Pulmonary Arterial Hypertension RELATED TO CONNECTIVE TISSUE DISORDER The strategy of INITIAL COMBINATION THERAPY
|
|
|
- Gerard Page
- 5 years ago
- Views:
Transcription

1 Pulmonary Arterial Hypertension RELATED TO CONNECTIVE TISSUE DISORDER The strategy of INITIAL COMBINATION THERAPY Eftychia Demerouti MD, MSc, PhD Cardiologist Onassis Cardiac Surgery Center
2 None related to this presentation NAME OF COMPANIES WITH WICH RELATIONSHIP EXISTS Actelion Pharmaceuticals Ltd, Bayer Schering, Galenica, GlaxoSmithKline, Lilly, MSD, Pfizer Ltd NAME OF RELATIONSHIP Consultant, Honoraria, Advisory Board Member

3
4 68% 85% 48% 68% 34% 57% Eur Respir Rev 2012; 21:123,8-18

5 PATHWAY TO IMPROVING LONG-TERM OUTCOMES IN PAH
6 Scleroderma limited cutaneous Emphysema Arterial Hypertension ΒΜΙ 28 Kg/m2 Methotrexate Antihypertensive treatment O2 Dyspnea Echocardiogram 2 years ago, PASP 40 mmhg
 DLCO: 43% HIGH PROBABILITY OF PE IN LEFT UPER LOBE AND RIGHT")
7 po2 (room air) 61 mmhg, PaCO2 36 mmhg P(A-a)O2 25 FiO2 0,21 FVC 80% FEV1 48% FEV1/FVC 59.5% TLC 138,2% (9,23L) DLCO: 43% HIGH PROBABILITY OF PE IN LEFT UPER LOBE AND RIGHT APEX


8



9


10
11 RA (mmhg) 13 PA (mmhg) 104/55/73 PAP (mmhg) 18 Oxymetry PA (O2%) 71.4 LV (O2) 96% WHO III NT-pro BNP 1400 pg/ml 6MWT 320 m CI (l/min/m2) 1,7 PVR (WU) 22


12
13 PATHWAY TO IMPROVING LONG-TERM OUTCOMES IN PAH In CTD patients
14
15 Annual screening WITH DLCO <60% AND DISEASE DURATION>3YEARS WITH SIGNS AND SYMPTOMS RHC Without clinical signs or symptoms 1 st STEP 2 nd STEP Assessment for telangiectasia, anticentromere antibodies, PFT, DLCO ECG, biomarkers (uric acid, NT-proBNP) IF ABNORMAL FINDINGS Echocardiography (TR jet and RA area) and RHC Ann Rheum Dis 2014; 73:
16 J Gerry Coghlan et al. Ann Rheum Dis 2014;73:
17 J Gerry Coghlan et al. Ann Rheum Dis 2014;73:

.")
18 ESC/ERS GUIDELINES, 2015 In patients with SSc spectrum of diseases (defined as patients with systemic sclerosis, mixed connective tissue disease, or other CTDs with prominent scleroderma features such as sclerodactyly, nail fold capillary abnormalities, SSc-specific autoantibodies). No such guidelines exist for other CTDs.


19
20 PATHWAY TO IMPROVING LONG-TERM OUTCOMES IN PAH PAH
21 Idiopathic Heritable 1. BMPR2, 2. ALK1, ENG, SMAD9, CAV1, KCNK3 3.Unknown Drug and toxin induced Associated with CONNECTIVE TISSUE DISORDER CHD HIV Portal Hypertension Schistosomiasis
22 PH classification RA (mmhg) 13 PA (mmhg) 104/55/73 PAP (mmhg) 18 Oxymetry PA (O2%) 71.4 LV (O2) 96% 1. PAH CI (l/min/m2) 1,7 PVR (WU) PH due to Left Heart Disease 3. PH due to Lung Diseases 4. Chronic Thromboembolic Pulmonary Hypertension 5. PH due to unclear or multifactorial mechanisms
23 DIAGNOSTIC APPROACH TO PH SYMPTOMS, SIGNS, HISTORY suggestive of PH ECHOCARDIOGRAM LEFT HEART OR LUNG DISEASE? V/Q SCINTIGRAPHY RHC +/- ANGIO PAH LIKELY COMPATIBLE WITH PH UNDERLYING DISEASE IF SIGNS OF SEVERE PH DISEASE EXPERT CENTER CTEPH EXPERT CENTER CTD PORTOPULMONARY SCHISTOSOMIASIS HIV PVOD, PCH DRUGS, TOXINS JACC 2013; 62: D42-50

24


25 Myocardial fibrosis is thought to occur after repeated focal ischaemia

 18")

26 PA (mmhg) 104/55/73 PAP (mmhg) 18 DPG: 37 mmhg

27 LUNG RHC: PAPmean>25mmHg, PVR>3WU
28 Idiopathic Heritable 1. BMPR2, 2. ALK1, ENG, SMAD9, CAV1, KCNK3 3.Unknown Drug and toxin induced Associated with RA (mmhg) 13 PA (mmhg) 104/55/73 PAP (mmhg) 18 Oxymetry PA (O2%) 71.4 LV (O2) 96% CI (l/min/m2) 1,7 PVR (WU) 22 CONNECTIVE TISSUE DISORDER CHD HIV Portal Hypertension Schistosomiasis
 group mostly resembling a plexiform lesion : localisation adjacent to a bronchiolus (arrow); intimal fibrosis with")
29 PAH in limited cutaneous systemic sclerosis: a distinctive vasculopathy Eur Respir J 2009;34: Early-onset PAH is as frequent among patients with diffuse SSc as those with limited SSc a) Single lesion in the systemic sclerosis-associated pulmonary arterial hypertension (PAH) group mostly resembling a plexiform lesion : localisation adjacent to a bronchiolus (arrow); intimal fibrosis with recanalisation (black arrowheads)... PAH was almost equal (19% v 17%) in dsc and LSc EULAR Scl trials and EUSTAR group.

30 Is PAH really a late complication of systemic sclerosis? Hyperinflammation, dysregulated humoral autoimmunity, and platelet overactivation are common to both and in each case mediate endothelial dysfunction, fibrillar collagen deposition, and intimal thickening of pulmonary arterioles. Circulation. 2016;133: A pulmonary arteriole from a patient with systemic sclerosis-associated pulmonary artery hypertension showing significant medial hypertrophy Chest 2009 Nov;136(5):1211-9
, and idiopathic inflammatory myopathy")
31 CTD-associated ILD, with a focus on systemic sclerosis (SSc), rheumatoid arthritis (RA), and idiopathic inflammatory myopathy (IIM)
 EULAR Scl trials and")
32 In the Scleroderma Lung Study, there were no significant differences in the frequency of alveolitis on HRCT scan between lcssc and dcssc, suggesting that all patients with SSc are at risk for ILD More pulmonary fibrosis was seen in the dcssc group (53% v 30%) EULAR Scl trials and EUSTAR group

33

34 V/Q SCAN FOR SCREENING (INITIAL STEP) Sensitivity > 96% (CTPA: sensitivity 51%) less radiation exposure, no complications related to i.v. contrast, cost benefit, less likelihood for detection of incidental findings, less training J Nucl Med 2007; 48: J Am Coll Cardiol 2013; 62:D92-9

35

36 OUR PATIENT : GROUP 1, 2, 3
37 PATHWAY TO IMPROVING LONG-TERM OUTCOMES IN PAH SPECIFIC PAH DRUGS?


38 GROUP 2 PH GROUP 3 PH

39

40 EVIDENCED BASED TREATMENT ALGORITHM
41 2015 ESC GUIDELINES

42 EVIDENCED BASED TREATMENT ALGORITHM
43 PATHWAY TO IMPROVING LONG-TERM OUTCOMES IN PAH WHICH STRATEGY INITIAL COMBINATION THERAPY SEVERE HAEMODYNAMIC IMPAIRMENT SCLERODERMA DISEASE


44 6. Eur Respir J 2012; 40: Eur Respir J 2010; 35: Circulation 2010; 122: Eur Respir J 2012; 40: Chest 2011; 140: Chest 2012; 141: JACC 2013; 62:25
45 11/ / /2016 RA (mmhg) PA (mmhg) 104/55/73 87/19/58 84/16/53 PAP (mmhg) Oxymetry PA (O2%) LV (O2 %) CI (l/min) 1, PVR (WU)


46 11/2016: WHO II, 6MWT: 410m, NT-proBNP 280 pg/ml

47 2015 ESC GUIDELINES
48 2015 ESC/ERS GUIDELINES INITIAL COMBINATION THERAPY


49 PRIMARY ENDPOINT: TIME TO CLINICAL FAILURE N Engl J Med. 2015;373:
50 Baseline Characteristics Characteristic Combination Therapy (n=253) Pooled Monotherapy (n=247) Ambrisentan monotherapy (n=126) Tadalafil Monotherapy (n=121) Baseline Who Functional Class II 76 (30%) 79 (32%) 38 (30%) 41 (34%) III 177 (70%) 168 (68%) 88 (70%) 80 (66%) Baseline 6MWD (m) ± SD (87.9) (91.8) (92.3) (91.6) Hemodynamic variables RAP, mm Hg, mean ± SD 7.7 ± ± ± ± 4.8 PAP, mm Hg, mean ± SD 48.1 ± ± ± ± 12.6 PCWP, mm Hg, mean ± SD 8.4 ± ± ± ± 3.5 CI, L/min/m 2, mean ± SD 2.41 ± ± ± ± 0.77 PVR, dyne.sec/cm 5, mean ± SD ± ± ± ± Time on study medication to FAV, ± NA ± ± days, mean ± SD N. Galiè, et al. N Engl J Med 2015;373:834-44

51 AMBITION TRIAL PRIMARY ENDPOINT BY CLINICAL FAILURE EVENT N Engl J Med. 2015;373:

52 REVEAL REGISTRY HOSPITALISATION WORSENS LONG-TERM OUTCOMES 25.4% ± 3.2% remained hospitalization-free for 3 years Survival estimates at 3 years post-discharge were 56.8% ± 3.5% and 67.8% ± 3.6% (P =.037) for patients with PAH-related and PAH-unrelated hospitalization, respectively. Chest 2014 Nov;146(5):
53 NT-proBNP: change from baseline to week 24 and treatment differences Ratio of NT-proBNP (pg/ml) to BASELINE Treatment ratios to COMBO Week 24 Combo vs pooled mono p< Combo vs ambrisentan mono p= Combo vs tadalafil mono p< Vertical bars represent 95% CIs. Graph is a mixed models repeated measures (MMRM) analysis adjusted for baseline aetiology of PAH (IPAH/HPAH vs non-ipah), WHO FC (II vs III) and baseline, with no imputation for missing data. N. Galiè, et al. N Engl J Med 2015;373:834-44
54 NT-proBNP

55 AMBITION SELECTED BASELINE CHARACTERISTICS
56 Coghlan et al. Ann Rheum Dis 2015;74:Suppl % Risk Reduction
57
58 Event-Free (%) Combination therapy Pooled monotherapy 79% mortality risk reduction At EORT+7, 3 (1%) of combo patients had died compared with 13 (4%) of mono patients (HR 0.21; 95% CI ; p=0.0065) 1 It would be a signal for reduction in mortality considering that all patients were treatment naive at trial commencement. A pretty strong signal. Number at risk: Time (weeks) Combination Pooled Mono Hoeper et al. Lancet Respir Med 2016;4:
59 People are dying οn monotherapies before physicians have the opportunity to step-up treatments? Patients on monotherapy who have treatment failure can be rescued by addition of further drugs? A radically different therapeutic approach (upfront combination therapy) might improve the only meaningful endpoint (death) in this disease AMBITION used ambrisentan and tadalafil. It is not known if these findings can be extrapolated to other combinations 1.Hoeper et al. Lancet Respir Med 2016;4:
60 Mortality at 7 days after the end of assigned treatment was reduced by active therapy compared with placebo, but the difference was not significant (HR 0.64, p=0.20) Similar results were obtained with the end-of-study analysis (HR 0.77, p=0.25) T Pulido, et al. N Engl J Med 2013;369:
61 Cumulative RR estimate of death in active treatment groups when compared with control groups (RR [95% CI]). In various meta-analyses of subsequent trials (12 16 weeks in duration), survival was not shown convincingly to be improved with monotherapy or combined therapy Eur Heart J 2009;30:
 in this disease.")
62 2015 ESC/ERS GUIDELINES INITIAL COMBINATION THERAPY It strongly raises the possibility that a radically different therapeutic approach might improve the only meaningful endpoint (ie, death) in this disease. IN TREATMENT NAÏVE PATIENTS, THE MOST APPROPRIATE APPROACH.
63 This is a fundamental approach and probably a shift from a goaloriented treatment strategy to an outcome-oriented treatment strategy TREATMENT GOALS IMPROVE LONG TERM OUTCOME

64

65 ADVERSE EVENTS N Engl J Med. 2015;373:
66 Specific PAH oral drugs PRICES Euro/month Revatio 450,19 Adcirca 544,30 Riociguat 2600 Klimurtan 1350,60 Tracleer 2043,21 Volibris 2115,94 Opsumit 2762,18 BOSENTAN RIOCIGUAT AMBRISENTAN TADALAFIL SILDENAFIL Greece, November 2016 Pharmaco-Economics (2016) 34:
67 We cannot cure PAH in most cases today, but at least we can control the disease so it is no longer progressive Initial Combination Therapy
68 THANK YOU

69

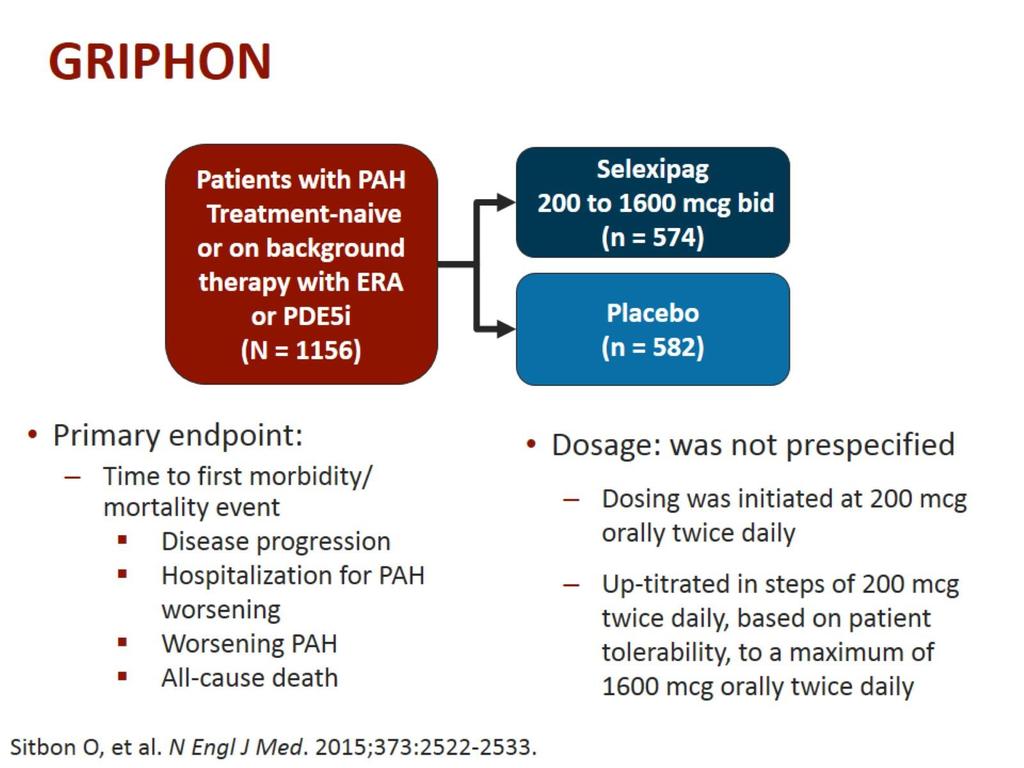
70 SERAPHIN TRIAL & GRIPHON TRIAL

71

72
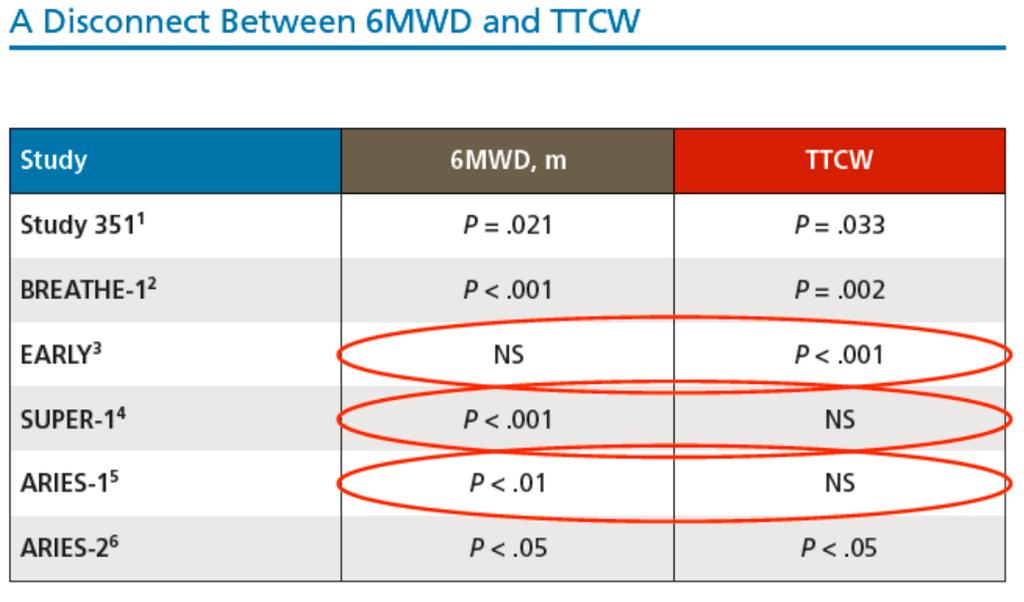
73 Selexipag Prolongs the Time to Morbidity/Mortality Events in Key Subgroup Populations: Results from GRIPHON, a Randomized Controlled Study in PAH The patients with SSc-PAH had a 54.8% risk reduction in the primary end point, a treatment effect that exceeded the 41% risk reduction in the entire study population Could it be that the 6-minute-walk test has limitations as a primary end point in patients with SSc-PAH? Could it be that PAH-specific therapies really do benefit patients with SSc-PAH if studied in adequate numbers with hard and clinically relevant end points?

74

75 SLE- or MCTD-associated PAH Conventional therapy WHO II OR III with C.I.>3.1 l/min/m2 Immunosuppresive therapy alone WHO III WITH C.I.<3.1 or WHO IV Pulmonary vasodilators +/- Immunosuppresive therapy? Evaluation 4-6months after response No response Start maintenance regimen Azathioprine, mycophenolate, mofetil Stop immunosuppressive Pulmonary vasodilators Arthritis & Rheumatism 2008; 58: Patients who could benefit from this immunosuppressive therapy could be those who have less severe disease at baseline
76 Six randomized controlled trials including 729 patients met inclusion criteria Compared to MT, CT resulted in a modest increase in 6-minute walk distance at the end of follow-up (weighted mean difference 25.2 m, 95% confidence interval [CI] 13.3 to 37.2). CT did not decrease mortality (risk ratio [RR] 0.42, 95% CI 0.08 to 2.25), admissions for worsening PAH (RR 0.72, 95% CI 0.36 to 1.44), or escalation of therapy (RR 0.36, 95% CI 0.09 to 1.39) and did not improve New York Heart Association functional class (RR 1.32, 95% CI 0.38 to 4.5) compared to MT Combined therapy did not decrease the composite endpoint of mortality, hospital admission for worsening PAH, lung transplantation, or escalation of therapy. Am J Cardiol Oct 15;108(8):
77 Improvement in functional status and a reduction in risk of clinical worsening with combination therapy, but the reduction in mortality was non-significant Lancet Respir Med 2016 Apr;4(4):

78

79
80
81
82

83

84
85
86 Patient randomised to treatment Pre-specified analysis: all deaths to end of study Patient experiences 1 st event No event Patient remains on randomised treatment Death included in analysis Patient switches to BCT or other Tx Death at any point included End of Study Patient randomised to treatment Post-hoc analysis: All deaths up to EOR (+7 days) Patient experiences 1 st event No event Patient remains on randomised treatment Death included in analysis Patient switches to BCT or other treatment Death up to 7 days after switch included in analysis including those who discontinued medication but remained in the study End of Study BCT = blinded combination therapy 1.Hoeper et al. Lancet Respir Med 2016;4:
87 Lancet Respir Med Nov;4(11): Initial combination therapy with ambrisentan and tadalafil and mortality in patients with pulmonaryarterial hypertension: a secondary analysis of the results from the randomised, controlled AMBITIONstudy. We analysed survival data from the modified intention-totreat population of the Ambrisentan and Tadalafil in Patients with Pulmonary Arterial Hypertension (AMBITION) trial. The study population consisted of 605 patients with pulmonary arterial hypertension who were randomly assigned and received combination therapy (n=302) or monotherapy (n=303; 152 patients assigned to ambrisentan monotherapy and 151 patients to tadalafil monotherapy). At the end of the study, 29 (10%) of 302 patients in the combination therapy group had died compared with 41 (14%) of 303 patients in the monotherapy group (hazard ratio 0 67, 95% CI ; stratified log-rank p=0 10). At 7 days after the end of randomised treatment, fewer patients had died in the combination therapy group (3 [1%] of 302 patients) compared with the monotherapy group (13 [4%] of 303 patients; hazard ratio 0 21, 95% CI ).
88 The following baseline factors were found to be predictive of better survival 1 6MWD 6MWD 357m < or median (median) NT-proBNP NT-proBNP < 870 ng/l < or median (median) Haemodynamics PVR, CI < 2.37 mpap, L/min/m CI, RAP 2 < or (median) Population PAS or PAS Ex-PAS 1.Hoeper et al. Lancet Respir Med 2016;4:
89
90 However, it is unclear whether patients with mild PAH (mean pulmonary artery pressure, mm Hg), especially functional class II, which is more typical of those identified via aggressive screening programs, should also be treated with up-front combination therapy. Further trials are needed in this patient population to advocate up-front combination therapies. Until then, the rheumatology, cardiology, and pulmonary communities should work together to be proactive in screening, early detection, and treatment of PAH in patients with CTDs, especially The AMBITION and GRIPHON subgroup analyses demonstrate a treatment benefit in patients with CTD-PAH Whether up-front combination therapy is superior to goal-directed sequential therapy in all patient populations remains a topic of debate. However, given the poor prognosis of CTD-PAH, up-front combination therapy is a reasonable approach, particularly in symptomatic patients with similar clinical characteristics to those in the study of Hassoun and colleagues (New York Heart Association functional class II [35%] and III [65%], with a mean pulmonary artery pressure of 42 mm Hg).
91

92
93
94
95

96

97
98 We defined a classification listing of Pre-PAH based on the presence of any one of these three criteria on study entry: 1. Diffusing capacity for carbon monoxide (DLCO) < 55% predicted without severe ILD (as defined by forced vital capacity (FVC) < 65% predicted and/or a thoracic high resolution computed tomography (HRCT) scan that showed moderate to severe ILD according to the local radiologist)(7) or 2. FVC %predicted / DLCO %predicted ratio 1.6 or 3. Estimated right ventricular systolic pressure (RVSP) > 35 mmhg on Doppler echocardiography. At baseline, 16 subjects (10%) of the Pre-PAH group had symptoms, an elevated RVSP (mean +/ SD 38 +/ 10, range 19 62), or PFT abnormalities that led individual investigators to do a RHC that revealed a normal mpap. Four of these had an estimated RVSP on echocardiogram > 40mm Hg, the mean +/ SD DLCO% predicted in this group was markedly reduced (38% +/ 16) and the mean PCWP was 8 mm Hg. Ten RHC-negative subjects had undergone a thoracic HRCT that revealed no (n=5), mild (n=3), moderate (n=1), or severe (n=1) fibrosis.
99 We found that one-third (22/71) of subjects thought to be at high-risk for PAH according to our three criteria were found to have PVH or PH-ILD. Thus, it is imperative that clinicians treating patients with SSc realize that a right heart catheterization is necessary to accurately establish the diagnosis of PAH Only 14% of those with PH had a DLCO that was > 55% predicted. Interestingly, the mean DLCO was lowest in Groups 2 and 3 showing that a low DLCO itself does not necessarily predict PAH compared to PVH and PH-ILD. However, the mean FVC% predicted was significantly lower in the non-pah groups, and importantly the mean FVC%/DLCO% ratio was highest in those with PAH. Eighty-two percent of those with PAH, 70% with PVH and only 25% with PH-ILD had a FVC/DLCO ratio >1.6. Thus, the high ratio may be a useful parameter to use as part of the determination of whether an SSc-PH patient has PAH compared to other causes of PH.
100
101 DECREASED NO production in PAH and SSc DECREASED enos expression in IPAH lung DECREASED enos expression in SSc dermal microvasculature ROLE OF ENDOTHELIN ET-1 increased in SSc serum Vasc Med 2000; 5: N Engl J Med 1995; 333:


102 EPOPROSTENOL FOR DIGITAL ISCHEMIA

103 Prevalence abnormal physiology % Restrictive ventilator pattern 25-41% Isolated reduction in DLCO 18-47% early sign of SSc ILD also suggestive of PAH Exercise desaturation: earliest abnormality

104 Eur Heart J 2006; 27:


105 Arthritis Rheum 2003; 43: Courtesy of James Seibdd


106 DD PAH GROUP 3


107
108

109

110

111



112 CPFE + + mpap > 25 mmhg COPD + FEV1 < 60% + mpap > 25mmHg IPF + FVC < 70% + mpap > 25mmHg PH GROUP 3 RHC is indicated :Clinical worsening and progressive exercise limitation disproportionate to ventilator impairment (alternative diagnosis-pah,cteph,lv dysfunction)

113 PULMONARY HYPERTENSION Haemodynamic & Pathophysiologic Condition mpap 25 mmhg ESC GUIDELINES 2015


114

115 ESC Guidelines 2015
116 *Worst case imputation (0) was used for missing data following death or adjudicated hospitalisation; otherwise, LOCF imputation was used. Baseline data have not been used for imputation. p value from CMH tests stratified by baseline aetiology of PAH (IPAH/HPAH vs non-ipah) and WHO FC (II vs III). WHO FC change at week 24 Combin ation thera py (n=25 3) Pooled monotherap y (n=247) N. Galiè, et al. N Engl J Med 2015;373: Ambrisenta n monotherap y (n=126) Tadalafil monotherap y (n=121) Baseline WHO FC, observed, n II 76 (30%) 79 (32%) 38 (30%) 41 (34%) III 177 (70%) 168 (68%) 88 (70%) 80 (66%) Week 24 WHO FC, observed, n Improved 89 (38%) 80 (36%) 41 (38%) 39 (35%) No change 138 (59%) 133 ( 60%) 63 (58%) 70 (63%) It is possible that the FC assessment is not sensitive enough to pick up differences in improvements in FC between two active treatment groups Deteriorated 6 (3%) 7 (3%) 5 (5%) 2 (2%) Week 24 WHO FC, imputed*, n Improved 94 (37%) 81 (33%) 42 (34%) 39 (33%) No change 146 (58%) 147 (60%) 73 (59%) 74 (62%) Deteriorated 12 (5%) 16 (7%) 9 (7%) 7 (6%) p value

117 SECONDARY ENDPOINTS: SELECTED RESULTS AT WEEK 24 N Engl J Med. 2015;373:
118 Only adverse events on randomised treatment, with onset between first dose of study drug and last dose+30 days are shown AE Term n, (%) COMB (n=253) AMB Mono (n=126) TAD Mono (n=121) Any AE 247 (98%) 120 (95%) 114 (94%) Oedema peripheral 115 (45%) 41 (33%) 34 (28%) Headache 107 (42%) 41 (33%) 42 (35%) Nasal congestion 54 (21%) 19 (15%) 15 (12%) Diarrhoea 50 (20%) 29 (23%) 23 (19%) Dizziness 50 (20%) 24 (19%) 14 (12%) Dyspnoea 44 (17%) 22 (17%) 20 (17%) Nausea 43 (17%) 18 (14%) 20 (17%) Cough 40 (16%) 14 (11%) 21 (17%) Flushing 38 (15%) 18 (14%) 11 (9%) Anemia 37 (15%) 8 (6%) 14 (12%) Nasopharyngitis 37 (15%) 26 (21%) 18 (15%) Pain in extremity 37 (15%) 14 (11%) 18 (15%) Syncope 13 (5%) 7 (6%) 10 (8%)
 0 1 (<1%) Pulmonary Hypertension 1 (<1%) 2 (2%) 1 (<1%) Anaemia 1 (<1%) 2 (2%) 0 Myalgia 0 0 3 (2%) Cardiac Failure 0 2 (2%) 0 Only adverse events on randomised treatment, with onset")
119 AE leading to discontinuation n, (%) Combinatio n AMB Mono TAD Mono (n=253) (n=126) (n=121) Any event 31 (12%) 14 (11%) 14 (12%) Dyspnoea 5 (2%) 0 1 (<1%) Oedema, peripheral 4 (2%) 3 (2%) 1 (<1%) Headache 4 (2%) 0 1 (<1%) Pulmonary Hypertension 1 (<1%) 2 (2%) 1 (<1%) Anaemia 1 (<1%) 2 (2%) 0 Myalgia (2%) Cardiac Failure 0 2 (2%) 0 Only adverse events on randomised treatment, with onset between first dose of study drug and last dose+30 days are shown
120 Liver Events AST/ALT >3xULN Subjects with ALT/AST >3xULN Combination Therapy N = 253 On Randomized Treatment Ambrisentan Monotherapy N = 126 Tadalafil Monotherapy N = (2%) 0 2 (2%) Data on file
121 Group EoT+7 Combination therapy 3/302 (<1) Events Patients with events/ total patients (%) Hazard Ratio (95% CI) Pooled monotherapy 13/303 (4) 0.21 (0.06, 0.73) AMB monotherapy 3/152 (2) 0.46 (0.09, 2.26) TAD monotherapy 10/151 (7) 0.13 (0.04, 0.49) Final EoS Combination therapy 29/302 (10) Pooled monotherapy 41/303 (14) 0.67 (0.42, 1.08) AMB monotherapy 19/152 (13) 0.74 (0.41, 1.32) TAD monotherapy 22/151 (15) 0.60 (0.35, 1.05) Favours combination Favours monotherapy Hoeper et al. Lancet Respir Med 2016;4:

122 AMBITION: TITRATING THE DOSES OF COMBINATION THERAPY days 609 days
123 Event-Free (%) "long-term survival might have been affected by treatment modifications during the course of the study as patients who had an investigator-reported clinical failure event were allowed to receive additional treatments. Combination therapy Pooled monotherapy 33% mortality risk reduction At EOS, 29/302 (10%) of combo patients had died compared with 41/303 (14%) of mono patients (HR 0.67; 95% CI ; p=0.10) 1 Number at risk: Time (weeks) Combination Pooled Mono Hoeper et al. Lancet Respir Med 2016;4:
Πνευμονική Υπέρταση: Μια ΚΡΙΤΙΚΗ ματιά στις κλινικές μελέτες - AMBITION. Αναστασία Ανθη
 Πανελλήνια Σεμινάρια Ομάδων Εργασίας 2017 k Πνευμονική Υπέρταση: Μια ΚΡΙΤΙΚΗ ματιά στις κλινικές μελέτες - AMBITION Αναστασία Ανθη Β Κλιν. Εντατικής Θεραπείας & Διακλινικό Ιατρείο Πνευμ. Υπέρτασης Π.Γ.Ν.
Πανελλήνια Σεμινάρια Ομάδων Εργασίας 2017 k Πνευμονική Υπέρταση: Μια ΚΡΙΤΙΚΗ ματιά στις κλινικές μελέτες - AMBITION Αναστασία Ανθη Β Κλιν. Εντατικής Θεραπείας & Διακλινικό Ιατρείο Πνευμ. Υπέρτασης Π.Γ.Ν.
SATELLITE SYMPOSIUM OF MSD. sgc Stimulation for the treatment of PH. Real life management of PAH: case presentation
 SATELLITE SYMPOSIUM OF MSD sgc Stimulation for the treatment of PH Real life management of PAH: case presentation Eftychia Demerouti MD, MSc, PhD Cardiologist Onassis Cardiac Surgery Center Conflict of
SATELLITE SYMPOSIUM OF MSD sgc Stimulation for the treatment of PH Real life management of PAH: case presentation Eftychia Demerouti MD, MSc, PhD Cardiologist Onassis Cardiac Surgery Center Conflict of
The Case of Marco Nazzareno Galiè, M.D.
 The Case of Marco Nazzareno Galiè, M.D. DIMES Disclosures Consulting fees and research support from Actelion Pharmaceuticals Ltd, Bayer HealthCare, Eli Lilly and Co, GlaxoSmithKline and Pfizer Ltd Clinical
The Case of Marco Nazzareno Galiè, M.D. DIMES Disclosures Consulting fees and research support from Actelion Pharmaceuticals Ltd, Bayer HealthCare, Eli Lilly and Co, GlaxoSmithKline and Pfizer Ltd Clinical
Pulmonary arterial hypertension. Pulmonary arterial hypertension: newer therapies. Definition of PH 12/18/16. WHO Group classification of PH
 Pulmonary arterial hypertension Pulmonary arterial hypertension: newer therapies Ramona L. Doyle, MD Clinical Professor of Medicine, UCSF Attending Physician UCSF PH Clinic Definition and classification
Pulmonary arterial hypertension Pulmonary arterial hypertension: newer therapies Ramona L. Doyle, MD Clinical Professor of Medicine, UCSF Attending Physician UCSF PH Clinic Definition and classification
Therapeutic approaches in P(A)H and the new ESC Guidelines
H and the new ESC Guidelines") Therapeutic approaches in P(A)H and the new ESC Guidelines Jean-Luc Vachiéry, FESC Head Pulmonary Vascular Diseases and Heart Failure Clinic Hôpital Universitaire Erasme Université Libre de Bruxelles Belgium
Therapeutic approaches in P(A)H and the new ESC Guidelines Jean-Luc Vachiéry, FESC Head Pulmonary Vascular Diseases and Heart Failure Clinic Hôpital Universitaire Erasme Université Libre de Bruxelles Belgium
Case Presentation : Pulmonary Hypertension: Diagnosis and Imaging
 Case Presentation 9.40-11.20: Pulmonary Hypertension: Diagnosis and Imaging Eftychia Demerouti MD, MSc, PhD Cardiologist Onassis Cardiac Surgery Center Conflicts of interest Consulting fees and fees for
Case Presentation 9.40-11.20: Pulmonary Hypertension: Diagnosis and Imaging Eftychia Demerouti MD, MSc, PhD Cardiologist Onassis Cardiac Surgery Center Conflicts of interest Consulting fees and fees for
Effective Strategies and Clinical Updates in Pulmonary Arterial Hypertension
 Effective Strategies and Clinical Updates in Pulmonary Arterial Hypertension Hap Farber Director, Pulmonary Hypertension Center Boston University School of Medicine Disclosures 1) Honoria: Actelion, Gilead,
Effective Strategies and Clinical Updates in Pulmonary Arterial Hypertension Hap Farber Director, Pulmonary Hypertension Center Boston University School of Medicine Disclosures 1) Honoria: Actelion, Gilead,
THERAPEUTICS IN PULMONARY ARTERIAL HYPERTENSION Evidences & Guidelines
 THERAPEUTICS IN PULMONARY ARTERIAL HYPERTENSION Evidences & Guidelines Vu Nang Phuc, MD Dinh Duc Huy, MD Pham Nguyen Vinh, MD, PhD, FACC Tam Duc Cardiology Hospital Faculty Disclosure No conflict of interest
THERAPEUTICS IN PULMONARY ARTERIAL HYPERTENSION Evidences & Guidelines Vu Nang Phuc, MD Dinh Duc Huy, MD Pham Nguyen Vinh, MD, PhD, FACC Tam Duc Cardiology Hospital Faculty Disclosure No conflict of interest
22nd Annual Heart Failure 2018 an Update on Therapy. Pulmonary Arterial Hypertension: Contemporary Approach to Treatment
 22nd Annual Heart Failure 2018 an Update on Therapy Pulmonary Arterial Hypertension: Contemporary Approach to Treatment Ronald J. Oudiz, MD, FACP, FACC, FCCP Professor of Medicine The David Geffen School
22nd Annual Heart Failure 2018 an Update on Therapy Pulmonary Arterial Hypertension: Contemporary Approach to Treatment Ronald J. Oudiz, MD, FACP, FACC, FCCP Professor of Medicine The David Geffen School
Approach to Pulmonary Hypertension in the Hospital
 Approach to Pulmonary Hypertension in the Hospital Todd M Bull MD Professor of Medicine Director Pulmonary Vascular Disease Center Director Center for Lungs and Breathing Division of Pulmonary Sciences
Approach to Pulmonary Hypertension in the Hospital Todd M Bull MD Professor of Medicine Director Pulmonary Vascular Disease Center Director Center for Lungs and Breathing Division of Pulmonary Sciences
The Case of Lucia Nazzareno Galiè, M.D.
 The Case of Lucia Nazzareno Galiè, M.D. DIMES Disclosures Consulting fees and research support from Actelion Pharmaceuticals Ltd, Bayer HealthCare, Eli Lilly and Co, GlaxoSmithKline and Pfizer Ltd Clinical
The Case of Lucia Nazzareno Galiè, M.D. DIMES Disclosures Consulting fees and research support from Actelion Pharmaceuticals Ltd, Bayer HealthCare, Eli Lilly and Co, GlaxoSmithKline and Pfizer Ltd Clinical
CONUNDRUMS IN PULMONARY ARTERIAL HYPERTENSION
 CONUNDRUMS IN PULMONARY ARTERIAL HYPERTENSION MOHAMMED RAFIQUE ESSOP MILPARK HOSPITAL and UNIVERSITY OF THE WITWATERSRAND POINTS FOR DISCUSSION What is the pathogenetic mechanism of PAH? Importance of
CONUNDRUMS IN PULMONARY ARTERIAL HYPERTENSION MOHAMMED RAFIQUE ESSOP MILPARK HOSPITAL and UNIVERSITY OF THE WITWATERSRAND POINTS FOR DISCUSSION What is the pathogenetic mechanism of PAH? Importance of
Real-world experience with riociguat in CTEPH
 Real-world experience with riociguat in CTEPH Matthias Held Center of Pulmonary Hypertension and Pulmonary Vascular Disease, Medical Mission Hospital, Würzburg, Germany Tuesday, 29 September ERS International
Real-world experience with riociguat in CTEPH Matthias Held Center of Pulmonary Hypertension and Pulmonary Vascular Disease, Medical Mission Hospital, Würzburg, Germany Tuesday, 29 September ERS International
Progress in PAH. Gerald Simonneau
 Progress in PAH Gerald Simonneau National Reference center for Pulmonary Hypertension Bicetre University Hospital, INSERM U 999 Paris-Sud University Le Kremlin Bicêtre France Clinical Classification of
Progress in PAH Gerald Simonneau National Reference center for Pulmonary Hypertension Bicetre University Hospital, INSERM U 999 Paris-Sud University Le Kremlin Bicêtre France Clinical Classification of
Pulmonary Hypertension. Pulmonary Arterial Hypertension Diagnosis, Impact and Outcomes
 Pulmonary Hypertension Pulmonary Arterial Hypertension Diagnosis, Impact and Outcomes Pulmonary Arterial Hypertension Disease of small pulmonary arteries Characteristic changes Medial hypertrophy Intimal
Pulmonary Hypertension Pulmonary Arterial Hypertension Diagnosis, Impact and Outcomes Pulmonary Arterial Hypertension Disease of small pulmonary arteries Characteristic changes Medial hypertrophy Intimal
Update in Pulmonary Arterial Hypertension
 Update in Pulmonary Arterial Hypertension Michael J Sanley, MD April 12, 2018 Disclosures I have nothing to disclose 2 1 Case Presentation 67 yo male with atrial fibrillation, CLL on IVIG, presents with
Update in Pulmonary Arterial Hypertension Michael J Sanley, MD April 12, 2018 Disclosures I have nothing to disclose 2 1 Case Presentation 67 yo male with atrial fibrillation, CLL on IVIG, presents with
Pulmonary Hypertension in 2012
 Pulmonary Hypertension in 2012 Evan Brittain, MD December 7, 2012 Kingston, Jamaica VanderbiltHeart.com Disclosures None VanderbiltHeart.com Outline Definition and Classification of PH Hemodynamics of
Pulmonary Hypertension in 2012 Evan Brittain, MD December 7, 2012 Kingston, Jamaica VanderbiltHeart.com Disclosures None VanderbiltHeart.com Outline Definition and Classification of PH Hemodynamics of
MACITENTAN DEVELOPMENT IN CHILDREN WITH PULMONARY HYPERTENSION (PAH)
") MACITENTAN DEVELOPMENT IN CHILDREN WITH PULMONARY HYPERTENSION (PAH) ORPHAN DRUG AND RARE DISEASE 11 MAY 2017 Catherine Lesage, MD, Pediatrics Program Head, Actelion Copyright AGENDA Pulmonary Arterial
MACITENTAN DEVELOPMENT IN CHILDREN WITH PULMONARY HYPERTENSION (PAH) ORPHAN DRUG AND RARE DISEASE 11 MAY 2017 Catherine Lesage, MD, Pediatrics Program Head, Actelion Copyright AGENDA Pulmonary Arterial
Oral Therapies for Pulmonary Arterial Hypertension
 Oral Therapies for Pulmonary Arterial Hypertension Leslie Wooten, PharmD PGY2 Internal Medicine Pharmacy Resident University of Cincinnati Medical Center April 30 th, 2018 Objectives Pharmacist Objectives
Oral Therapies for Pulmonary Arterial Hypertension Leslie Wooten, PharmD PGY2 Internal Medicine Pharmacy Resident University of Cincinnati Medical Center April 30 th, 2018 Objectives Pharmacist Objectives
different phenotypes
 Pulmonary hypertension in scleroderma: different phenotypes UMR 995 Pr David LAUNAY, MD, PhD launayd@gmail.com Service de Médecine Interne. Unité d'immunologie Clinique CNRMR Maladies Systémiques et Autoimmunes
Pulmonary hypertension in scleroderma: different phenotypes UMR 995 Pr David LAUNAY, MD, PhD launayd@gmail.com Service de Médecine Interne. Unité d'immunologie Clinique CNRMR Maladies Systémiques et Autoimmunes
Comparison between adult and pediatric populations with I/HPAH and PAH-CHD in the Bologna ARCA registry
 nazzareno.galie@unibo.it Comparison between adult and pediatric populations with I/HPAH and PAH-CHD in the Bologna ARCA registry Nazzareno Galiè, MD, FESC, FRCP (Hon), DIMES 2 Comprehensive clinical classification
nazzareno.galie@unibo.it Comparison between adult and pediatric populations with I/HPAH and PAH-CHD in the Bologna ARCA registry Nazzareno Galiè, MD, FESC, FRCP (Hon), DIMES 2 Comprehensive clinical classification
Pulmonary Hypertension: When to Initiate Advanced Therapy. Jonathan D. Rich, MD Associate Professor of Medicine Northwestern University
 Pulmonary Hypertension: When to Initiate Advanced Therapy Jonathan D. Rich, MD Associate Professor of Medicine Northwestern University Disclosures Medtronic, Abbott: Consultant Hemodynamic Definition of
Pulmonary Hypertension: When to Initiate Advanced Therapy Jonathan D. Rich, MD Associate Professor of Medicine Northwestern University Disclosures Medtronic, Abbott: Consultant Hemodynamic Definition of
Pulmonary hypertension in sarcoidosis
 Pulmonary hypertension in sarcoidosis Olivier SITBON Centre de Référence de l Hypertension Pulmonaire Sévère Hôpital Universitaire de Bicêtre INSERM U999 Université Paris-Sud Le Kremlin-Bicêtre France
Pulmonary hypertension in sarcoidosis Olivier SITBON Centre de Référence de l Hypertension Pulmonaire Sévère Hôpital Universitaire de Bicêtre INSERM U999 Université Paris-Sud Le Kremlin-Bicêtre France
Chronic Thromboembolic Pulmonary Hypertention CTEPH
 Chronic Thromboembolic Pulmonary Hypertention CTEPH Medical Management Otto Schoch, Prof. Dr. Klinik für Pneumologie und Schlafmedizin Kantonsspital St.Gallen CTEPH: Medical Management Diagnostic aspects
Chronic Thromboembolic Pulmonary Hypertention CTEPH Medical Management Otto Schoch, Prof. Dr. Klinik für Pneumologie und Schlafmedizin Kantonsspital St.Gallen CTEPH: Medical Management Diagnostic aspects
PULMONARY HYPERTENSION
 PULMONARY HYPERTENSION REVIEW & UPDATE Olga M. Fortenko, M.D. Pulmonary & Critical Care Medicine Pulmonary Vascular Diseases Sequoia Hospital 650-216-9000 Olga.Fortenko@dignityhealth.org Disclosures None
PULMONARY HYPERTENSION REVIEW & UPDATE Olga M. Fortenko, M.D. Pulmonary & Critical Care Medicine Pulmonary Vascular Diseases Sequoia Hospital 650-216-9000 Olga.Fortenko@dignityhealth.org Disclosures None
Real life management of CTEPH: patient case
 2 nd International Congress on cardiovascular imaging in clinical practice k Real life management of CTEPH: patient case Anastasia Anthi Pulmonary Hypertension Clinic, Attikon University Hospital, Athens
2 nd International Congress on cardiovascular imaging in clinical practice k Real life management of CTEPH: patient case Anastasia Anthi Pulmonary Hypertension Clinic, Attikon University Hospital, Athens
Pulmonary Arterial Hypertension - Overview
 Pulmonary Arterial Hypertension - Overview J. Shaun Smith, MD Co-Director, Pulmonary Vascular Disease Program Assistant Professor of Medicine Division of Pulmonary, Critical Care and Sleep Medicine The
Pulmonary Arterial Hypertension - Overview J. Shaun Smith, MD Co-Director, Pulmonary Vascular Disease Program Assistant Professor of Medicine Division of Pulmonary, Critical Care and Sleep Medicine The
Pulmonary Arterial Hypertension - Overview
 Pulmonary Arterial Hypertension - Overview J. Shaun Smith, MD Co-Director, Pulmonary Vascular Disease Program Assistant Professor of Medicine Division of Pulmonary, Critical Care and Sleep Medicine The
Pulmonary Arterial Hypertension - Overview J. Shaun Smith, MD Co-Director, Pulmonary Vascular Disease Program Assistant Professor of Medicine Division of Pulmonary, Critical Care and Sleep Medicine The
ΔΙΑΓΝΩΣΗ ΚΑΙ ΘΕΡΑΠΕΙΑ ΤΗΣ ΧΡΟΝΙΑΣ ΘΡΟΜΒΟΕΜΒΟΛΙΚΗΣ ΥΠΕΡΤΑΣΗΣ (CTEPH)
") Aristotle University of Thessaloniki Cardiology Clinic, AHEPA Hospital ΔΙΑΓΝΩΣΗ ΚΑΙ ΘΕΡΑΠΕΙΑ ΤΗΣ ΧΡΟΝΙΑΣ ΘΡΟΜΒΟΕΜΒΟΛΙΚΗΣ ΥΠΕΡΤΑΣΗΣ (CTEPH) Charalampos I. Karvounis, MD Professor of Cardiology Aristotle
Aristotle University of Thessaloniki Cardiology Clinic, AHEPA Hospital ΔΙΑΓΝΩΣΗ ΚΑΙ ΘΕΡΑΠΕΙΑ ΤΗΣ ΧΡΟΝΙΑΣ ΘΡΟΜΒΟΕΜΒΟΛΙΚΗΣ ΥΠΕΡΤΑΣΗΣ (CTEPH) Charalampos I. Karvounis, MD Professor of Cardiology Aristotle
Pulmonary Hypertension: Clinical Features & Recent Advances
 Pulmonary Hypertension: Clinical Features & Recent Advances Lisa J. Rose-Jones, MD Assistant Professor of Medicine, Division of Cardiology Advanced Heart Failure/Cardiac Transplantation & Pulmonary Hypertension
Pulmonary Hypertension: Clinical Features & Recent Advances Lisa J. Rose-Jones, MD Assistant Professor of Medicine, Division of Cardiology Advanced Heart Failure/Cardiac Transplantation & Pulmonary Hypertension
Pulmonary Arterial Hypertension: Biomarkers and Treatment
 Pulmonary Arterial Hypertension: Biomarkers and Treatment Demos Papamatheakis, MD Assistant Clinical Professor Division of Pulmonary, Critical Care and Sleep Medicine UC San Diego Health Definition EHJ
Pulmonary Arterial Hypertension: Biomarkers and Treatment Demos Papamatheakis, MD Assistant Clinical Professor Division of Pulmonary, Critical Care and Sleep Medicine UC San Diego Health Definition EHJ
The COPD-PH Consult. When to Consider Pulmonary Vascular Disease. Diagnostic Algorithm for Pulmonary Hypertension
 The COPD-PH Consult 52-year-old white male with COPD, HTN, presents with progressive DOE Current Meds: LABA/LAMA 5 years ACEI year 2 exacerbations in last year 2 LPM oxygen 6 mo An echo is ordered Function
The COPD-PH Consult 52-year-old white male with COPD, HTN, presents with progressive DOE Current Meds: LABA/LAMA 5 years ACEI year 2 exacerbations in last year 2 LPM oxygen 6 mo An echo is ordered Function
Instructions: This form is completed and entered for all participants. Database will skip over sections that do not apply.
 Revision of 08/30/2017 Form #102 Page 1 of 6 PVDOMICS STUDY PVD Assessment - Form #102 Instructions: This form is completed and entered for all participants. Database will skip over sections that do not
Revision of 08/30/2017 Form #102 Page 1 of 6 PVDOMICS STUDY PVD Assessment - Form #102 Instructions: This form is completed and entered for all participants. Database will skip over sections that do not
ACTIVITY DESCRIPTION Target Audience Learning Objectives
 ACTIVITY DESCRIPTION Target Audience This continuing medical education activity is planned to meet the needs of primary care physicians who can contribute to early detection of disease and who are responsible
ACTIVITY DESCRIPTION Target Audience This continuing medical education activity is planned to meet the needs of primary care physicians who can contribute to early detection of disease and who are responsible
Navigating the identification, diagnosis and management of pulmonary hypertension using the updated ESC/ERS guidelines
 Navigating the identification, diagnosis and management of pulmonary hypertension using the updated ESC/ERS guidelines Host: Marc Humbert Speaker: Simon Gibbs Marc HUMBERT, MD, PhD Professor of Respiratory
Navigating the identification, diagnosis and management of pulmonary hypertension using the updated ESC/ERS guidelines Host: Marc Humbert Speaker: Simon Gibbs Marc HUMBERT, MD, PhD Professor of Respiratory
Pulmonary Hypertension in Chronic Obstructive Pulmonary Disease
 Pulmonary Hypertension in Chronic Obstructive Pulmonary Disease Deedre Boekweg RN, BSN, CCRP Intermountain Medical Center Murray, UT Kerri Akaya Smith, MD University of Pennsylvania Philadelphia, PA PHPN
Pulmonary Hypertension in Chronic Obstructive Pulmonary Disease Deedre Boekweg RN, BSN, CCRP Intermountain Medical Center Murray, UT Kerri Akaya Smith, MD University of Pennsylvania Philadelphia, PA PHPN
Anjali Vaidya, MD, FACC, FASE, FACP Associate Director, Pulmonary Hypertension, Right Heart Failure, Pulmonary Thromboendarterectomy Program Advanced
 Anjali Vaidya, MD, FACC, FASE, FACP Associate Director, Pulmonary Hypertension, Right Heart Failure, Pulmonary Thromboendarterectomy Program Advanced Heart Failure & Cardiac Transplant Temple University
Anjali Vaidya, MD, FACC, FASE, FACP Associate Director, Pulmonary Hypertension, Right Heart Failure, Pulmonary Thromboendarterectomy Program Advanced Heart Failure & Cardiac Transplant Temple University
Connective tissue disease related Pulmonary arterial hypertension
 Connective tissue disease related Pulmonary arterial hypertension DM Seminar: Dr.Vamsi Krishna PAH in connective tissue diseases CTD accounts for 30% of PAH according to US PAH registry. Incidence is on
Connective tissue disease related Pulmonary arterial hypertension DM Seminar: Dr.Vamsi Krishna PAH in connective tissue diseases CTD accounts for 30% of PAH according to US PAH registry. Incidence is on
9/15/11. Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September Scleroderma. Hard skin
 Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September 2011 Scleroderma Hard skin 1 No diagnostic test for scleroderma Pathogenesis is unknown prominent features of disease reflect
Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September 2011 Scleroderma Hard skin 1 No diagnostic test for scleroderma Pathogenesis is unknown prominent features of disease reflect
Risk populations moving to screening programs
 Risk populations moving to screening programs Maurice Beghetti Pediatric Cardiology University Children s Hospital HUG and CHUV Pulmonary Hypertension Program HUG Centre Universitaire Romand de Cardiologie
Risk populations moving to screening programs Maurice Beghetti Pediatric Cardiology University Children s Hospital HUG and CHUV Pulmonary Hypertension Program HUG Centre Universitaire Romand de Cardiologie
Out of proportion pulmonary hypertension
 IPF the missing link Out of proportion pulmonary hypertension Rome 29-30 May 2015 Sergio Harari U.O. di Pneumologia e UTIR Servizio di Emodinamica e Fisiopatologia Respiratoria Ospedale San Giuseppe -
IPF the missing link Out of proportion pulmonary hypertension Rome 29-30 May 2015 Sergio Harari U.O. di Pneumologia e UTIR Servizio di Emodinamica e Fisiopatologia Respiratoria Ospedale San Giuseppe -
ACTIVITY DESCRIPTION Target Audience Learning Objectives
 ACTIVITY DESCRIPTION Target Audience This continuing medical education activity is planned to meet the needs of primary care providers who can contribute to early detection of disease and who are responsible
ACTIVITY DESCRIPTION Target Audience This continuing medical education activity is planned to meet the needs of primary care providers who can contribute to early detection of disease and who are responsible
Where are we now in the longterm. of PAH and CTEPH? Hits and misses of medical treatment. Hap Farber Boston University School of Medicine, Boston, USA
 Where are we now in the longterm management of PAH and CTEPH? Hits and misses of medical treatment Hap Farber Boston University School of Medicine, Boston, USA Monday, 28 September ERS International Congress
Where are we now in the longterm management of PAH and CTEPH? Hits and misses of medical treatment Hap Farber Boston University School of Medicine, Boston, USA Monday, 28 September ERS International Congress
Φαρµακοθεραπεία στη Πνευµονική Αρτηριακή Υπέρταση: Αρχική ή διαδοχική συνδυαστική θεραπεία
 37 ο Πανελλήνιο Καρδιολογικό Συνέδριο Αθήνα, Οκτώβριος 2016 k Φαρµακοθεραπεία στη Πνευµονική Αρτηριακή Υπέρταση: Αρχική ή διαδοχική συνδυαστική θεραπεία Αναστασία Ανθη Β Κλιν. Εντατικής Θεραπείας & Διακλινικό
37 ο Πανελλήνιο Καρδιολογικό Συνέδριο Αθήνα, Οκτώβριος 2016 k Φαρµακοθεραπεία στη Πνευµονική Αρτηριακή Υπέρταση: Αρχική ή διαδοχική συνδυαστική θεραπεία Αναστασία Ανθη Β Κλιν. Εντατικής Θεραπείας & Διακλινικό
Disclosures. Inhaled Therapy in Pediatric Pulmonary Hypertension. Inhaled Prostacyclin: Rationale. Outline
 Disclosures Inhaled Therapy in Pediatric Pulmonary Hypertension The University of Colorado receives fees for Dr Ivy to be a consultant for Actelion, Gilead, Lilly, Pfizer, and United Therapeutics Dunbar
Disclosures Inhaled Therapy in Pediatric Pulmonary Hypertension The University of Colorado receives fees for Dr Ivy to be a consultant for Actelion, Gilead, Lilly, Pfizer, and United Therapeutics Dunbar
Πνευμονική υπέρταση: Τα 10 πιο σημαντικά κενά και παραλείψεις των Κατευθυντήριων Οδηγιών του 2015
 Πνευμονική υπέρταση: Τα 10 πιο σημαντικά κενά και παραλείψεις των Κατευθυντήριων Οδηγιών του 2015 Γεωργία Γ. Πίτσιου, MD, MSc, PhD Πνευμονολόγος- Εντατικολόγος Επίκουρη Καθηγήτρια Ιατρική Σχολή ΑΠΘ Γ.Ν.
Πνευμονική υπέρταση: Τα 10 πιο σημαντικά κενά και παραλείψεις των Κατευθυντήριων Οδηγιών του 2015 Γεωργία Γ. Πίτσιου, MD, MSc, PhD Πνευμονολόγος- Εντατικολόγος Επίκουρη Καθηγήτρια Ιατρική Σχολή ΑΠΘ Γ.Ν.
INHALED TREPROSTINIL IN PULMONARY HYPERTENSION DUE TO INTERSTITIAL LUNG DISEASE (PH-ILD)
") THE INCREASE STUDY INHALED TREPROSTINIL IN PULMONARY HYPERTENSION DUE TO INTERSTITIAL LUNG DISEASE (PH-ILD) Peter Smith, PharmD Senior Director Product Development, United Therapeutics Corporation 2 SAFE
THE INCREASE STUDY INHALED TREPROSTINIL IN PULMONARY HYPERTENSION DUE TO INTERSTITIAL LUNG DISEASE (PH-ILD) Peter Smith, PharmD Senior Director Product Development, United Therapeutics Corporation 2 SAFE
NOT COPY. Choice of the primary outcome: Pro Lung 03/09/2018. Lung assessment in clinical trials
 Choice of the primary outcome: Pro Lung Christopher P. Denton Professor of Experimental Rheumatology Royal Free Hospital and University College London, UK Florence 7 th September 218 Improved clinical
Choice of the primary outcome: Pro Lung Christopher P. Denton Professor of Experimental Rheumatology Royal Free Hospital and University College London, UK Florence 7 th September 218 Improved clinical
Pulmonary Arterial Hypertension: The Approach to Management in 2019
 Pulmonary Arterial Hypertension: The Approach to Management in 2019 Munir S. Janmohamed M.D. FACC Medical Director Mechanical Circulatory Support/Heart Failure Program Mercy General Hospital/Mercy Medical
Pulmonary Arterial Hypertension: The Approach to Management in 2019 Munir S. Janmohamed M.D. FACC Medical Director Mechanical Circulatory Support/Heart Failure Program Mercy General Hospital/Mercy Medical
PULMONARY HYPERTENSION RESPIRATORY & CRITICAL CARE CONFERENCE APRIL 21, 2016 LAURA G. HOOPER
 PULMONARY HYPERTENSION RESPIRATORY & CRITICAL CARE CONFERENCE APRIL 21, 2016 LAURA G. HOOPER OUTLINE Brief review of WHO Group Classification Scheme Subgroups we ll focus on: WHO Group I Pulmonary Arterial
PULMONARY HYPERTENSION RESPIRATORY & CRITICAL CARE CONFERENCE APRIL 21, 2016 LAURA G. HOOPER OUTLINE Brief review of WHO Group Classification Scheme Subgroups we ll focus on: WHO Group I Pulmonary Arterial
Pharmacy Management Drug Policy
 SUBJECT: Pulmonary Arterial Hypertension (PAH) POLICY NUMBER: Pharmacy-42 Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed
SUBJECT: Pulmonary Arterial Hypertension (PAH) POLICY NUMBER: Pharmacy-42 Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed
ELIGIBILITY CRITERIA FOR PULMONARY ARTERIAL HYPERTENSION THERAPY
 ELIGIBILITY CRITERIA FOR PULMONARY ARTERIAL HYPERTENSION THERAPY Contents Eligibility criteria for Pulmonary Arterial Hypertension therapy...2-6 Initial Application for funding of Pulmonary Arterial Hypertension
ELIGIBILITY CRITERIA FOR PULMONARY ARTERIAL HYPERTENSION THERAPY Contents Eligibility criteria for Pulmonary Arterial Hypertension therapy...2-6 Initial Application for funding of Pulmonary Arterial Hypertension
Θεραπεία με βάση τη βαρύτητα ή εξαρχής επιθετική συνδυαστική θεραπεία. Φραντζέσκα Φραντζεσκάκη Πνευμονολόγος-Εντατικολόγος ΠΓΝ «ΑΤΤΙΚΟΝ»
 Θεραπεία με βάση τη βαρύτητα ή εξαρχής επιθετική συνδυαστική θεραπεία Φραντζέσκα Φραντζεσκάκη Πνευμονολόγος-Εντατικολόγος ΠΓΝ «ΑΤΤΙΚΟΝ» S.Gaine and V.McLaughlin, Eur Respi Rev 2017;26 Ultimate goal of
Θεραπεία με βάση τη βαρύτητα ή εξαρχής επιθετική συνδυαστική θεραπεία Φραντζέσκα Φραντζεσκάκη Πνευμονολόγος-Εντατικολόγος ΠΓΝ «ΑΤΤΙΚΟΝ» S.Gaine and V.McLaughlin, Eur Respi Rev 2017;26 Ultimate goal of
PFIZER INC. THERAPEUTIC AREA AND FDA APPROVED INDICATIONS: See United States Package Insert (USPI)
") PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
PVDOMICS. Study Introduction. Kristin Highland, MD Gerald Beck, PhD. NHLBI Pulmonary Vascular Disease Phenomics Program
 PVDOMICS Study Introduction Kristin Highland, MD Gerald Beck, PhD NHLBI Pulmonary Vascular Disease Phenomics Program Funded by the National Heart, Lung, and Blood Institute of the National Institutes of
PVDOMICS Study Introduction Kristin Highland, MD Gerald Beck, PhD NHLBI Pulmonary Vascular Disease Phenomics Program Funded by the National Heart, Lung, and Blood Institute of the National Institutes of
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST ESC Congress 2011 Pathophysiology of HFPEF Vascular Remodeling & Pulmonary Hypertension Carolyn S.P. Lam MBBS, MRCP, MS Case Presentation 81 yo woman with dyspnoea &
DECLARATION OF CONFLICT OF INTEREST ESC Congress 2011 Pathophysiology of HFPEF Vascular Remodeling & Pulmonary Hypertension Carolyn S.P. Lam MBBS, MRCP, MS Case Presentation 81 yo woman with dyspnoea &
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Health Technology Appraisal. Drugs for the treatment of pulmonary arterial hypertension
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Drugs for the treatment of Draft remit / appraisal objective: Draft scope To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Drugs for the treatment of Draft remit / appraisal objective: Draft scope To appraise the clinical and cost effectiveness
Therapy Update: ERAs. Review of Mechanism. Disclosure Statements. Outline. Disclosure: Research support from United Therapeutics
 1 Therapy Update: ERAs Disclosure Statements Disclosure: Research support from United Therapeutics Most of the medications discussed in this presentation are off-label usage Nidhy Varghese, MD Pulmonary
1 Therapy Update: ERAs Disclosure Statements Disclosure: Research support from United Therapeutics Most of the medications discussed in this presentation are off-label usage Nidhy Varghese, MD Pulmonary
Teaching Round Claudio Sartori
 Teaching Round 14.03.2017 Claudio Sartori Cas clinique Femme 47 ans, connue pour un BPCO, asthénie, douleurs thoraciques, dyspnée à l effort, œdèmes membres inférieurs, deux syncopes. Tabac, BMI 31 kg/m2
Teaching Round 14.03.2017 Claudio Sartori Cas clinique Femme 47 ans, connue pour un BPCO, asthénie, douleurs thoraciques, dyspnée à l effort, œdèmes membres inférieurs, deux syncopes. Tabac, BMI 31 kg/m2
Treatment of Paediatric Pulmonary Hypertension
 Treatment of Paediatric Pulmonary Hypertension Dunbar Ivy, MD The Children s Hospital Heart Institute University of Colorado School of Medicine 1 Disclosures I have the following financial relationships
Treatment of Paediatric Pulmonary Hypertension Dunbar Ivy, MD The Children s Hospital Heart Institute University of Colorado School of Medicine 1 Disclosures I have the following financial relationships
What You Need to Know About Pulmonary Arterial Hypertension: The Role of Primary Care Physicians
 Saturday General Session What You Need to Know About Pulmonary Arterial Hypertension: The Role of Primary Care Physicians Trushil Shah, MD, MS Assistant Professor of Internal Medicine Pulmonary Hypertension
Saturday General Session What You Need to Know About Pulmonary Arterial Hypertension: The Role of Primary Care Physicians Trushil Shah, MD, MS Assistant Professor of Internal Medicine Pulmonary Hypertension
Update on pulmonary HTN
 Update on pulmonary HTN Feras Bader, MD, MS, FACC Associate Professor of Medicine- Cardiology University of Utah School of Medicine Director, Advanced Heart Failure and Transplant Program Dabbous Cardiac
Update on pulmonary HTN Feras Bader, MD, MS, FACC Associate Professor of Medicine- Cardiology University of Utah School of Medicine Director, Advanced Heart Failure and Transplant Program Dabbous Cardiac
Dr.Fayez EL Shaer Consultant cardiologist Assistant professor of cardiology KKUH
 Pulmonary Hypertension in patients with Heart Failure with Preserved Ejection Fraction Dr.Fayez EL Shaer Consultant cardiologist Assistant professor of cardiology KKUH Recent evaluation of available data
Pulmonary Hypertension in patients with Heart Failure with Preserved Ejection Fraction Dr.Fayez EL Shaer Consultant cardiologist Assistant professor of cardiology KKUH Recent evaluation of available data
An Inconvenient Choice Pulmonary Artery Systolic Pressure of 43 mmhg: Is a Work Up for Pulmonary Hypertension Warranted?
 An Inconvenient Choice Pulmonary Artery Systolic Pressure of 43 mmhg: Is a Work Up for Pulmonary Warranted? Michael D. McGoon, MD Professor of Medicine Consultant in Cardiovascular Diseases Mayo Clinic
An Inconvenient Choice Pulmonary Artery Systolic Pressure of 43 mmhg: Is a Work Up for Pulmonary Warranted? Michael D. McGoon, MD Professor of Medicine Consultant in Cardiovascular Diseases Mayo Clinic
Contreversies in the management of PH What is controversial in treatment?
 Contreversies in the management of PH What is controversial in treatment? Service de Pneumologie et Réanimation National reference center for pulmonary hypertension Université Paris Sud Hôpital Antoine
Contreversies in the management of PH What is controversial in treatment? Service de Pneumologie et Réanimation National reference center for pulmonary hypertension Université Paris Sud Hôpital Antoine
Pharmacy Management Drug Policy
 SUBJECT: POLICY NUMBER: PHARMACY-42 EFFECTIVE DATE: 6/2005 LAST REVIEW DATE: 4/19/2018 If the member s subscriber contract excludes coverage for a specific service or prescription drug, it is not covered
SUBJECT: POLICY NUMBER: PHARMACY-42 EFFECTIVE DATE: 6/2005 LAST REVIEW DATE: 4/19/2018 If the member s subscriber contract excludes coverage for a specific service or prescription drug, it is not covered
Updates in Pulmonary Hypertension Pharmacotherapy. Ziad Sadik PharmD BCPS
 Updates in Pulmonary Hypertension Pharmacotherapy Ziad Sadik PharmD BCPS Disclosure Information I have no financial relationship to disclose AND I will not discuss off label use and/or investigational
Updates in Pulmonary Hypertension Pharmacotherapy Ziad Sadik PharmD BCPS Disclosure Information I have no financial relationship to disclose AND I will not discuss off label use and/or investigational
Pulmonary Hypertension A-Z
 Pulmonary Hypertension A-Z Lana Melendres-Groves UNM Pulmonary Hypertension Program Director Assistant Professor of Medicine Pulmonary/Critical Care Division 9/17/16 Disclosures Advisory board member Actelion
Pulmonary Hypertension A-Z Lana Melendres-Groves UNM Pulmonary Hypertension Program Director Assistant Professor of Medicine Pulmonary/Critical Care Division 9/17/16 Disclosures Advisory board member Actelion
2015 State-of-the-Art Management of Pulmonary Hypertension Based on an Understanding of the Various Etiologies
 2015 State-of-the-Art Management of Pulmonary Hypertension Based on an Understanding of the Various Etiologies Vallerie V. McLaughlin, MD, FACC, FAHA Kim A Eagle MD Endowed Professor of Cardiovascular
2015 State-of-the-Art Management of Pulmonary Hypertension Based on an Understanding of the Various Etiologies Vallerie V. McLaughlin, MD, FACC, FAHA Kim A Eagle MD Endowed Professor of Cardiovascular
Role of Combination PAH Therapies
 Role of Combination PAH Therapies Ronald J. Oudiz, MD, FACP, FACC Associate Professor of Medicine, David Geffen School of Medicine at UCLA Director, Liu Center for Pulmonary Hypertension Los Angeles Biomedical
Role of Combination PAH Therapies Ronald J. Oudiz, MD, FACP, FACC Associate Professor of Medicine, David Geffen School of Medicine at UCLA Director, Liu Center for Pulmonary Hypertension Los Angeles Biomedical
Combination therapy in the treatment of pulmonary arterial hypertension 2015 update
 Journal of Rare Cardiovascular Diseases 2015; 2 (4): 103 107 www.jrcd.eu REVIEW ARTICLE Rare diseases of pulmonary circulation Combination therapy in the treatment of pulmonary arterial hypertension 2015
Journal of Rare Cardiovascular Diseases 2015; 2 (4): 103 107 www.jrcd.eu REVIEW ARTICLE Rare diseases of pulmonary circulation Combination therapy in the treatment of pulmonary arterial hypertension 2015
Clinical Commissioning Policy: Selexipag for treating pulmonary arterial hypertension (all ages)
") Clinical Commissioning Policy: Selexipag for treating pulmonary arterial hypertension (all ages) NHS England Reference: 170065P 1 NHS England INFORMATION READER BOX Directorate Medical Operations and Information
Clinical Commissioning Policy: Selexipag for treating pulmonary arterial hypertension (all ages) NHS England Reference: 170065P 1 NHS England INFORMATION READER BOX Directorate Medical Operations and Information
Pulmonary Arterial Hypertension: A Journey to Lung Transplant
 PH GRAND ROUNDS Pulmonary Arterial Hypertension: A Journey to Lung Transplant Section Editor Deborah J. Levine, MD Bravein Amalakuhan, MD Pulmonary and Critical Care Medicine Fellow University of Texas
PH GRAND ROUNDS Pulmonary Arterial Hypertension: A Journey to Lung Transplant Section Editor Deborah J. Levine, MD Bravein Amalakuhan, MD Pulmonary and Critical Care Medicine Fellow University of Texas
Clinical Science Working Group 6: Diagnosis & Assessment of PAH. Co-chairs: David B. Badesch, MD Marius M. Hoeper, MD. Working Group 6 Members
 Clinical Science Working Group 6: Diagnosis & Assessment of PAH Co-chairs: David B. Badesch, MD Marius M. Hoeper, MD Working Group 6 Members Harm Jan Bogaard, Robin Condliffe, Robert Frantz, Dinesh Khanna,
Clinical Science Working Group 6: Diagnosis & Assessment of PAH Co-chairs: David B. Badesch, MD Marius M. Hoeper, MD Working Group 6 Members Harm Jan Bogaard, Robin Condliffe, Robert Frantz, Dinesh Khanna,
Pulmonary Hypertension: Another Use for Viagra
 Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A
Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A
Pulmonary Hypertension: We have come a Long Way
 Pulmonary Hypertension: We have come a Long Way Shelley Shapiro M.D. Ph.D Pulmonary Hypertension Program 9001.01 1 2 Disclosures Grant Support Gilead, United Therapeutics, Actelion, GeNO, Medtonics, Bellerphon,
Pulmonary Hypertension: We have come a Long Way Shelley Shapiro M.D. Ph.D Pulmonary Hypertension Program 9001.01 1 2 Disclosures Grant Support Gilead, United Therapeutics, Actelion, GeNO, Medtonics, Bellerphon,
Prognostic value of echocardiographic parameters in patients with pulmonary arterial hypertension (PAH) treated with targeted therapies
 treated with targeted therapies") Prognostic value of echocardiographic parameters in patients with pulmonary arterial hypertension (PAH) treated with targeted therapies E. Beciani, M. Palazzini, C. Bachetti, F. Sgro, E. Conficoni, E.
Prognostic value of echocardiographic parameters in patients with pulmonary arterial hypertension (PAH) treated with targeted therapies E. Beciani, M. Palazzini, C. Bachetti, F. Sgro, E. Conficoni, E.
Pulmonary Arterial Hypertension in Pa)ents with HIV Infec)on: New Thoughts, BeGer Outcomes
ents with HIV Infec)on: New Thoughts, BeGer Outcomes") Pulmonary Arterial Hypertension in Pa)ents with HIV Infec)on: New Thoughts, BeGer Outcomes Hap Farber, MD Director, Pulmonary Hypertension Center Boston University School of Medicine Disclosures Consultant:
Pulmonary Arterial Hypertension in Pa)ents with HIV Infec)on: New Thoughts, BeGer Outcomes Hap Farber, MD Director, Pulmonary Hypertension Center Boston University School of Medicine Disclosures Consultant:
Emerging Challenges in Primary Care: Evolving Strategies of Care in Pulmonary Arterial Hypertension: Integrating the Data into Practice
 Emerging Challenges in Primary Care: 2018 Evolving Strategies of Care in Pulmonary Arterial Hypertension: Integrating the Data into Practice 1 Alexander Duarte, MD Professor Division of Pulmonary Critical
Emerging Challenges in Primary Care: 2018 Evolving Strategies of Care in Pulmonary Arterial Hypertension: Integrating the Data into Practice 1 Alexander Duarte, MD Professor Division of Pulmonary Critical
Understanding Complex Pulmonary Hypertension through Advanced Hemodynamics
 Understanding Complex Pulmonary Hypertension through Advanced Hemodynamics Franz Rischard, DO, MS Director, Pulmonary Hypertension Program Assistant Professor of Medicine University of Arizona Lillian
Understanding Complex Pulmonary Hypertension through Advanced Hemodynamics Franz Rischard, DO, MS Director, Pulmonary Hypertension Program Assistant Professor of Medicine University of Arizona Lillian
The World Health Organization (WHO) has classified pulmonary hypertension into five different groups: (3)
 has classified pulmonary hypertension into five different groups: (3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.15 Subject: Flolan Veletri Page: 1 of 5 Last Review Date: September 15, 2017 Flolan Veletri Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.15 Subject: Flolan Veletri Page: 1 of 5 Last Review Date: September 15, 2017 Flolan Veletri Description
Pulmonary Arterial Hypertension (PAH): Emerging Therapeutic Strategies
: Emerging Therapeutic Strategies") Pulmonary Arterial Hypertension (PAH): Emerging Therapeutic Strategies Nick H. Kim, M.D. Clinical Professor of Medicine Director, Pulmonary Vascular Medicine Clinical Service Chief, PCCSM La Jolla Pulmonary,
Pulmonary Arterial Hypertension (PAH): Emerging Therapeutic Strategies Nick H. Kim, M.D. Clinical Professor of Medicine Director, Pulmonary Vascular Medicine Clinical Service Chief, PCCSM La Jolla Pulmonary,
Clinical implication of exercise pulmonary hypertension: when should we measure it?
 Clinical implication of exercise pulmonary hypertension: when should we measure it? Jang-Young, Kim Wonju College of Medicine, Yonsei Univ. Exercise pulmonary hypertension (EPH) Introduction of pulmonary
Clinical implication of exercise pulmonary hypertension: when should we measure it? Jang-Young, Kim Wonju College of Medicine, Yonsei Univ. Exercise pulmonary hypertension (EPH) Introduction of pulmonary
Advances in Pharmacotherapy of PAH
 24 th Annual Advances in Heart Disease Advances in Pharmacotherapy of PAH Gabriel Gregoratos, MD 12/14/2007 UCSF Cardiology 1 Faculty Disclosure Statement for Gabriel Gregoratos, MD Nothing to disclose
24 th Annual Advances in Heart Disease Advances in Pharmacotherapy of PAH Gabriel Gregoratos, MD 12/14/2007 UCSF Cardiology 1 Faculty Disclosure Statement for Gabriel Gregoratos, MD Nothing to disclose
Tadalafil for the Treatment of Pulmonary Arterial Hypertension
 Journal of the American College of Cardiology Vol. 60, No. 8, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2012.05.004
Journal of the American College of Cardiology Vol. 60, No. 8, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2012.05.004
Modern Management of Pulmonary Hypertension: Expert Guidance for Individualized Care in the Community Practice Setting
 Modern Management of Pulmonary Hypertension: Expert Guidance for Individualized Care in the Community Practice Setting Agenda 1. Welcome & introduction 2. Brief summary of best practices for optimal screening,
Modern Management of Pulmonary Hypertension: Expert Guidance for Individualized Care in the Community Practice Setting Agenda 1. Welcome & introduction 2. Brief summary of best practices for optimal screening,
Scleroderma and PAH Overview. PH Resource Network Martha Kingman, FNP C UTSW Medical Center at Dallas
 Scleroderma and PAH Overview PH Resource Network 2007 Martha Kingman, FNP C UTSW Medical Center at Dallas Scleroderma and PAH Outline: Lung involvement in scleroderma Evaluation of the scleroderma patient
Scleroderma and PAH Overview PH Resource Network 2007 Martha Kingman, FNP C UTSW Medical Center at Dallas Scleroderma and PAH Outline: Lung involvement in scleroderma Evaluation of the scleroderma patient
Scottish Medicines Consortium
 Scottish Medicines Consortium sildenafil, 20mg (as citrate) tablets (Revatio ) No. (596/10) Pfizer Ltd 15 January 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
Scottish Medicines Consortium sildenafil, 20mg (as citrate) tablets (Revatio ) No. (596/10) Pfizer Ltd 15 January 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
Challenging the 2015 PH Guidelines. Pulmonary Hypertension Definitions and Diagnosis Comments and Proposals
 Challenging the 2015 PH Guidelines Pulmonary Hypertension Definitions and Diagnosis Comments and Proposals Professor Sean Gaine Mater Misericordiae University Hospital Dublin, Ireland Definitions and Diagnosis:
Challenging the 2015 PH Guidelines Pulmonary Hypertension Definitions and Diagnosis Comments and Proposals Professor Sean Gaine Mater Misericordiae University Hospital Dublin, Ireland Definitions and Diagnosis:
*Division of Pulmonary, Sleep, and Critical Care Medicine, Rhode Island Hospital, Alpert Medical School of Brown University, Providence, RI, USA
 The Relationship between NO Pathway Biomarkers and Response to Riociguat in the RESPITE Study of Patients with PAH Not Reaching Treatment Goals with Phosphodiesterase 5 Inhibitors James R Klinger,* Raymond
The Relationship between NO Pathway Biomarkers and Response to Riociguat in the RESPITE Study of Patients with PAH Not Reaching Treatment Goals with Phosphodiesterase 5 Inhibitors James R Klinger,* Raymond
The World Health Organization (WHO) has classified pulmonary hypertension into five different groups: (2)
 has classified pulmonary hypertension into five different groups: (2)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.16 Subject: Letairis Page: 1 of 6 Last Review Date: June 24, 2016 Letairis Description Letairis (ambrisentan)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.16 Subject: Letairis Page: 1 of 6 Last Review Date: June 24, 2016 Letairis Description Letairis (ambrisentan)
Therapeutic Categories Outlook
 Equity Research Health Care Therapeutic Categories Outlook Comprehensive Study February 2017 Alzheimer s Disease Bone Diseases Cardiovascular Central Nervous System Dermatology Diabetes/Obesity Epilepsy
Equity Research Health Care Therapeutic Categories Outlook Comprehensive Study February 2017 Alzheimer s Disease Bone Diseases Cardiovascular Central Nervous System Dermatology Diabetes/Obesity Epilepsy
Pulmonary manifestations of CTDs Diagnosis, differential diagnosis and treatment
 Prague, June 2014 Pulmonary manifestations of CTDs Diagnosis, differential diagnosis and treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
Prague, June 2014 Pulmonary manifestations of CTDs Diagnosis, differential diagnosis and treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
4/14/2010. Pulmonary Hypertension: An Update. Tim Williamson, MD, FCCP. University of Kansas Hospital. Normal Physiology
 Pulmonary Hypertension: An Update Tim Williamson, MD, FCCP Director, Pulmonary Vascular Program University of Kansas Hospital Normal Physiology 1 Pulmonary Perfusion 101 High Pressure Low Pressure Pulmonary
Pulmonary Hypertension: An Update Tim Williamson, MD, FCCP Director, Pulmonary Vascular Program University of Kansas Hospital Normal Physiology 1 Pulmonary Perfusion 101 High Pressure Low Pressure Pulmonary
Pulmonary Hypertension: Definition and Unmet Needs
 Heart Failure Center Hadassah University Hospital Pulmonary Hypertension: Definition and Unmet Needs Israel Gotsman The Heart Failure Center Hadassah University Hospital I DO NOT have a financial interest/
Heart Failure Center Hadassah University Hospital Pulmonary Hypertension: Definition and Unmet Needs Israel Gotsman The Heart Failure Center Hadassah University Hospital I DO NOT have a financial interest/
Filtering through the Facts: Portopulmonary Hypertension Saturday, September 19, :15 10:05 a.m.
 Filtering through the Facts: Portopulmonary Hypertension Saturday, September 19, 2015 9:15 10:05 a.m. Joel Wirth, MD Pulmonary & Critical Care Medicine Maine Medical Center, Portland, ME Disclosures Dr.
Filtering through the Facts: Portopulmonary Hypertension Saturday, September 19, 2015 9:15 10:05 a.m. Joel Wirth, MD Pulmonary & Critical Care Medicine Maine Medical Center, Portland, ME Disclosures Dr.
Dr. Tracy Luckhardt Division of Pulmonary, Allergy and Critical Care Medicine University of Alabama at Birmingham
 Dr. Tracy Luckhardt Division of Pulmonary, Allergy and Critical Care Medicine University of Alabama at Birmingham Types of Questions you Will Be Asked Rhetorical Participatory Disclosure of Relevant Financial
Dr. Tracy Luckhardt Division of Pulmonary, Allergy and Critical Care Medicine University of Alabama at Birmingham Types of Questions you Will Be Asked Rhetorical Participatory Disclosure of Relevant Financial
Objectives. Disclosure. Objectives. Treatment of Pulmonary Hypertension 3/4/2016. Pharmacist Objectives: 3. Technician Objectives:
 Objectives Treatment of Pulmonary Hypertension Janet Job PGY-1 Pharmacy Practice Resident Memorial Regional Hospital March 12, 2016 Pharmacist Objectives: Identify the pathophysiology, clinical presentation,
Objectives Treatment of Pulmonary Hypertension Janet Job PGY-1 Pharmacy Practice Resident Memorial Regional Hospital March 12, 2016 Pharmacist Objectives: Identify the pathophysiology, clinical presentation,