OPHTHALMIC ASSESSMENT. Nehal MANDOUR Associate Specialist Urgent Care Lead Clinician REI - PLYMOUTH
|
|
|
- Arline Singleton
- 6 years ago
- Views:
Transcription
1 OPHTHALMIC ASSESSMENT Nehal MANDOUR Associate Specialist Urgent Care Lead Clinician REI - PLYMOUTH




2 Patients presenting with an eye complaint may strike fear in some practitioner's hearts as they recall student days standing in dimly lit rooms looking at incomprehensible machines which obscure both patient and doctor, wondering what on earth was going on.
3 OUTLINE Anatomy overview Instruments used for eye exam History taking important?! Assessment of Eye Functions Assessment of Eye Structures

4 General appearance The eye is one of the few organs of the body which can be looked at both outside and in and whose basic function can be assessed using simple desk-top tools.
5

6 Cross section appearance
7
8 EYE ASSESSMENT
9 Good History Taking is Essential Complaint History of present complaint Past ocular history Medical history Drug history Family history Allergy
10 Is History Taking REALLY Important? B4E
 Duration Analgesia taken? Trauma (high velocity, organic, power tool, chemical) When Change in Vision: (Please circle.) Duration Blur: all over, central Peripheral shadow (where).")
11 History of Present Complaint Patient initial report of condition Which Eye Right Vision Left Vision Pain (sharp, fb sensation, ache, throbbing, pressure, headache) Duration Lid abnormality (lump,droop, oedema) Duration Analgesia taken? Trauma (high velocity, organic, power tool, chemical) When Change in Vision: (Please circle.) Duration Blur: all over, central Peripheral shadow (where)... Distortion Onset: sudden days, weeks, months Intermittent, Persistent Progression: stable, getting worse Associated pain headache Discharge (sticky, watery) Duration Floaters (how many) Duration Flashes (day, night) Duration Redness(where, how did you notice it) Duration Diplopia (vertical, horizontal, both eyes, one eye) Duration Associated with headache? Photophobia Duration GP ref for GCA (only if vision affected or diplopia- assess as above) ESR... Requested? CRP... Requested?
12 Previous Ocular History: Glasses wear ( distance,near), Contact lens wear Previous eye condition / treatment Previous ocular trauma or surgery Level of Visual Acuity in involved eye before injury Level of vision in the other eye. Medical History: Routine + Use of anticoagulant medications ---- especially over-the-counter medications containing aspirin Status of tetanus prophylaxis Any difficulties with previous anaesthesia or surgery
13 Instruments used for Eye Examination








14 In General Practice VA Chart Pen torch +/- blue filter Magnifying lens Slit lamp(?) Hand-held direct Ophthalmoscope Drops: Fluorescein drop / fluorescein impregnated paper Topical anaesthesia Topical short acting mydriatics preferably G.Tropicamide Ruler
 Posterior examination Red Reflex Fundus exam")
15 EYE EXAMINATION Visual Acuity Pupil Reflexes Visual Field EOM Pressure Anterior segment: Lid /Lacrimal system Conjunctiva /Sclera Cornea Anterior Chamber Iris / Pupil Lens Orbit ( If you can get that far GREAT ) Posterior examination Red Reflex Fundus exam Vitreous/Disc/Retina/Macula
16 Examining Eye Function
17 1.Visual Acuity First step (EXCEPT in CHEMICAL INJURY) Prior to shining light or manipulating the eye. Injured eye and uninjured eye Best corrected (ideal)-i.e. with correct glasses Pinhole: important ( reduction in vision with the pinhole can be a sign of ophthalmic pathology rather than a refractive error ) Pain relief, Tissue paper, Blinking, Guessing!



18 Each eye is tested independently. "Best corrected vision." Ask patients to read smallest line they can see. Repeat with the other eye.
19


 Counting fingers :")


20 Recording Visual acuity Rt eye and Lt eye Unaided vs with glasses With pin hole ( Improvement vs no improvement) 6/6 6/60 (+ or -) Counting fingers : Meters Hand movement : HM Light perception: LP No light perception : NPL ( Do not write: BLIND or UNABLE TO SEE)
.")

21 2. Pupillary Light Reflexes Darkened room Ask the patient to fix on a distant object (to avoid the accommodation reflex that causes constriction of the pupil). Shine bright a pen torch into one eye and assess if the pupil constricts. Then repeat this in the other eye. Observe for the : Direct response (constriction of the same pupil) Consensual response (simultaneous constriction of other pupil)
22 NORMAL
23 Swinging Flashlight" Test If it dilates rather than constricts, this is known as an RAPD. A positive finding is a strong indicator of retinal or optic nerve pathology. Ask the patient to fixate on an object in the distance, and then direct a bright light to one eye. Move the light quickly to the other eye and repeat the process, swinging the light from eye to eye. A normal reaction would be a brisk pupil constriction of the stimulated eye; as the light is moved to the fellow eye it should constrict (or stay constricted).
24 RAPD




25 3.a.Peripheral Visual Field Assessment Sit at the same horizontal and vertical level as patient, 1 meter away Ask patient to close one eye and you close your eye facing it Ask patient continue looking at your eye without moving eyes while you hold up your fingers and ask patient How many fingers you can see? in each quadrant. Repeat with your other eye. Assessing Right Eye Assessing Left Eye



26 3.b. Central Visual Field Look at my face (Is any part missing or blurred?) Amsler chart
27

28 4. Ocular Movements / Alignment Corneal Reflex Extra ocular movement in all directions of gaze Accommodation



29 Ocular Motility a. Corneal Reflex Use pen torch to create a light reflex on cornea. Normal corneal reflex should fall in the same position in each eye Misalignment: Esotropia: Convergent squint Exotropia: Divergent Squint Hypertopia: one eye is higher than the other Hypotropia: one eye is lower than other

30 Extra ocular Muscle movement in all directions of gaze Each of the 6 positions of gaze isolate the action of each of EOM SO '4', LR '6', all the rest '3'
31 Ocular Motility c. Accommodation The room light should be turned on. Ask patient to gaze to a far wall. Tell them that as soon as they see the your finger /pen/other object, they should focus straight on it. Bring your finger directly in towards the patient's nose. This will cause : the patient to look cross-eyed and the pupils should constrict briskly (Failure to do so is known as light-near dissociation.)
32 EYE STRUCTURE Assessment Anatomical examination Work systematically from front to back.
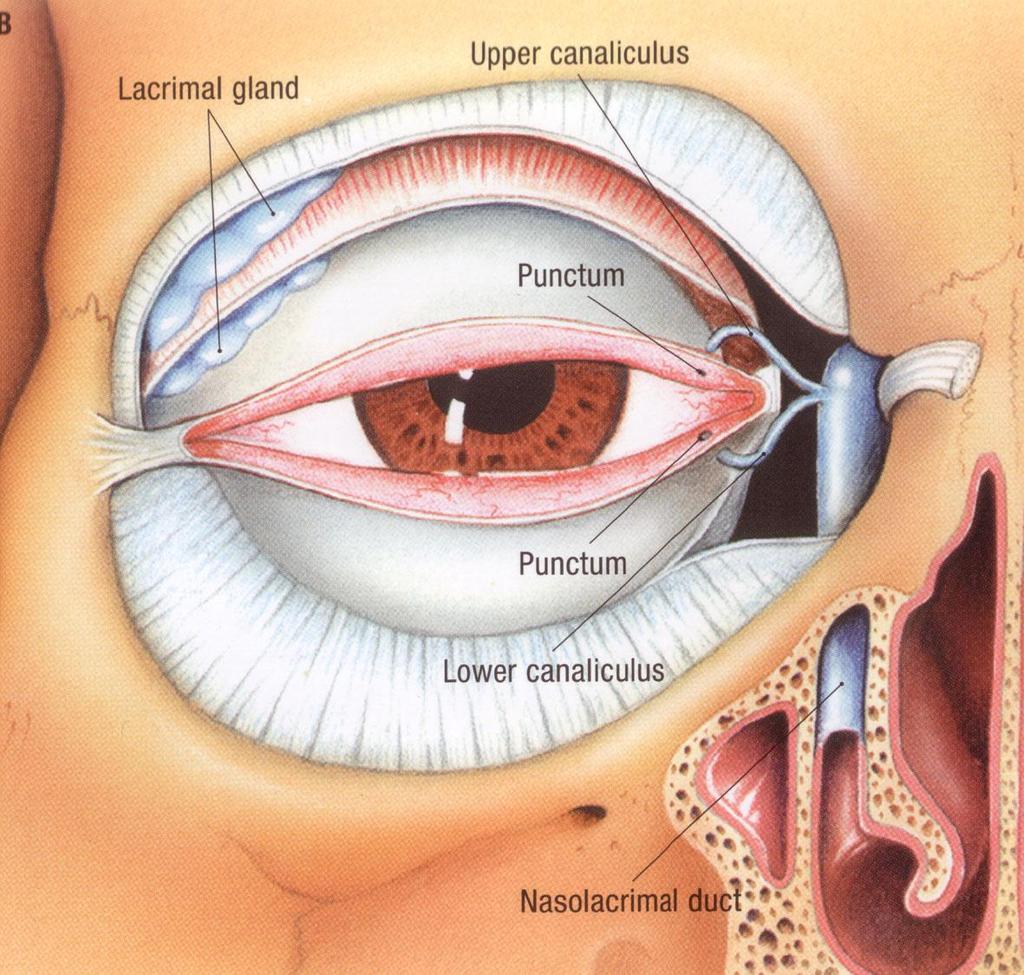
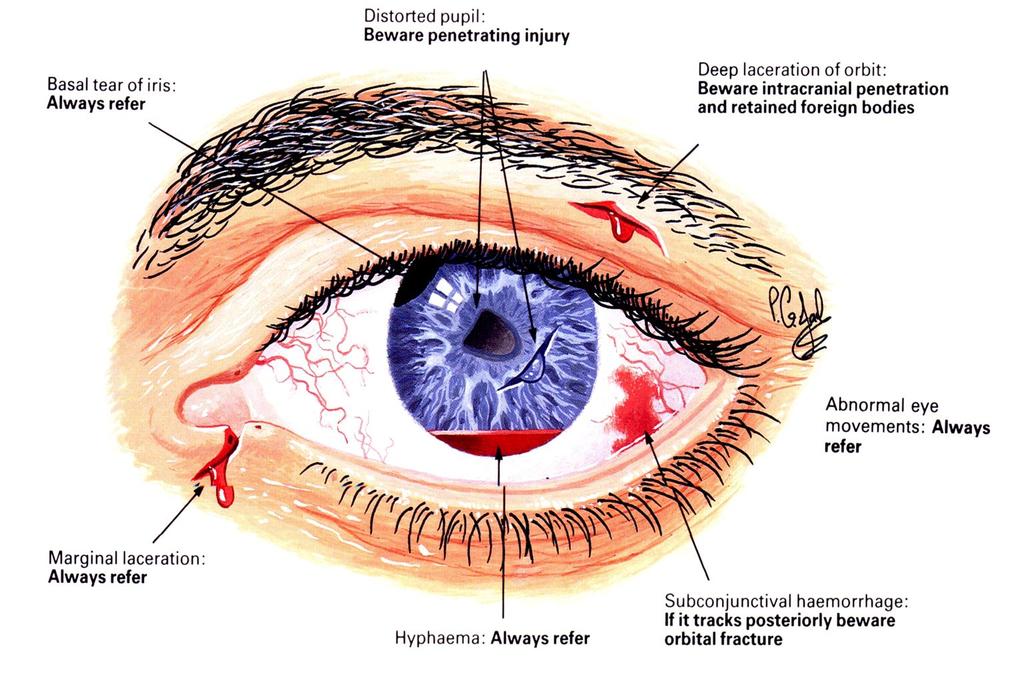
33 Lid/Lacrimal Haematoma / Swelling/ Signs of infection Wounds : Lacerations ( full or partial thickness ) esp. to margin / lacrimal puncti or canaliculi /Puncture wounds FB Position: Ptosis ( drooping)/ Retraction Ectropion / Entropion Lagophthalmos (inability to close eye fully ) Lumps and bumps (cysts, warts, chalazion, BCCs, SCCs) Skin rash / ulceration Lashes ( maldirected-rubbing) Margin (inflammation- Blephritis)





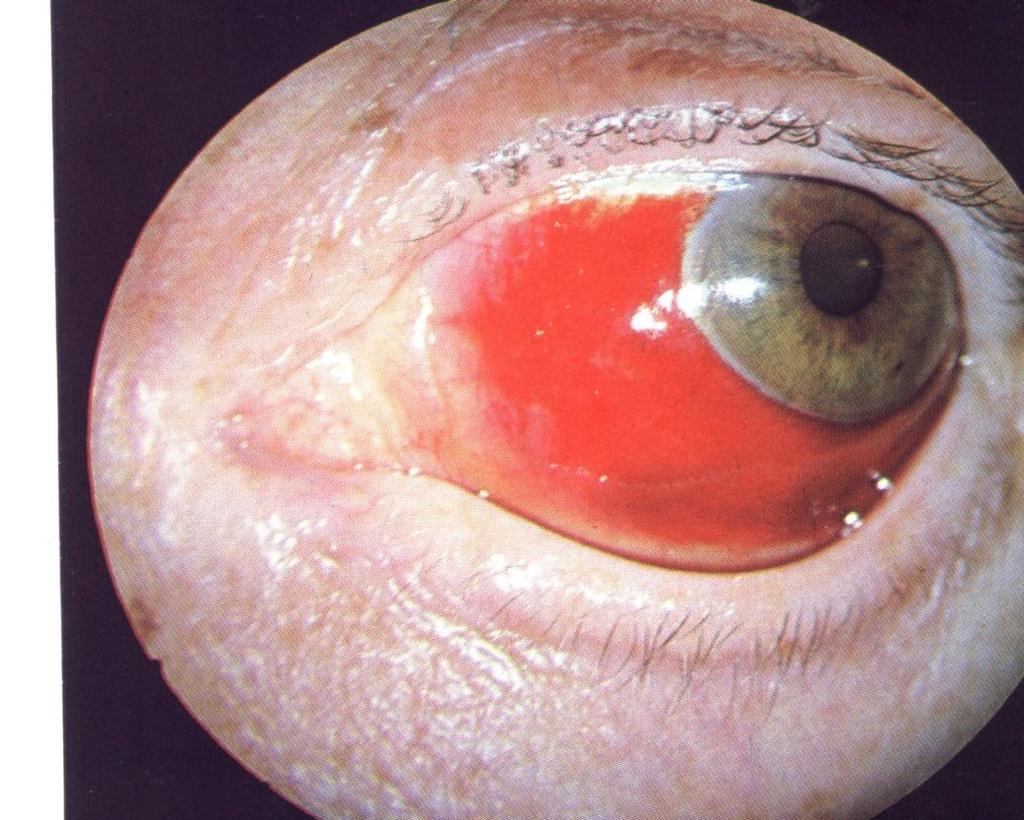
34 Lid Haematoma (Black Eye) The most common type of blunt eye injury Usually innocent ALWAYS exclude more serious conditions: Associated globe or orbit trauma: examine the integrity of globe before lids become oedematous Anterior fossa fracture: assoc. subconj. hge without a posterior limit Basal skull fracture: characteristic bilateral ring haematoma= panda eyes)



35 Eyelid lacerations REFER Deeper lacerations, Involving the lid margin Involving lacrimal punctum/canliculus Any associated tissue loss




36 Allergic lid oedema Ectropion Entropion Rubbing lashes
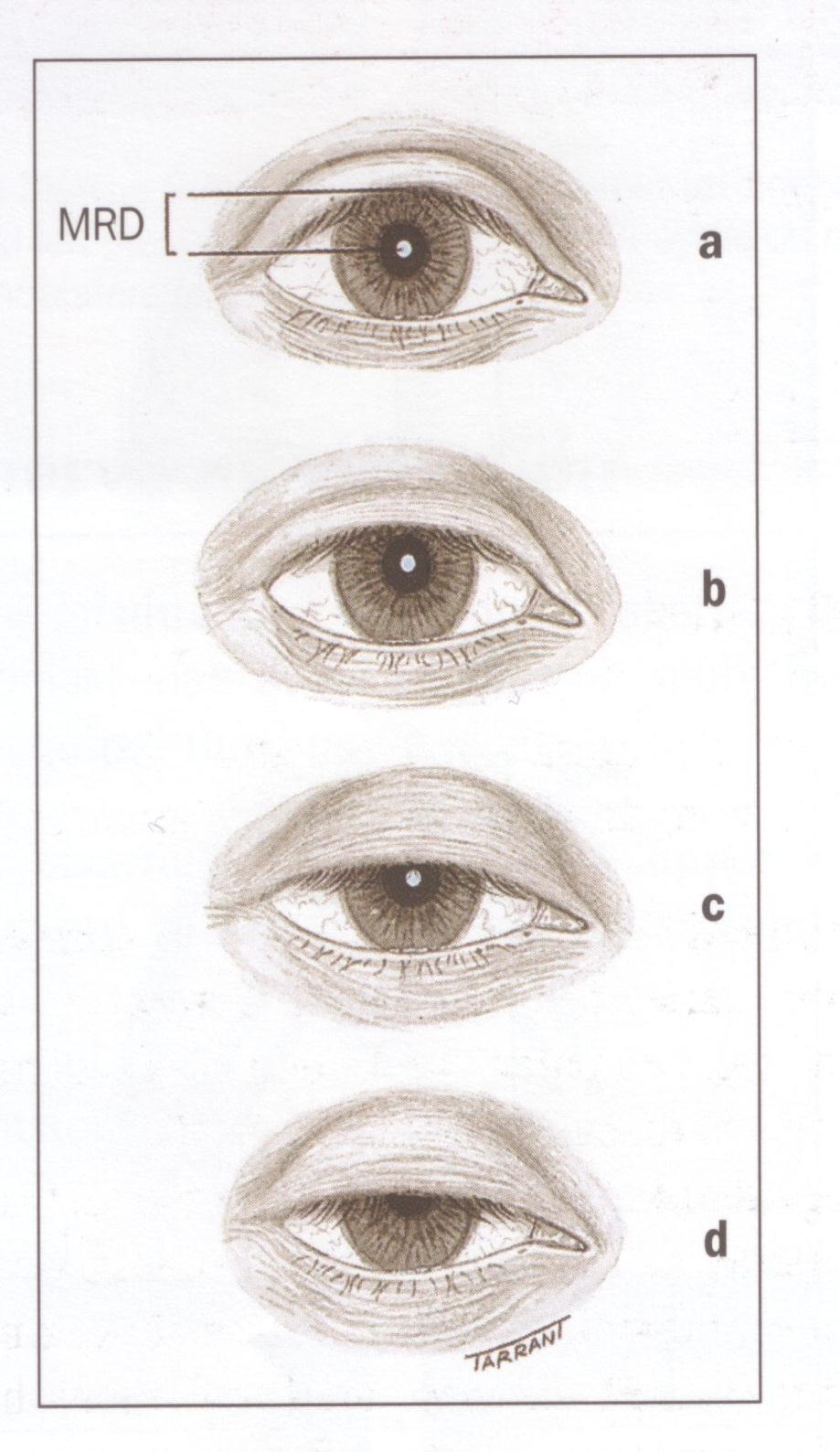
37 Ptosis Assessment
 Lid")

38 Lagophthalmos (ask patient to tightly squeeze eye lids) Lid retraction (visible sclera above the superior limbus+/- below inferior limbus)


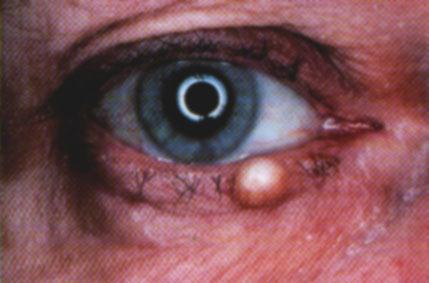





39 Lumps and Bumps





40 Lacrimal sac Inflammation ( Dacryocystitis) Acute Chronic +ve regurge NOT Lactimal


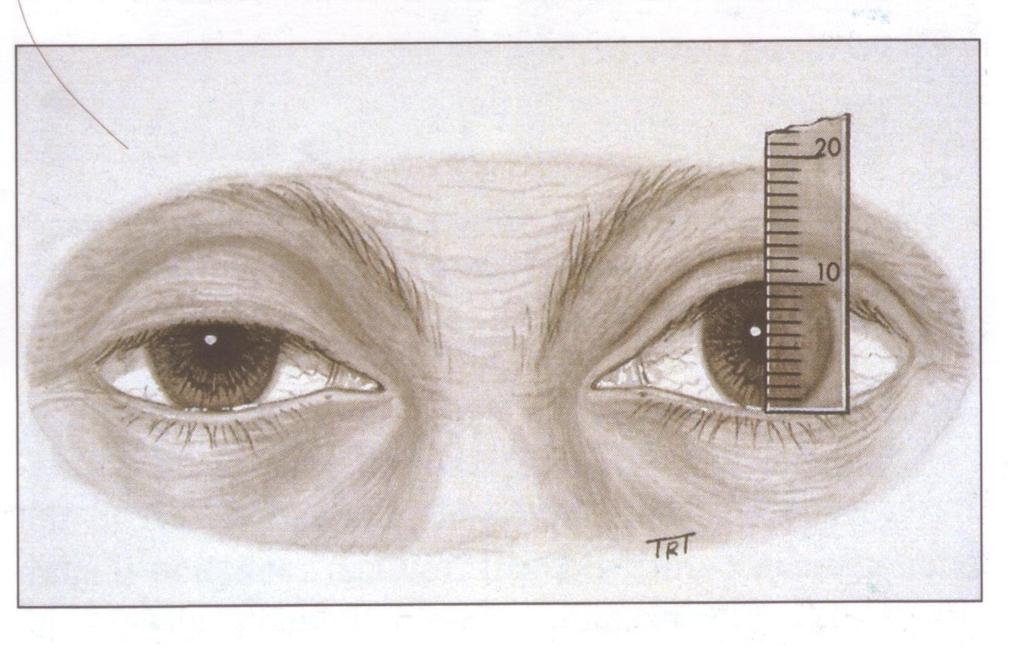
41 Orbit Look Listen Feel
42 Look Bruises Chemosis of conjunctiva Lid swellings/ haematoma /emphysema Nose bleeds Check the EOMs Proptosis (exophthalmos) Enophthalmos

43 Proptosis or Enophthalmos: Direction Severity: Look plastic ruler resting on lateral canthus Ideally in both erect and supine positions Proptosis : Readings > 20mm Difference of 2mm between both eyes regardless absolute

44 Retrobulbar Haemorrhage When an orbital vessel ruptures blood products into the orbit. Since closed space, any added contents increase pressure inside the orbit potential damage to the ocular structures. Look for: non-pulsating exophthalmos with resistance to retropulsion, elevated IOP, EOM restriction, central retinal artery pulsation (indicating a possible impending central retinal artery occlusion), choroidal folds, and possibly signs of optic neuropathy.
 diplopia: mechanical entrapment of")


45 Orbital Floor Blow-out fracture Symptoms Vertical (UP + Down Gaze) diplopia: mechanical entrapment of inferior rectus inferior oblique belly Adjacent fat / CT Hge + oedema of orbital fat/ CT Direct injury to muscle. look for : infraorbital hyposthesia and enophthalmos. Limited vertical mobility Intraocular damage



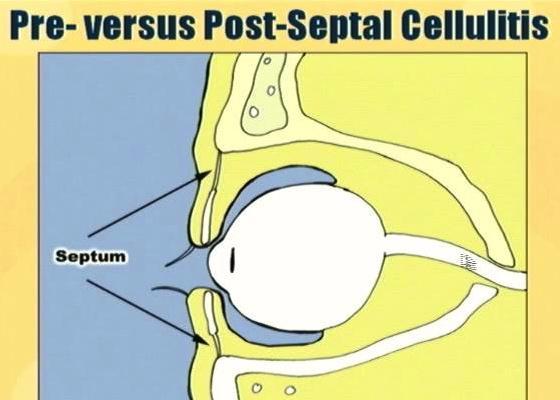
46 ORBITAL CELLULITIS Potentially blinding + life threatening especially in children Source of infection: Spread from periorbital tissues: sinuses, face, eye Direct inoculation of orbit from trauma or surgery Haematogenous spread from bacteraemia


47 ORBITAL CELLULITIS Cardinal signs: Proptosis Restricted eye movement Other signs: Patient is unwell, malaise Fever, headache Tenderness over sinuses Pain on eye movements Lid oedema and Chemosis Reduced vision/diplopia RAPD

")

48 Preseptal Cellulitis NO proptosis NO limited eye movement NO reduced vision ( after clearing any discharge) Patient is NOT toxic (Fever, lid oedema and hyperaemia, facial pain)

49 Palpate the eyelids for crepitus or subcutaneous emphysema. A positive finding indicates that air from a sinus has formed pockets within the orbital tissues. Feel Pulsations /Thrill Carotid-cavernous Fistula Evaluate orbital integrity: Palpate the orbital margins for a bony step-off that would be a clear sign of a fracture.

50 Feel Compare ipsilateral and contralateral cheek and forehead sensitivity:
 an abrupt onset usually caused by a traumatic basal skull")

51 Listen Audible Orbital Bruit Carotidocavernous Fistula ( High velocity fistula) an abrupt onset usually caused by a traumatic basal skull fracture. Look for: an audible orbital bruit, pulsatile proptosis, chemosis, orbital swelling, elevated IOP, ophthalmoplegia, and retinal vessel congestion.
52 Conjunctiva
53
54 Conjunctiva Look for: Local or generalised inflammation Discolouration Lesions wounds Pull down lower lid and evert upper lid

55
")
56 Chemosis (oedema)

57 Conjunctival Abrasions/ Lacerations Abrasions: fluorescein staining and may produce some degree of subconjunctival haemorrhage Lacerations significant haemorrhaging and typically have exposed white sclera. conjunctival edges have a tendency to be rolled due to the elastic nature of conjunctive. If a laceration is large, consider suturing, but most lacerations will heal without surgical repair.



58 Always : Inspect the fornices thoroughly Evert the eyelids to look for occult palpebral conjunctival FB which can cause corneal track marks.
59 Look for : Colour Wounds inflammation Sclera


60 Sclera Yellow sclera (icterus): in liver or blood disorders that cause hyperbilirubinemia. Muddy-brown discoloration common among dark / African people (a variant of normal).
 More florid")


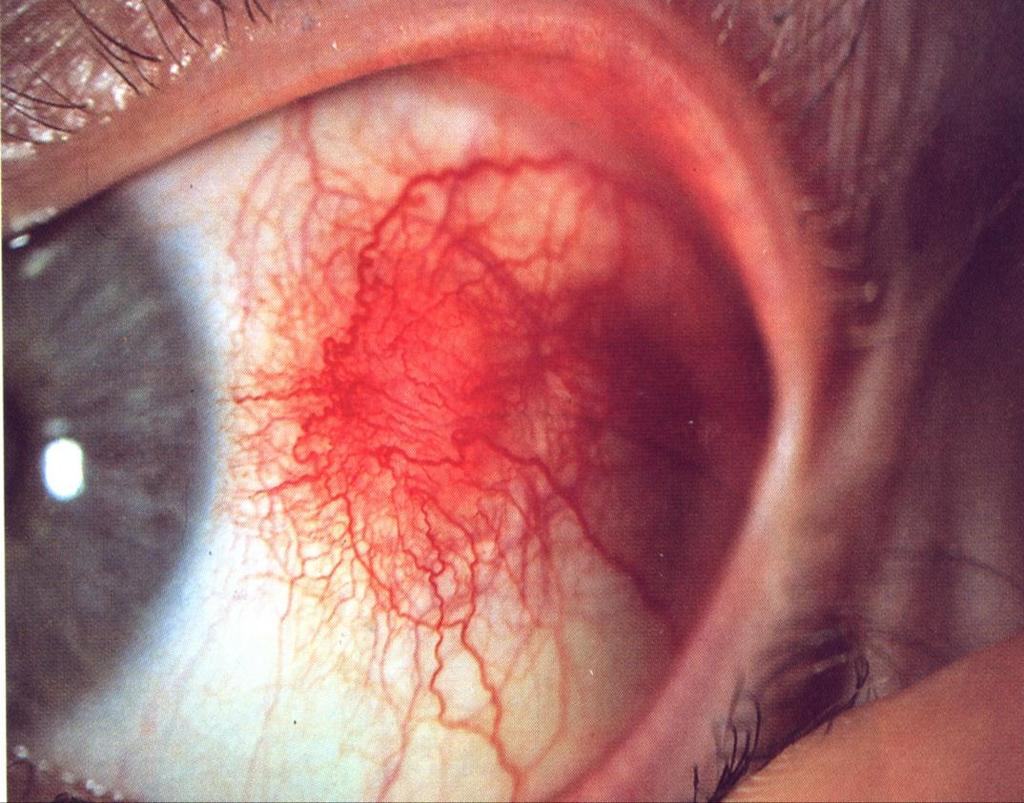
61 SCLERITIS Very painful (BORING+++) More florid inflammation Distortion of pattern of vascular plexus with loss of radial pattern No blanching with Phenylepherine 10% drops

62 Scleral Lacerations Refer
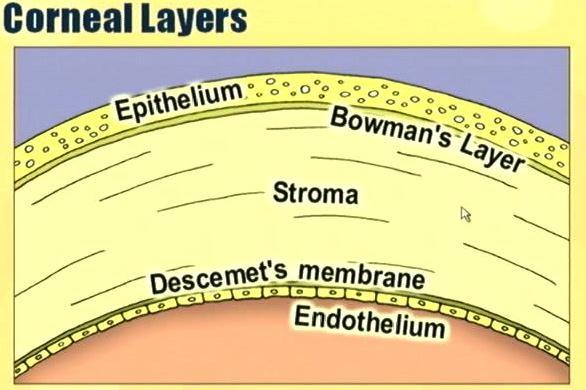
63 Cornea


64 Cornea Look for : Clarity Wounds/FB Stain with fluorescein Abrasions/ ulcers Seidle test (if suspecting penetrating injury)

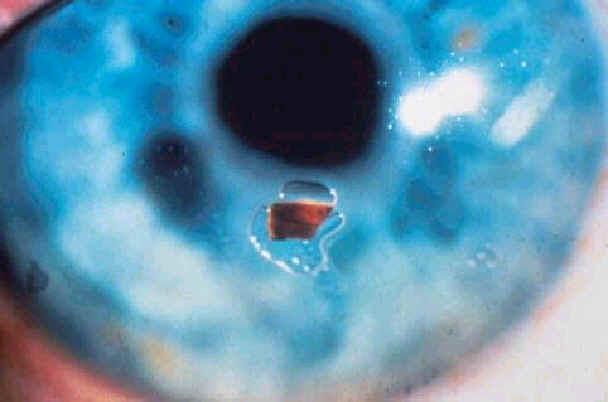

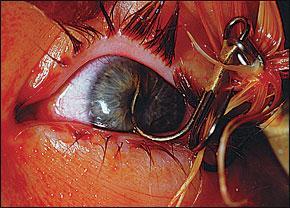

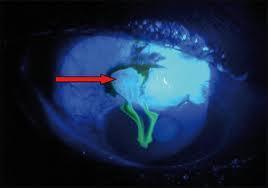
65 Corneal and conjunctival FB Corneal abrasions negative Seidel test. +ve fluorescein stain Corneal laceration +ve seidle test






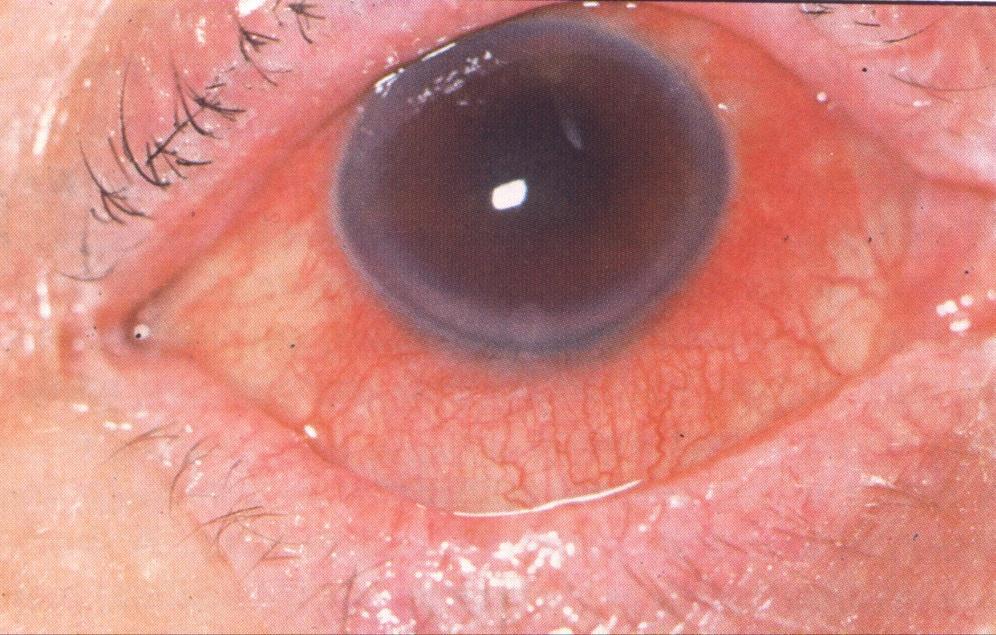
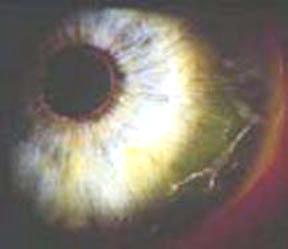
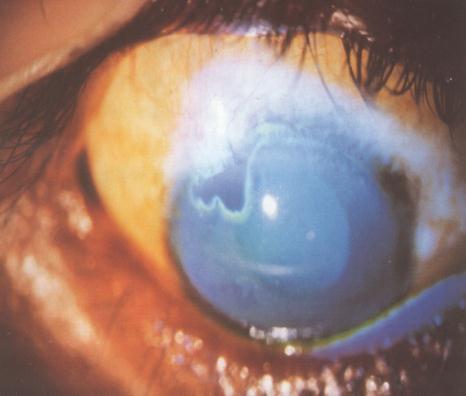
66 Corneal ulcers and Keratitis Corneal oedema ( cloudy cornea)

67 The Anterior Chamber
68 Anterior Chamber Content: Blood Pus FB Lens Depth: compare both eyes Shallow Deep Irregular

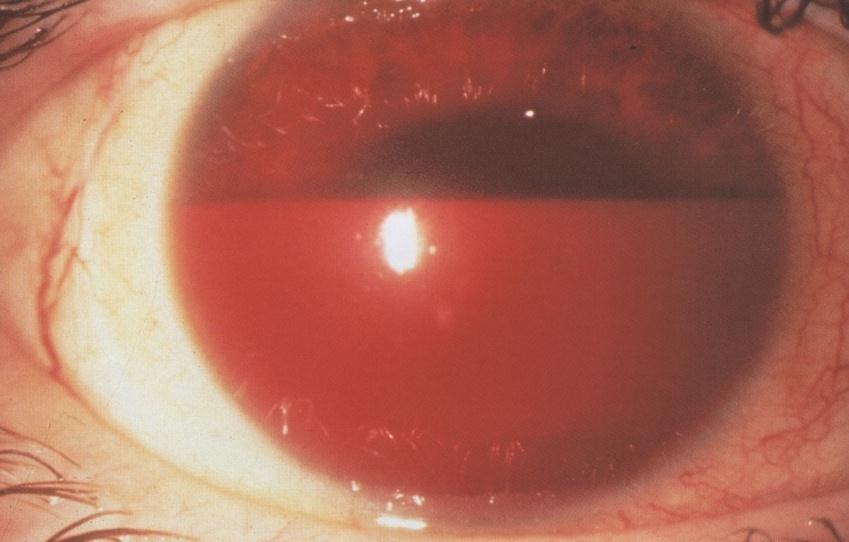
69 AC contents




70 Anterior Chamber Depth Fully illuminated = Grade4 >2/3 illuminated = Grade3 1/3-2/3 illuminated=grade2 <1/3 illuminated=grade1 DEEP AC angle DEEP AC angle Shallow AC angle Closed/very narrow AC angle Iris closer to cornea Eclipse sign
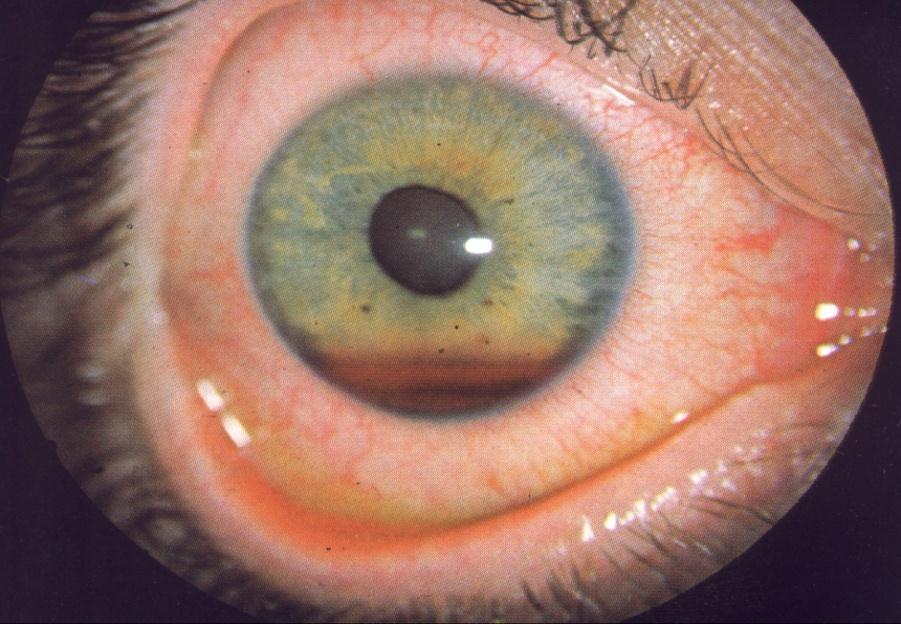
71 Iris and Pupil Look for: Size & shape of pupil margin Normal light reflex/ RAPD Distortion towards limbus ( Peaked Pupil) Iris defects Normal pupil ( Round regular reactive equal in size, no RAPD)



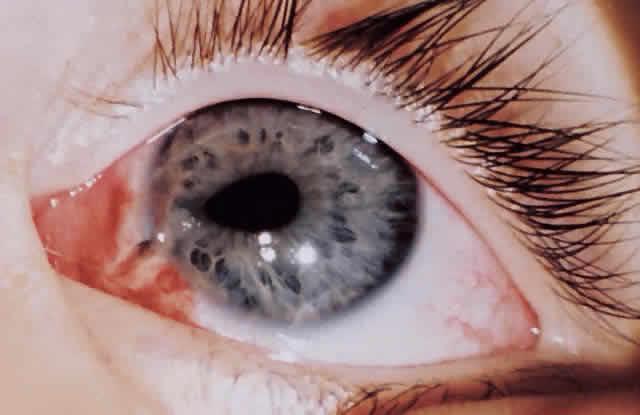
72 Traumatic iritis History of trauma is critical Presentation: photophobia in both the involved + uninvolved eye (because of consensual pupillary constriction), perilimbal injection, cells and flare in the anterior chamber.



73 Pupil Sphincter Tear Peaked Pupil

74 Iridodialysis Detachment of the iris root from the ciliary body Presentation: irregular pupil shape- D shaped, pseudopolycoria, diplopia. Be aware of other iris defects

75 Different iris colour Congenital Acquired ( History of trauma + retained iron FB)

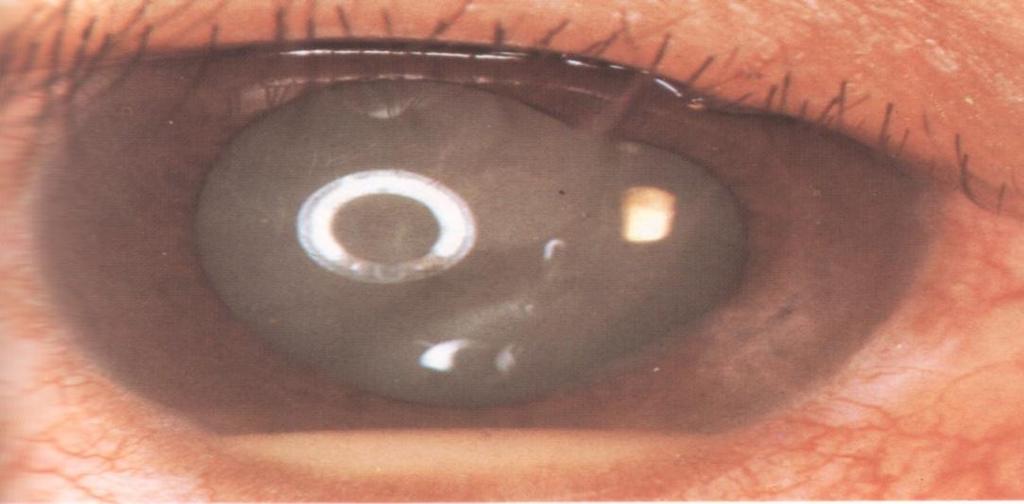
76 Lens Clarity Position In place AC PC In Pupil Stability: Tremors

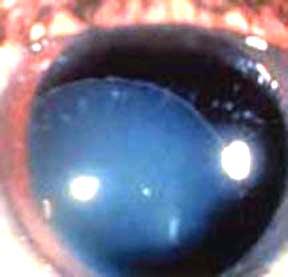
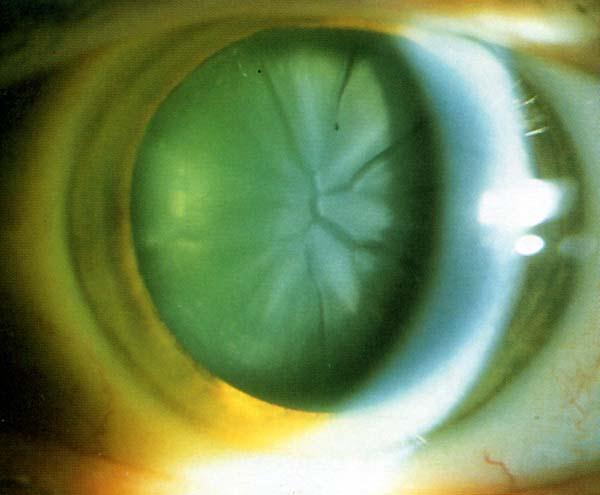
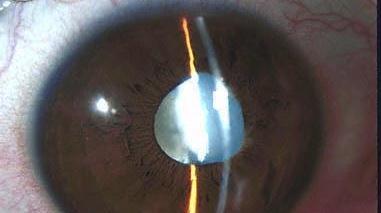

77 Clarity/Position
78
79 Posterior Segment Examination

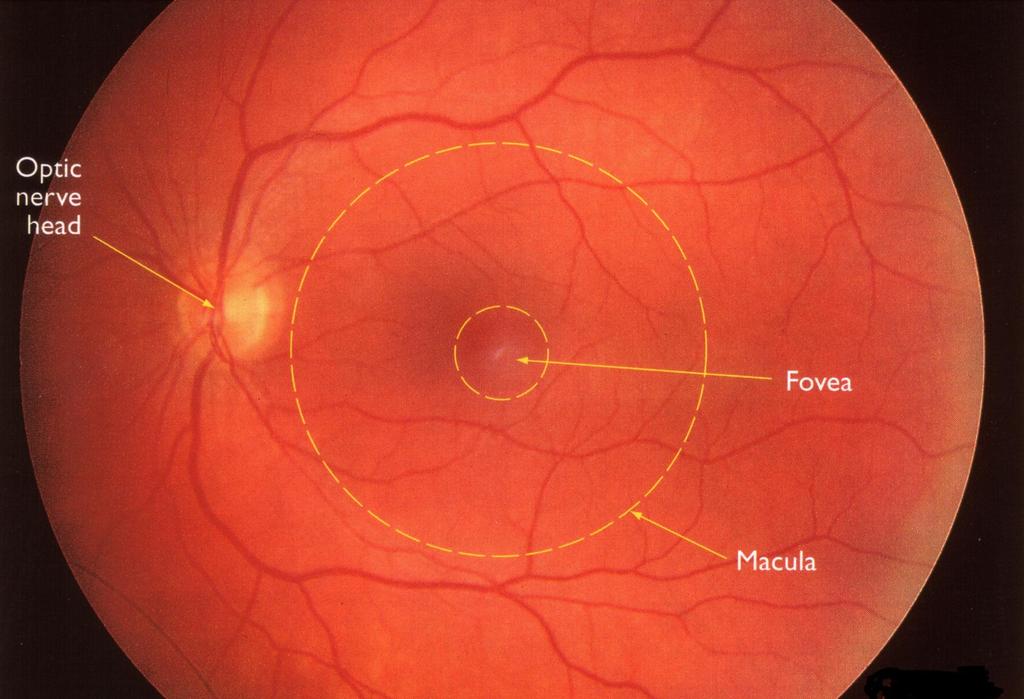
80 Posterior Segment Examination Look for: red reflex: Bright Dim Grey Absent Details: Optic nerve Retina Vessels Vitreous



81 Direct Ophthalmoscopy Get to know your scope FIRST


82 Direct Ophthalmoscopy(1) Red Reflex: With lens power of ophthalmoscope turned to 0 stand at arm's length from the patient and shine the light from the ophthalmoscope into the pupil.
.")

83 Normal red reflex: Yellow/orange/bright red glow (reflection from choroidal vessels). The area is round in shape and evenly lighted Indicates no obstruction between you and patient retina Abnormal reflex Any opacity =dark area In retinal detachment reflex appears grey instead of red


84 Do you see clear red?

85 Fundus: Direct Ophthalmoscopy(2) When you do get a red reflex, move slowly as close as possible towards patient Your forehead touches your thumb which is used to lift upper lid of eye examined.
86 Fundus: The refractive power of the examiner and patient should be compensated for by adjusting the lens power of ophthalmoscope. Ask patient to look at a distant object. For right fundus examination: Hold instrument with right hand Use your right eye Approach patient from the right side
87
88 Various Findings


89 Pre-retinal Haemorrhage/ Vitreous Hge Visual acuity can be severely reduced if it lies in front of the macula. Gravity will cause the blood to settle into the quintessential "keel-shape" with the blood being darker on the bottom. In Vitreous hge : very dim red reflex

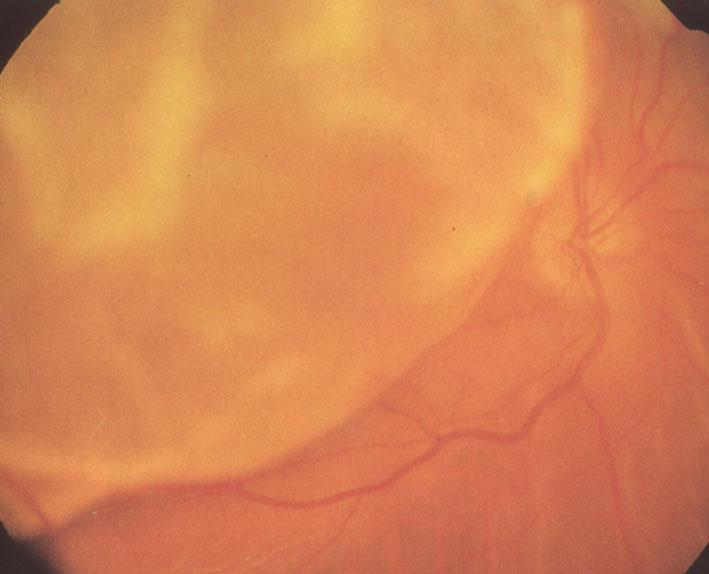
90 (Traumatic) retinal detachment

91 Purtscher's Retinopathy An injury that includes either : major chest compression (air bags) or head trauma Signs: cotton-wool spots and hemorrhages along the retinal arcades This diagnosis is driven first by history and then by the clinical presentation. Although not completely understood, Purtscher's retinopathy may be due to arterial and venous back-flow into the retinal vessels. Patients should be reassured that the condition tends to resolve without treatment, but they should be dilated every 2 to 3 weeks until resolution occurs



92 Disc oedema Optic disc atrophy


93 Optic nerve avulsion Avulsion can occur after severe trauma or relatively minor insults, but always results in devastating loss of vision.


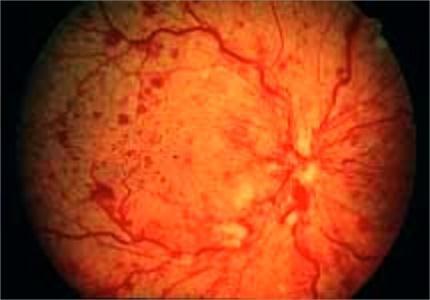
94 Central / Branch Retinal Vein Occlusion


95 Central Retinal Artery Occlusion


96 Putting it all together Know your anatomy History is of great importance Assess function of the eye VA/Pupil/VF/EOM/IOP Assess structure of eye from outside in. Lid /lacrimal/orbit Conj/sclera Cornea AC Pupil /iris Lens Red reflex /fundus

97
Acute Eyes for ED. Enis Kocak. The Alfred Ophthalmology
 Acute Eyes for ED Enis Kocak The Alfred Ophthalmology The problem with eyes Things to cover Ocular anatomy Basic assessment Common presentations Eye first aid and procedures Ophthalmic emergencies What
Acute Eyes for ED Enis Kocak The Alfred Ophthalmology The problem with eyes Things to cover Ocular anatomy Basic assessment Common presentations Eye first aid and procedures Ophthalmic emergencies What
Ophthalmic Trauma Update
 Ophthalmic Trauma Update Richard S. Davidson, M.D. Professor of Ophthalmology Vice Chair for Quality and Clinical Affairs UCHealth Eye Center University of Colorado School of Medicine August 5, 2017 Financial
Ophthalmic Trauma Update Richard S. Davidson, M.D. Professor of Ophthalmology Vice Chair for Quality and Clinical Affairs UCHealth Eye Center University of Colorado School of Medicine August 5, 2017 Financial
Ocular Urgencies and Emergencies
 Ocular Urgencies and Emergencies Pam Boyce, O.D., F.A.A.O. Boyce Family Eye Care, Ltd. 528 Devon Ave. Park Ridge, IL 60068 847-518-0303 Somebody s going to lose an eye Epidemiology 2.4 million ocular and
Ocular Urgencies and Emergencies Pam Boyce, O.D., F.A.A.O. Boyce Family Eye Care, Ltd. 528 Devon Ave. Park Ridge, IL 60068 847-518-0303 Somebody s going to lose an eye Epidemiology 2.4 million ocular and
ASSESSING THE EYES. Structures. Eyelids Extraocularmuscles Eyelashes Lacrimal glands: Lacrimal ducts Cornea Conjunctiva Sclera Pupils Iris.
 ASSESSING THE EYES Structures External Eyelids Extraocularmuscles Eyelashes Lacrimal glands: Lacrimal ducts Cornea Conjunctiva Sclera Pupils Iris 1 2 Structures Internal Optic disc Physiological cup Retinal
ASSESSING THE EYES Structures External Eyelids Extraocularmuscles Eyelashes Lacrimal glands: Lacrimal ducts Cornea Conjunctiva Sclera Pupils Iris 1 2 Structures Internal Optic disc Physiological cup Retinal
EYE TRAUMA: INCIDENCE
 Introduction EYE TRAUMA: INCIDENCE 2.5 million eye injuries per year in U.S. 40,000 60,000 of eye injuries lead to visual loss Introduction Final visual outcome of many ocular emergencies depends on prompt,
Introduction EYE TRAUMA: INCIDENCE 2.5 million eye injuries per year in U.S. 40,000 60,000 of eye injuries lead to visual loss Introduction Final visual outcome of many ocular emergencies depends on prompt,
Focusing on A&E. By Sandy Cooper, (Ophthalmic Nurse Practitioner), Tel
, Tel") Focusing on A&E By Sandy Cooper, (Ophthalmic Nurse Practitioner), Tel 01752 439331 Email sandra.cooper5@nhs.net sandracooper041@btinternet.com THINGS TO WORRY ABOUT WITH ANY EYE PROBLEM CHANGES IN VISION
Focusing on A&E By Sandy Cooper, (Ophthalmic Nurse Practitioner), Tel 01752 439331 Email sandra.cooper5@nhs.net sandracooper041@btinternet.com THINGS TO WORRY ABOUT WITH ANY EYE PROBLEM CHANGES IN VISION
Examining Children s Eyes
 Paediatric Ophthalmology What to refer & when? Aims Tips for assessing a child s eyes in general practice Common paediatric ophthalmology symptoms and signs What needs to be referred and when? MISS FARIHA
Paediatric Ophthalmology What to refer & when? Aims Tips for assessing a child s eyes in general practice Common paediatric ophthalmology symptoms and signs What needs to be referred and when? MISS FARIHA
A Case of Carotid-Cavernous Fistula
 A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
MRI masterfile Part 5 WM Heme Strokes.ppt 1
 Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
UC SF. g h. Eye Trauma. Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California
 UC SF Eye Trauma sf g h Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California Goals Recognize vision threatening eye emergencies Treat them when we can Know when
UC SF Eye Trauma sf g h Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California Goals Recognize vision threatening eye emergencies Treat them when we can Know when
EYE INJURIES OBJECTIVES COMMON EYE EMERGENCIES 7/19/2017 IMPROVE ASSESSMENT OF EYE INJURIES
 EYE INJURIES BRITTA ANDERSON D.O. DMC PRIMARY CARE SPORTS MEDICINE ASSOCIATE TEAM PHYSICIAN DETROIT TIGERS OBJECTIVES IMPROVE ASSESSMENT OF EYE INJURIES UNDERSTAND WHAT IS CONSIDERED AN EMERGENCY DEVELOP
EYE INJURIES BRITTA ANDERSON D.O. DMC PRIMARY CARE SPORTS MEDICINE ASSOCIATE TEAM PHYSICIAN DETROIT TIGERS OBJECTIVES IMPROVE ASSESSMENT OF EYE INJURIES UNDERSTAND WHAT IS CONSIDERED AN EMERGENCY DEVELOP
Management of specific eye problems in the ED
 of specific eye problems in the ED CORNEAL ABRASION Causes Foreign bodies Tangential shearing injuries, e.g. poking finger into eye Exact cause of injury (Remember to exclude possibility of intraocular
of specific eye problems in the ED CORNEAL ABRASION Causes Foreign bodies Tangential shearing injuries, e.g. poking finger into eye Exact cause of injury (Remember to exclude possibility of intraocular
Ophthalmology. Corneal Abrasion. History
 Ophthalmology Corneal Abrasion - Usually clear history of very recent trauma - Foreign Body Sensation - Pain +++ - Lacrimation - Photophobia Fig. 1 Corneal Abrasion - Abrasion stains yellow / green with
Ophthalmology Corneal Abrasion - Usually clear history of very recent trauma - Foreign Body Sensation - Pain +++ - Lacrimation - Photophobia Fig. 1 Corneal Abrasion - Abrasion stains yellow / green with
Assessment and Management of Ocular Trauma. Disclosure I have no direct financial interests in today s subject matter. 3/25/2019. Normal Eye Anatomy
 Assessment and Management of Ocular Trauma Samiksha Fouzdar Jain, MD,FRCS Department of Ophthalmology & Visual Sciences Truhlsen Eye Institute Disclosure I have no direct financial interests in today s
Assessment and Management of Ocular Trauma Samiksha Fouzdar Jain, MD,FRCS Department of Ophthalmology & Visual Sciences Truhlsen Eye Institute Disclosure I have no direct financial interests in today s
OPHTHALMOLOGY REFERRAL GUIDE FOR GPS
 OPHTHALMOLOGY REFERRAL GUIDE FOR GPS A guidebook to support general practitioners in the management and referral of a range of common eye problems. Contents 3 Introduction 4 Ophthalmic Workup 6 Acute Visual
OPHTHALMOLOGY REFERRAL GUIDE FOR GPS A guidebook to support general practitioners in the management and referral of a range of common eye problems. Contents 3 Introduction 4 Ophthalmic Workup 6 Acute Visual
Clues of a Ruptured Globe
 Definition any eye that has sustained a full thickness traumatic disruption of the cornea or sclera Overwhelmingly, rupture accidents occur in young men, small children and the elderly Corneal laceration
Definition any eye that has sustained a full thickness traumatic disruption of the cornea or sclera Overwhelmingly, rupture accidents occur in young men, small children and the elderly Corneal laceration
By Darlene Jones, Nurse. May 2017
 By Darlene Jones, Nurse May 2017 Disclosure of potential conflict of interest Darlene Jones, Nurse I have no conflict of interest Course objectives Become familiar with the different pathologies in ophthalmology
By Darlene Jones, Nurse May 2017 Disclosure of potential conflict of interest Darlene Jones, Nurse I have no conflict of interest Course objectives Become familiar with the different pathologies in ophthalmology
Ocular and periocular trauma
 Ocular and periocular trauma No financial disclosures. Tina Rutar M.D. Assistant Professor of Clinical Ophthalmology and Pediatrics Director, Visual Center for the Child University of California San Francisco
Ocular and periocular trauma No financial disclosures. Tina Rutar M.D. Assistant Professor of Clinical Ophthalmology and Pediatrics Director, Visual Center for the Child University of California San Francisco
Ocular Lecture. Sue Bednar NP Ali Atwater PA-C
 Ocular Lecture Sue Bednar NP Ali Atwater PA-C Triaging Ocular Complaints Painful Eye/Red eye +/-blurry vision +/-visual loss +/-floaters +/-fevers If any of the above findings exist, pt is likely to have
Ocular Lecture Sue Bednar NP Ali Atwater PA-C Triaging Ocular Complaints Painful Eye/Red eye +/-blurry vision +/-visual loss +/-floaters +/-fevers If any of the above findings exist, pt is likely to have
Paediatric acute ophthalmology. Harry Bradshaw
 Paediatric acute ophthalmology Harry Bradshaw Approach Red eye Leukocoria Neurological Trauma Visual loss Red eye Orbital Eyelid Conjunctiva Cornea Uvea Orbital Orbit fixed volume Contiguous with sinuses,
Paediatric acute ophthalmology Harry Bradshaw Approach Red eye Leukocoria Neurological Trauma Visual loss Red eye Orbital Eyelid Conjunctiva Cornea Uvea Orbital Orbit fixed volume Contiguous with sinuses,
LECTURE # 7 EYECARE REVIEW: PART III
 LECTURE # 7 EYECARE REVIEW: PART III HOW TO TRIAGE EYE EMERGENCIES STEVE BUTZON, O.D. EYECARE REVIEW: HOW TO TRIAGE EYE EMERGENCIES FOR PRIMARY CARE PHYSICIANS Steve Butzon, O.D. Member Director IDOC President
LECTURE # 7 EYECARE REVIEW: PART III HOW TO TRIAGE EYE EMERGENCIES STEVE BUTZON, O.D. EYECARE REVIEW: HOW TO TRIAGE EYE EMERGENCIES FOR PRIMARY CARE PHYSICIANS Steve Butzon, O.D. Member Director IDOC President
Identify the choice that best completes the statement or answers the question.
 Chapter 5. The Eye Multiple Choice Identify the choice that best completes the statement or answers the question. 1. The most common type of eye disorder is: A. Refractive errors B. Macular conditions
Chapter 5. The Eye Multiple Choice Identify the choice that best completes the statement or answers the question. 1. The most common type of eye disorder is: A. Refractive errors B. Macular conditions
Year 2 MBChB Clinical Skills Session Ophthalmoscopy. Reviewed & ratified by: Mr M Batterbury Consultant Ophthalmologist
 Year 2 MBChB Clinical Skills Session Ophthalmoscopy Reviewed & ratified by: o Mr M Batterbury Consultant Ophthalmologist Learning objectives o To understand the anatomy and physiology of the external and
Year 2 MBChB Clinical Skills Session Ophthalmoscopy Reviewed & ratified by: o Mr M Batterbury Consultant Ophthalmologist Learning objectives o To understand the anatomy and physiology of the external and
Scrub In. What is the function of vitreous humor? What does the pupil do when exposed to bright light? a. Maintain eye shape and provide color vision
 Scrub In What is the function of vitreous humor? a. Maintain eye shape and provide color vision b. Maintain eye shape and refract light rays c. Provide night vision and color vision d. Provide night vision
Scrub In What is the function of vitreous humor? a. Maintain eye shape and provide color vision b. Maintain eye shape and refract light rays c. Provide night vision and color vision d. Provide night vision
Differential diagnosis of the red eye. Carol Slight Nurse Practitioner Ophthalmology
 Differential diagnosis of the red eye Carol Slight Nurse Practitioner Ophthalmology The red eye Conjunctivitis HSV Keratitis Acute angle closure glaucoma Anterior Uveitis Red eye Scleritis Subconjunctival
Differential diagnosis of the red eye Carol Slight Nurse Practitioner Ophthalmology The red eye Conjunctivitis HSV Keratitis Acute angle closure glaucoma Anterior Uveitis Red eye Scleritis Subconjunctival
Ocular and Periocular Trauma. Tina Rutar, MD. Assistant Professor of Ophthalmology and Pediatrics. Director, Visual Center for the Child
 Ocular and Periocular Trauma Tina Rutar, MD Assistant Professor of Ophthalmology and Pediatrics Director, Visual Center for the Child University of California, San Francisco Phone: 415-353-2560 Fax: 415-353-2468
Ocular and Periocular Trauma Tina Rutar, MD Assistant Professor of Ophthalmology and Pediatrics Director, Visual Center for the Child University of California, San Francisco Phone: 415-353-2560 Fax: 415-353-2468
Orbital and Ocular Adnexal Disorders with Red Eyes
 Orbital and Ocular Adnexal Disorders with Red Eyes Jason Lee Associate Consultant Department of Ophthalmology and Visual Sciences Practical Ophthalmology for the Family Physician 21 Jan 2017 No financial
Orbital and Ocular Adnexal Disorders with Red Eyes Jason Lee Associate Consultant Department of Ophthalmology and Visual Sciences Practical Ophthalmology for the Family Physician 21 Jan 2017 No financial
Eyes, ears, teeth and everything in between
 Eyes, ears, teeth and everything in between E M E R G E N C Y D E P A R T M E N T J U N I O R T E A C H created 14/11/10 by S.R. Bruijns, version 1.0 Objectives Eyes Ears Teeth Maxilla- facial EYES Approaching
Eyes, ears, teeth and everything in between E M E R G E N C Y D E P A R T M E N T J U N I O R T E A C H created 14/11/10 by S.R. Bruijns, version 1.0 Objectives Eyes Ears Teeth Maxilla- facial EYES Approaching
Ocular Emergencies. What is an emergency to the patient is not necessarily an emergency to the staff
 OCULAR EMERGENCIES Ophthalmic Photographers Society November 15, 2013 Michael A. DellaVecchia MD PhD FACS Wills Eye Emergency Department Philadelphia PA Ocular Emergencies What is an emergency to the patient
OCULAR EMERGENCIES Ophthalmic Photographers Society November 15, 2013 Michael A. DellaVecchia MD PhD FACS Wills Eye Emergency Department Philadelphia PA Ocular Emergencies What is an emergency to the patient
2/5/2018. Trauma. Subdivided into two main categories: Closed globe Open Globe
 1 2 3 4 5 Ocular Trauma Guide for Eye Care Office Staff Winter Thaw 2018 Aaron Yatskevich OD Definition A broad term used to describe a physical or chemical wound to the eye or eye socket. Ocular trauma
1 2 3 4 5 Ocular Trauma Guide for Eye Care Office Staff Winter Thaw 2018 Aaron Yatskevich OD Definition A broad term used to describe a physical or chemical wound to the eye or eye socket. Ocular trauma
THE 35 GOLDEN EYE RULES
 THE 35 GOLDEN EYE RULES The Sense of Sight, from La Dame a la Licorne, The Lady and the Unicorn Tapestries, Late 15th Century Flemish Tapestry in wool and silk, Musée Nationale du Moyen Age, Paris. 1.
THE 35 GOLDEN EYE RULES The Sense of Sight, from La Dame a la Licorne, The Lady and the Unicorn Tapestries, Late 15th Century Flemish Tapestry in wool and silk, Musée Nationale du Moyen Age, Paris. 1.
Eye Trauma. Lid Laceration. Orbital Fracture
 Eye Trauma Lid Laceration The presence of a lid laceration, however insignificant, mandates careful exploration of the wound and examination of the globe. 1. Superficial lacerations parallel to the lid
Eye Trauma Lid Laceration The presence of a lid laceration, however insignificant, mandates careful exploration of the wound and examination of the globe. 1. Superficial lacerations parallel to the lid
MRI masterfile Part 5 WM Heme Strokes.ppt 2
 Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
Ocular warning signs in GP practice: Paediatric Eye Pointers
 Ocular warning signs in GP practice: Paediatric Eye Pointers Dr Benjamin Chang MB, BCh, BAO, MMedSci, FRCS(Irel), FRCS(Edin), FRCOphth(Lond) Senior Consultant Ophthalmology and Visual Sciences Khoo Teck
Ocular warning signs in GP practice: Paediatric Eye Pointers Dr Benjamin Chang MB, BCh, BAO, MMedSci, FRCS(Irel), FRCS(Edin), FRCOphth(Lond) Senior Consultant Ophthalmology and Visual Sciences Khoo Teck
Ocular Anatomy for the Paraoptometric
 Ocular Anatomy for the Paraoptometric Minnesota Optometric Association Paraoptometric CE Friday September 30, 2016 Lindsay A. Sicks, OD, FAAO Assistant Professor, Illinois College of Optometry lsicks@ico.edu
Ocular Anatomy for the Paraoptometric Minnesota Optometric Association Paraoptometric CE Friday September 30, 2016 Lindsay A. Sicks, OD, FAAO Assistant Professor, Illinois College of Optometry lsicks@ico.edu
Phone Triage for Optometric Staff ???????? CHEMICAL BURN CHEMICAL BURN
 Phone Triage for Optometric Staff There are very few ocular emergencies that you will have to deal with in practice, but it is imperative that you be able to Michelle Welch, O.D. NSU Oklahoma College of
Phone Triage for Optometric Staff There are very few ocular emergencies that you will have to deal with in practice, but it is imperative that you be able to Michelle Welch, O.D. NSU Oklahoma College of
PEDIATRIC OCULAR INJURIES. Sapna Tibrewal MD
 PEDIATRIC OCULAR INJURIES Sapna Tibrewal MD 1 Learning Objectives Learn to recognize the common pediatric ocular injuries Immediate management tips to be instituted in your office/ ER Know when to call
PEDIATRIC OCULAR INJURIES Sapna Tibrewal MD 1 Learning Objectives Learn to recognize the common pediatric ocular injuries Immediate management tips to be instituted in your office/ ER Know when to call
For details on measurement and recording of visual acuity, refer to Annex 1. VISION INTERPRETING RESULTS ABSTRACT
 management update on functional decline in older adults 2012 Unit No. 5 VISION Dr Au Eong Kah Guan, Ms Yulianti, Ms Fifiana ABSTRACT Among Singaporean adults of Chinese origin aged 40 to 79 years old,
management update on functional decline in older adults 2012 Unit No. 5 VISION Dr Au Eong Kah Guan, Ms Yulianti, Ms Fifiana ABSTRACT Among Singaporean adults of Chinese origin aged 40 to 79 years old,
Ears. Mouth. Jowls 6 Major Bones of the Face Nasal bone Two
 1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
GNK485 The eye and related structures. Prof MC Bosman 2012
 GNK485 The eye and related structures Prof MC Bosman 2012 Surface anatomy Bony orbit Eyeball and Lacrimal apparatus Extra-ocular muscles Movements of the eye Innervation Arterial supply and venous drainage
GNK485 The eye and related structures Prof MC Bosman 2012 Surface anatomy Bony orbit Eyeball and Lacrimal apparatus Extra-ocular muscles Movements of the eye Innervation Arterial supply and venous drainage
Year 1 MBChB Clinical Skills Session Ophthalmoscopy
 Year 1 MBChB Clinical Skills Session Ophthalmoscopy Reviewed & ratified by: Dr V Taylor-Jones, Mr M Batterbury Consultant Ophthalmologist Learning objectives o To understand the anatomy and physiology
Year 1 MBChB Clinical Skills Session Ophthalmoscopy Reviewed & ratified by: Dr V Taylor-Jones, Mr M Batterbury Consultant Ophthalmologist Learning objectives o To understand the anatomy and physiology
Around The Globe in 60 Minutes
 Around The Globe in 60 Minutes Around the GLOBE in Sixty Minutes Basic Ocular Anatomy, Examination, and Diagnostic Techniques Introduction Focusing on canine and feline ocular anatomy and basic examination
Around The Globe in 60 Minutes Around the GLOBE in Sixty Minutes Basic Ocular Anatomy, Examination, and Diagnostic Techniques Introduction Focusing on canine and feline ocular anatomy and basic examination
CENTRAL MERSEY LOCAL OPTICAL COMMITTEE
 CENTRAL MERSEY LOCAL OPTICAL COMMITTEE OPTOMETRIC REFERRAL GUIDELINES The ocular conditions listed in this document are intended to reflect those that might be encountered in optometric practice and this
CENTRAL MERSEY LOCAL OPTICAL COMMITTEE OPTOMETRIC REFERRAL GUIDELINES The ocular conditions listed in this document are intended to reflect those that might be encountered in optometric practice and this
Work Sheet And Course Hand Out
 Work Sheet And Course Hand Out This course provides the primary care health professional with a basic understanding of the eye, its function and the assessment of common sight- and non-sight threatening
Work Sheet And Course Hand Out This course provides the primary care health professional with a basic understanding of the eye, its function and the assessment of common sight- and non-sight threatening
Dr Jo-Anne Pon. Dr Sean Every. 8:30-9:25 WS #70: Eye Essentials for GPs 9:35-10:30 WS #80: Eye Essentials for GPs (Repeated)
") Dr Sean Every Ophthalmologist Southern Eye Specialists Christchurch Dr Jo-Anne Pon Ophthalmologist Southern Eye Specialists, Christchurch Hospital, Christchurch 8:30-9:25 WS #70: Eye Essentials for GPs
Dr Sean Every Ophthalmologist Southern Eye Specialists Christchurch Dr Jo-Anne Pon Ophthalmologist Southern Eye Specialists, Christchurch Hospital, Christchurch 8:30-9:25 WS #70: Eye Essentials for GPs
Bony orbit Roof The orbital plate of the frontal bone Lateral wall: the zygomatic bone and the greater wing of the sphenoid
 Bony orbit Roof: Formed by: The orbital plate of the frontal bone, which separates the orbital cavity from the anterior cranial fossa and the frontal lobe of the cerebral hemisphere Lateral wall: Formed
Bony orbit Roof: Formed by: The orbital plate of the frontal bone, which separates the orbital cavity from the anterior cranial fossa and the frontal lobe of the cerebral hemisphere Lateral wall: Formed
02/03/2014. Average Length: 23mm (Infant ~16mm) Approximately the size of a quarter Volume: ~5mL
 Approximately the size of a quarter Volume: ~5mL") Identify the anatomy of the eye. Explain the basic physiology of the parts of the eye. Briefly discuss various surgeries related to different parts of the anatomy. Average Length: 23mm (Infant ~16mm) Approximately
Identify the anatomy of the eye. Explain the basic physiology of the parts of the eye. Briefly discuss various surgeries related to different parts of the anatomy. Average Length: 23mm (Infant ~16mm) Approximately
10/4/2013. Bruce K.Williams, MSN, RN,ACNP-BC Sisters of Charity Providence Hospitals. What is the worst thing that can go wrong with an eye?
 Red Eyes, Red Alert! Bruce K.Williams, MSN, RN,ACNP-BC Sisters of Charity Providence Hospitals Red Eyes, Red Alert! Red Eyes, Red Alert! What is the worst thing that can go wrong with an eye? 1 Red Eyes,
Red Eyes, Red Alert! Bruce K.Williams, MSN, RN,ACNP-BC Sisters of Charity Providence Hospitals Red Eyes, Red Alert! Red Eyes, Red Alert! What is the worst thing that can go wrong with an eye? 1 Red Eyes,
OPHTHALMOLOGY DEPARTMENT Primary care referral guidelines
 OPHTHALMOLOGY DEPARTMENT Primary care referral guidelines Contents REFERRAL CATEGIES... 2 Emergency... 2 Urgent... 2 Semi urgent/routine... 2 Not accepted... 2 OPHTHALMOLOGY CONDITIONS NOT ACCEPTED...
OPHTHALMOLOGY DEPARTMENT Primary care referral guidelines Contents REFERRAL CATEGIES... 2 Emergency... 2 Urgent... 2 Semi urgent/routine... 2 Not accepted... 2 OPHTHALMOLOGY CONDITIONS NOT ACCEPTED...
9/23/2014. Emily Thomas, O.D. MOA Paraoptometric Education October 5, 2014
 Emily Thomas, O.D. MOA Paraoptometric Education October 5, 2014 Anterior toward the front of the body Posterior toward the rear of the body Unilateral only one eye involved Bilateral both eyes involved
Emily Thomas, O.D. MOA Paraoptometric Education October 5, 2014 Anterior toward the front of the body Posterior toward the rear of the body Unilateral only one eye involved Bilateral both eyes involved
Anatomy: There are 6 muscles that move your eye.
 Thyroid Eye Disease Your doctor thinks you have thyroid orbitopathy. This is an autoimmune condition where your body's immune system is producing factors that stimulate enlargement of the muscles that
Thyroid Eye Disease Your doctor thinks you have thyroid orbitopathy. This is an autoimmune condition where your body's immune system is producing factors that stimulate enlargement of the muscles that
JINNAH SINDH MEDICAL UNIVERSITY STUDY GUIDE- OPHTHALMOLOGY YEAR 4,
 INTRODUCTION Pakistan, the 7th most populous country in the world, has an urban population of 38.8% and rural dwellers of 61.2%. The country has faced challenges with vision impairment and blindness as
INTRODUCTION Pakistan, the 7th most populous country in the world, has an urban population of 38.8% and rural dwellers of 61.2%. The country has faced challenges with vision impairment and blindness as
OCCLUSIVE VASCULAR DISORDERS OF THE RETINA
 OCCLUSIVE VASCULAR DISORDERS OF THE RETINA Learning outcomes By the end of this lecture the students would be able to Classify occlusive vascular disorders (OVD) of the retina. Correlate the clinical features
OCCLUSIVE VASCULAR DISORDERS OF THE RETINA Learning outcomes By the end of this lecture the students would be able to Classify occlusive vascular disorders (OVD) of the retina. Correlate the clinical features
Ocular Trauma. Breaking Down Blunt. Blunt ocular trauma occurs frequently in sporting
 Focus on CME at the University of Saskatchewan Breaking Down Blunt Ocular Trauma By Dan Ash, MD, BA, FRCSC, FACS, FAAO Blunt ocular trauma occurs frequently in sporting activities, as well as in industrial
Focus on CME at the University of Saskatchewan Breaking Down Blunt Ocular Trauma By Dan Ash, MD, BA, FRCSC, FACS, FAAO Blunt ocular trauma occurs frequently in sporting activities, as well as in industrial
Flashers and Floaters
 Flashers and Floaters Introduction Sometimes people see small, moving spots or specks in their field of vision. These sensations are called floaters. About 7 out of 10 people experience floaters at some
Flashers and Floaters Introduction Sometimes people see small, moving spots or specks in their field of vision. These sensations are called floaters. About 7 out of 10 people experience floaters at some
Imaging Orbit/Periorbital Injury
 Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
Sepideh Tara Rousta, MD FAAO Robert Wood Johnson University Hospital Saint Peter s University Hospital Wills Eye Hospital
 Sepideh Tara Rousta, MD FAAO Robert Wood Johnson University Hospital Saint Peter s University Hospital Wills Eye Hospital 14 mo old w R eye cross (parents) 9 mo old R eye crossing getting worse for past
Sepideh Tara Rousta, MD FAAO Robert Wood Johnson University Hospital Saint Peter s University Hospital Wills Eye Hospital 14 mo old w R eye cross (parents) 9 mo old R eye crossing getting worse for past
Carotid Cavernous Fistula
 Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
Test Bank for Medical Surgical Nursing An Integrated Approach 3rd Edition by White
 Test Bank for Medical Surgical Nursing An Integrated Approach 3rd Edition by White Link full download : http://testbankair.com/download/test-bank-for-medical-surgical-nursing-anintegrated-approach-3rd-edition-by-white/
Test Bank for Medical Surgical Nursing An Integrated Approach 3rd Edition by White Link full download : http://testbankair.com/download/test-bank-for-medical-surgical-nursing-anintegrated-approach-3rd-edition-by-white/
Maxillofacial and Ocular Injuries
 Maxillofacial and Ocular Injuries Objectives At the conclusion of this presentation the participant will be able to: Identify the key anatomical structures of the face and eye and the impact of force on
Maxillofacial and Ocular Injuries Objectives At the conclusion of this presentation the participant will be able to: Identify the key anatomical structures of the face and eye and the impact of force on
Injury. Contusion Lamellar Laceration Laceration Rupture. Penetrating IOFB. Perforating
 Mechanical Ocular Trauma Došková Hana, MD. Department of Ophthalmology Medicine Faculty of Masaryk University Brno General Considerations Ocular trauma constitude about 6% of all injuries, but eyes set
Mechanical Ocular Trauma Došková Hana, MD. Department of Ophthalmology Medicine Faculty of Masaryk University Brno General Considerations Ocular trauma constitude about 6% of all injuries, but eyes set
Eye Examination Techniques in Horses
 Eye Examination Techniques in Horses Dennis E. Brooks DVM, PhD Dip ACVO University of Florida brooksd@mail.vetmed.ufl.edu Basic Instruments How to tell the potential of vision? PLRs (retina, CN 2, chiasm,
Eye Examination Techniques in Horses Dennis E. Brooks DVM, PhD Dip ACVO University of Florida brooksd@mail.vetmed.ufl.edu Basic Instruments How to tell the potential of vision? PLRs (retina, CN 2, chiasm,
Cataract. What is a Cataract?
 Cataract What is a Cataract? We all have a lens in our eye. This is positioned just behind the iris, which is the coloured ring in the eye that gives your eye its colour. The lens s function is to focus
Cataract What is a Cataract? We all have a lens in our eye. This is positioned just behind the iris, which is the coloured ring in the eye that gives your eye its colour. The lens s function is to focus
Mild NPDR. Moderate NPDR. Severe NPDR
 Diabetic retinopathy Diabetic retinopathy is the most common cause of blindness in adults aged 35-65 years-old. Hyperglycaemia is thought to cause increased retinal blood flow and abnormal metabolism in
Diabetic retinopathy Diabetic retinopathy is the most common cause of blindness in adults aged 35-65 years-old. Hyperglycaemia is thought to cause increased retinal blood flow and abnormal metabolism in
PAINFUL PAINLESS Contact lens user BOV
 Common Causes Allergies Infections Ocular Cornea, uveitis, endophthalmitis Orbital Orbital cellulitis Inflammation Uveitis Scleritis / episcleritis Glaucomas Trauma Foreign bodies Chemical injuries History
Common Causes Allergies Infections Ocular Cornea, uveitis, endophthalmitis Orbital Orbital cellulitis Inflammation Uveitis Scleritis / episcleritis Glaucomas Trauma Foreign bodies Chemical injuries History
For further reading we recommend the following excellent textbooks:
 FURTHER READING Intravitreal Injections Downloaded from www.worldscientific.com For further reading we recommend the following excellent textbooks: Clinical Anatomy of the Eye by Richard S Snell and Michael
FURTHER READING Intravitreal Injections Downloaded from www.worldscientific.com For further reading we recommend the following excellent textbooks: Clinical Anatomy of the Eye by Richard S Snell and Michael
SILA THONGLAI MD. Bangkok Eye center Bangkok Hospital Thailand
 SILA THONGLAI MD. Bangkok Eye center Bangkok Hospital Thailand Ocular Anatomy Bony Components of Orbit 1 1. Frontal bone 4 5 7 6 2. Zygomatic bone 3. Maxillary bone 4. Sphenoid bone 5. Ethmoid bone 2 3
SILA THONGLAI MD. Bangkok Eye center Bangkok Hospital Thailand Ocular Anatomy Bony Components of Orbit 1 1. Frontal bone 4 5 7 6 2. Zygomatic bone 3. Maxillary bone 4. Sphenoid bone 5. Ethmoid bone 2 3
3/16/2018. Optic Nerve Examination. Hassan Eisa Swify FRCS Ed (Ophthalmology) Air Force Hospital
 Air Force Hospital") Optic Nerve Examination Hassan Eisa Swify FRCS Ed (Ophthalmology) Air Force Hospital 1 Examination Structure ( optic disc) Function Examination of the optic disc The only cranial nerve (brain tract) which
Optic Nerve Examination Hassan Eisa Swify FRCS Ed (Ophthalmology) Air Force Hospital 1 Examination Structure ( optic disc) Function Examination of the optic disc The only cranial nerve (brain tract) which
Clinical Approach To Refractive Errors. Dr. Faizur Rahman Associate Professor Peshawar Medical College
 Clinical Approach To Refractive Errors Dr. Faizur Rahman Associate Professor Peshawar Medical College Learning objectives By the end of this lecture the students would be able to; Correlate optics with
Clinical Approach To Refractive Errors Dr. Faizur Rahman Associate Professor Peshawar Medical College Learning objectives By the end of this lecture the students would be able to; Correlate optics with
PRECISION PROGRAM. Injection Technique Quick-Reference Guide. Companion booklet for the Video Guide to Injection Technique
 Injection Technique Quick-Reference Guide PRECISION PROGRAM Companion booklet for the Video Guide to Injection Technique Available at www.ozurdexprecisionprogram.com Provides step-by-step directions with
Injection Technique Quick-Reference Guide PRECISION PROGRAM Companion booklet for the Video Guide to Injection Technique Available at www.ozurdexprecisionprogram.com Provides step-by-step directions with
Handbook for Medical Students Learning Ophthalmology
 International Council of Ophthalmology Handbook for Medical Students Learning Ophthalmology 2009 Compiled by the Task Force on Undergraduate Teaching in Ophthalmology of the International Council of Ophthalmology
International Council of Ophthalmology Handbook for Medical Students Learning Ophthalmology 2009 Compiled by the Task Force on Undergraduate Teaching in Ophthalmology of the International Council of Ophthalmology
Cataract. What is a Cataract?
 Cataract What is a Cataract? We all have a lens in our eye. This is positioned just behind the iris, which is the coloured ring in the eye that gives your eye its colour. The lens function is to focus
Cataract What is a Cataract? We all have a lens in our eye. This is positioned just behind the iris, which is the coloured ring in the eye that gives your eye its colour. The lens function is to focus
Fast Facts. Fast Facts: Ophthalmology. Peter Simcock and Andre Burger. Second edition
 Fast Facts Fast Facts: Ophthalmology Peter Simcock and Andre Burger Second edition A fantastic companion for all clinicians involved in primary eye care. Dr Amit Jinabhai, Lecturer in Optometry, University
Fast Facts Fast Facts: Ophthalmology Peter Simcock and Andre Burger Second edition A fantastic companion for all clinicians involved in primary eye care. Dr Amit Jinabhai, Lecturer in Optometry, University
Ocular Emergencies. Pisit Preechawat, MD Department of Ophthalmology, Ramathibodi Hospital
 Ocular Emergencies Pisit Preechawat, MD Department of Ophthalmology, Ramathibodi Hospital Ocular Anatomy Bony Components of Orbit 1 1. Frontal bone 4 5 7 6 2. Zygomatic bone 3. Maxillary bone 4. Sphenoid
Ocular Emergencies Pisit Preechawat, MD Department of Ophthalmology, Ramathibodi Hospital Ocular Anatomy Bony Components of Orbit 1 1. Frontal bone 4 5 7 6 2. Zygomatic bone 3. Maxillary bone 4. Sphenoid
Dry Eye Assessment and Management Study ELIGIBILITY OCULAR EVALUATION FORM
 Page 1 of 13 BEFORE COMPLETING THE OCULAR EXAMINATION, YOU MUST BE ABLE TO ANSWER YES TO THE FOLLOWING QUESTIONS: Have you done MMP9? (SVonly) The Following are done at Baseline: Have you done Tear Osmolarity?
Page 1 of 13 BEFORE COMPLETING THE OCULAR EXAMINATION, YOU MUST BE ABLE TO ANSWER YES TO THE FOLLOWING QUESTIONS: Have you done MMP9? (SVonly) The Following are done at Baseline: Have you done Tear Osmolarity?
Acute Ophthalmology for A&E Practice
 Acute Ophthalmology for A&E Practice Dr. LEUNG Yu-lung, Dexter MBChB, BMedSci(Hons),FRCS (Glas),MRCS(Edin), DRCOphth(London),FCOphthHK, FHKAM(Ophth) Associate Consultant Clinical Assistant Professor (Honorary)
Acute Ophthalmology for A&E Practice Dr. LEUNG Yu-lung, Dexter MBChB, BMedSci(Hons),FRCS (Glas),MRCS(Edin), DRCOphth(London),FCOphthHK, FHKAM(Ophth) Associate Consultant Clinical Assistant Professor (Honorary)
Glaucoma. Cornea. Iris
 Glaucoma Introduction Glaucoma is a group of eye diseases that can lead to blindness if not treated. Openangle glaucoma, the most common form of glaucoma, affects about 3 million Americans. Half of those
Glaucoma Introduction Glaucoma is a group of eye diseases that can lead to blindness if not treated. Openangle glaucoma, the most common form of glaucoma, affects about 3 million Americans. Half of those
ation is essential. Whether on the playing it is important to keep in mind that severe
 JENNIFER LAIO, MD, and BRUCE M. ZAGELBAUM, MD NYU School of Medicine, Manhasset, NY North Shore University Hospital, Eye injuries sustained in sports and recreational activities are common in the United
JENNIFER LAIO, MD, and BRUCE M. ZAGELBAUM, MD NYU School of Medicine, Manhasset, NY North Shore University Hospital, Eye injuries sustained in sports and recreational activities are common in the United
Case #1: 68 M with floaters OS
 Case #1: 68 M with floaters OS Point-of-Care Ocular Sonography for the Emergency Department Nate Teismann MD Dept of Emergency Medicine, UCSF Topics in EM 2012 Acute onset of dark spots in L eye 2 days
Case #1: 68 M with floaters OS Point-of-Care Ocular Sonography for the Emergency Department Nate Teismann MD Dept of Emergency Medicine, UCSF Topics in EM 2012 Acute onset of dark spots in L eye 2 days
Pupil Exams and Visual Fields
 Pupil Exams and Visual Fields A Closer Look at Cranial Nerves No Financial Interests Amy Jost does not have any financial interests related to this presentation AMY JOST, BS, COMT, CCRC, OSC CINCINNATI
Pupil Exams and Visual Fields A Closer Look at Cranial Nerves No Financial Interests Amy Jost does not have any financial interests related to this presentation AMY JOST, BS, COMT, CCRC, OSC CINCINNATI
Faculty Financial Disclosure. Learning Objectives: Office Ophthalmology. Basic Eye Exam: What s in your pocket/office? Office Ophthalmology
 Faculty Financial Disclosure Office Ophthalmology Lynn K. Gordon, MD, PhD, has no financial relationships to disclose. Lynn K. Gordon, MD, PhD Professor and Vernon O Underwood Family Chair Department of
Faculty Financial Disclosure Office Ophthalmology Lynn K. Gordon, MD, PhD, has no financial relationships to disclose. Lynn K. Gordon, MD, PhD Professor and Vernon O Underwood Family Chair Department of
Ocular Injuries in Sports. Rance McClain, D.O. Associate Dean, Clinical Sciences William Carey University FM/NMM-OMM/Sports Medicine
 Ocular Injuries in Sports Rance McClain, D.O. Associate Dean, Clinical Sciences William Carey University FM/NMM-OMM/Sports Medicine http://sudc.org/vienna/ Learning Objectives 1. Know the sport classification
Ocular Injuries in Sports Rance McClain, D.O. Associate Dean, Clinical Sciences William Carey University FM/NMM-OMM/Sports Medicine http://sudc.org/vienna/ Learning Objectives 1. Know the sport classification
Global Health Implementation & Vision 2020 Links. Global Health Implementation & Vision 2020 Links. University of St Andrews & NHS Fife/Lothian
 ARCLIGHT - MALAWI Global Health Implementation & Vision 2020 Links University of St Andrews & NHS Fife/Lothian Global Health Implementation & Vision 2020 Links University of St Andrews & NHS Fife/Lothian
ARCLIGHT - MALAWI Global Health Implementation & Vision 2020 Links University of St Andrews & NHS Fife/Lothian Global Health Implementation & Vision 2020 Links University of St Andrews & NHS Fife/Lothian
HealthHarmonie Limited Minor Eye Conditions Services Guide
 HealthHarmonie Limited Minor Eye Conditions Services Guide 2017 Contents Introduction... 3 Experience, Qualifications and Competencies... 3 Required Equipment... 3 Clinical assessment... 3 Management of
HealthHarmonie Limited Minor Eye Conditions Services Guide 2017 Contents Introduction... 3 Experience, Qualifications and Competencies... 3 Required Equipment... 3 Clinical assessment... 3 Management of
Bleeding in the anterior chamber, obstructing vision Caused by surgery, injury, coagulopathy, sickle cell or idiopathic Needs urgent care to prevent
 Bleeding in the anterior chamber, obstructing vision Caused by surgery, injury, coagulopathy, sickle cell or idiopathic Needs urgent care to prevent long-term vision loss TX by elevating head of bed, reducing
Bleeding in the anterior chamber, obstructing vision Caused by surgery, injury, coagulopathy, sickle cell or idiopathic Needs urgent care to prevent long-term vision loss TX by elevating head of bed, reducing
RETINAL CONDITIONS RETINAL CONDITIONS
 GENERAL INFORMATION RETINAL CONDITIONS RETINAL CONDITIONS WHAT ARE RETINAL CONDITIONS? Retinal conditions affect the light-sensitive tissue at the back of eye known as the retina. They include diseases
GENERAL INFORMATION RETINAL CONDITIONS RETINAL CONDITIONS WHAT ARE RETINAL CONDITIONS? Retinal conditions affect the light-sensitive tissue at the back of eye known as the retina. They include diseases
EXAMINATION INTRODUCTION
 1 EXAMINATION INTRODUCTION HISTORY In the assessment of a patient with eye disease, it is important to take a good history, examine the eyes with adequate illumination and test the visual function. Recently,
1 EXAMINATION INTRODUCTION HISTORY In the assessment of a patient with eye disease, it is important to take a good history, examine the eyes with adequate illumination and test the visual function. Recently,
Index. C Canalicular system, 4 Carbonic anhydrase inhibitors, 29 30
 A Acanthamoeba keratitis (AK), 82, 83 Acute angle-closure crisis, 156 Acute angle-closure glaucoma (AACG), 121, 141, 284 causes of, 122 clinical presentation, 153 evaluation, 156 157 management/treatment,
A Acanthamoeba keratitis (AK), 82, 83 Acute angle-closure crisis, 156 Acute angle-closure glaucoma (AACG), 121, 141, 284 causes of, 122 clinical presentation, 153 evaluation, 156 157 management/treatment,
Aristotle University Thessaloniki Medical School I. & II. Departments of Ophthalmology 90 DIAGNOSTIC & THERAPEUTIC APPROACHES IN OPHTHALMOLOGY
 Aristotle University Thessaloniki Medical School I. & II. Departments of Ophthalmology 90 DIAGNOSTIC & THERAPEUTIC APPROACHES IN OPHTHALMOLOGY The medical student should be able to... I. Pathophysiology
Aristotle University Thessaloniki Medical School I. & II. Departments of Ophthalmology 90 DIAGNOSTIC & THERAPEUTIC APPROACHES IN OPHTHALMOLOGY The medical student should be able to... I. Pathophysiology
5/2/2016 EYE EMERGENCIES. Nathaniel Pelsor, O.D., FAAO Talley Medical-Surgical Eye Care Associates. Anatomy. Tools
 EYE EMERGENCIES Nathaniel Pelsor, O.D., FAAO Talley Medical-Surgical Eye Care Associates Anatomy Tools 1 Contact dermatitis Blepharitis HSV Preseptal Cellulitis Anterior Chamber Subconjunctival hemorrhage
EYE EMERGENCIES Nathaniel Pelsor, O.D., FAAO Talley Medical-Surgical Eye Care Associates Anatomy Tools 1 Contact dermatitis Blepharitis HSV Preseptal Cellulitis Anterior Chamber Subconjunctival hemorrhage
Children's Eye Assessment
 Children's Eye Assessment Dr Antony Bedggood, Children s Specialist Centre Paediatric Ophthalmologist, Cataract & Strabismus Surgeon Why kids need early referral Children s eye problems are often subtle:
Children's Eye Assessment Dr Antony Bedggood, Children s Specialist Centre Paediatric Ophthalmologist, Cataract & Strabismus Surgeon Why kids need early referral Children s eye problems are often subtle:
PERIORBITAL SWELLING - COMPLICATION FROM ADJACENT STRUCTURES CASE REPORTS AND REVIEW OF LITERATURE
 VOLUME 26, NO. 3 JUNE 1985 PERIORBITAL SWELLING - COMPLICATION FROM ADJACENT STRUCTURES CASE REPORTS AND REVIEW OF LITERATURE K Sukumaran S Chandran N Janakarajah P K Garg Department of Ophthalmology Faculty
VOLUME 26, NO. 3 JUNE 1985 PERIORBITAL SWELLING - COMPLICATION FROM ADJACENT STRUCTURES CASE REPORTS AND REVIEW OF LITERATURE K Sukumaran S Chandran N Janakarajah P K Garg Department of Ophthalmology Faculty
213: HUMAN FUNCTIONAL ANATOMY: PRACTICAL CLASS 12 Cranial cavity, eye and orbit
 213: HUMAN FUNCTIONAL ANATOMY: PRACTICAL CLASS 12 Cranial cavity, eye and orbit OSTEOLOGY Identify the bones which comprise the walls of the orbit: maxilla, zygomatic, ethmoid, lachrymal, frontal, and
213: HUMAN FUNCTIONAL ANATOMY: PRACTICAL CLASS 12 Cranial cavity, eye and orbit OSTEOLOGY Identify the bones which comprise the walls of the orbit: maxilla, zygomatic, ethmoid, lachrymal, frontal, and
Lower Eyelid Blepharoplasty. Mid-Year Seminar AOCOO-HNS Foundation September 21 st, 2013
 Lower Eyelid Blepharoplasty Mid-Year Seminar AOCOO-HNS Foundation September 21 st, 2013 The beauty of a woman must be seen from in her eyes, because that is the doorway to her heart, the place where love
Lower Eyelid Blepharoplasty Mid-Year Seminar AOCOO-HNS Foundation September 21 st, 2013 The beauty of a woman must be seen from in her eyes, because that is the doorway to her heart, the place where love
The orbit-2. Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology
 The orbit-2 Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology Eyelids The eyelids (act like the curtains) protect the eye from injury and excessive light by their closure The upper eyelid
The orbit-2 Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology Eyelids The eyelids (act like the curtains) protect the eye from injury and excessive light by their closure The upper eyelid
Vision I. Steven McLoon Department of Neuroscience University of Minnesota
 Vision I Steven McLoon Department of Neuroscience University of Minnesota 1 Eye Cornea Sclera Conjunctiva 2 Eye The conjunctiva lines the inner surface of the eyelids and outer surface of the sclera. 3
Vision I Steven McLoon Department of Neuroscience University of Minnesota 1 Eye Cornea Sclera Conjunctiva 2 Eye The conjunctiva lines the inner surface of the eyelids and outer surface of the sclera. 3
EYE ASSESSMENT - ADULT
 For more information or to provide feedback on this or any other decision support tool, email certifiedpractice@crnbc.ca EYE ASSESSMENT - ADULT Nurses with RN First Call Certified Practice designation
For more information or to provide feedback on this or any other decision support tool, email certifiedpractice@crnbc.ca EYE ASSESSMENT - ADULT Nurses with RN First Call Certified Practice designation
The eye in ED. Dr Steve Costa Emergency Medicine Training Hub Ballarat & Grampians Region 18 th July 2013
 The eye in ED Dr Steve Costa Emergency Medicine Training Hub Ballarat & Grampians Region 18 th July 2013 Learning objectives Diagnostic reasoning Describe the common injuries and diagnostic dilemmas seen
The eye in ED Dr Steve Costa Emergency Medicine Training Hub Ballarat & Grampians Region 18 th July 2013 Learning objectives Diagnostic reasoning Describe the common injuries and diagnostic dilemmas seen
Frequently Asked Questions about General Ophthalmology:
 1. Normal Eye Structure The eye is a slightly asymmetrical globe, about an inch in diameter. The parts of the eye include: Cornea (a clear dome over the iris), Iris (the pigmented part); Pupil (the black
1. Normal Eye Structure The eye is a slightly asymmetrical globe, about an inch in diameter. The parts of the eye include: Cornea (a clear dome over the iris), Iris (the pigmented part); Pupil (the black