Ventriculo-arterial coupling and diastolic elastance. MasterclassIC Schiermonnikoog 2015
|
|
|
- Erin Randall
- 5 years ago
- Views:
Transcription
1 Ventriculo-arterial coupling and diastolic elastance MasterclassIC Schiermonnikoog 2015
2 Ventriculo-arterial coupling Dynamic interaction between heart and systemic circulation (modulation of compliance / stiffness / resistance) allowing the system to provide adequate CO and arterial pressures necessary for sufficient organ perfusion under different circumstances Optimizes cardiovascular performance and cardiac energetics

3 Ventriculo-arterial coupling Cardiac contractility End-systolic arterial pressure Cardiac contractility End-systolic arterial pressure EDV Low ESV EDV Low ESV EDV Normal ESV EDV High ESV EDV High ESV EDV Normal ESV

4 Diastole Systole Baseline LVEF 70% Norepinephrine LVEF 40% Veillard-Baron A. Ann Int Care 2011;1:6
5 Ventriculo-arterial coupling Ratio of arterial- to ventricular elastance (Ea/Ees) Ea/Ees approximating unity is optimal for the system (adequate SV with lowest possible energetic consumption) Ees is the slope of the end-systolic pressure-volume relationship Ea represents the total afterload of LV and is the capability of the arterial vessels to increase pressure when LV stroke volume increases
6 LVESP Ees Ea LVEDP ESV EDV
7
8
9 Ea1 Ea2
10 Effects of increased afterload in normal and failing heart 120" 100" Stroke'volume'(mL)' 80" 60" 40" 20" 0" 0" 25" 50" 75" 100" 125" 150" Mean'arterial'pressure'(mmHg)'



 EDV E e Chen CH.")
11 1 Stroke Volume End-systolic pressure = 0.9 systolic blood pressure 3 2 Pressure at onset of injection = diastolic blood arterial pressure Ees Ea 4 End-Diastolic pressure = (0.596 E/e )? V0 5 ESV Single beat method by Chen (Stroke volume, SBP, DBP, isovolumic contraction time and ejection time) EDV E e Chen CH. J Am Col Cardiol 2001;38:
12 V-A decoupling (Ea/Ees > 1) Due to decreased Ees Due to decreased Ea Acute heart failure Acute systemic hypertension Cardiac surgery Acute systemic hypotension Could be an additional clue what is wrong and how it should be treated
13 Levosimendan and V-A coupling Bolus Levosimendan of 12 μg followed by 0.1 μg/kg/min 3 Ea/Ees 2,5 2 1,5 1 0,5 0 Before After Ischemic cardiomyopathy Guarracino F. Acta Anaesthesiol Scand 2007;51:
14 V-A decoupling in sepsis Septic shock Median 1.81 (IQR ) Critically ill without septic shock Median 1.07 (IQR ) Frequency Frequency Ea/Ees (sb) ratio Ea usually increases due to pharmacologic vasoconstriction Ea/Ees (sb) ratio Guarracino F. Crit Care 2014;18:R80
15 Levosimendan and myocardial depression in sepsis Levosimendan Dobutamine Baseline 24 h Baseline 24 h EDVI (ml/m 2 ) 75.8 ± ± 24.6 ** 84.2 ± ± 26.4 ESVI (ml/m 2 ) 46.7 ± ± 19.4 ** 52.4 ± ± 25.3 LVEF (%) 37.1 ± ± 8.4 ** 37.3 ± ± Before After ** ** SVI LVSWI SVI LVSWI Levosimendan Dobutamine Morelli A. Intensive Care Med 2005;31:
16 Ees (lev) Ees (base) Ea (lev) Ea (base)
17
18


19 Ventriculo-arterial coupling in aortic arch replacement Ees Ea Wegmann A. PLOS ONE 2014;9:e103588


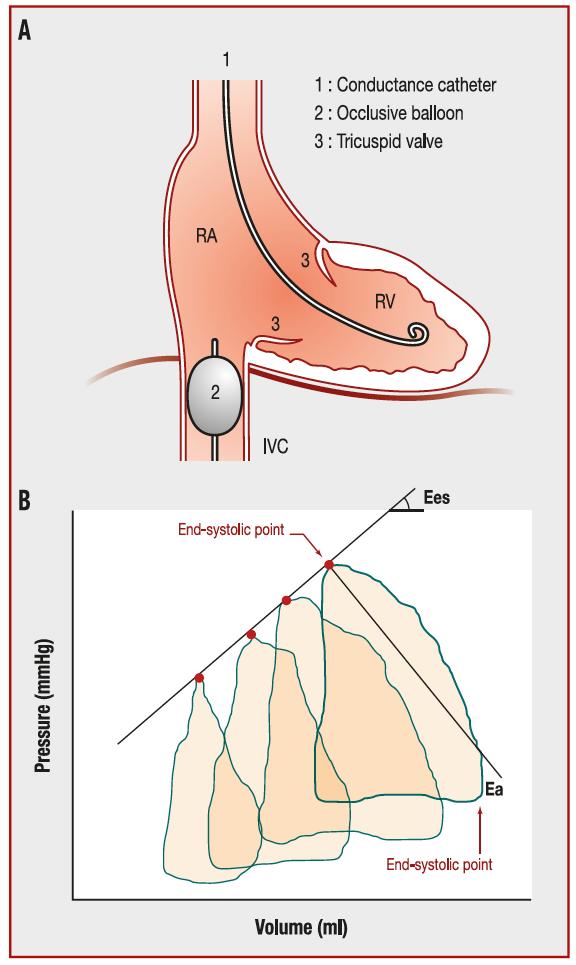
20 Right ventricle Acute Pulmonary Hypertension Chronic Minutes C Heterometric adaption Homeometric adaption Hypertrophy homeometric Dilatation heterometric Decrease afterload Increase afterload
21
22 Pressure Ees Ees = (Pmax-mPAP)/Sv Ea = mpap/sv Ea ESP Ea/Ees = (ESP/SV) / (ESP/ESV) = ESV/SV Normal ESV Volume EDV Increase in Ea/Ees ratio is invariably associated with EDV Vanderpool RR. Heart 2015
23 RV diastolic function Active relaxation Stiffness of the right ventricle
24
25
26 Right ventricular relaxation in PHT 150 P < 0.05 RV τ (ms) Controle PHT 18.3 ± 3.2 mmhg 53.3 ± 32.4 mmhg N = 25 Murch SD. Pulm Circ 2015;5:
27 RV τ correlates with RV DP R = 0.93, P < Minimal RV DP (mmhg) RV τ (ms) Murch SD. Pulm Circ 2015;5:
28 Right ventricular pressure Diastolic stiffness correlates with RAP and SV Right ventricular volume Rain S. Circulation 2013;128:
29 Mild PHT decreases LV relaxation 18 ** ** 14 LVEDP (mmhg) X LVEDV (ml) X Normal VCO E/E (lateral) Change in cardiac output after VCO (%) Control DD IPAH Control DD IPAH Kasner M. Am J Respir Crit Care Med 2012;186:
30 Ea/Ees changes with different medications Drug Ea/Ees Dobutamine Decrease Levosimendan Decrease Milrinone Decrease Norepinephrine Decrease

31 Ea/Ees Isovolemic CP RVEF Ejection time RV dilatation Inhaled NO, PGI, milrinone RV pressure PDE-3/Levosimendan Dobutamine MVO2 Diuretics/CRRT T3 insufficiency Open FO RV output Hypoxemia RCA only perfused during diastole RV ischemia Vasopressin LV preload Cardiac output Organ failure Septal shift
32 Effect of fluid challenge on EA in sepsis N = Normotensive Ea 1.81 Sepsis N = 81 N=9 N = 18 Preload responder Hypotensive N = 27 Ea Preload nonresponder Pressure responders Ea 12 ± 7% Pressure nonresponders N=9 N=9 Explains why some septic patients increase CO without improving blood pressure after a FC Monge García MI. Intensive Care Med 2015;41:
33 Hypotension - will a fluid challenge help? Increased SV not always results in a higher arterial pressure (dependent on arterial tone) Arterial elastance (Ea) is the best integrative parameter of overall arterial system behavior
34 LVESP Ees Ea LVEDP ESV EDV
35 ABP (mmhg) SVI (ml/m2) Time (s) ABP SVI Pressure (mmhg) Time (s) CVP Ppc Paw Ppl
36 Dynamic arterial elastance Defined by ratio PPV/SVV during single MV breath N =25 - MAP responder 16, MAP non-responder 9 Responder# Non7responder# Responder" Non7responder" MAP$(mmHg)$ 100# 90# 80# 70# 60# 50# 40# Before# A0er# Cardiac'output'(l/min)' 9" 8" 7" 6" 5" 4" 3" 2" Before" A0er" Responder" Non4responder" Dynamic(arterial(elastance( 2" 1,5" 1" 0,5" 0" Before" A-er" García MIM. Crit Care 2011;15:R15
37 Dynamic arterial elastance Prediction of volume expansion on MAP AUC 95% CI Eadyn ± SVR ± MAP ± PP/SV 0.50 ± García MIM. Crit Care 2011;15:R15
# 3\" 2,5\" 2\" 1,5\" 1\" 0,5\" C\"(mL/mmHg)\" 2\" 1,5\" 1\" 0,5\" SVR$(dyn*s*cm-5)$ 2000\" 1500\"")
 García MIM.")
38 N = VEs All fluid responders (increase CO 10%) Eadyn& 1,4" 1,2" 1" 0,8" 0,6" 0,4" 0,2" *** Ea#(mmHg/mL)# 3" 2,5" 2" 1,5" 1" 0,5" C"(mL/mmHg)" 2" 1,5" 1" 0,5" SVR$(dyn*s*cm-5)$ 2000" 1500" 1000" 500" 0" Responder" Non2Responder" 0" Responder" Non1Responder" 0" Responder" Non0Responder" 0" Responder" Non/Responder" MAP responders defined by increase MAP 10%) García MIM. Crit Care 2014;18:626
39 Predicting MAP after fluid challenge García MIM. Crit Care 2014;18:626
![Eadyn also predicts MAP after NE N = 35 - Septic shock - decrease in NE 0.04 μg/kg/min (13 [37%] were NE responders - MAP > 15%) 2.0 1.8 AUC 95% CI 1.6 Eadyn 1.4 1.2 1.](/docs-images/90/104455125/images/40-2.jpg "0 0.8 Eadyn 0.87 0.72-0.96 SVR 0.54 0.54-0.77 0.6 0.4 Compliance 0.61 0.43-0.77 Non-responders Responders < 0.90 gives 70% change of MAP Guinot PG.")
40 Eadyn also predicts MAP after NE N = 35 - Septic shock - decrease in NE 0.04 μg/kg/min (13 [37%] were NE responders - MAP > 15%) AUC 95% CI 1.6 Eadyn Eadyn SVR Compliance Non-responders Responders < 0.90 gives 70% change of MAP Guinot PG. Crit Care 2015;19:14
41 Conclusions Estimation of the Ea/Ees ratio may provide another clue for a rational therapeutic choice Early right ventricular dysbalance in Ea/Ees ratio immediately results in increased EDV with septal shift and compromise of left ventricle In a FR patient with hypotension a Eadyn > 0.8 predicts an increase in MAP
How to resuscitate the patient in early sepsis? A physiological approach. J.G. van der Hoeven, Nijmegen
 How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
Right Ventricle. Interaction with the pulmonary circulation. Fellowship Intensive Care Nijmegen
 Right Ventricle Interaction with the pulmonary circulation Fellowship Intensive Care Nijmegen Normal right ventricle PAP 25/10 EF 62 ± 8% Constant low pressure perfusion of the lung Maintain low RA pressure
Right Ventricle Interaction with the pulmonary circulation Fellowship Intensive Care Nijmegen Normal right ventricle PAP 25/10 EF 62 ± 8% Constant low pressure perfusion of the lung Maintain low RA pressure
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Sepsis and septic shock Practical hemodynamic consequences. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities
 The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling. What is the pathophysiology at presentation?
 Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling What is the pathophysiology at presentation? Ventricular-arterial coupling elastance Central arterial pressure
Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling What is the pathophysiology at presentation? Ventricular-arterial coupling elastance Central arterial pressure
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Sepsis and septic shock
 Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
RV dysfunction and failure PATHOPHYSIOLOGY. Adam Torbicki MD, Dept Chest Medicine Institute of Tuberculosis and Lung Diseases Warszawa, Poland
 RV dysfunction and failure PATHOPHYSIOLOGY Adam Torbicki MD, Dept Chest Medicine Institute of Tuberculosis and Lung Diseases Warszawa, Poland Normal Right Ventricle (RV) Thinner wall Weaker myocytes Differences
RV dysfunction and failure PATHOPHYSIOLOGY Adam Torbicki MD, Dept Chest Medicine Institute of Tuberculosis and Lung Diseases Warszawa, Poland Normal Right Ventricle (RV) Thinner wall Weaker myocytes Differences
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS
 Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
SymBioSys Exercise 2 Cardiac Function Revised and reformatted by C. S. Tritt, Ph.D. Last updated March 20, 2006
 SymBioSys Exercise 2 Cardiac Function Revised and reformatted by C. S. Tritt, Ph.D. Last updated March 20, 2006 The goal of this exercise to explore the behavior of the heart as a mechanical pump. For
SymBioSys Exercise 2 Cardiac Function Revised and reformatted by C. S. Tritt, Ph.D. Last updated March 20, 2006 The goal of this exercise to explore the behavior of the heart as a mechanical pump. For
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Review of Cardiac Mechanics & Pharmacology 10/23/2016. Brent Dunworth, CRNA, MSN, MBA 1. Learning Objectives
 Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Topics to be Covered. Cardiac Measurements. Distribution of Blood Volume. Distribution of Pulmonary Ventilation & Blood Flow
 Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Physiologic Based Management of Circulatory Shock Kuwait 2018
 Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
The Use of Dynamic Parameters in Perioperative Fluid Management
 The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART
 FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension
 ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Impedance Cardiography (ICG) Application of ICG for Hypertension Management
 Application of ICG for Hypertension Management") Application of ICG for Hypertension Management 1mA @ 100 khz Impedance Cardiography (ICG) Non-invasive Beat-to-beat Hemodynamic Monitoring Diastole Systole Aortic valve is closed No blood flow in the aorta
Application of ICG for Hypertension Management 1mA @ 100 khz Impedance Cardiography (ICG) Non-invasive Beat-to-beat Hemodynamic Monitoring Diastole Systole Aortic valve is closed No blood flow in the aorta
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)
of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)") Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Cardiac Output (C.O.) Regulation of Cardiac Output
 Regulation of Cardiac Output") Cardiac Output (C.O.) Is the volume of the blood pumped by each ventricle per minute (5 Litre) Stroke volume: Is the volume of the blood pumped by each ventricle per beat. Stroke volume = End diastolic
Cardiac Output (C.O.) Is the volume of the blood pumped by each ventricle per minute (5 Litre) Stroke volume: Is the volume of the blood pumped by each ventricle per beat. Stroke volume = End diastolic
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Impedance Cardiography (ICG) Method, Technology and Validity
 Method, Technology and Validity") Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Heart Pump and Cardiac Cycle. Faisal I. Mohammed, MD, PhD
 Heart Pump and Cardiac Cycle Faisal I. Mohammed, MD, PhD 1 Objectives To understand the volume, mechanical, pressure and electrical changes during the cardiac cycle To understand the inter-relationship
Heart Pump and Cardiac Cycle Faisal I. Mohammed, MD, PhD 1 Objectives To understand the volume, mechanical, pressure and electrical changes during the cardiac cycle To understand the inter-relationship
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
From PV loop to Starling curve. S Magder Division of Critical Care, McGill University Health Centre
 From PV loop to Starling curve S Magder Division of Critical Care, McGill University Health Centre Otto Frank 1890 s Frank-Starling Relationship ( The Law of the Heart ) The greater the initial stretch
From PV loop to Starling curve S Magder Division of Critical Care, McGill University Health Centre Otto Frank 1890 s Frank-Starling Relationship ( The Law of the Heart ) The greater the initial stretch
Hemodynamic monitoring beyond cardiac output
 Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Pulmonary hypertension and right ventricular failure
 Pulmonary hypertension and right ventricular failure Sven-Erik Ricksten Dept. Anaesthesiology and Intensive Care, Sahlgrenska Academy, University of Gothenburg, Sahlgrenska University Hospital, Gothenburg,
Pulmonary hypertension and right ventricular failure Sven-Erik Ricksten Dept. Anaesthesiology and Intensive Care, Sahlgrenska Academy, University of Gothenburg, Sahlgrenska University Hospital, Gothenburg,
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
Καθετηριασμός δεξιάς κοιλίας. Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ
 Καθετηριασμός δεξιάς κοιλίας Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ The increasing interest in pulmonary arterial hypertension (PAH), the increasing interest in implantation of LVADs, and the evolution
Καθετηριασμός δεξιάς κοιλίας Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ The increasing interest in pulmonary arterial hypertension (PAH), the increasing interest in implantation of LVADs, and the evolution
Heart Rate Control in sepsis and septic shock
 Heart Rate Control in sepsis and septic shock Antonia Koutsoukou Associate Professor of Intensive Care Medicine University of Athens/ Sotiria General Chest Diseases Hospital Introduction Sepsis, is a clinical
Heart Rate Control in sepsis and septic shock Antonia Koutsoukou Associate Professor of Intensive Care Medicine University of Athens/ Sotiria General Chest Diseases Hospital Introduction Sepsis, is a clinical
SIKLUS JANTUNG. Rahmatina B. Herman
 SIKLUS JANTUNG Rahmatina B. Herman The Cardiac Cycle Definition: The cardiac events that occur from the beginning of one heartbeat to the beginning of the next The cardiac cycle consists of: - Diastole
SIKLUS JANTUNG Rahmatina B. Herman The Cardiac Cycle Definition: The cardiac events that occur from the beginning of one heartbeat to the beginning of the next The cardiac cycle consists of: - Diastole
Cardiac Output MCQ. Professor of Cardiovascular Physiology. Cairo University 2007
 Cardiac Output MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 90- Guided by Ohm's law when : a- Cardiac output = 5.6 L/min. b- Systolic and diastolic BP
Cardiac Output MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 90- Guided by Ohm's law when : a- Cardiac output = 5.6 L/min. b- Systolic and diastolic BP
Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft
 Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft M. Buerke, K. Krohe, M. Russ, C. Schneider, H. Lemm, R. Prondzinsky, I. Friedrich,
Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft M. Buerke, K. Krohe, M. Russ, C. Schneider, H. Lemm, R. Prondzinsky, I. Friedrich,
Ventricular-Pulmonary Vascular Coupling after the Total Cavopulmonary Anastomosis (Fontan)
") Ventricular-Pulmonary Vascular Coupling after the Total Cavopulmonary Anastomosis (Fontan) 6th International Neonatal & Childhood Pulmonary Vascular Disease Conference Fontan Physiology Single ventricular
Ventricular-Pulmonary Vascular Coupling after the Total Cavopulmonary Anastomosis (Fontan) 6th International Neonatal & Childhood Pulmonary Vascular Disease Conference Fontan Physiology Single ventricular
Value of echocardiography in chronic dyspnea
 Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
Age-related changes in cardiovascular system. Dr. Rehab Gwada
 Age-related changes in cardiovascular system Dr. Rehab Gwada Objectives explain the main structural and functional changes in cardiovascular system associated with normal aging Introduction aging results
Age-related changes in cardiovascular system Dr. Rehab Gwada Objectives explain the main structural and functional changes in cardiovascular system associated with normal aging Introduction aging results
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Weeks 1-3:Cardiovascular
 Weeks 1-3:Cardiovascular Cardiac Output The total volume of blood ejected from the ventricles in one minute is known as the cardiac output. Heart Rate (HR) X Stroke Volume (SV) = Cardiac Output Normal
Weeks 1-3:Cardiovascular Cardiac Output The total volume of blood ejected from the ventricles in one minute is known as the cardiac output. Heart Rate (HR) X Stroke Volume (SV) = Cardiac Output Normal
Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment
 ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
BUSINESS. Articles? Grades Midterm Review session
 BUSINESS Articles? Grades Midterm Review session REVIEW Cardiac cells Myogenic cells Properties of contractile cells CONDUCTION SYSTEM OF THE HEART Conduction pathway SA node (pacemaker) atrial depolarization
BUSINESS Articles? Grades Midterm Review session REVIEW Cardiac cells Myogenic cells Properties of contractile cells CONDUCTION SYSTEM OF THE HEART Conduction pathway SA node (pacemaker) atrial depolarization
Special Lecture 10/28/2012
 Special Lecture 10/28/2012 HYPERTENSION Dr. HN Mayrovitz Special Lecture 10/28/2012 Arterial Blood Pressure (ABP) - Definitions ABP Review Indirect Oscillographic Method Resistance (R), Compliance (C)
Special Lecture 10/28/2012 HYPERTENSION Dr. HN Mayrovitz Special Lecture 10/28/2012 Arterial Blood Pressure (ABP) - Definitions ABP Review Indirect Oscillographic Method Resistance (R), Compliance (C)
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Supplemental methods Pericardium In several studies, it has been shown that the pericardium significantly modulates ventricular interaction. 1-4 Since ventricular interaction has
SUPPLEMENTAL MATERIAL Supplemental methods Pericardium In several studies, it has been shown that the pericardium significantly modulates ventricular interaction. 1-4 Since ventricular interaction has
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST ESC Congress 2011 Pathophysiology of HFPEF Vascular Remodeling & Pulmonary Hypertension Carolyn S.P. Lam MBBS, MRCP, MS Case Presentation 81 yo woman with dyspnoea &
DECLARATION OF CONFLICT OF INTEREST ESC Congress 2011 Pathophysiology of HFPEF Vascular Remodeling & Pulmonary Hypertension Carolyn S.P. Lam MBBS, MRCP, MS Case Presentation 81 yo woman with dyspnoea &
The Failing Systemic Right Ventricle European Society of Cardiology 2012
 The Failing Systemic Right Ventricle European Society of Cardiology 2012 I have nothing to disclose. Is the right ventricle an inherently weaker ventricle? Functionally single ventricle TGA (after atrial
The Failing Systemic Right Ventricle European Society of Cardiology 2012 I have nothing to disclose. Is the right ventricle an inherently weaker ventricle? Functionally single ventricle TGA (after atrial
Agenda เอกราช อร ยะช ยพาณ ชย. - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure 9/6/2016
 6 September 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Agenda - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure http://fullpulse.weebly.com/conversation
6 September 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Agenda - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure http://fullpulse.weebly.com/conversation
Disclosures. ICU Management of Advanced Lung Disease 5/9/2015. No Disclosures. All pictures from commercial sources
 Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Anesthesia for the cardiac compromised patient Right ventricular failure
 Anesthesia for the cardiac compromised patient 26th International Winter Symposium Steffen Rex Update in Cardiothoracic Anesthesia January 7th - 8th, 2011 Leuven, Belgium Dept. of Anesthesiology University
Anesthesia for the cardiac compromised patient 26th International Winter Symposium Steffen Rex Update in Cardiothoracic Anesthesia January 7th - 8th, 2011 Leuven, Belgium Dept. of Anesthesiology University
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Rationale for Prophylactic Support During Percutaneous Coronary Intervention
 Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Examen MMD Which of the following causes increased inotropy and chronotropy? A Ca gluconate B Glucagon C Atropine D Digoxin E Phenylephrine
 1-Which of the following causes an increase in HR in a denervated heart? A Pancuronium B Atropine C Propranolol D Norepinephrine E Neostigmine 2-Which of the following causes increased inotropy and chronotropy?
1-Which of the following causes an increase in HR in a denervated heart? A Pancuronium B Atropine C Propranolol D Norepinephrine E Neostigmine 2-Which of the following causes increased inotropy and chronotropy?
Das recht Ventrikel ist auch noch da! RV function The RV operates as. Physiology Not very sensitive to preload Good compliance of the free wall
 Das recht Ventrikel ist auch noch da! I.Michaux Intensive Care Medicine University Hospital CHU UCL Namur Mont-Godinne Belgium RV function The RV operates as a low pressure, volume pump, moving the blood
Das recht Ventrikel ist auch noch da! I.Michaux Intensive Care Medicine University Hospital CHU UCL Namur Mont-Godinne Belgium RV function The RV operates as a low pressure, volume pump, moving the blood
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล
 การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
Outline. Pathophysiology: Heart Failure. Heart Failure. Heart Failure: Definitions. Etiologies. Etiologies
 Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Cardiogenic shock: Current management
 Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Ventriculo-arterial decoupling in acutely altered hemodynamic states
 REVIEW Ventriculo-arterial decoupling in acutely altered hemodynamic states Fabio Guarracino 1 *, Rubia Baldassarri 1, Michael R Pinsky 2 This article is one of ten reviews selected from the Annual Update
REVIEW Ventriculo-arterial decoupling in acutely altered hemodynamic states Fabio Guarracino 1 *, Rubia Baldassarri 1, Michael R Pinsky 2 This article is one of ten reviews selected from the Annual Update
I have nothing to disclose.
 I have nothing to disclose. ESC Congress, München, 2012 Pulmonary Circulation and the Right and Left Ventricles Left Ventricle in Pulmonary Hypertension Robert Naeije Erasme University Hospital Brussels,
I have nothing to disclose. ESC Congress, München, 2012 Pulmonary Circulation and the Right and Left Ventricles Left Ventricle in Pulmonary Hypertension Robert Naeije Erasme University Hospital Brussels,
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
Disclosure Information : No conflict of interest
 Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Mechanisms of False Positive Exercise Electrocardiography: Is False Positive Test Truly False?
 Mechanisms of False Positive Exercise Electrocardiography: Is False Positive Test Truly False? Masaki Izumo a, Kengo Suzuki b, Hidekazu Kikuchi b, Seisyo Kou b, Keisuke Kida b, Yu Eguchi b, Nobuyuki Azuma
Mechanisms of False Positive Exercise Electrocardiography: Is False Positive Test Truly False? Masaki Izumo a, Kengo Suzuki b, Hidekazu Kikuchi b, Seisyo Kou b, Keisuke Kida b, Yu Eguchi b, Nobuyuki Azuma
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
An Integrated Approach to Study LV Diastolic Function
 An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
Cardiovascular hemodynamics in the stress echo lab with open-source software
 Cardiovascular hemodynamics in the stress echo lab with open-source software T. Bombardini, D. Cini, E. Picano Institute of Clinical Physiology of CNR, Pisa, Italy no conflict of interest Background Stress
Cardiovascular hemodynamics in the stress echo lab with open-source software T. Bombardini, D. Cini, E. Picano Institute of Clinical Physiology of CNR, Pisa, Italy no conflict of interest Background Stress
Cardiac Output Monitoring - 6
 Cardiac Output Monitoring - 6 How to use Wrexham s Cardiac Output Monitors. Wrexham Maelor Critical Care Version 02.05.16 Introduction Types of Devices: NICOM - Cheetah Oesophageal Doppler +/- Pulse Contour
Cardiac Output Monitoring - 6 How to use Wrexham s Cardiac Output Monitors. Wrexham Maelor Critical Care Version 02.05.16 Introduction Types of Devices: NICOM - Cheetah Oesophageal Doppler +/- Pulse Contour
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #12 Understanding Preload and Afterload
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #12 Understanding Preload and Afterload Cardiac output (CO) represents the volume of blood that is delivered
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #12 Understanding Preload and Afterload Cardiac output (CO) represents the volume of blood that is delivered
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Jan M. Headley, R.N. BS
 Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia.
 STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia. PART 1 Systems of care for STEMI. STEMI Management Coronary angiogram +/- stenting. Prehospital thrombolysis
STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia. PART 1 Systems of care for STEMI. STEMI Management Coronary angiogram +/- stenting. Prehospital thrombolysis
THE RIGHT VENTRICLE IN PULMONARY HYPERTENSION R. DRAGU
 THE RIGHT VENTRICLE IN PULMONARY HYPERTENSION R. DRAGU Cardiology Dept. Rambam Health Care Campus Rappaport Faculty of Medicine Technion, Israel Why the Right Ventricle? Pulmonary hypertension (PH) Right
THE RIGHT VENTRICLE IN PULMONARY HYPERTENSION R. DRAGU Cardiology Dept. Rambam Health Care Campus Rappaport Faculty of Medicine Technion, Israel Why the Right Ventricle? Pulmonary hypertension (PH) Right
CARDIOGENIC SHOCK. Antonio Pesenti. Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI)
") CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
DESCRIBE THE FACTORS AFFECTING CARDIAC OUTPUT.
 DESCRIBE THE FACTORS AFFECTING CARDIAC OUTPUT. BY: DISHA PRAKASH I MBBS, ROLL NO: 16M069 OBJECTIVES OF LEARNING Terminology and conceptual understanding of Cardiac Output. Factors regulating Cardiac Output.
DESCRIBE THE FACTORS AFFECTING CARDIAC OUTPUT. BY: DISHA PRAKASH I MBBS, ROLL NO: 16M069 OBJECTIVES OF LEARNING Terminology and conceptual understanding of Cardiac Output. Factors regulating Cardiac Output.
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
UPMC Critical Care
 UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
TOPIC : Cardiogenic Shock
 University of Ferrara Department of Morphology, Surgery and Experimental Medicine. Section of Anaesthesia and Intensive Care Medicine TOPIC : Cardiogenic Shock What is shock? Shock is a condition of inadequate
University of Ferrara Department of Morphology, Surgery and Experimental Medicine. Section of Anaesthesia and Intensive Care Medicine TOPIC : Cardiogenic Shock What is shock? Shock is a condition of inadequate
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
5/30/2014. Pulmonary Hypertension PULMONARY HYPERTENSION. mean PAP > 25 mmhg at rest. Disclosure: none
 Disclosure: Pulmonary Hypertension none James Ramsay MD Medical Director, CV ICU, Moffitt Hospital, UCSF PULMONARY HYPERTENSION mean PAP > 25 mmhg at rest Pulmonary Hypertension and Right Ventricular Dysfunction:
Disclosure: Pulmonary Hypertension none James Ramsay MD Medical Director, CV ICU, Moffitt Hospital, UCSF PULMONARY HYPERTENSION mean PAP > 25 mmhg at rest Pulmonary Hypertension and Right Ventricular Dysfunction:
Evaluation of Native Left Ventricular Function During Mechanical Circulatory Support.: Theoretical Basis and Clinical Limitations
 Review Evaluation of Native Left Ventricular Function During Mechanical Circulatory Support.: Theoretical Basis and Clinical Limitations Tohru Sakamoto, MD, PhD Left ventricular function on patients with
Review Evaluation of Native Left Ventricular Function During Mechanical Circulatory Support.: Theoretical Basis and Clinical Limitations Tohru Sakamoto, MD, PhD Left ventricular function on patients with
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Pre-discussion questions
 Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Fetal gene upregulation by 1-wk TAC is significantly increased in mice lacking RGS2.
 3562-RG-1 Supplementary Figure 1 Fetal gene upregulation by 1-wk is significantly increased in mice lacking RGS2. ANP(Nppa) /BNP(Nppb) A-type and B-type natriuretic peptide; β-mhc (Myh7) beta myosin heavy
3562-RG-1 Supplementary Figure 1 Fetal gene upregulation by 1-wk is significantly increased in mice lacking RGS2. ANP(Nppa) /BNP(Nppb) A-type and B-type natriuretic peptide; β-mhc (Myh7) beta myosin heavy
Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH
 Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH Javier Jimenez MD PhD FACC Director, Advanced Heart Failure and Pulmonary Hypertension Miami Cardiac & Vascular Institute
Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH Javier Jimenez MD PhD FACC Director, Advanced Heart Failure and Pulmonary Hypertension Miami Cardiac & Vascular Institute
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction
 Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
Clinical application of Arterial stiffness. pulse wave analysis pulse wave velocity
 Clinical application of Arterial stiffness pulse wave analysis pulse wave velocity Arterial system 1. Large arteries: elastic arteries Aorta, carotid, iliac, Buffering reserve: store blood during systole
Clinical application of Arterial stiffness pulse wave analysis pulse wave velocity Arterial system 1. Large arteries: elastic arteries Aorta, carotid, iliac, Buffering reserve: store blood during systole
Special Lecture 11/08/2013. Hypertension Dr. HN Mayrovitz
 Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Cardiovascular Physiology. Heart Physiology. Introduction. The heart. Electrophysiology of the heart
 Cardiovascular Physiology Heart Physiology Introduction The cardiovascular system consists of the heart and two vascular systems, the systemic and pulmonary circulations. The heart pumps blood through
Cardiovascular Physiology Heart Physiology Introduction The cardiovascular system consists of the heart and two vascular systems, the systemic and pulmonary circulations. The heart pumps blood through
Pulmonary Hypertension: Another Use for Viagra
 Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A
Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A