Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
|
|
|
- Emmeline Barrett
- 6 years ago
- Views:
Transcription
1 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Diaz MD.
2 Introduction: Severe traumatic brain injury (TBI) is one of the major causes of death in younger age groups in the world. The incidence of head trauma in United State of America is 1.4 million / year, are admitted and die from head injury. In Cuba traffic accidents are the fourth cause of death in adults and, the commonest cause in those under the 45 years old. Fifty percent of those suffering from traffic accident sustain a head injury.
3 The control of elevated intracranial pressure (ICP), is fundamental to the management of patients with severe head injury. Approximately 40% of patients suffering traumatic loss of consciousness will develop intracranial hypertension during the course of their treatment. Brain edema, increased ICP and reduced cerebral blood flow, are the main prognostic factors despite progress in the diagnosis and treatment of severe post-traumatic brain injury.
4 There is today enough evidence that the implementation of protocols to standardize therapy in patients with post-traumatic intracranial hypertension have, resulted in an improvement in neurological outcome. The steps of protocol driven include, medical measures such as maintaining blood pressure and oxygenation, prophylactic hypothermia, using anaesthetics, analgesics and sedatives, drainage of cerebrospinal fluid (CSF) by ventriculostomy, mild hyperventilation, administering mannitol, hypertonic saline and barbiturates.
5 Decompressive craniectomy (DC), is considered to be one of the second tier therapies in posttraumatic medically refractory intracranial hypertension. It is a kind of the urgent neurosurgical cerebral rescue procedures, to increase the volume of the cranial cavity and decrease the secondary damage in patients with severe traumatic brain injury.

6 The literature published to date does not reveal a definitive evidence regarding the effectiveness and indications of DC. In this article we present our analysis of the clinical data from a non-randomized control trial using early decompressive craniectomy in patients with severe head injuries with intracranial hypertension. Moron General Hospital
7 Objectives: The aims of this investigation were to know the effectiveness of early decompressive craniectomy in patients with severe head injury associated with refractory intracranial hypertension using this procedure as the initial second tier surgical therapy; also to describe CT findings and the effects over ICP, CPP, compliance, hemodynamic and other intracranial parameters in this kind of patients. This study was carried out to examine with particular attention the relation between early decompressive craniectomy to long-term functional outcome.
8 Methods: We have conducted a non-randomized controlled trial, in 68 patients admitted at intensive care unit of Moron General Hospital in Ciego de Avila, Cuba, with severe head injury (Glasgow coma scale (GCS) < 8), in the period between January 2003 and December Initial computarized tomography (CT) scans were obtained from all patients on admission; they were classified according to Marshall s system. Sequentials CT scan were indicated to assess neurological deterioration in the ICU patients or every 72 hours.
9 According to initial CT scan results, the time span between admission and starting intracranial hypertension and the treatment modality, the patients were distributed in two groups. Group I (Early DC): Included patients with diffuse injury IV (midline shift > 5 mm, not high or mixed density lesion > 25 cc) or non-evacuated mass lesion (high or mixed density lesion > 25 cc not surgically evacuated). DC was performed in the first 12 hours post-trauma in patients with clinical, radiological and by continuous ICP monitoring evidence of refractory intracranial hypertension (ICP> 25 mmhg) as the first second tier therapy. DC was performed without ICP monitoring only in patients who require urgent surgery.
10 Group II (Conventional treatment): Included patients with diffuse injury I - III, whom were admitted in intensive care unit to continuous ICP monitoring and medical treatment, showing clinical deterioration, worsening of GCS score and/or dilation of pupils unresponsive to light, with intracranial hypertension to more than 25 mmhg and or reduction of cerebral perfusion pressure to less than 55 mmhg longer than 12 hours after head trauma. If sequential CT scan showed worsening of images with appearance of diffuse injury IV or high/mixed density lesions > 25 cc and refractory intracranial hypertension appeared, surgical treatment was needed at this moment and it was considered as delayed DC.

11 Patients with CT scan imaging demonstration of severe brainstem injury, with initial GCS of 3, without improvement and bilateral dilated and fixed pupils were excluded. Moron s train station
12 Surgical Technique: The surgical procedure included a large unilateral or bilateral curvilinear incision in the fronto-temporalparietal (F-T-P) area or a large bifrontal skin incision. After preparation of a myocutaneous flap, a craniectomy with a free F-T-P bone flap is performed (>12 cms), with expansive duroplasty starting at the temporal base. In bilateral frontal-temporal-parietal DC, only a rim of bone remains on the sagittal suture to avoid ligating the sagittal sinus.
13 The extension of bifrontal DC with expansive duroplasty was from the floor of the anterior cranial base to the coronal suture posteriorly, and to the pterion laterally. A bridge of bone in the midline can be left over the superior sagittal sinus. We advocate to avoid the frontal air sinus an sagittal sinus. In both procedures the dura is enlarged with temporal fascia followed by watertight closure and the bone flap was preserved in anterior abdominal wall.

14 Bifrontal decompressive craniectomy with bone flap prepared to keep out in anterior abdominal wall.


15 Hydrocephalus after decompressive craniectomy. VP CSF shunt

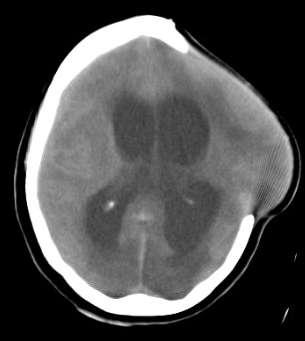
16 Petient with 58 years old, He was received in the emergency room 1 hour after head trauma, 7 points in GCS, initial CT scan is showed below. He was taken to operating room and ICP was monitored by external ventriculostomy showing values over 25 mmhg after manitol bolus administration. A bifrontal decompressive craniectomy was performed. Initial CT Scan

17 Intraoperative images

18 A 30 year old patient operated on with intracranial hypertension after initial unenough decompressive FTP hemicraniectomy
19 ICP monitoring: The ICP monitoring was performed by external strain gauge pressure transduction technology. External strain gauge transducer was coupled to the patient s lateral ventriculostomy, where the catheter tip transducer was placed, via fluid-filled lines. The external transducer was maintained fixed at the ventricular level to avoid measurement error. The duration of ICP monitoring was 5 days on average and all patients received prophylactic antibiotics.
20 Standardized protocol for medical therapy: Medical management of intracranial hypertension included the following measures: elevation of the head 20º, hemodynamic stabilization, sedation with analgesics and sedative, CSF drainage, intravenous administration of manitol in intermittent boluses (0,25g / kg / dosis / 4 hours), controlled mild hyperventilation (PaCO2: mmhg) and muscle relaxation if indicated. Barbiturate medication was not used.
21 Data collection: The following patient data were prospectively collected: date of the accident, mechanism of injury, age of the patient, neurological status at admission (GCS score), pupillary response, initial and sequential CT scan results, data of medical ICP therapy, surgical procedures and complications. Outcome was scored using the Glasgow Outcome Scale (GOS). A GOS score of good recovery (grade 5) and with moderate disability (grade 4) was considered to be a satisfactory outcome. A GOS score with severe disability (grade III), vegetative state (grade II) or dead (grade I), was considered to be unsatisfactory outcome.
22 Statistical analysis: A data base was created using SPSS system, version The Chi-Square test was used to tabulates the variables into categories and compares the observed and expected frequencies in each category. p-value of less than 0.05 was deemed significant. The bivariate Pearson s correlation coefficient, was used to measure how variables were related in linear association with GOS.

23
24 Group I Group II Age distribution >60 21,74% ,39% ,07% ,78% 8 >60 13,33% ,11% ,33% ,22%
25 Group I Group II Mean time of patients arrival to Emergency Room after head trauma 7-12hs 13,04% 3 4-6h 34,78% 8 0-3h 52,17% hs 2 4,44% 4-6h 51,11% h 44,44%
26 Group I Group II Initial Glasgow Coma Scale. 5-4 points 13,04% points 43,48% 10 8 points 43,48% points 26,67% points 46,67% 21 8 points 26,67%
27 Group I Group II Relation between initial GCS and Outcome. 5-4 points 100% points 20% 2 80% 8 8 points 30% 3 70% 7 Unsatisfactory 5-4 points 25% 3 75% 9 Satisfactory 7-6 points 38,10% 8 61,90% 13 8 points 1 8,33% 91,67%
28 Group I Group II Initial CT classification of severe head injury. Non evacuated mass lesion 69,57% 16 Diffuse injury IV 3 13,04% Diffuse injury III 17,39% 4 Non evacuated mass lesion 64,44% 29 Diffuse injury IV 24,44% 11 Diffuse injury III 11,11%
29 Group I Group II Presence of midline shift deviation on initial CT scan mm 69,57% mm 30,43% 7 > 10 mm 17,78% mm 71,11% mm 11,11%
30 Group I Group II Relation between midline shift deviation and ICP (in patients monitoring before operation) mm 37,5% 62,5% mm 100% 7 > 25 mmhg 6-10 mm 27,27% 3 72,73% mmhg 1-5 mm 20% 1 80%
31 Group I Group II Sequential CT scan. Worst 21,74% 5 Non modified 56,52% 13 Better 21,74% 5 Worst 20% 9 Non modified 20% 9 Better 60%
32 Relation between initial CT scan and sequential CT scan. Sequential CT scan Initial CT scan Group I Group II Better Non modified Worst Better Non modified Worst Diffuse injury III 4 (8,89%) 1 (2,22%) - 1 (4,35%) 3 (13,04%) - Diffuse iinjury IV 9 * (20%) 1 (2,22%) 1 (2,22%) 1 (4,35%) 2 (8,70%) - Non evacuated mass lession 14 (31,11%) 7 (15,56%) 8 (17,78%) 3 (13,04%) 8 (34,78%) 5 (21,74%) Total 27 * (60%) 9 (20%) 9 (20%) 5 (21,74%) 13 (56,52%) 5 (21,74%)
33 Group I Group II Relation between sequential CT scan and Outcome. Worst 100% 5 Non modified 76,92% 23,06% 3 10 Better 1 80% 20% 4 Unsatisfactory Worst 55,56% 44,44% 4 5 Satisfactory Non modified 66,67% ,33% Better 25,93% 7 74,07%
34 Group I Group II ICP at first 24 hours of treatment. >25mmHg 26,09% mmHg 43,48% 10 <20mmHg 30,43% 7 >25mmHg 15,56% mmHg 33,33% 15 <20mmHg 51,11%
35 Group I Group II ICP between 2nd-5th days of treatment. >25mmHg 21,74% mmHg 26,09% 6 <20mmHg 52,17% 12 >25mmHg 13,33% mmHg 13,33% 6 <20mmHg 73,34%
36 Group I Group II Relation between mean ICP and Outcome. >25mmHg 100% mmHg <20mmHg 75% 2 55,56% 25% ,44% Unsatisfactory >25mmHg 100% 6 Satisfactory 20-25mmHg ,67% 33,33% <20mmHg 24,24% 8 75,76%
37 Group I Group II Compliance behavior. <15 ml 38,46% ml 2 15,38% N=13 >20 ml 43,15% 6 <15 ml 10,71% ml 17,86% 5 N=28 >20 ml 71,43%
38 Group I Group II Relation between compliance behavior and outcome. <15 ml 60% 40% ml 100% 2 >20 ml 50% 50% 3 Unsatisfactory <15 ml 100% 3 Satisfactory ml 100% 5 >20 ml 10% 2 90%
39 Group I Group II Treatment for intracranial hypertension. Delayed decompressive craniectomy 43.48% 10 Mild hyperventilation % CSF drainage,manitol and muscle relaxant % CSF drainage and manitol % CSF drainage % Non treatment 71.11% 32 Mild hyperventilation 13.33% 6 CSF drainage,manitol and muscle relaxant % CSF drainage and manitol % CSF drainage %
40 Group I Group II Cerebral Perfusion Pressure (CPP) mmhg 34.79% 8 < 60 mmhg 65.21% 15 > 70 mmhg % mmhg 75.56% 34 < 60 mmhg 17.78%
41 Group I Group II Relation between CPP and Outcome mmhg % 37.5% 5 < 60 mmhg % 13.33% 13 > 70 mmhg % 66.67% Unsatisfactory Satisfactory mmhg 29.41% % 24 < 60 mmhg % 12.5%
42 Group I Group II Cerebral Hemodynamic. Normohemic 43.48% 10 Hyperhemic % Ischemic 52.17% 12 Normohemic 75.56% 34 Hyperhemic % Ischemic 17.78%
43 Group I Group II Relation between Cerebral Hemodynamic and Outcome. Normohemic 30% 3 70% 7 Hyperhemic 1 100% Ischemic 100% 12 Unsatisfactory Normohemic 38,24% 61,76% Satisfactory Hyperhemic ,33% 66,67% Ischemic 50% 50%
44 Neurosurgicals Generals Complications. Systemic Hypotension 5 14 Fluid, electrolyte and acid-basic disbalances 86,96% Pneumonia 16 88,44% 38 CSF fistulae 2 Group II Non enough craniectomy 5 Group I Skin flap infection 6 Hydrocephalus Intracranial hypertension 5 65,22% 26,67%
45 Group I Group II Glasgow Outcome Scale. Mild disability 2 8,70% Moderate disability 21,74% 5 Severe disability 34,78% 8 Persistent vegetative state Dead 34,78% 8 Mild disability 13,33% 6 Moderate disability 46,67% 21 Severe disability 15,56% 7 Persistent vegetative state 2 4,44% Dead 20%
46 General Outcome. Group II 30,43% 69,57% 7 16 Unsatisfactory Satisfactory Group I 40% 60%
47 Comparison between early and delayed decompressive craniectomy. Mild disability 1 13,33% 10% 6 Moderate disability Severe disability Persistent Vegetative State % 15,56% 30% 46,67% 7 4,44% 21 Delayed decompressive craniectomy (Group II) Early decompressive craniectomy (Group I) Dead 50% 5 20%

48 Severe head injury mortality in Moron General Hospital.
49 Conclusion: 1. Our results seem to support that decompressive craniectomy may be an effective way to reduce intractable raised intracranial pressure, and probably to improve patients outcome. 2. A linear relationship exists between characteristics of initial CT scan and ICP level monitoring in the first 24 hours. 3. There was correlation between CPP values over 60 mmhg and good results. 4. A high number of patients with early DC (Group I) didn t need other medical therapy to control intracranial pressure.


50 5. The majority of survivors after decompressive craniectomy have a good functional outcome. 6. Complications related to surgical decompression not affect the benefits of decompressive craniec tomy.
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD.
 Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Supplementary Online Content
 Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Decompressive craniectomy following traumatic brain injury
 Decompressive craniectomy following traumatic brain injury Peter Hutchinson Division of Academic Neurosurgery University of Cambridge Escalating cycle of brain swelling Primary insult Brain swelling Secondary
Decompressive craniectomy following traumatic brain injury Peter Hutchinson Division of Academic Neurosurgery University of Cambridge Escalating cycle of brain swelling Primary insult Brain swelling Secondary
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer
 Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Chapter 8: Cerebral protection Stephen Lo
 Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
Brain under pressure Managing ICP. Giuseppe
 Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Update sulle lesioni emorragiche posttraumatiche
 Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
To date, head injury remains the leading cause of. Outcome in patients with blunt head trauma and a Glasgow Coma Scale score of 3 at presentation
 J Neurosurg 111:683 687, 2009 Outcome in patients with blunt head trauma and a Glasgow Coma Scale score of 3 at presentation Clinical article Ro u k o z B. Ch a m o u n, M.D., Cl a u d i a S. Ro b e r
J Neurosurg 111:683 687, 2009 Outcome in patients with blunt head trauma and a Glasgow Coma Scale score of 3 at presentation Clinical article Ro u k o z B. Ch a m o u n, M.D., Cl a u d i a S. Ro b e r
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
THREE HUNDRED AND ten TBI patients with a
 Acute Medicine & Surgery 2014; 1: 31 36 doi: 10.1002/ams2.5 Original Article Outcome prediction model for severe traumatic brain injury Jiro Iba, 1 Osamu Tasaki, 2 Tomohito Hirao, 2 Tomoyoshi Mohri, 3
Acute Medicine & Surgery 2014; 1: 31 36 doi: 10.1002/ams2.5 Original Article Outcome prediction model for severe traumatic brain injury Jiro Iba, 1 Osamu Tasaki, 2 Tomohito Hirao, 2 Tomoyoshi Mohri, 3
Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature
 Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature Anand Sharma 1, Arti Sharma 2, Yashbir Dewan 1 1 Artemis
Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature Anand Sharma 1, Arti Sharma 2, Yashbir Dewan 1 1 Artemis
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
Evaluation & Management of Elevated Intracranial Pressure in Adults. Dr. Tawfiq Almezeiny
 Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary Hospital of South India
 International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio
 Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Changing Demographics in Death After Devastating Brain Injury
 Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
UAMS MEDICAL CENTER TRAUMA and CRITICAL CARE SERVICES MANUAL. SUPERSEDES: New PAGE: 1 of 5. RECOMMENDATION(S): Drs. Bill Beck/J.R.
: Drs. Bill Beck/J.R.") SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without
SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Medicines Protocol HYPERTONIC SALINE 5%
 Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
Role of Invasive ICP Monitoring in Patients with Traumatic Brain Injury: An Experience of 98 Cases
 31 Original Article Indian Journal of Neurotrauma (IJNT) 2006, Vol. 3, No. 1, pp. 31-36 Role of Invasive ICP Monitoring in Patients with Traumatic Brain Injury: An Experience of 98 Cases Deepak Kumar Gupta
31 Original Article Indian Journal of Neurotrauma (IJNT) 2006, Vol. 3, No. 1, pp. 31-36 Role of Invasive ICP Monitoring in Patients with Traumatic Brain Injury: An Experience of 98 Cases Deepak Kumar Gupta
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN
 Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience
 80 Original Article THIEME Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience V. Velho 1 Hrushikesh U. Kharosekar 1 Jasmeet S. Thukral 1 Shonali Valsangkar
80 Original Article THIEME Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience V. Velho 1 Hrushikesh U. Kharosekar 1 Jasmeet S. Thukral 1 Shonali Valsangkar
11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome?
 11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome? Critical levels of CPP, ICP and PRx Percentage of patients in outcome
11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome? Critical levels of CPP, ICP and PRx Percentage of patients in outcome
Only 30% to 40% of acute subdural hematoma (SDH)
") Contralateral Acute Epidural Hematoma After Decompressive Surgery of Acute Subdural Hematoma: Clinical Features and Outcome Thung-Ming Su, MD, Tsung-Han Lee, MD, Wu-Fu Chen, MD, Tao-Chen Lee, MD, and Ching-Hsiao
Contralateral Acute Epidural Hematoma After Decompressive Surgery of Acute Subdural Hematoma: Clinical Features and Outcome Thung-Ming Su, MD, Tsung-Han Lee, MD, Wu-Fu Chen, MD, Tao-Chen Lee, MD, and Ching-Hsiao
Outcome Evaluation of Chronic Subdural Hematoma Using Glasgow Outcome Score
 Outcome Evaluation of Chronic Subdural Hematoma Using Glasgow Outcome Score Mehdi Abouzari, Marjan Asadollahi, Hamideh Aleali Amir-Alam Hospital, Medical Sciences/University of Tehran, Tehran, Iran Introduction
Outcome Evaluation of Chronic Subdural Hematoma Using Glasgow Outcome Score Mehdi Abouzari, Marjan Asadollahi, Hamideh Aleali Amir-Alam Hospital, Medical Sciences/University of Tehran, Tehran, Iran Introduction
CEREBRAL DECONGESTANTS. Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS
 CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Traumatic Brain Injury Pathways for Adult ED Patients Being Admitted to Trauma Service
 tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
Surgical Management & Clinical Outcome of Severe Brain Trauma due to Acute Subdural Hematoma.
 International Journal of Sciences: Basic and Applied Research (IJSBAR) ISSN 2307-4531 (Print & Online) http://gssrr.org/index.php?journal=journalofbasicandapplied ----------------------------------------------------------------------------------------------------------------
International Journal of Sciences: Basic and Applied Research (IJSBAR) ISSN 2307-4531 (Print & Online) http://gssrr.org/index.php?journal=journalofbasicandapplied ----------------------------------------------------------------------------------------------------------------
Comparison of Burr Holes and Decompressive Craniotomy in the Surgical Treatment of Traumatic Acute Subdural Hematoma
 Med. J. Cairo Univ., Vol. 83, No. 1, March: 259-266, 2015 www.medicaljournalofcairouniversity.net Comparison of Burr Holes and Decompressive Craniotomy in the Surgical Treatment of Traumatic Acute Subdural
Med. J. Cairo Univ., Vol. 83, No. 1, March: 259-266, 2015 www.medicaljournalofcairouniversity.net Comparison of Burr Holes and Decompressive Craniotomy in the Surgical Treatment of Traumatic Acute Subdural
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Predicting the need for operation in the patient with an occult traumatic intracranial hematoma
 J Neurosurg 55:75-81, 1981 Predicting the need for operation in the patient with an occult traumatic intracranial hematoma SAM GALBRAITH, M.D., F.R.C.S., AND GRAHAM TEASDALE, M.R.C.P., F.R.C.S. Department
J Neurosurg 55:75-81, 1981 Predicting the need for operation in the patient with an occult traumatic intracranial hematoma SAM GALBRAITH, M.D., F.R.C.S., AND GRAHAM TEASDALE, M.R.C.P., F.R.C.S. Department
11 th Annual Cerebrovascular Symposium 5/11-12/2017. Hypertonic Use D E R E K C L A R K
 Hypertonic Use D E R E K C L A R K 1 Outline Types of hyperosmolar therapy Review Cerebral Na Physiology Differences between periphery and BBB Acute phase Subacute phase Chronic changes Hypertonic Saline
Hypertonic Use D E R E K C L A R K 1 Outline Types of hyperosmolar therapy Review Cerebral Na Physiology Differences between periphery and BBB Acute phase Subacute phase Chronic changes Hypertonic Saline
Recent trends in the management of head injury
 Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Efficacy of neuroendoscopic evacuation of traumatic intracerebral or intracerebellar hematoma
 Original Contribution Kitasato Med J 2017; 47: 141-147 Efficacy of neuroendoscopic evacuation of traumatic intracerebral or intracerebellar hematoma Hiroyuki Koizumi, 1,2 Daisuke Yamamoto, 1 Yasushi Asari,
Original Contribution Kitasato Med J 2017; 47: 141-147 Efficacy of neuroendoscopic evacuation of traumatic intracerebral or intracerebellar hematoma Hiroyuki Koizumi, 1,2 Daisuke Yamamoto, 1 Yasushi Asari,
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
ecompressive craniectomy in TBI
 ecompressive craniectomy in TBI Andras Buki M.D., Ph.D.,D.Sc. Department of Neurosurgery, Medical Faculty of Pecs University, Pecs, Hungary, H-7624 AZ ÉLETTUDOMÁNYI- KLINIKAI FELSŐOKTATÁS GYAKORLATORIENTÁLT
ecompressive craniectomy in TBI Andras Buki M.D., Ph.D.,D.Sc. Department of Neurosurgery, Medical Faculty of Pecs University, Pecs, Hungary, H-7624 AZ ÉLETTUDOMÁNYI- KLINIKAI FELSŐOKTATÁS GYAKORLATORIENTÁLT
Original Article CT grouping and microsurgical treatment strategies of hypertensive cerebellar hemorrhage
 Int J Clin Exp Med 2016;9(8):15921-15927 www.ijcem.com /ISSN:1940-5901/IJCEM0022273 Original Article CT grouping and microsurgical treatment strategies of hypertensive cerebellar hemorrhage Xielin Tang
Int J Clin Exp Med 2016;9(8):15921-15927 www.ijcem.com /ISSN:1940-5901/IJCEM0022273 Original Article CT grouping and microsurgical treatment strategies of hypertensive cerebellar hemorrhage Xielin Tang
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury
 Pragmatic Evidence-based Review Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury Reviewer Mark Ayson MBChB DPH Date Report Completed August 2011 Important Note: It is not
Pragmatic Evidence-based Review Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury Reviewer Mark Ayson MBChB DPH Date Report Completed August 2011 Important Note: It is not
Index. Note: Page numbers of article titles are in bold face type.
 Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Traumatic Brain Injury Pathway, GCS 15 Closed head injury
 Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Two-Stage Management of Mega Occipito Encephalocele
 Two-Stage Management of Mega Occipito Encephalocele CASE REPORT A I Mardzuki*, J Abdullah**, G Ghazaime*, A R Ariff!'*, M Ghazali* *Department of Neurosciences, **Department of Radiology, Hospital Universiti
Two-Stage Management of Mega Occipito Encephalocele CASE REPORT A I Mardzuki*, J Abdullah**, G Ghazaime*, A R Ariff!'*, M Ghazali* *Department of Neurosciences, **Department of Radiology, Hospital Universiti
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
Extradural hematoma (EDH) accounts for 2% of all head injuries (1). In
 accounts for 2% of all head injuries (1). In") CASE REPORT Conservative management of extradural hematoma: A report of sixty-two cases A. Rahim H. Zwayed 1, Brandon Lucke-Wold 2 Zwayed ARH, Lucke-wold B. Conservative management of extradural hematoma:
CASE REPORT Conservative management of extradural hematoma: A report of sixty-two cases A. Rahim H. Zwayed 1, Brandon Lucke-Wold 2 Zwayed ARH, Lucke-wold B. Conservative management of extradural hematoma:
excellence in care Procedure Neuroprotection For Review Aug 2015
 Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Anesthetic Management of a Patient with Traumatic Brain Injury
 Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
Paediatric Neurosurgical Emergencies. Kate Parkins Consultant Paediatric Intensivist Alder Hey
 Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report
 214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
Pediatric Trauma Initial Evaluation and management
 Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Management of head injury in the intensive-care unit
 Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality
 Original articles Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality J. A. MYBURGH*, S. B. LEWIS *Intensive Care Unit, Royal Adelaide Hospital, Adelaide, SOUTH
Original articles Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality J. A. MYBURGH*, S. B. LEWIS *Intensive Care Unit, Royal Adelaide Hospital, Adelaide, SOUTH
Correspondence should be addressed to Sorayouth Chumnanvej;
 Neurology Research International Volume 2016, Article ID 2737028, 7 pages http://dx.doi.org/10.1155/2016/2737028 Research Article Assessment and Predicting Factors of Repeated Brain Computed Tomography
Neurology Research International Volume 2016, Article ID 2737028, 7 pages http://dx.doi.org/10.1155/2016/2737028 Research Article Assessment and Predicting Factors of Repeated Brain Computed Tomography
L'Ecografia del nervo ottico nel monitoraggio della PIC nel traumatizzato cranico
 Roma 25 Maggio 2018 L'Ecografia del nervo ottico nel monitoraggio della PIC nel traumatizzato cranico behind the cotton wool of papilledema Dott. Elena Casiello Scuola di Specializzazione in Anestesia
Roma 25 Maggio 2018 L'Ecografia del nervo ottico nel monitoraggio della PIC nel traumatizzato cranico behind the cotton wool of papilledema Dott. Elena Casiello Scuola di Specializzazione in Anestesia
Sign up to receive ATOTW weekly
 MANAGEMENT OF PAEDIATRIC TRAUMATIC BRAIN INJURY ANAESTHESIA TUTORIAL OF THE WEEK 127 30 TH MARCH 2009 Kavitha Raghavan, King s College Hospital, London Richard Waddington, Kingston Hospital, Surrey Correspondence
MANAGEMENT OF PAEDIATRIC TRAUMATIC BRAIN INJURY ANAESTHESIA TUTORIAL OF THE WEEK 127 30 TH MARCH 2009 Kavitha Raghavan, King s College Hospital, London Richard Waddington, Kingston Hospital, Surrey Correspondence
Decompressive Hemicraniectomy in Acute Neurological Diseases
 Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins
 ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
Retired Brigadier of the Croatian Army (HV), War Commander of the Surgical Team of the Croatian Ministry of Internal Affairs (MUP) Special Police 2
, War Commander of the Surgical Team of the Croatian Ministry of Internal Affairs (MUP) Special Police 2") Acta Chir Croat 0; 9: 9-5 Ozljede glave Running head: Head injuries Josip Husar, Israel Oserohwovo Introduction The prognosis of brain injuries is good in patients who respond to simple commands, are not
Acta Chir Croat 0; 9: 9-5 Ozljede glave Running head: Head injuries Josip Husar, Israel Oserohwovo Introduction The prognosis of brain injuries is good in patients who respond to simple commands, are not
Pediatric Head Injury:
 Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
ESCMID Online Lecture Library. by author
 Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Cerebral Blood Flow and Metabolism during Mild Hypothermia in Patients with Severe Traumatic Brain Injury
 J Med Dent Sci 2010; 57: 133-138 Original Article Cerebral Blood Flow and Metabolism during Mild Hypothermia in Patients with Severe Traumatic Brain Injury Hiroyuki Masaoka Department of Neurosurgery,
J Med Dent Sci 2010; 57: 133-138 Original Article Cerebral Blood Flow and Metabolism during Mild Hypothermia in Patients with Severe Traumatic Brain Injury Hiroyuki Masaoka Department of Neurosurgery,
Improving TBI outcome
 Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
The Lund Concept in 1999
 The Lund Concept in 1999 Carl-Henrik Nordström, M.D., Ph.D. Department of Neurosurgery Lund University Hospital S-221 85 Lund Sweden A new therapeutic approach to reduce increased ICP, denoted the Lund
The Lund Concept in 1999 Carl-Henrik Nordström, M.D., Ph.D. Department of Neurosurgery Lund University Hospital S-221 85 Lund Sweden A new therapeutic approach to reduce increased ICP, denoted the Lund
1st Turku Traumatic Brain Injury Symposium Turku, Finland, January 2014
 The TBIcare decision support tool aid for the clinician Jyrki Lötjönen & Jussi Mattila, VTT Technical Research Centre of Finland Validation of the decision support tool Ari Katila University of Turku 1st
The TBIcare decision support tool aid for the clinician Jyrki Lötjönen & Jussi Mattila, VTT Technical Research Centre of Finland Validation of the decision support tool Ari Katila University of Turku 1st
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Management of Traumatic Brain Injury. Olaide O. Ajayi, MD
 Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
Protocol for emergency surgical intervention in patients with a brain tumour v3
 Protocol for emergency surgical intervention in patients with a brain tumour v3 West Midlands Cancer Alliance Coversheet for Cancer Alliance Expert Advisory Group Agreed Documentation This sheet is to
Protocol for emergency surgical intervention in patients with a brain tumour v3 West Midlands Cancer Alliance Coversheet for Cancer Alliance Expert Advisory Group Agreed Documentation This sheet is to