Vascular a ccess access for Dialysis a surgeon s perspecti e v. some observations
|
|
|
- Sheila May
- 5 years ago
- Views:
Transcription
1 Vascular access for Dialysis a surgeon s perspective e. some observations
2
3 Age of New Haemodialysis Patients 2005 Australia Number (Total=1957) 0.7% 3% 5% 10% 15% 20% 26% 19% 2% >=85 No. Pats
4 Method and Location of Dialysis Number of Patients t 5000 SAT HD 3629 (43%) HOSP HD 2289 (27%) CAPD 1027 (12%) HOME HD 799 (9%) APD 784 (9%)
5 RPAH Waiting time for Kidney Transplant in 2006 (n=69) Deceased Donor Living Donor Pre- Emptive 1m-1yr 1-2yr 2-3yr 3-4yr 4-5yr >5yr
6 Stock and Flow of Haemodialysis Patients Number of Patients New Patients Transplants Perm. Transfer Deaths No. Dialysing 6717 Patients t
7 Pr robability of surviv val Patient Survival - HD at 90 days Censored for Transplant Australia (1907) (2462) (3156) (3506) Years
8 CRF in Australia 1. Number of kidney failure patients in Australia could triple 2. Dialysis patient number increasing by 7% per year 3. 47% of new patients are over 65 years old 4. Commonest treatment option is satellite haemodialysis 5. Transplantation is not a viable option for most patients 6. Haemodialysis is the commonest long term treatment 7. Death is commonest endpoint 50% at 5 years
9 Long term reliable vascular access 1. Demonstrate why AVF are better than AVG 2. Ask who are the decision makers for choice of vascular access? 3. The role of central venous catheters? 4. A plan for maximising AVF 5. Surveillance of AVF 6. Home versus satellite haemodialysis
10 K Polkinghorne/ANZDATA 2003
11 Association of Angioaccess and Mortality Haz zard Rat tio Ref < (2528) (402) (129) (28) AV Native AV Synthetic Tunnelled CV Catheter Type of Angioaccess Non-Tunnelled CV Catheter K Polkinghorne/ANZDATA 2003
12 Access Intervention in Previous Twelve Months - December 2005 n = Number of Patients Revision of Access Declotting of Access AVF AVG CVC AVF AVG CVC Australia n= % 35% 18% 5% 26% 14% Diabetics n= % 41% 17% 6% 29% 13% F emale n= % 35% 18% 6% 25% 15% AVG in 2005 were: 1. five times more likely to clot 2. three times more likely to require revision 3. less satisfactory than central venous catheters
13 Type of Access for Haemodialysis Australia December 2005 CVC AVG AVF 76% 74% 77% Only significant factors correlating with use of AVG are length of time 67% 82% on dialysis and the HD centre 12% 10% 13% 18% 9% All Pts Diabetic Non Diab Female Male (n=6717) (n=1660) (n=5057) (n=2672) (n=4045)
14 2003 Western Australia AVG 12% Catheters 18% 9% 3% Northern Territory AVG 6% Catheters 6% 8% Queensland AVG 16% Catheters 10% South Australia AVG 6% Catheters 4% New South NSW 20% Wales/ACT 10% AVG 30% Catheters 7% ACT 36% Victoria AVG 9% Catheters 8% 8% 8% Tasmania AVG 1% Catheters 20%
15 Mode of HAEMODIALYSIS NSW December NSW TEMP CVC Synthetic Native L'POO OOL WEST NSW STG TGH WGN GNG NEW EWC RPA/CO CON RNSH percent
16 First Haemodialysis Access Initial RRT By Referral - Australia Perce entage Non-Tunnel CVC Tunnel CVC AVG AVF Mar 04 Dec 05 Dec 04 Early Late 1 8 Dec 04 Mar 04 Dec 05
17 Mode of INITIAL vascular access NSW in perce ent 60 TEMP 40 CVC Synthetic 20 Native 0 WEST L'POOL WGNG NSW NSW NEWC RNSH RPA/CON
18 h th d isi k s f h i who are the decision makers for choice of vascular access in your hospital?
19 Decision i makers 1. Nephrologist 2. Patient t 3. Patient s family 4. Dialysis nursing staff 5. Vascular surgeon time ease of surgery $$$
20
21
22 Central Venous Catheters temporary late presentation, BMI>35 and female necessary for bridging to native or synthetic AVF high complication rate thrombosis insertion? where and when? long term solution
23 Central Venous Catheters










24 Imaging of the IJV
25
26 Non-tunneled CVCs avoid use in neck






27 Positioning CVC junction of SVC and right atrium in sitting position risk of thrombosis right atrium
28 SVC obstruction - mechanical injury to SVC
29 Biofilm inevitable it and on outer side of catheter t - not tin the lumen. Bacteria adhere with source being at time of insertion or circulating organisms at any time thereafter. Usually S. aureus or S. epidermidis and therefore skin source. Patient to patient spread of staphylococcus demonstrated by?? Lab technique identification and therefore implication dialysis nursing staff and not patient source. Multiple options for catheter locking solutions. Need for perhaps p determined by Catheter Related Bacteraemia rate (events/1,000 catheter days). If CRB rate low, randomised trials have difficulty showing advantages over heparin alone. Centres should monitor CRB rates should be about 2/1,000 days. RCTs show Gentamicin to best at lowering CRB rate but antibiotic resistance rate unacceptable. Next best is. with 4% citrate. Not available in Australia ampoule worth about 12 Euro.
30 Long term reliable vascular access 1. Demonstrate why AVF are better than AVG 2. Ask who are the decision makers for choice of vascular access? 3. The role of central venous catheters? 4. A plan for maximising AVF 5. Surveillance of AVF 6. Home versus satellite haemodialysis
31 FISTULA FIRST National Vascular Access Improvement Initiative initiative to increase AVF prevalence started Northwest network in 2003 aim for 50% AVF
32 The team approach 1. Designate staff member in dialysis facility (RN if feasible) responsible for vascular access 2. Assemble multi-disciplinary vascular access team 3. Representatives of all key disciplines including access surgeons, ultrasonographers and interventionalists. 4. Investigate and track all non-avf access placements, and AVF failures 5. Benchmark against others
33 Referral 1. Nephrologist/skilled nurse performs appropriate evaluation and physical exam prior to surgery referral. 2. Nephrologist refers for vessel mapping where feasible, prior to surgery referral. 3. Nephrologist refers patients to surgeons for AVF only evaluation. Surgery scheduled with sufficient lead-time for AVF maturation. 4. Nephrologist defines AVF expectations to surgeon
34






35
36 Vascular access surgeon Nephrologists refer to surgeons willing and able to meet the standards and expectations. Surgeons utilize current techniques for AVF placement including vein transposition. Surgeons ensure mapping is performed for any patient t not clearly suitable for AVF based only on physical exam. Surgeons are evaluated on frequency, quality and patency of access placements. Surgeons work with nephrologists to plan for and place secondary AVFs in suitable AV graft patients.
37 AV grafts to AVF evaluate and identify every AV graft patient for possible secondary AV fistula conversion, and document the plan in the patient s t record. examine outflow vein of all graft patients with sleeves up during dialysis treatments (minimum frequency, monthly). refer to surgeon for placement of secondary AVF before failure of AVG.
38 Cannulation Facility uses best cannulators and best teaching tools. Dialysis staff use specific protocols for initial dialysis treatments Assign the most skilled staff to patients with new AVFs Facility offers option of self-cannulation to patients who are interested and able.
39 Surveillance Facilities adopt standard procedures for monitoring, surveillance, and timely referral for the failing AVF. Nephrologists, interventional radiologists, and surgeons adopt standard criteria, and a plan for each patient Review data monthly or quarterly in facility staff meetings. Present and evaluate data trended over time





40 ? experience of surgeon
41
42 Obese patients
43
44
45 AVF vs AVG Saphenous vein loops unpopular because of aneurysms and stenoses. Large numbers of brachiocephalic and brachiobasilic AVF (latter performed as two stage procedure). For example, 70% of native vein AVF were in upper arm in large and recent series from University it of Miami. i Same trend in Europe. Upper arm fistulae associated with high flows and cephalic arch stenoses interesting relationship between these two problems, particularly with respect to dilation and effect cardiac output. High venous return pressures can be a result of high flow. See later discussion on flow monitoring.
46 Brachiocephalic fistula
47 Surveillance of fistulae 1. Improve patient care reliability and predictability of access prolong and preserve access vessels 2. Reduce access related costs morbidity related home haemodialysis
48










49 sleeves up and arm up
50
51
52 Movie 1340
53 Movie 1347
54 Movie 1344
55
56
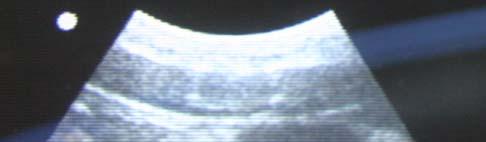
57
58







59


60 Venous hypertension
61 Whilst on dialysis Ease of cannulation Ability to rotate cannulation points Arterial inflow pressures Pump speed Venous return pressures Decannulation bleeding times






62
63 Distribution of Blood Flow Rates Number of Patients 5000 Mar 2004 (5924) Dec 2004 (6206) Dec 2005 (6717) Australia >=400 mls/min
64 Ultrasound
65
66
67
68
69 dysfunction hypothesis Fistula stenosis causes graft dysfunction and dysfunction precedes and accurately predicts thrombosis Surveillance relies on:- 1. Reproducible measurements 2. Stenosis progressing slowly 3. Other factors such as hypercoagulability, low BP etc do not influence 4. Correlation with clinical examination
70 a must get!








71 Digital Ischaemia incidence 1 3% invariably diabetic patient radial = brachial incidence treat by banding or ligation DRIL procedure
72
73 Surveillance recommendations 1. High quality and continuous clinical assessment 2. Initial ultrasound assessment dialysis nurse driven 3. Early intervention
74 Mr T
75
76 5. Cannulation techniques Description three cannulation techniques: rope ladder or snail track for AVGs and good veins provided aneurysms do not develop in latter area technique which is prone to aneurysm formation, particularly in high flow fistulae button hole which I now have a very revised and more positive appreciation of. Should not be confused with area cannulation technique. button hole is a very precise technique and very operator dependent. Preparation and angle of entry very important, initially with sharp needles. Nursing recommendation that it be employed by limited number of staff for a given patient. No nurse should cannulate ate a given fistula without having witnessed another with knowledge of that given fistula.
77 educated smiling home HD patient
78
CHAPTER 5. Haemodialysis. Kevan Polkinghorne Hannah Dent Aarti Gulyani Kylie Hurst Stephen McDonald
 CHAPTER Haemodialysis Kevan Polkinghorne Hannah Dent Aarti Gulyani Kylie Hurst Stephen McDonald STOCK AND FLOW AUSTRALIA The annual stock and flow of HD patients during the period - is shown in Figures.,.
CHAPTER Haemodialysis Kevan Polkinghorne Hannah Dent Aarti Gulyani Kylie Hurst Stephen McDonald STOCK AND FLOW AUSTRALIA The annual stock and flow of HD patients during the period - is shown in Figures.,.
Introduction to the Native Arteriovenous Fistula: A primer for medical students and radiology residents
 Introduction to the Native Arteriovenous Fistula: A primer for medical students and radiology residents Jesus Contreras, D.O. PGY-4 John Yasmer, D.O. Department of Radiology No Disclosures Objectives Introduce
Introduction to the Native Arteriovenous Fistula: A primer for medical students and radiology residents Jesus Contreras, D.O. PGY-4 John Yasmer, D.O. Department of Radiology No Disclosures Objectives Introduce
AMMAR SERAWAN, MD. Ain Wzain Hospital. April 21, 2012 Vascular Access Study Workshop
 AMMAR SERAWAN, MD Ain Wzain Hospital April 21, 2012 Vascular Access Study Workshop 1 Inspection for signs of: - infection (redness, discharge, edema) -aneurysms (may be cannulated using the lateral side
AMMAR SERAWAN, MD Ain Wzain Hospital April 21, 2012 Vascular Access Study Workshop 1 Inspection for signs of: - infection (redness, discharge, edema) -aneurysms (may be cannulated using the lateral side
Vascular Access for Haemodialysis. Mike Stephens
 Vascular Access for Haemodialysis Mike Stephens Overview Learning Objectives History and development of vascular access Standards in vascular access surgery Types of vascular access Complications Objectives
Vascular Access for Haemodialysis Mike Stephens Overview Learning Objectives History and development of vascular access Standards in vascular access surgery Types of vascular access Complications Objectives
Sichol sooksee,rn. Hemodialysis Unit Rajavej Chiang Mai Hospital
 Sichol sooksee,rn. Hemodialysis Unit Rajavej Chiang Mai Hospital Button hole or Ladder?? Vascular Access Cannulation It s a Life Line of Hemodialysis patient Arterio-venous fistula(avf) is the K/DOQI
Sichol sooksee,rn. Hemodialysis Unit Rajavej Chiang Mai Hospital Button hole or Ladder?? Vascular Access Cannulation It s a Life Line of Hemodialysis patient Arterio-venous fistula(avf) is the K/DOQI
Technical and Clinical Barriers to Implementing an Optimal Case Mix of Vascular Access
 Technical and Clinical Barriers to Implementing an Optimal Case Mix of Vascular Access Louise Moist Associate Professor Lead Vascular Access Ontario Renal Network Schulich School of Medicine University
Technical and Clinical Barriers to Implementing an Optimal Case Mix of Vascular Access Louise Moist Associate Professor Lead Vascular Access Ontario Renal Network Schulich School of Medicine University
ASDIN 7th Annual Scientific Meeting
 Strategies for Decreasing the Use of Hemodialysis Catheters ASDIN 7 th Annual Scientific Meeting Outline Late referral Primary failure Why Not PD? Summary Micah Chan MD MPH FACP Assistant Professor of
Strategies for Decreasing the Use of Hemodialysis Catheters ASDIN 7 th Annual Scientific Meeting Outline Late referral Primary failure Why Not PD? Summary Micah Chan MD MPH FACP Assistant Professor of
Medical Director/Surgeon as Partners WebEx February 11, 2010
 Medical Director/Surgeon as Partners WebEx February 11, 2010 Over 400,000 patients are treated yearly for ESRD in the USA; 60% of these patients receive some form of hemodialysis Despite major advances
Medical Director/Surgeon as Partners WebEx February 11, 2010 Over 400,000 patients are treated yearly for ESRD in the USA; 60% of these patients receive some form of hemodialysis Despite major advances
CATHETER REDUCTION. Angelo N. Makris, M.D. Medical Director Chicago Access Care
 CATHETER REDUCTION Angelo N. Makris, M.D. Medical Director Chicago Access Care Objectives Discuss tools/techniques proven to improve AVF rates & decrease catheter rates Implement a change process in your
CATHETER REDUCTION Angelo N. Makris, M.D. Medical Director Chicago Access Care Objectives Discuss tools/techniques proven to improve AVF rates & decrease catheter rates Implement a change process in your
Evaluation of AVF and AVG
 Evaluation of AVF and AVG 2013 Nephrology Nursing Symposium Albuquerque Vascular Access Leading cause of hospitalization in the ESRD population Annual cost approaching $1.5 billion (USRDS, 2004) Current
Evaluation of AVF and AVG 2013 Nephrology Nursing Symposium Albuquerque Vascular Access Leading cause of hospitalization in the ESRD population Annual cost approaching $1.5 billion (USRDS, 2004) Current
UPDATE IN VASCULAR ACCESS Mercedeh Kiaii MD FRCPC Rick Luscombe RN BSN CNeph(C) Elizabeth Lee MD FRCPC
 Elizabeth Lee MD FRCPC") UPDATE IN VASCULAR ACCESS Mercedeh Kiaii MD FRCPC Rick Luscombe RN BSN CNeph(C) Elizabeth Lee MD FRCPC Background Endovascular AVF Outline Data from FLEX and NEAT study SPH data Clinical experience Cannulation
UPDATE IN VASCULAR ACCESS Mercedeh Kiaii MD FRCPC Rick Luscombe RN BSN CNeph(C) Elizabeth Lee MD FRCPC Background Endovascular AVF Outline Data from FLEX and NEAT study SPH data Clinical experience Cannulation
PREVENTION AND TREATMENT OF ANEURYSMS OF AUTOGENOUS DIALYSIS ACCESSES STEPHEN L. HILL, M.D.,F.A.C.S
 PREVENTION AND TREATMENT OF ANEURYSMS OF AUTOGENOUS DIALYSIS ACCESSES STEPHEN L. HILL, M.D.,F.A.C.S THE INCREASE IN THE CONSTRUCTION OF AUTOGENOUS FISTULAE OVER THE PAST TEN YEARS HAS BROUGHT WITH IT 1.
PREVENTION AND TREATMENT OF ANEURYSMS OF AUTOGENOUS DIALYSIS ACCESSES STEPHEN L. HILL, M.D.,F.A.C.S THE INCREASE IN THE CONSTRUCTION OF AUTOGENOUS FISTULAE OVER THE PAST TEN YEARS HAS BROUGHT WITH IT 1.
ASDIN 8th Annual Scientific Meeting
 Fistula First Breakthrough Initiative Fistula First Breakthrough Initiative Marianne Neumann, RN, CNN FFBI Clinical Lead New Orleans, LA February 26, 2012 Initiated in 2003 by CMS, Goals Include: to ensure
Fistula First Breakthrough Initiative Fistula First Breakthrough Initiative Marianne Neumann, RN, CNN FFBI Clinical Lead New Orleans, LA February 26, 2012 Initiated in 2003 by CMS, Goals Include: to ensure
Why Can't I Cannulate This Fistula? Fistula Immaturity: The Simple But Critical Steps for a Functioning (Mature) AVF
 AVF") Why Can t I Cannulate This Access? Steven J. Bander M.D. Adjunct Professor of Nephrology St. Louis University Director, Vascular Access Center, St. Luke s Hospital Saint Louis, MO Why Can't I Cannulate
Why Can t I Cannulate This Access? Steven J. Bander M.D. Adjunct Professor of Nephrology St. Louis University Director, Vascular Access Center, St. Luke s Hospital Saint Louis, MO Why Can't I Cannulate
Sid Bhende MD Sentara Vascular Specialists April 28 th Dialysis Access Review: Understanding the Access Options our Patients Face
 Sid Bhende MD Sentara Vascular Specialists April 28 th 2018 Dialysis Access Review: Understanding the Access Options our Patients Face Disclosures Dialysis Background Why is it important? Outline National
Sid Bhende MD Sentara Vascular Specialists April 28 th 2018 Dialysis Access Review: Understanding the Access Options our Patients Face Disclosures Dialysis Background Why is it important? Outline National
What s on the Horizon in Dialysis Access? Libby Watch, MD, FACS Miami Cardiac & Vascular Institute
 What s on the Horizon in Dialysis Access? Libby Watch, MD, FACS Miami Cardiac & Vascular Institute Disclosures No relevant disclosures Employee Advanced Access Care Dialysis Work 5 operating surgeons 3
What s on the Horizon in Dialysis Access? Libby Watch, MD, FACS Miami Cardiac & Vascular Institute Disclosures No relevant disclosures Employee Advanced Access Care Dialysis Work 5 operating surgeons 3
Vascular access. The KidneyCare Audit
 Vascular access The KidneyCare Audit Renal National Service Framework The challenge of vascular access Standard 3 All children, young people and adults with established renal failure are to have timely
Vascular access The KidneyCare Audit Renal National Service Framework The challenge of vascular access Standard 3 All children, young people and adults with established renal failure are to have timely
Vascular Access Options for Apheresis Medicine
 Vascular Access Options for Apheresis Medicine Josh King, MD Divisions of Nephrology and Medical Toxicology University of Virginia September 21, 2018 Disclosure I have no personal or professional financial
Vascular Access Options for Apheresis Medicine Josh King, MD Divisions of Nephrology and Medical Toxicology University of Virginia September 21, 2018 Disclosure I have no personal or professional financial
Distal Hypoperfusion Ischemic Syndrome (DHIS)
") Pathophysiology Traditional View ( Steal Syndrome ) Distal Hypoperfusion Ischemic Syndrome (DHIS) Steven Wu, MD Director of Interventional Nephrology Massachusetts General Hospital Harvard Medical School
Pathophysiology Traditional View ( Steal Syndrome ) Distal Hypoperfusion Ischemic Syndrome (DHIS) Steven Wu, MD Director of Interventional Nephrology Massachusetts General Hospital Harvard Medical School
CHAPTER 4 METHOD AND LOCATION OF DIALYSIS. Nancy Briggs Kylie Hurst Stephen McDonald Annual Report 35th Edition
 CHAPTER 4 METHOD AND LOCATION OF DIALYSIS Nancy Briggs Kylie Hurst Stephen McDonald 212 Annual Report 35th Edition METHOD AND LOCATION OF DIALYSIS ANZDATA Registry 212 Report AUSTRALIA Figure 4.1 Aust
CHAPTER 4 METHOD AND LOCATION OF DIALYSIS Nancy Briggs Kylie Hurst Stephen McDonald 212 Annual Report 35th Edition METHOD AND LOCATION OF DIALYSIS ANZDATA Registry 212 Report AUSTRALIA Figure 4.1 Aust
HD Scanning: Velocities and Volume Flow
 HD Scanning: Velocities and Volume Flow Non-Invasive Lab Symposium West Orange, NJ April 27, 2018 Volume Flow Cindy Sturt, MD, FACS, RVT 500,000 Americans on dialysis 20-25% annual mortality 65% 5 year
HD Scanning: Velocities and Volume Flow Non-Invasive Lab Symposium West Orange, NJ April 27, 2018 Volume Flow Cindy Sturt, MD, FACS, RVT 500,000 Americans on dialysis 20-25% annual mortality 65% 5 year
Vascular Access Care Plans: How Can a Care Plan Really Improve Care and Make Everyone s Job Easier?
 Vascular Access Care Plans: How Can a Care Plan Really Improve Care and Make Everyone s Job Easier? Plan the Work Work the Plan What is a plan? A method for achieving an end An orderly arrangement of parts
Vascular Access Care Plans: How Can a Care Plan Really Improve Care and Make Everyone s Job Easier? Plan the Work Work the Plan What is a plan? A method for achieving an end An orderly arrangement of parts
Selection of Permanent Hemodialysis Vascular Access
 Selection of Permanent Hemodialysis Vascular Access TABLE OF CONTENTS 1.0 Scope...1 2.0 Recommendations & Rationale... 2 3.0 References... 3 4.0 Sponsors... 9 5.0 Effective Date... 10 Appendix 1: Key Elements
Selection of Permanent Hemodialysis Vascular Access TABLE OF CONTENTS 1.0 Scope...1 2.0 Recommendations & Rationale... 2 3.0 References... 3 4.0 Sponsors... 9 5.0 Effective Date... 10 Appendix 1: Key Elements
Dr. Murty Mantha MD FRACP Cairns Base Hospital Cairns. DNT 2011 Hunter Valley
 Dr. Murty Mantha MD FRACP Cairns Base Hospital Cairns DNT 2011 Hunter Valley Approximately 45% of AVF are functional without intervention after creation The procedure rate is 1.45-3.3 procedures/avf
Dr. Murty Mantha MD FRACP Cairns Base Hospital Cairns DNT 2011 Hunter Valley Approximately 45% of AVF are functional without intervention after creation The procedure rate is 1.45-3.3 procedures/avf
Vascular Access for Patients affected by non Renal Disorders. Eric S Chemla St George s vascular Institute London UK
 Vascular Access for Patients affected by non Renal Disorders Eric S Chemla St George s vascular Institute London UK Disclosures Gore Covidien Maquet Proteon Therapeutics INTRODUCTION I First fistula in
Vascular Access for Patients affected by non Renal Disorders Eric S Chemla St George s vascular Institute London UK Disclosures Gore Covidien Maquet Proteon Therapeutics INTRODUCTION I First fistula in
Vascular Access Study Overview and Implementation
 Vascular Access Study Overview and Implementation Salim Kabalan, MD Co-Principal Investigator Hafez Elzein, MD, MS Managing Director April 21, 2012 Investigator Meeting & Workshop Introduction Majority
Vascular Access Study Overview and Implementation Salim Kabalan, MD Co-Principal Investigator Hafez Elzein, MD, MS Managing Director April 21, 2012 Investigator Meeting & Workshop Introduction Majority
UC SF. End Stage Renal Disease. National Kidney Foundation Dialysis Outcomes Quality Initiative (K/DOQI) BUT-- No Cephalic Vein What s Next
 BUT-- No Cephalic Vein What s Next") No Cephalic Vein What s Next End Stage Renal Disease Charles Eichler MD Clinical Professor of Surgery Division of Vascular Surgery UCSF April 5, 2014 Population of patients with ESRD growing rapidly -
No Cephalic Vein What s Next End Stage Renal Disease Charles Eichler MD Clinical Professor of Surgery Division of Vascular Surgery UCSF April 5, 2014 Population of patients with ESRD growing rapidly -
St George Hospital Renal Department Internal Only
 RENAL VASCULAR ACCESS CANNULATION POLICY AND PROCEDURE SUMMARY: A functioning arteriovenous fistula (AVF) or arteriovenous graft (AVG) is paramount in the maintenance of regular and optimal haemodialysis
RENAL VASCULAR ACCESS CANNULATION POLICY AND PROCEDURE SUMMARY: A functioning arteriovenous fistula (AVF) or arteriovenous graft (AVG) is paramount in the maintenance of regular and optimal haemodialysis
Cannulation Techniques Webinar
 Cannulation Techniques Webinar March 28, 2012 ESRD Network of Texas Lynda K. Ball, MSN, RN, CNN Objectives Discuss assessment skills inspection, palpation, and auscultation of an AV fistula to determine
Cannulation Techniques Webinar March 28, 2012 ESRD Network of Texas Lynda K. Ball, MSN, RN, CNN Objectives Discuss assessment skills inspection, palpation, and auscultation of an AV fistula to determine
It is important to learn all you can about your access so you can take better care of yourself.
 PEP CONNECT PEP Talk Outline Topic Vascular Access P A T I E N T E D U C A T I O N P R O G R A M An adequate permanent vascular access is the key to living long and well on dialysis. There are three kinds
PEP CONNECT PEP Talk Outline Topic Vascular Access P A T I E N T E D U C A T I O N P R O G R A M An adequate permanent vascular access is the key to living long and well on dialysis. There are three kinds
Victoria Chapman BS, RN, HP (ASCP)
") Victoria Chapman BS, RN, HP (ASCP) Considerations: Age Sex Body Composition Hydration Status Chemotherapy Use Access History Considerations: Immunosuppression Use Chemotherapy Frequency of plasma exchanges
Victoria Chapman BS, RN, HP (ASCP) Considerations: Age Sex Body Composition Hydration Status Chemotherapy Use Access History Considerations: Immunosuppression Use Chemotherapy Frequency of plasma exchanges
Case #1. Case #1- Possible codes. Unraveling the -59 modifier. Principles of Interventional. CASE 1: Simple angioplasty
 Unraveling the -59 modifier Principles of Interventional Coding Donald Schon, MD, FACP Debra Lawson, CPC, PCS Distinct or independent from other services performed on the same day Normally not reported
Unraveling the -59 modifier Principles of Interventional Coding Donald Schon, MD, FACP Debra Lawson, CPC, PCS Distinct or independent from other services performed on the same day Normally not reported
Nursing Care of the Dialysis Patient. Adrian Hordon, MSN, RN
 Nursing Care of the Dialysis Patient Adrian Hordon, MSN, RN Understand principles of hemodialysis Recognize different access ports Identify side effects and complications Discuss nursing care for pre and
Nursing Care of the Dialysis Patient Adrian Hordon, MSN, RN Understand principles of hemodialysis Recognize different access ports Identify side effects and complications Discuss nursing care for pre and
Fistula/Graft Protection. Leslie Dork Renal Medicine Associates
 + Fistula/Graft Protection Leslie Dork Renal Medicine Associates + Disclaimer Renal Medicine Associates employee I have no conflicts of interest. + Access failure Infections Infiltrations Stenoses/Thrombosis
+ Fistula/Graft Protection Leslie Dork Renal Medicine Associates + Disclaimer Renal Medicine Associates employee I have no conflicts of interest. + Access failure Infections Infiltrations Stenoses/Thrombosis
CHAPTER 12 END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND. Stephen McDonald. Matthew Jose. Kylie Hurst INDIGENOUS 12-1
 ANZDATA Registry 213 Report INDIGENOUS END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND CHAPTER 12 Stephen McDonald Matthew Jose Kylie Hurst 213 Annual Report - 36th Edition
ANZDATA Registry 213 Report INDIGENOUS END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND CHAPTER 12 Stephen McDonald Matthew Jose Kylie Hurst 213 Annual Report - 36th Edition
Pitfalls in pushing fistulas ----
 Pitfalls in pushing fistulas ---- An argument for more grafts Marc Webb, MD, FACS Michigan Vascular Access, PC March 27 th, 2009 Vascular Access for Hemodialysis ------- Basic facts - the need for Access
Pitfalls in pushing fistulas ---- An argument for more grafts Marc Webb, MD, FACS Michigan Vascular Access, PC March 27 th, 2009 Vascular Access for Hemodialysis ------- Basic facts - the need for Access
7/7/2015. Objectives. Pros and Cons of Buttonhole Cannulation
 Objectives Pros and Cons of Buttonhole Cannulation Charmaine Lok, MD, FRCPC, MSc University of Toronto Toronto General Hospital To gain an appreciation of the importance of proper vascular access cannulation
Objectives Pros and Cons of Buttonhole Cannulation Charmaine Lok, MD, FRCPC, MSc University of Toronto Toronto General Hospital To gain an appreciation of the importance of proper vascular access cannulation
Does cannulation technique impact arteriovenous fistula and graft survival? Maria Teresa Parisotto CANNT 2017 Halifax October 20 th, 2017
 Does cannulation technique impact arteriovenous fistula and graft survival? Maria Teresa Parisotto CANNT 2017 Halifax October 20 th, 2017 Survival Preserving the AVF as the patient lifeline: reduced mortality
Does cannulation technique impact arteriovenous fistula and graft survival? Maria Teresa Parisotto CANNT 2017 Halifax October 20 th, 2017 Survival Preserving the AVF as the patient lifeline: reduced mortality
Acceptance onto dialysis guidelines: St George Hospital
 Acceptance onto dialysis guidelines: St George Hospital The following information is a guideline to support clinicians in decision making regarding acceptance onto dialysis. A review of international guidelines
Acceptance onto dialysis guidelines: St George Hospital The following information is a guideline to support clinicians in decision making regarding acceptance onto dialysis. A review of international guidelines
2006 NKF-DOQI Guidelines Preferred Vascular Access Order 1. Radiocephalic (wrist) fistula 2. Brachiocephalic (elbow) fistula 3. Basilic vein transposi
 fistula 2. Brachiocephalic (elbow) fistula 3. Basilic vein transposi") Stage 5 Chronic Kidney Disease Assessing the Results of AV Access: Realistic Outcomes in 2009 Sean P. Roddy, MD Albany, NY Defined as a GFR
Stage 5 Chronic Kidney Disease Assessing the Results of AV Access: Realistic Outcomes in 2009 Sean P. Roddy, MD Albany, NY Defined as a GFR
Interventions for AV-Shunt stenosis: What works best PTA, Stent or DCB?
 Interventions for AV-Shunt stenosis: What works best PTA, Stent or DCB? Martin Forlee Vascular Surgeon Cape Town Disclosure Speaker name: Martin Forlee I have the following potential conflicts of interest
Interventions for AV-Shunt stenosis: What works best PTA, Stent or DCB? Martin Forlee Vascular Surgeon Cape Town Disclosure Speaker name: Martin Forlee I have the following potential conflicts of interest
Novel solutions for access challenges
 Novel solutions for access challenges Mr James Gilbert Consultant Transplant & Vascular Access Surgeon Disclosures I have the following potential conflicts of interest to report: I currently hold a consultancy
Novel solutions for access challenges Mr James Gilbert Consultant Transplant & Vascular Access Surgeon Disclosures I have the following potential conflicts of interest to report: I currently hold a consultancy
AV ACESS COMPLICATIONS. Ass. Prof. Dr. Habas
 AV ACESS COMPLICATIONS Ass. Prof. Dr. Habas COMPLICATION AVF IS CONSIDERED A MINOR PROCEDURE INCIDENCE OF COMPLICATION- 20-27% MANY A COMPLICATION LEADS TO FAILURE OF FISTULA LOSS OF SITE AND VEIN FOR
AV ACESS COMPLICATIONS Ass. Prof. Dr. Habas COMPLICATION AVF IS CONSIDERED A MINOR PROCEDURE INCIDENCE OF COMPLICATION- 20-27% MANY A COMPLICATION LEADS TO FAILURE OF FISTULA LOSS OF SITE AND VEIN FOR
End Stage Kidney Disease Among Indigenous Peoples of Australia and New Zealand
 Chapter 12 End Stage Kidney Disease Among Indigenous Peoples of and New Zealand 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, rates of end-stage kidney disease
Chapter 12 End Stage Kidney Disease Among Indigenous Peoples of and New Zealand 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, rates of end-stage kidney disease
BUTTONHOLE CANNULATION
 BUTTONHOLE CANNULATION What is a Buttonhole? Technique in which an AV fistula is cannulated in the exact same spot, at the same angle and at the same depth of penetration every time. Benefits Reduction
BUTTONHOLE CANNULATION What is a Buttonhole? Technique in which an AV fistula is cannulated in the exact same spot, at the same angle and at the same depth of penetration every time. Benefits Reduction
IN.PACT AV Access IDE Study Full Baseline Data. Robert Lookstein, MD MHCDL New York, NY On Behalf of the IN.PACT AV ACCESS Investigators
 IN.PACT AV Access IDE Study Full Baseline Data Robert Lookstein, MD MHCDL New York, NY On Behalf of the IN.PACT AV ACCESS Investigators Disclosures Speaker name: Robert Lookstein, MD... I have the following
IN.PACT AV Access IDE Study Full Baseline Data Robert Lookstein, MD MHCDL New York, NY On Behalf of the IN.PACT AV ACCESS Investigators Disclosures Speaker name: Robert Lookstein, MD... I have the following
Chapter 12. End Stage Kidney Disease in Indigenous Peoples of Australia and Aotearoa/New Zealand. ANZDATA Registry 39th Annual Report
 Chapter 12 End Stage Kidney Disease in Indigenous Peoples of and Aotearoa/ 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, the rates and practice patterns for end-stage
Chapter 12 End Stage Kidney Disease in Indigenous Peoples of and Aotearoa/ 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, the rates and practice patterns for end-stage
Preservation of Veins and Timing for Vascular Access
 Preservation of Veins and Timing for Vascular Access Vassilis Liakopoulos, MD, PhD Department of Nephrology School of Medicine University of Thessaly Greece Hemodialysis VA A sound long-term dialysis access
Preservation of Veins and Timing for Vascular Access Vassilis Liakopoulos, MD, PhD Department of Nephrology School of Medicine University of Thessaly Greece Hemodialysis VA A sound long-term dialysis access
Tale of Neglected Aneurysm
 Disclosures Tale of Neglected Aneurysm Consultant to FFCL Tushar Vachharajani, MD, FASN Chief, Nephrology Section Salisbury VAMC, NC Objectives How do you define Aneurysm? When and How do you treat? Defining
Disclosures Tale of Neglected Aneurysm Consultant to FFCL Tushar Vachharajani, MD, FASN Chief, Nephrology Section Salisbury VAMC, NC Objectives How do you define Aneurysm? When and How do you treat? Defining
Juxta-anastomotic stenoses: angioplasty or surgery (or when/why should we wait)?
?") Juxta-anastomotic stenoses: angioplasty or surgery (or when/why should we wait)? Richard Shoenfeld MD, FSIR, FAHA The Access Center at West Orange West Orange, New Jersey USA SEDAV 2015 Madrid November
Juxta-anastomotic stenoses: angioplasty or surgery (or when/why should we wait)? Richard Shoenfeld MD, FSIR, FAHA The Access Center at West Orange West Orange, New Jersey USA SEDAV 2015 Madrid November
Postoperative AV Fistula Evaluation. Postoperative examination protocol. Postoperative AVF Protocol. Hemodialysis Access Surveillance
 Hemodialysis Access Surveillance Postoperative AV Fistula Evaluation Failure of maturation Stenosis Perigraft mass/fluid collection Joseph L. Mills, Sr., M.D. Professor of Surgery Chief, Division of Vascular
Hemodialysis Access Surveillance Postoperative AV Fistula Evaluation Failure of maturation Stenosis Perigraft mass/fluid collection Joseph L. Mills, Sr., M.D. Professor of Surgery Chief, Division of Vascular
End Stage Renal Disease (ESRD) Network Learning and Action Network (LAN) Series: Bloodstream Infection (BSI) Quality Improvement Activity
 Network Learning and Action Network (LAN) Series: Bloodstream Infection (BSI) Quality Improvement Activity") End Stage Renal Disease (ESRD) Network Learning and Action Network (LAN) Series: Bloodstream Infection (BSI) Quality Improvement Activity October 2, 2018 Note: Computer speakers or headphones are necessary
End Stage Renal Disease (ESRD) Network Learning and Action Network (LAN) Series: Bloodstream Infection (BSI) Quality Improvement Activity October 2, 2018 Note: Computer speakers or headphones are necessary
The HeRO Graft. Shawn M. Gage, PA Division of Vascular Surgery Duke University Medical Center
 The HeRO Graft Shawn M. Gage, PA Division of Vascular Surgery Duke University Medical Center Faculty Disclosure I disclose the following financial relationships: CryoLife/Hemosphere, Inc. & W.L. Gore and
The HeRO Graft Shawn M. Gage, PA Division of Vascular Surgery Duke University Medical Center Faculty Disclosure I disclose the following financial relationships: CryoLife/Hemosphere, Inc. & W.L. Gore and
St George Hospital Renal Department Internal Policy
 COMPLICATIONS OF VASCULAR ACCESS FOR HAEMODIALYSIS. SUMMARY: Any type of complication for either a centrally placed venous catheter or arterio-venous fistula/graft can place the patient at risk of sub-optimal
COMPLICATIONS OF VASCULAR ACCESS FOR HAEMODIALYSIS. SUMMARY: Any type of complication for either a centrally placed venous catheter or arterio-venous fistula/graft can place the patient at risk of sub-optimal
AV Access Technology and Innovation DEVICES CHANGING HOW WE THINK ABOUT VASCULAR ACCESS
 AV Access Technology and Innovation DEVICES CHANGING HOW WE THINK ABOUT VASCULAR ACCESS Vascular Access New Technology What problem are you trying to solve for? Most common problem is inadequate outflow
AV Access Technology and Innovation DEVICES CHANGING HOW WE THINK ABOUT VASCULAR ACCESS Vascular Access New Technology What problem are you trying to solve for? Most common problem is inadequate outflow
Renal Physicians Association Kidney Quality Improvement Registry, Powered by Premier, Inc non-mips Measure Specifications
 Renal Physicians Association Kidney Quality Improvement Registry, Powered by Premier, Inc. 2018 non-mips Measure Specifications Last updated January 2, 2018 RPAQIR1: Angiotensin Converting Enzyme (ACE)
Renal Physicians Association Kidney Quality Improvement Registry, Powered by Premier, Inc. 2018 non-mips Measure Specifications Last updated January 2, 2018 RPAQIR1: Angiotensin Converting Enzyme (ACE)
Surgical Options in Thrombectomy for Non-Surgeons
 Surgical Options in Thrombectomy for Non-Surgeons Shouwen Wang, MD, PhD, FASDIN AKDHC Ambulatory Surgery Center Arizona Kidney Disease and Hypertension Center Phoenix, Arizona Disclosure No relevant financial
Surgical Options in Thrombectomy for Non-Surgeons Shouwen Wang, MD, PhD, FASDIN AKDHC Ambulatory Surgery Center Arizona Kidney Disease and Hypertension Center Phoenix, Arizona Disclosure No relevant financial
Renal Patient s Information Leaflet
 Renal (Haemodialysis) Unit Patient Information Renal Patient s Information Leaflet Opening hours: If you need this information in large print, easy read, on audiotape or in another language please call
Renal (Haemodialysis) Unit Patient Information Renal Patient s Information Leaflet Opening hours: If you need this information in large print, easy read, on audiotape or in another language please call
MIHÁLY TAPOLYAI, MD, FASN, FACP Associate Professor, Louisiana State University; Shreveport, Louisiana, USA Associate Professor; University of Hawai
 MIHÁLY TAPOLYAI, MD, FASN, FACP Associate Professor, Louisiana State University; Shreveport, Louisiana, USA Associate Professor; University of Hawai i Postgraduate Training Program at Chubu Hospital, Okinawa,
MIHÁLY TAPOLYAI, MD, FASN, FACP Associate Professor, Louisiana State University; Shreveport, Louisiana, USA Associate Professor; University of Hawai i Postgraduate Training Program at Chubu Hospital, Okinawa,
Steal Syndrome: The Role of the Vascular Lab
 Steal Syndrome: The Role of the Vascular Lab Eighth Overlook Noninvasive Vascular Lab Symposium Larry A. Scher, M.D. Professor of Surgery Division of Vascular Surgery Montefiore Medical Center Albert Einstein
Steal Syndrome: The Role of the Vascular Lab Eighth Overlook Noninvasive Vascular Lab Symposium Larry A. Scher, M.D. Professor of Surgery Division of Vascular Surgery Montefiore Medical Center Albert Einstein
Medical Emergencies in Dialysis Patients
 Medical Emergencies in Dialysis Patients John Anderton Consultant Renal Physician Lancashire Teaching Hospitals NHS Foundation Trust Talk Plan A Flavour of Dialysis patients Emergencies in HD patients
Medical Emergencies in Dialysis Patients John Anderton Consultant Renal Physician Lancashire Teaching Hospitals NHS Foundation Trust Talk Plan A Flavour of Dialysis patients Emergencies in HD patients
STOCK and FLOW. ANZDATA Registry 2011 Report CHAPTER 1 STOCK & FLOW. Blair Grace Kylie Hurst Stephen McDonald 1-1
 CHAPTER 1 STOCK & FLOW Blair Grace Kylie Hurst Stephen McDonald 1-1 ANZDATA Registry 2011 Report The number of new patients in Australia decreased slightly to 2257 in 2010. While there is variation in
CHAPTER 1 STOCK & FLOW Blair Grace Kylie Hurst Stephen McDonald 1-1 ANZDATA Registry 2011 Report The number of new patients in Australia decreased slightly to 2257 in 2010. While there is variation in
COVERA Vascular Covered Stents in the Management of Dysfunctional AV Access
 COVERA Vascular Covered Stents in the Management of Dysfunctional AV Access Bart L. Dolmatch, M.D., FSIR Palo Alto Medical Foundation Mountain View, CA USA This presentation is being made on behalf of
COVERA Vascular Covered Stents in the Management of Dysfunctional AV Access Bart L. Dolmatch, M.D., FSIR Palo Alto Medical Foundation Mountain View, CA USA This presentation is being made on behalf of
PROVINCIAL STANDARDS & GUIDELINES
 PROVINCIAL STANDARDS & GUIDELINES CARE OF NEEDLING SITES POST-HEMODIALYSIS FOR FISTULAS & GRAFTS (HEMOSTASIS) Updated July 2015 Approved by the BCPRA Hemodialysis Committee Table of Contents 1.0 Practice
PROVINCIAL STANDARDS & GUIDELINES CARE OF NEEDLING SITES POST-HEMODIALYSIS FOR FISTULAS & GRAFTS (HEMOSTASIS) Updated July 2015 Approved by the BCPRA Hemodialysis Committee Table of Contents 1.0 Practice
JVA ISSN Hemodialysis vascular access management in the Netherlands. Introduction ORIGINAL ARTICLE
 JVA ISSN 1129-7298 J Vasc Access 2015; 16 (Suppl 9): S11-S15 DOI: 10.5301/jva.5000366 ORIGINAL ARTICLE Hemodialysis vascular access management in the Netherlands Jan H.M. Tordoir 1, Magda M. van Loon 1,
JVA ISSN 1129-7298 J Vasc Access 2015; 16 (Suppl 9): S11-S15 DOI: 10.5301/jva.5000366 ORIGINAL ARTICLE Hemodialysis vascular access management in the Netherlands Jan H.M. Tordoir 1, Magda M. van Loon 1,
 Developing a Quality Assurance Performance Improvement (QAPI) Program at Your Dialysis Center Rudolph P. Valentini, M.D. Associate Professor of Pediatrics Director of Dialysis Services Vice Chief of Staff
Developing a Quality Assurance Performance Improvement (QAPI) Program at Your Dialysis Center Rudolph P. Valentini, M.D. Associate Professor of Pediatrics Director of Dialysis Services Vice Chief of Staff
COVERA covered stent to treat stenosis in arteriovenous fistula: 6-month results from the prospective, multi-center, randomized AVeNEW study
 COVERA covered stent to treat stenosis in arteriovenous fistula: 6-month results from the prospective, multi-center, randomized AVeNEW study Panagiotis Kitrou MD, MSc, PhD, EBIR Consultant Interventional
COVERA covered stent to treat stenosis in arteriovenous fistula: 6-month results from the prospective, multi-center, randomized AVeNEW study Panagiotis Kitrou MD, MSc, PhD, EBIR Consultant Interventional
Dialysis Overview S J Fratesi MD FRCS
 Dialysis Overview 2005 S J Fratesi MD FRCS By the end of this session you should have an better understanding of : Ø Ø Ø Ø Ø Ø Ø Ø concept of dialysis alternative methods of dialysis indications for hemodialysis
Dialysis Overview 2005 S J Fratesi MD FRCS By the end of this session you should have an better understanding of : Ø Ø Ø Ø Ø Ø Ø Ø concept of dialysis alternative methods of dialysis indications for hemodialysis
Kidney Decisions Aid
 Kidney Decisions Aid A G U I D E F O R P E O P L E W H O H A V E, O R K N O W S O M E O N E, W I T H C H R O N I C K I D N E Y D I S E A S E, A N D T O A I D I N T H E D E C I S I O N A B O U T W H I C
Kidney Decisions Aid A G U I D E F O R P E O P L E W H O H A V E, O R K N O W S O M E O N E, W I T H C H R O N I C K I D N E Y D I S E A S E, A N D T O A I D I N T H E D E C I S I O N A B O U T W H I C
Recurrent lesions in AV access & Initial DCB experience in India
 Recurrent lesions in AV access & Initial DCB experience in India Dr. Virender K Sheorain Consultant Interventional Radiologist Medanta-The Medicity Hospital Gurgaon, INDIA Disclosure Speaker name:... I
Recurrent lesions in AV access & Initial DCB experience in India Dr. Virender K Sheorain Consultant Interventional Radiologist Medanta-The Medicity Hospital Gurgaon, INDIA Disclosure Speaker name:... I
Superficialización de la vena basílica. Pierre BOURQUELOT, Paris
 Superficialización de la vena basílica. Pierre BOURQUELOT, Paris 1 Basilic Vein Superficialization. Pierre BOURQUELOT, Paris 2 (Upper arm) Basilic Vein 3 Technique 2-stage Basilic Vein Tunnel-Superficialization
Superficialización de la vena basílica. Pierre BOURQUELOT, Paris 1 Basilic Vein Superficialization. Pierre BOURQUELOT, Paris 2 (Upper arm) Basilic Vein 3 Technique 2-stage Basilic Vein Tunnel-Superficialization
Proven Performance Through Innovative Design *
 Proven Performance Through Innovative Design * Deliver Our Next Generation AV Covered Stent Results The COVERA Vascular Covered Stent builds upon proven technologies from the category leader in AV Access.
Proven Performance Through Innovative Design * Deliver Our Next Generation AV Covered Stent Results The COVERA Vascular Covered Stent builds upon proven technologies from the category leader in AV Access.
Lutonix in AV fistula and Early look AV IDE trial data
 Lutonix in AV fistula and Early look AV IDE trial data Jackie P Ho Dept of Cardiac, Thoracic & Vascular Surgery National University of Singapore NUHS, Singapore Lutonix in AV fistula and final AV IDE trial
Lutonix in AV fistula and Early look AV IDE trial data Jackie P Ho Dept of Cardiac, Thoracic & Vascular Surgery National University of Singapore NUHS, Singapore Lutonix in AV fistula and final AV IDE trial
Quality ID #329: Adult Kidney Disease: Catheter Use at Initiation of Hemodialysis National Quality Strategy Domain: Effective Clinical Care
 Quality ID #329: Adult Kidney Disease: Catheter Use at Initiation of Hemodialysis National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Quality ID #329: Adult Kidney Disease: Catheter Use at Initiation of Hemodialysis National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Hemodialysis Fistula Maturation Consortium
 Hemodialysis Fistula Maturation Consortium Rationale for Fistula Maturation Study Dialysis Access Consortium AVF study 60% of new AVFs were unusable for dialysis at 4-5 months post surgery No predictors
Hemodialysis Fistula Maturation Consortium Rationale for Fistula Maturation Study Dialysis Access Consortium AVF study 60% of new AVFs were unusable for dialysis at 4-5 months post surgery No predictors
CHAPTER 12 END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND. Matthew Jose Stephen McDonald Leonie Excell
 CHAPTER 12 END-STAGE KIDNEY DISEASE AMONG PEOPLES OF AUSTRALIA AND NEW ZEALAND Matthew Jose Stephen McDonald Leonie Excell INTRODUCTION Rates of end-stage kidney disease among the Peoples of and are substantially
CHAPTER 12 END-STAGE KIDNEY DISEASE AMONG PEOPLES OF AUSTRALIA AND NEW ZEALAND Matthew Jose Stephen McDonald Leonie Excell INTRODUCTION Rates of end-stage kidney disease among the Peoples of and are substantially
The Role of LUTONIX 035 DCB in AV Fistula Dysfunction Management in our Practice
 The Role of LUTONIX 035 DCB in AV Fistula Dysfunction Management in our Practice Dr Kate Steiner Consultant Interventional Radiologist East and North Hertfordshire NHS Trust Disclosure Speaker name: Dr
The Role of LUTONIX 035 DCB in AV Fistula Dysfunction Management in our Practice Dr Kate Steiner Consultant Interventional Radiologist East and North Hertfordshire NHS Trust Disclosure Speaker name: Dr
NKF K/DOQI GUIDELINES
 NKF K/DOQI GUIDELINES Executive Summaries Anemia Hemodialysis Peritoneal Dialysis Vascular Access Nutrition CKD 2002 Dyslipidemias Bone Metabolism Hypertension and Antihypertensive Agents Cardiovascular
NKF K/DOQI GUIDELINES Executive Summaries Anemia Hemodialysis Peritoneal Dialysis Vascular Access Nutrition CKD 2002 Dyslipidemias Bone Metabolism Hypertension and Antihypertensive Agents Cardiovascular
UW MEDICINE PATIENT EDUCATION. Hemodialysis. A treatment option for kidney disease. Treatment Options for Kidney Disease
 UW MEDICINE PATIENT EDUCATION Hemodialysis A treatment option for kidney disease Class Goals 1. Understand the purpose and care of blood access. 2. Understand the purpose and basic principles of hemodialysis.
UW MEDICINE PATIENT EDUCATION Hemodialysis A treatment option for kidney disease Class Goals 1. Understand the purpose and care of blood access. 2. Understand the purpose and basic principles of hemodialysis.
Assessment, Monitoring, and. Svetlana (Lana) Kacherova, ESRD Network 18, QI Director WebEx session, December 18, 2008
 Kacherova, ESRD Network 18, QI Director WebEx session, December 18, 2008") Vascular Access Assessment, Monitoring, and Surveillance Svetlana (Lana) Kacherova, ESRD Network 18, QI Director WebEx session, December 18, 2008 1 Special Acknowledgement for Content Contributions: RMS
Vascular Access Assessment, Monitoring, and Surveillance Svetlana (Lana) Kacherova, ESRD Network 18, QI Director WebEx session, December 18, 2008 1 Special Acknowledgement for Content Contributions: RMS
Treatment choices for someone with Stage 5 kidney disease are:
 Information for patients about advanced kidney disease Dialysis and non-dialysis treatments DOCUMENT PREPARED FOR This information is to help you understand some key issues about dialysis; it is designed
Information for patients about advanced kidney disease Dialysis and non-dialysis treatments DOCUMENT PREPARED FOR This information is to help you understand some key issues about dialysis; it is designed
What vascular access for which patient : obesity
 What vascular access for which patient : obesity C. Sessa, J. Coudurier A. De Lambert, C. Ducos, M. Guergour, O. Pichot Department of Vascular Surgery Grenoble France Controversies & Updates in Vascular
What vascular access for which patient : obesity C. Sessa, J. Coudurier A. De Lambert, C. Ducos, M. Guergour, O. Pichot Department of Vascular Surgery Grenoble France Controversies & Updates in Vascular
Haemodialysis central venous catheter-related sepsis management guideline Version 3. NAME M. Letheren Chair Clinical Effectiveness Advisory Group
 Lancashire Teaching Hospitals NHS Foundation Trust Haemodialysis central venous catheter-related sepsis management guideline Version 3 AUTHOR APPROVED BY DATE AUTH REF. NO NAME REBG/00018/July12 Michael
Lancashire Teaching Hospitals NHS Foundation Trust Haemodialysis central venous catheter-related sepsis management guideline Version 3 AUTHOR APPROVED BY DATE AUTH REF. NO NAME REBG/00018/July12 Michael
VA Session: A Team-Based Approach to Solving Vascular Access Problems. October 7, 2016
 2016 VA Session: A Team-Based Approach to Solving Vascular Access Problems October 7, 2016 Panel discussion with: Dr. Mercedeh Kiaii (nephrologist) Dr. Jerry Chen (surgeon) Mirita Zerr (vascular access
2016 VA Session: A Team-Based Approach to Solving Vascular Access Problems October 7, 2016 Panel discussion with: Dr. Mercedeh Kiaii (nephrologist) Dr. Jerry Chen (surgeon) Mirita Zerr (vascular access
KDOQI Guidelines. Overview. Predicting Successful Fistula Maturation Warren Gasper MD UCSF Vascular Surgery Fellow 2011 UCSF Vascular Symposium
 DISCLOSURES: NONE Predicting Successful Fistula Maturation Warren Gasper MD UCSF Vascular Surgery Fellow 2011 UCSF Vascular Symposium KDOQI Guidelines AV fistulas have better outcomes than grafts or catheters
DISCLOSURES: NONE Predicting Successful Fistula Maturation Warren Gasper MD UCSF Vascular Surgery Fellow 2011 UCSF Vascular Symposium KDOQI Guidelines AV fistulas have better outcomes than grafts or catheters
Measure #330: Adult Kidney Disease: Catheter Use for Greater Than or Equal to 90 Days National Quality Strategy Domain: Patient Safety
 Measure #330: Adult Kidney Disease: Catheter Use for Greater Than or Equal to 90 Days National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES REGISTRY ONLY This is a
Measure #330: Adult Kidney Disease: Catheter Use for Greater Than or Equal to 90 Days National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES REGISTRY ONLY This is a
First experience with DCB for treatment of dialysis access stenosis The Greek experience
 First experience with DCB for treatment of dialysis access stenosis The Greek experience D Karnabatidis Department of Interventional Radiology Patras University Hospital Patras, Greece Background Vessel
First experience with DCB for treatment of dialysis access stenosis The Greek experience D Karnabatidis Department of Interventional Radiology Patras University Hospital Patras, Greece Background Vessel
The Buttonhole Technique for AV Fistula Cannulation
 The Buttonhole Technique for AV Fistula Cannulation Lynda K. Ball, RN, MSN, CNN October 16 & 17, 2008 Trends in Nephrology Nursing Kaiser Permanente Acute Dialysis Symposium 1 CMS Disclaimer This publication
The Buttonhole Technique for AV Fistula Cannulation Lynda K. Ball, RN, MSN, CNN October 16 & 17, 2008 Trends in Nephrology Nursing Kaiser Permanente Acute Dialysis Symposium 1 CMS Disclaimer This publication
CHAPTER 3 ARTERIOVENOUS ACCESS: INFECTION, NEUROPATHY AND OTHER COMPLICATIONS
 CHAPTER 3 ARTERIOVENOUS ACCESS: INFECTION, NEUROPATHY AND OTHER COMPLICATIONS AUTHORS: Jennifer MacRae MSc MD, Christine Dipchand MD MSc, Matthew Oliver MD MSc, Louise Moist MD MSc, Serdar Yilmaz MD Phd,
CHAPTER 3 ARTERIOVENOUS ACCESS: INFECTION, NEUROPATHY AND OTHER COMPLICATIONS AUTHORS: Jennifer MacRae MSc MD, Christine Dipchand MD MSc, Matthew Oliver MD MSc, Louise Moist MD MSc, Serdar Yilmaz MD Phd,
Difference in practical dialysis therapy between East Asia and US/EU
 Difference in practical dialysis therapy between East Asia and US/EU Jer-Ming Chang. M.D., Ph.D. 1 Professor, Attending physician, Kaohsiung Medical University Hospital; 2 Secretary General, Taiwan Society
Difference in practical dialysis therapy between East Asia and US/EU Jer-Ming Chang. M.D., Ph.D. 1 Professor, Attending physician, Kaohsiung Medical University Hospital; 2 Secretary General, Taiwan Society
Access Preservation: Recurrent Central Venous Stenosis, Pacemaker Wires and other Nightmares. Who am I? Disclosures
 Access Preservation: Recurrent Central Venous Stenosis, Pacemaker Wires and other Nightmares Jason Burgess, MD RVT Surgical Specialists of Charlotte CMC-Mercy Charlotte, NC Disclosures Gore Vascular- Consultant
Access Preservation: Recurrent Central Venous Stenosis, Pacemaker Wires and other Nightmares Jason Burgess, MD RVT Surgical Specialists of Charlotte CMC-Mercy Charlotte, NC Disclosures Gore Vascular- Consultant
Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality
 Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality Shannon H. Norris, BSN, RN June 6, 2018 Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality DISCUSSION: End Stage
Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality Shannon H. Norris, BSN, RN June 6, 2018 Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality DISCUSSION: End Stage
Ultrasound and the dialysis patient
 Ultrasound and the dialysis patient Poster No.: C-1765 Congress: ECR 2011 Type: Educational Exhibit Authors: T. M. O. Couto, H. Matos, Â. Moreira, A. Estevao ; vila conde/ 1 2 2 2 1 2, Coimbra/ Keywords:
Ultrasound and the dialysis patient Poster No.: C-1765 Congress: ECR 2011 Type: Educational Exhibit Authors: T. M. O. Couto, H. Matos, Â. Moreira, A. Estevao ; vila conde/ 1 2 2 2 1 2, Coimbra/ Keywords:
CSI (Clinical Scenario Investigation): Hyperkalemia
: Hyperkalemia") CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
National Surveillance System for Dialysis Centre and Dialysis Associated Diseases
 National Surveillance System for Dialysis Centre and Dialysis Associated Diseases Dr Richard Fluck Consultant Renal Physician & Clinical Director, Royal Derby Hospital UK RA Vascular Access Survey 2005
National Surveillance System for Dialysis Centre and Dialysis Associated Diseases Dr Richard Fluck Consultant Renal Physician & Clinical Director, Royal Derby Hospital UK RA Vascular Access Survey 2005
MANITOBA RENAL PROGRAM
 SUBJECT Venipuncture of Arteriovenous Fistula/Graft MANITOBA RENAL PROGRAM SECTION CODE 30.20.01 30.20 Vascular Access AUTHORIZATION Professional Advisory Committee, Manitoba Renal Program Nursing Practice
SUBJECT Venipuncture of Arteriovenous Fistula/Graft MANITOBA RENAL PROGRAM SECTION CODE 30.20.01 30.20 Vascular Access AUTHORIZATION Professional Advisory Committee, Manitoba Renal Program Nursing Practice
Dialysis and Transplantation Audit
 New Zealand Dialysis and Transplantation Audit and A summary report of activity for New Zealand nephrology services Dr Suetonia Palmer On behalf of the National Renal Advisory Board NRAB Standard and Audits
New Zealand Dialysis and Transplantation Audit and A summary report of activity for New Zealand nephrology services Dr Suetonia Palmer On behalf of the National Renal Advisory Board NRAB Standard and Audits
CHAPTER 2. Prevalence of Renal Replacement Therapy for End Stage Kidney Disease
 CHAPTER 2 Prevalence of Renal Replacement Therapy for End Stage Kidney Disease Summarising the number of prevalent renal replacement therapy patients in Australia and New Zealand, the prevalence rate per
CHAPTER 2 Prevalence of Renal Replacement Therapy for End Stage Kidney Disease Summarising the number of prevalent renal replacement therapy patients in Australia and New Zealand, the prevalence rate per