Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
|
|
|
- Suzan Bradford
- 5 years ago
- Views:
Transcription
1 Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
2 Reorganization of Recommendations RECOMMENDATIONS: 2008 RECOMMENDATIONS: 1. Public Awareness (1) 2. Patient and Caregiver Education (1) 3. Stroke Prevention (7) 4. Acute Stroke Management (8) 5. Stroke Rehabilitation (6) 6. Follow-up and Community Reengagement (1) 1. Public Awareness and Patient Education (2) 2. Stroke Prevention (7) 3. Hyperacute Stroke Care (7) 4. Acute Inpatient Stroke Management (2) 5. Stroke Rehabilitation & Community Reintegration (5) 6. Selected Topics in Stroke Management (4)
3 Canadian Best Practice Recommendations for Stroke Care (2008) Topic Areas 1.0 Public Awareness and Patient Education Public awareness and responsiveness Patient and family education 2.0 Prevention of Stroke Lifestyle and risk factor management Blood pressure management Lipid management Diabetes management Antiplatelet therapy Antithrombotic therapy for atrial fibrillation Carotid intervention 3.0 Hyperacute Stroke Management Emergency medical services prior to hospital arrival Acute management of transient ischemic attack and minor stroke Neurovascular imaging Blood glucose Acute thrombolytic therapy Acute aspirin therapy Management of subarachnoid and intracerebral hemorrhage
4 Canadian Best Practice Recommendations for Stroke Care (2008) Topic Areas 4.0 Acute Stroke Management Acute stroke unit care Components of acute inpatient care 5.0 Stroke Rehabilitation and Recovery Initial stroke rehabilitation assessment Provision of inpatient rehabilitation Components of inpatient stroke rehabilitation Outpatient and communitybased rehabilitation Follow-up and evaluation in the community 6.0 Selected Key Topics in Stroke Management Dysphagia assessment Identification and management of poststroke depression Vascular cognitive impairment and dementia Shoulder pain assessment and treatment
5 Recommendation Format Best Practice Recommendation Rationale System Implications Performance Measures Measurement Notes Summary of Current Evidence
6 Recommendation # 3 Hyperacute Stroke Management
7 3.0 Hyperacute Stroke Management Hyperacute care is defined as the health care activities that take place from the time of first contact between a patient with potential stroke and medical care until the patient is either admitted to hospital or discharged back into the community
8 3.0 Hyperacute Stroke Management 3.1 Emergency medical services management of acute stroke patients 3.2 Acute management of transient ischemic attack and minor stroke 3.3 Neurovascular imaging 3.4 Blood glucose abnormalities 3.5 Acute thrombolytic therapy 3.6 Acute ASA therapy 3.7 Management of subarachnoid and intracerebral hemorrhage


9 3.1 Emergency Medical Services Management of Acute Stroke Patients Patients who show signs and symptoms of hyperacute stroke, usually defined as symptom onset within the previous 4.5 hours, must be treated as time-sensitive emergency cases and should be transported without delay to the closest institution that provides emergency stroke care
10 3.1 Emergency Medical Services Management of Acute Stroke Patients Immediate contact with emergency services (e.g.911) by patients or other members of the public is strongly recommended because it reduces time to treatment for acute stroke Emergency medical services dispatchers must triage patients showing signs and symptoms of hyperacute stroke as a priority dispatch. A standardized acute stroke diagnostic screening tool should be used by paramedics Out-of hospital patient management should be optimized to meet the needs of suspected acute stroke patients
11 3.1 Emergency Medical Services Management of Acute Stroke Patients Direct Transfer Protocols must be in place to facilitate the transfer of eligible patients to the closest and most appropriate facility providing acute stroke care Direct Transport Protocol criteria must be based on: 1. Both symptom duration and anticipated transport duration being less than the therapeutic window 2. Other acute care needs of the patient
12 3.1 Emergency Medical Services Management of Acute Stroke Patients History of event including: Time of onset Signs and symptoms Previous medical and drug history Must be obtained from the patient or informant The receiving facility must be notified of a suspected acute stroke patient in order for the facility to prepare Transfer of care from paramedics to receiving facility personnel must occur without delay
13 System Implications Scope of out-of-hospital care is from first patient contact with emergency medical services to the transfer of care to the receiving facility Dispatchers training Paramedic education Direct transport agreements Coordinated, seamless transport and disposition Communication systems to support access
14 Performance Measures Percentage of suspected stroke patients arriving in the ED who were transported by EMS Time from initial call received by emergency dispatch centre to EMS arrival on patient scene Time from EMS arrival on patient scene to arrival at appropriate ED Percentage of potential stroke patients transported by EMS who received a final diagnosis of stroke or TIA during hospital stay
15 3.2 Acute Management of Transient Ischemic Attack and Minor Stroke Patients who present with symptoms suggestive of minor stroke or transient ischemic attack must undergo a comprehensive evaluation to confirm the diagnosis and begin treatment to reduce the risk of major stroke as soon as is appropriate to the clinical situation
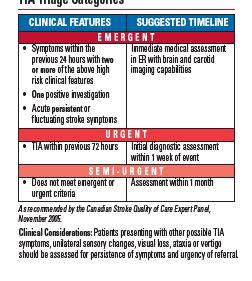
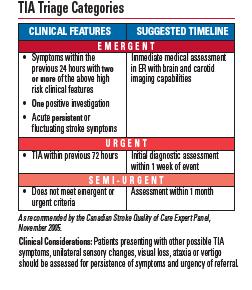
16 3.2a Assessment Immediate clinical evaluation and additional investigations as required to establish the diagnosis, rule out stroke mimics and develop a plan of care Use of standardized risk stratification tool at the initial point of healthcare contact should be used to guide the triage process Patients should be referred to a designated stroke prevention clinic or to a physician with expertise in stroke assessment and management
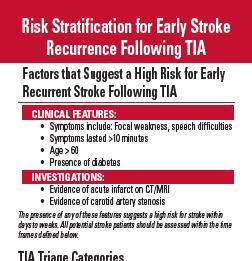
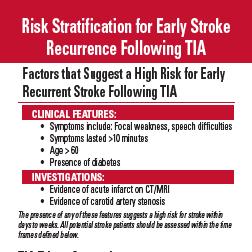
17 Risk Stratification for Early Stroke Recurrence Following TIA
18 3.2a Assessment Patients require brain imaging with computed tomography or magnetic resonance imaging Emergent patients classified at highest risk of recurrent stroke should have neurovascular imaging within 24 hours Those patients classified as urgent should have neurovascular imaging within 7 days Patients who may be candidates for carotid revascularization should have computed tomographic angiography (CTA),magnetic resonance angiography (MRA) or a carotid duplex ultrasound as soon as possible (within 24 hours for emergent patients and seven days for urgent patients)
19 3.2a Assessment The following should be undertaken routinely: CBC Electrolytes Renal function Cholesterol level Glucose level Electrocardiogram Pts. with confirmed cerebral infarction on brain imaging should undergo comprehensive outpatient assessment for functional impairment within 2 weeks including: Cognitive evaluation Screen for depression Determination of fitness to drive Functional assessment for potential rehabilitation treatment
20 3.2b Management All patients with transient ischemic attack or minor stroke not on an antiplatelet agent at the time of presentation should be started on antiplatelet therapy immediately after brain imaging has excluded intracranial hemorrhage. The initial dose of ASA should be at least 160 mg. The loading dose for clopidogrel is 300mg.
21 3.2b Management Patients with transient ischemic attack or minor stroke and >70% carotid stenosis and select patients with acutely symptomatic 50-56% carotid stenosis on the side implicated by their neurological symptoms, who are otherwise candidates for carotid revascularization, should have carotid endarterectomy performed as soon as possible within 2 weeks

22 Carotid Artery Disease
23 Computerized Tomography Imaging and Angiogram s/cad.shtml


24 Magnetic Resonance Imaging/Angiography
25 3.2b Management Patients with TIA or minor stroke and atrial fibrillation should begin anticoagulation using warfarin immediately after brain imaging has excluded intracranial hemorrhage, aiming for a therapeutic INR 2 to 3 All risk factors for cerebrovascular disease must be aggressively managed both with pharmacological and non-pharmacological means to achieve optimal control Patients with TIA or minor stroke who smoke cigarettes should be strongly counseled to quit immediately and be provided with both pharmacological and non-pharmacological strategies.
26 System Implications Processes and protocols in place to enable patients with TIA or minor stroke to rapidly access services Physicians have training and knowledge to manage patients Stroke prevention clinics are accessible
27 Selected Performance Measures Recurrence of stroke or transient ischemic attack within: 30 days 90 days 1 year Time from first encounter with medical care (primary care or emergency department) to neurological assessment by a stroke expert Time from first encounter with medical care to brain imaging (CT/MRI) and other vascular imaging
28 3.3. Neurovascular Imaging All patients with suspected acute stroke or transient ischemic attack should undergo brain imaging immediately The initial modality of choice is a non-contrast Computed Tomography scan Vascular Imaging should be done as soon as possible to better understand the cause of the stroke event and to guide management Imaging includes: CTA, MRA, catheter angiography and duplex ultrasound
29 3.3 Neurovascular Imaging If MRI is performed, it should include diffusionweighted sequences to detect ischemia and gradient echo and FLAIR sequences to determine extent of infarct or presence of hemorrhage Carotid imaging should be performed within 24 hours of a carotid territory transient ischemic attack or non-disabling ischemic stroke ( if not done as part of the original assessment) unless the patient is clearly not a candidate for carotid endarterectomy.
30 3.3 Neurovascular Imaging In children, if the initial CT is negative,mri should be performed to assist diagnosis and management plans In pediatric cases, cerebral and cervical In pediatric cases, cerebral and cervical arteries should be imaged as soon as possible, preferably within 24 hours.
31 System Implications Initial assessment performed by experienced clinicians Timely access to diagnostic services Organized system of care across regions to Organized system of care across regions to ensure timely access to diagnostic services if not available at the initial hospital
32 Selected Performance Measures Proportion of stroke patients who receive a brain CT/MRI within 25 minutes of hospital arrival (if tpa eligible) Proportion of stroke patients who receive a brain CT/MRI within 24 hours of hospital arrival Proportion of stroke patients who receive carotid imaging prior to hospital discharge Proportion of patients who do not undergo carotid imaging in hospital who have an appointment booked before discharge for carotid imaging as an outpatient
33 3.4 Blood Glucose Abnormalities All patients with suspected acute stroke should have their blood glucose concentration checked immediately. Blood glucose measurement should be repeated if the first value is abnormal or if the patient is known to have diabetes Elevated blood glucose concentrations should be treated with glucose lowering agents
34 Selected Performance Measures Proportion of patients with blood glucose levels documented during assessment in the emergency department or on the inpatient ward Proportion of patients with known diabetes who have blood glucose levels in therapeutic range for that patient
35 3.5 Acute Thrombolytic Therapy All patients with disabling acute ischemic stroke who can be treated within 4.5 hours after symptom onset should be evaluated without delay to determine their eligibility for treatment with intravenous tissue plasminogen activator (alteplase). Eligible patients are those who can receive intravenous alteplase within 4.5 hours of the onset of stroke symptoms in accordance with criteria adapted from the NINDS rt-pa Stroke Study and ECASSIII
36 3.5 Acute Thrombolytic Therapy All eligible patients should receive tpa within one hour of hospital arrival. Administration of alteplase should follow the American Stroke Association guidelines In cases where the initial CT shows greater than 1/3 MCA (ASPECTS score < 5), physician judgment and wishes of the patient/family are important considerations in the decision to treat with alteplase For pediatric patients, tpa should only be considered within a clinical research protocol Note: in Canada, alteplase is currently approved by Health Canada for use in adults with acute ischemic stroke within 3 hours of symptom onset (Dec. 2008)
37 Selected Performance Measures Proportion of all ischemic stroke patients who receive treatment with alteplase Proportion of all eligible ischemic stroke patients who receive treatment with alteplase Proportion of all thrombolysed stroke patients who receive alteplase within 1 hour of hospital arrival Median time from patient arrival in the ED to administration of alteplase (in minutes) Proportion of patients in rural or remote communities who receive alteplase through use of telestroke technology
38 3.6 Acute ASA Therapy All acute stroke patients should be given at least 160mg of acetylsalicylic acid (ASA) immediately as a one time loading dose after brain imaging has excluded intracranial hemorrhage In patients treated with t-pa, ASA should be delayed until after the 24 hour post-thrombolysis scan has excluded intracranial hemorrhage ASA ( mg daily) should then be continued indefinitely or until an alternative antithrombotic regime is started
39 3.6 Acute Aspirin Therapy In dysphagic patients, ASA may be given by enteral tube or by rectal suppository In pediatric patients, initial treatment with low molecular weight heparin should be considered and continued until vertebral artery dissection and intracardiac thrombus is excluded. If neither is present, switch to acute aspirin therapy at dose of 3-5 mg/kg
40 Selected Performance Measures Proportion of ischemic stroke patients who receive acute ASA therapy within the first 48 hours following a stroke event Median time from stroke onset to administration of first dose of ASA in hospital
41 3.7 Management of Subarachnoid and Intracerebral Hemorrhage Patients with suspected subarachnoid hemorrhage should have an urgent neurosurgical consultation for diagnosis and treatment Patients with cerebellar hemorrhage should have an urgent neurosurgical consultation for consideration of craniotomy and evaluation of the hemorrhage Patients with supratentorial intracerebral hemorrhage should be cared for on a stroke unit
42 Selected Performance Measures Proportion of hemorrhagic stroke patients treated in an acute stroke unit Proportion of total time in hospital spent on an acute stroke unit Percentage of hemorrhagic stroke patients who receive a neurosurgical consult while in hospital Proportion of hemorrhagic stroke patients discharged to their place of residence, inpatient stroke rehabilitation, complex continuing care or long-term care Mortality rate for subarachnoid and intracerebral hemorrhage at 30 days in hospital
43 Implementation Tips Form a working group- consider both local and regional representation Assess current practices using the Canadian Best Practice Recommendations for Stroke Care Update (2008) Gap Analysis Tool Identify strengths, challenges, opportunities Identify 2-3 priorities for action Identify local and regional champions
44 Implementation Tips Identify professional education needs and develop a professional education learning plan Consider local or regional workshops to focus on acute stroke management Access resources such as Heart and Stroke Foundation, Provincial Contacts Consult with other strategies for lessons learned, resources


45 Coordination of stroke care makes a difference
46 Resources American Association of Neuroscience Nurses American Stroke Association Brain Attack Coalition Canadian Association of Neuroscience Nurses Canadian Hypertension Education Program Canadian Stroke Strategy European Stroke Initiative
47 Resources Heart and Stroke Foundation Heart and Stroke Foundation of Canada Internet Stroke Centre National Institute of Neurological Disorders and Stroke National Stroke Association Scottish Intercollegiate Guidelines Network StrokeEngine
48
Standards of excellence
 The Accreditation Canada Stroke Distinction program was launched in March 2010 to offer a rigorous and highly specialized process above and beyond the requirements of Qmentum. The comprehensive Stroke
The Accreditation Canada Stroke Distinction program was launched in March 2010 to offer a rigorous and highly specialized process above and beyond the requirements of Qmentum. The comprehensive Stroke
for Stroke Care (Update 2013)
") Overview (Version 1.0) May 23 rd, 2013 Page 1 TAKING ACTION TOWARDS OPTIMAL STROKE CARE 2 Table of Contents Section Content Page About this Resource 3 1.0 Overview 4 1.1 Purpose of the Resource Kit 4 2.0
Overview (Version 1.0) May 23 rd, 2013 Page 1 TAKING ACTION TOWARDS OPTIMAL STROKE CARE 2 Table of Contents Section Content Page About this Resource 3 1.0 Overview 4 1.1 Purpose of the Resource Kit 4 2.0
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
CONCISE GUIDE National Clinical Guidelines for Stroke 2nd Edition
 CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
Get With the Guidelines Stroke PMT. Quality Measure Descriptions
 Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Nebraska Medicine Stroke and Neurovascular Center Outcomes
 Nebraska Medicine Stroke and Neurovascular Center Outcomes Stroke Procedure/Treatment Our Performance Joint Commission Benchmark Diagnostic Cerebral Angiogram Stroke within 24 hours post procedure Death
Nebraska Medicine Stroke and Neurovascular Center Outcomes Stroke Procedure/Treatment Our Performance Joint Commission Benchmark Diagnostic Cerebral Angiogram Stroke within 24 hours post procedure Death
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Emergency Department Stroke Registry Process of Care Indicator Specifications (July 1, 2011 June 30, 2012 Dates of Service)
") Specifications Description Methodology NIH Stroke Scale (NIHSS) Performed in Initial Evaluation used to assess the percentage of adult stroke patients who had the NIHSS performed during their initial evaluation
Specifications Description Methodology NIH Stroke Scale (NIHSS) Performed in Initial Evaluation used to assess the percentage of adult stroke patients who had the NIHSS performed during their initial evaluation
TABLE OF CONTENTS. MODULE 1: Pathophysiology of Stroke, Neuroanatomy, and Stroke Syndromes. MODULE 2: Acute Stroke Management
 TABLE OF CONTENTS Orientation Pre-Test (ONLINE ONLY) i. Acknowledgements ii. Acute Stroke Unit Orientation Introduction iii. Nursing/Interprofessional (Self Evaluation Tool) MODULE 1: Pathophysiology of
TABLE OF CONTENTS Orientation Pre-Test (ONLINE ONLY) i. Acknowledgements ii. Acute Stroke Unit Orientation Introduction iii. Nursing/Interprofessional (Self Evaluation Tool) MODULE 1: Pathophysiology of
Antithrombotics: Percent of patients with an ischemic stroke or TIA prescribed antithrombotic therapy at discharge. Corresponding
 Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
TRANSIENT ISCHEMIC ATTACK (TIA)
") TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Section Editor Scott E Kasner, MD
 1 of 6 9/29/2013 6:55 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
1 of 6 9/29/2013 6:55 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
CMAJ JAMC. Canadian Best Practice Recommendations for Stroke Care: Summary. (updated 2008)
") CMAJ JAMC DECEMBER 2, 2008, VOLUME 179(12) LE 2 DÉCEMBRE 2008, VOLUME 179(12) Canadian Best Practice Recommendations for Stroke Care: Summary (updated 2008) CMAJ 2008;179(12 SUPPL):S1-S25 Canadian best
CMAJ JAMC DECEMBER 2, 2008, VOLUME 179(12) LE 2 DÉCEMBRE 2008, VOLUME 179(12) Canadian Best Practice Recommendations for Stroke Care: Summary (updated 2008) CMAJ 2008;179(12 SUPPL):S1-S25 Canadian best
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
2017 Stroke Statistics
 2017 Stroke Statistics 2017 LUMC Stroke Volumes by Type of Stroke Ischemic Stroke Treatment by Type 2017 17% 8% 75% Ischemic Intracerebral Hemorrhage Aneurysmal Subarachnoid Hemorrhage 31 42 25 r-tpa Administered
2017 Stroke Statistics 2017 LUMC Stroke Volumes by Type of Stroke Ischemic Stroke Treatment by Type 2017 17% 8% 75% Ischemic Intracerebral Hemorrhage Aneurysmal Subarachnoid Hemorrhage 31 42 25 r-tpa Administered
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Emergency Department Stroke Registry Indicator Specifications 2018 Report Year (07/01/2017 to 06/30/2018 Discharge Dates)
") 2018 Report Year (07/01/2017 to 06/30/2018 Discharge Dates) Summary of Changes I62.9 added to hemorrhagic stroke ICD-10-CM diagnosis code list (table 3) Measure Description Methodology Rationale Measurement
2018 Report Year (07/01/2017 to 06/30/2018 Discharge Dates) Summary of Changes I62.9 added to hemorrhagic stroke ICD-10-CM diagnosis code list (table 3) Measure Description Methodology Rationale Measurement
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
List of Exhibits Adult Stroke
 List of Exhibits Adult Stroke List of Exhibits Adult Stroke i. Ontario Stroke Audit Hospital and Patient Characteristics Exhibit i. Hospital characteristics from the Ontario Stroke Audit, 200/ Exhibit
List of Exhibits Adult Stroke List of Exhibits Adult Stroke i. Ontario Stroke Audit Hospital and Patient Characteristics Exhibit i. Hospital characteristics from the Ontario Stroke Audit, 200/ Exhibit
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council
 American Society of Neuroradiology What Is a Stroke? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair
American Society of Neuroradiology What Is a Stroke? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Guideline Stroke and transient ischaemic attack in over 16s: diagnosis and initial management
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline Stroke and transient ischaemic attack in over s: diagnosis and initial management Draft for consultation, November 0 This guideline covers interventions
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline Stroke and transient ischaemic attack in over s: diagnosis and initial management Draft for consultation, November 0 This guideline covers interventions
Appendix A: Summary of evidence from surveillance
 Appendix A: Summary of evidence from surveillance 8-year surveillance (2016) stroke and transient ischaemic attack in over 16s (2008) NICE guideline CG68 Summary of new evidence from surveillance... 1
Appendix A: Summary of evidence from surveillance 8-year surveillance (2016) stroke and transient ischaemic attack in over 16s (2008) NICE guideline CG68 Summary of new evidence from surveillance... 1
The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs
 The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs WA State Cardiac & Stroke Conference Brian R. Johnson, Ph.D. Associate Director Hospital Business Development
The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs WA State Cardiac & Stroke Conference Brian R. Johnson, Ph.D. Associate Director Hospital Business Development
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
HAAD quality KPI; waiting time
 Type: Waiting Time Indicator Indicator Number: WT001 Primary Care Appointment- Outpatient Setting Time to see a HAAD licensed family physician or member of their team (GP) Time of request (walk-in or by
Type: Waiting Time Indicator Indicator Number: WT001 Primary Care Appointment- Outpatient Setting Time to see a HAAD licensed family physician or member of their team (GP) Time of request (walk-in or by
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Clinical Guidelines for Stroke Management 2017 Summary Nursing
 Clinical Guidelines for Stroke Management 2017 Summary Nursing This summary is a quick reference to the recommendations in the Clinical Guidelines for Stroke Management 2017 most relevant to nurses. While
Clinical Guidelines for Stroke Management 2017 Summary Nursing This summary is a quick reference to the recommendations in the Clinical Guidelines for Stroke Management 2017 most relevant to nurses. While
Stroke Special Project 640 and 740 Resource For Health Information Management Professionals
 Stroke Special Project 640 and 740 Resource For Health Information Management Professionals Linda Gould RPN Erin Kelleher, BA, CHIM Stefan Pagliuso PT, B.A. Kin(Hon.) Overview of this Resource Overview
Stroke Special Project 640 and 740 Resource For Health Information Management Professionals Linda Gould RPN Erin Kelleher, BA, CHIM Stefan Pagliuso PT, B.A. Kin(Hon.) Overview of this Resource Overview
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Secondary Prevention of Stroke Order and Documentation Template
 The following actions are based on the 2014 Update of for (www.strokebestpractices.ca). This document is intended to be used as a template to ensure alignment of organization specific care with the Stroke
The following actions are based on the 2014 Update of for (www.strokebestpractices.ca). This document is intended to be used as a template to ensure alignment of organization specific care with the Stroke
QUALITY OF STROKE CARE IN CANADA STROKE KEY QUALITY INDICATORS. Update 2016 AND STROKE CASE DEFINITIONS
 QUALITY OF STROKE CARE IN CANADA STROKE KEY QUALITY INDICATORS AND STROKE CASE DEFINITIONS Update 2016 Canadian Stroke Best Practices Stroke Quality Advisory Committee 2016 Heart and Stroke Foundation
QUALITY OF STROKE CARE IN CANADA STROKE KEY QUALITY INDICATORS AND STROKE CASE DEFINITIONS Update 2016 Canadian Stroke Best Practices Stroke Quality Advisory Committee 2016 Heart and Stroke Foundation
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Strategies for Stroke
 Ischemic stroke is a complex disease, the management of which involves features of cardiology, internal medicine and rehabilitative medicine. Is there a thorough, yet simplified, approach to acute ischemic
Ischemic stroke is a complex disease, the management of which involves features of cardiology, internal medicine and rehabilitative medicine. Is there a thorough, yet simplified, approach to acute ischemic
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Operation Stroke. How to Reduce the Risk of Stroke Complications
 Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
GWTG Post-Discharge Follow-up Form
 Bold font = Required field Patient ID: Date of Hospital Admission: / / mm / dd / yyyy Date Follow-up Completed: / / mm / dd / yyyy PATIENT LOGISTICS Method used for Patient follow-up: Chart Review Health
Bold font = Required field Patient ID: Date of Hospital Admission: / / mm / dd / yyyy Date Follow-up Completed: / / mm / dd / yyyy PATIENT LOGISTICS Method used for Patient follow-up: Chart Review Health
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
<INSERT COUNTRY/SITE NAME> All Stroke Events
 WHO STEPS STROKE INSTRUMENT For further guidance on All Stroke Events, see Section 5, page 5-15 All Stroke Events Patient Identification and Patient Characteristics (I 1) Stroke
WHO STEPS STROKE INSTRUMENT For further guidance on All Stroke Events, see Section 5, page 5-15 All Stroke Events Patient Identification and Patient Characteristics (I 1) Stroke
Basilar artery stenosis with bilateral cerebellar strokes on coumadin
 Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Supplementary Online Content
 Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
JAWDA Quarterly Waiting Time Guidelines for (Specialized and General Hospitals)
") JAWDA Waiting Time Guidelines for (Specialized and General Hospitals) January 2019 Page 1 of 22 Table of Contents Executive Summary... 3 About this Guidance... 4 Performance Indicators... 5 APPENDIX -
JAWDA Waiting Time Guidelines for (Specialized and General Hospitals) January 2019 Page 1 of 22 Table of Contents Executive Summary... 3 About this Guidance... 4 Performance Indicators... 5 APPENDIX -
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
2016 Stroke Statistics
 2016 Stroke Statistics Carotid Artery Procedure Mortality Rate *The Joint Commission Requirement < 6 % LUMC 3.0% *The Joint Commission Requirement < 3 % LUMC 0.0% Rate of stroke or death within 30 days
2016 Stroke Statistics Carotid Artery Procedure Mortality Rate *The Joint Commission Requirement < 6 % LUMC 3.0% *The Joint Commission Requirement < 3 % LUMC 0.0% Rate of stroke or death within 30 days
STROKE SERVICE STANDARDS. CLINICAL STANDARDS COMMITTEE June 2014
 STROKE SERVICE STANDARDS CLINICAL STANDARDS COMMITTEE June 2014 A Bhalla (Chair), G Subramanian P Gompertz, D Wilson, B Patel, K Harkness, T Hassan, MR Chowdhury, J Korner, F Doubal STROKE SERVICE STANDARDS
STROKE SERVICE STANDARDS CLINICAL STANDARDS COMMITTEE June 2014 A Bhalla (Chair), G Subramanian P Gompertz, D Wilson, B Patel, K Harkness, T Hassan, MR Chowdhury, J Korner, F Doubal STROKE SERVICE STANDARDS
Anticoagulants and Head Injuries. Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar
 Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Acute Stroke with Alteplase Administration Order Set
 Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
Your Risk for Stroke and How to Be Prepared
 Your Risk for Stroke and How to Be Prepared TABLE OF CONTENTS 01 / 02 / 03 / 04 / 06 / 07 / 08 / 09 / 14 / Stroke Education Stroke: The No. 5 Cause Of Death In The U.S. Is Stroke Preventable? Stroke Risk
Your Risk for Stroke and How to Be Prepared TABLE OF CONTENTS 01 / 02 / 03 / 04 / 06 / 07 / 08 / 09 / 14 / Stroke Education Stroke: The No. 5 Cause Of Death In The U.S. Is Stroke Preventable? Stroke Risk
New Jersey Department of Health ACUTE STROKE REGISTRY (NJASR) VERSION 2.1
 VERSION 2.1") New Jersey Department of Health ACUTE STROKE REGISTRY (NJASR) VERSION 2.1 A. DEMOGRAPHIC DATA *Hospital Type (1): 1=Primary 2=Comprehensive 3=Other *Hospital Code (2): *Hospital Transferred From Code (3):
New Jersey Department of Health ACUTE STROKE REGISTRY (NJASR) VERSION 2.1 A. DEMOGRAPHIC DATA *Hospital Type (1): 1=Primary 2=Comprehensive 3=Other *Hospital Code (2): *Hospital Transferred From Code (3):
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Stroke Systems of Care
 Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary
 SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Team Work in Treatment of Acute Ischemic Stroke
 Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
Variables in Riksstroke - TIA
 Variables in Riksstroke - TIA The TIA registration started 2010 for patients treated in hospital and 2015 it was 67 of 72 hospitals are registrating TIA On the www.riksstroke.org/forms/ you find the Riksstroke
Variables in Riksstroke - TIA The TIA registration started 2010 for patients treated in hospital and 2015 it was 67 of 72 hospitals are registrating TIA On the www.riksstroke.org/forms/ you find the Riksstroke
Canadian Stroke Best Practices Prevention of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 4)
 Order Set (Order Set 4)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department or outpatient setting (family physician s office, ambulatory clinic, out-patient setting etc.)
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department or outpatient setting (family physician s office, ambulatory clinic, out-patient setting etc.)
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
PATIENT S NOTES History and Physical Brain Attack Stroke
 UNIVERSITY HOSPITALS OF CLEVELAND PATIENT S NOTES History and Physical Brain Attack Stroke 040527.01 page 1 of 8 Name Hospital # Date Sex Age Dr. Service Division Rm No Date and Time: Current inpatient
UNIVERSITY HOSPITALS OF CLEVELAND PATIENT S NOTES History and Physical Brain Attack Stroke 040527.01 page 1 of 8 Name Hospital # Date Sex Age Dr. Service Division Rm No Date and Time: Current inpatient
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Do Not Cite. Draft for Work Group Review.
 Defect Free Acute Inpatient Ischemic Stroke Measure Bundle Measure Description Percentage of patients aged 18 years and older with a diagnosis of ischemic stroke OR transient ischemic attack who were admitted
Defect Free Acute Inpatient Ischemic Stroke Measure Bundle Measure Description Percentage of patients aged 18 years and older with a diagnosis of ischemic stroke OR transient ischemic attack who were admitted
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE
 KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE Dr. Grant Stotts Staff Neurologist, Ottawa Hospital Director, Ottawa Stroke Program Medical Director, Champlain Regional Stroke Program
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE Dr. Grant Stotts Staff Neurologist, Ottawa Hospital Director, Ottawa Stroke Program Medical Director, Champlain Regional Stroke Program
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
Acute ischemic stroke is a major cause of morbidity
 Outcomes of Treatment with Recombinant Tissue Plasminogen Activator in Patients Age 80 Years and Older Presenting with Acute Ischemic Stroke Jennifer C. Drost, DO, MPH, and Susana M. Bowling, MD ABSTRACT
Outcomes of Treatment with Recombinant Tissue Plasminogen Activator in Patients Age 80 Years and Older Presenting with Acute Ischemic Stroke Jennifer C. Drost, DO, MPH, and Susana M. Bowling, MD ABSTRACT
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
Brain Attack. Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship. Case Medical Center
 Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Intracranial Atherosclerosis in Asians
 Intracranial Atherosclerosis in Asians Anthony S. Kim, MD Assistant Clinical Professor of Neurology UCSF Neurovascular Service February 27, 2010 Disclosures Research Support National Institutes of Health
Intracranial Atherosclerosis in Asians Anthony S. Kim, MD Assistant Clinical Professor of Neurology UCSF Neurovascular Service February 27, 2010 Disclosures Research Support National Institutes of Health
Diagnosis: Allergies with reaction type:
 Patient Name: Diagnosis: Allergies with reaction type: ICU Stroke-Ischemic S/P tpa Version 2 5/29/14 This order set is designed to be used with an admission set or for a patient already admitted Nursing
Patient Name: Diagnosis: Allergies with reaction type: ICU Stroke-Ischemic S/P tpa Version 2 5/29/14 This order set is designed to be used with an admission set or for a patient already admitted Nursing
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of