Pulmonary embolism. Paweł Balsam MD, PhD
|
|
|
- Kerry Preston
- 5 years ago
- Views:
Transcription

1 Pulmonary embolism Paweł Balsam MD, PhD
2 Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism
3 Pulmonary embolism A pulmonary embolism is a blockage in one of the blood vessels in your lungs. It can be fatal if the obstruction is very large and blocks the main blood supply to the lungs.

4 Pulmonary embolism
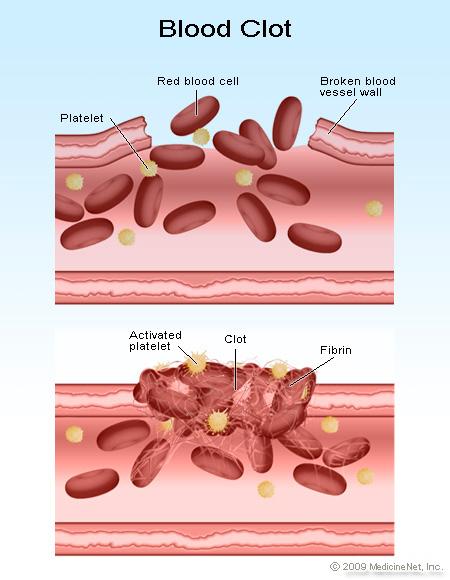
5 CLOT
6 Pulmonary embolism Virchow's Triad - Causes of Thrombosis Changes in the blood vessel wall Changes in the blood flow Changes in the blood composition
7 Changes in the blood flow The first category, alterations in normal blood flow, refers to several situations. These includeturbulence, stasis, mitral stenosis, and varicose veins. The equivalence of Virchow's version and the modern version has been disputed.
8 Changes in the blood vessel wall The second category, injuries and/or trauma to endothelium includes damage to the veins arising from shear stress or hypertension.
9 Changes in the blood composition The last category, alterations in the constitution of blood, has numerous possible risk factors such as hyperviscosity, deficiency of antithrombin III, nephrotic syndrome, changes after severetrauma or burn, disseminated cancer, late pregnancy and delivery, race, age, whether the patient is a smoker, and obesity. All of these risk factors cause the situation called hypercoagulability.

10 Pulmonary embolism
11 Pulmonary embolism Pulmonary embolism (PE) is cardiovascular emergency. Occlusion of pulmonary artery may lead to life threatning but potientially reversible right ventricle failure.
12 Epidemology The prevalence of PE among hospitalized patients is 0.4% It gives about patients cases/year in USA
13 Mortality 2-8% treated (diagnosed) 30% non-treated (non-diagnosed)
14 Predisposing factors Strong predisposing factors: -fracture (hip or leg) -hip or knee replacement -major general surgery -major trauma -spinal cord injury
15 Predisposing factors Moderate predisposing factors: -arthroscopic knee surgery -central venous lines -chemotherapy -chronic heart or respiratory failure -hormone replacement therapy -malignancy -oral contraceptive therapy -paralytic stroke -pregnancy -previous VTE -thrombofilia
16 Predisposing factors Weak predisposing factors: - Bed rest > 3 days - Immobilitydueto sitting (prolonged trip) - Increasing age - Laparoscopic surgery - Obesity - Varicose veins
17 Primary risk factors AT III deficiency factor V Leiden (APC-R) mutation of protromine gene 20210A dysfibrynogenemia hiperhomocysteinemia anticardiolipin a-bodies protein C deficiency plasminogen deficiency protein S deficiency
18 PE Risk factors - secondary CHF immobilization older age neoplasm stroke obesity surgery central iv lines smoking pregnancy/peripartum oral contraceptives long distance travels
19 Pathophysiology Key consequences of pulmonary embolism are hemodynamic. Large and mutiple emobli may increase pulmonary vascular resistance to a level of afterload which cannot be matched by a right ventricle (RV)
20 Pathophysiology Sudden death occurs mainly in the mechanism of electromechanical dissociation.
21 Severity of PE Markers of severity: 1. Clinical markers: Shock and Hypotension 2. Markers of RV dysfunction: dilation, hypokinesis or pressure overload on echocardiography RV dilation on spiral computed tomography BNP or NT-proBNP elevation Elevated right heart pressure on RHC 3. Markers of myocardial injury: cardiac troponin T or I
22 Risk stratification PE related EARLY MORTALITY RISK CLINICAL RISK MARKERS RV dysfuntion Myocardia l injury Treatment implications HIGH (15%) + (+)* (+)* Thrombolysis or embolectomy NON HIGH Intermed iate (3-15%) - Low <1% Hospital admission Early discharge or home treatment
23 Prognostic assesment Shock and hypotension are principal markers of high risk of early death in acute PE
24 Prognostic assesment RV dysfunction is related to intermediate risk of short-term mortality Its prognostic value is limited by the lack of universally accepted criteria
25 Prognostic assesment Myocardial injury isrelated to intermediaterisk of short-term mortality Its prognostic value is limited by the lack of universally accepted criteria.
26 Diagnosis Clinical presentation D-dimer Compression ultrasonography and computed tomographic venography Ventilation-perfusion scintigraphy Computed tomography Pulmonary angiography Echocardiography
27 Clinical presentation Symptoms: -dyspnoea 80% -chest pain 52% -cough 20% -hemoptysis -cyanosis -collapse
28 Clinical presentation Signs: Tachypnea (respiratory rate >16/min): 96% Rales: 58% Accentuated second heart sound: 53% Tachycardia (heart rate >100/min): 44% Fever (temperature >37.8 C): 43% Diaphoresis: 36% S 3 or S 4 gallop: 34% Clinical signs and symptoms suggesting thrombophlebitis: 32% Lower extremity edema: 24% Cardiac murmur: 23% Cyanosis: 19%
29 Assesment of clnical probability of Variable PE Wells score Predisposing factors: Previous DVT or PE Recent surgery or immobilization Cancer Points Symptoms Hemoptysis +1 Clinical signs Heart rate >100 beats/min Clinical signs of DVT Clinical judgement Alternative diagnosis less likely than PE +3
30 Assesment of clnical probability of PE Wells score Clinical probability Low Intermediate High Total
31 Differential diagnosis of PE: Pneumonia or bronchitis Asthma Exacerbation of chronic obstructive disease MI Pulmonary edema Anxiety
32 Differential diagnosis of PE: Dissection of the aorta Pericardial tamponade Lung cancer Primary pulmonary hipertension Rib fracture Pneumothorax
33 D-dimer The product of a cross-linked fibrin. Very high negative predictive value. Very low positive predictive value increased level: cancer, inflamation, necrosis, dissection of the aorta Negative D-dimer result in a higly sensitive assay safely excludes the PE in a patientns with low ormoderate clinical risk
34 Compression ultrasonography (CUS) 90% of PE is due to DVT in lower limb. CUS has 90% sensitivity and 95% specificity for diagnosing proximal DVT Thus finding a proximal DVT in patients with suspected PE is sufficient to start anticoagualnt treatment
35 Ventilation-perfusion scintigraphy Combination of perfusion and ventilation scans. In case of PE the perfusion scan is abnormal but the ventilation scan is normal Thereisperfusion-ventilation mismatch
36 Ventilation-perfusion scintigraphy Normal perfusion scan is very safe to exclude PE Combination of non-diagnostic V/Q in a patient with low clinical probability of PE i acceptable for excluding PE. High probability ventilation-perfusion scans establish the diagnosis of PE with a high degree of probability, but further tests are required
37 Computed tomography SDCT single detector computed tomography SENSITIVITY 70%; SPECIFICITY 90% Negative SDCT test is not safe for ruling out PE In association with absence of proximal DVT is a good method for ruling out the PE
38 Computed tomography MDCT multi detector computed tomography has high spatial and temporal resolution. SENSITIVITY 83%; SPECIFICITY 96% MDCT showing a thrombus up to the segmental level can be adequate evidence of PE. In a patient with non-high clinical probability of PE, negative MDCT may be used as a stand alone test to exclude PE
39 Pulmonary angiography Is an invasive method associated with some risk. Currently it is useful when the results of noninvasive methods are equivocal.
40 Echocardiography In the presence of shock and hypotension the lack of echocardiographic signs of RV overload or dysfunction excludes PE as the cause of hemodynamic compromise. It also helps to find the reason of such a condition: tamponade, acute valvular dysfunction, acutemyocardial infarction.
41 Diagnostic strategies Suspected high-risk PE Suspected non-high risk PE

42 Diagnostic strategies Suspected high-risk PE CT immediately available no yes Echo RV overload no yes CT available CT stable patient positive negative Search for No other test available other causes orpatient unstable PE-specific Search for other causes treatment justified
 Multidetector CT No PE PE No PE PE No treatment TREATMENT!!! No treatment TREATMENT!! Investigate further 24.05.")
43 Diagnostic strategies Suspected non-high-risk PE Asses clinical probability of PE Low/intermediate clinical probability of PE D dimer High clinical probability of PE negative positive Multidetector CT (no treatment) Multidetector CT No PE PE No PE PE No treatment TREATMENT!!! No treatment TREATMENT!! Investigate further
44 Treatment The scheme of treatment depends on severity of PE.
45 Treatment In high risk patients the respiratory and hemodynamicsupport isnecessary. Hemodynamic support: dopamine, dobutamine, epinephrine, norepinephrine
46 Treatment High risk patients Thrombolytic therapy is the first line treatment in high-risk patients presenting with cardiogenic shock and/or persistent arterial hypotension with a very few absolute cantraindications.
47 Treatment High risk patients Routine use of thrombolysis in non-high risk patients is not recomended. It may be considered in intermediate risk patients after thorough consideration of conditions increasing the risk of bleeding.
48 Thrombolysis contraindications Absolute: -Haemorrhagic stroke or stroke of unkown origin at any time -Ishemic stroke in preceding 6 months -Central nervous system damage or neoplasms -Recent major trauma/surgery/head injury (within preceding 3 weeks) -Gastrointestinal bleeding within thelastmonth -Known bleeding
49 Thrombolytic regimens for PE treatment Streptokinase: IU as a loading dose over 30 minutes -followed by IU/h over 12-24h Urokinase: -4400IU/kg as a loading dose over 10min -followed by 4400IU/kg/h over 12-24h
50 Thrombolytic regimens for PE treatment rtpa 100mg over 2h or 0.6 mg/kg over 15 min (maxium dose 50mg)
51 Surgical pulmonary embolectomy With current surgical techniques, pulmonary emobolectomy is a valuable therapeutic option in patients with high-risk PE in whom thrombolysis is absolutely contraindicated or has failed.
52 Percutaneous catheter embolectomy and fragmentation Catheter embolectomy or fragmentation of proximal pulmonary clots may be considered as an alternative to surgical treatment in patients with high-risk PE in whom thrombolysis is absolutely contraindicated or has failed.
53 Anticoagulant therapy Anticoagulant therapy with unfractioned heparin, LMWH or fondaparinux should be initiated without delay in patients with confirmed PE and those with high or intermediate risk clinical probability of PE while diagnostic workup is still ongoing.
54 Anticoagulant therapy Except for patients at high risk of bleeding and those with severe renal dysfunction, subcutaneous LMWH or fondaparinux rather than intravenous unfractioned heparin should be considered for initial treatment
55 Anticoagulant therapy Unfractioned heparin: -bolus of 80U/kg, followed by infusion at the rate of 18U/kg/h. -subsequent doses should be adjusted using the activated partial thromboplastin time(aptt). -reach and maintain the prolongation of aptt between 1.5 and 2.5 -aptt should be measured 3-4 hours after bolus and 3 hours after each dose adjustment
56 Anticoagulant therapy - UFH aptt Change of dosage <35 s (<1.2 times control) 80 U/kg bolus; increase infusion rate by 4U/kg/h 35-45s ( times control) 46-70s ( times control) 71-90s ( times control) 40 U/kg bolus; increase infusion rate by 2U/kg/h No change Reduce the infusion rate by 2 U/kg >90s (>3.0 times) Stop infusion for 1 hour then reduce infusion rate by 3 U/kg/h
57 Anticoagulant therapy In patients at high risk of bleeding (non-high risk PE) and in those with severe renal dysfunction, unfractioned heparin with an aptt target range of times normal is a recommended form of initial treatment.
58 Anticoagulant therapy LMWH enoxaparin -dose: 1.0 mg/kg every 12h -contraindicated in severe renal failure (creatinine clearance <30 ml/min) Fondaparinux selective factor Xa inhibitor -dose: 5mg body weight <50g 7.5mg body weight kg 10mg body weight > 100kg
59 Anticoagulant therapy Rivaroxaban 2 x 15 mg Dabigatran 2 x 150 mg
60 Anticoagulant therapy Parenteral anticoagulation should be continued for at least 5 days VKA a should be initiated as soon as possible and preferably on the same day as initial anticoagulant. Parenteral anticoagulant should be stopped when the INR lies between 2.0 and 3.0 for at least 2 consecutive days
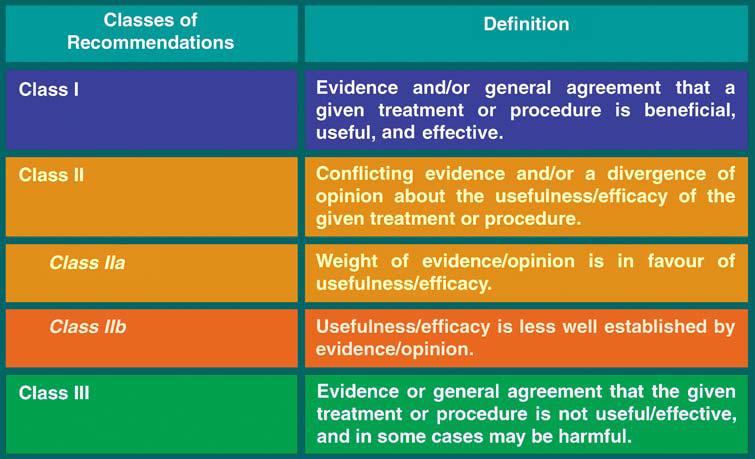
61 Class o recomedation

62 Level of evidence
63
64
65 Oral anticoagulant therapy
66 Thank You
Pulmonary embolism. Paweł Balsam
 Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
PULMONARY EMBOLISM -CASE REPORT-
 University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Venous thrombosis is common and often occurs spontaneously, but it also frequently accompanies medical and surgical conditions, both in the community
 Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks
 Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks 1. What is the most common cause of death in hospitalized patients? 1. Hospital-acquired infection 2. Pulmonary embolism 3. Myocardial infarction
Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks 1. What is the most common cause of death in hospitalized patients? 1. Hospital-acquired infection 2. Pulmonary embolism 3. Myocardial infarction
Heart Health ESC Guidelines on the diagnosis and management of acute pulmonary embolism
 Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Thrombolysis in PE. Outline. Disclosure. Overview on Pulmonary Embolism. Hot Topics in Emergency Medicine 2012 Midyear Clinical Meeting
 Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
PE and DVT. Dr Anzo William Adiga WatsApp or Call Medical Officer/RHEMA MEDICAL GROUP
 PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE is a difficult diagnosis that may be missed because of non-specific clinical presentation.
 Pulmonary embolism (PE) is a relatively common cardiovascular emergency. By occluding the pulmonary arterial bed it may lead to acute life-threatening (3% early mortality rate), but potentially reversible
Pulmonary embolism (PE) is a relatively common cardiovascular emergency. By occluding the pulmonary arterial bed it may lead to acute life-threatening (3% early mortality rate), but potentially reversible
October 2017 Pulmonary Embolism
 October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Pulmonary Thromboembolism
 Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM. Gordon Lowe Professor of Vascular Medicine University of Glasgow
 CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
Acute Pulmonary Embolism and Deep Vein Thrombosis. Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center COPYRIGHT
 Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Pulmonary Embolectomy:
 Pulmonary Embolectomy: Recommendation for early surgical intervention Tomas A. Salerno, M.D. Professor of Surgery, University of Miami Miller School of Medicine and Jackson Memorial Hospital Epidemiology
Pulmonary Embolectomy: Recommendation for early surgical intervention Tomas A. Salerno, M.D. Professor of Surgery, University of Miami Miller School of Medicine and Jackson Memorial Hospital Epidemiology
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Risk factors for DVT. Venous thrombosis & pulmonary embolism. Anticoagulation (cont d) Diagnosis 1/5/2018. Ahmed Mahmoud, MD
 Diagnosis 1/5/2018. Ahmed Mahmoud, MD") Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism. Ahmed Mahmoud, MD
 Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Proper Diagnosis of Venous Thromboembolism (VTE)
") Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Slide 1. Slide 2. Slide 3. Outline of This Presentation
 Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Approach to Thrombosis
 Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
Misunderstandings of Venous thromboembolism prophylaxis
 Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
Pulmonary embolism - the great masquerader
 Pulmonary embolism - the great masquerader V.N. Karazin Kharkov National University Department of Internal Medicine Associate professor Makharynska О.S., MD, PhD 2016 Pulmonary embolism (PE) is a blockage
Pulmonary embolism - the great masquerader V.N. Karazin Kharkov National University Department of Internal Medicine Associate professor Makharynska О.S., MD, PhD 2016 Pulmonary embolism (PE) is a blockage
Pulmonary Thromboembolism
 Pulmonary Thromboembolism Jing ZHANG ( 张静 ), MD, PhD zhang.jing@zs-hospital.sh.cn Department of Pulmonary Medicine Zhongshan Hospital Fudan University OUTLINE Understand the historical context of pulmonary
Pulmonary Thromboembolism Jing ZHANG ( 张静 ), MD, PhD zhang.jing@zs-hospital.sh.cn Department of Pulmonary Medicine Zhongshan Hospital Fudan University OUTLINE Understand the historical context of pulmonary
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Reducing the risk of venous thrombo-embolism (VTE) in hospital and after discharge
 in hospital and after discharge") Reducing the risk of venous thrombo-embolism (VTE) in hospital and after discharge What is a venous thromboembolism (VTE)? This is a medical term that describes a blood clot that develops in a deep vein
Reducing the risk of venous thrombo-embolism (VTE) in hospital and after discharge What is a venous thromboembolism (VTE)? This is a medical term that describes a blood clot that develops in a deep vein
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Acute Pulmonary Embolism SB Gupta
 Acute Pulmonary Embolism 2010 SB Gupta Pulmonary Embolism accounts for more than 650,000 cases each year and as many as 300,000 deaths annually in the US alone. PE is the 3rd most common cause acute cardiovascular
Acute Pulmonary Embolism 2010 SB Gupta Pulmonary Embolism accounts for more than 650,000 cases each year and as many as 300,000 deaths annually in the US alone. PE is the 3rd most common cause acute cardiovascular
CHAPTER 2 VENOUS THROMBOEMBOLISM
 CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
THROMBOSIS RISK FACTOR ASSESSMENT
 Name: Procedure: Doctor: Date: THROMBOSIS RISK FACTOR ASSESSMENT CHOOSE ALL THAT APPLY EACH RISK FACTOR REPRESENTS 1 POINT Age 41 60 years Minor Surgery Planned History of Prior Major Surgery (< 1 month)
Name: Procedure: Doctor: Date: THROMBOSIS RISK FACTOR ASSESSMENT CHOOSE ALL THAT APPLY EACH RISK FACTOR REPRESENTS 1 POINT Age 41 60 years Minor Surgery Planned History of Prior Major Surgery (< 1 month)
Case. Case. Management of Pulmonary Embolism in the ICU
 Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
REVIEW ON PULMONARY EMBOLISM
 REVIEW ON PULMONARY EMBOLISM * Shashi Kumar Yadav, Prof. Xiao Wei, Roshan Kumar Yadav, Sanjay Kumar Verma and Deepika Dhakal * Department of Medicine, Clinical College of Yangtze University, The first
REVIEW ON PULMONARY EMBOLISM * Shashi Kumar Yadav, Prof. Xiao Wei, Roshan Kumar Yadav, Sanjay Kumar Verma and Deepika Dhakal * Department of Medicine, Clinical College of Yangtze University, The first
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY
 INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information
 Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Is Thrombolysis Only for a Crisis?
 Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Epidemiology: Incidence VTE: Mortality Morbidity Risk Factors: Acute Chronic : Genetic
 Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Pathology of pulmonary vascular disease. Dr.Ashraf Abdelfatah Deyab. Assistant Professor of Pathology Faculty of Medicine Almajma ah University
 Pathology of pulmonary vascular disease Dr.Ashraf Abdelfatah Deyab Assistant Professor of Pathology Faculty of Medicine Almajma ah University Pulmonary vascular disease Type of pulmonary circulation: Types
Pathology of pulmonary vascular disease Dr.Ashraf Abdelfatah Deyab Assistant Professor of Pathology Faculty of Medicine Almajma ah University Pulmonary vascular disease Type of pulmonary circulation: Types
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism
 Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
ADULT TRANSCATHETER AORTIC VALVE REPLACEMENT (TAVR) TELEMETRY BED TRANSFER ORDERS 1 of 4
 TELEMETRY BED TRANSFER ORDERS 1 of 4") TELEMETRY BED TRANSFER 1 of 4 9 Actual 9 Estimated Patient ID Area Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Transfer to: 10 South Attending Physician: Diagnosis:
TELEMETRY BED TRANSFER 1 of 4 9 Actual 9 Estimated Patient ID Area Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Transfer to: 10 South Attending Physician: Diagnosis:
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Objectives. Venous Thromboembolism (VTE) Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?
 Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?") Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Objectives DVT PE 5/11/2011. Venous Thromboembolism (VTE) Venous Thromboembolism (VTE) Virchow s Triad. VTE Incidence
 Venous Thromboembolism (VTE) Virchow s Triad. VTE Incidence") Objectives Current Concepts in the Diagnosis and Management of Venous Thromboembolism 1. Discuss antithrombotic treatment options for venous thromboembolism. 2. Describe the role of thrombolytic therapy
Objectives Current Concepts in the Diagnosis and Management of Venous Thromboembolism 1. Discuss antithrombotic treatment options for venous thromboembolism. 2. Describe the role of thrombolytic therapy
PE Pathway. The charts are listed as follows:
 PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
This chapter will describe the effectiveness of antithrombotic
 Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,
Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,
Epidermiology Early pulmonary embolism
 Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Pulmonary Embolism. Dr.V.Maruthi Rama Krishna Rao
 Pulmonary Embolism Dr.V.Maruthi Rama Krishna Rao Assistant prof EMD Pulmonary embolism (PE) refers to the lodging of a embolic material from a distant site in the pulmonary circulation The term embolus
Pulmonary Embolism Dr.V.Maruthi Rama Krishna Rao Assistant prof EMD Pulmonary embolism (PE) refers to the lodging of a embolic material from a distant site in the pulmonary circulation The term embolus
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis. By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan
 Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients. David Liff MD Oklahoma Heart Institute Vascular Center
 DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
Jordan M. Garrison, MD FACS, FASMBS
 Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Intraoperative Pulmonary Embolus
 PBLD Table #5 Intraoperative Pulmonary Embolus Holly Richter, M.D. and Sean Benton, D.O. Objectives 1. Determine patients who are at risk for perioperative pulmonary embolism 2. Form a differential diagnosis
PBLD Table #5 Intraoperative Pulmonary Embolus Holly Richter, M.D. and Sean Benton, D.O. Objectives 1. Determine patients who are at risk for perioperative pulmonary embolism 2. Form a differential diagnosis
Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis?
 Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
8/16/2012. Pulmonary Embolism
 Pulmonary Embolism Rita M. Williams, NP-C, PA PeaceHealth Medical Group, Pulmonary & Critical Care Pulmonary Embolism Acute pulmonary embolism (PE) is a common and frequently fatal disease Clinical presentation
Pulmonary Embolism Rita M. Williams, NP-C, PA PeaceHealth Medical Group, Pulmonary & Critical Care Pulmonary Embolism Acute pulmonary embolism (PE) is a common and frequently fatal disease Clinical presentation
Diagnosis and management of pulmonary embolism
 Follow the link from the online version of this article to obtain certified continuing medical education credits bmj.com Respiratory Medicine updates from BMJ Group are at bmj.com/specialties/respiratory-medicine
Follow the link from the online version of this article to obtain certified continuing medical education credits bmj.com Respiratory Medicine updates from BMJ Group are at bmj.com/specialties/respiratory-medicine
ACUTE VASCULAR SYNDROMES
 7 CHAPTER 7 ACUTE VASCULAR SYNDROMES 7.1 ACUTE AORTIC SYNDROMES p.92 A. Evangelista 7.2 ACUTE PULMONARY EMBOLISM p.102 A. Torbicki ACUTE AORTIC SYNDROMES: Concept and classification (1) Types of presentation
7 CHAPTER 7 ACUTE VASCULAR SYNDROMES 7.1 ACUTE AORTIC SYNDROMES p.92 A. Evangelista 7.2 ACUTE PULMONARY EMBOLISM p.102 A. Torbicki ACUTE AORTIC SYNDROMES: Concept and classification (1) Types of presentation
Anticoagulation for prevention of venous thromboembolism
 Anticoagulation for prevention of venous thromboembolism Original article by: Michael Tam Note: updated in June 2009 with the eighth edition (from the seventh) evidence-based clinical practice guidelines
Anticoagulation for prevention of venous thromboembolism Original article by: Michael Tam Note: updated in June 2009 with the eighth edition (from the seventh) evidence-based clinical practice guidelines
Pulmonary Embolism. Supportive module 3 "Basics of diagnosis, treatment and prevention of major pulmonary diseases "
 Supportive module 3 "Basics of diagnosis, treatment and prevention of major pulmonary diseases " Pulmonary Embolism LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky, L. Bogun, L. Martymianova,
Supportive module 3 "Basics of diagnosis, treatment and prevention of major pulmonary diseases " Pulmonary Embolism LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky, L. Bogun, L. Martymianova,
Management of Intermediate-Risk Pulmonary Embolism
 Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University of Mainz,
Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University of Mainz,
CARDIAC PROBLEMS IN PREGNANCY
 CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE. Mark Goodwin, MD
 Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
PULMONARY EMBOLISM MANAGEMENT GUIDELINES
 PULMONARY EMBOLISM MANAGEMENT GUIDELINES This document is adapted from the NICE guidelines titled Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia
PULMONARY EMBOLISM MANAGEMENT GUIDELINES This document is adapted from the NICE guidelines titled Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies
 VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
The Johns Hopkins Hospital Patient Information. How Do I Prevent Blood Clots? Venous Thromboembolism (VTE) Deep Vein Thrombosis (DVT)
 Deep Vein Thrombosis (DVT)") Page 1 of 11 Venous Thromboembolism () What is a clot or Venous Thromboembolism ()? Blood clots are called Venous Thromboembolism (). There are 2 main types: is a clot in a deep vein, usually an arm or
Page 1 of 11 Venous Thromboembolism () What is a clot or Venous Thromboembolism ()? Blood clots are called Venous Thromboembolism (). There are 2 main types: is a clot in a deep vein, usually an arm or
Oxford Medicine Online
 Oxford Medicine Online The ESC Textbook of Intensive and Acute Cardiovascular Care (2 ed.) Edited by Marco Tubaro, Pascal Vranckx, Susanna Price, and Christiaan Vrints Latest update This online textbook
Oxford Medicine Online The ESC Textbook of Intensive and Acute Cardiovascular Care (2 ed.) Edited by Marco Tubaro, Pascal Vranckx, Susanna Price, and Christiaan Vrints Latest update This online textbook
Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1
 CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
Severe pulmonary embolism: surgical aspects. Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland
 Severe pulmonary embolism: surgical aspects Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland Severe pulmonary embolism Acute pulmonary embolism Chronic pulmonary thromboembolism
Severe pulmonary embolism: surgical aspects Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland Severe pulmonary embolism Acute pulmonary embolism Chronic pulmonary thromboembolism
CANCER ASSOCIATED THROMBOSIS. Pankaj Handa Department of General Medicine Tan Tock Seng Hospital
 CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
Guideline for Thrombolysis Therapy in Pulmonary Embolism
 Guideline for Thrombolysis Therapy in Pulmonary Embolism Dr Jane Strong Consultant Haematologist Trust ref: B24/2016 1. Introduction / Scope All Patients with pulmonary embolism (PE) require rapid risk
Guideline for Thrombolysis Therapy in Pulmonary Embolism Dr Jane Strong Consultant Haematologist Trust ref: B24/2016 1. Introduction / Scope All Patients with pulmonary embolism (PE) require rapid risk
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Clinical Guide - Suspected PE (Reviewed 2006)
") Clinical Guide - Suspected (Reviewed 2006) Principal Developer: B. Geerts Secondary Developers: C. Demers, C. Kearon Background Investigation of patients with suspected pulmonary emboli () remains problematic
Clinical Guide - Suspected (Reviewed 2006) Principal Developer: B. Geerts Secondary Developers: C. Demers, C. Kearon Background Investigation of patients with suspected pulmonary emboli () remains problematic
COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP)
") The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use London, 16 December 1999 COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP) NOTE FOR GUIDANCE ON CLINICAL
The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use London, 16 December 1999 COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP) NOTE FOR GUIDANCE ON CLINICAL
Challenges in the management of acute pulmonary embolism
 Challenges in the management of acute pulmonary embolism Case: A pregnant woman presenting with clinical suspicion of acute venous thromboembolism: Appropriate diagnostic and therapeutic strategy in pregnancy.
Challenges in the management of acute pulmonary embolism Case: A pregnant woman presenting with clinical suspicion of acute venous thromboembolism: Appropriate diagnostic and therapeutic strategy in pregnancy.
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Lung diseases of Vascular Origin. By: Shefaa Qa qqa
 Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital Foundation Trust
 MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
Chapter 1. Introduction
 Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150
Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150
Acute Management of Pulmonary Embolism
 Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
VENOUS THROMBOEMBOLISM DR. AMITESH AGGARWAL
 VENOUS THROMBOEMBOLISM DR. AMITESH AGGARWAL Pulmonary embolism and deep venous thrombosis spectrum of one disease venous thromboembolism PE is not a disease it is a complication of DVT 79% PE DVT LL 50%
VENOUS THROMBOEMBOLISM DR. AMITESH AGGARWAL Pulmonary embolism and deep venous thrombosis spectrum of one disease venous thromboembolism PE is not a disease it is a complication of DVT 79% PE DVT LL 50%
Handbook for Venous Thromboembolism
 Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
Surgical approach for DVT. Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine
 Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
How long to continue anticoagulation after DVT?
 How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
Supplementary Online Content
 Supplementary Online Content Mismetti P, Laporte S, Pellerin O, Ennezat P-V, Couturaud F, Elias A, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone
Supplementary Online Content Mismetti P, Laporte S, Pellerin O, Ennezat P-V, Couturaud F, Elias A, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone
Pathophysiology. Tutorial 3 Hemodynamic Disorders
 Pathophysiology Tutorial 3 Hemodynamic Disorders ILOs Recall different causes of thrombosis. Explain different types of embolism and their predisposing factors. Differentiate between hemorrhage types.
Pathophysiology Tutorial 3 Hemodynamic Disorders ILOs Recall different causes of thrombosis. Explain different types of embolism and their predisposing factors. Differentiate between hemorrhage types.
PE MANAGEMENT. Objectives
 PE MANAGEMENT Dr. Zohair Al aseri FRCPC Emergency Medicine FRCPC Critical Care Medicine Assistant Professor & Chairman Dept. of Emergency Medicine College of Medicine King Saud University Hospitals Objectives
PE MANAGEMENT Dr. Zohair Al aseri FRCPC Emergency Medicine FRCPC Critical Care Medicine Assistant Professor & Chairman Dept. of Emergency Medicine College of Medicine King Saud University Hospitals Objectives
Pulmonary Embolism Newer Concepts and Role of Thrombolysis
 CHAPTER 69 Pulmonary Embolism Newer Concepts and Role of Thrombolysis J. P. S. Sawhney, A. Bakhshi, B. Kandpal Introduction Pulmonary embolism (PE) is a common cardiovascular and cardiopulmonary illness
CHAPTER 69 Pulmonary Embolism Newer Concepts and Role of Thrombolysis J. P. S. Sawhney, A. Bakhshi, B. Kandpal Introduction Pulmonary embolism (PE) is a common cardiovascular and cardiopulmonary illness
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES
 DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES Jose M. Borromeo M.D. Vascular Surgeon Iowa Heart Center Disclosures: AstraZeneca Pharmaceuticals Cook CVRx LeMaitre Vascular,
DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES Jose M. Borromeo M.D. Vascular Surgeon Iowa Heart Center Disclosures: AstraZeneca Pharmaceuticals Cook CVRx LeMaitre Vascular,
DOAC and NOAC are terms for a novel class of directly acting oral anticoagulant drugs including Rivaroxaban, Apixaban, Edoxaban, and Dabigatran.
 Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
THROMBOSIS AND BLEEDING
 THROMBOSIS AND BLEEDING Klara Gadó MD. PhD. Senior Professor of Internal Medicine Semmelweis University, Budapest What is thrombosis? formation of a blood clot in a blood vessel Blood can not flow Organ
THROMBOSIS AND BLEEDING Klara Gadó MD. PhD. Senior Professor of Internal Medicine Semmelweis University, Budapest What is thrombosis? formation of a blood clot in a blood vessel Blood can not flow Organ
Deep Vein Thrombosis
 Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
A 50-year-old woman with syncope
 Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local