Unrestricted. Dr ppooransari fellowship of perenatalogy
|
|
|
- Ashley Lamb
- 5 years ago
- Views:
Transcription


1 Unrestricted Dr ppooransari fellowship of perenatalogy
2
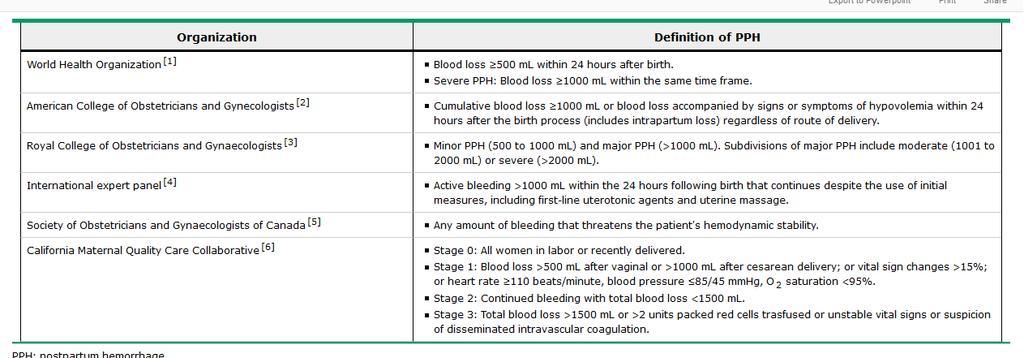
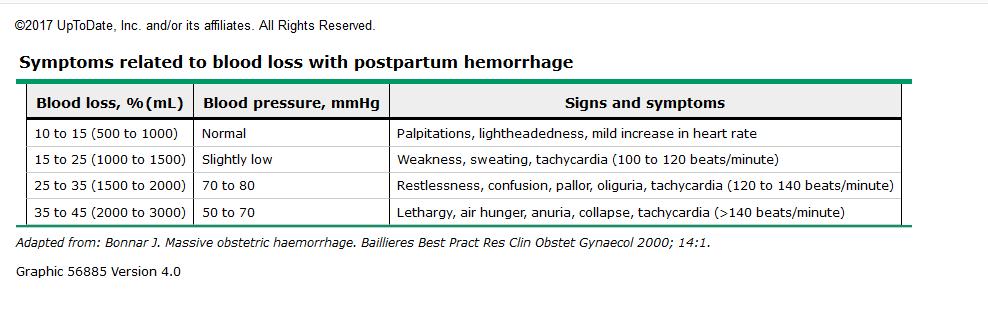
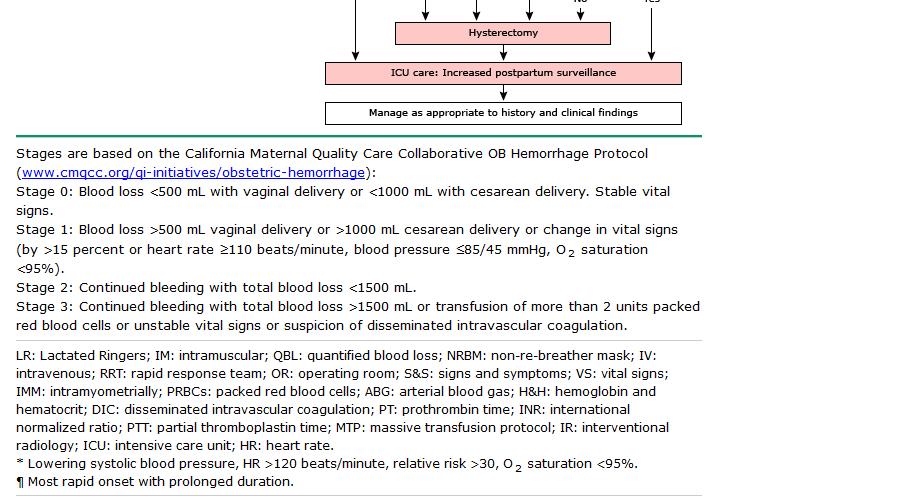
3 Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and up to 25 percent of a patient's blood volume ( 1500 ml in pregnancy) can be lost before blood pressure falls and heart rate rises.hemoglobin and hematocrit values are poor indicators of acute blood loss since they may not decline immediately after an acute bleed.
4
5
6
7 Evaluate blood pressure, heart rate, respiratory rate, peripheral oxygen saturation, and urine output. Tachypnea, tachycardia, hypotension, low oxygen saturation, and air hunger are signs of hypovolemia, which may be due to both inadequate hemoglobin level and circulatory volume
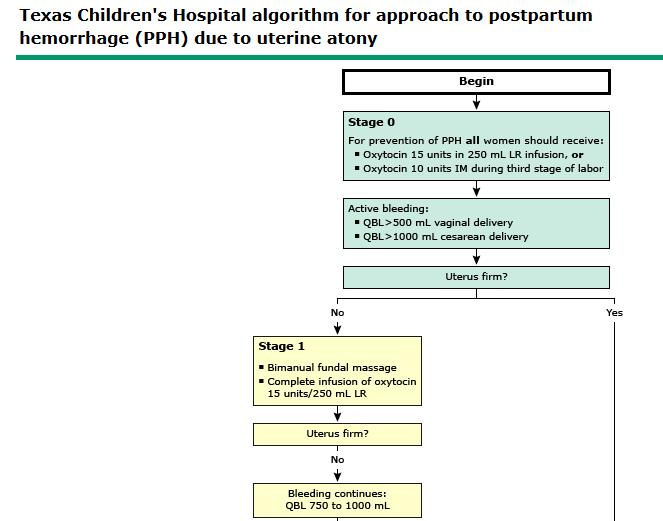
8 BLOOD LOSS >500 ML AT VAGINAL DELIVERY OR >1000 ML AT CESAREAN DELIVERY BUT <1500 ML WITH ONGOING EXCESSIVE BLEEDING These patients are generally hemodynamically stable, but may have mild tachycardia (heart rate 110 beats/min), mild hypotension (systolic blood pressure 80 to 85 mmhg), fall in oxygen saturation (O 2 sat <95 percent), and/or lightheadedness, before initiation of therapy.
9 Establish adequate intravenous access Resuscitate with crystalloid Isotonic crystalloid should be infused to prevent hypotension (target systolic pressure 90 mmhg) and maintain urine output at >30 ml/hour.. Rapid infusion of large volumes of crystalloid (eg, >3 to 4 L) may promote dilutional coagulopathy, electrolyte imbalances, and hypothermia, so appropriately monitoring of hematocrit, coagulation status, core temperature, and electrolytes is essential
10 . Risk factors for significant cervical lacerations (ie, associated with excessive bleeding or requiring repair) include precipitous labor, operative vaginal delivery, and cerclage.
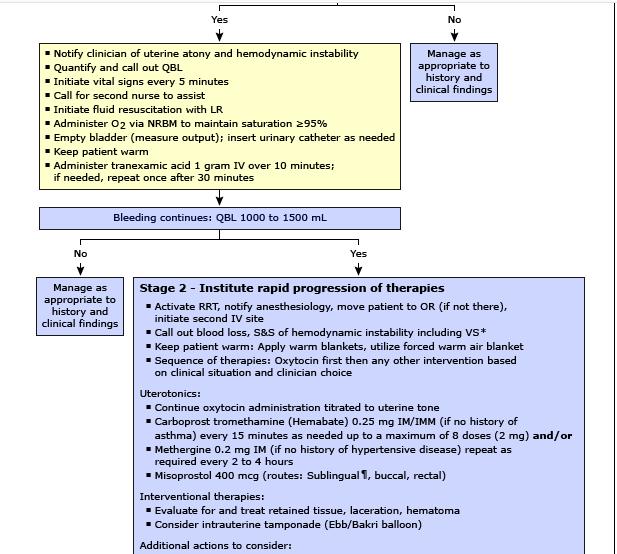
11 Administer tranexamic acid Tranexamic acid is an anti-fibrinolytic drug that has been useful for prevention and treatment of bleeding in various clinical settings, such as surgery and trauma. Reduced death due to bleeding by 19 percent overall Reduced the incidence of laparotomy to control bleeding by 36 percent not increase the risk of thromboembolic events, which had been a concern based on data in case reports.
12 Tranexamic acid is given concomitantly with other drugs and procedures for control of bleeding, and should not be regarded as an alternative therapy. One gram (10 ml of a 100mg/mL solution) is infused over 10 to 20 minutes, as infusion >1 ml/minute can cause hypotension.
13 as infusion >1 ml/minute can cause hypotension. If bleeding persists after 30 minutes, a second 1 g dose may be administered. The half-life is two hours and the antifibrinolytic effect lasts up to 7 to 8 hours in serum.
14 Tranexamic acid should not be mixed with blood or given through a line with blood, or mixed with solutions containing penicillin. It should not be given to patients with subarachnoid hemorrhage or active intravascular clotting (disseminated intravascular coagulation). The dose should be reduced in patients with renal insufficiency, venous or arterial thrombosis, or ureteral bleeding.
15 Increase oxytocin infusion Therefore, if a high-dose oxytocin regimen is used, it is advisable to prepare smaller volumes (ie, 15 units in 250 ml) to limit the total dose infused over a short period of time. Administer additional uterotonic drugs uterotonic drugs are administered for presumed atony until a therapeutic effect is observed or until it is obvious that these drugs are ineffective
16 we promptly administer carboprost tromethamine (contraindication: asthma) and/or methylergonovine (contraindications: hypertension, coronary or cerebral artery disease, Raynaud's syndrome). Up to eight doses of carboprost tromethamine may be given intramuscularly at least 15 minutes apart, but if bleeding continues unabated after two doses are given, further benefit of repeated doses is unclear. Methylergonovine may be repeated every two to four hours as needed.
17 if no asthma, carboprost tromethamine (15 methyl-pgf2alpha, Hemabate) 250 mcg intramuscularly every 15 to 90 minutes, as needed, to a total cumulative dose of 2 mg (eight doses). About 75 percent of patients respond to a single dose; move on to a different uterotonic agent if no response after one or two doses. The author prefers to use a dilute solution of 250 mcg in 20 ml normal saline for injection given via a six-inch spinal needle. Prior to the blind injection of this solution into the myometrium, aspiration should be performed to prevent intravenous administration.
18 these pharmacologic interventions are ineffective or only partially effective, or if there is any delay in getting these uterotonic drugs, we expeditiously move on to placing a tamponade balloon to decrease bleeding and plan for interventional radiology or surgical options. Uterotonic drugs are continued until bleeding is controlled.
19 If no hypertension or other significant arterial disease, methylergonovine 0.2 mg intramuscularly or directly into the myometrium (never intravenously). May repeat at two- to four-hour intervals, as needed Misoprostol (PGE1) is most useful for reducing blood loss in settings where injectable uterotonics are unavailable or contraindicated (eg, hypertension, asthma). i n addition, the side effect of hyperthermia is a significant disadvantage of this drug because it is uncomfortable, triggers a work up for sepsis, and may lead to unnecessary empiric antibiotic therapy.
20 Rectally administered misoprostol has a longer duration of action than oral/sublingual routes (four hours versus two to three hours), which is advantageous in PPH and may be necessary in semi-conscious or unconscious patients. unlike methylergonovine and carboprost, misoprostol can be given to women with hypertension or asthma. Dinoprostone (PGE2) 20 mg vaginal or rectal suppository is an alternative prostaglandin to misoprostol (PGE1). It can be repeated at two-hour intervals.
21 Carbetocin, a long-acting analog of oxytocin, it appears to be as effective as oxytocin. Carbetocin 100 mcg is given by a single slow intravenous injection (ie, over one minute), although lower doses may be effective. The toxicity spectrum is similar to that of oxytocin.
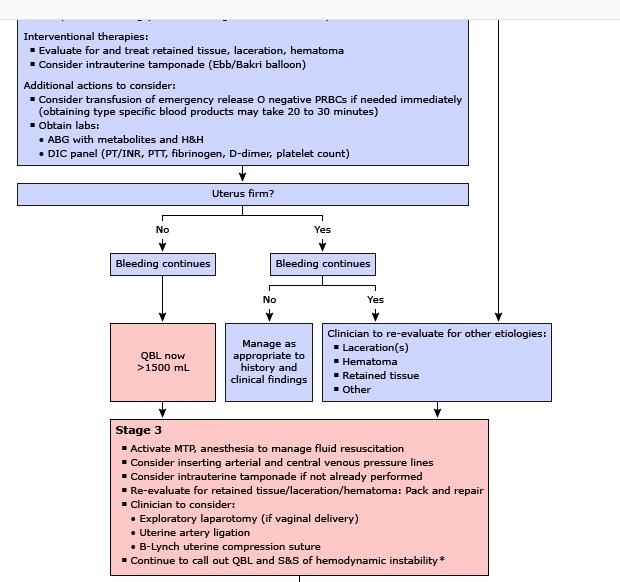
22 BLOOD LOSS >1500 ML WITH ONGOING EXCESSIVE BLEEDING These patients may be hemodynamically unstable. Any unstable patient who is not already in an operating room should be moved to an operating room as soon as practically possible. Central venous access via the subclavian or internal jugular route should be considered early (while the patient is still in compensated shock) as it is often very difficult to gain such access in a shocked and hemodynamically unstable patient. In addition, it may take time to assemble appropriate personnel (anesthesia team, vascular access team) to place the lines. A bladder catheter with urometer should be inserted to monitor urine output.
23 Fibrinogen falls to critically low levels earlier than other coagulation factors during PPH, thus the fibrinogen level is a more sensitive indicator of ongoing major blood loss than the prothrombin time, activated partial thromboplastin time, or platelet count. The fibrinogen level at the time of diagnosis of PPH is predictive of severity and can be used to guide the aggressiveness of management In multiple studies of women with PPH, a low fibrinogen level (less than 200 mg/dl) was predictive of severe PPH defined as need for transfusion of multiple units of blood and blood products, need for angiographic embolization or surgical management of hemorrhage, or maternal death
24 Thromboelastography and rotational thromboelastometry Thromboelastography (TEG) and rotational thromboelastometry (ROTEM), where available, can be useful for guiding plasma and coagulation product therapy. These tests provide a global assessment of hemostasis in whole blood (contributions from platelets, soluble coagulation factors, fibrinogen, fibrinolysis) and can be performed at the bedside, so results are available within minutes.
25 In nonpregnant patients, these values decline more rapidly than fibrinogen levels and can be useful for choosing specific blood components for transfusion and assessing the efficacy of interventions ; however, there is minimal information on use of the tests in pregnancy. In pregnancy, mean clot firmness and alpha angle (TEG) are larger, and clot time (ROTEM) and reaction time (TEG) are shorter. FIBTEM A5 <7 mm has been suggested as a trigger for administration of fibrinogen concentrate in the obstetric setting.
26 Before laboratory studies are available, we suggest transfusing 2 units of packed red blood cells (prbcs) if hemodynamics do not improve after the administration of 2 to 3 liters of normal saline, estimated blood loss is under 1500 ml, and continued bleeding is likely. In addition, aggressive use of plasma replacement is import.ant to reverse dilutional coagulopathy.
27
28
29
30
31

32
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH
 Unrestricted M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH Patients at imminent risk of exsanguination Manual aortic compression Resuscitative endovascular balloon occlusion of the aorta Uterine tourniquet
Unrestricted M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH Patients at imminent risk of exsanguination Manual aortic compression Resuscitative endovascular balloon occlusion of the aorta Uterine tourniquet
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification
 Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Pediatric massive transfusion protocols
 University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
Intraoperative haemorrhage and haemostasis. Dr. med. Christian Quadri Capoclinica Anestesia, ORL
 Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
EMSS17: Bleeding patients course material
 EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
Massive Transfusion. MPQC Spring Summit April 29, Roger Belizaire MD PhD
 Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Policy REVISED: 6/30/2016 3:30 PM. Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016
 Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
12/1/2009. Chapter 19: Hemorrhage. Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system Internal hemorrhage
 Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Maternal Collapse Guideline
 Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Major Haemorrhage Protocol. Commentary
 Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
BECLOT 500MG. INJECTION Composition : Each ml. contains : Tranexamic Acid I.P. 100mg.
 BECLOT 500MG. INJECTION Composition : Each ml. contains : Tranexamic Acid I.P. 100mg. DESCRIPTION Tranexamic acid is a synthetic analog of the amino acid lysine. It is used to treat or prevent excessive
BECLOT 500MG. INJECTION Composition : Each ml. contains : Tranexamic Acid I.P. 100mg. DESCRIPTION Tranexamic acid is a synthetic analog of the amino acid lysine. It is used to treat or prevent excessive
Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department
 Dr. Klara Vezendi Szeged University Transfusiology Department") Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department Disseminated intravascular coagulation (DIC, consumptive coagulopathy) is a clinicopathologic
Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department Disseminated intravascular coagulation (DIC, consumptive coagulopathy) is a clinicopathologic
Massive Transfusion Initiation & Implication
 Massive Transfusion Initiation & Implication Katayoun Fayaz MD Blood Bank Medical Director Northwell Health April 2017 Trauma Statistics/Facts Each year trauma accounts for 41 million emergency department
Massive Transfusion Initiation & Implication Katayoun Fayaz MD Blood Bank Medical Director Northwell Health April 2017 Trauma Statistics/Facts Each year trauma accounts for 41 million emergency department
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
Unit 5: Blood Transfusion
 Unit 5: Blood Transfusion Blood transfusion (BT) therapy: Involves transfusing whole blood or blood components (specific portion or fraction of blood lacking in patient). Learn the concepts behind blood
Unit 5: Blood Transfusion Blood transfusion (BT) therapy: Involves transfusing whole blood or blood components (specific portion or fraction of blood lacking in patient). Learn the concepts behind blood
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant. Lab Matters study day Oake Manor, Taunton, 8 th July 2015
 Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant Lab Matters study day Oake Manor, Taunton, 8 th July 2015 NPSA Rapid Response Report 2010 Transfusion of blood and blood components
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant Lab Matters study day Oake Manor, Taunton, 8 th July 2015 NPSA Rapid Response Report 2010 Transfusion of blood and blood components
Approach to disseminated intravascular coagulation
 Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
When Should I Use Tranexamic Acid for Children? Dr Andrea Kelleher Consultant Adult and Paediatric Cardiac Anaesthetist
 When Should I Use Tranexamic Acid for Children? Dr Andrea Kelleher Consultant Adult and Paediatric Cardiac Anaesthetist When? When a drug is licenced for (the proposed) use When its use is supported by
When Should I Use Tranexamic Acid for Children? Dr Andrea Kelleher Consultant Adult and Paediatric Cardiac Anaesthetist When? When a drug is licenced for (the proposed) use When its use is supported by
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Use of Condom tamponade to manage Massive Obstetric Hemorrhage at a tertiary centre in Rajasthan.
 Use of Condom tamponade to manage Massive Obstetric Hemorrhage at a tertiary centre in Rajasthan. INTRODUCTION: Conventionally PPH has been defined as blood loss of more than 500ml following vaginal delivery
Use of Condom tamponade to manage Massive Obstetric Hemorrhage at a tertiary centre in Rajasthan. INTRODUCTION: Conventionally PPH has been defined as blood loss of more than 500ml following vaginal delivery
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Section 3: Prevention and Treatment of AKI
 http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
NYU School of Medicine Department of Radiology Rotation-Specific House Staff Evaluation
 Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Shock, Hemorrhage and Thrombosis
 Shock, Hemorrhage and Thrombosis 1 Shock Systemic hypoperfusion due to: Reduction in cardiac output Reduction in effective circulating blood volume Hypotension Impaired tissue perfusion Cellular hypoxia
Shock, Hemorrhage and Thrombosis 1 Shock Systemic hypoperfusion due to: Reduction in cardiac output Reduction in effective circulating blood volume Hypotension Impaired tissue perfusion Cellular hypoxia
Prehospital Care Bundles
 Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Nitroglycerin and Heparin Drip Interfacility Protocols
 Nitroglycerin and Heparin Drip Interfacility Protocols EMS Protocol This protocol applies to nitroglycerin and Heparin drips that are initiated at the transferring facility prior to transport and are not
Nitroglycerin and Heparin Drip Interfacility Protocols EMS Protocol This protocol applies to nitroglycerin and Heparin drips that are initiated at the transferring facility prior to transport and are not
EDUCATIONAL COMMENTARY DISSEMINATED INTRAVASCULAR COAGULATION
 EDUCATIONAL COMMENTARY DISSEMINATED INTRAVASCULAR COAGULATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY DISSEMINATED INTRAVASCULAR COAGULATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
OBSTETRIC ADMISSION ORDERS 1 of 4
 OBSTETRIC ADMISSION 1 of 4 Actual Estimated Weight kg Actual Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART ADMIT TO: Labor and Delivery ( ) Check, circle and/or fill in all orders
OBSTETRIC ADMISSION 1 of 4 Actual Estimated Weight kg Actual Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART ADMIT TO: Labor and Delivery ( ) Check, circle and/or fill in all orders
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
CASE 5 - Toy et al. CASE FILES: Obstetrics & Gynecology
 z CASE 5 - Toy et al. CASE FILES: Obstetrics & Gynecology A 28-year-old woman is brought into the emergency room with a blood pressure of 60/40. The patient s husband states that she had 2 days of nausea
z CASE 5 - Toy et al. CASE FILES: Obstetrics & Gynecology A 28-year-old woman is brought into the emergency room with a blood pressure of 60/40. The patient s husband states that she had 2 days of nausea
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
anesthesia & mass casualty events
 anesthesia & mass casualty events marc p steurer, md, desa president, trauma anesthesiology society (www.tashq.org) director, trauma anesthesiology UCSF/ SFGH associate professor UCSF faculty disclosure
anesthesia & mass casualty events marc p steurer, md, desa president, trauma anesthesiology society (www.tashq.org) director, trauma anesthesiology UCSF/ SFGH associate professor UCSF faculty disclosure
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
What would be the response of the sympathetic system to this patient s decrease in arterial pressure?
 CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
SUMMARY OF PRODUCT CHARACTERISTICS
 SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Medsamic 100 mg/ml solution for injection 2. QUALITATIVE AND QUANTITATIVE COMPOSITION 1 ml contains: tranexamic acid 100 mg. For the
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Medsamic 100 mg/ml solution for injection 2. QUALITATIVE AND QUANTITATIVE COMPOSITION 1 ml contains: tranexamic acid 100 mg. For the
Septic shock. Babak Tamizi Far M.D Isfahan university of medical sciences
 Septic shock Babak Tamizi Far M.D Isfahan university of medical sciences Definitions Used to Describe the Condition of Septic Patients Approximately 750,000 cases of severe sepsis or septic shock occur
Septic shock Babak Tamizi Far M.D Isfahan university of medical sciences Definitions Used to Describe the Condition of Septic Patients Approximately 750,000 cases of severe sepsis or septic shock occur
Hematology Review. CCRN exam. The Coagulation Cascade. The Coagulation Cascade. Components include: Intrinsic pathway Extrinsic pathway Common pathway
 CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Inpatient care of polytrauma victims requires careful attention
 Special Feature Update of Inpatient Management of Polytrauma Patients Weinacker A, MD email: AWeinacker@stanfordmed.org Ann Weinacker, MD 1 Keywords: inpatient management of polytrauma patients, intensive
Special Feature Update of Inpatient Management of Polytrauma Patients Weinacker A, MD email: AWeinacker@stanfordmed.org Ann Weinacker, MD 1 Keywords: inpatient management of polytrauma patients, intensive
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Medical APMLE. Podiatry and Medical.
 Medical APMLE Podiatry and Medical http://killexams.com/exam-detail/apmle Question: 290 Signs and symptoms of hemolytic transfusion reactions include: A. Hypothermia B. Hypertension C. Polyuria D. Abnormal
Medical APMLE Podiatry and Medical http://killexams.com/exam-detail/apmle Question: 290 Signs and symptoms of hemolytic transfusion reactions include: A. Hypothermia B. Hypertension C. Polyuria D. Abnormal
Code Blue Caesarean at midnight!
 Code Blue Caesarean at midnight! Disclaimer / Pre-amble These cases have been de-identified to protect the identity of the patient and the treating teams. These are all real cases and real ROTEMs. The
Code Blue Caesarean at midnight! Disclaimer / Pre-amble These cases have been de-identified to protect the identity of the patient and the treating teams. These are all real cases and real ROTEMs. The
Bachelor of Chinese Medicine Shock
 BCM Year 2 Dr. Irene Ng Jan 28, 2003 9:30 am 1:00 pm Rm 004 UPB Bachelor of Chinese Medicine 2002 2003 Shock Learning objectives Be able to: know the definition of shock know the classification and causes
BCM Year 2 Dr. Irene Ng Jan 28, 2003 9:30 am 1:00 pm Rm 004 UPB Bachelor of Chinese Medicine 2002 2003 Shock Learning objectives Be able to: know the definition of shock know the classification and causes
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
1 Transfusion Medicine and Blood Bank Department, H. São João, Centro
 Original Article Interventional Algorithms for the Control of Coagulopathic Bleeding in Surgical, Trauma, and Postpartum Settings: Recommendations From the Share Network Group Clinical and Applied Thrombosis/Hemostasis
Original Article Interventional Algorithms for the Control of Coagulopathic Bleeding in Surgical, Trauma, and Postpartum Settings: Recommendations From the Share Network Group Clinical and Applied Thrombosis/Hemostasis
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
2 Liters. Goal: Basic Algorithm Volume Resuscitation in Trauma. Initial Fluids. Blood. Where do Blood Products Come From?
 Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
COMPANY CORE PACKAGE INSERT CCPI (PI/CORE/ENGLISH)
") COMPANY CORE PACKAGE INSERT CCPI (PI/CORE/ENGLISH) HUMAN ALBUMIN 20 % BEHRING Rev.: 05-MAR-2008 / PEI approval 26.02.08 Supersedes previous versions Rev.: 28-NOV-2007 / Adaptation to Core SPC Rev.: 02-JAN-2007
COMPANY CORE PACKAGE INSERT CCPI (PI/CORE/ENGLISH) HUMAN ALBUMIN 20 % BEHRING Rev.: 05-MAR-2008 / PEI approval 26.02.08 Supersedes previous versions Rev.: 28-NOV-2007 / Adaptation to Core SPC Rev.: 02-JAN-2007
Unit 11. Objectives. Indications for IV Therapy. Intravenous Access Devices & Common IV Fluids. 3 categories. Maintenance Replacement Restoration
 Unit 11 Fluids, Electrolytes and Acid Base Imbalances Intravenous Access Devices & Common IV Fluids Objectives Review the purpose and types of intravenous (IV) therapy. Recall the nursing care related
Unit 11 Fluids, Electrolytes and Acid Base Imbalances Intravenous Access Devices & Common IV Fluids Objectives Review the purpose and types of intravenous (IV) therapy. Recall the nursing care related
HEMODYNAMIC DISORDERS
 HEMODYNAMIC DISORDERS Normal fluid homeostasis requires vessel wall integrity as well as maintenance of intravascular pressure and osmolarity within certain physiologic ranges. Increases in vascular volume
HEMODYNAMIC DISORDERS Normal fluid homeostasis requires vessel wall integrity as well as maintenance of intravascular pressure and osmolarity within certain physiologic ranges. Increases in vascular volume
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Approach to bleeding disorders &treatment. by RAJESH.N General medicine post graduate
 Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acid base balance pregnancy-related changes to, 640 Acquired heart disease, 731 Acute fatty liver of pregnancy (AFLP), 618 Acute kidney
Index Note: Page numbers of article titles are in boldface type. A Acid base balance pregnancy-related changes to, 640 Acquired heart disease, 731 Acute fatty liver of pregnancy (AFLP), 618 Acute kidney
Pediatric Code Blue. Goals of Resuscitation. Focus Conference November Ensure organ perfusion
 Pediatric Code Blue Focus Conference November 2015 Duane C. Williams, MD Pediatric Critical Care Department of Pediatrics Children s Hospital of Richmond at VCU Goals of Resuscitation Ensure organ perfusion
Pediatric Code Blue Focus Conference November 2015 Duane C. Williams, MD Pediatric Critical Care Department of Pediatrics Children s Hospital of Richmond at VCU Goals of Resuscitation Ensure organ perfusion
Tranexamic acid, USP is a white crystalline powder. The aqueous solution for injection has a ph of 6.5 to 8.0.
 TRANEXAMIC ACID- tranexamic acid injection Cadila Healthcare Limited ---------- Tranexamic Acid Injection 100 mg/ml, 10 ml Antifibrinolytic agent Rx only DESCRIPTION Each ml of the sterile solution for
TRANEXAMIC ACID- tranexamic acid injection Cadila Healthcare Limited ---------- Tranexamic Acid Injection 100 mg/ml, 10 ml Antifibrinolytic agent Rx only DESCRIPTION Each ml of the sterile solution for
Bleeding and Shock. Circulatory System
 Bleeding and Shock Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to body tissues Delivers
Bleeding and Shock Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to body tissues Delivers
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Activated partial thromboplastin time abnormality, perioperative approach to, 104 105 Acute kidney injury, perioperative, 89 99 early
Index Note: Page numbers of article titles are in boldface type. A Activated partial thromboplastin time abnormality, perioperative approach to, 104 105 Acute kidney injury, perioperative, 89 99 early
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Specific Basic Standards for Osteopathic Fellowship Training in Pulmonary / Critical Care Medicine
 Specific Basic Standards for Osteopathic Fellowship Training in Pulmonary / Critical Care Medicine American Osteopathic Association and American College of Osteopathic Internists BOT Rev. 2/2011 These
Specific Basic Standards for Osteopathic Fellowship Training in Pulmonary / Critical Care Medicine American Osteopathic Association and American College of Osteopathic Internists BOT Rev. 2/2011 These
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
CSL Behring LLC Albuminar -25 US Package Insert Albumin (Human) USP, 25% Revised: 01/2008 Page 1
 USP, 25% Revised: 01/2008 Page 1") Page 1 CSL Behring Albuminar -25 Albumin (Human) USP, 25% R x only DESCRIPTION Albuminar -25, Albumin (Human) 25%, is a sterile aqueous solution of albumin obtained from large pools of adult human venous
Page 1 CSL Behring Albuminar -25 Albumin (Human) USP, 25% R x only DESCRIPTION Albuminar -25, Albumin (Human) 25%, is a sterile aqueous solution of albumin obtained from large pools of adult human venous
Blood products and plasma substitutes
 Blood products and plasma substitutes Plasma substitutes Dextran 70 and polygeline are macromolecular substances which are metabolized slowly; they may be used to expand and maintain blood volume in shock
Blood products and plasma substitutes Plasma substitutes Dextran 70 and polygeline are macromolecular substances which are metabolized slowly; they may be used to expand and maintain blood volume in shock
Intra-operative Effects of Cardiac Surgery Influence on Post-operative care. Richard A Perryman
 Intra-operative Effects of Cardiac Surgery Influence on Post-operative care Richard A Perryman Intra-operative Effects of Cardiac Surgery Cardiopulmonary Bypass Hypothermia Cannulation events Myocardial
Intra-operative Effects of Cardiac Surgery Influence on Post-operative care Richard A Perryman Intra-operative Effects of Cardiac Surgery Cardiopulmonary Bypass Hypothermia Cannulation events Myocardial
CLINICAL GUIDELINES ID TAG
 Title: Author: Speciality/ Division: Directorate: Date Uploaded: Review Date: September 2019 CG ID TAG CG0423 CLINICAL GUIDELINES ID TAG Clinical Guideline for Alteplase in intra-arterial thrombolysis
Title: Author: Speciality/ Division: Directorate: Date Uploaded: Review Date: September 2019 CG ID TAG CG0423 CLINICAL GUIDELINES ID TAG Clinical Guideline for Alteplase in intra-arterial thrombolysis
University of Wisconsin - Madison Cardiovascular Medicine Fellowship Program UW CICU Rotation Goals and Objectives
 Background: The field of critical care cardiology has evolved considerably over the past 2 decades. Contemporary critical care cardiology is increasingly focused on the management of patients with advanced
Background: The field of critical care cardiology has evolved considerably over the past 2 decades. Contemporary critical care cardiology is increasingly focused on the management of patients with advanced
ST Elevation Myocardial Infarction (STEMI) Reperfusion Order Set
 Reperfusion Order Set") Form Title Form Number CH-0454 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The license does not
Form Title Form Number CH-0454 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The license does not
GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS
 GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS 1.0 Definitions & Acronyms 1.1 Massive Hemorrhage Event (MHE): Transfusion of a volume of blood components equivalent to a patient s estimated
GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS 1.0 Definitions & Acronyms 1.1 Massive Hemorrhage Event (MHE): Transfusion of a volume of blood components equivalent to a patient s estimated
FISTULA CARE. FISTULA TREATMENT COMPLICATIONS: Reporting Guidelines. Updated 12/12/12
 FISTULA CARE FISTULA TREATMENT COMPLICATIONS: Reporting Guidelines Updated 12/12/12 EngenderHealth, 440 Ninth Avenue, New York, NY 10001, USA Telephone: 212-561-8000; Fax: 212-561-8067; E-mail: fistulacare@engenderhealth.org
FISTULA CARE FISTULA TREATMENT COMPLICATIONS: Reporting Guidelines Updated 12/12/12 EngenderHealth, 440 Ninth Avenue, New York, NY 10001, USA Telephone: 212-561-8000; Fax: 212-561-8067; E-mail: fistulacare@engenderhealth.org
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Coagulopathy: Measuring and Management. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe