HYPERTENSION: UPDATE 2018
|
|
|
- Cynthia Woods
- 5 years ago
- Views:
Transcription
1 HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD
2 I have no disclosures

3 HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM

4 BUT SOMETIMES IT CHARGES
5 HTN IN US ~78 million adults (33% of population) By 2030 ~41.4% NHANES % aware 74.9% current treatment 52.5% controlled 47.5% not controlled ~75% have visits at least 2x/y Heart disease and stroke statistics 2014 update: AHA. Circulation 14;129:e28-e292 Vital signs: awareness and treatment of uncontrolled HTN among adults MMWR MorbMortal WklyRep. 12;61:703-9
6 HYPERTENSION Most common modifiable CVD risk factor Contributes to >50% of adverse CVD outcomes JAMAD 16;17: edit. Morbidity/mortality correlates with BP > 115/75 BP control Reduces HF 50%; CVA 40%; MI 25% Presence of other CV risk factors multiplicative increase in risk for CV events Circulation 15;131:e435-e70
7

8 JNC 7 GUIDELINES 2003
9 TREATING BP TO GOAL STUDIES African American Study of Kidney Disease and Hypertension (AASK) trial SBP <140 vs <130 No decrease in progression of CKD or mortality NEJM 10;363: Action to Control Cardiovascular Risk in Diabetes(ACCORD) trial SBP <140 vs <120 No decrease in composite of CV events CVA reduced 0.32% vs. 0.53% (HR 0.59, p=0.01) Serious ADEs 3.3% vs 1.3% (p<0.001) NEJM 10;362:
10 RELAXED TREATMENT TARGETS JNC 8 BP target of 140/90 mmhg People <60 years of age Diabetes Chronic Kidney Disease BP target of 150/90 mmhg People >60 years of age Without Diabetes or Chronic Kidney Disease
11 CONCERN FOR JNC 8 TREATMENT TARGETS Multiple groups expressed concern around the new treatment targets Five members of the JNC 8 committee published a letter expressing concern regarding the relaxation of the treatment guidelines Drs Jackson Wright (University Hospitals Case Medical Center, Cleveland, OH) Lawrence Fine (National Heart, Lung, and Blood Institute (Bethesda, MD) Daniel Lackland (Medical University of South Carolina, Charleston) Gbenga Ogedegbe (New York University School of Medicine, New York) Cheryl Dennison Himmelfarb (Johns Hopkins University School of Nursing, Baltimore, MD) A series of letters and articles were published in the Major Journals including the Annals of Internal Med and JAMA
12 SPECIFIC CONCERNS TO JNC 8 Increasing the systolic BP target in those 60 years or older will have the effect of reducing the intensity of antihypertensive treatment among patients already being treated, among them a large population with established CVD or at high risk for CVD (including African Americans and patients with multiple CVD risk factors other than chronic kidney disease) The evidence supporting upping the target from 140 mm Hg to 150 mm Hg in people 60 or older was insufficient and inconsistent
13 SPECIFIC CONCERNS TO JNC 8 Evidence from trials and observational studies that the panel did not use as part of its review supports the lower goal, especially in high-risk patients Raising the target may have the unintended effect of reversing decades of declining CVD rates, especially stroke mortality

14
15 Background High BP very common High SBP leading risk factor for mortality and disability-adjusted life years Worldwide, >1 billion adults have hypertension Observational studies identify strong association between BP and risk of CVD, with no evidence of threshold for the relationship Clinical trials demonstrate antihypertensive drug therapy reduces risk of CVD However, optimal target for SBP lowering uncertain
16 SPRINT Research Question Examine effect of more intensive high blood pressure treatment than is currently recommended Randomized Controlled Trial Target Systolic BP Intensive Treatment Goal SBP < 120 mm Hg Standard Treatment Goal SBP < 140 mm Hg SPRINT design details available at: ClinicalTrials.gov (NCT ) Ambrosius WT et al. Clin. Trials. 2014;11:
17 Major Inclusion Criteria 50 years old Systolic blood pressure : mm Hg (treated or untreated) Additional cardiovascular disease (CVD) risk Clinical or subclinical CVD (excluding stroke) Chronic kidney disease (CKD), defined as egfr 20 <60 ml/min/1.73m 2 Framingham Risk Score for 10-year CVD risk 15% At least one Age 75 years
18 Major Exclusion Criteria Stroke Diabetes mellitus Polycystic kidney disease Congestive heart failure (symptoms or EF < 35%) Proteinuria >1g/d CKD with egfr < 20 ml/min/1.73m 2 (MDRD) Adherence concerns

19 Location of 102 SPRINT Clinical Centers Clinical Center Networks -Ohio -Southeast -Utah -UAB -VA Central Laboratory MRI Reading Center Project Office, NIH Coordinating Center Wake Forest School of Medicine ECG Reading Center Drug Distribution Center
20 SPRINT: Enrollment and Follow-up Experience Screened (N=14,692) Randomized (N=9,361) Intensive Treatment (N=4,678) Standard Treatment (N=4,683) Consent withdrawn Discontinued intervention Lost to follow-up Analyzed 4,678 4,683 (Intention to treat) (Vital status assessment: entire cohort)
21 Primary Outcome and Primary Hypothesis Primary outcome CVD composite: first occurrence of Myocardial infarction (MI) Acute coronary syndrome (non-mi ACS) Stroke Acute decompensated heart failure (HF) Cardiovascular disease death Primary hypothesis* CVD composite event rate lower in intensive compared to standard treatment *Estimated power of 88.7% to detect a 20% difference - based on recruitment of 9,250 participants, 4-6 years of follow-up and loss to follow-up of 2%/year.
22 BP Intervention BP monitored monthly for 3 months and every 3 months thereafter (additional visits could be scheduled) Antihypertensive medication titration decisions based on mean BP (3 readings at each visit), using a structured stepped-care approach Agents from all major antihypertensive drug classes available free of charge Periodic assessment for orthostatic hypotension and related symptoms
23 Systolic BP During Follow-up Year 1 Mean SBP mm Hg Standard Average SBP (During Follow-up) Standard: mm Hg Mean SBP mm Hg Intensive Intensive: mm Hg Average number of antihypertensive medications Number of participants
24 SPRINT Primary Outcome Cumulative Hazard Hazard Ratio = 0.75 (95% CI: 0.64 to 0.89) Standard (319 events) Intensive (243 events) During Trial (median follow-up = 3.26 years) Number Needed to Treat (NNT) to prevent a primary outcome = 61 Number of Participants
25 Primary Outcome Experience in the Six Pre-specified Subgroups of Interest *Treatment by subgroup interaction
 <0.001 All MI 97 0.65 116 0.78 0.83 (0.64, 1.09) 0.19 Non-MI ACS 40 0.27 40 0.27 1.00 (0.64, 1.55) 0.99 All Stroke 62 0.41 70 0.47 0.89 (0.63, 1.25) 0.50 All HF 62 0.41 100 0.")
26 SPRINT Primary Outcome and its Components Event Rates and Hazard Ratios Intensive Standard No. of Events Rate, %/year No. of Events Rate, %/year HR (95% CI) P value Primary Outcome (0.64, 0.89) <0.001 All MI (0.64, 1.09) 0.19 Non-MI ACS (0.64, 1.55) 0.99 All Stroke (0.63, 1.25) 0.50 All HF (0.45, 0.84) CVD Death (0.38, 0.85) 0.005
27 Serious Adverse Events* (SAE) During Follow-up All SAE reports Number (%) of Participants Intensive Standard HR (P Value) 1793 (38.3) 1736 (37.1) 1.04 (0.25) SAEs associated with Specific Conditions of Interest Hypotension 110 (2.4) 66 (1.4) 1.67 (0.001) Syncope 107 (2.3) 80 (1.7) 1.33 (0.05) Injurious fall 105 (2.2) 110 (2.3) 0.95 (0.71) Bradycardia 87 (1.9) 73 (1.6) 1.19 (0.28) Electrolyte abnormality 144 (3.1) 107 (2.3) 1.35 (0.020) Acute kidney injury or acute renal failure 193 (4.1) 117 (2.5) 1.66 (<0.001) *Fatal or life threatening event, resulting in significant or persistent disability, requiring or prolonging hospitalization, or judged important medical event.
28 Decision to Stop BP Intervention On August 20 th, 2015, NHLBI Director accepted DSMB recommendation to inform SPRINT investigators and participants of CVD results Concurrently, decision made to stop BP intervention This presentation based on adjudicated events that occurred through August 20 th, 2015 Median follow-up = 3.26 years Data for some secondary non-cvd outcomes (e.g. dementia and cognitive impairment) being collected at final close-out visit and this process will be completed in 2016
29 Summary and Conclusions SPRINT examined effects of more intensive antihypertensive therapy than currently recommended Participants were US adults 50 years with hypertension and additional risk for CVD Rapid and sustained difference in SBP achieved between the two treatment arms Trial stopped early, due to benefit, after median follow-up of 3.26 years Incidence of primary outcome (composite of CVD events) 25% lower in Intensive compared to Standard Group and all-cause mortality reduced by 27%. Treatment effect similar in all six pre-specified groups of interest. The number needed to treat to prevent primary outcome event or death 61 and 90, respectively
30 Summary and Conclusions In participants with CKD at baseline, no differences in renal outcomes In participants without CKD at baseline, incidence of egfr reduction 30% more common in Intensive Group No overall difference in serious adverse events (SAEs) between treatment groups SAEs associated with hypotension, syncope, electrolyte abnormalities, and hospital discharge reports of acute kidney injury or acute renal failure more common in Intensive Group Overall, benefits of more intensive BP lowering exceeded the potential for harm

31 MAYBE WE CAN FINALLY SEE THE ELEPHANT FOR WHAT HE IS

32 WELL NOT SO FAST..

33 CONCERN WITH SPRINT TRIAL

34 A SCIENTIFIC POLL OF CARDIOLOGISTS European Society of Cardiology
35
36 DEFINING THE PROBLEM OLD VS NEW JNC 7/8 ACC/AHA 2017 Stage 2 - Hypertension >160/100 Stage 1 - Hypertension Pre-Hypertension Stage 2 - Hypertension / />80 Stage 1 - Hypertension /<80 Elevated BP Normal <120/<80 Normal 32% of US pop 46% of US pop

37 GRAPHICAL 2017 GUIDELINES
38

39 ASCVD RISK ESTIMATOR

40 ASCVD RISK ESTIMATOR

41 ASCVD RISK ESTIMATOR

42 ASCVD RISK ESTIMATOR

43 ASCVD RISK REDUCTION SCENARIOS

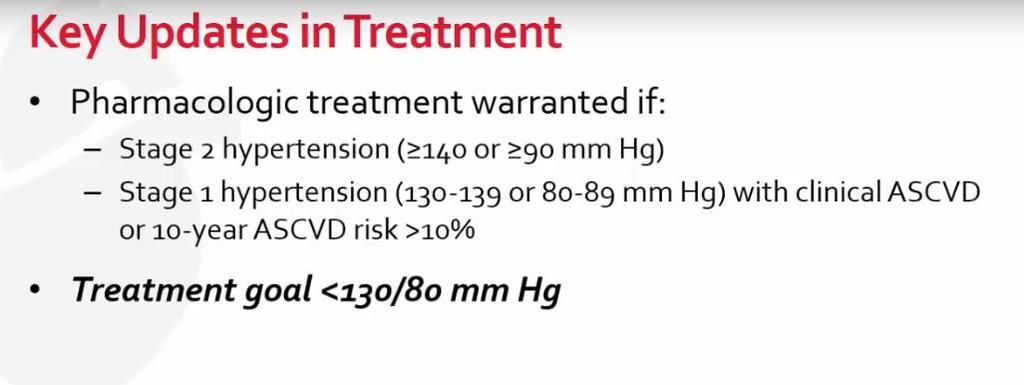
44 UPDATES IN CLASSIFYING HYPERTENSION Diet/Lifestyle Medications CAD ASCVD >10%
45
46
47
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
The earlier BP control the better cardiovascular outcome. Jin Oh Na Cardiovascular center Korea University Medical College
 The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
TREATMENT OF GERIATRIC HYPERTENSION: THE SPRINT TRIAL AND RECENT GUIDELINES
 Treatment of Geriatric Hypertension: the SPRINT Trial and the Evolving Systolic Blood Pressure Target TREATMENT OF GERIATRIC HYPERTENSION: THE SPRINT TRIAL AND RECENT GUIDELINES MARK A. SUPIANO, M.D. PROFESSOR
Treatment of Geriatric Hypertension: the SPRINT Trial and the Evolving Systolic Blood Pressure Target TREATMENT OF GERIATRIC HYPERTENSION: THE SPRINT TRIAL AND RECENT GUIDELINES MARK A. SUPIANO, M.D. PROFESSOR
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD?
 Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Blood Pressure Measurement in SPRINT
 Blood Pressure Measurement in SPRINT Karen C. Johnson, MD, MPH, FAHA Vice Chair, SPRINT Steering Committee University of Tennessee Health Science Center, Department of Preventive Medicine For the SPRINT
Blood Pressure Measurement in SPRINT Karen C. Johnson, MD, MPH, FAHA Vice Chair, SPRINT Steering Committee University of Tennessee Health Science Center, Department of Preventive Medicine For the SPRINT
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD
 New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Recent Hypertension Guidelines
 Recent Hypertension Guidelines Lawrence J. Fine, MD, DrPH, FAHA Division of Cardiovascular Sciences NHLBI/NIH February 19, 2014 Disclosures: Member of Panel Appointed to the Eighth Joint National Committee
Recent Hypertension Guidelines Lawrence J. Fine, MD, DrPH, FAHA Division of Cardiovascular Sciences NHLBI/NIH February 19, 2014 Disclosures: Member of Panel Appointed to the Eighth Joint National Committee
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA
 Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
SPRINT: Consequences for CKD patients
 SPRINT: Consequences for CKD patients 29 e Workshop Nierziekten Papendal 2018 December 12, 2018 MICHAEL ROCCO, MD, MSCE VARDAMAN M. BUCKALEW JR. PROFESSOR OF MEDICINE PROFESSOR OF PUBLIC HEALTH SCIENCES
SPRINT: Consequences for CKD patients 29 e Workshop Nierziekten Papendal 2018 December 12, 2018 MICHAEL ROCCO, MD, MSCE VARDAMAN M. BUCKALEW JR. PROFESSOR OF MEDICINE PROFESSOR OF PUBLIC HEALTH SCIENCES
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH)
") Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Unpacking Recent Hypertension Guidelines
 Unpacking Recent Hypertension Guidelines Lawrence J. Fine, MD, DrPH, FAHA Division of Cardiovascular Sciences NHLBI/NIH August 21, 2014 Disclosures: Member of Panel Appointed to the Eighth Joint National
Unpacking Recent Hypertension Guidelines Lawrence J. Fine, MD, DrPH, FAHA Division of Cardiovascular Sciences NHLBI/NIH August 21, 2014 Disclosures: Member of Panel Appointed to the Eighth Joint National
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Hypertension: 2016 Clinical Update
 PHASE Safety Net Community Benefit Hypertension: 2016 Clinical Update Presented by: Joseph Young, MD Hypertension Clinical Lead Kaiser Permanente Northern California October 6, 2016 Dr. Joseph Young Hypertension
PHASE Safety Net Community Benefit Hypertension: 2016 Clinical Update Presented by: Joseph Young, MD Hypertension Clinical Lead Kaiser Permanente Northern California October 6, 2016 Dr. Joseph Young Hypertension
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
None. Disclosure: Relationships with Industry Conflicts of Interests. Learning Objectives: Participants will be able to:
 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Evaluation and Management of Hypertension in Women. Vesna D. Garovic, M.D. Moscow, Russia, December 2016
 Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Hypertension Guidelines 2017
 Hypertension Guidelines 2017 (American College of Cardiology and the American Heart Association) In 1977, the 1st comprehensive guideline for detection, evaluation, and management of high BP was published,
Hypertension Guidelines 2017 (American College of Cardiology and the American Heart Association) In 1977, the 1st comprehensive guideline for detection, evaluation, and management of high BP was published,
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
New Clinical Trends in Geriatric Medicine. April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine
 New Clinical Trends in Geriatric Medicine April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine Objectives Review current guidelines for blood pressure (BP) control in older adults
New Clinical Trends in Geriatric Medicine April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine Objectives Review current guidelines for blood pressure (BP) control in older adults
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Optimal blood pressure targets in chronic kidney disease
 Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
2. Measurement Specifications 3. Patient Messaging 4. Provider Messaging Other Recent Guidelines
 Measure Up/Pressure Down Response to the Release of 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National
Measure Up/Pressure Down Response to the Release of 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2018
 MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly
 Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly Paul Muntner, PhD MHS Professor and Vice Chair Department of Epidemiology University of Alabama
Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly Paul Muntner, PhD MHS Professor and Vice Chair Department of Epidemiology University of Alabama
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Supplement materials:
 Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Consensus Core Set: Cardiovascular Measures Version 1.0
 Consensus Core Set: Cardiovascular s NQF 0330 Hospital 30-day, all-cause, riskstandardized readmission rate (RSRR) following heart failure hospitalization 0229 Hospital 30-day, all-cause, riskstandardized
Consensus Core Set: Cardiovascular s NQF 0330 Hospital 30-day, all-cause, riskstandardized readmission rate (RSRR) following heart failure hospitalization 0229 Hospital 30-day, all-cause, riskstandardized
NIH Public Access Author Manuscript JAMA Intern Med. Author manuscript; available in PMC 2015 August 01.
 NIH Public Access Author Manuscript Published in final edited form as: JAMA Intern Med. 2014 August ; 174(8): 1397 1400. doi:10.1001/jamainternmed.2014.2492. Prevalence and Characteristics of Systolic
NIH Public Access Author Manuscript Published in final edited form as: JAMA Intern Med. 2014 August ; 174(8): 1397 1400. doi:10.1001/jamainternmed.2014.2492. Prevalence and Characteristics of Systolic
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Hypertension Guidelines: Lessons for Primary Care. Paul A James MD Professor and Chair Department of Family Medicine University of Washington
 Hypertension Guidelines: Lessons for Primary Care Paul A James MD Professor and Chair Department of Family Medicine University of Washington Disclaimer and Financial Disclosure I have no financial interests
Hypertension Guidelines: Lessons for Primary Care Paul A James MD Professor and Chair Department of Family Medicine University of Washington Disclaimer and Financial Disclosure I have no financial interests
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Controlling Hypertension in Primary Care: Hitting a moving target?
 Controlling Hypertension in Primary Care: Hitting a moving target? David J. Hyman, MD,MPH Professor of Medicine and Family & Community Medicine Chief, Section General Medicine Baylor College of Medicine
Controlling Hypertension in Primary Care: Hitting a moving target? David J. Hyman, MD,MPH Professor of Medicine and Family & Community Medicine Chief, Section General Medicine Baylor College of Medicine
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
PHASE Preventing Heart Attacks & Strokes Everyday
 PHASE Preventing Heart Attacks & Strokes Everyday Welcome to the PHASE Learning Community! Joseph D. Young, MD Kaiser Permanente Northern California Jean Nudelman Kaiser Permanente Northern California
PHASE Preventing Heart Attacks & Strokes Everyday Welcome to the PHASE Learning Community! Joseph D. Young, MD Kaiser Permanente Northern California Jean Nudelman Kaiser Permanente Northern California
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Blood pressure treatment target in diabetes. Should it be <130 mmhg?
 Blood pressure treatment target in diabetes Should it be
Blood pressure treatment target in diabetes Should it be
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Consensus Core Set: ACO and PCMH / Primary Care Measures Version 1.0
 Consensus Core Set: ACO and PCMH / Primary Care s 0018 Controlling High Blood Pressure patients 18 to 85 years of age who had a diagnosis of hypertension (HTN) and whose blood pressure (BP) was adequately
Consensus Core Set: ACO and PCMH / Primary Care s 0018 Controlling High Blood Pressure patients 18 to 85 years of age who had a diagnosis of hypertension (HTN) and whose blood pressure (BP) was adequately
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
What s the evidence, why do guidelines differ, and what should the GP do?
 What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
2/9/2017. Financial Disclosures/Unapproved Use. Achieving Harmony in Blood Pressure Guidelines Around the Globe. Roger S. Blumenthal, MD.
 Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Hypertension Controversies: SPRINTing to New Goals
 Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
2016 Update in Geriatrics Elizabeth Eckstrom, MD, MPH Oregon Health & Science University Oregon Geriatrics Society October 7, 2016
 2016 Update in Geriatrics Elizabeth Eckstrom, MD, MPH Oregon Health & Science University Oregon Geriatrics Society October 7, 2016 I have no conflicts of interest Photos thanks to Google images This year
2016 Update in Geriatrics Elizabeth Eckstrom, MD, MPH Oregon Health & Science University Oregon Geriatrics Society October 7, 2016 I have no conflicts of interest Photos thanks to Google images This year
Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine
 Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine The Scope of Optimal BP BP Reduction CV outcomes & mortality CKD progression - Albuminuria - egfr decline
Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine The Scope of Optimal BP BP Reduction CV outcomes & mortality CKD progression - Albuminuria - egfr decline
Retour sur le congrès de l AHA 2017
 Retour sur le congrès de l AHA 2017 Paul Poirier MD, PhD, FRCPC, FACC, FAHA, FCCS Professeur Faculté de pharmacie Université Laval Responsable du programme de prévention/réadaptation cardiaque Canagliflozin
Retour sur le congrès de l AHA 2017 Paul Poirier MD, PhD, FRCPC, FACC, FAHA, FCCS Professeur Faculté de pharmacie Université Laval Responsable du programme de prévention/réadaptation cardiaque Canagliflozin
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Bress AP, Bellows BK, King JB, et al. Cost-effectiveness of
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Bress AP, Bellows BK, King JB, et al. Cost-effectiveness of
Status Report on the NHLBI-Sponsored CVD Prevention Guidelines
 Status Report on the NHLBI-Sponsored CVD Prevention Guidelines HIGH BLOOD PRESSURE Paul A. James, M.D. Roy J. and Lucille A. Carver College of Medicine The University of Iowa Iowa City IA NHLBI Adult CVD
Status Report on the NHLBI-Sponsored CVD Prevention Guidelines HIGH BLOOD PRESSURE Paul A. James, M.D. Roy J. and Lucille A. Carver College of Medicine The University of Iowa Iowa City IA NHLBI Adult CVD
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
Update in Outpatient Medicine ACP Scientific Session November 12, 2016
 Update in Outpatient Medicine ACP Scientific Session November 12, 2016 Robert Gluckman MD, MACP Chief Medical Officer Providence Health Plans Disclosures Stock Holdings Abbott Labs Abbvie Bristol Myers
Update in Outpatient Medicine ACP Scientific Session November 12, 2016 Robert Gluckman MD, MACP Chief Medical Officer Providence Health Plans Disclosures Stock Holdings Abbott Labs Abbvie Bristol Myers
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
Making Sense of the US Hypertension Guideline in 2018
 Making Sense of the US Hypertension Guideline in 2018 William J. Elliott, M.D., Ph.D. 04 MAY 18 Presenter Disclosure Information William J. Elliott, M.D., Ph.D. Making Sense of the US Hypertension Guideline
Making Sense of the US Hypertension Guideline in 2018 William J. Elliott, M.D., Ph.D. 04 MAY 18 Presenter Disclosure Information William J. Elliott, M.D., Ph.D. Making Sense of the US Hypertension Guideline
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3)
") Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
Hypertension JNC 8 (2014)
") Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Implications of Drug-related Increases in Blood Pressure
 Implications of Drug-related Increases in Blood Pressure Preston M. Dunnmon, MD, FACP, FACC Division of Cardiovascular and Renal Products US Food and Drug Administration July 18, 2012 Disclaimer The findings
Implications of Drug-related Increases in Blood Pressure Preston M. Dunnmon, MD, FACP, FACC Division of Cardiovascular and Renal Products US Food and Drug Administration July 18, 2012 Disclaimer The findings
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
Osama Sanad (MD) Prof. of Cardiology Benha University 2016
 Prof. of Cardiology Benha University 2016") Osama Sanad (MD) Prof. of Cardiology Benha University 2016 Back in time. 1912 Back in time. 1912 No body knows that hypertension is a lethal disease Hypertension in 1940s Among anti-hypertensives mentioned
Osama Sanad (MD) Prof. of Cardiology Benha University 2016 Back in time. 1912 Back in time. 1912 No body knows that hypertension is a lethal disease Hypertension in 1940s Among anti-hypertensives mentioned
J-curve Revisited. An Analysis of Blood Pressure and Cardiovascular Events in the Treating to New Targets (TNT) Trial
 Trial") J-curve Revisited An Analysis of Blood Pressure and Cardiovascular Events in the Treating to New Targets (TNT) Trial Sripal Bangalore, MD, MHA, Franz H Messerli, MD, Chuan-Chuan Wun, PhD, Andrea L. Zuckerman,
J-curve Revisited An Analysis of Blood Pressure and Cardiovascular Events in the Treating to New Targets (TNT) Trial Sripal Bangalore, MD, MHA, Franz H Messerli, MD, Chuan-Chuan Wun, PhD, Andrea L. Zuckerman,
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Objective & Outline. How the JNC Process Has Evolved. Expertise Represented on JNC 8 Panel
 Implementation: Joint National Committee on High Blood Pressure JNC 8 Joel Handler, MD Kaiser Permanente Care Management Institute Hypertension Lead Southern California Permanente Group Objective & Outline
Implementation: Joint National Committee on High Blood Pressure JNC 8 Joel Handler, MD Kaiser Permanente Care Management Institute Hypertension Lead Southern California Permanente Group Objective & Outline
Hypertension: Update
 Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Health Benefits of Lowering Sodium Intake in the US
 Health Benefits of Lowering Sodium Intake in the US Lawrence J Appel, MD, MPH Professor of Medicine, Epidemiology and International Health (Human Nutrition) Director, Welch Center for Prevention, Epidemiology
Health Benefits of Lowering Sodium Intake in the US Lawrence J Appel, MD, MPH Professor of Medicine, Epidemiology and International Health (Human Nutrition) Director, Welch Center for Prevention, Epidemiology
HYPERTENSION: WHAT'S YOUR GOAL?
 HYPERTENSION: WHAT'S YOUR GOAL? SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-243-L01-P 0.1 CEU/1.0 hr Activity Type: Application-Based Learning Objectives for Pharmacists: Upon completion of this CPE activity
HYPERTENSION: WHAT'S YOUR GOAL? SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-243-L01-P 0.1 CEU/1.0 hr Activity Type: Application-Based Learning Objectives for Pharmacists: Upon completion of this CPE activity