TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
|
|
|
- Alexandrina Preston
- 5 years ago
- Views:
Transcription
1 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD
2 Aortic Valve Pathology and Treatment


3 Valvular Aortic Stenosis in Adults Average Course (Post mortem data) Circulation 38 (Suppl. 5) 61, 1968
 AI, MI, MS AS Rappaport E: Am J Cardiol")
4 Medically Treated Valvular Disease Average Course (Survival) AI, MI, MS AS Rappaport E: Am J Cardiol 35:221, 1975
5 Valve Surgery Growth over 10 years ( ) Represents a growing public health problem!

6 Valve Anatomy 4 Valves Semilunar Pulmonic Aortic Atrioventricular Tricuspid Mitral
7 Aortic Valve Normal Valve 3 Leaflets Right Coronary ] Noncoronary ] Left Coronary ] cross-sectional area of about 3 cm sq

8 Aortic Valve Conduction system Anterior leaflet mitral valve
9 Clinical findings Exam Murmur Chest X-Ray ECG Imaging Echocardiography Angiography MRI Diagnostic Approach
10 Cardiac Cycle As ventricular pressure ( ) increases and exceeds atrial pressure ( ) atrioventricular valves close causing the S1 heart sound
 the semilunar valves close causing the S2")
11 Cardiac Cycle Aortic pressure ( ) exceeds Ventricular pressure ( ) the semilunar valves close causing the S2 heart sound
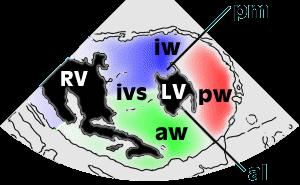

12 Transesophageal Echo LV short axis Papillary view
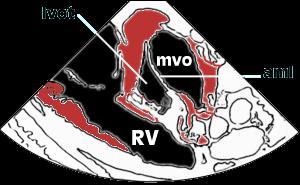

13 Transesophageal Echo LV short axis mitral view
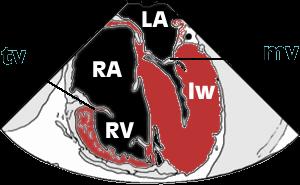

14 Transesophageal Echo Four chamber view



15 Cardiac Catheterization Left Coronary Right coronary


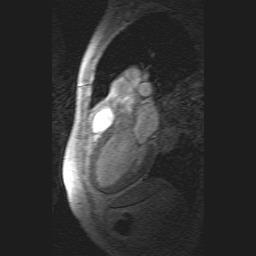
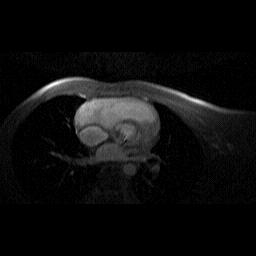
16 MRI The Future Aortic Regurgitation Trileaflet Pulmonary Valve Bileaflet Pulmonary Valve
17 Aortic Valve Stenosis Regurgitation
18 Preoperative Data: AVR Valvular Lesion 100% Insufficiency 13% Mixed 22% % of Patients 80% 60% 40% 28% 57% Stenosis 65% 20% 0% 13% 2% I II III IV NYHA Class


19 Aortic Stenosis Disease of the Elderly Symptoms begin: yrs. of age Causes: Scarring Calcification Rheumatic fever Bicuspid valve

20 Aortic Stenosis Pathophysiology Increased resistance to blood flow from the left ventricle to the aorta Increased work Left ventricular hypertrophy Smaller ventricular cavity Increased oxygen demand Can lead to ischemia Heart failure
21 Aortic Stenosis Symptoms Chest pain (angina) occurs during exertion blood supply to the enlarged heart muscle is inadequate Heart failure develops fatigue shortness of breath during exertion Syncope Exertion leads to peripheral arterial vasodilatation AS limits cardiac output preventing compensation Sudden Death
22 Aortic Stenosis Diagnosis Physical Examination Heart Murmur Heard over aortic area 2 nd right intercostal border Midsystolic murmur Radiates down left sternal border ECG Left ventricular hypertrophy

23 Aortic Stenosis Chest X-ray Prominent left ventricle


24 Aortic Stenosis Diagnosis Echocardiography Cardiac Cath >45 years Short Axis Long Axis
25 Aortic Stenosis Treatment Asymptomatic Regular follow-up Serial Echo Symptomatic Aortic valve area less than 1.2 cm 2 /M 2 Severe Aortic Stenosis Valve area 1cm 2 Mean Gradient >40 mm Hg (normal LV) Max vel> 4.0m/sec2 Medical Therapy Diuretics Surgical replacement before irreversible damage
26 Aortic Stenosis Survival Symptomatic Surgery vs Medical NEJM, Carabello 346 (9): 677 February 28, 2002


27 Aortic Regurgitation Increasing volume and pressure in the left ventricle Result: increased work ventricles thicken to compensate hypertrophy chambers dilate Eventually CHF
28 Aortic Regurgitation Rheumatic Fever Historical cause myxomatous degeneration aortic aneurysms & dissection bicuspid valve infective endocarditis
29 Aortic Regurgitation Symptoms Mild Asymptomatic heart murmur Severe Palpitations LVH Congestive heart failure Shortness of breath Fatigue Angina Reduce SBP during ventricular diastole Wide pulse pressure
30 Aortic Regurgitation Physical exam Murmur Heard with diaphragm Midsystolic ECG: LVH Chest X-ray cardiomegaly

31 Echo Aortic Regurgitation Cardiac Cath 20% of people with aortic regurgitation also have coronary artery disease

32 Aortic Regurgitation Treatment Mild Medical management Digoxin, Diuretics Calcium channel blocker Ace Moderate to severe: Surgery Cardiac Cath 20% of people with aortic regurgitation also have coronary artery disease
 -Stentless (porcine) Pulmonary Autograft Aortic")
33 Aortic Valve Replacement Possible Prostheses Mechanicals valves Homografts Engineered Tissue Valves -Stented (porcine or bovine) -Stentless (porcine) Pulmonary Autograft Aortic Remodeling




34 Mechanical Valve Products SJM Regent valve (bileaflet) Carbomedics Standard bileaflet valve Medtronic Hall tilting disc valve



35 Tissue Valve Products Stented Valve Stentless Valve Homograft Edwards Lifesciences Carpentier - Edwards Perimount valve St. Jude Medical Toronto SPV valve LifeNet Homograft

36 Stentless Aortic Valves Modeled after native aortic valve Eliminates residual stenosis caused by stents Near-normal hemodynamics Normalizes LV mass and performance


37 Stentless Porcine Valves Toronto SPV Valve Freestyle Valve


38 Sutureless Aortic Valves
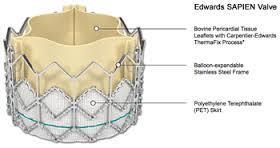
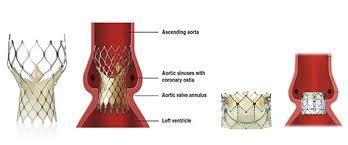
39 Percutaneous Aortic Valves

40 Stented Aortic Valves Obstructive to flow Decreased effective orifice areas Increased transvalvular pressure gradients Residual left ventricular hypertrophy Calcification at stent/tissue interfaces Rigid, non-compliant with aorta


41 Aortic Root Reconstruction Aortic Root Replacement Coronary Reimplantation

42 Aortic Root Remodeling Aortic valve preservation Remodeling of root geometry Coronary Reimplantation

43 Echo Stentless Freestyle Bioprosthesis Natural Valve


44 Valve Surgery Trends Durability Anticoagulation Lim JTCVS patients composite TE Risk 7% per pt yr

45 Mechanical Valves Thromboembolic event rate 1-4%/pt-year Anticoagulant related hemorrhage rate 2-5%/pt-year

46 Risk Factors for Thromboembolism Mechanical valve implant Atrial Fibrillation Increased LV cavity size/lv dysfunction Regional Wall Motion Abnormality Depressed Ejection Fraction Previous Thromboembolism Hypercoagulability
47 Anticoagulants - Coumarins Development/clinical use began in the 1920s Used for long-term anticoagulation therapy Oral anticoagulant Produces a functional deficiency of Vitamin K several clotting factors on Vitamin K Takes 36 hours to achieve a therapeutic blood level which will last 4-5 days Blood levels can vary patients must be checked regularly St. Jude Medical, Training and Education

48 Minimally Invasive Aortic Valve

49 Aortic Valve Freedom from Valve Dysfunction

50 Aortic Valve Complications Thromboembolism Anti-coagulant related hemorrhage Valve dysfunction/structural failure Para-valvular leak Re-operation Endocarditis Hemolysis Death
51 Aortic Valve Survival Early (hospital) death - 3-6% Time-related survival 5 years - 75% 10 years - 60% 15 years - 40% Mode of death Early due to CHF, hemorrhage, infection, CVA Sudden - 20% Device related - 20% CTSNet, Residents Section
52 Aortic Valve Risk Factors for Survival after AVR Advanced age Functional status (NHYA class) Depressed LV function (aortic incompetence) Coronary artery disease Presence of endocarditis Aneurysm of ascending aorta Mismatch of prosthesis and body size
Adult Cardiac Surgery
 Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease. Dr. HANAN ALBACKR
 Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Heart Valves: Before and after surgery
 Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should.
 What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Mitral Valve Disease. Prof. Sirchak Yelizaveta Stepanovna
 Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
By the end of this session, the student should be able to:
 Valvular Heart disease HVD By Dr. Ashraf Abdelfatah Deyab VHD- Objectives By the end of this session, the student should be able to: Define and classify valvular heart disease. Enlist the causes of acquired
Valvular Heart disease HVD By Dr. Ashraf Abdelfatah Deyab VHD- Objectives By the end of this session, the student should be able to: Define and classify valvular heart disease. Enlist the causes of acquired
Valvular Heart Disease
 Valvular Heart Disease MITRAL STENOSIS Pathophysiology rheumatic fever. calcific degeneration, malignant carcinoid disease, congenital mitral stenosis. SLE. The increased pressure gradient across the mitral
Valvular Heart Disease MITRAL STENOSIS Pathophysiology rheumatic fever. calcific degeneration, malignant carcinoid disease, congenital mitral stenosis. SLE. The increased pressure gradient across the mitral
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
Which one of the following echocardiographic profiles most strongly indicates the need for aortic valve replacement? FS [
 Question 46 A 45-year-old asymptomatic man returns for follow-up. He was diagnosed 10 years ago with aortic regurgitation due to a congentia lbicuspid aortic valve, He has never had endocarditis Which
Question 46 A 45-year-old asymptomatic man returns for follow-up. He was diagnosed 10 years ago with aortic regurgitation due to a congentia lbicuspid aortic valve, He has never had endocarditis Which
The Ross Procedure: Outcomes at 20 Years
 The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
Comprehensive Cardiology: Matters of the Heart Class III SARAH BEANLANDS RN BSCN MSC
 Comprehensive Cardiology: Matters of the Heart Class III SARAH BEANLANDS RN BSCN MSC Overview ACS continued Heart Failure Valvular Disorders and Endocarditis Diagnosis Nuclear stress test- stable angina
Comprehensive Cardiology: Matters of the Heart Class III SARAH BEANLANDS RN BSCN MSC Overview ACS continued Heart Failure Valvular Disorders and Endocarditis Diagnosis Nuclear stress test- stable angina
Valvular Stenosis and Regurgitation: Barriers to Flow
 Valvular Stenosis and Regurgitation: Barriers to Flow Presented By: Cynthia Webner BSN, RN,CCRN-CMC www.cardionursing.com CNEA 2009 1 Cardiac Valves Prevent Backward Flow Permit Forward Flow 2 www.cardionursing.com
Valvular Stenosis and Regurgitation: Barriers to Flow Presented By: Cynthia Webner BSN, RN,CCRN-CMC www.cardionursing.com CNEA 2009 1 Cardiac Valves Prevent Backward Flow Permit Forward Flow 2 www.cardionursing.com
PATIENT BOOKLET MEDTRONIC SURGICAL VALVE REPLACEMENT. Tissue Valve for Aortic and Mitral Valve Replacement
 PATIENT BOOKLET MEDTRONIC SURGICAL VALVE REPLACEMENT Tissue Valve for Aortic and Mitral Valve Replacement ARE MEDTRONIC SURGICAL TISSUE HEART VALVES RIGHT FOR YOU? Medtronic surgical heart valves are for
PATIENT BOOKLET MEDTRONIC SURGICAL VALVE REPLACEMENT Tissue Valve for Aortic and Mitral Valve Replacement ARE MEDTRONIC SURGICAL TISSUE HEART VALVES RIGHT FOR YOU? Medtronic surgical heart valves are for
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Echocardiographic Evaluation of Mitral Valve Prostheses
 Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
Tricuspid and Pulmonic Valve Disease
 Chapter 31 Tricuspid and Pulmonic Valve Disease David A. Tate Acquired disease of the right-sided cardiac valves is much less common than disease of the leftsided counterparts, possibly because of the
Chapter 31 Tricuspid and Pulmonic Valve Disease David A. Tate Acquired disease of the right-sided cardiac valves is much less common than disease of the leftsided counterparts, possibly because of the
Cardiac catheterisation in AS
 AORTIC STENOSIS MANAGEMENT OF VALVULAR AORTIC STENOSIS Dr Badri Paudel Third most common cardiovascular disease Most prevalent valvular heart disease in the world Commonest acquired valvular lesion with
AORTIC STENOSIS MANAGEMENT OF VALVULAR AORTIC STENOSIS Dr Badri Paudel Third most common cardiovascular disease Most prevalent valvular heart disease in the world Commonest acquired valvular lesion with
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Mitral Stenosis: A Review
 Cardiovascular Innovations and Applications Vol. x No. x (2016) x x ISSN 2009-8618 DOI 10.15212/CVIA.2016.0041 REVIEW Mitral Stenosis: A Review By C. Richard Conti, MD, MACC 1 1 Department of Medicine,
Cardiovascular Innovations and Applications Vol. x No. x (2016) x x ISSN 2009-8618 DOI 10.15212/CVIA.2016.0041 REVIEW Mitral Stenosis: A Review By C. Richard Conti, MD, MACC 1 1 Department of Medicine,
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD
 2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD David L Saint M.D. Tallahassee Memorial Hospital Southern Medical Group Division of Cardiothoracic
2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD David L Saint M.D. Tallahassee Memorial Hospital Southern Medical Group Division of Cardiothoracic
For more information about how to cite these materials visit
 Author: Michael Shea, M.D., 2008 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Author: Michael Shea, M.D., 2008 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new
 Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
CoreValve in a Degenerative Surgical Valve
 CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
PATIENT BOOKLET MEDTRONIC MITRAL AND TRICUSPID HEART VALVE REPAIR
 PATIENT BOOKLET MEDTRONIC MITRAL AND TRICUSPID HEART VALVE REPAIR ARE MEDTRONIC HEART VALVE REPAIR THERAPIES RIGHT FOR YOU? Prosthetic (artificial) heart valve repair products are used by physicians to
PATIENT BOOKLET MEDTRONIC MITRAL AND TRICUSPID HEART VALVE REPAIR ARE MEDTRONIC HEART VALVE REPAIR THERAPIES RIGHT FOR YOU? Prosthetic (artificial) heart valve repair products are used by physicians to
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
TSDA ACGME Milestones
 TSDA ACGME Milestones Short MW and Edwards JA. Assessing resident milestones using a CASPE March 2012 Short MW and Edwards JA. Assessing resident milestones using a CASPE March 2012 Short
TSDA ACGME Milestones Short MW and Edwards JA. Assessing resident milestones using a CASPE March 2012 Short MW and Edwards JA. Assessing resident milestones using a CASPE March 2012 Short
Long-term results (22 years) of the Ross Operation a single institutional experience
 of the Ross Operation a single institutional experience") Long-term results (22 years) of the Ross Operation a single institutional experience Authors: Costa FDA, Schnorr GM, Veloso M,Calixto A, Colatusso D, Balbi EM, Torres R, Ferreira ADA, Colatusso C Department
Long-term results (22 years) of the Ross Operation a single institutional experience Authors: Costa FDA, Schnorr GM, Veloso M,Calixto A, Colatusso D, Balbi EM, Torres R, Ferreira ADA, Colatusso C Department
A Health Care Professional s Guide Aortic Stenosis in Seniors
 A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Valve Stenosis and TAVR: Putting it all together.
 Aortic Valve Stenosis and TAVR: Putting it all together. Maria L. Held, MSN CNS Valve Clinic Coordinator at The Cleveland Clinic Alliance of Cardiovascular Professionals April 14 th, 2018 Brief Anatomy
Aortic Valve Stenosis and TAVR: Putting it all together. Maria L. Held, MSN CNS Valve Clinic Coordinator at The Cleveland Clinic Alliance of Cardiovascular Professionals April 14 th, 2018 Brief Anatomy
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
Aortic stenosis and regurgitation
 1 Aortic stenosis and regurgitation valvuloplasty and replacement Mitral regurgitation and stenosis valvuloplasty and repair/replacement 2 ASD PFO VSD PDA occlusion Left atrial appendage occlusion for
1 Aortic stenosis and regurgitation valvuloplasty and replacement Mitral regurgitation and stenosis valvuloplasty and repair/replacement 2 ASD PFO VSD PDA occlusion Left atrial appendage occlusion for
Indications and Late Results of Aortic Valve Repair
 Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Aortic valve disease. Acknowledgement for slides. Heart Valves 4/28/2018. Adopted from
 Aortic valve disease Senthil Kumar, MD 4.26.2018 28 th Annual Coming Together in Advanced Practice Conference Acknowledgement for slides Adopted from http://www.slideshare.net/ Dr. Anand Chockalingam Dr.
Aortic valve disease Senthil Kumar, MD 4.26.2018 28 th Annual Coming Together in Advanced Practice Conference Acknowledgement for slides Adopted from http://www.slideshare.net/ Dr. Anand Chockalingam Dr.
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
16 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 6900
 CLINICAL COMMUNIQUé 6 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 69 The Carpentier-Edwards PERIMOUNT Mitral Pericardial Valve, Model 69, was introduced into clinical
CLINICAL COMMUNIQUé 6 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 69 The Carpentier-Edwards PERIMOUNT Mitral Pericardial Valve, Model 69, was introduced into clinical
Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves
 Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves Speaker's name: I have the following potential conflicts of interest to report: Proctorship for Medtronic Agenda Failure modes
Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves Speaker's name: I have the following potential conflicts of interest to report: Proctorship for Medtronic Agenda Failure modes
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
Pulmonary Valve Regurgitation
 Pulmonary Valve Regurgitation Ziyad M. Hijazi, MD, FSCAI, FACC James A. Hunter,MD, University Chair Professor Of Pediatrics & Internal Medicine Rush Center For Congenital & Structural Heart Disease Rush
Pulmonary Valve Regurgitation Ziyad M. Hijazi, MD, FSCAI, FACC James A. Hunter,MD, University Chair Professor Of Pediatrics & Internal Medicine Rush Center For Congenital & Structural Heart Disease Rush
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
I (312) Mitral Regurgitation What Should You Know?
 Mitral Regurgitation What Should You Know?") Mitral Regurgitation What Should You Know? Table of Contents What is Mitral Regurgitation? 3 What are the Symptoms? 4 What are the risks? 5 Who Gets Mitral Regurgitation? 6 Diagnosing Mitral Regurgitation
Mitral Regurgitation What Should You Know? Table of Contents What is Mitral Regurgitation? 3 What are the Symptoms? 4 What are the risks? 5 Who Gets Mitral Regurgitation? 6 Diagnosing Mitral Regurgitation
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Gender Differences in Valvular Heart Disease. Linda D. Gillam, MD FESC Disclosure: Core Lab services Edwards Lifesciences
 Gender Differences in Valvular Heart Disease Linda D. Gillam, MD FESC Disclosure: Core Lab services Edwards Lifesciences Obstacles Interest in gender differences is a relatively new phenomenon Registries/RCT
Gender Differences in Valvular Heart Disease Linda D. Gillam, MD FESC Disclosure: Core Lab services Edwards Lifesciences Obstacles Interest in gender differences is a relatively new phenomenon Registries/RCT
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications
 24th Annual Advances in Heart Disease 16 December 2007 Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications Melvin D. Cheitlin, M.D. Emeritus Professor of
24th Annual Advances in Heart Disease 16 December 2007 Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications Melvin D. Cheitlin, M.D. Emeritus Professor of
UNDERSTANDING YOUR HEART VALVE. Mosaic Tissue Valve
 UNDERSTANDING YOUR HEART VALVE Mosaic Tissue Valve A Message to You from the Employees at Medtronic, Inc. We understand that having heart valve replacement surgery is an important change in your life.
UNDERSTANDING YOUR HEART VALVE Mosaic Tissue Valve A Message to You from the Employees at Medtronic, Inc. We understand that having heart valve replacement surgery is an important change in your life.
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
Cardiology. the Sounds: #7 HCM. LV Outflow Obstruction: Aortic Stenosis. (Coming Soon - HCM)
") A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital,
 Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital, Oslo, Norway Aortic regurgitation Prevalence in Framingham
Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital, Oslo, Norway Aortic regurgitation Prevalence in Framingham
Treatment of Bio-Prosthetic Valve Deterioration Using Transcatheter Techniques
 Treatment of Bio-Prosthetic Valve Deterioration Using Transcatheter Techniques Pablo Codner, Abid Assali, Hanna Vaknin-Assa, Katia Orvin, Ram Sharony, Leor Perl, Gabriel Greenberg, Marina Kupershmidt,
Treatment of Bio-Prosthetic Valve Deterioration Using Transcatheter Techniques Pablo Codner, Abid Assali, Hanna Vaknin-Assa, Katia Orvin, Ram Sharony, Leor Perl, Gabriel Greenberg, Marina Kupershmidt,
Iatrogenic pathology of the heart:
 Iatrogenic pathology of the heart: Complications of mitral valve plasty and replacement Patrick Bruneval D pt of Pathology Hôpital Européen Georges Pompidou Enterprise Interest None Mitral valve surgery
Iatrogenic pathology of the heart: Complications of mitral valve plasty and replacement Patrick Bruneval D pt of Pathology Hôpital Européen Georges Pompidou Enterprise Interest None Mitral valve surgery
Worldwide rheumatic fever is the most common cause of valve disease. In industrialized areas, valvular disease of old age predominates
 Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Disclosures. ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech
 Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease
 Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to:
 The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
TAVI and Valve Replacement Thromboprophylaxis. Warren Prokopiw Pharmacy Resident
 TAVI and Valve Replacement Thromboprophylaxis Warren Prokopiw Pharmacy Resident 2011-2012 Case Mr MW 76 yo Admitted 14 May for worsening CHF PMH: Aortic Stenosis, CVD (CABG x4 1980, PCI x3 stent 2008)
TAVI and Valve Replacement Thromboprophylaxis Warren Prokopiw Pharmacy Resident 2011-2012 Case Mr MW 76 yo Admitted 14 May for worsening CHF PMH: Aortic Stenosis, CVD (CABG x4 1980, PCI x3 stent 2008)
Patient/prosthesis mismatch: how to evaluate and when to act?
 Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz
 Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Cardiac Radiography. Jared D. Christensen, M.D.
 Cardiac Radiography Jared D. Christensen, M.D. Cardiac radiography Jared D. Christensen, M.D. Overview Basic Concepts Technique Normal anatomy Cases Technique 3 Standard Views Posterior-Anterior (PA) Anterior-Posterior
Cardiac Radiography Jared D. Christensen, M.D. Cardiac radiography Jared D. Christensen, M.D. Overview Basic Concepts Technique Normal anatomy Cases Technique 3 Standard Views Posterior-Anterior (PA) Anterior-Posterior
Congestive Heart Failure or Heart Failure
 Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
CONGENITAL AORTIC STENOSIS PRODUCED BY A UNICOMMISSURAL VALVE
 Brit. Heart J., 1965, 27, 505. CONGENITAL AORTIC STENOSIS PRODUCED BY A UNICOMMISSURAL VALVE WILLIAM C. BY ROBERTS AND ANDREW G. MORROW From the Clinic of Surgery, National Heart Institute, National Institutes
Brit. Heart J., 1965, 27, 505. CONGENITAL AORTIC STENOSIS PRODUCED BY A UNICOMMISSURAL VALVE WILLIAM C. BY ROBERTS AND ANDREW G. MORROW From the Clinic of Surgery, National Heart Institute, National Institutes
Case 47 Clinical Presentation
 93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong
 Pol.Col.Dr.Kasem Ratanasumawong") Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
DISCLOSURE. Echocardiography in Systemic Diseases: Questions. Relevant Financial Relationship(s) None. Off Label Usage None 5/7/2018
 None. Off Label Usage None 5/7/2018") Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504
 Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
CLINICAL COMMUNIQUE 16 YEAR RESULTS
 CLINICAL COMMUNIQUE 6 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 6900 Introduction The Carpentier-Edwards PERIMOUNT Mitral Pericardial Valve, Model 6900, was introduced
CLINICAL COMMUNIQUE 6 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 6900 Introduction The Carpentier-Edwards PERIMOUNT Mitral Pericardial Valve, Model 6900, was introduced
Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia.
, FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia.") Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia. Decision process for Management of any valve Timing Feasibility
Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia. Decision process for Management of any valve Timing Feasibility
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Outline 9/17/2016. Advances in Percutaneous Mitral Valve Repair and Replacement. Scope of the Problem and Guidelines
 Advances in Percutaneous Mitral Valve Repair and Replacement Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando,
Advances in Percutaneous Mitral Valve Repair and Replacement Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando,