V. CENTRAL NERVOUS SYSTEM TRAUMA
|
|
|
- Evelyn Phillips
- 6 years ago
- Views:
Transcription
1 V. CENTRAL NERVOUS SYSTEM TRAUMA
2 I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested by impact on a rigid surface)
3 - The characteristic neurologic picture includes Instantaneous onset of transient neurologic dysfunction including 1. Loss of consciousness, 2. Temporary respiratory arrest 3. Loss of reflexes.
4 - Although neurologic recovery is complete, amnesia for the event persists - Pathogenesis is unknown but may result fromtemporary deregulation of the reticular activating system in the brainstem
5 Complications 1. Post concussive neuropsychiatric syndromes typically associate with repetitive trauma are well recognized 2. Significant cognitive impairment with distinct pathologic findings called chronic traumatic encephalopathy
6 II. Direct parenchymal injuries 1. Contusions - Caused by blunt trauma to the brain - The pia- arachnoid is not breached Mechanism - A blow to the surface of the brain transmitted through the skull leads to rapid tissue displacement, disruption of vessels, hemorrhage, tissue injury
7 - Blood can extend into the subarachnoid space - The crest of gyri are most susceptible than the depth of sulci - Are common in regions of the brain overlying rough and irregular inner skull surfaces, such as:
8 a. The frontal poles b. The orbital surfaces of the frontal lobes c. And the temporal lobe tips Note - Contusions are less frequent over the occipital lobes, brainstem and cerebellum until these sites are adjacent to a skull fracture
9 - A person who suffers a blow to the head may develop a contusion at the point of the contact called coup contusions - Or may suffer a contusion on the brain surface opposite to the site of the contact called contrecoup contusion
10 - Both types of contusions have similar gross and microscopic appearances - The distinction is made on identification of the point impact a. If the head is immobile at the time of trauma, only a coup injury is found - Is caused by contact between the surface of the brain and skull at the site of impact
11 b. If the head is mobile at the time of the trauma, both coup and contrecoup contusions may be found - Is thought to arise when the brain strikes the opposite inner surface of the skull after sudden deceleration
12 .MORPHOLOGY : - Are wedge-shaped with the broad base lying along the surface at the point of the impact - Microscopic examination a. In the earliest stage: Edema and hemorrhage
13 b. During next few hours: - Extravasation of blood extend throughout the cortex to white matter then to the subarachnoid space c. Old traumatic lesions - Are depressed retracted yellow brown patches ( called plaque jaune)

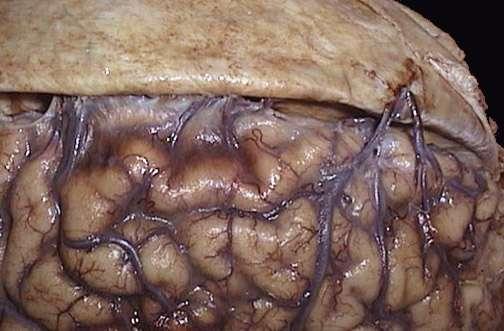
14 Early contusions at orbital gyri of frontal lobes

15 Old contusions

16 Contusions: Recent and old
17 III. Diffuse axonal injury - Trauma can also cause more subtle but widespread injury to axons within the brain with devastating consequences - Axons are injured by a. The direct action of mechanical forces with subsequent alteration of axoplasmic flow
18 b. Or by angular acceleration alone, which can cause axonal injury even in the absence of impact Note: - As many as 50% of patients who develop coma shortly after trauma are believed to have white matter damage and diffuse axonal injury.
19 -These injuries are widespread, and asymmetric and are most commonly found in a. Corpus callosum b. Paraventricular area c. Cerebral peduncles d. Reticular activating formation
20 Morphology - They take the form of axonal swellings that appear within hours of the injury and may persist for much longer - The swelling can be demonstrated immunostains for axonally transported proteins such as amyloid precursor protein
21 IV. Traumatic vascular injuries - It results from direct trauma and disruption of the vessel wall and leads to hemorrhage in different anatomic sites
22 1. Epidural hematoma - Normally the dura is fused with the periosteum on the internal surface of the brain - Dural arteries, most importantly, the middle meningeal artery are vulnerable to injury especially with skill fracture in which the fracture cross the course of the vessel
23 Note - In children in whom the skull is deformable, a temporary displacement of skull bones leading to lacerations of a vessel can occur in the absence of skull fracture
24 - Once a vessel is torn, blood accumulating under arterial pressure can dissect the tightly applied dura away from the inner skull surface producing a epidural hematoma that compresses the brain surface.
25 - When blood accumulates slowly, patients can be lucid for several hours between the moment of trauma and the development of neurologic signs.. - An epidural hematoma may expand rapidly and constitutes a neurosurgical emergency necessitating prompt drainage and repair to prevent death

26 Epidural hematoma
27 B. Subdural Hematoma - The dura is composed of two layer, a. The external collagenous layer b. and inner border cell layer with scant fibroblasts and abundant extracellular space devoid of collagen
28 Notes: - When bleeding occurs, these two layers separate and create the subdural space in which the blood accumulates - Bridging veins travel from convexities of the cerebral hemispheres through the subarachnoid space and the subdural space to empty into superior sagittal sinus
29
30 - These vessels are prone to tearing along their course through the dural layers - The venous sinuses are fixed relative to the dura, so the displacement of the brain that occurs in trauma can tear the veins at the point where they penetrate the dura
31 Susceptible people: 1. Old people with brain atrophy - Patients with brain atrophy, the bridging veins are stretched out, and the brain has additional space within which to move, accounting for the higher rate of subdural hematomas in elderly persons. 2. Infants also are susceptible to subdural hematomas because their bridging veins are thin-walled.
32 Morphology Grossly, - Acute subdural hematomas appear as a collection of freshly clotted blood along the brain surface, without extension into the depths of sulci - Flattened underlying brain and subarachnoid space is often clear.
33 - Typically, venous bleeding is self-limited; breakdown and organization of the hematoma take place over time 1. Lysis of the blood within one week 2. Growth of granulation tissue from the dural surface into the hematoma (2 weeks)
34 - Typically, the organized hematoma is firmly attached to the inner surface of the dura and is free of the underlying arachnoid, which does not contribute to healing. - The lesion can eventually retract as the granulation tissue matures until only a thin layer of reactive connective tissue remains ( subdural membranes ).
35 - In other cases, however, multiple recurrent episodes of bleeding occur (chronic subdural hematomas), presumably from the thin-walled vessels of the granulation tissue. - The risk of repeat bleeding is greatest in the first few months after the initial hemorrhage
36 Clinically - Neurologic signs are attributable to the pressure exerted on the adjacent brain. - Symptoms may be localizing but more often are nonlocalizing, taking the form of headache confusion, and slowly progressive neurologic deterioration.
37 - Subdural hematomas typically become manifest within the first 48 hours after injury. - They are most common over the lateral aspects of the cerebral hemispheres and may be bilateral.
38 - Symptomatic subdural hematomas are treated by surgical removal of the blood and associated reactive tissue
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Once a vessel is torn, blood accumulating under arterial pressure can dissect the tightly applied dura away from the inner skull surface producing a
 Once a vessel is torn, blood accumulating under arterial pressure can dissect the tightly applied dura away from the inner skull surface producing a hematoma that compresses the brain surface. - Clinically,
Once a vessel is torn, blood accumulating under arterial pressure can dissect the tightly applied dura away from the inner skull surface producing a hematoma that compresses the brain surface. - Clinically,
Neuropathology Of Head Trauma. Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center
 Neuropathology Of Head Trauma Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center Nothing to disclose Disclosure Introduction 500,000 cases/year of serious head injury
Neuropathology Of Head Trauma Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center Nothing to disclose Disclosure Introduction 500,000 cases/year of serious head injury
The dura is sensitive to stretching, which produces the sensation of headache.
 Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Meninges and Ventricles
 Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
THE ESSENTIAL BRAIN INJURY GUIDE
 THE ESSENTIAL BRAIN INJURY GUIDE Neuroanatomy & Neuroplasticity Section 2 Contributors Erin D. Bigler, PhD Michael R. Hoane, PhD Stephanie Kolakowsky-Hayner, PhD, CBIST, FACRM Dorothy A. Kozlowski, PhD
THE ESSENTIAL BRAIN INJURY GUIDE Neuroanatomy & Neuroplasticity Section 2 Contributors Erin D. Bigler, PhD Michael R. Hoane, PhD Stephanie Kolakowsky-Hayner, PhD, CBIST, FACRM Dorothy A. Kozlowski, PhD
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
Brain ميهاربا لض اف دمح ا د The Meninges 1- Dura Mater of the Brain endosteal layer does not extend meningeal layer falx cerebri tentorium cerebelli
 .احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
.احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes
 Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes Jessica Matthes, Ph.D., ABN Barrow TBI Symposium March 23, 2019 jessica.matthes@dignityhealth.org Outline TBI Mechanisms of Injury Types
Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes Jessica Matthes, Ph.D., ABN Barrow TBI Symposium March 23, 2019 jessica.matthes@dignityhealth.org Outline TBI Mechanisms of Injury Types
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
The Human Brain: Anatomy, Functions, and Injury
 The Human Brain: Anatomy, Functions, and Injury Main Menu Brain Anatomy Brain Functions Injury Mechanisms Brain Anatomy Menu Skull Anatomy Interior Skull Surface Blood Vessels of the Brain Arteries of
The Human Brain: Anatomy, Functions, and Injury Main Menu Brain Anatomy Brain Functions Injury Mechanisms Brain Anatomy Menu Skull Anatomy Interior Skull Surface Blood Vessels of the Brain Arteries of
Cerebrovascular diseases-2
 Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
NEURORADIOLOGY DIL part 3
 NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
10/6/2017. Notice. Traumatic Brain Injury & Head Trauma
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Pediatric Abusive Head Trauma
 Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8:
 Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and
 1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
Mild Traumatic Brain Injury
 Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage
 July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
Organization of The Nervous System PROF. MOUSAED ALFAYEZ & DR. SANAA ALSHAARAWY
 Organization of The Nervous System PROF. MOUSAED ALFAYEZ & DR. SANAA ALSHAARAWY Objectives At the end of the lecture, the students should be able to: List the parts of the nervous system. List the function
Organization of The Nervous System PROF. MOUSAED ALFAYEZ & DR. SANAA ALSHAARAWY Objectives At the end of the lecture, the students should be able to: List the parts of the nervous system. List the function
Chapter 7: Head & Neck
 Chapter 7: Head & Neck Osteology I. Overview A. Skull The cranium is composed of irregularly shaped bones that are fused together at unique joints called sutures The skull provides durable protection from
Chapter 7: Head & Neck Osteology I. Overview A. Skull The cranium is composed of irregularly shaped bones that are fused together at unique joints called sutures The skull provides durable protection from
Department of Forensic Medicine, University of Dundee HEAD INJURY
 Department of Forensic Medicine, University of Dundee Lecture Notes Head Injury Scalp injury Skull fracture Intracranial haemorrhage (extradural, subdural, subarachnoid, intracerebral) Brain injury Complications
Department of Forensic Medicine, University of Dundee Lecture Notes Head Injury Scalp injury Skull fracture Intracranial haemorrhage (extradural, subdural, subarachnoid, intracerebral) Brain injury Complications
Chapter 14. The Brain Meninges and Cerebral Spinal Fluid
 Chapter 14 The Brain Meninges and Cerebral Spinal Fluid Meninges of the Brain Skull Brain: Blood vessel Pia mater Gray matter White matter Dura mater: Periosteal layer Meningeal layer Arachnoid villus
Chapter 14 The Brain Meninges and Cerebral Spinal Fluid Meninges of the Brain Skull Brain: Blood vessel Pia mater Gray matter White matter Dura mater: Periosteal layer Meningeal layer Arachnoid villus
IV. Cerebrovascular diseases
 IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
Concussion. Concussion is a disturbance of brain function caused by a direct or indirect force to the head.
 Concussion Concussion is a disturbance of brain function caused by a direct or indirect force to the head. Disturbances of brain tissue is largely related to neurometabolic dysfunction rather then structural
Concussion Concussion is a disturbance of brain function caused by a direct or indirect force to the head. Disturbances of brain tissue is largely related to neurometabolic dysfunction rather then structural
POST-INJURY INTERVALS 1
 POST-INJURY INTERVALS 1 Introduction 1 Contusion dating 2 Skin 2 Brain 5 Hypoxic/ischemic injury and increased intracranial pressure 18 Brain incidentals (non-injurious) 21 Sexual violence 27 INTRODUCTION
POST-INJURY INTERVALS 1 Introduction 1 Contusion dating 2 Skin 2 Brain 5 Hypoxic/ischemic injury and increased intracranial pressure 18 Brain incidentals (non-injurious) 21 Sexual violence 27 INTRODUCTION
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Brain Meninges, Ventricles and CSF
 Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
BATLS Battlefield Advanced Trauma Life Support
 J R Army Med Corps 2002; 148: 151-158 BATLS Battlefield Advanced Trauma Life Support CHAPTER 8 HEAD INJURIES Aim 0801. On successfully completing this topic you will be able to: Discuss general management
J R Army Med Corps 2002; 148: 151-158 BATLS Battlefield Advanced Trauma Life Support CHAPTER 8 HEAD INJURIES Aim 0801. On successfully completing this topic you will be able to: Discuss general management
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Department of Cognitive Science UCSD
 Department of Cognitive Science UCSD Verse 1: Neocortex, frontal lobe, Brain stem, brain stem, Hippocampus, neural node, Right hemisphere, Pons and cortex visual, Brain stem, brain stem, Sylvian fissure,
Department of Cognitive Science UCSD Verse 1: Neocortex, frontal lobe, Brain stem, brain stem, Hippocampus, neural node, Right hemisphere, Pons and cortex visual, Brain stem, brain stem, Sylvian fissure,
Ventricles, CSF & Meninges. Steven McLoon Department of Neuroscience University of Minnesota
 Ventricles, CSF & Meninges Steven McLoon Department of Neuroscience University of Minnesota 1 Coffee Hour Thursday (Sept 14) 8:30-9:30am Surdyk s Café in Northrop Auditorium Stop by for a minute or an
Ventricles, CSF & Meninges Steven McLoon Department of Neuroscience University of Minnesota 1 Coffee Hour Thursday (Sept 14) 8:30-9:30am Surdyk s Café in Northrop Auditorium Stop by for a minute or an
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
The Nervous System PART B
 7 The Nervous System PART B PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB Central Nervous System
7 The Nervous System PART B PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB Central Nervous System
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cranial cavity. Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology
 Cranial cavity Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology Cerebrum Cerebral hemispheres The Meninges The brain in the skull is surrounded by three membranes or meninges: 1-THE DURA
Cranial cavity Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology Cerebrum Cerebral hemispheres The Meninges The brain in the skull is surrounded by three membranes or meninges: 1-THE DURA
Organization of The Nervous System PROF. SAEED ABUEL MAKAREM
 Organization of The Nervous System PROF. SAEED ABUEL MAKAREM Objectives By the end of the lecture, you should be able to: List the parts of the nervous system. List the function of the nervous system.
Organization of The Nervous System PROF. SAEED ABUEL MAKAREM Objectives By the end of the lecture, you should be able to: List the parts of the nervous system. List the function of the nervous system.
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
Cranial cavity. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Cranial cavity Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology The Meninges The brain in the skull is surrounded by three membranes or meninges: 1-DURA MATER 2-ARACHNOID MATER 3-PIA MATER
Cranial cavity Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology The Meninges The brain in the skull is surrounded by three membranes or meninges: 1-DURA MATER 2-ARACHNOID MATER 3-PIA MATER
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults
 Research Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults Mark T. Pfefer, RN, MS, DC *1 ; Richard Strunk MS, DC 2 Address: 1 Professor and Director of Research, Cleveland Chiropractic
Research Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults Mark T. Pfefer, RN, MS, DC *1 ; Richard Strunk MS, DC 2 Address: 1 Professor and Director of Research, Cleveland Chiropractic
TRAUMATIC BRAIN INJURY. Moderate and Severe Brain Injury
 TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Most hypertensive: headache, vomiting, seizures, changes in mental status, fever, changes EKG
 Wk 2. Management of Clients with Stroke 1. Stroke neurologic changes by interruption in blood supply to brain 1) Etiology Ischemia: thrombosis or embolism thrombotic strokes > embolic strokes (1) Thrombosis
Wk 2. Management of Clients with Stroke 1. Stroke neurologic changes by interruption in blood supply to brain 1) Etiology Ischemia: thrombosis or embolism thrombotic strokes > embolic strokes (1) Thrombosis
M555 Medical Neuroscience Blood Flow in CNS Meninges Blood Brain Barrier CSF
 M555 Medical Neuroscience Blood Flow in CNS Meninges Blood Brain Barrier CSF Arterial Blood Flow to CNS approximately % of what goes wrong within the skull that produces neurological deficits is vascular
M555 Medical Neuroscience Blood Flow in CNS Meninges Blood Brain Barrier CSF Arterial Blood Flow to CNS approximately % of what goes wrong within the skull that produces neurological deficits is vascular
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
The Nervous System. PowerPoint Lecture Slides C H A P T E R 7. Prepared by Patty Bostwick-Taylor, Florence-Darlington Technical College
 PowerPoint Lecture Slides Prepared by Patty Bostwick-Taylor, Florence-Darlington Technical College C H A P T E R 7 The Nervous System NERVOUS SYSTEM OVERVIEW Essential Question: What are the primary functions
PowerPoint Lecture Slides Prepared by Patty Bostwick-Taylor, Florence-Darlington Technical College C H A P T E R 7 The Nervous System NERVOUS SYSTEM OVERVIEW Essential Question: What are the primary functions
Injuries to the head and spine
 Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Central Nervous System - Brain & Cranial Nerves. Chapter 14 Part A
 Central Nervous System - Brain & Cranial Nerves Chapter 14 Part A Central Nervous System Central nervous system (CNS) is responsible for: Receiving impulses from receptors Integrating information Sending
Central Nervous System - Brain & Cranial Nerves Chapter 14 Part A Central Nervous System Central nervous system (CNS) is responsible for: Receiving impulses from receptors Integrating information Sending
Cerebral Blood Vessel Damage in Traumatic Brain Injury. Department of Mechanical Engineering, University of Utah 2
 Cerebral Blood Vessel Damage in Traumatic Brain Injury Kenneth L. Monson, 1,2,* Matthew Converse, 1 Geoffrey T. Manley 3 1 Department of Mechanical Engineering, University of Utah 2 Department of Bioengineering,
Cerebral Blood Vessel Damage in Traumatic Brain Injury Kenneth L. Monson, 1,2,* Matthew Converse, 1 Geoffrey T. Manley 3 1 Department of Mechanical Engineering, University of Utah 2 Department of Bioengineering,
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
CSF. Cerebrospinal Fluid(CSF) System
 System") Cerebrospinal Fluid(CSF) System By the end of the lecture, students must be able to describe Physiological Anatomy of CSF Compartments Composition Formation Circulation Reabsorption CSF Pressure Functions
Cerebrospinal Fluid(CSF) System By the end of the lecture, students must be able to describe Physiological Anatomy of CSF Compartments Composition Formation Circulation Reabsorption CSF Pressure Functions
Chapter 10 The Nervous System: The Brain and Cranial Nerves
 Chapter 10 The Nervous System: The Brain and Cranial Nerves Copyright 2015 Wolters Kluwer Health Lippincott Williams & Wilkins Overview Key Terms aphasia corpus callosum meninges basal nuclei diencephalon
Chapter 10 The Nervous System: The Brain and Cranial Nerves Copyright 2015 Wolters Kluwer Health Lippincott Williams & Wilkins Overview Key Terms aphasia corpus callosum meninges basal nuclei diencephalon
Biological Bases of Behavior. 3: Structure of the Nervous System
 Biological Bases of Behavior 3: Structure of the Nervous System Neuroanatomy Terms The neuraxis is an imaginary line drawn through the spinal cord up to the front of the brain Anatomical directions are
Biological Bases of Behavior 3: Structure of the Nervous System Neuroanatomy Terms The neuraxis is an imaginary line drawn through the spinal cord up to the front of the brain Anatomical directions are
Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE
 Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE") Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE 1 The two parietal bones articulate in the midline AT THE SAGITTAL
Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE 1 The two parietal bones articulate in the midline AT THE SAGITTAL
Essential Neurology for Concussion Evaluations. Aftab Merchant, MBBS, FCPS Professor Pre-Clinical Sciences Cleveland University Kansas City
 Essential Neurology for Concussion Evaluations Aftab Merchant, MBBS, FCPS Professor Pre-Clinical Sciences Cleveland University Kansas City Learning Objectives Recognize the clinical features of concussion
Essential Neurology for Concussion Evaluations Aftab Merchant, MBBS, FCPS Professor Pre-Clinical Sciences Cleveland University Kansas City Learning Objectives Recognize the clinical features of concussion
BRAIN PART I (A & B): VENTRICLES & MENINGES
: VENTRICLES & MENINGES") BRAIN PART I (A & B): VENTRICLES & MENINGES Cranial Meninges Cranial meninges are continuous with spinal meninges Dura mater: inner layer (meningeal layer) outer layer (endosteal layer) fused to periosteum
BRAIN PART I (A & B): VENTRICLES & MENINGES Cranial Meninges Cranial meninges are continuous with spinal meninges Dura mater: inner layer (meningeal layer) outer layer (endosteal layer) fused to periosteum
Characteristic features of CNS pathology. By: Shifaa AlQa qa
 Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
ACTIVITY 7: NERVOUS SYSTEM HISTOLOGY, BRAIN, CRANIAL NERVES
 ACTIVITY 7: NERVOUS SYSTEM HISTOLOGY, BRAIN, CRANIAL NERVES LABORATORY OBJECTIVES: 1. Histology: Identify structures indicated on three different slides or images of nervous system tissue. These images
ACTIVITY 7: NERVOUS SYSTEM HISTOLOGY, BRAIN, CRANIAL NERVES LABORATORY OBJECTIVES: 1. Histology: Identify structures indicated on three different slides or images of nervous system tissue. These images
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage ILOS To list the causes of intracranial haemorrhage. To understand the pathogenesis of each cause.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage ILOS To list the causes of intracranial haemorrhage. To understand the pathogenesis of each cause.
THE ESSENTIAL BRAIN INJURY GUIDE
 THE ESSENTIAL BRAIN INJURY GUIDE Carolyn Scott PhD, CBIST Rainbow Rehab Centers Neuroanatomy & Neuroplasticity Section 2 Neuroanatomy and Neuroimaging Chapter 2 2 Learning Objectives Understand the anatomy
THE ESSENTIAL BRAIN INJURY GUIDE Carolyn Scott PhD, CBIST Rainbow Rehab Centers Neuroanatomy & Neuroplasticity Section 2 Neuroanatomy and Neuroimaging Chapter 2 2 Learning Objectives Understand the anatomy
The Dangers of CTE. James Ryan Cox. Skylar Spriggs. Sawyer Solfest. Team THS131
 The Dangers of CTE James Ryan Cox Skylar Spriggs Sawyer Solfest Team THS131 Dec 10th, 2017 The human body works alike to a well-oiled machine, each vital organ working as a valuable gear or cog. Yet if
The Dangers of CTE James Ryan Cox Skylar Spriggs Sawyer Solfest Team THS131 Dec 10th, 2017 The human body works alike to a well-oiled machine, each vital organ working as a valuable gear or cog. Yet if
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Dissection of the Sheep Brain
 Dissection of the Sheep Brain Laboratory Objectives After completing this lab, you should be able to: 1. Identify the main structures in the sheep brain and to compare them with those of the human brain.
Dissection of the Sheep Brain Laboratory Objectives After completing this lab, you should be able to: 1. Identify the main structures in the sheep brain and to compare them with those of the human brain.
NOTES CHAPTER 9 (Brief) The Nervous System LECTURE NOTES
 The Nervous System LECTURE NOTES") NOTES CHAPTER 9 (Brief) The Nervous System LECTURE NOTES I. Divisions of the Nervous System two major divisions A. Central Nervous System (CNS) 1. brain 2. spinal cord B. Peripheral Nervous System (PNS)
NOTES CHAPTER 9 (Brief) The Nervous System LECTURE NOTES I. Divisions of the Nervous System two major divisions A. Central Nervous System (CNS) 1. brain 2. spinal cord B. Peripheral Nervous System (PNS)
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Nervous system, integration: Overview, and peripheral nervous system:
 Nervous system, integration: Overview, and peripheral nervous system: Some review & misc. parts [Fig. 28.11B, p. 573]: - white matter --> looks white due to the myelinated sheaths, which are quite fatty.
Nervous system, integration: Overview, and peripheral nervous system: Some review & misc. parts [Fig. 28.11B, p. 573]: - white matter --> looks white due to the myelinated sheaths, which are quite fatty.
CEREBROVASCULAR DISEASES. By: Shifaa AlQa qa
 CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
Neurology study of the nervous system. nervous & endocrine systems work together to maintain homeostasis
 Nervous System Neurology study of the nervous system nervous & endocrine systems work together to maintain homeostasis Nervous System works very fast Uses electrical signals called nerve impulses Short-lived
Nervous System Neurology study of the nervous system nervous & endocrine systems work together to maintain homeostasis Nervous System works very fast Uses electrical signals called nerve impulses Short-lived
The CNS Part II pg
 The CNS Part II pg. 455-474 Protection of the Brain Objectives Describe how the meninges, cerebrospinal fluid, and the blood brain barrier protect the CNS. Explain how Cerebrospinal fluid is formed, and
The CNS Part II pg. 455-474 Protection of the Brain Objectives Describe how the meninges, cerebrospinal fluid, and the blood brain barrier protect the CNS. Explain how Cerebrospinal fluid is formed, and
meninges Outermost layer of the meninge dura mater arachnoid mater pia mater membranes located between bone and soft tissue of the nervous system
 membranes located between bone and soft tissue of the nervous system meninges Outermost layer of the meninge dura mater middle layer of the meninges, contains no blood vessels arachnoid mater Innermost
membranes located between bone and soft tissue of the nervous system meninges Outermost layer of the meninge dura mater middle layer of the meninges, contains no blood vessels arachnoid mater Innermost
Central Nervous System Practical Exam. Chapter 12 Nervous System Cells. 1. Please identify the flagged structure.
 Central Nervous System Practical Exam Chapter 12 Nervous System Cells 1. Please identify the flagged structure. 2. Please identify the flagged structure. 3. Please identify the flagged structure. 4. A
Central Nervous System Practical Exam Chapter 12 Nervous System Cells 1. Please identify the flagged structure. 2. Please identify the flagged structure. 3. Please identify the flagged structure. 4. A
HAEMORRHAGIA Bleeding
 HAEMORRHAGIA Bleeding Cassification Size Location pathomechanism Hematoma: external or may be enclosed within a tissue petechiae : 1-2 mm hemorrhages into skin, mucous membranes, or serosal surfaces increased
HAEMORRHAGIA Bleeding Cassification Size Location pathomechanism Hematoma: external or may be enclosed within a tissue petechiae : 1-2 mm hemorrhages into skin, mucous membranes, or serosal surfaces increased
Overview of Abusive Head Trauma: What Everyone Needs to Know. 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012
 Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
The SCALP. Prof. Dr. Muhammad Imran Qureshi
 The SCALP By Prof. Dr. Muhammad Imran Qureshi The SCALP includes FIVE layers external to the Calvaria. These are: S: Skin & Superficial Fascia C: Connective Tissue A: Aponeurosis (Epicranial) L: Loose
The SCALP By Prof. Dr. Muhammad Imran Qureshi The SCALP includes FIVE layers external to the Calvaria. These are: S: Skin & Superficial Fascia C: Connective Tissue A: Aponeurosis (Epicranial) L: Loose
Alterations of Neurologic Function
 Pathophysiology JP Advis DVM, Ph.D. Bartlett Hall, Animal Sciences, Cook, 932-9240, advis@aesop.rutgers.edu 08 Course website: rci.rutgers.edu/~advis Lectures, tests, grades, office hours, textbook, Material
Pathophysiology JP Advis DVM, Ph.D. Bartlett Hall, Animal Sciences, Cook, 932-9240, advis@aesop.rutgers.edu 08 Course website: rci.rutgers.edu/~advis Lectures, tests, grades, office hours, textbook, Material
BIOL Dissection of the Sheep and Human Brain
 BIOL 2401 Dissection of the Sheep and Human Brain Laboratory Objectives After completing this lab, you should be able to: Identify the main structures in the sheep brain and to compare them with those
BIOL 2401 Dissection of the Sheep and Human Brain Laboratory Objectives After completing this lab, you should be able to: Identify the main structures in the sheep brain and to compare them with those
Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review
 Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review M B Moss, MD; L Lanier, MD; R Slater; C L Sistrom, MD; R G Quisling, MD; I M Schmalfuss, MD; and D Rajderkar, MD Contact:
Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review M B Moss, MD; L Lanier, MD; R Slater; C L Sistrom, MD; R G Quisling, MD; I M Schmalfuss, MD; and D Rajderkar, MD Contact:
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Slide 1. Slide 2. Slide 3
 Slide 1 Eric S. Hart, Psy.D., ABPP-CN Associate Clinical Professor Director of Adult Neuropsychology Associate Chair University of Missouri-Columbia Department of Health Psychology Slide 2 A traumatic
Slide 1 Eric S. Hart, Psy.D., ABPP-CN Associate Clinical Professor Director of Adult Neuropsychology Associate Chair University of Missouri-Columbia Department of Health Psychology Slide 2 A traumatic
Pediatric Trauma Initial Evaluation and management
 Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Basic Brain Information
 Basic Brain Information Brain facts Your brain weighs about 3lbs, or just under 1.5Kg It has the texture of blancmange Your brain is connected to your spinal cord by the brain stem Behind your brain stem
Basic Brain Information Brain facts Your brain weighs about 3lbs, or just under 1.5Kg It has the texture of blancmange Your brain is connected to your spinal cord by the brain stem Behind your brain stem
Tutorials. By Dr Sharon Truter
 Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Head & Brain Trauma. Presented By: Steven Jones, NREMT-P
 Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common