THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
|
|
|
- Madison Jennings
- 5 years ago
- Views:
Transcription
1 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO
2 Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions in ARDS Address salvage therapies for severe hypoxia in ARDS.
3 Case Presentations A 23 year old male college student 18 year old female 60 year old male SNF resident 40 year old female with an SBO
4 Case presentations...is found down after ODing on Heroin. comes to the ICU after DCS for abdominal trauma from an MVC. is sent to the ED with a fever and cough. vomits on the wards and collapses.
5 Next they develop severe hypoxia.

6 And a CXR reveals
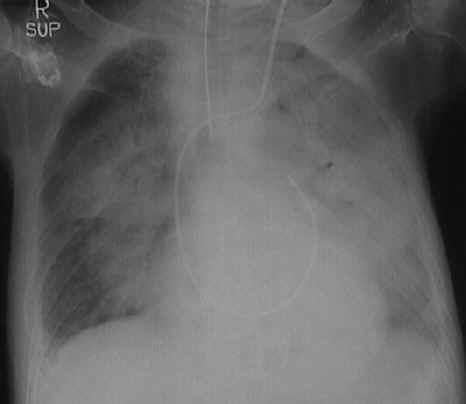
7 Or this
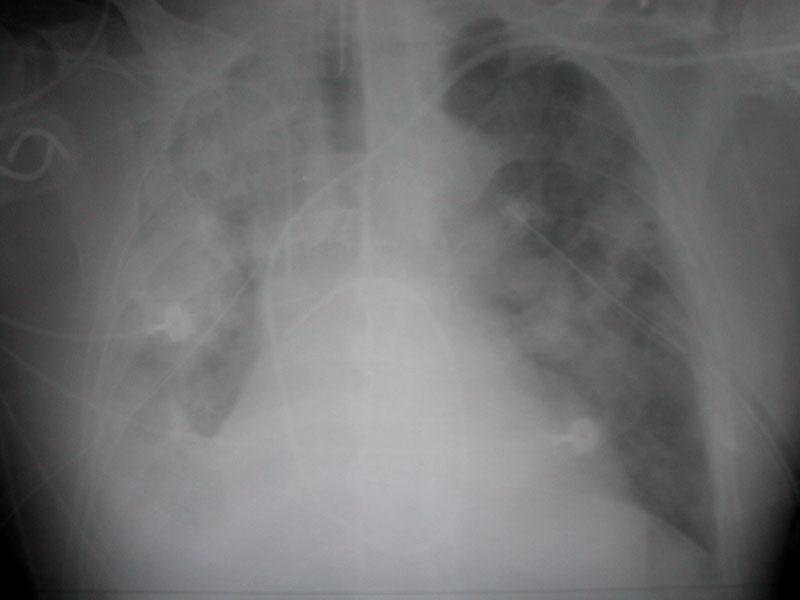
8 Or this


9 Or maybe it was a CT to r/o PE
10 Epidemiology Approximately 190, ,000 cases annually reported. Incidence estimated to be 86 case per 100,000 Increased incidence in the elderly 306 case per 100,000 Estimated mortality between 30-40%.
11 Historical Perspective During the Vietnam War a clinical syndrome of severe hypoxia was identified soldiers who suffered serious injuries.
12 The Adult Respiratory Distress Syndrome In 1967 a case series reported 12 cases of sudden onset severe hypoxia associated with diffuse patchy infiltrates on chest X-ray. The condition was termed the Adult Respiratory Distress Syndrome. The X-ray appeared very similar to the Infant Respiratory Distress Syndrome.
13 Pediatricians are for babies As the condition was diagnosed more it became apparent that ARDS occurred in all ages. Pediatricians REALLY don t like writing the word adult and were quite vocal about it. Therefore the name was changed to ACUTE Respiratory Distress Syndrome
14 Shortly there after Tom Petty, MD had a new ABG machine Discovered in a patient with what was later identified as ARDS after trauma that retarding expiratory flow resulted in an increase in PaO2(40->130). This maneuver was repeated in 12 additional patients with similar clinical picture with consistent improvements in oxygenation.
15 So what is ARDS? Diffuse pulmonary edema due to fluid leaking in to alveolar spaces and damage to lung tissues from inflammation and loss of oncotic forces.
16 So all of these: Neurogenic Pulmonary Edema Fat Embolism Shock Lung TRALI Pump Lung Capillary Leak Syndrome Are just ARDS
17 Clinical Diagnosis AECC Definition: Due to the disparate causes and unclear definition a diagnostic criteria was composed in 1994 to standardize the definition of ARDS Main diagnostic points were Acute Onset Hypoxia Bilateral Infiltrates Absence of Heart Failure
18 Refining the Diagnosis The Berlin Criteria was devised by a panel of experts in 2011 and released in Provided more concrete criteria for some of the diagnostic requirements. Added a severity scale to diagnosis. Not very different from AECC in actuality.
19 AECC vs. Berlin Acute Onset. Diffuse patchy infiltrates on CXR. Absence of LV dysfunction on Echo or PAWP<18. PaO2/FiO2 <200. Onset within 7 days. Diffuse patchy infiltrates on CXR or CT scan. No clinical suspicion of heart failure or absence of LV dysfunction on Echo. PaO2/FiO2<300 on at least 5 of PEEP or EPAP.
20 Berlin Criteria Severity Scale Based on PaO2/FiO2 ratio. Mild Moderate Severe <101 Correlates with mortality Mild: 27% Moderate: 32% Severe: 45%
21 So if you want to be technical Patient s with cardiomyopathies can t have ARDS. Patient s with a pneumonectomy can t have ARDS
22 Pathophysiology Inciting event causes release of inflammatory markers causing damage to capillaries and alveoli resulting in fluid exiting the vascular space into the lung parenchyma resulting in filling of or collapse of alveoli.
23 Pathophysiology Results in patches of alveoli that receive no ventilation causing shunting of deoxygenated venous blood through portions of the lung without oxygenation.
24 Phases of ARDS Acute(or exudative) Phase Edema and diffuse alveolar damage. Generally Days 1-6


25 Phases of ARDS Healthy Lung Acute ARDS

26 Phases of ARDS Proliferative Phase Edema begins to improve, overgrowth of Type 2 Aveolar Cells, myofibroblasts invade into interstitium and collagen deposition occurs.

27 Thank you Pediatricians Chronic Acute Respiratory Distress Syndrome Also called Fibrotic Phase of ARDS Fibrosis of lung parenchyma, formation of cysts in damaged parts of the Lung.
28 Inciting Events Pulmonary Pneumonia Aspiration Pulmonary Contusion Near Drowning Smoke Inhalation Extrapulmonary Sepsis Severe Trauma Burns Pancreatitis Blood Transfusions Drug Overdose/Reaction Head Injury Cardiac Bypass Bone Marrow Transplant
29 Complications Pneumothorax Pneumomediastinum Decreased venous return-hypotension Worsening of pulmonary edema and worsening oxygenation Organ dysfunctiomn Many are actually are complications of mechanical ventilation in ARDS
30 Barotrauma Injury to lung due to High Ventilatory pressures. Pneumothorax Pneumomediatinum
31 Volutrauma Increase in inflammatory markers caused by distension of alveola. Leads to further lung injury from inflammation and extrapulmonary organ injury.
32 Atelectrauma Increase in both inflammatory cytokines and alveolar injury due to shearing caused by the repeated opening and closing of alveolar units.
33 Optimizing Treatment in ARDS Low Tidal Volume Ventilation Controlling Plateau Pressures Permissive Hypercapnia Providing adequate Oxygentaion Early Neuromuscular Blockade
34 The ARMA Trial Randomized control trial 861 patients meeting AECC definition of Acute Lung Injury (PaO2/FiO2<300) Randomized to: 6 ml/kg(pbw) and Plateau pressure <30 12 ml/kg(pbw) and Plateau pressure <50 Stopped early due to significantly higher mortality in 12 ml/kg group
35 Demographics
36 Results 12 ml/kg 6 ml/kg P-value Mortality 39.8% 31.0% Ventilator free days Days without other organ failure Barotrauma Events
37 PEEP strategies Best PEEP using flow volume loops Super PEEP Optimum PEEP for compliance Minimum PEEP for oxygenation No good evidence to support one strategy over another for determining PEEP.
38 Some points about PEEP It takes time to recruit alveoli with PEEP, don t expect rapid changes in oxygenation. A lung opening procedure or recruitment maneuver can be used to more rapidly open the lung and improve oxygenation. Increase PEEP to for seconds.
39 Early Neuromuscular Blockade Randomized Double Blind Placebo Controllede Trial 340 patients with AECC definition of ARDS and PaO2/FiO2<150 on at least 5 of PEEP Randomized to Deep Sedation for 24 hours Deep Sedation plus Neuromuscular Blockade with cisatricurium for 48 hours.
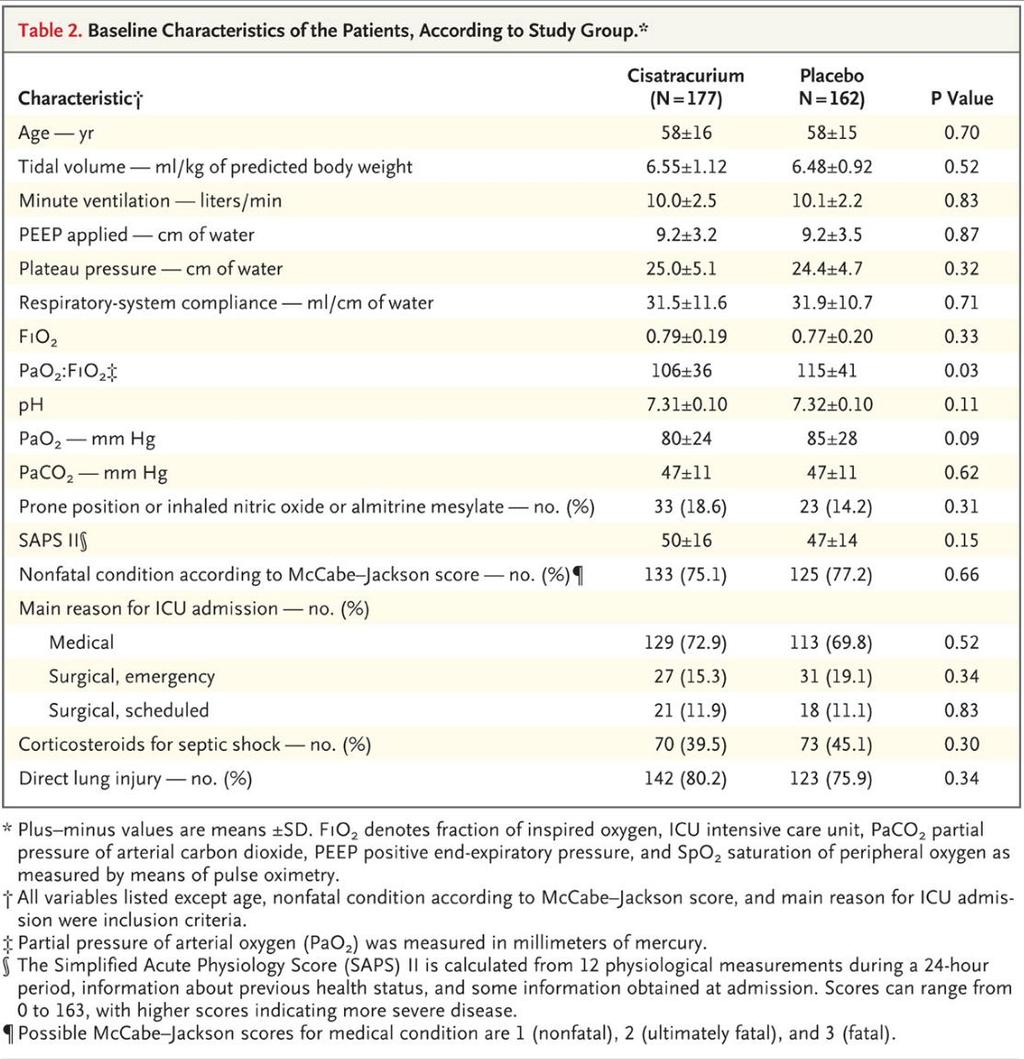
40 Demographics
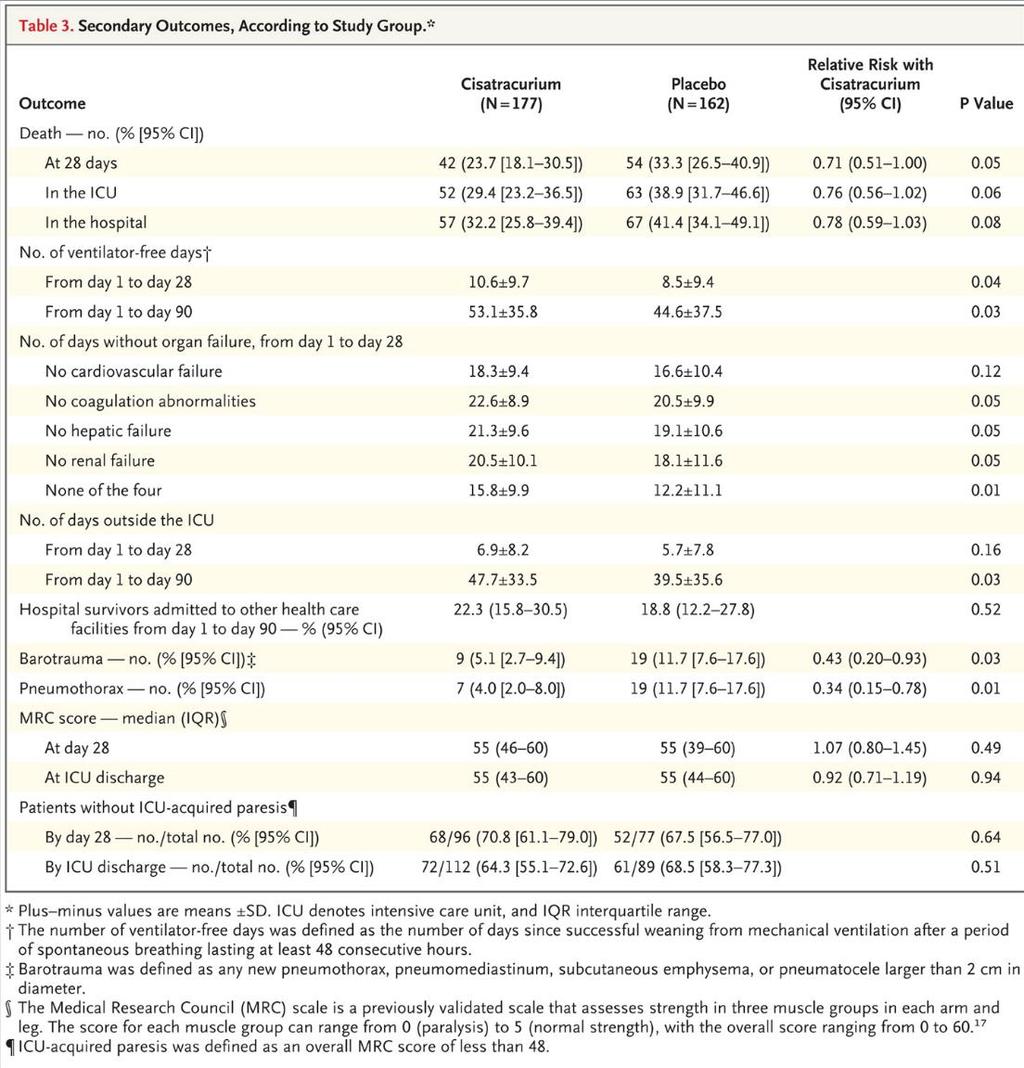
41 Results
42 Results Adjust 90 day Hazard Ratio for Death: 0.68 (p-value: 0.04)
43 Neuromuscular Blockade Subgroup analysis based on severity of ARDS defined by PaO2/FiO2 ratio demonstrated that mortality benefit occurred in patients with PaO2/FiO2 ratio <120.
44 Fluid Management(The FACCT Trial) Randomized Controlled Trial Two major questions: Do PAC s help management of ARDS Keep this short: NO Liberal(give fluid) vs restrictive(diurese) management
")
45 The FACCT Trial 1000 patient meeting AECC definition of Acute Lung Injury (PaO2/FiO2<300) Randomized to:
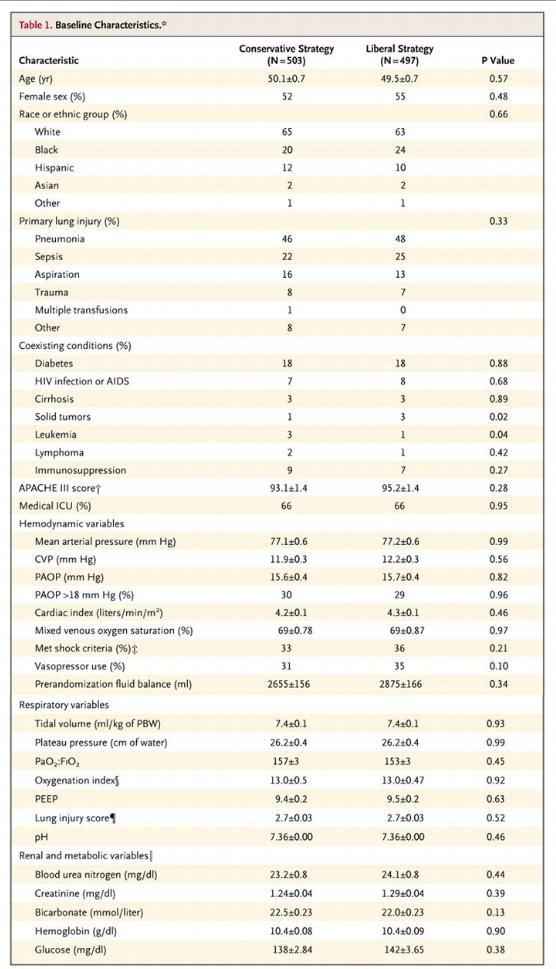
46 Demographics
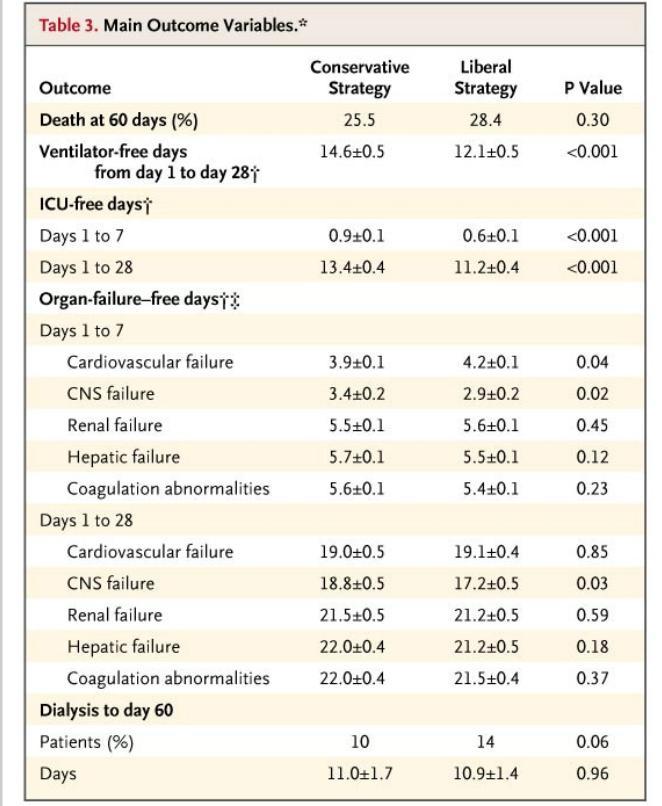
47 Results
48 Salvage/Rescue Therapies Proning Inhaled Vasodilators APRV HFOV ECMO



49 Proning
50 Proning Reverses dependant areas of lung leading to decreased V/Q mismatch. Creates increase in extrathoracic pressure. Recent NEJM study showed improved mortality in patients with severe ARDS (PaO2/FiO2<100 after 36 hours of treatment) kept prone for 14 hrs a day.
51 Inhaled Nitric Oxide Vasodilator Enters opened areas of lung and dilates capillaries increasing blood flow to open areas of lung. Improves V/Q matching. Expensive. Improves oxygenation but no proven mortality benefit. Increased incidence of renal failure.
52 Epoprostenol Same mechanism of action as INO. Administered as continuous 50 ng/kg/min Again improves oxygenation but no proven mortality benefit Significantly cheaper than INO. No evidence of increased renal failure.
53 Iloprost Another inhaled vasodilator Administered Ever 2 to 4 hours Has the least evidence supporting its effectiveness. Cheapest option of Inhaled Vasodilators
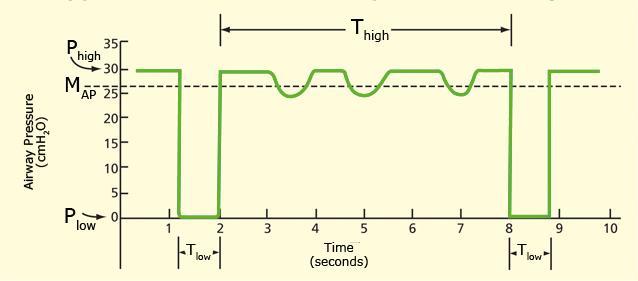
54 APRV
55 APRV Alternate mode of ventilation high steady airway pressure that drops to a lower pressure for a brief period of time. Allows higher airway pressures. Some small studies show decreased rates of developing ARDS, but no other evidence of outcomes differences in patients with ARDS.

56 HFOV
57 HFOV Continuous high airway pressures, a piston rapidly pushes tiny amounts of air into and out of the lungs. Allows higher mean airway pressures without large tidal volumes or shearing improving recruitment and oxygenation. In 2 large studies no benefit or worsened outcomes if used in early ARDS.
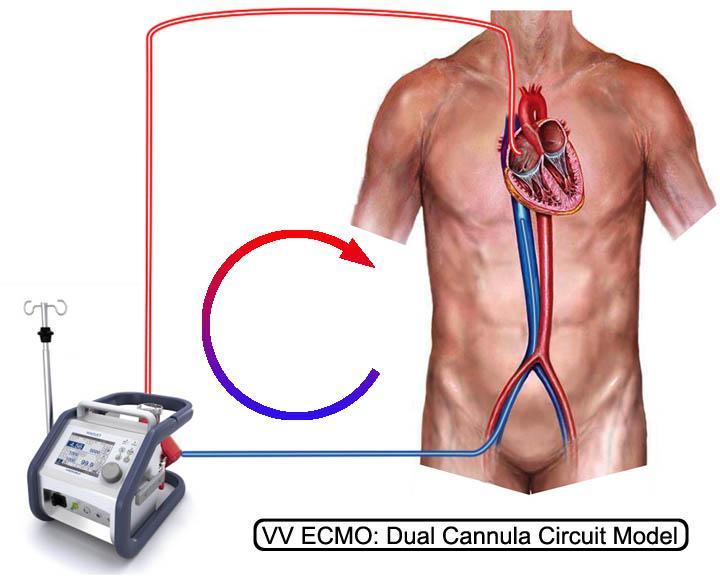
58 ECMO
59 ECMO By running Venous blood through a membrane oxygenator the patient can have effective CO2 removal and oxygenation without relying on the lungs. Allows for minimal vent settings to rest the lungs. Evidence is limited but shows some potential benefit in severe ARDS.
60 Key Points ARDS is a clinical diagnosis with specific criteria. Acute Onset <7 days PaO2/FiO2 <300 Bilateral patchy infiltrates Not cardiac related
61 Key Points Low tidal volume ventilation improves mortality. 6 ml/kg PBW(based on Height) Diuresis decreases ventilator days and organ failure in hemodynamically stable patients. Early Neuromuscular Blockade of benefit in moderately severe cases Variety of salvage therapies Proning, Inhaled Vasodilators, APRV, HFOV, ECMO Only proning has shown any mortality benefit.
62 Key Points Variety of salvage therapies Proning, Inhaled Vasodilators, APRV, HFOV, ECMO Only proning has shown any mortality benefit.
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
ARDS A Brief Overview. Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine
 ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Acute Respiratory Failure. Respiratory Failure. Respiratory Failure. Acute Respiratory Failure. Ventilatory Failure. Type 1 Respiratory Failure
 Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
ARDS: MANAGEMENT UPDATE
 ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Acute Respiratory Distress Syndrome
 Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS?
 Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Replacement of air with fluid, inflammatory. cells or cellular debris. Parenchymal, Interstitial (Restrictive) and Vascular Diseases.
 and Vascular Diseases.") Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
 Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Acute respiratory distress syndrome
 20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Acute Respiratory Distress Syndrome
 Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015
: Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015") Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
CASE PRESENTATION VV ECMO
 CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
RESCUE VENTILATION SUMMARY
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Oregon Health and Science University Portland, Oregon USA
 Classifying ARDS The Role of EVLW Ch l Philli MD Charles Phillips MD Oregon Health and Science University Portland, Oregon USA Incidence High ARDS 2013 150,000 200,000 per year in US alone. Mortality persists
Classifying ARDS The Role of EVLW Ch l Philli MD Charles Phillips MD Oregon Health and Science University Portland, Oregon USA Incidence High ARDS 2013 150,000 200,000 per year in US alone. Mortality persists
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
ECMO and refractory Hypoxemia
 ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
") & & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
& & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
Neuromuscular Blockade in ARDS
 Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq
 Dr.Ahmad farooq") Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Acute Respiratory Distress Syndrome (ARDS):Evidence Based Management
:Evidence Based Management") Acute Respiratory Distress Syndrome (ARDS):Evidence Based Management John C. Klick, M.D., F.C.C.P. Assistant Professor Department of Anesthesiology and Perioperative Medicine University Hospitals Case
Acute Respiratory Distress Syndrome (ARDS):Evidence Based Management John C. Klick, M.D., F.C.C.P. Assistant Professor Department of Anesthesiology and Perioperative Medicine University Hospitals Case
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Pro: Early use of VV ECMO for ARDS
 Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS
 REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
RESPIRATORY FAILURE. Dr Graeme McCauley KGH
 RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
Successful use of extracorporeal membrane oxygenation in a patient with transfusion-related acute lung injury
 Case Report Crit Care & Shock (2011) 14:40-45 Successful use of extracorporeal membrane oxygenation in a patient with transfusion-related acute lung injury Jarrod Mosier, Terence O Keeffe, Holly Graham,
Case Report Crit Care & Shock (2011) 14:40-45 Successful use of extracorporeal membrane oxygenation in a patient with transfusion-related acute lung injury Jarrod Mosier, Terence O Keeffe, Holly Graham,
Mechanical ventilation in the emergency department
 Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
INTRODUCTION. Acute respiratory distress syndrome (ARDS) is a common complication of critical illness
 is a common complication of critical illness") Breanna Keller NDFS 356 Acute Respiratory Distress Syndrome INTRODUCTION Acute respiratory distress syndrome (ARDS) is a common complication of critical illness and results in the sudden failure of the
Breanna Keller NDFS 356 Acute Respiratory Distress Syndrome INTRODUCTION Acute respiratory distress syndrome (ARDS) is a common complication of critical illness and results in the sudden failure of the
Biomarkers for ARDS not so simple. John Laffey. Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA
 Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Adjunct Therapies for Pediatric ARDS: Where are the Data?
 Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
The 1918 flu pandemic (January 1918 December 1920) was an unusually deadly influenza pandemic, the first of the two pandemics involvingh1n1 influenza
 was an unusually deadly influenza pandemic, the first of the two pandemics involvingh1n1 influenza") PANEL DISCUSSION The 1918 flu pandemic (January 1918 December 1920) was an unusually deadly influenza pandemic, the first of the two pandemics involvingh1n1 influenza virus. [1] It infected 500 million
PANEL DISCUSSION The 1918 flu pandemic (January 1918 December 1920) was an unusually deadly influenza pandemic, the first of the two pandemics involvingh1n1 influenza virus. [1] It infected 500 million
7 Initial Ventilator Settings, ~05
 Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Disclosures. ICU Management of Advanced Lung Disease 5/9/2015. No Disclosures. All pictures from commercial sources
 Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases
 i and Vascular Diseases") Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Seminar. Current Concepts
 Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Introduction Definition Etiology Epidemiology Lung injury prediction score. Pathophysiology Diagnosis Clinical presentation Management Conclusion
 Introduction Definition Etiology Epidemiology Lung injury prediction score Pathophysiology Diagnosis Clinical presentation Management Conclusion During the 1960s, a distinct type of a life threatening
Introduction Definition Etiology Epidemiology Lung injury prediction score Pathophysiology Diagnosis Clinical presentation Management Conclusion During the 1960s, a distinct type of a life threatening
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Postoperative chest x-ray May Mats Beckman Emergency Radiology. Shutter use!
 Postoperative chest x-ray May 2009 Mats Beckman Emergency Radiology Shutter use! 2Postoperative chest x-ray May 2009 Exposure/ window settings Quick resorption of infiltrations= water logged lung 3Postoperative
Postoperative chest x-ray May 2009 Mats Beckman Emergency Radiology Shutter use! 2Postoperative chest x-ray May 2009 Exposure/ window settings Quick resorption of infiltrations= water logged lung 3Postoperative
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Permissive hypoxaemia. Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK
 Permissive hypoxaemia Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK Is mechanical ventilation such a good idea? ventilator-induced lung injury (short- & long-term)
Permissive hypoxaemia Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK Is mechanical ventilation such a good idea? ventilator-induced lung injury (short- & long-term)
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Pneumonia in the Hospitalized
 Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of