Comorbidities and Complications of TBI. Rocco A Chiappini, MD
|
|
|
- Nancy Horn
- 6 years ago
- Views:
Transcription
1 Comorbidities and Complications of TBI Rocco A Chiappini, MD
2 TBI: A Disease Process, Not an Event WHO definition of a chronic disease Permanent Caused by non-reversible pathological alterations Requires special training of patient May require a long period of observation, supervision or care
3 Masel and DeWitt, J Neurotrauma 2010 TBI increases long term mortality and decreases life expectancy. It is associated with increased incidence of seizures, sleep disorders, neurodegenerative disease, neuroendocrine dysregulation and psychiatric diseases as well as nonneurologic disorders such as sexual dysfunction, bladder and bowel
4 Masel and Dewitt J Neurotrauma 2010 incontinence and systemic metabolic dysregulation that may arise and/or persist for months or years after injury.
5 TBI Complications and Comorbidities Seizures Sleep disturbance Fatigue Infections Craniectomy Hydrocephalus Shunt issues
6 TBI Complications and Comorbidities Subdural/Epidural Hematoma Neuro-endocrine dysfunction Spasticity Post-traumatic headache
7 Seizures TBI is the leading cause of epilepsy in young adults Early seizures- within the first week Late seizures- after the first week Incidence of late seizures Nonpenetrating severe TBI 17% Penetrating TBI 35-65%

8 Seizures- risk factors Depressed skull fracture Bone/metal fragments Focal contusions Intracranial hemorrhage

9 Gunshot wound
10 Types of Seizures Partial 25% Generalized 25% Partial with secondary generalization 50%
11 Frontal Lobe Epilepsy Complex, semipurposeful motor automatisms
12 Temporal Lobe Epilepsy May have emotional symptoms like panic followed by post-ictal confusion or amnesia
13 Seizures Current Recommendations Prophylaxis for the first week Discontinue prophylaxis and monitor Treat late seizures with carbamazepine, valproate, lamotrigine or levetiracetam Avoid phenytoin
14 Sleep Disorders Guilleminault studied 184 TBI survivors Restless sleep 49% Regular loud snoring 36% Leg and body jerking during sleep 18%
15 Sleep Disorders Ouellet studied 452 TBI survivors (avg time since injury 8 years) 50% had symptoms of insomnia 30% met criteria for insomnia (general public 10%)
16 Sleep disorders TBI population Decreased REM Decreased total sleep time More frequent awakenings Decreased deep sleep stages
17 Sleep Disorders Causes Damage to brain centers involved in sleep (hypothalamus, midbrain, ascending reticular activating system) Disruption of circadian pacemaker in the hypothalamus with decrease in level of melatonin production
18 Pain Depression Anxiety Medications Environment Sleep Disorders Causes
19 Sleep Disorders Treatment Treat depression, anxiety, pain Treat sleep apnea if present Improve sleep hygiene Melatonin Hypnotics, TCAs, antiepileptics may be helpful although no studies have shown best pharmacotherapy for insomnia in TBI
20 Fatigue The awareness of a decreased capacity for physical and/or mental activity due to an imbalance in the availability, utilization and/or restoration of resources needed to perform activity.
21 Fatigue Physiologic- arises from depletion of energy, hormones, neurotransmitters, or neural connections Psychologic- weariness related to reduced motivation, prolonged mental activity or boredom
22 Fatigue Kreutzer found 46% of 722 outpatients with TBI self reported fatigue
23 Fatigue May result from diffuse neuronal injury, particularly from damage to brain centers that control arousal, attention and response speed including the ARAS, limbic system, anterior cingulate, basal ganglia Alteration in chemistry. Histamine and growth factor.
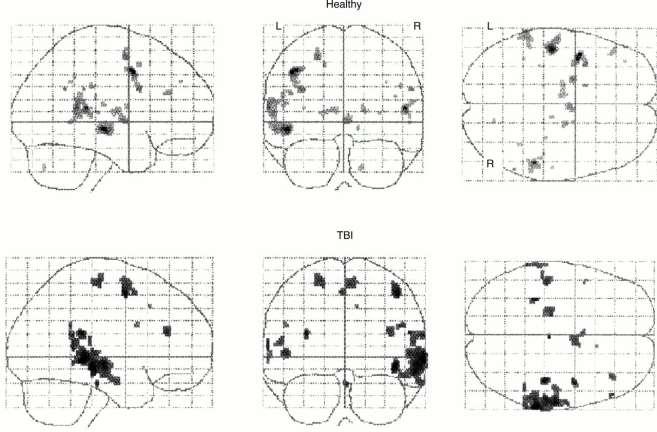
24 Fatigue
25 Exercise Sleep assessment Hormonal screening Light therapy Fatigue Treatments Assessment of meds. D/C meds that increase fatigue Try antidepressants with activating effect Modafinil

26 Infections Meningitis Headache, fever, stiff neck, confusion

27 Infections Subdural empyema Usually due to septic skull fracture Acute presentation with fever, headache, obtundation
28 Infections Brain abscess 3 times more likely with gunshot wound Usually 2-3 weeks post injury Headache, vomiting, change in mental status 50%, seizure 33%

29 Craniectomy Syndrome of the trephined Deficits that may improve with cranioplasty Headaches, apathy, hemiparesis, tremor, gait, cognitive dysfunction

30 Trephination
31 Hydrocephalus Occurs in about 40% of patients with severe TBI Usually begins to appear within the first 2 weeks post injury

32 Hydrocephalus Communicating Different portions of the ventricular system are interconnected and fluid may exit the ventricular system freely to the cisterns and subarachnoid space

33 Hydrocephalus Non-communicating (obstructive) CSF flow is obstructed either between the ventricles or in exiting the ventricular system Due to cerebral edema, blood or infection which interferes with CSF flow May present with nausea, vomiting and lethargy
34 Shunting Study of 356 adults with VP shunts over 18 years. Incidence of revision 30%. Shunt failure Shunt infection Overdrainage
35 VP Shunt
36 Shunt failure Proximal occlusion of the ventricular catheter is the most common source of blockage (30%) Disconnection of shunt components account for 15% Distal shunt obstruction due to encystment and loculation of peritoneal contents around distal tip
37 Shunt infection 70% present within the first 2 months after shunt placement Low grade fever, malaise, irritability, nausea, erythema over shunt site
38 Overdrainage Not seen as much with modern shunt components (programmable valves) Orthostatic headache, dizziness, nausea, lethargy, diplopia Can lead to chronic subdural hematoma
39 Overdrainage

40 Subdural hematoma Change in mental status, signs of increased intracranial pressure Especially consider in older patients Treatment is neurosurgical; burr hole or craniotomy

41 Epidural hematoma Due to injury of the middle meningeal artery
42 Spasticity Components of UMNS Spasticity Mass synergy patterns Weakness Loss of finger dexterity
43 Spasticity Rule out exacerbating factors Non-pharmacological treatments Oral medications Intrathecal baclofen Focal treatments Surgery
44 Neuroendocrine Dysfunction More common than once thought Autopsy study of 100 patients with TBI found 62% had injury to pituitary Studies of hormone levels in patients with severe TBI found 36-69% had abnormal levels of at least 1 hormone

45 Pituitary Gland
46 Neuroendocrine Dysfunction All of the following have been reported abnormal in TBI survivors Antidiuretic hormone Cortisol Growth hormone Thyroxine FSH/LH Prolactin Glucagon Somatostatin
47 Normal Pressure Hydrocephalus Classic triad- incontinence, gait disorder and dementia Classic gait is short, wide based, magnetic steps Some believe this is the most common cause of post trauma HA IGF1 Urine assessment if polyuria Patients with moderate to severe TBI should undergo hormone evaluation at 3 months and 12 months post ICU discharge
48 Neuroendocrine Dysfunction Recommendations of Global Experts Consensus Panel 2005 Patients with moderate to severe TBI should undergo hormonal evaluation at 3 months and 12 months post ICU discharge
49 Neuroendocrine Dysfunction Hormone evaluation should include 9 AM cortisol level ft3, ft4 TSH FSH LH Testosterone in males E2 in females Prolactin IGF1
50 SIADH Inappropriate ADH release will produce hyponatremia by interfering with urinary dilution and decreasing excretion of ingested water Na < 135 Nausea, fatigue, muscle cramps, change in mental status, seizure, coma
51 Post Traumatic Headache Most common complaint after mtbi Consider causes such as hematomas, hydrocephalus, VP shunt malfunction Types Musculoskeletal Cervicogenic Neuralgic Post traumatic migraine Post traumatic sinus headache
52 Musculoskeletal Headache Referred pain from muscles such as trapezius and SCM Pattern often refers pain to retro or peri orbital area Treatment with trigger point management, acupuncture, postural correction, meds
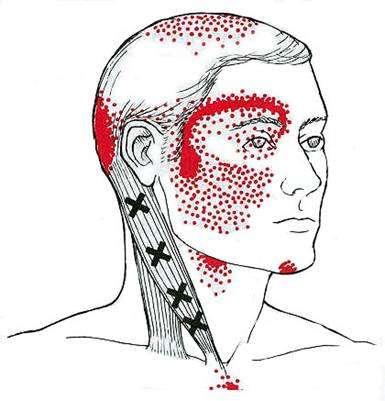
53 Musculoskeletal HA

54 Cervicogenic Headache Pain referred from zygapophyseal joints of c-spine especially C2 and C3
55 Neuralgic Headache Most common is greater occipital nerve Splenius muscle spasm or overactivity exacerbates Ipsilateral frontotemporal scalp Treatment with trigger point management, gabapentin, TCAs, NSAIDs, blocks, surgical decompression

56 Occipital Neuralgia
57 Post Traumatic Migraine Described as throbbing, unilateral, worse with cough or bending over. May have visual issues, nausea, vomiting Treatment like migraine in general population. Prophylactic meds (NSAIDs, beta blockers, calcium channel blockers, TCAs, depakote) and abortive meds (triptans, ergot, dihydroergotamine). Possible role for botox
58 Post Traumatic Sinus HA Patient with history of facial bone fractures HA pattern may be based on drainage angles Frontal and ethmoid worse with supine Maxillary and sphenoid better supine
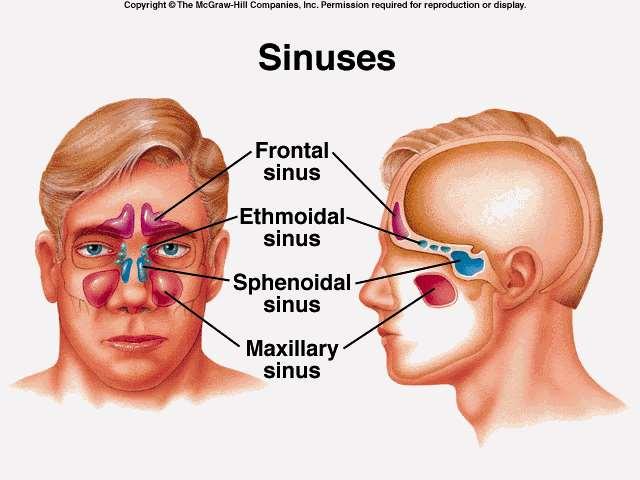
59 Sinuses
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
PERSPECTIVE INJURY SEVERITY. REHABILITATION PHYSICIAN Team approach Functional implications Long term consequences
 MANAGEMENT OF INDIVIDUALS STATUS POST BRAIN INJURY: IMPACT ON LIFE CARE PLANNING Richard Bonfiglio, M.D. PERSPECTIVE REHABILITATION PHYSICIAN Team approach Functional implications Long term consequences
MANAGEMENT OF INDIVIDUALS STATUS POST BRAIN INJURY: IMPACT ON LIFE CARE PLANNING Richard Bonfiglio, M.D. PERSPECTIVE REHABILITATION PHYSICIAN Team approach Functional implications Long term consequences
TRAUMATIC BRAIN INJURY. Moderate and Severe Brain Injury
 TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury
 Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury BACKGROUND Trauma related acquired brain injury (ABI) is known to
Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury BACKGROUND Trauma related acquired brain injury (ABI) is known to
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
TRAUMATIC BRAIN INJURY
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences TRAUMATIC BRAIN INJURY GARY STOBBE, MD UNIVERSITY OF WASHINGTON GENERAL DISCLOSURES The University of Washington
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences TRAUMATIC BRAIN INJURY GARY STOBBE, MD UNIVERSITY OF WASHINGTON GENERAL DISCLOSURES The University of Washington
THE ESSENTIAL BRAIN INJURY GUIDE
 THE ESSENTIAL BRAIN INJURY GUIDE Neuroanatomy & Neuroplasticity Section 2 Contributors Erin D. Bigler, PhD Michael R. Hoane, PhD Stephanie Kolakowsky-Hayner, PhD, CBIST, FACRM Dorothy A. Kozlowski, PhD
THE ESSENTIAL BRAIN INJURY GUIDE Neuroanatomy & Neuroplasticity Section 2 Contributors Erin D. Bigler, PhD Michael R. Hoane, PhD Stephanie Kolakowsky-Hayner, PhD, CBIST, FACRM Dorothy A. Kozlowski, PhD
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Chronic Daily Headaches
 Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
Non-Motor Symptoms of Parkinson s Disease
 Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
Introduction. 1 person in 20 will have an epileptic seizure at some time in their life
 Introduction 1 person in 20 will have an epileptic seizure at some time in their life Epilepsy is diagnosed on the basis of two or more epileptic seizures. Around 450,000 people in the UK have epilepsy
Introduction 1 person in 20 will have an epileptic seizure at some time in their life Epilepsy is diagnosed on the basis of two or more epileptic seizures. Around 450,000 people in the UK have epilepsy
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes
 Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes Jessica Matthes, Ph.D., ABN Barrow TBI Symposium March 23, 2019 jessica.matthes@dignityhealth.org Outline TBI Mechanisms of Injury Types
Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes Jessica Matthes, Ph.D., ABN Barrow TBI Symposium March 23, 2019 jessica.matthes@dignityhealth.org Outline TBI Mechanisms of Injury Types
Continuum of Care: Post Acute Brain Injury Rehabilitation
 Continuum of Care: Post Acute Brain Injury Rehabilitation Laura Wiggs, PT, NCS, CBIS Mentis Neuro Rehabilitation Traumatic Brain Injury (TBI) When an outside mechanical force is applied to the head and
Continuum of Care: Post Acute Brain Injury Rehabilitation Laura Wiggs, PT, NCS, CBIS Mentis Neuro Rehabilitation Traumatic Brain Injury (TBI) When an outside mechanical force is applied to the head and
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
2/20/2019 BRAIN DISSECTION CODING AND DOCUMENTATION OBJECTIVES INTRODUCTION
 BRAIN DISSECTION CODING AND DOCUMENTATION Diana R. Phelps, CPC, CPC-I, CEMC OBJECTIVES Identify general structure of the human brain Describe how the different parts work Recognized the two hemispheres
BRAIN DISSECTION CODING AND DOCUMENTATION Diana R. Phelps, CPC, CPC-I, CEMC OBJECTIVES Identify general structure of the human brain Describe how the different parts work Recognized the two hemispheres
10/19/12. Post-Traumatic Headache. Lawrence J. Horn, MD Disclosures. Speakers Bureau: Allergan, Inc.
 10/19/12 Post-Traumatic Headache Professor and Interim Chair, Department of PM&R Wayne State University School of Medicine Detroit, MI Medical Director Neuroscience Rehabilitation Institute of Michigan
10/19/12 Post-Traumatic Headache Professor and Interim Chair, Department of PM&R Wayne State University School of Medicine Detroit, MI Medical Director Neuroscience Rehabilitation Institute of Michigan
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Objectives. Amanda Diamond, MD
 Amanda Diamond, MD Objectives Recognize symptoms suggestive of seizure and what those clinical symptoms represent Understand classification of epilepsy and why this is important Identify the appropriate
Amanda Diamond, MD Objectives Recognize symptoms suggestive of seizure and what those clinical symptoms represent Understand classification of epilepsy and why this is important Identify the appropriate
Neurology Clerkship Learning Objectives
 Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
NEUROSURGEON VS. HOSPITALIST Pediatric Hospital Medicine meeting Nashville, TN July 21, 2017*±
 NEUROSURGEON VS. HOSPITALIST Pediatric Hospital Medicine meeting Nashville, TN July 21, 2017*± *no pediatricians were harmed in the making of this presentation ±nonetheless, please do not try this at home
NEUROSURGEON VS. HOSPITALIST Pediatric Hospital Medicine meeting Nashville, TN July 21, 2017*± *no pediatricians were harmed in the making of this presentation ±nonetheless, please do not try this at home
Neurosurgery. Neurosurgery
 Neurosurgery Neurosurgery Neurosurgery Telephone Numbers: Appointment: 202-476-3020 Fax: 202-476-3091 Administration: 202-476-3020 Evenings and Weekends: 202-476-5000 Robert Keating, MD, Chief The Division
Neurosurgery Neurosurgery Neurosurgery Telephone Numbers: Appointment: 202-476-3020 Fax: 202-476-3091 Administration: 202-476-3020 Evenings and Weekends: 202-476-5000 Robert Keating, MD, Chief The Division
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abuse alcohol, aggression and, 52 53 substance, aggression and, 52 54 ACE. See Aid to Capacity Evaluation (ACE). AEDs. See Antiepileptic
Index Note: Page numbers of article titles are in boldface type. A Abuse alcohol, aggression and, 52 53 substance, aggression and, 52 54 ACE. See Aid to Capacity Evaluation (ACE). AEDs. See Antiepileptic
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abscess(es) epidural anesthesia-related, 825 826 ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors Acetaminophen for
Index Note: Page numbers of article titles are in boldface type. A Abscess(es) epidural anesthesia-related, 825 826 ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors Acetaminophen for
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
New Patient Form. Patient Demographics. Emergency Information. Employment Information. Page 1 of 7. Family Health Chiropractic Care
 Page 1 of 7 Patient Demographics First Name* Last Name* Date Of Birth* Home Phone* Mobile Phone Phone Gender* Email Preferred Communication Street Address 1* Street Addresss 2 Zip* City* State* Emergency
Page 1 of 7 Patient Demographics First Name* Last Name* Date Of Birth* Home Phone* Mobile Phone Phone Gender* Email Preferred Communication Street Address 1* Street Addresss 2 Zip* City* State* Emergency
Headache Assessment In Primary Eye Care
 Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
UNDERSTANDING HYDROCEPHALUS
 UNDERSTANDING HYDROCEPHALUS Offering solutions for patients. 1 UNDERSTANDING HYDROCEPHALUS Dear Reader: Your doctor has either recommended the CODMAN HAKIM Precision Fixed Pressure Valve, the CODMAN HAKIM
UNDERSTANDING HYDROCEPHALUS Offering solutions for patients. 1 UNDERSTANDING HYDROCEPHALUS Dear Reader: Your doctor has either recommended the CODMAN HAKIM Precision Fixed Pressure Valve, the CODMAN HAKIM
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Assistant Professor of Neurology and Psychiatry University of Colorado Denver Goals 1) What are the most common non-motor
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Assistant Professor of Neurology and Psychiatry University of Colorado Denver Goals 1) What are the most common non-motor
Strategies in Migraine Care
 Strategies in Migraine Care Julie L. Roth, MD Rhode Island Hospital Assistant Professor, Neurology The Warren Alpert Medical School of Brown University March 28, 2015 Financial Disclosures None. Objectives
Strategies in Migraine Care Julie L. Roth, MD Rhode Island Hospital Assistant Professor, Neurology The Warren Alpert Medical School of Brown University March 28, 2015 Financial Disclosures None. Objectives
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Accidents, risk of, with insufficient sleep, 318 Acquired immunodeficiency syndrome (AIDS), comorbid with narcolepsy, 298 299 Actigraphy, in
Note: Page numbers of article titles are in boldface type. A Accidents, risk of, with insufficient sleep, 318 Acquired immunodeficiency syndrome (AIDS), comorbid with narcolepsy, 298 299 Actigraphy, in
Workbook Answers Chapter 13. Neurologic Diseases and Conditions
 Workbook Answers Chapter 13 Neurologic Diseases and Conditions Short Answer 1. Afferent nerves transmit impulses from parts of the body to the spinal cord; efferent nerves transmit impulses away from the
Workbook Answers Chapter 13 Neurologic Diseases and Conditions Short Answer 1. Afferent nerves transmit impulses from parts of the body to the spinal cord; efferent nerves transmit impulses away from the
Interrelation between Neuroendocrine Disturbances and Medical Complications Encountered during Rehabilitation after TBI
 J. Clin. Med. 2015, 4, 1815-1840; doi:10.3390/jcm4091815 Review OPEN ACCESS Journal of Clinical Medicine ISSN 2077-0383 www.mdpi.com/journal/jcm Interrelation between Neuroendocrine Disturbances and Medical
J. Clin. Med. 2015, 4, 1815-1840; doi:10.3390/jcm4091815 Review OPEN ACCESS Journal of Clinical Medicine ISSN 2077-0383 www.mdpi.com/journal/jcm Interrelation between Neuroendocrine Disturbances and Medical
Managing Medical Complications of Brain Injury. Katie Turpin, NP-C
 Managing Medical Complications of Brain Injury Katie Turpin, NP-C Objectives: 1. Describe the role of the medical team in a setting focused on therapy/rehabilitation. 2. Identify common disabilities or
Managing Medical Complications of Brain Injury Katie Turpin, NP-C Objectives: 1. Describe the role of the medical team in a setting focused on therapy/rehabilitation. 2. Identify common disabilities or
Causes of TBI vary with age
 Endocrinopathies after Traumatic Brain Injury Susan R. Rose, MD Professor Cincinnati Children s Hospital Medical Center University of Cincinnati Supported by Pfizer, Inc Investigator-Initiated Research
Endocrinopathies after Traumatic Brain Injury Susan R. Rose, MD Professor Cincinnati Children s Hospital Medical Center University of Cincinnati Supported by Pfizer, Inc Investigator-Initiated Research
+ Color Change - + Hearing Loss - + Apnea - + Enuresis (urine - + Tremors - + Rash -
 Review of Systems: 0-1 year old Constitution neg Eyes neg GI neg Neurological neg + Activity Change - + Eye Discharge - + Reflux - + Facial Asymmetry - + Appetite Change - + Eye Redness - + Vomiting -
Review of Systems: 0-1 year old Constitution neg Eyes neg GI neg Neurological neg + Activity Change - + Eye Discharge - + Reflux - + Facial Asymmetry - + Appetite Change - + Eye Redness - + Vomiting -
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
CASE 1. Female 21 years old DOL: November 28, 2016
 CASE 1 Female 21 years old DOL: November 28, 2016 Injuries and Sequelae: GCS: 4 / 15 and coma for 3 weeks Multifocal intracranial hemorrhage at right thalamus and left frontal and temporal lobe Diffuse
CASE 1 Female 21 years old DOL: November 28, 2016 Injuries and Sequelae: GCS: 4 / 15 and coma for 3 weeks Multifocal intracranial hemorrhage at right thalamus and left frontal and temporal lobe Diffuse
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
Index. Prim Care Clin Office Pract 31 (2004) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Prim Care Clin Office Pract 31 (2004) 441 447 Index Note: Page numbers of article titles are in boldface type. A Abscess, brain, headache in, 388 Acetaminophen for migraine, 406 407 headache from, 369
Prim Care Clin Office Pract 31 (2004) 441 447 Index Note: Page numbers of article titles are in boldface type. A Abscess, brain, headache in, 388 Acetaminophen for migraine, 406 407 headache from, 369
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Procedures commonly seen at Vanderbilt Medical Center PACU s: Cervical, thoracic, lumbar, and sacral spine surgeries. Goes to 6N
 Procedures commonly seen at Vanderbilt Medical Center PACU s: Cervical, thoracic, lumbar, and sacral spine surgeries Goes to 6N Burr holes and Craniotomies for hemorrhage, tumors, trauma, debulking Goes
Procedures commonly seen at Vanderbilt Medical Center PACU s: Cervical, thoracic, lumbar, and sacral spine surgeries Goes to 6N Burr holes and Craniotomies for hemorrhage, tumors, trauma, debulking Goes
Neurosurgery Review. Mudit Sharma, MD May 16 th, 2008
 Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Brain Meninges, Ventricles and CSF
 Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
The Child with Alterations in Cerebral Function
 The Child with Alterations in Cerebral Function Neurologic Assessment VS HR, BP, Respirations, Temperature LOC Orientation Pediatric Glasgow Coma Scale Eyes Pupillary response and movement, extraoccular
The Child with Alterations in Cerebral Function Neurologic Assessment VS HR, BP, Respirations, Temperature LOC Orientation Pediatric Glasgow Coma Scale Eyes Pupillary response and movement, extraoccular
Aurora Health Care South Region EMS st Quarter CE Packet
 Name: Dept: Date: Aurora Health Care South Region EMS 2010 1 st Quarter CE Packet Meningitis Meningitis is an inflammatory disease of the leptomeninges. Leptomeninges refer to the pia matter and the arachnoid
Name: Dept: Date: Aurora Health Care South Region EMS 2010 1 st Quarter CE Packet Meningitis Meningitis is an inflammatory disease of the leptomeninges. Leptomeninges refer to the pia matter and the arachnoid
Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults
 Research Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults Mark T. Pfefer, RN, MS, DC *1 ; Richard Strunk MS, DC 2 Address: 1 Professor and Director of Research, Cleveland Chiropractic
Research Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults Mark T. Pfefer, RN, MS, DC *1 ; Richard Strunk MS, DC 2 Address: 1 Professor and Director of Research, Cleveland Chiropractic
Hydrocephalus 1/16/2015. Hydrocephalus. Functions of Cerebrospinal fluid (CSF) Flow of CSF
 Flow of CSF") Hydrocephalus Hydrocephalus Ruth Arms, MSN, CNS-BC, SCRN Hydrocephalus is the buildup of fluid in the cavities (ventricles) deep within the brain. The excess fluid increases the size of the ventricles
Hydrocephalus Hydrocephalus Ruth Arms, MSN, CNS-BC, SCRN Hydrocephalus is the buildup of fluid in the cavities (ventricles) deep within the brain. The excess fluid increases the size of the ventricles
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
Meninges and Ventricles
 Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
The dura is sensitive to stretching, which produces the sensation of headache.
 Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
1/31/2009. Paroxysmal, uncontrolled electrical discharge of neurons in brain interrupting normal function
 Paroxysmal, uncontrolled electrical discharge of neurons in brain interrupting normal function In epilepsy abnormal neurons undergo spontaneous firing Cause of abnormal firing is unclear Firing spreads
Paroxysmal, uncontrolled electrical discharge of neurons in brain interrupting normal function In epilepsy abnormal neurons undergo spontaneous firing Cause of abnormal firing is unclear Firing spreads
Plan for Today. Brain Injury: 8/4/2017. Effective Services for People Living with Brain Injury. What is it & what causes it?
 Effective Services for People Living with Brain Injury Jean Capler, MSW, LSW Local Support Network Leader The Rehabilitation Hospital of Indiana Department of Resource Facilitation Plan for Today Brain
Effective Services for People Living with Brain Injury Jean Capler, MSW, LSW Local Support Network Leader The Rehabilitation Hospital of Indiana Department of Resource Facilitation Plan for Today Brain
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
North Oaks Trauma Symposium Friday, November 3, 2017
 + Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
+ Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
PRIVILEGE APPLICATION FORM - [Mercy Medical Center]
![PRIVILEGE APPLICATION FORM - [Mercy Medical Center]](/thumbs/89/98821167.jpg "PRIVILEGE APPLICATION FORM - [Mercy Medical Center]") Current Privilege Status Key Practitioner's Current Privilege status is signified in ( ) preceding each privilege. G = W = Withdrawn T = Temporary P = With Proctor A = Assist with C = With Consult E =
Current Privilege Status Key Practitioner's Current Privilege status is signified in ( ) preceding each privilege. G = W = Withdrawn T = Temporary P = With Proctor A = Assist with C = With Consult E =
Impact on our Mental Health. Biological Changes Psychological Changes Social Changes Professional Services Coping Skills
 Impact on our Mental Health Biological Changes Psychological Changes Social Changes Professional Services Coping Skills Biological Changes After a brain injury, biological impacts may affect mental health
Impact on our Mental Health Biological Changes Psychological Changes Social Changes Professional Services Coping Skills Biological Changes After a brain injury, biological impacts may affect mental health
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PEDIATRIC BRAIN CARE
 PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
Anatomy and Physiology. Neurological Topics. Common Signs and Symptoms
 Anatomy and Physiology Neurological Topics HIHIM 409 Nervous system: brain, spinal cord, nerves Central Nervous System (CNS) and Peripheral Nervous System (PNS) CNS: brain and spinal cord PNS: autonomic
Anatomy and Physiology Neurological Topics HIHIM 409 Nervous system: brain, spinal cord, nerves Central Nervous System (CNS) and Peripheral Nervous System (PNS) CNS: brain and spinal cord PNS: autonomic
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Moath Darweesh. Zaid Emad. Anas Abu -Humaidan
 3 Moath Darweesh Zaid Emad Anas Abu -Humaidan Introduction: First two lectures we talked about acute and chronic meningitis, which is considered an emergency situation. If you remember, CSF examination
3 Moath Darweesh Zaid Emad Anas Abu -Humaidan Introduction: First two lectures we talked about acute and chronic meningitis, which is considered an emergency situation. If you remember, CSF examination
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Pituitary Disorders. Eiman Ali Basheir Mob: /1/2019
 Pituitary Disorders Eiman Ali Basheir Mob: 0915020385 31/1/2019 Objectives By the end of this lecture the students will be able to: Understand basic Pituitary axis physiology State the common causes of
Pituitary Disorders Eiman Ali Basheir Mob: 0915020385 31/1/2019 Objectives By the end of this lecture the students will be able to: Understand basic Pituitary axis physiology State the common causes of
Referral Criteria for Medical CT Radiation Exposures. Neuro Referrals
 Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Head Injury: Classification Most Severe to Least Severe
 Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
Care for patients with Neurological disorders
 King Saud University College of Nursing Medical Surgical Department Application of Adult Health Nursing Skills ( NUR 317 ) Care for patients with Neurological disorders Outline; EEG Overview. Nursing Interventions;
King Saud University College of Nursing Medical Surgical Department Application of Adult Health Nursing Skills ( NUR 317 ) Care for patients with Neurological disorders Outline; EEG Overview. Nursing Interventions;
Not Sleeping Well? Chronic physical conditions. There May Be a Medical Cause. Diabetes. Heartburn
 Not Sleeping Well? There May Be a Medical Cause People who feel they sleep perfectly well may still be troubled by excessive daytime sleepiness because of a variety of underlying medical illnesses. A sleep
Not Sleeping Well? There May Be a Medical Cause People who feel they sleep perfectly well may still be troubled by excessive daytime sleepiness because of a variety of underlying medical illnesses. A sleep
Traumatic Brain Injury
 General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
Intracranial hypotension secondary to spinal CSF leak: diagnosis
 Intracranial hypotension secondary to spinal CSF leak: diagnosis Spinal cerebrospinal fluid (CSF) leak is an important and underdiagnosed cause of new onset headache that is treatable. Cerebrospinal fluid
Intracranial hypotension secondary to spinal CSF leak: diagnosis Spinal cerebrospinal fluid (CSF) leak is an important and underdiagnosed cause of new onset headache that is treatable. Cerebrospinal fluid
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
Overview. Surviving shift work. What is the circadian rhythm? Components of a Generic Biological Timing System 31/10/2017
 Overview Surviving shift work Dr Claire M. Ellender Respiratory and Sleep Physician Princess Alexandra Hospital Conflicts nil relevant Circadian rhythm Impacts of shift work on health Case example Circadian
Overview Surviving shift work Dr Claire M. Ellender Respiratory and Sleep Physician Princess Alexandra Hospital Conflicts nil relevant Circadian rhythm Impacts of shift work on health Case example Circadian
CHRONIC HEADACHES IN CHILDHOOD
 CHRONIC HEADACHES IN CHILDHOOD EDWIN LIU, MD PEDIATRIC NEUROLOGISTS OF PALM BEACH PEDIATRIC SLEEP CENTERS OF FLORIDA ASSISTANT CLINICAL PROFESSOR FSU ASSISTANT CLINICAL PROFESSOR NOVA SOUTHEASTERN PEDIATRIC
CHRONIC HEADACHES IN CHILDHOOD EDWIN LIU, MD PEDIATRIC NEUROLOGISTS OF PALM BEACH PEDIATRIC SLEEP CENTERS OF FLORIDA ASSISTANT CLINICAL PROFESSOR FSU ASSISTANT CLINICAL PROFESSOR NOVA SOUTHEASTERN PEDIATRIC
The Central Nervous System
 The Central Nervous System Bởi: OpenStaxCollege The central nervous system (CNS) is made up of the brain, a part of which is shown in [link] and spinal cord and is covered with three layers of protective
The Central Nervous System Bởi: OpenStaxCollege The central nervous system (CNS) is made up of the brain, a part of which is shown in [link] and spinal cord and is covered with three layers of protective
Mild TBI (Concussion) Not Just Less Severe But Different
 Not Just Less Severe But Different") Mild TBI (Concussion) Not Just Less Severe But Different Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Mild TBI (Concussion) Not Just Less Severe But Different Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Phenytoin versus Levetiracetam for Prevention of Early Posttraumatic Seizures: A Prospective Comparative Study
 136 Original Article Phenytoin versus Levetiracetam for Prevention of Early Posttraumatic Seizures: A Prospective Comparative Study Kairav S. Shah 1 Jayun Shah 1 Ponraj K. Sundaram 1 1 Department of Neurosurgery,
136 Original Article Phenytoin versus Levetiracetam for Prevention of Early Posttraumatic Seizures: A Prospective Comparative Study Kairav S. Shah 1 Jayun Shah 1 Ponraj K. Sundaram 1 1 Department of Neurosurgery,
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute
 Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Brain Tumors. Andrew J. Fabiano, MD FAANS. Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine
 Brain Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases Brain
Brain Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases Brain
Mild Traumatic Brain Injury
 Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Surgery for Medically Refractory Focal Epilepsy
 Surgery for Medically Refractory Focal Epilepsy Seth F Oliveria, MD PhD The Oregon Clinic Neurosurgery Director of Functional Neurosurgery: Providence Brain and Spine Institute Portland, OR Providence
Surgery for Medically Refractory Focal Epilepsy Seth F Oliveria, MD PhD The Oregon Clinic Neurosurgery Director of Functional Neurosurgery: Providence Brain and Spine Institute Portland, OR Providence
Pituitary Apoplexy. Updated: April 22, 2018 CLINICAL RECOGNITION
 Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline. Scottish intercollegiate Guidelines Network SIGN
 A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
11. HEADACHE 1. Pablo Lapuerta, MD, Steven Asch, MD, MPH, and Kenneth Clark, MD, MPH
 11. HEADACHE 1 Pablo Lapuerta, MD, Steven Asch, MD, MPH, and Kenneth Clark, MD, MPH We identified articles on the evaluation and management of headache by conducting a MEDLINE search of English language
11. HEADACHE 1 Pablo Lapuerta, MD, Steven Asch, MD, MPH, and Kenneth Clark, MD, MPH We identified articles on the evaluation and management of headache by conducting a MEDLINE search of English language
ENDOCRINOLOGY COORDINATION OF PHYSIOLOGICAL PROCESSES:
 ENDOCRINOLOGY COORDINATION OF PHYSIOLOGICAL PROCESSES: -In a living organism there must be coordination of number of physiological activities taking place simultaneously such as: movement, respiration,
ENDOCRINOLOGY COORDINATION OF PHYSIOLOGICAL PROCESSES: -In a living organism there must be coordination of number of physiological activities taking place simultaneously such as: movement, respiration,
Pharmacy Name/Location/Phone number:
 Pharmacy Name/Location/Phone number: Family Physician Name: Phone: Address: Referring Physician Name: Phone: Address: First Emergency Contact: Relationship: Home/cell phone: Work phone: Second Emergency
Pharmacy Name/Location/Phone number: Family Physician Name: Phone: Address: Referring Physician Name: Phone: Address: First Emergency Contact: Relationship: Home/cell phone: Work phone: Second Emergency
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Non epileptiform abnormality J U LY 2 7,
 Non epileptiform abnormality S U D A J I R A S A K U L D E J, M D. C H U L A L O N G KO R N C O M P R E H E N S I V E E P I L E P S Y C E N T E R J U LY 2 7, 2 0 1 6 Outline Slow pattern Focal slowing
Non epileptiform abnormality S U D A J I R A S A K U L D E J, M D. C H U L A L O N G KO R N C O M P R E H E N S I V E E P I L E P S Y C E N T E R J U LY 2 7, 2 0 1 6 Outline Slow pattern Focal slowing