 Paolo
J Neurosurg 120:908 918, 2014 AANS, 2014 Patients with brain contusions: predictors of outcome and relationship between radiological and clinical evolution Clinical article Corrado Iaccarino, M.D., 1 Paolo
USE OF NEAR INFRARED SPECTROSCOPY TO IDENTIFY TRAUMATIC INTRACRANIAL HEMATOMAS
 JOURNAL OF BIOMEDICAL OPTICS 2(1), 31 41 (JANUARY 1997) USE OF NEAR INFRARED SPECTROSCOPY TO IDENTIFY TRAUMATIC INTRACRANIAL HEMATOMAS Claudia S. Robertson, Shankar P. Gopinath, and Britton Chance* Baylor
JOURNAL OF BIOMEDICAL OPTICS 2(1), 31 41 (JANUARY 1997) USE OF NEAR INFRARED SPECTROSCOPY TO IDENTIFY TRAUMATIC INTRACRANIAL HEMATOMAS Claudia S. Robertson, Shankar P. Gopinath, and Britton Chance* Baylor
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Role of Invasive ICP Monitoring in Patients with Traumatic Brain Injury: An Experience of 98 Cases
 31 Original Article Indian Journal of Neurotrauma (IJNT) 2006, Vol. 3, No. 1, pp. 31-36 Role of Invasive ICP Monitoring in Patients with Traumatic Brain Injury: An Experience of 98 Cases Deepak Kumar Gupta
31 Original Article Indian Journal of Neurotrauma (IJNT) 2006, Vol. 3, No. 1, pp. 31-36 Role of Invasive ICP Monitoring in Patients with Traumatic Brain Injury: An Experience of 98 Cases Deepak Kumar Gupta
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Ventriculostomy and Risk of Upward Herniation in Patients with Obstructive Hydrocephalus from Posterior Fossa Mass Lesions
 https://doi.org/10.1007/s12028-017-0487-3 ORIGINAL ARTICLE Ventriculostomy and Risk of Upward Herniation in Patients with Obstructive Hydrocephalus from Posterior Fossa Mass Lesions Sherri A. Braksick
https://doi.org/10.1007/s12028-017-0487-3 ORIGINAL ARTICLE Ventriculostomy and Risk of Upward Herniation in Patients with Obstructive Hydrocephalus from Posterior Fossa Mass Lesions Sherri A. Braksick
Revisiting the Futility Debate in Neurocritical Care
 Revisiting the Futility Debate in Neurocritical Care Honeybul S* KM Ho** GR Gillett *Department of Neurosurgery, Sir Charles Gairdner Hospital and Royal Perth Hospital, Western Australia; **Department
Revisiting the Futility Debate in Neurocritical Care Honeybul S* KM Ho** GR Gillett *Department of Neurosurgery, Sir Charles Gairdner Hospital and Royal Perth Hospital, Western Australia; **Department
Case Report. Annals of Rehabilitation Medicine INTRODUCTION
 Case Report Ann Rehabil Med 2017;41(1):153-157 pissn: 2234-0645 eissn: 2234-0653 https://doi.org/10.5535/arm.2017.41.1.153 Annals of Rehabilitation Medicine Diagnostic Challenge of Diffusion Tensor Imaging
Case Report Ann Rehabil Med 2017;41(1):153-157 pissn: 2234-0645 eissn: 2234-0653 https://doi.org/10.5535/arm.2017.41.1.153 Annals of Rehabilitation Medicine Diagnostic Challenge of Diffusion Tensor Imaging
Neurosurgery Review. Mudit Sharma, MD May 16 th, 2008
 Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Surgical management of diastatic linear skull fractures in infants
 Surgical management of diastatic linear skull fractures in infants JOHN B. THOMPSON, M.D., THOMAS H. MASON, M.D., GERALD L. HAINES, M.D., AND ROBERT J. CASSIDY, M.D. Divisions of Neurosurgery and Neurology,
Surgical management of diastatic linear skull fractures in infants JOHN B. THOMPSON, M.D., THOMAS H. MASON, M.D., GERALD L. HAINES, M.D., AND ROBERT J. CASSIDY, M.D. Divisions of Neurosurgery and Neurology,
What is elevated ICP?
 What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Management of pediatric brain tumors, strategies and long term outcome
 Management of pediatric brain tumors, strategies and long term outcome SAN The Sudanese association of neurosurgeons By Dr. Abubakr Darrag Salim Ahmed Dr. Mohammed Awad Elzain Khartoum Sudan Pediatric
Management of pediatric brain tumors, strategies and long term outcome SAN The Sudanese association of neurosurgeons By Dr. Abubakr Darrag Salim Ahmed Dr. Mohammed Awad Elzain Khartoum Sudan Pediatric
HHS Public Access Author manuscript Neurocrit Care. Author manuscript; available in PMC 2017 February 01.
 Derivation of a Predictive Score for Hemorrhagic Progression of Cerebral Contusions in Moderate and Severe Traumatic Brain Injury Randall Z. Allison 1, Kazuma Nakagawa 2,3, Michael Hayashi 4,5, Daniel
Derivation of a Predictive Score for Hemorrhagic Progression of Cerebral Contusions in Moderate and Severe Traumatic Brain Injury Randall Z. Allison 1, Kazuma Nakagawa 2,3, Michael Hayashi 4,5, Daniel
Neurosurgery (Orthopaedic PGY-1) Goals. Objectives
 Goals. Objectives") Neurosurgery (Orthopaedic PGY-1) Length: 1 month of PGY-1 (Orthopaedic Designated Residents) or 1 month of PGY-2, -3, or -4 year Location: The Queen's Medical Center Primary Supervisor: William Obana,
Neurosurgery (Orthopaedic PGY-1) Length: 1 month of PGY-1 (Orthopaedic Designated Residents) or 1 month of PGY-2, -3, or -4 year Location: The Queen's Medical Center Primary Supervisor: William Obana,
Changing Demographics in Death After Devastating Brain Injury
 Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary