OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
|
|
|
- Doris McKinney
- 5 years ago
- Views:
Transcription
1 & & the Future of High Frequency Oscillatory Ventilation (HFOV)

2 What do we know already? Sud S et al. BMJ 2010
3 & Multi-centre randomised controlled trials of HFOV verses current ventilation practice in adults with ARDS
4 n = 795 (1006 intended) n = 548 (1200 intended) 29 centres 39 centres Expert and non-expert centres Expert and non-expert centres England, Scotland and Wales Canada, USA, Saudi, Chile and India Day mortality, - days of paralysis, sedation, vasopressors, and antibiotics, duration of treatment in ICU and hospital 60 Day mortality - total dose of paralysis and sedation, vasopressors, duration of treatment in ICU and hospital
5 Inclusion Respiratory failure Intubated for less than 7 days since onset of failure Intubated within 2 weeks of onset of failure Expected to need ventilation for more than 2 days Hypoxaemia PEEP 5 mmhg PaO2:FiO2 200 Radiology Bilateral air space opacification on chest X ray Age
6 Exclusion Evidence of right atrial hypertension Suspected vascular pulmonary haemorrhage Neuromuscular disorders known to prolong MV Lung disease characterised by airway narrowing or air trapping Weight < 35 Kg Recent lung surgery Severe chronic respiratory disease Weight < 35 Kg or > 1 Kg per cm height Pre-existing conditions with > 50% 1 year mortality Participating in other trial
7 Control Stipulation Usual practice with guidance Strict protocol Recruitment none 40 s of 40 mmhg Mode PCV Vt 6 8 ml/kg IBW 6 ml/kg IBW PEEP Titrated to FiO2 Pplat Spont breaths < 35 mmhg Daily trial Rescue HFOV At physicians discretion Yes with clear indications
8 Intervention Recruitment Ventilator Novalung R100 (Metran) 40 s of 40 mmhg Sensor Medics 3100B (CareFusion) PMaw 5 cmh2o > Pplat 30 cmh2o PaO mmhg mmhg f 10 Hz then ph Hz then ph 7.2 I:E 1:1 1:2 Bias flow 100 ml
9 Exit from HFOV 12 hours of: - FiO PaO2 60 mmhg - PMaw 24 cmh2o Restart HFOV up to 2 days later
10 Randomisation Allocation Independent telephone randomisation system Central web-based randomisation system Stratification PaO2:FiO2 ratio, sex, age, centre Blocks of 2 or 4 centre Baseline Slight advantage to intervention (age) Slight intervention to control (age and inotropes)
11 Blinding Treatment - No blinding Analysis - Unclear Outcomes are objective
12 Results: Follow Up 100% on intention to treat - 2.5% of control arm received rescue HFOV - 2.5% of intervention arm died before HFOV could be commenced 97.5% intervention vs 2.5% control received HFOV median duration of 3 days (IQR 2 5) 100% on intention to treat - 12% of control arm received rescue HFOV - 1.5% of intervention arm didn t receive HFOV 98% intervention vs 12% control received HFOV median duration of 3 days (IQR 2 8)
13 Cross Over Pre planed conditions for rescue therapy including HFOV - Refractory hypoxaemia (PaO2 60 mmhg with FiO2 of 1.0 with neuromuscular blockade) - Refractory barotrauma (persistent pneumothorax or increasing subcutaneous emphysema despite two intercostal catheters on the involved side) - Refractory acidosis (ph 7.05 despite neuromuscular blockade) 12% crossed over to HFOV (91% according to protocol) Average duration of rescue HFOV was 7 days Mortality 71% in the crossed over patients Maximum number of patients that might have been saved was 10 (3.5%)
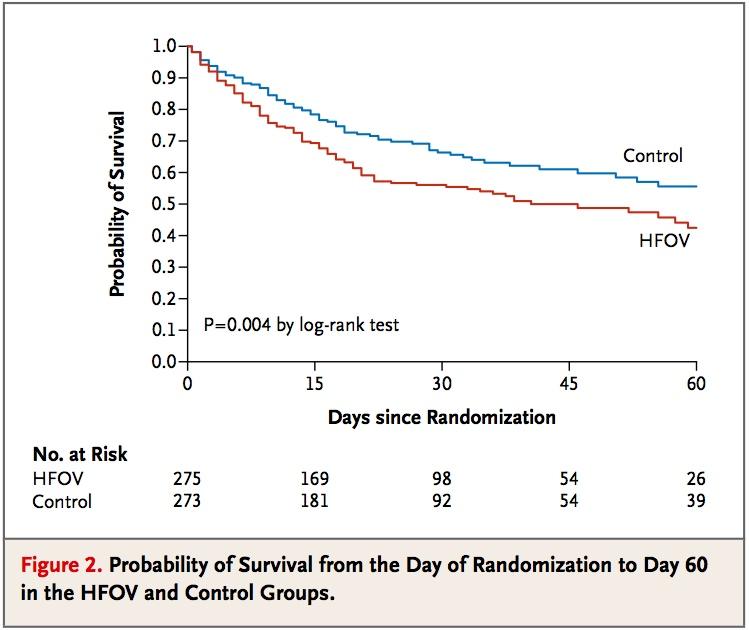
14 Primary Outcomes 30 Day mortality 60 Day mortality Control HFOV Control HFOV 166 (41.7%) 163 (41.1%) 96 (35%) 129 (47%) (P = 0.85) (P = 0.005) Stopped early for futility Relative risk of death in the HFOV cohort 1.33 (CI ) Stopped early for risk of harm
15 Results
16 Results
17 Multivariate Analysis on 60 Day Mortality No significant association with - Baseline hypoxia - Respiratory compliance - BMI - Vasopressors - Treatment centre experience
18 Secondary Outcomes Intervention vs Control Midazolam: 199 mg vs 144 mg (P<0.001) Sedation 9.4 vs 8.5 days Fentanyl: 2980 μg vs 2400 μg (P=0.06) NMJ blockade 2.5 vs 2.0 days 98% vs 63% (P<0.001) Vasopressors 2.9 days vs 2.8 days 91% vs 84% (P=0.01) Antibiotics 12.8 vs 12.4 days Refractory hypoxia 7% vs 14% (P=0.007)
19 The Future for HFOV Dubious
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Does proning patients with refractory hypoxaemia improve mortality?
 Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS
 THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS Recommendation 1 on website Hyperinflation (Ventilator or manual) might be included in the management
THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS Recommendation 1 on website Hyperinflation (Ventilator or manual) might be included in the management
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Post Arrest Ventilation/Oxygenation Management
 Post Arrest Ventilation/Oxygenation Management Richard Branson MSc RRT Professor of Surgery University of Cincinnati Editor-In-Chief Respiratory Care 0 Presenter Disclosure Information Richard Branson
Post Arrest Ventilation/Oxygenation Management Richard Branson MSc RRT Professor of Surgery University of Cincinnati Editor-In-Chief Respiratory Care 0 Presenter Disclosure Information Richard Branson
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
Exclusion Criteria 1. Operator or supervisor feels specific intra- procedural laryngoscopy device will be required.
 FELLOW Study Data Analysis Plan Direct Laryngoscopy vs Video Laryngoscopy Background Respiratory failure requiring endotracheal intubation occurs in as many as 40% of critically ill patients. Procedural
FELLOW Study Data Analysis Plan Direct Laryngoscopy vs Video Laryngoscopy Background Respiratory failure requiring endotracheal intubation occurs in as many as 40% of critically ill patients. Procedural
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
CLINICAL VIGNETTE 2016; 2:3
 CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
ECMO/ECCO 2 R in Acute Respiratory Failure
 ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal
 Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
Neuromuscular Blockade in ARDS
 Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE)
") Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE) John Laffey, Giacomo Bellani, Tai Pham, Eddy Fan, Antonio Pesenti on behalf of the LUNG SAFE Investigators
Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE) John Laffey, Giacomo Bellani, Tai Pham, Eddy Fan, Antonio Pesenti on behalf of the LUNG SAFE Investigators
RESEARCH. High frequency oscillation in patients with acute lung injury andacuterespiratorydistresssyndrome(ards):systematic review and meta-analysis
:systematic review and meta-analysis") High frequency oscillation in patients with acute lung injury andacuterespiratorydistresssyndrome(ards):systematic review and meta-analysis Sachin Sud, fellow, 1 Maneesh Sud, medical student, 2 Jan O Friedrich,
High frequency oscillation in patients with acute lung injury andacuterespiratorydistresssyndrome(ards):systematic review and meta-analysis Sachin Sud, fellow, 1 Maneesh Sud, medical student, 2 Jan O Friedrich,
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Care Unit (FELLOW)
") Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Ventilation update Anaesthesia departmental PGME. Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care
 Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
Clinical Practice Guidelines for Cases with Pneumonia associated with Pandemic H1N infection As of 7 August 2009
 Clinical Practice Guidelines for Cases with Pneumonia associated with Pandemic H1N1 2009 infection As of 7 August 2009 This Clinical Practice Guideline contains basic information to be considered when
Clinical Practice Guidelines for Cases with Pneumonia associated with Pandemic H1N1 2009 infection As of 7 August 2009 This Clinical Practice Guideline contains basic information to be considered when
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Dr. Yasser Fathi M.B.B.S, M.Sc, M.D. Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah
 BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
Year in Review Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
ARDS: MANAGEMENT UPDATE
 ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
ARDS and treatment strategies
 ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
Non- conventional forms of respiratory support
 Non- conventional forms of respiratory support Dr Liesel Bosenberg Specialist Physician & Fellow in Critical Care Medicine Kalafong & Steve Biko Academic Hospitals Points we will ponder: ECMO Liquid Ventilation
Non- conventional forms of respiratory support Dr Liesel Bosenberg Specialist Physician & Fellow in Critical Care Medicine Kalafong & Steve Biko Academic Hospitals Points we will ponder: ECMO Liquid Ventilation
CASE PRESENTATION VV ECMO
 CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
RESCUE VENTILATION SUMMARY
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS
 with surfactant in pediatric ARDS") Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Seminar. Current Concepts
 Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
AVOIDING THE CRASH 3: RELAX, OPTIMAL POST-AIRWAY MANAGEMENT AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT
 AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
Recognizing and Correcting Patient-Ventilator Dysynchrony
 2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
Trial protocol - NIVAS Study
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 Trial protocol - NIVAS Study METHODS Study oversight The Non-Invasive Ventilation after Abdominal Surgery
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 Trial protocol - NIVAS Study METHODS Study oversight The Non-Invasive Ventilation after Abdominal Surgery
LAS VEGAS Case Report Form 1 Intra-Operative
 LAS VEGAS Case Report Form 1 Intra-Operative Patient Informed Consent 1. Informed consent applicable: yes no (choose no if waived by local EC) 1.1 If applicable; was consent obtained? yes no 1.2 If yes,
LAS VEGAS Case Report Form 1 Intra-Operative Patient Informed Consent 1. Informed consent applicable: yes no (choose no if waived by local EC) 1.1 If applicable; was consent obtained? yes no 1.2 If yes,
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Indirect Calorimetry and the GE Engstrom Carestation. Jorge E. Rodriguez BSRC, RRT
 Jorge E. Rodriguez BSRC, RRT Indirect tcl Calorimetry and the GE To obtain the most accurate metabolic data from Indirect Calorimetry, one must: Evaluate the patient. Obtain consistent, Steady State data.
Jorge E. Rodriguez BSRC, RRT Indirect tcl Calorimetry and the GE To obtain the most accurate metabolic data from Indirect Calorimetry, one must: Evaluate the patient. Obtain consistent, Steady State data.
Non-Invasive Bed-Side Assessment of Pulmonary Vascular Resistance in Critically Ill Pediatric Patients with Acute Respiratory Distress Syndrome
 Aim of the Work This study aimed to evaluate the degree of pulmonary hypertension as well as alterations in the pulmonary vascular resistance in critically ill children with ARDS using bed- side echocardiography.
Aim of the Work This study aimed to evaluate the degree of pulmonary hypertension as well as alterations in the pulmonary vascular resistance in critically ill children with ARDS using bed- side echocardiography.
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1).
.") PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
INTELLiVENT -ASV insight. Alexandra Geiger CAS, Dr. Marc Wysocki, Head of Medical Research Hamilton Medical
 INTELLiVENT -ASV insight Alexandra Geiger CAS, Dr. Marc Wysocki, Head of Medical Research Hamilton Medical First Automation of HAMILTON MEDICAL 1998 Adaptive Support Ventilation (ASV) ASV optimize VT and
INTELLiVENT -ASV insight Alexandra Geiger CAS, Dr. Marc Wysocki, Head of Medical Research Hamilton Medical First Automation of HAMILTON MEDICAL 1998 Adaptive Support Ventilation (ASV) ASV optimize VT and
Airway management problem during anaesthesia. Airway management problem in ICU / HDU. Airway management problem occurring in the Emergency Department
 4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support
 The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support Laveena Munshi, MD, MSc November 1, 2016 Critical Care Canada Forum Interdepartmental Division of Critical
The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support Laveena Munshi, MD, MSc November 1, 2016 Critical Care Canada Forum Interdepartmental Division of Critical
QuickLung Breather Patient Settings
 The QuickLung Breather is capable of simulating a spontaneously breathing patient in a variety of modes and patterns. In response to customer requests, we have compiled five common respiratory cases below.
The QuickLung Breather is capable of simulating a spontaneously breathing patient in a variety of modes and patterns. In response to customer requests, we have compiled five common respiratory cases below.
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) REFERRAL FORM
 REFERRAL FORM") Patient Label This form is accessible on www.royalpapworth.nhs.uk Intensive Care Unit EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) REFERRAL FORM Please always phone Papworth ECMO Coordinator on 01480 830541,
Patient Label This form is accessible on www.royalpapworth.nhs.uk Intensive Care Unit EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) REFERRAL FORM Please always phone Papworth ECMO Coordinator on 01480 830541,
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
2. To provide an ethical, moral and practical framework for decision-making during a public health emergency.
 November 2010 TABLE TOP EXERCISE PARTICIPANT GUIDE When Routine Critical Care Resources Are Not Available Time expectations for each session: SECTION ACTIVITY TIME I Introduction 5 minutes II Exercise
November 2010 TABLE TOP EXERCISE PARTICIPANT GUIDE When Routine Critical Care Resources Are Not Available Time expectations for each session: SECTION ACTIVITY TIME I Introduction 5 minutes II Exercise
ARDS & TBI - Trading Off Ventilation Targets
 ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
INDEPENDENT LUNG VENTILATION
 INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy?
 Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy? Michelle Kho, PT, PhD Assistant Professor, School of Rehabilitation Science, McMaster University Adjunct Assistant Professor, Department
Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy? Michelle Kho, PT, PhD Assistant Professor, School of Rehabilitation Science, McMaster University Adjunct Assistant Professor, Department
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
The 1918 flu pandemic (January 1918 December 1920) was an unusually deadly influenza pandemic, the first of the two pandemics involvingh1n1 influenza
 was an unusually deadly influenza pandemic, the first of the two pandemics involvingh1n1 influenza") PANEL DISCUSSION The 1918 flu pandemic (January 1918 December 1920) was an unusually deadly influenza pandemic, the first of the two pandemics involvingh1n1 influenza virus. [1] It infected 500 million
PANEL DISCUSSION The 1918 flu pandemic (January 1918 December 1920) was an unusually deadly influenza pandemic, the first of the two pandemics involvingh1n1 influenza virus. [1] It infected 500 million
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Tracking lung recruitment and regional tidal volume at the bedside. Antonio Pesenti
 Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
. L. min. 4 min. min. L. min. I. A 64 year old female with pulmonary edema NORMAL
 NSWR KY TO NOTS on RSPT 350 - Module G - PaCO and lveolar Ventilation 1 Problems Given a fixed alveolar ventilation of L/, calculate the PaCO when the CO production is 300 ml/ VCO 300mL 863 863 PaCO 589
NSWR KY TO NOTS on RSPT 350 - Module G - PaCO and lveolar Ventilation 1 Problems Given a fixed alveolar ventilation of L/, calculate the PaCO when the CO production is 300 ml/ VCO 300mL 863 863 PaCO 589
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study
 D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
Inhaled nitric oxide: clinical evidence for use in adults
 Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
PAEDIATRIC RESPIRATORY FAILURE. Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre
 PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
An introduction to mechanical ventilation. Fran O Higgins, Adrian Clarke Correspondence
 Update in Anaesthesia An introduction to mechanical ventilation Respiratory Summary Mechanical ventilation is the major invasive intervention offered in the ICU. In low income countries, where the facilities
Update in Anaesthesia An introduction to mechanical ventilation Respiratory Summary Mechanical ventilation is the major invasive intervention offered in the ICU. In low income countries, where the facilities
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Agenda. Mechanical Ventilation in Morbidly Obese Patients. Paolo Pelosi. ESPCOP, Ostend, Belgium Saturday, November 14, 2009.
 Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Non Invasive Ventilation In Preterm Infants. Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid
 Non Invasive Ventilation In Preterm Infants Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid Summary Noninvasive ventilation begings in the delivery room
Non Invasive Ventilation In Preterm Infants Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid Summary Noninvasive ventilation begings in the delivery room
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation