Decompressive craniectomy following traumatic brain injury
|
|
|
- Augustus Houston
- 6 years ago
- Views:
Transcription

1 Decompressive craniectomy following traumatic brain injury Peter Hutchinson Division of Academic Neurosurgery University of Cambridge Escalating cycle of brain swelling Primary insult Brain swelling Secondary insult Energy failure Increase in brain injury and poor outcome Increase in ICP Decrease in O² delivery Decrease in cerebral blood flow



2 Decompressive Craniectomy If there is no CSF pressure, but brain pressure exists, then pressure relief must be achieved by opening the skull Kocher 1901 Decompressive Craniectomy in TBI Concerns Does it control raised ICP? Does herniated brain escalate the problems? Do the results justify the treatment? Good prognosis patients will do well anyway Poor prognosis patients move from mortality to persistent vegetative state and severe disability What are the complications?
3 NCCU Head injury management ICP<25 mmhg CPP>60 mmhg Stage I Propofol, fentanyl, atracurium º head up PaCO kpa SaO 2 >97%, PaO 2 >11kPa Temp < 37 ºC Stage II External ventricular drain Stage III Inotropes / 5% NaCl / Mannitol PaCO kpa Temp 35 C Stage IV Temp ºC Stage V Thiopentone Decompressive craniectomy Decompressive craniectomy pubmed publications F Servadei N of publications Years

4 Decompressive craniectomy in TBI >50% ~20% Brain Trauma Foundation Bifrontal decompressive craniectomy within 48 hours of injury is a treatment option for patients with diffuse, medically refractory posttraumatic cerebral edema and resultant intracranial hypertension
5 Cochrane review No evidence from RCTs that supports the routine use of secondary decompressive craniectomy to reduce unfavorable outcomes in adults with severe TBI and refractory high ICP. Brain trauma Foundation option 2 trials started recruiting in DECRA (Australia, New Zealand, Saudi Arabia) RESCUEicp (43 centres in 17 countries, mainly UK) Effect of DC on ICP Timofeev et al, J Neurosurgery, 2008
6 Physiological effects of craniectomy impact on autoregulation Operative technique Primary decompressive craniectomy Leaving the bone flap out following initial surgery for a mass lesion acute haematoma Secondary decompressive craniectomy Removing the bone flap to control raised and refractory intracranial pressure


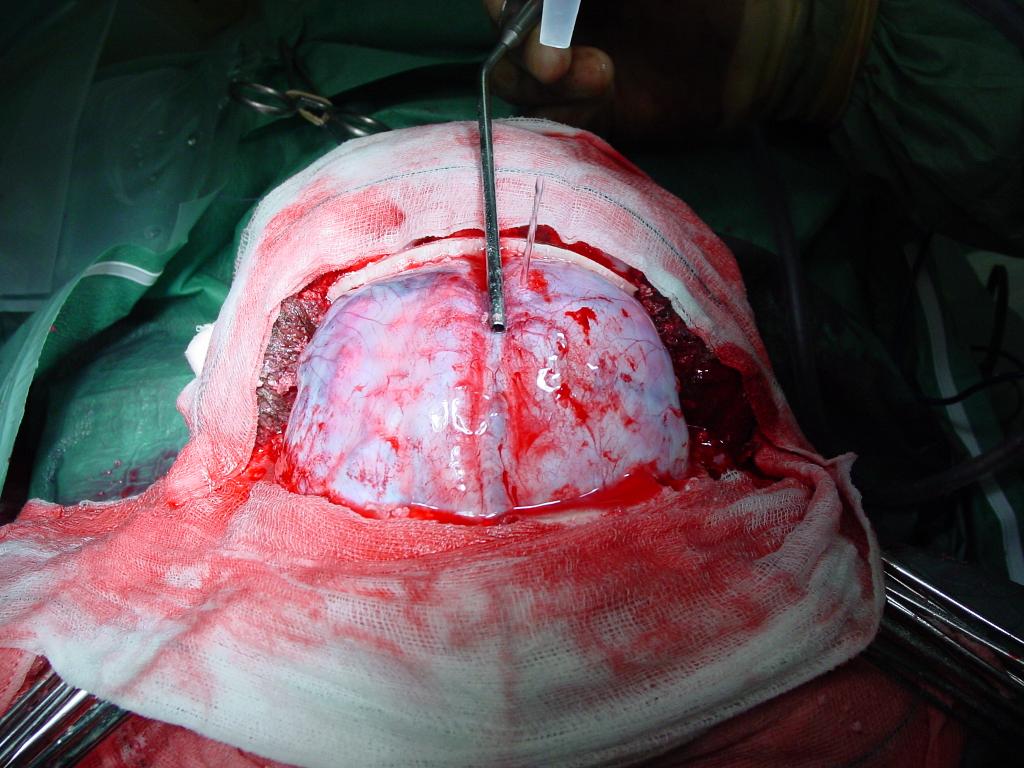
7 Operation type Unilateral - frontotemporoparietal Unilateral brain swelling with midline shift Large unilateral craniectomy Bilateral Diffuse brain injury Bi-coronal scalp flap Bilateral frontal craniectomy to coronal suture posteriorly and pterion laterally Unilateral decompressive craniectomy
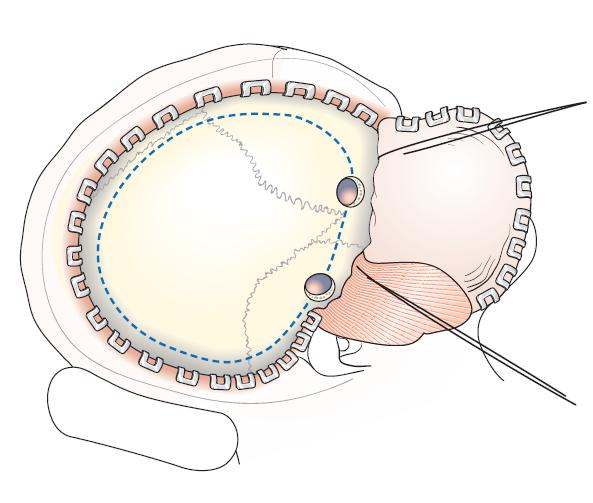
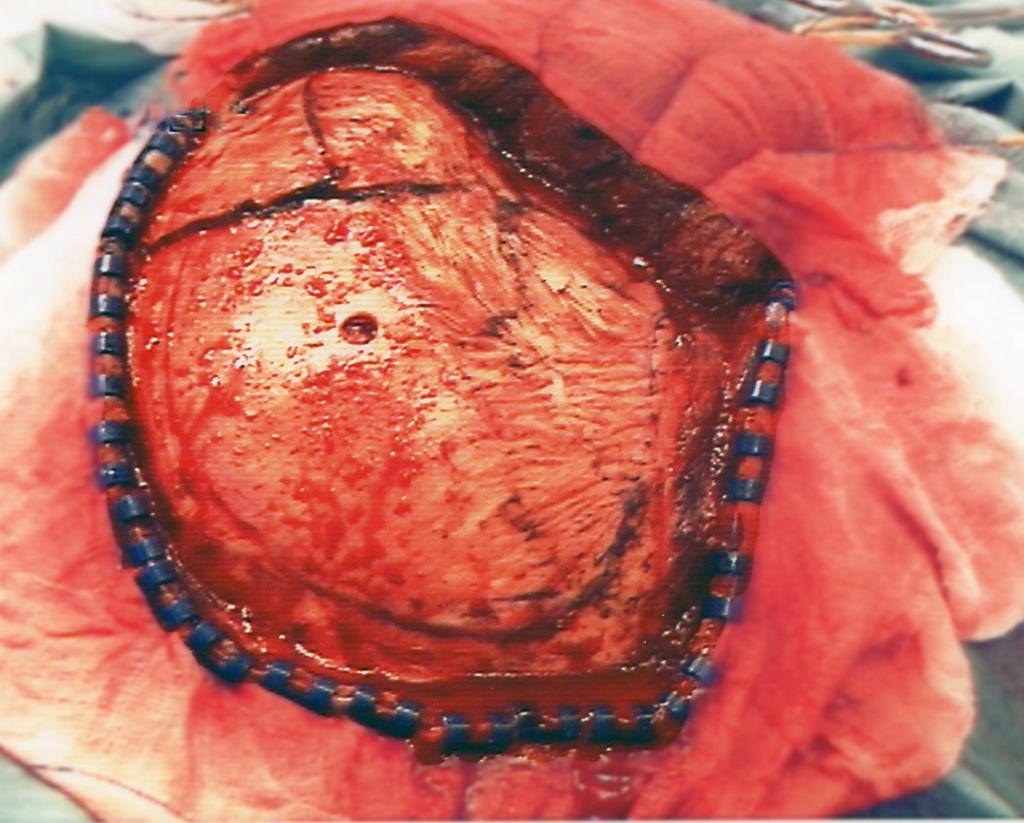

8 Unilateral decompressive craniectomy Unilateral decompressive craniectomy
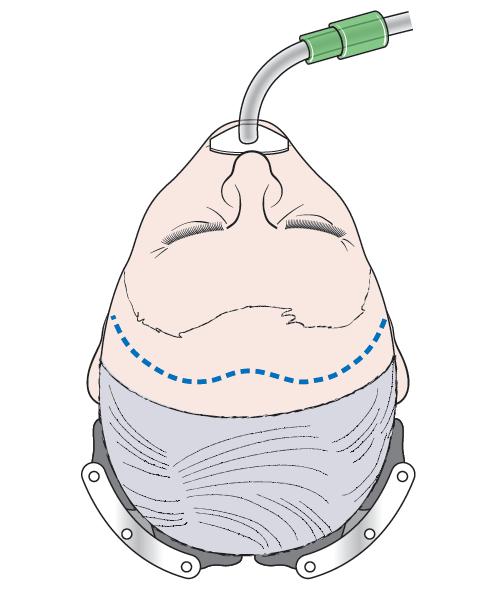


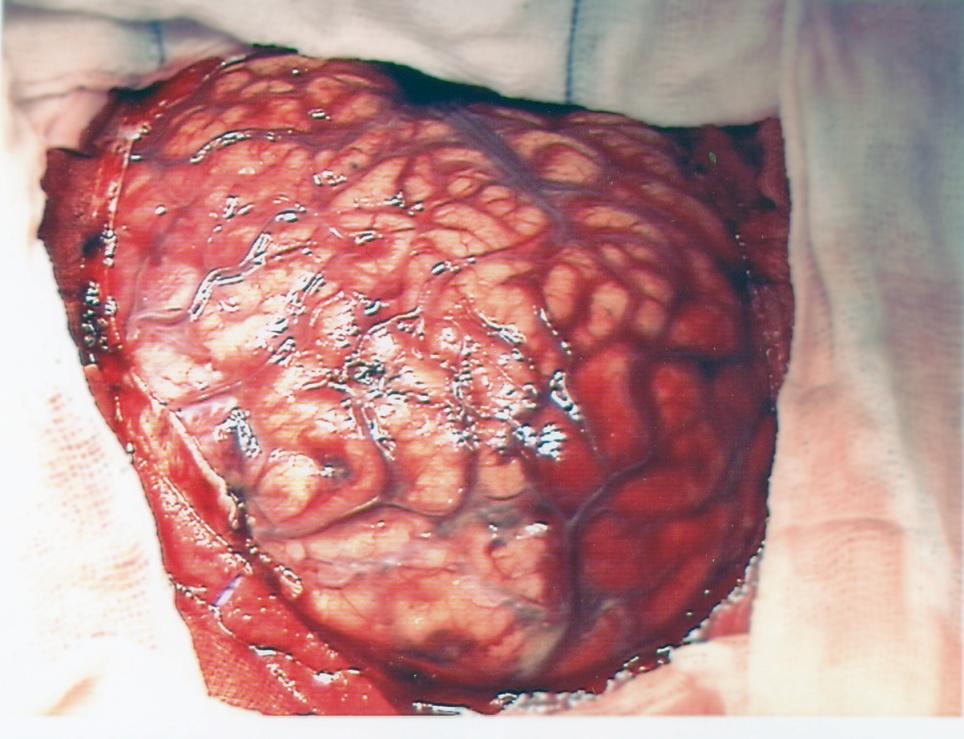
9 Bifrontal decompressive craniectomy Bifrontal decompressive craniectomy


10 Bifrontal decompressive craniectomy Division of the falx
11 Cranialisation and occlusion of the frontal sinus Volume [ml] Calculated Volume gained by Surgical Compression Kalkuliert als < 10 cm³ Volume Zylinder (Rand nur zu 50% berücksichtigt) 6 < 50 cm³ Effective! Diameter Defect [cm] Acknowledgement Aschoff and Piek 14



12 Complications of decompressive craniectomy for traumatic brain injury S Stiver, Neurosurgical Focus 2009 ed G Manley Subdural hygroma Contusion / hematoma progression Infection New contralateral extraaxial haematoma Hydrocephalus Bone flap resorption Re-operation Complications of cranioplasty Skull reconstruction is not without its complications Management of hydrocephalus Infection Seizures Cosmesis

13 Randomised trials of decompressive craniectomy for TBI RESCUEicp Cambridge UK 400 patients Recruitment on-going years Raised ICP refractory to protocolbased medical management ICP threshold 25mmHg DECRA Melbourne Australia 155 patients randomised Completed years Severe diffuse brain injury within 72 hours injury ICP threshold 20mmHg Li et al, Anaesth Analg, 2010 Hypotheses of trials RESCUEicp Decompressive craniectomy can improve outcomes (compared to barbiturates) as last-tier therapy for refractory post-traumatic intracranial hypertension DECRA Early/neuroprotective bifrontal decompression can improve outcomes following diffuse TBI

14 DECRA - CONSORT DECRA - Demographics
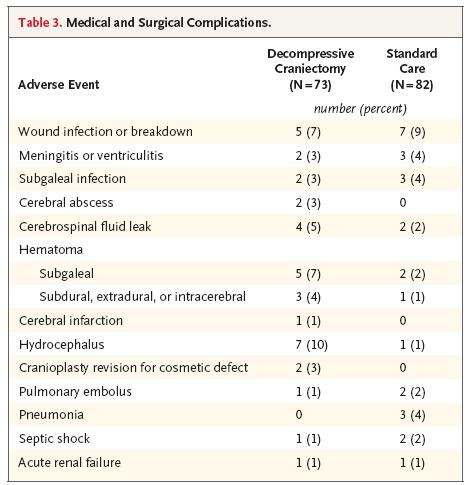

15 DECRA - Complications DECRA - Endpoints
16 DECRA - Results Craniectomy group had less time with ICP above the treatment threshold (P<0.001) fewer interventions for increased ICP (P<0.02) fewer days in ITU (P<0.001) However, craniectomy group had worse scores on the egos (OR: 1.84; 95% CI: 1.05 to 3.24; P = 0.03) greater risk of an unfavourable outcome (OR 2.21; 95% CI: ; P = 0.02) Mortality at 6 months similar in the craniectomy group (19%) and the standard-care group (18%) DECRA - comments ICP was lower in the craniectomy group but it was not excessively high (i.e. remained less than 25mmHg) in the medical group 27% of craniectomy patients had neither pupil reacting vs 12% in the medical group post hoc adjustment for pupil reactivity at baseline à outcome differences not significant Low median GCS motor response (3) and pupil reactivity indicate that DECRA included predominantly patients with significant diffuse axonal injury and possibly some with brainstem injury These patients, without significant intracranial hypertension, were shifted from mortality to unfavourable outcomes by decompressive craniectomy

17 DECRA ICP control DECRA - comments ICP was lower in the craniectomy group but it was not excessively high (i.e. remained less than 25mmHg) in the medical group 27% of craniectomy patients had neither pupil reacting vs 12% in the medical group post hoc adjustment for pupil reactivity at baseline à outcome differences not significant Low median GCS motor response (3) and pupil reactivity indicate that DECRA included predominantly patients with significant diffuse axonal injury and possibly some with brainstem injury These patients, without significant intracranial hypertension, were shifted from mortality to unfavourable outcomes by decompressive craniectomy
18 The RESCUE icp study Randomised Evaluation of Surgery with Craniectomy for Uncontrollable Elevation of ICP The application of decompressive craniectomy to head-injured patients with raised and refractory ICP results in improvement in outcome compared to optimal medical management Prospective randomised study Target study group Ventilated patients with refractory intracranial hypertension Advanced medical management (inc barbiturates) V Surgical management (decompressive craniectomy) Outcome assessed at 6 months and 2 years using extended Glasgow Outcome Score and SF-36 includes health economic analysis

19 Study population Inclusion criteria Patients with head injury requiring ICP monitoring Age years Abnormal CT scan Patients may have had an immediate operation for a mass lesion but not a decompressive craniectomy Exclusion criteria Bilateral fixed and dilated pupils Bleeding diathesis Devastating injury not expected to survive 24 hours Brainstem damage Follow up not possible


20 Study centres 46 centres are currently contributing patients 40 initiating / ready to start recruitment Aim 80 centres worldwide > 100 interested centres, N=326 / 400 As of 10 Dec 2011
21 RESCUEicp recruitment by country (n=323) Canada 3% Brazil 3% Spain 4% Saudi Arabia China 3% 2% Singapore 3% Peru 3% Italy 5% Other 5% UK 69%
22 RESCUEicp study recruitment (n=323) Highest recruiter per quarter Quarter Hospital 1 st 2010 Leeds 2 nd 2010 Royal London 3 rd 2010 Hospital De Oeste, Brazil 4 th 2010 Southampton 1 st 2011 AMH/St George s 2 nd 2011 Southampton 3 rd 2011 Liverpool and Lima, Peru 4 th 2011???
23 Cumulative recruitment Quarterly recruitment
 December 2013: 1 year follow-up completed December 2014: 2 year")
24 Cumulative recruitment (actual & projected) Project timeline August 2011: trial extension granted by MRC/NIHR ( 117,000) December 2012: end of recruitment (according to extension request) May need to be extended by 1 year if decreased recruitment of last 2 quarters continues June 2013: 6 months follow-up completed (primary endpoint) December 2013: 1 year follow-up completed December 2014: 2 year follow-up completed (end of trial)
")


25 Surgical and medical arms (n= 270; 2004 Sept 2010) Crossover No crossover n= 56 21% n= % Surgical arm (n=140) Crossover No crossover n= 13 9% n= %

 Survey closed 30 Nov 2011 https://www.")
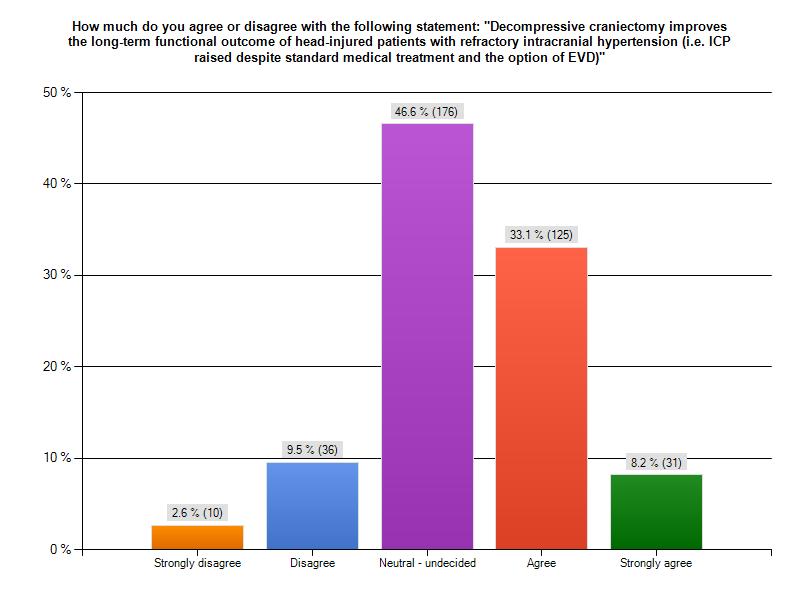
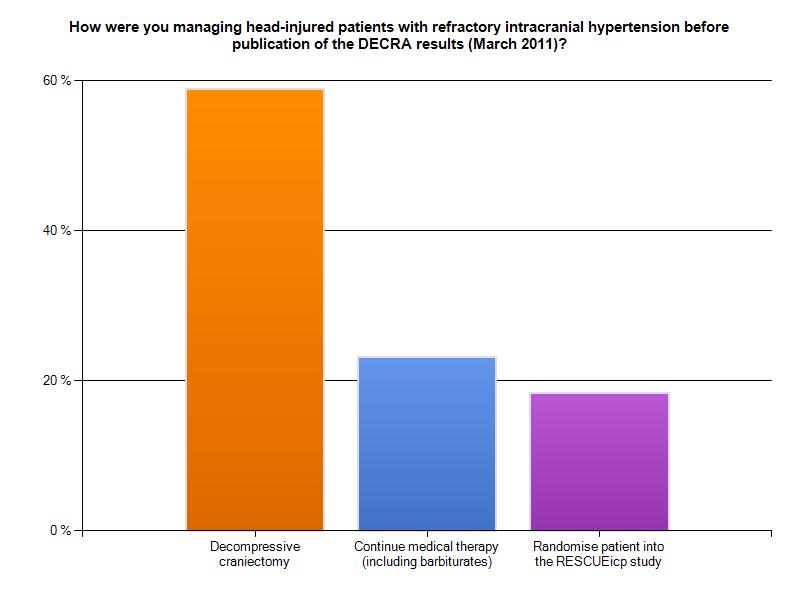
26 Medical arm (n=130) Crossover No crossover n= 87 67% n= 43 33% Decompressive craniectomy survey Participating societies n=378 SBNS/BNTA EANS NeuroCritical Care Network (UK) Neurocritical Care Society (mainly USA) Survey closed 30 Nov
27

28 Conclusion Decompressive craniectomy is a treatment option for patients with refractory posttraumatic cerebral oedema and resultant intracranial hypertension But!! Has a significant complication rate May being performed in patients who will do well with medical treatment alone Risks severe disability and vegetative state DECRA trial completed; RESCUEicp continues Secondary decompressive craniectomy to control raised intracranial pressure is an unproven therapy that ideally should be undertaken as part of a randomised study
29 Acknowledgements- thank you! Peter Kirkpatrick John Pickard Angelos Kolias Ivan Timofeev Liz Corteen Marek Czosnyka David Menon Barbara Sahakian Medical / Nursing Staff on NCCU Martin Buxton David Mendelow Patrick Mitchell Graham Teasdale Franco Servadei Gordon Murray Juan Sahuquillo Andy Unterberg Local investigators Hugh Richards Anthony Bell Donald Shaw Mark Dearden Martin Smith Nicola Latronico Lennart Persson Eckhard Rickels pjah2@cam.ac.uk
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Trauma is the leading cause of death in the first four decades of life, with head injury being
 Correspondence to: Mr PJ Hutchinson, Academic Department of Neurosurgery, University of Cambridge, Box 167, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK: p.hutch@which.net ACUTE HEAD INJURY FOR THE NEUROLOGIST
Correspondence to: Mr PJ Hutchinson, Academic Department of Neurosurgery, University of Cambridge, Box 167, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK: p.hutch@which.net ACUTE HEAD INJURY FOR THE NEUROLOGIST
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Brain under pressure Managing ICP. Giuseppe
 Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Improving TBI outcome
 Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
What is elevated ICP?
 What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Update sulle lesioni emorragiche posttraumatiche
 Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Supplementary Online Content
 Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Chapter 8: Cerebral protection Stephen Lo
 Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
journal of medicine The new england Trial of Decompressive Craniectomy for Traumatic Intracranial Hypertension abstract
 The new england journal of medicine established in 1812 September 22, 2016 vol. 375 no. 12 Trial of Decompressive Craniectomy for Traumatic Intracranial Hypertension P.J. Hutchinson, A.G. Kolias, I.S.
The new england journal of medicine established in 1812 September 22, 2016 vol. 375 no. 12 Trial of Decompressive Craniectomy for Traumatic Intracranial Hypertension P.J. Hutchinson, A.G. Kolias, I.S.
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
A bs tr ac t. n engl j med 364;16 nejm.org april 21,
 The new england journal of medicine established in 1812 april 21, 2011 vol. 364 no. 16 Decompressive Craniectomy in Diffuse Traumatic Brain Injury D. James Cooper, M.D., Jeffrey V. Rosenfeld, M.D., Lynnette
The new england journal of medicine established in 1812 april 21, 2011 vol. 364 no. 16 Decompressive Craniectomy in Diffuse Traumatic Brain Injury D. James Cooper, M.D., Jeffrey V. Rosenfeld, M.D., Lynnette
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature
 Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature Anand Sharma 1, Arti Sharma 2, Yashbir Dewan 1 1 Artemis
Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature Anand Sharma 1, Arti Sharma 2, Yashbir Dewan 1 1 Artemis
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
Multimodal monitoring to individualize care in TBI
 Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome?
 11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome? Critical levels of CPP, ICP and PRx Percentage of patients in outcome
11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome? Critical levels of CPP, ICP and PRx Percentage of patients in outcome
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Effect of decompressive craniectomy on intracranial pressure and cerebrospinal compensation following traumatic brain injury
 J Neurosurg 108:66 73, 2008 Effect of decompressive craniectomy on intracranial pressure and cerebrospinal compensation following traumatic brain injury IVAN TIMOFEEV, M.R.C.S., 1 MAREK CZOSNYKA, PH.D.,
J Neurosurg 108:66 73, 2008 Effect of decompressive craniectomy on intracranial pressure and cerebrospinal compensation following traumatic brain injury IVAN TIMOFEEV, M.R.C.S., 1 MAREK CZOSNYKA, PH.D.,
Recent trends in the management of head injury
 Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
PACT module. Traumatic Brain Injury. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY. Dr Nick Taylor MBBS FACEM
 PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
Only 30% to 40% of acute subdural hematoma (SDH)
") Contralateral Acute Epidural Hematoma After Decompressive Surgery of Acute Subdural Hematoma: Clinical Features and Outcome Thung-Ming Su, MD, Tsung-Han Lee, MD, Wu-Fu Chen, MD, Tao-Chen Lee, MD, and Ching-Hsiao
Contralateral Acute Epidural Hematoma After Decompressive Surgery of Acute Subdural Hematoma: Clinical Features and Outcome Thung-Ming Su, MD, Tsung-Han Lee, MD, Wu-Fu Chen, MD, Tao-Chen Lee, MD, and Ching-Hsiao
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Management of head injury in the intensive-care unit
 Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Management of Traumatic Brain Injury. Olaide O. Ajayi, MD
 Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
Pediatric Head Injury:
 Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
The role of decompressive craniectomy in the management
 J Neurosurg 120:1131 1137, 2014 AANS, 2014 Validation of the CRASH model in the prediction of 18-month mortality and unfavorable outcome in severe traumatic brain injury requiring decompressive craniectomy
J Neurosurg 120:1131 1137, 2014 AANS, 2014 Validation of the CRASH model in the prediction of 18-month mortality and unfavorable outcome in severe traumatic brain injury requiring decompressive craniectomy
Bone flap preservation in abdominal wall after decompressive craniectomy in head injury: A single institute experience
 DOI: 10.2478/romneu-2018-0063 Article Bone flap preservation in abdominal wall after decompressive craniectomy in head injury: A single institute experience Pavan Kumar, Ashok Kumar, Gaurav Jaiswal, Tarun
DOI: 10.2478/romneu-2018-0063 Article Bone flap preservation in abdominal wall after decompressive craniectomy in head injury: A single institute experience Pavan Kumar, Ashok Kumar, Gaurav Jaiswal, Tarun
Surgical Management & Clinical Outcome of Severe Brain Trauma due to Acute Subdural Hematoma.
 International Journal of Sciences: Basic and Applied Research (IJSBAR) ISSN 2307-4531 (Print & Online) http://gssrr.org/index.php?journal=journalofbasicandapplied ----------------------------------------------------------------------------------------------------------------
International Journal of Sciences: Basic and Applied Research (IJSBAR) ISSN 2307-4531 (Print & Online) http://gssrr.org/index.php?journal=journalofbasicandapplied ----------------------------------------------------------------------------------------------------------------
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Outcomes of 33 patients from the wars in Iraq and Afghanistan undergoing bilateral or bicompartmental craniectomy
 J Neurosurg 115:124 129, 2011 Outcomes of 33 patients from the wars in Iraq and Afghanistan undergoing bilateral or bicompartmental craniectomy Clinical article Robert D. Ecker, M.D., LCDR, USN, 1 Lisa
J Neurosurg 115:124 129, 2011 Outcomes of 33 patients from the wars in Iraq and Afghanistan undergoing bilateral or bicompartmental craniectomy Clinical article Robert D. Ecker, M.D., LCDR, USN, 1 Lisa
Journal of Clinical Neuroscience
 Journal of Clinical Neuroscience 19 (2012) 1222 1227 Contents lists available at SciVerse ScienceDirect Journal of Clinical Neuroscience journal homepage: www.elsevier.com/locate/jocn Clinical Study Craniectomy-Associated
Journal of Clinical Neuroscience 19 (2012) 1222 1227 Contents lists available at SciVerse ScienceDirect Journal of Clinical Neuroscience journal homepage: www.elsevier.com/locate/jocn Clinical Study Craniectomy-Associated
Intracranial pressure monitoring in severe traumatic brain injury
 188 Apetrei et al Intracranial pressure monitoring in severe traumatic brain injury Intracranial pressure monitoring in severe traumatic brain injury Al. Cosmin Apetrei 1,2, A.Şt. Iencean 2, A Iordache
188 Apetrei et al Intracranial pressure monitoring in severe traumatic brain injury Intracranial pressure monitoring in severe traumatic brain injury Al. Cosmin Apetrei 1,2, A.Şt. Iencean 2, A Iordache
He-xiang Zhao 1, Yi Liao 2, Ding Xu 1, Qiang-ping Wang 1, Qi Gan 1, Chao You 1 and Chao-hua Yang 1*
 Zhao et al. BMC Surgery (2015) 15:111 DOI 10.1186/s12893-015-0100-7 RESEARCH ARTICLE Open Access The value of intraoperative intracranial pressure monitoring for predicting re-operation using salvage decompressive
Zhao et al. BMC Surgery (2015) 15:111 DOI 10.1186/s12893-015-0100-7 RESEARCH ARTICLE Open Access The value of intraoperative intracranial pressure monitoring for predicting re-operation using salvage decompressive
Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples.
. Pressure-reactivity index, computational methods. Clinical examples.") Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples. Optimization of cerebral perfusion pressure: Relationship
Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples. Optimization of cerebral perfusion pressure: Relationship
Is Neuromonitoring an expensive waste of time, in Severe Traumatic Brain Injury?
 Is Neuromonitoring an expensive waste of time, in Severe Traumatic Brain Injury? Edema Engorgement Contusion Hematoma Hypoxia Diffuse Axonal Injury Ross Bullock, MD, PhD. Director, Neurotrauma,- University
Is Neuromonitoring an expensive waste of time, in Severe Traumatic Brain Injury? Edema Engorgement Contusion Hematoma Hypoxia Diffuse Axonal Injury Ross Bullock, MD, PhD. Director, Neurotrauma,- University
Index. Note: Page numbers of article titles are in bold face type.
 Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP?
 7. Cerebral perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP? Douglas J. Miller Miller JD, Stanek A, Langfitt
7. Cerebral perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP? Douglas J. Miller Miller JD, Stanek A, Langfitt
Conflict of Interest Disclosure J. Claude Hemphill III, MD,MAS. Difficult Diagnosis and Treatment: New Onset Obtundation
 Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
Traumatic Brain Injury Pathway, GCS 15 Closed head injury
 Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Outcome Determinants of Decompressive Craniectomy in Patients with Traumatic Brain Injury; A Single Center Experience from Southern Iran
 Bull Emerg Trauma 2017;5(3):190-196. Original Article Outcome Determinants of Decompressive Craniectomy in Patients with Traumatic Brain Injury; A Single Center Experience from Southern Iran Hosseinali
Bull Emerg Trauma 2017;5(3):190-196. Original Article Outcome Determinants of Decompressive Craniectomy in Patients with Traumatic Brain Injury; A Single Center Experience from Southern Iran Hosseinali
Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Changing Demographics in Death After Devastating Brain Injury
 Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Cerebral autoregulation is a complex intrinsic control. Time course for autoregulation recovery following severe traumatic brain injury
 J Neurosurg 111:695 700, 2009 Time course for autoregulation recovery following severe traumatic brain injury Clinical article Gi l l E. Sv i r i, M.D., M.Sc., 1 Ru n e Aa s l i d, Ph.D., 2 Co l l e e
J Neurosurg 111:695 700, 2009 Time course for autoregulation recovery following severe traumatic brain injury Clinical article Gi l l E. Sv i r i, M.D., M.Sc., 1 Ru n e Aa s l i d, Ph.D., 2 Co l l e e
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8:
 Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Cooper DJ, Rosenfeld JV, Murray L, et al. Decompressive craniectomy
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Cooper DJ, Rosenfeld JV, Murray L, et al. Decompressive craniectomy
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Decompressive Hemicraniectomy in Acute Neurological Diseases
 Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Outcomes of cranial repair after craniectomy
 J Neurosurg 112:1120 1124, 2010 Outcomes of cranial repair after craniectomy Clinical article Vi c t o r Ch a n g, M.D., 1 Pa u l Ha rt z f e l d, M.D., 1 Mar i a n n e La n g l o i s, P.A.-C, 2 Asi m
J Neurosurg 112:1120 1124, 2010 Outcomes of cranial repair after craniectomy Clinical article Vi c t o r Ch a n g, M.D., 1 Pa u l Ha rt z f e l d, M.D., 1 Mar i a n n e La n g l o i s, P.A.-C, 2 Asi m
Efficacy of Decompressive Craniectomy in Acute Subdural Hematoma in Head Injury Patients, Madurai Medical College, Madurai
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/107 Efficacy of Decompressive Craniectomy in Acute Subdural Hematoma in Head Injury Patients, Madurai Medical College,
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/107 Efficacy of Decompressive Craniectomy in Acute Subdural Hematoma in Head Injury Patients, Madurai Medical College,
Sign up to receive ATOTW weekly
 MANAGEMENT OF PAEDIATRIC TRAUMATIC BRAIN INJURY ANAESTHESIA TUTORIAL OF THE WEEK 127 30 TH MARCH 2009 Kavitha Raghavan, King s College Hospital, London Richard Waddington, Kingston Hospital, Surrey Correspondence
MANAGEMENT OF PAEDIATRIC TRAUMATIC BRAIN INJURY ANAESTHESIA TUTORIAL OF THE WEEK 127 30 TH MARCH 2009 Kavitha Raghavan, King s College Hospital, London Richard Waddington, Kingston Hospital, Surrey Correspondence
Comparison of Burr Holes and Decompressive Craniotomy in the Surgical Treatment of Traumatic Acute Subdural Hematoma
 Med. J. Cairo Univ., Vol. 83, No. 1, March: 259-266, 2015 www.medicaljournalofcairouniversity.net Comparison of Burr Holes and Decompressive Craniotomy in the Surgical Treatment of Traumatic Acute Subdural
Med. J. Cairo Univ., Vol. 83, No. 1, March: 259-266, 2015 www.medicaljournalofcairouniversity.net Comparison of Burr Holes and Decompressive Craniotomy in the Surgical Treatment of Traumatic Acute Subdural
Head trauma is one of the leading causes of death
 clinical article J Neurosurg Pediatr 16:508 514, 2015 Outcome of children with severe traumatic brain injury who are treated with decompressive craniectomy Maroun J. Mhanna, MD, MPH, 1 Wael El Mallah,
clinical article J Neurosurg Pediatr 16:508 514, 2015 Outcome of children with severe traumatic brain injury who are treated with decompressive craniectomy Maroun J. Mhanna, MD, MPH, 1 Wael El Mallah,
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Measuring severity of TBI. Traumatic Brain injury: TBI. Glasgow Coma Scale & score. Glasgow coma scale/score. Glasgow coma scale with score (GCS)
") Measuring severity of TBI Glasgow coma scale with score (GCS) ก กก functional outcome Post traumatic Amnesia (PTA) cognitive & functional deficit Assist. Prof.Savai Norasan First National Neuroscience
Measuring severity of TBI Glasgow coma scale with score (GCS) ก กก functional outcome Post traumatic Amnesia (PTA) cognitive & functional deficit Assist. Prof.Savai Norasan First National Neuroscience
Early Decompression of Acute Subdural Hematoma for Postoperative Neurological Improvement: A Single Center Retrospective Review of 10 Years
 CLINICAL ARTICLE Korean J Neurotrauma 2016;12(1):11-17 pissn 2234-8999 / eissn 2288-2243 http://dx.doi.org/10.13004/kjnt.2016.12.1.11 Early Decompression of Acute Subdural Hematoma for Postoperative Neurological
CLINICAL ARTICLE Korean J Neurotrauma 2016;12(1):11-17 pissn 2234-8999 / eissn 2288-2243 http://dx.doi.org/10.13004/kjnt.2016.12.1.11 Early Decompression of Acute Subdural Hematoma for Postoperative Neurological
The significance of traumatic haematoma in the
 Journal of Neurology, Neurosurgery, and Psychiatry 1986;49:29-34 The significance of traumatic haematoma in the region of the basal ganglia P MACPHERSON, E TEASDALE, S DHAKER, G ALLERDYCE, S GALBRAITH
Journal of Neurology, Neurosurgery, and Psychiatry 1986;49:29-34 The significance of traumatic haematoma in the region of the basal ganglia P MACPHERSON, E TEASDALE, S DHAKER, G ALLERDYCE, S GALBRAITH
Late decompressive craniectomyafter traumatic brain injury: neurological outcome at 6 months after ICU discharge
 Cianchi et al. Journal of Trauma Management & Outcomes 2012, 6:8 RESEARCH Open Access Late decompressive craniectomyafter traumatic brain injury: neurological outcome at 6 months after ICU discharge Giovanni
Cianchi et al. Journal of Trauma Management & Outcomes 2012, 6:8 RESEARCH Open Access Late decompressive craniectomyafter traumatic brain injury: neurological outcome at 6 months after ICU discharge Giovanni
Anesthetic Management of a Patient with Traumatic Brain Injury
 Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Traumatic Brain Injury Pathways for Adult ED Patients Being Admitted to Trauma Service
 tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
Abstract. The first surgeon promoting DC in post traumatic brain swelling was Kocher in 1901 [9].
![Abstract. The first surgeon promoting DC in post traumatic brain swelling was Kocher in 1901 [9].](/thumbs/74/69632405.jpg "Abstract. The first surgeon promoting DC in post traumatic brain swelling was Kocher in 1901 [9].") Med. J. Cairo Univ., Vol. 80, No. 2, March: 143-149, 2012 www.medicaljournalofcairouniversity.com Unilateral Decompressive Craniectomy in Traumatic Brain Injury Patients with Poor Glasgow Coma Scale as
Med. J. Cairo Univ., Vol. 80, No. 2, March: 143-149, 2012 www.medicaljournalofcairouniversity.com Unilateral Decompressive Craniectomy in Traumatic Brain Injury Patients with Poor Glasgow Coma Scale as
Clinical application of the supraorbital key-hole approach to the treatment of unilateral-dominant bilateral frontal contusions
 /, 2017, Vol. 8, (No. 29), pp: 48343-48349 Clinical application of the supraorbital key-hole approach to the treatment of unilateral-dominant bilateral frontal contusions Shuguang Zhang 1,*, Chunfa Qian
/, 2017, Vol. 8, (No. 29), pp: 48343-48349 Clinical application of the supraorbital key-hole approach to the treatment of unilateral-dominant bilateral frontal contusions Shuguang Zhang 1,*, Chunfa Qian
Continuous cerebral autoregulation monitoring
 Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
A Comprehensive Study on Post Traumatic Temporal Contusion in Adults
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/318 A Comprehensive Study on Post Traumatic Temporal Contusion in Adults R Renganathan 1, P John Paul 2, Heber Anandan
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/318 A Comprehensive Study on Post Traumatic Temporal Contusion in Adults R Renganathan 1, P John Paul 2, Heber Anandan
l1'ijj Surgical treatment for ~brain compartment syndrome' in children with severe head injury
 Surgical treatment for ~brain compartment syndrome' in children with severe head injury A A Figaji, A G Fieggen, A Argent, J C Peter Objectives. Traumatic brain injury accounts for a high percentage of
Surgical treatment for ~brain compartment syndrome' in children with severe head injury A A Figaji, A G Fieggen, A Argent, J C Peter Objectives. Traumatic brain injury accounts for a high percentage of
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report
 214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN
 Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Management Guidelines For St Mary s Major Trauma Centre
 Head Injury Management Guidelines For St Mary s Major Trauma Centre Table of Contents Introduction... 2 Referral Process, Admission and Resuscitation... 2 The Trauma Tree Pathway:... 2 Neurosurgery Registrar
Head Injury Management Guidelines For St Mary s Major Trauma Centre Table of Contents Introduction... 2 Referral Process, Admission and Resuscitation... 2 The Trauma Tree Pathway:... 2 Neurosurgery Registrar
Traumatic Head Injury
 Traumatic Head Injury Liu Yi, MD. PhD, associate professor Dept. Neurosurgery Conception Any injury to the skull, or brain, caused by external physical forces, in stead of degenerative or congenital nature
Traumatic Head Injury Liu Yi, MD. PhD, associate professor Dept. Neurosurgery Conception Any injury to the skull, or brain, caused by external physical forces, in stead of degenerative or congenital nature
Intracranial hypertension and cerebral perfusion pressure: influence on neurological deterioration and outcome in severe head injury*
 J Neurosurg 92:1 6, 2000, Click here to return to Table of Contents Intracranial hypertension and cerebral perfusion pressure: influence on neurological deterioration and outcome in severe head injury*
J Neurosurg 92:1 6, 2000, Click here to return to Table of Contents Intracranial hypertension and cerebral perfusion pressure: influence on neurological deterioration and outcome in severe head injury*
Severe Head dinjury Management and Recent Advances
 Severe Head dinjury ent and Recent Advances Presenter Dr Shejoy P Joshua Moderator Dr AK Mahapatra Dr Deepak Kumar Gupta 1 KEY Epidemiology Resuscitation Primary survey Secondary survey Neurological evaluation
Severe Head dinjury ent and Recent Advances Presenter Dr Shejoy P Joshua Moderator Dr AK Mahapatra Dr Deepak Kumar Gupta 1 KEY Epidemiology Resuscitation Primary survey Secondary survey Neurological evaluation
Role of Invasive ICP Monitoring in Patients with Traumatic Brain Injury: An Experience of 98 Cases
 31 Original Article Indian Journal of Neurotrauma (IJNT) 2006, Vol. 3, No. 1, pp. 31-36 Role of Invasive ICP Monitoring in Patients with Traumatic Brain Injury: An Experience of 98 Cases Deepak Kumar Gupta
31 Original Article Indian Journal of Neurotrauma (IJNT) 2006, Vol. 3, No. 1, pp. 31-36 Role of Invasive ICP Monitoring in Patients with Traumatic Brain Injury: An Experience of 98 Cases Deepak Kumar Gupta
Quiz 43. This quiz is being published on behalf of the Education Committee of the SNACC. Start. Traumatic Brain Injury 101
 Quiz 43 Traumatic Brain Injury 101 SUNEETA GOLLAPUDY, M.D ASSOCIATE PROFESSOR, DIVISION DIRECTOR - NEUROANESTHESIA, MEDICAL COLLEGE OF WISCONSIN, MILWAUKEE, WI QUIZ TEAM: SHOBANA RAJAN, M.D; SUNEETA GOLLAPUDY,
Quiz 43 Traumatic Brain Injury 101 SUNEETA GOLLAPUDY, M.D ASSOCIATE PROFESSOR, DIVISION DIRECTOR - NEUROANESTHESIA, MEDICAL COLLEGE OF WISCONSIN, MILWAUKEE, WI QUIZ TEAM: SHOBANA RAJAN, M.D; SUNEETA GOLLAPUDY,
Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience
 80 Original Article THIEME Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience V. Velho 1 Hrushikesh U. Kharosekar 1 Jasmeet S. Thukral 1 Shonali Valsangkar
80 Original Article THIEME Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience V. Velho 1 Hrushikesh U. Kharosekar 1 Jasmeet S. Thukral 1 Shonali Valsangkar
19. Monitoring of CA using TCD- Mx and Sx
 19. Monitoring of CA using TCD- Mx and Sx Drawing the autoregulatory curve: in clinical practice such dramatic changes in CPP are not permissible Monitoring cerebral autoregulation - certainly not a new
19. Monitoring of CA using TCD- Mx and Sx Drawing the autoregulatory curve: in clinical practice such dramatic changes in CPP are not permissible Monitoring cerebral autoregulation - certainly not a new
Management of pediatric head injury
 IJCCM October-December 2003 Vol 7 Issue 4 Indian J Crit Care Med April-June 2004 Vol 8 Issue 2 Pediatric Section Management of pediatric head injury Praveen Khilnani Introduction Exact incidence of head
IJCCM October-December 2003 Vol 7 Issue 4 Indian J Crit Care Med April-June 2004 Vol 8 Issue 2 Pediatric Section Management of pediatric head injury Praveen Khilnani Introduction Exact incidence of head