Fractional Flow Reserve (FFR) estimation GRAIDIS CHRISTOS. EUROMEDICA-KYΑNOUS STAVROS Interventional Cardiologist, FSCAI
|
|
|
- Nora Lorena Hampton
- 5 years ago
- Views:
Transcription
 estimation Why, how,")




1 Fractional Flow Reserve (FFR) estimation Why, how, when? GRAIDIS CHRISTOS EUROMEDICA-KYΑNOUS STAVROS Interventional Cardiologist, FSCAI "Innovations in Interventional Cardiology & Electrophysiology IICE 2013" NOVEMBER 2013 ELECTRA PALACE HOTEL, THESSALONIKI
2 Coronary revascularization should aim at: 1) Relieve symptoms? 2) Improve outcome? 3) Relieve symptoms and improve outcome? 4) Place a drug eluting stent? 5) I have no idea The goal of any treatment is to improve a patient s prognosis and/or symptoms. Accordingly, any diagnostic tool should help guide decision making in order to achieve optimal treatment for a patient.


3 Coronary angiography still plays a pivotal role in invasive imaging of the coronary arteries. ARE THESE HORIZONTAL LINES STRAICHT? While coronary angiography is widely accepted as the gold standard investigation to diagnose coronary artery disease, and has contributed hugely to our understanding of coronary anatomy, it is highly subjective and does not provide any information about the haemodynamicsignificance of a stenosis.

4 It is important to emphasize that in coronary artery disease, the most important factor related to outcome is the presence and extent of inducible ischemia. The modern target for PCI is: ischemia first and anatomy second. Proof of ischemia, both at a patient level and then at lesion level,should become a consideration as part of our routine practice.



")
5 It is of paramount importance to determine whether a stenosisis inducing reversible ischemia in other words, to assess whether a stenosis is functionally significant Non invasive functional tests: -Exercise elctrocardiogram -Perfusion scintigraphy -Stress echocardiography -Stress MRI -Positron emission tomography (PET) imaging -Stress dual-source computed tomography (DSCT) -Combined/hybrid approaches


6 Prediction of cardiac death and nonfatal myocardial infarction (MI) by assessment of ischemia by nuclear imaging/cardiac MRI in seven large studies comprising more than 20,000 patients. In patients without ischemia, outcome was excellent. The corresponding annual event rates were 0.45% per year for nonischemic MPI patients

7
8 Concept of fundamental importance Data suggest that non-ischemic lesions can be Data suggest that non-ischemic lesions can be managed safely with a non-interventional approach without incurring an increased event rate or mortality, provided a complete clinical risk assessment has been performed



9 Non-Invasive Functional Assessment Before PCI Underutilized 23,887 Medicare Pts Referred for Elective PCI in 2004 Lin GA, et al. JAMA 2008;300: The vast majority of patients with suspected coronary artery disease never undergo any form of non-invasive test before having a coronary angiogram.


10 Proportion of Adequate Stress Tests Marwick et al. Circulation 1994


11 Inaccuracy of Perfusion SPECT imaging in MVD Technetium-99m sestamibisinglephotonemission computed tomography, and other classic noninvasive tests often indicate ischemia in patients with multivesseldisease but fail to distinguish the specific ischemic territories and responsible stenoses. Lima RS, et al. J Am Coll Cardiol. 2003;42:64-70 In addition, findings on technetium-99m sestamibi singlephoton emission computed tomography may even be normal in multivesseldisease because of balanced ischemia.



12 The time has come to move from coronary angiography to physiological assessment of coronary lesions? An ideal parameter should account for the interaction between epicardial stenosis severity, extent of the perfusion territory, myocardial blood flow including collaterals microvascular function Physiologic evaluation Fractional Flow Reserve-FFR


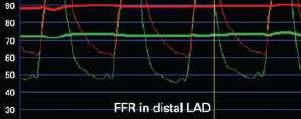
13 Fractional flowreserve is calculated as the ratio of distal coronary pressure to aortic pressure measured during maximal hyperaemia.


14 FFR of 0.66 means that the maximum blood flow (and oxygen supply) to the myocardial distribution of the respective artery only reaches 66% of what it would be if that artery were completely normal.




15







16 Step 1: Pressure wire and analyzer setting Step 2: Pa/Pd pressure equalization Step3: Wiring, check Step3: Wiring, check baseline pressure gradient and induce hyperemia
17 Features of FFR Differently from most physiologic indices, the normal value of the FFR is 1.0 for every patient,every coronary artery and every segment. Not influenced by systemic haemodynamics.(hr, BP, contractility). Extremely reproducible, low intra-operator variability, easy to measure (success rate 99 %) Independent of gender, and other factors such as hypertension and diabetes. Specifically related to epicardiallesions, independent of micro-circulation. Takes into account the contribution of collaterals. High spatial resolution (pull-back).

18 FFR: ischaemic threshold A cut-off value reflecting the presence or absence of ischaemiahasbeen prospectively defined and compared with the gold standard non-invasive tests for ischaemia NO PCI PCI De BruyneB et al. Circulation 1995;92: PijlsNH et al. N EnglJ Med 1996;334:
19 FFR «grey zone»: In most of cases in which the FFR value falls in the grey zone, functional noninvasive tests are abnormal, and they become normal after revascularization (*). Is recommended to take into account the 0.80 value for the main vessels, whose revascularization has a pronosticvalue, and to consider the 0.75 value (more restrictive) for the secondary vessels, whose revascularization has a benefit only with respect to symptoms. (**). DECISION MAKING MAY BE SUPPORTED BY PATIENT SPECIFIC CLINICAL ASSESMENT If single vessel disease, no or atypical complaints, no evidence of ischemia: NO REVASCULARIZATION If more extensive disease, typical complaints, positive non-invasive test or diabetes: REVASCULARIZATION *De BruyneB, PijlsNH, et al. Circulation 2001;104: **DeBruyneB,Sarma.J. Heart2008;94:

20 FFR is determined by the size of myocardial mass FFR FFR FFR normalizes for the perfusion area: Anatomic severity remains unchanged but physiologic severity has decreased

21 FFR is determined by the size of myocardial mass



22 FFR with collateral contribution






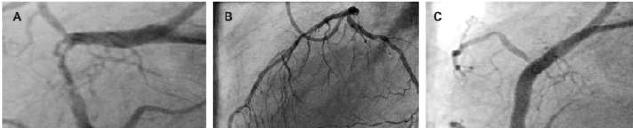
23 VISUAL-FUNCTIONAL MISMATCH One of them should be revascularized, and the other should not. 2 angiographically similar stenosesmay have a completely different hemodynamic severity.

 with Negative FFR Reverse Mismatch Insignificant Stenosis(<50%)")
24 FFR is determined by many lesion specific local factors at maximal hyperemia Lesion severity determined by coronary angiography has not been well-correlated with the physiologic significance of the stenosis.however, the reasons why mismatches between the two, are still poorly understood. Mismatch Significant Stenosis(>50%) with Negative FFR Reverse Mismatch Insignificant Stenosis(<50%) with Positive FFR



25 MLA 2.8 mm2


26
27 FFR is influenced by Many Lesion Specific Factors The same degree of stenosiscan make a different FFR value according to the different lesion morphologic factors. Degree of diameter stenosis Reference vessel diameter (myocardium) Lesion morphology Eccentricity Lesion length Plaque burden, Plaque rupture Surface roughness (thrombus) Viscous friction, flow separation, turbulence, and eddies FFR, a very sensitive index integrating various local factors, is more reliable than angiographically determined stenosis severity.
28 FFR : Applications Intermediate Stenoses Multivessel disease Left main Ostial lesions Bifurcations (before and after PCI of the «mother» vessel) Multiple stenoses, diffuse disease PCI results ACS
 are")

29 FFR IN INTERMEDIATE LESIONS One of the standard indications for FFR is the precise assessment of the functional consequences of a given coronary stenosiswith unclear hemodynamic significance Intermediate lesions (40-70%) are the most common in patients with CAD (47% in FAME) and with great variability in interpretation Furthermore, results of different noninvasive tests are often contradictory, which renders appropriate clinical decision making difficult.



30 DEFER Trial Flow chart Safety of Deferring PCI Based on FFR


31 Safety of Deferring PCI Based on FFR DEFER Trial: 5-Year Follow-up The prognosis of non-ischaemic stenosis(ffr > 0.75) is excellent The risk that a hemodynamically nonsignificantstenosiswill cause death or AMI is<1% per year and is not decreased by stenting. Pijls, et al. J Am Coll Cardiol 2007;49:




32 Safety of Deferring PCI Based on FFR Fearon W. TCT 2011
33 Safety of Deferring PCI Based on FFR These results strongly support the use of FFR measurements as a guide for decision making about the need for revascularization in intermediate lesions.


34 A 69-Year-Old Man With Severe Angina This mid LAD stenosis, was considered non-significant on the angiogram Myocardial perfusion imaging showed a reversible defect in the inferolateralsegments

35 However, the mid left descending artery (LAD) stenosis, considered non-significant on the angiogram, appears to be hemodynamicallysignificant. By nuclear scintigraphy, the significant defect in the anterior wall is masked by the more severe defects in the other areas.
36 FFR & multivesseldisease Patients with multi-vessel disease actually represent a very heterogeneous population. All the angiographicallymulti-vessel diseases are not functionally equivalent. What we should treat is ischaemia, not lesions. In patients with multi-vessel disease, determining which lesion(s) warrant stentingand which do not can be difficult if one chooses to use non-invasive imaging modalities. Systematically measuring FFR can maximize the benefit of PCI by Systematically measuring FFR can maximize the benefit of PCI by accurately discriminating those lesions for which revascularisation will provide the most benefit from those for which PCI may only increase the risk.
")
37 Angio-guided group: anatomical complete revascularization Stenting all lesions >50% on the angiogram FFR-guided group: functionally complete revascularization Stenting isschemic lesions only (FFR<0.80)

38 FAME Trial: Study Flowchart Tonino PA, et al. NEJM 2009;360:213 24

39 FAME Trial: One Year Outcomes It was demonstrated that all types of adverse events were decreased by 30% in the first year after PCI in multivessel disease Tonino, et al. New Engl J Med 2009;360:


40 FAME Trial: Two Year Outcomes Death/MI was significantly reduced from 12.9% to 8.4% (p=0.02) Very little risk with deferral of stentingin patients with lesions with an FFR >0.80 MI rate of 0.2 %(1 late MI) and Revascularization rate of 3.2 % (16 late PCIs),

41 FAME Trial: Two Year Outcomes NO DIFFERENCE IN SYMPTOM OUTCOME Angina in FFR-guided patients was relieved at least as effectively
42 FAME: Economic Evaluation The FAME trial showed improved patient outcomes with FFR-guided PCI. This was achieved at a lower cost and without prolonging the interventional procedure FFR-guided PCI saved >$2,000 per patient at one year compared to Angio-guided PCI Circulation 2010;122:

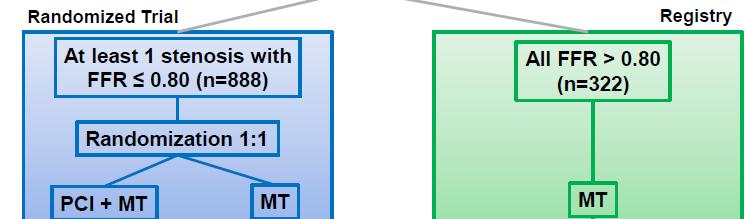
43 FAME 2 : Flow Chart
44 Recruitment for the FAME 2 study was halted in January 2012, when an independent Data and Safety Monitoring Board (DSMB) recommended early termination of the study. The preliminary results were considered so compelling that research was stopped so patients with FFR <0.80 randomized to optimal medical therapy only could also receive the benefits of PCI

45 In patients with stable coronary. artery disease, FFR guided PCI improves patient outcome and is cost effective when compared to medical therapy alone De Bruyne, et al. New Engl J Med 2012;367:

46 FAME 2 : FFR-Guided PCI versus Medical Therapy in Stable CAD This improvement is driven by a dramatic decrease in the need for urgent revascularization for ACS. Neither the rate of death from any cause nor the rate of myocardial infarction differed significantly between the PCI group and the medical-therapy group
47 FAME 2 : FFR-Guided PCI versus Medical Therapy in Stable CAD Among patients with stenosesthat were not functionally significant (25%), the best available medical therapy alone resulted in an excellent outcome, regardless of the angiographic appearance of the stenoses. Only 3 % experienced a primary endpoint


48
49 FFR in left main coronary artery stenosis. Why? The presence of a significant stenosisin the left main stem is of critical prognostic importance. The left main is among the most difficult segments to assess by angiography Noninvasive testing is often noncontributivein patients with a left main stenosis. Furthermore, revascularization of a non-significant stenosisin the left main may lead to early occlusion of the conduits, especially when internal mammary arteries are used. Consequently ambiguous LMCA disease sometimes results in considerable uncertainty when deciding on the best therapeutic strategy for the patient In most of the cases, therapeutic decision for its treatment is based on the angiographic appearance of the lesion


50 What LM MLA is ischemic? Fassa JACC, 2005: , Jasti Circulation 2004;2831-6, Koo JACC ,




51 Does these left main stenoses need revascularization?


52 QCA-FFR Discordance in Left Main Stem Stenoses Park et al JACC Interv In 35% of patients with LM stenosis>50%, FFR was >0.80 In 40% of patients with LM stenosis<50%, FFR was <0.80


53 Does this left main stenosis need revascularization? Can you really leave lesions that looks significant to your eyes. but have negative FFR?

54 Several small studies and one larger study, published recently, showed that an FFR-aided strategy for equivocal LMCA lesions is safe and related to a favorable clinical outcome.


55 Is it safe to differ revascularization on LM lesions with FFR>0.80? In 23% of patients with LM stenosis <50%, FFR was <0.80 Hamilos et al., Circulation 2009;120:1505
56 Is it safe to differ revascularization on LM lesions with FFR>0.80?



57 FFR in the LMCA: Practical Aspects

58 FFR in the LMCA: Practical Aspects With distal stenosis, FFR should be measured in both LAD and Cx
59 Left Main Stem Stenosesare Rarely Isolated When tight stenosesare present in the LAD or in the LCxthe presence of these lesions will tend to increase the FFR measured across the left main. Influence of proximal LAD lesion will be more pronounced than a stenosisof a small marginal branch The influence of a LAD/left circumflex coronary artery (LCx) lesion on the FFR value of the left main will depend on the severity of this distal stenosisbut, even more, on the vascular territory supplied by this distal stenosis



60 FFR of Jailed Left Circumflex
61 FFR of Jailed Left Circumflex Nam CW, et al. Korean Circ J 2011;41:304-7.







62 Use and utility of FFR during Bifurcation PCI
63 Use and utility of FFR during Bifurcation PCI Pre-intervention FFR Mainly to assess the functional significance of main branch lesion FFR of side branch lesion Practical tips you should know. FFR should be measured in a large SB. FFR <0.75 does not always mean the clinical relevance of that side branch (SB) stenosis. When SB FFR is measured, the influence of main branch stenosisshould always be considered. Pre-intervention SB FFR is usually not helpful to predict the jailed SB FFR. To assess the functional significance of pure ostialsb lesion

64 Use and utility of FFR during Bifurcation PCI After main branch stent implantation After stentingthe main branch, the ostiumof the side branch often looks pinched. Yet such stenosesare grossly overestimated by angiography: few of these ostiallesions with a stenosisdiameter 75% were found to have FFR< 0.75


65 Use and utility of FFR during Bifurcation PCI After main branch stent implantation In Jailed side branch lesions, Angiographic severity Presence of ischemia


66 Use and utility of FFR during Bifurcation PCI After main branch stent implantation Can FFR measurement of jailed side branches provide useful information about the indication for further treatment in the absence of obvious indications (egpain/st change)? FFR<0.75?
 stenosis had FFR<0.75.")
67 Correlation Between FFR and % Stenosis(QCA) in Jailed Side Branches In Jailed side branch lesions, Angiographic severity Presence of ischemia At 10 months FU, no death, MI or SB TLR No lesion <75% (green) stenosis had FFR<0.75. Among 73 lesions with 75% stenosis, only 20 lesions (red) were functionally significant (PPV=27%) while 53 (73%) were not (white) Koo BK et al JACC 2005;46:633 7 Dilating >75% SB stenosisis approriatein 1 out of 4 patients (since 1 out of 4 will have FFR<0.75)
. The pressure wire should not be jailed by a stent.")
68 Use and utility of FFR during Bifurcation PCI After main branch stent implantation: If FFR of the side branch is >0.75, the outcome is excellent without further intervention. SB FFR is not recommended in very complicated SB lesions (severe tortuosity, heavy calcification, diffuse multiple stenosis..). The pressure wire should not be jailed by a stent. SB FFR is not recommended in case of slow flow or severe dissection. If you are intent on measuring the FFR of a jailed side branch, but cannot wire the vessel with a pressure wire, can wire with another wire and exchange over a transit catheter



69 FFR in sequential stenoses Practically a pull-back maneuver under maximal hyperemia is the best way to appreciate the exact location and physiologic significance of sequential stenosesand to guide the interventional procedure step-by-step Place the wire in the most distal part of the artery (at least distally to the most distal lesion of interest) Induce hyperemia (i.vadenosine) and determine FFR. If FFR < , inducible ischemia related to this artery is established and PCI is appropriate.


70 FFR in sequential stenoses Start the pull-back recording under fluoroscopy and establish those spots or segments with a sudden pressure drop. If local pressure drops 10 mmhg are present, stentingof those spots can be considered.
 is stentedfirstand the pull-back recording can be repeated thereafter")

71 FFR in sequential stenoses Generally, the most severe spot (i.e., the stenosiswith the largest gradient) is stentedfirstand the pull-back recording can be repeated thereafter to check the remaining lesionsand it can be decided whether and where a second stent should be placed. Sometimes, for technical reasons, the most distal lesion is stentedfirst, even if not the worst one Realize that by stentingthe most severe lesion the gradient across the other lesion(s) may increase Rule of thumb: a severe distal lesion can mask the gradient across a proximal lesion much more than vice versa. Stentingspots or segments with a gradient < 10 mm, does not make much sense.



72 FFR in sequential stenoses
73 FFR in diffuse disease The presence of diffuse disease is often associated with a progressive decrease in coronary pressure and flow, and this can often not be clearly assessed from the angiogram. In contrast, this decrease in pressure correlates with the total atherosclerotic burden. In approximately 10% of patients, this abnormal epicardial resistance may be responsible for reversible myocardial ischemia. In these patients, chest pain is often considered noncoronary because no single focal stenosisis found, and the myocardial perfusion imaging is wrongly considered false positive

74 FFR in diffuse disease The only way to demonstrate the hemodynamic impact of diffuse disease is to perform a careful pull-back maneuver of the pressure sensor under steady-state maximal hyperemia In a large multicenter registry of 750 patients, FFR was obtained after technically successful stenting. A post- PCI FFR value of 0.9 was still present in almost one third of patients (despite the absence of a gradient across the stent), reflecting diffuse disease, and was associated with a poor clinical outcome. Patients with a very gradual decline of pressure along the artery (diffuse disease), fundamentally cannot be helped by PCI
75 FFR never lies? False FFR readings ALWAYS: error is on high side
76 Pitfalls and artifacts of fractional FFR measurement Insufficient hyperemia If you know your enemy and yourself, you can win every battle Guide catheter problems Pressure drift Whipping Spasm/accordion effect Introducer in place Cursor position


77
78 Maximal Hyperemia is of paramount importance Insufficient hyperemia Underestimation of gradient Overestimation of FFR Underestimation of stenosis severity


79




80
81 Impact of Catheter Size on Hyperemic Flow If the guiding catheter is too large, an additional stenosisis created by the catheter, reducing blood flow in the coronary artery Underestimation of the pressure gradient across the stenosis Overestimation of the FFR



82 Recognize guiding catheter damping


83



84

85 Aware of Whipping artifact If the pressure wire sensor hits the coronary wall, spikes appear in the waveform - Whipping" SOLUTION: pull back or advance the wire 2-3mm




86 Aware of Accordion effect
 And most importantly, improve your")
87 CONCLUSIONS In pts with stable CAD, presence and extent of myocardial ischemia is associated with the occurrence of adverse events and long-term prognosis. In most cases, FFR will: Simplify and justify your procedure Save money (cost-saving in some settings and cost-effective in others) And most importantly, improve your patient s outcome!
88 But.. FFR is a bare number only and this value may definitely determine the future life of our patient Know your patient (Symptoms,Course of history, Ancillary testing ) The only guarantee on the validity is the Careful training on the steps of measurement (very simple) Awareness of the potential pitfalls and artifacts Continuous quality control of our FFR practice Give the patient the benefit of the doubt


89 Thank you for your attention!!!!!!!!!


90


91

92


93


94
95
FFR in Multivessel Disease
 FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
Fractional Flow Reserve: Review of the latest data
 Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
Fractional Flow Reserve: Basics, FAME 1, FAME 2. William F. Fearon, MD Associate Professor Stanford University Medical Center
 Fractional Flow Reserve: Basics, FAME 1, FAME 2 William F. Fearon, MD Associate Professor Stanford University Medical Center Conflict of Interest Advisory Board for HeartFlow Research grant from St. Jude
Fractional Flow Reserve: Basics, FAME 1, FAME 2 William F. Fearon, MD Associate Professor Stanford University Medical Center Conflict of Interest Advisory Board for HeartFlow Research grant from St. Jude
FFR Incorporating & Expanding it s use in Clinical Practice
 FFR Incorporating & Expanding it s use in Clinical Practice Suleiman Kharabsheh, MD Consultant Invasive Cardiology Assistant professor, Alfaisal Univ. KFHI - KFSHRC Concept of FFR Maximum flow down a vessel
FFR Incorporating & Expanding it s use in Clinical Practice Suleiman Kharabsheh, MD Consultant Invasive Cardiology Assistant professor, Alfaisal Univ. KFHI - KFSHRC Concept of FFR Maximum flow down a vessel
FFR in Left Main Disease
 FFR in Left Main Disease William F. Fearon, MD Associate Professor of Medicine Director, Interventional Cardiology Stanford University Medical Center Why FFR instead of IVUS? Physiologic versus anatomic
FFR in Left Main Disease William F. Fearon, MD Associate Professor of Medicine Director, Interventional Cardiology Stanford University Medical Center Why FFR instead of IVUS? Physiologic versus anatomic
FRACTIONAL FLOW RESERVE USE IN THE CATH LAB BECAUSE ANGIOGRAPHY ALONE IS NOT ENOUGH!!!!!!!!
 FRACTIONAL FLOW RESERVE USE IN THE CATH LAB BECAUSE ANGIOGRAPHY ALONE IS NOT ENOUGH!!!!!!!! Juan Antonio Pastor-Cervantes,M.D FSCAI, FACC Cardiovascular Institute Memorial Regional Hospital Hollywood Florida
FRACTIONAL FLOW RESERVE USE IN THE CATH LAB BECAUSE ANGIOGRAPHY ALONE IS NOT ENOUGH!!!!!!!! Juan Antonio Pastor-Cervantes,M.D FSCAI, FACC Cardiovascular Institute Memorial Regional Hospital Hollywood Florida
FRACTIONAL FLOW RESERVE: STANDARD OF CARE
 FRACTIONAL FLOW RESERVE: FROM INVESTIGATIONAL TOOL TO STANDARD OF CARE TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands FRACTIONAL FLOW
FRACTIONAL FLOW RESERVE: FROM INVESTIGATIONAL TOOL TO STANDARD OF CARE TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands FRACTIONAL FLOW
Debate Should we use FFR? I will say NO.
 Debate Should we use FFR? I will say NO. Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol Gwon Research fund from Abbott Korea
Debate Should we use FFR? I will say NO. Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol Gwon Research fund from Abbott Korea
Fractional Flow Reserve. A physiological approach to guide complex interventions
 Fractional Flow Reserve A physiological approach to guide complex interventions What is FFR? Fractional Flow Reserve (FFR) is a lesion specific, physiological index determining the hemodynamic severity
Fractional Flow Reserve A physiological approach to guide complex interventions What is FFR? Fractional Flow Reserve (FFR) is a lesion specific, physiological index determining the hemodynamic severity
FRACTIONAL FLOW RESERVE Step-by-step measurement, Practical tips & Pitfalls
 FRACTIONAL FLOW RESERVE Step-by-step measurement, Practical tips & Pitfalls Ahmed M ElGuindy, MSc, MRCP(UK) Division of Cardiology Aswan Heart Centre 2013 Fractional Flow Reserve Essential diagnostic tool
FRACTIONAL FLOW RESERVE Step-by-step measurement, Practical tips & Pitfalls Ahmed M ElGuindy, MSc, MRCP(UK) Division of Cardiology Aswan Heart Centre 2013 Fractional Flow Reserve Essential diagnostic tool
Coronary stenting: the appropriate use of FFR
 Coronary stenting: the appropriate use of FFR Morton J. Kern, MD Professor of Medicine Chief of Cardiology LBVA Associate Chief Cardiology University California Irvine Orange, California To treat or not
Coronary stenting: the appropriate use of FFR Morton J. Kern, MD Professor of Medicine Chief of Cardiology LBVA Associate Chief Cardiology University California Irvine Orange, California To treat or not
Σεμινάριο Ομάδων Εργασίας Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική
 Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική") ΕΛΛΗΝΙΚΗΚΑΡΔΙΟΛΟΓΙΚΗΕΤΑΙΡΕΙΑ Σεμινάριο Ομάδων Εργασίας 2011 Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική GUIDELINES ON MYOCARDIAL
ΕΛΛΗΝΙΚΗΚΑΡΔΙΟΛΟΓΙΚΗΕΤΑΙΡΕΙΑ Σεμινάριο Ομάδων Εργασίας 2011 Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική GUIDELINES ON MYOCARDIAL
Between Coronary Angiography and Fractional Flow Reserve
 Visual-Functional Mismatch Between Coronary Angiography and Fractional Flow Reserve Seung-Jung Park, MD., PhD. University of Ulsan, College of Medicine Asan Medical Center, Seoul, Korea Visual - Functional
Visual-Functional Mismatch Between Coronary Angiography and Fractional Flow Reserve Seung-Jung Park, MD., PhD. University of Ulsan, College of Medicine Asan Medical Center, Seoul, Korea Visual - Functional
CLINICAL CONSEQUENCES OF THE
 CLINICAL CONSEQUENCES OF THE FAME STUDY TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands GUIDELINES ESC SEPTEMBER 2010 FFR UPGRADED TO LEVEL
CLINICAL CONSEQUENCES OF THE FAME STUDY TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands GUIDELINES ESC SEPTEMBER 2010 FFR UPGRADED TO LEVEL
Dave Kettles, St Dominics Hospital East London.
 Dave Kettles, St Dominics Hospital East London. 110 x 150 Angina for a couple of months Trop T negative T wave inversion across the chest leads Not wanting to risk radial Huge struggle with femoral
Dave Kettles, St Dominics Hospital East London. 110 x 150 Angina for a couple of months Trop T negative T wave inversion across the chest leads Not wanting to risk radial Huge struggle with femoral
FFR-Guided PCI. 4 th Imaging and Physiology Summit October 29 th, 2010 Seoul, Korea. Stanford
 4 th Imaging and Physiology Summit October 29 th, 2010 Seoul, Korea FFR-Guided PCI William F. Fearon, M.D. Associate Professor Division of Cardiovascular Medicine University Medical Center Disclosure Statement
4 th Imaging and Physiology Summit October 29 th, 2010 Seoul, Korea FFR-Guided PCI William F. Fearon, M.D. Associate Professor Division of Cardiovascular Medicine University Medical Center Disclosure Statement
FFR and intravascular imaging, which of which?
 FFR and intravascular imaging, which of which? Ayman Khairy MD, PhD, FESC Associate professor of Cardiovascular Medicine Vice Director of Assiut University Hospitals Assiut, Egypt Diagnostic assessment
FFR and intravascular imaging, which of which? Ayman Khairy MD, PhD, FESC Associate professor of Cardiovascular Medicine Vice Director of Assiut University Hospitals Assiut, Egypt Diagnostic assessment
Fractional Flow Reserve (FFR) --Practical Set Up Pressure Measurement --
 --Practical Set Up Pressure Measurement --") Fractional Flow Reserve (FFR) --Practical Set Up Pressure Measurement -- JoonHyung Doh, MD, PhD Assistant Professor, Vision21 Cardiac and Vascular Center Inje University Ilsan Paik Hospital Goyang, Korea
Fractional Flow Reserve (FFR) --Practical Set Up Pressure Measurement -- JoonHyung Doh, MD, PhD Assistant Professor, Vision21 Cardiac and Vascular Center Inje University Ilsan Paik Hospital Goyang, Korea
PCIs on Intermediate Lesions NCDR Cath-PCI Registry
 Practical Application Of Coronary Physiology in The Cath Lab Talal T Attar, MD, MBA, FACC PCIs on Intermediate Lesions NCDR Cath-PCI Registry Fraction of stenoses 50-70% treated with PCI without further
Practical Application Of Coronary Physiology in The Cath Lab Talal T Attar, MD, MBA, FACC PCIs on Intermediate Lesions NCDR Cath-PCI Registry Fraction of stenoses 50-70% treated with PCI without further
Fractional Flow Reserve and instantaneous wave -free Ratio. Λάμπρος Κ. Μόσιαλος Επεμβατικός Καρδιολόγος ΓΝ Παπαγεωργίου
 Fractional Flow Reserve and instantaneous wave -free Ratio Λάμπρος Κ. Μόσιαλος Επεμβατικός Καρδιολόγος ΓΝ Παπαγεωργίου DISCLOSURES There are no financial conflicts of interest relevant to this presentation
Fractional Flow Reserve and instantaneous wave -free Ratio Λάμπρος Κ. Μόσιαλος Επεμβατικός Καρδιολόγος ΓΝ Παπαγεωργίου DISCLOSURES There are no financial conflicts of interest relevant to this presentation
Benefit of Performing PCI Based on FFR
 Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Management of stable CAD FFR guided therapy: the new gold standard
 Management of stable CAD FFR guided therapy: the new gold standard Suleiman Kharabsheh, MD Director; CCU, Telemetry and CHU Associate professor of Cardiology, Alfaisal Univ. KFHI - KFSHRC Should patients
Management of stable CAD FFR guided therapy: the new gold standard Suleiman Kharabsheh, MD Director; CCU, Telemetry and CHU Associate professor of Cardiology, Alfaisal Univ. KFHI - KFSHRC Should patients
Pressure Wire Study. Fractional Flow Reserve (FFR) Nishat Jahagirdar Principal Clinical Cardiac Physiologist Kings College Hospital
 Nishat Jahagirdar Principal Clinical Cardiac Physiologist Kings College Hospital") Pressure Wire Study Fractional Flow Reserve (FFR) Nishat Jahagirdar Principal Clinical Cardiac Physiologist Kings College Hospital History Andreas Gruentzig s paper on Non operative dilation of coronaryartery
Pressure Wire Study Fractional Flow Reserve (FFR) Nishat Jahagirdar Principal Clinical Cardiac Physiologist Kings College Hospital History Andreas Gruentzig s paper on Non operative dilation of coronaryartery
FFR= Qs/Qn. Ohm s law R= P/Q Q=P/R
 32 ο Πανελλήνιο Καρδιολογικό Συνζδριο, Θεσσαλονίκη 20/10/2011 Gould KL et al, JACC CARDIOVASC IMAG 2009 Gould KL et al AM J CARDIOL 1974 & JACC CARDIOVASC IMAG 2009 Under maximal hyperemia: Rs=Rn FFR=
32 ο Πανελλήνιο Καρδιολογικό Συνζδριο, Θεσσαλονίκη 20/10/2011 Gould KL et al, JACC CARDIOVASC IMAG 2009 Gould KL et al AM J CARDIOL 1974 & JACC CARDIOVASC IMAG 2009 Under maximal hyperemia: Rs=Rn FFR=
Integrated Use of IVUS and FFR for LM Stenting
 Integrated Use of IVUS and FFR for LM Stenting Gary S. Mintz, MD Cardiovascular Research Foundation Four studies have highlighted the inaccuracy of angiography in the assessment of LMCA disease Fisher
Integrated Use of IVUS and FFR for LM Stenting Gary S. Mintz, MD Cardiovascular Research Foundation Four studies have highlighted the inaccuracy of angiography in the assessment of LMCA disease Fisher
Coronary Physiology and FFR. David H. Sibley MD FACC, FSCAI, FACP
 Coronary Physiology and FFR David H. Sibley MD FACC, FSCAI, FACP Braunwald s Heart Disease, 7 th Edition Control of Coronary Blood Flow 1. CFR = max flow/basal flow and decreases with increasing stenosis
Coronary Physiology and FFR David H. Sibley MD FACC, FSCAI, FACP Braunwald s Heart Disease, 7 th Edition Control of Coronary Blood Flow 1. CFR = max flow/basal flow and decreases with increasing stenosis
FFR: Tips and Tricks. A/Prof (Adj) Yeo Khung Keong, MBBS, FAMS, FACC, FSCAI National Heart Centre Singapore
 Yeo Khung Keong, MBBS, FAMS, FACC, FSCAI National Heart Centre Singapore") FFR: Tips and Tricks A/Prof (Adj) Yeo Khung Keong, MBBS, FAMS, FACC, FSCAI National Heart Centre Singapore Disclosures Abbott Vascular: Speaker, Proctor (MitraClip) Boston Scientific: Consultant, honorarium
FFR: Tips and Tricks A/Prof (Adj) Yeo Khung Keong, MBBS, FAMS, FACC, FSCAI National Heart Centre Singapore Disclosures Abbott Vascular: Speaker, Proctor (MitraClip) Boston Scientific: Consultant, honorarium
Coronary artery disease (CAD): Fractional Flow Reserve (FFR) for Pilots Risk Assessment. B. Haaff, R. Quast
: Fractional Flow Reserve (FFR) for Pilots Risk Assessment. B. Haaff, R. Quast") Coronary artery disease (CAD): Fractional Flow Reserve (FFR) for Pilots Risk Assessment B. Haaff, R. Quast Aeromedical Center Germany, Stuttgart-Airport Westpfalz-Klinikum, Kaiserslautern, Germany Disclosure
Coronary artery disease (CAD): Fractional Flow Reserve (FFR) for Pilots Risk Assessment B. Haaff, R. Quast Aeromedical Center Germany, Stuttgart-Airport Westpfalz-Klinikum, Kaiserslautern, Germany Disclosure
CASE from South Korea
 CASE from South Korea Bon-Kwon Koo, MD, PhD, Seoul, Korea Outpatient clinic of a non-interventional cardiologist F/56 Chief complaint: Angina with recent aggravation, CCS II~III Brief history: # Stroke
CASE from South Korea Bon-Kwon Koo, MD, PhD, Seoul, Korea Outpatient clinic of a non-interventional cardiologist F/56 Chief complaint: Angina with recent aggravation, CCS II~III Brief history: # Stroke
Evaluation of Intermediate Coronary lesions: Can You Handle the Pressure? Jeffrey A Southard, MD May 4, 2013
 Evaluation of Intermediate Coronary lesions: Can You Handle the Pressure? Jeffrey A Southard, MD May 4, 2013 Disclosures Consultant- St Jude Medical Boston Scientific Speaker- Volcano Corporation Heart
Evaluation of Intermediate Coronary lesions: Can You Handle the Pressure? Jeffrey A Southard, MD May 4, 2013 Disclosures Consultant- St Jude Medical Boston Scientific Speaker- Volcano Corporation Heart
Fractional Flow Reserve (FFR) --Practical Set Up Pressure Measurement --
 --Practical Set Up Pressure Measurement --") Fractional Flow Reserve (FFR) --Practical Set Up Pressure Measurement -- Joon Hyung Doh, MD, PhD Associate Professor, Division of Cardiology Inje University Ilsan Paik Hospital Goyang, Korea 목차 Fractional
Fractional Flow Reserve (FFR) --Practical Set Up Pressure Measurement -- Joon Hyung Doh, MD, PhD Associate Professor, Division of Cardiology Inje University Ilsan Paik Hospital Goyang, Korea 목차 Fractional
Diffuse Disease and Serial Stenoses. Bernard De Bruyne Cardiovascular Center Aalst Belgium
 Diffuse Disease and Serial Stenoses Bernard De Bruyne Cardiovascular Center Aalst Belgium Atherosclerosis is a Diffuse Disease Serial Stenoses A B P a P m P d When A is isolated, hyperemic flow through
Diffuse Disease and Serial Stenoses Bernard De Bruyne Cardiovascular Center Aalst Belgium Atherosclerosis is a Diffuse Disease Serial Stenoses A B P a P m P d When A is isolated, hyperemic flow through
Prognostic Value of Gated Myocardial Perfusion SPECT
 Current Use of IVUS & FFR George D. Dangas, MD, PhD, FACC, FSCAI Professor of Medicine Mount Sinai School of Medicine Prognostic Value of Gated Myocardial Perfusion SPECT 0.6% / year, Cardiac Death and
Current Use of IVUS & FFR George D. Dangas, MD, PhD, FACC, FSCAI Professor of Medicine Mount Sinai School of Medicine Prognostic Value of Gated Myocardial Perfusion SPECT 0.6% / year, Cardiac Death and
ROLE OF CORONARY PRESSURE & FFR IN MULTIVESSEL DISEASE
 ROLE OF CORONARY PRESSURE & FFR IN MULTIVESSEL DISEASE Angioplasty Summit TCT ASIA Seoul, Korea, april 24th, 2008 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands A rather common
ROLE OF CORONARY PRESSURE & FFR IN MULTIVESSEL DISEASE Angioplasty Summit TCT ASIA Seoul, Korea, april 24th, 2008 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands A rather common
Diffuse Disease and Serial Stenoses
 Diffuse Disease and Serial Stenoses Bernard De Bruyne Cardiovascular Center Aalst Belgium Atherosclerosis is a Diffuse Disease Serial Stenoses A B P a P m P d When A is isolated, hyperemic flow through
Diffuse Disease and Serial Stenoses Bernard De Bruyne Cardiovascular Center Aalst Belgium Atherosclerosis is a Diffuse Disease Serial Stenoses A B P a P m P d When A is isolated, hyperemic flow through
Noninvasive Fractional Flow Reserve from Coronary CT Angiography
 2016 KSC Annual Spring Scientific Conference Noninvasive Fractional Flow Reserve from Coronary CT Angiography Bon-Kwon Koo, MD, PhD, Seoul, Korea Why the hemodynamics for coronary artery disease? Twinlifemarketing.com.au
2016 KSC Annual Spring Scientific Conference Noninvasive Fractional Flow Reserve from Coronary CT Angiography Bon-Kwon Koo, MD, PhD, Seoul, Korea Why the hemodynamics for coronary artery disease? Twinlifemarketing.com.au
FFR-guided Jailed Side Branch Intervention
 FFR-guided Jailed Side Branch Intervention - Pressure wire in Bifurcation lesions - Bon-Kwon Koo, MD, PhD Seoul National University Hospital, Seoul, Korea Bifurcation Lesions Bifurcation Lesions Still
FFR-guided Jailed Side Branch Intervention - Pressure wire in Bifurcation lesions - Bon-Kwon Koo, MD, PhD Seoul National University Hospital, Seoul, Korea Bifurcation Lesions Bifurcation Lesions Still
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD
 Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Plaque Shift vs. Carina Shift Prevalence and Implication
 TCTAP 2013 Fellowship Course Left Main and Bifurcation PCI: Bifurcation PCI Plaque Shift vs. Carina Shift Prevalence and Implication Soo-Jin Kang, MD., PhD. Department of Cardiology, University of Ulsan
TCTAP 2013 Fellowship Course Left Main and Bifurcation PCI: Bifurcation PCI Plaque Shift vs. Carina Shift Prevalence and Implication Soo-Jin Kang, MD., PhD. Department of Cardiology, University of Ulsan
Upgrade of Recommendation
 Challenges in LM PCI Decision-making process for stenting Young-Hak Kim, MD, PhD, Heart Institute, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea Upgrade of Recommendation for
Challenges in LM PCI Decision-making process for stenting Young-Hak Kim, MD, PhD, Heart Institute, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea Upgrade of Recommendation for
Fractional Flow Reserve and the Results of the FAME Study
 Imaging and Physiology Summit Seoul, Korea November 21 st, 2009 Fractional Flow Reserve and the Results of the FAME Study William F. Fearon, M.D. Assistant Professor Division of Cardiovascular Medicine
Imaging and Physiology Summit Seoul, Korea November 21 st, 2009 Fractional Flow Reserve and the Results of the FAME Study William F. Fearon, M.D. Assistant Professor Division of Cardiovascular Medicine
Κλινική Χρήση IVUS και OCT PERIKLIS A. DAVLOUROS ASSOCIATE PROFESSOR OF CARDIOLOGY INVASIVE CARDIOLOGY & CONGENITAL HEART DISEASE
 Κλινική Χρήση IVUS και OCT PERIKLIS A. DAVLOUROS ASSOCIATE PROFESSOR OF CARDIOLOGY INVASIVE CARDIOLOGY & CONGENITAL HEART DISEASE Conflict of interest None to declare While IVUS is the most used intravascular
Κλινική Χρήση IVUS και OCT PERIKLIS A. DAVLOUROS ASSOCIATE PROFESSOR OF CARDIOLOGY INVASIVE CARDIOLOGY & CONGENITAL HEART DISEASE Conflict of interest None to declare While IVUS is the most used intravascular
Controversies in Coronary Revascularization. Atlanta CCU April 15, 2016
 Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
Hybrid cardiac imaging Advantages, limitations, clinical scenarios and perspectives for the future
 Hybrid cardiac imaging Advantages, limitations, clinical scenarios and perspectives for the future Prof. Juhani Knuuti, MD, FESC Turku, Finland Disclosure: Juhani Knuuti, M.D. Juhani Knuuti, M.D. has financial
Hybrid cardiac imaging Advantages, limitations, clinical scenarios and perspectives for the future Prof. Juhani Knuuti, MD, FESC Turku, Finland Disclosure: Juhani Knuuti, M.D. Juhani Knuuti, M.D. has financial
Pearls & Pitfalls in nuclear cardiology
 Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
Anatomical, physiological and clinical relevance of a side branch
 Anatomical, physiological and clinical relevance of a side branch : Which branch really needs a stent? Bon-Kwon Koo, MD, PhD, Seoul, Korea Bifurcation lesion: The GREAT EQUALIZER! No intervention = Balloon
Anatomical, physiological and clinical relevance of a side branch : Which branch really needs a stent? Bon-Kwon Koo, MD, PhD, Seoul, Korea Bifurcation lesion: The GREAT EQUALIZER! No intervention = Balloon
Malaysian Healthy Ageing Society
 Organised by: Co-Sponsored: Malaysian Healthy Ageing Society CAD INVESTIGATIONS PHYSIOLOGICAL / FUNCTIONAL VS ANATOMICAL / STRUCTURAL Disclosure iheal medical centre is a one stop cardiac centre with
Organised by: Co-Sponsored: Malaysian Healthy Ageing Society CAD INVESTIGATIONS PHYSIOLOGICAL / FUNCTIONAL VS ANATOMICAL / STRUCTURAL Disclosure iheal medical centre is a one stop cardiac centre with
FFR in diffuse disease and serial stenoses
 FFR in diffuse disease and serial stenoses Educational Training Program ESC European Heart House Apr. 25-27 2013 Nils Witt MD PhD, Södersjukhuset, Stockholm, Sweden Single stenosis Functionally Functional
FFR in diffuse disease and serial stenoses Educational Training Program ESC European Heart House Apr. 25-27 2013 Nils Witt MD PhD, Södersjukhuset, Stockholm, Sweden Single stenosis Functionally Functional
MULTIVESSEL PCI. IN DRUG-ELUTING STENT RESTENOSIS DUE TO STENT FRACTURE, TREATED WITH REPEAT DES IMPLANTATION
 MULTIVESSEL PCI. IN DRUG-ELUTING STENT RESTENOSIS DUE TO STENT FRACTURE, TREATED WITH REPEAT DES IMPLANTATION C. Graidis, D. Dimitriadis, A. Ntatsios, V. Karasavvides Euromedica Kyanous Stavros, Thessaloniki.
MULTIVESSEL PCI. IN DRUG-ELUTING STENT RESTENOSIS DUE TO STENT FRACTURE, TREATED WITH REPEAT DES IMPLANTATION C. Graidis, D. Dimitriadis, A. Ntatsios, V. Karasavvides Euromedica Kyanous Stavros, Thessaloniki.
Technical Aspects and Clinical Indications of FFR
 Technical Aspects and Clinical Indications of FFR Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst - OLV Clinic Aalst, Belgium Potential conflicts of interest Consulting fees and honoraria on
Technical Aspects and Clinical Indications of FFR Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst - OLV Clinic Aalst, Belgium Potential conflicts of interest Consulting fees and honoraria on
Case report. Resistance in the cath lab : the utility of hyperemic stenosis resistance in the functional assessment of coronary artery disease
 Resistance in the cath lab : the utility of hyperemic stenosis resistance in the functional assessment of coronary artery disease Kalpa De Silva, Divaka Perera Cardiovascular Division, The Rayne Institute,
Resistance in the cath lab : the utility of hyperemic stenosis resistance in the functional assessment of coronary artery disease Kalpa De Silva, Divaka Perera Cardiovascular Division, The Rayne Institute,
FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium
 FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium Conflict of Interest Institutional research grants and speaker s fee from St. Jude Medical and Boston Scientic to Cardiovascular
FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium Conflict of Interest Institutional research grants and speaker s fee from St. Jude Medical and Boston Scientic to Cardiovascular
New Insight about FFR and IVUS MLA
 New Insight about FFR and IVUS MLA Can IVUS MLA Predict FFR
New Insight about FFR and IVUS MLA Can IVUS MLA Predict FFR
Instantaneous Wave-Free Ratio
 Instantaneous Wave-Free Ratio Alejandro Aquino MD Interventional Cardiology Fellow Washington University in St. Louis Barnes-Jewish Hospital Instantaneous Wave-Free Ratio Alejandro Aquino MD Disclosure
Instantaneous Wave-Free Ratio Alejandro Aquino MD Interventional Cardiology Fellow Washington University in St. Louis Barnes-Jewish Hospital Instantaneous Wave-Free Ratio Alejandro Aquino MD Disclosure
Can We Safely Defer PCI. Yes, already proven
 Can We Safely Defer PCI Just Based on FFR>0.80? Yes, already proven Seung-Jung Park, MD., PhD. Professor of Medicine, University of Ulsan, College of Medicine Heart Institute, Asan Medical Center, Seoul,
Can We Safely Defer PCI Just Based on FFR>0.80? Yes, already proven Seung-Jung Park, MD., PhD. Professor of Medicine, University of Ulsan, College of Medicine Heart Institute, Asan Medical Center, Seoul,
La FFR quoi d autre: En pratique? Pierre Deharo, CHU TIMONE, Marseille
 La FFR quoi d autre: En pratique? Pierre Deharo, CHU TIMONE, Marseille La FFR quoi d autre: En pratique? How to avoid non reliable results Management of MVD Non Culprit in STEMI Left main Severe AS Post
La FFR quoi d autre: En pratique? Pierre Deharo, CHU TIMONE, Marseille La FFR quoi d autre: En pratique? How to avoid non reliable results Management of MVD Non Culprit in STEMI Left main Severe AS Post
Left Main PCI. Integrated Use of IVUS and FFR. Seung-Jung Park, MD, PhD
 Left Main PCI Integrated Use of IVUS and FFR Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea Efficacy of Left
Left Main PCI Integrated Use of IVUS and FFR Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea Efficacy of Left
Anatomy is Destiny, But Physiology is Here Today
 Published on Journal of Invasive Cardiology (http://www.invasivecardiology.com) September, 2010 [1] Anatomy is Destiny, But Physiology is Here Today Thu, 9/9/10-10:54am 0 Comments Section: Commentary Issue
Published on Journal of Invasive Cardiology (http://www.invasivecardiology.com) September, 2010 [1] Anatomy is Destiny, But Physiology is Here Today Thu, 9/9/10-10:54am 0 Comments Section: Commentary Issue
IVUS-Guided d Provisional i Stenting: Plaque or Carina Shift. Soo-Jin Kang, MD., PhD.
 Left Main and Bifurcation Summit IVUS-Guided d Provisional i Stenting: ti Plaque or Carina Shift Soo-Jin Kang, MD., PhD. Department of Cardiology, University of Ulsan College of Medicine Asan Medical Center,
Left Main and Bifurcation Summit IVUS-Guided d Provisional i Stenting: ti Plaque or Carina Shift Soo-Jin Kang, MD., PhD. Department of Cardiology, University of Ulsan College of Medicine Asan Medical Center,
high SYNTAX Score? I Sheiban Division of Cardiology Interventional Card. University of Turin Turin / Italy
 What to do with patients with high SYNTAX Score? I Sheiban Division of Cardiology Interventional Card. University of Turin San Giovanni Battista Hospital Turin / Italy Who are the patients with high SYNTAX
What to do with patients with high SYNTAX Score? I Sheiban Division of Cardiology Interventional Card. University of Turin San Giovanni Battista Hospital Turin / Italy Who are the patients with high SYNTAX
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO!
 Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Effect of Intravascular Ultrasound- Guided vs. Angiography-Guided Everolimus-Eluting Stent Implantation: the IVUS-XPL Randomized Clinical Trial
 Effect of Intravascular Ultrasound- Guided vs. Angiography-Guided Everolimus-Eluting Stent Implantation: the IVUS-XPL Randomized Clinical Trial Myeong-Ki Hong, MD. PhD on behalf of the IVUS-XPL trial investigators
Effect of Intravascular Ultrasound- Guided vs. Angiography-Guided Everolimus-Eluting Stent Implantation: the IVUS-XPL Randomized Clinical Trial Myeong-Ki Hong, MD. PhD on behalf of the IVUS-XPL trial investigators
What do the guidelines say?
 Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Three-vessel fractional flow reserve measurement for predicting clinical prognosis in patients with coronary artery disease
 Editorial Three-vessel fractional flow reserve measurement for predicting clinical prognosis in patients with coronary artery disease Takashi Kubo, Hiroki Emori, Yosuke Katayama, Kosei Terada Department
Editorial Three-vessel fractional flow reserve measurement for predicting clinical prognosis in patients with coronary artery disease Takashi Kubo, Hiroki Emori, Yosuke Katayama, Kosei Terada Department
LM stenting - Cypher
 LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
ΑΝΤΙΓΝΩΜΙΕΣ ΣΤΗΝ ΕΠΕΜΒΑΤΙΚΗ ΚΑΡΔΙΟΛΟΓΙΑ:Νόσος στελέχους Αγγειοπλαστική
 ΑΝΤΙΓΝΩΜΙΕΣ ΣΤΗΝ ΕΠΕΜΒΑΤΙΚΗ ΚΑΡΔΙΟΛΟΓΙΑ:Νόσος στελέχους Αγγειοπλαστική X. ΓΡΑΪΔΗΣ Επεμβατικός καρδιολόγος, FSCAI Kλινική Euromedica-Κυανούς Σταυρός, Θεσσαλονίκη The Fear factor The two words LEFT MAIN
ΑΝΤΙΓΝΩΜΙΕΣ ΣΤΗΝ ΕΠΕΜΒΑΤΙΚΗ ΚΑΡΔΙΟΛΟΓΙΑ:Νόσος στελέχους Αγγειοπλαστική X. ΓΡΑΪΔΗΣ Επεμβατικός καρδιολόγος, FSCAI Kλινική Euromedica-Κυανούς Σταυρός, Θεσσαλονίκη The Fear factor The two words LEFT MAIN
Physiology (FFR & IFR) is Essential in Daily Pratice. Martine Gilard Brest University - France
 is Essential in Daily Pratice. Martine Gilard Brest University - France") Physiology (FFR & IFR) is Essential in Daily Pratice Martine Gilard Brest University - France Background Invasive assessment of atherosclerotic coronary artery lesion Morphological assessment IVUS X-ray
Physiology (FFR & IFR) is Essential in Daily Pratice Martine Gilard Brest University - France Background Invasive assessment of atherosclerotic coronary artery lesion Morphological assessment IVUS X-ray
CT FFR: Are you ready to totally change the way you diagnose Coronary Artery Disease?
 CT FFR: Are you ready to totally change the way you diagnose Coronary Artery Disease? Madan Mohan MD MRCP FACC CQO, Division of Cardiovascular Medicine University Hospitals Case Medical Center Assistant
CT FFR: Are you ready to totally change the way you diagnose Coronary Artery Disease? Madan Mohan MD MRCP FACC CQO, Division of Cardiovascular Medicine University Hospitals Case Medical Center Assistant
Novel insights into the complexity of ischaemic heart disease derived from combined coronary pressure and flow velocity measurements van de Hoef, T.P.
 UvA-DARE (Digital Academic Repository) Novel insights into the complexity of ischaemic heart disease derived from combined coronary pressure and flow velocity measurements van de Hoef, T.P. Link to publication
UvA-DARE (Digital Academic Repository) Novel insights into the complexity of ischaemic heart disease derived from combined coronary pressure and flow velocity measurements van de Hoef, T.P. Link to publication
ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions
 Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
Relations of Interest
 Relations of Interest Consulting Fees on my behalf go to the Cardiovascular Research Center Aalst Contracted Research between the Cardiovascular Research Center Aalst and several pharmaceutical and device
Relations of Interest Consulting Fees on my behalf go to the Cardiovascular Research Center Aalst Contracted Research between the Cardiovascular Research Center Aalst and several pharmaceutical and device
Approach to Multi Vessel disease with STEMI
 Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
Integrating IVUS, FFR, and Noninvasive Imaging to Optimize Outcomes. Gary S. Mintz, MD Cardiovascular Research Foundation
 Integrating IVUS, FFR, and Noninvasive Imaging to Optimize Outcomes Gary S. Mintz, MD Cardiovascular Research Foundation COURAGE Nuclear Substudy (n=314) Death/MI according the residual ischemia (SPECT)
Integrating IVUS, FFR, and Noninvasive Imaging to Optimize Outcomes Gary S. Mintz, MD Cardiovascular Research Foundation COURAGE Nuclear Substudy (n=314) Death/MI according the residual ischemia (SPECT)
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients
 Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
FFR vs icecg in Coronary Bifurcations FIESTA ClinicalTrials.gov Identifier: NCT
 FFR vs icecg in Coronary Bifurcations FIESTA ClinicalTrials.gov Identifier: NCT01724957 Dobrin Vassilev MD, PhD Assoc. Prof. in Cardiology Head Cardiology Clinic, Alexandrovska University Hospital Medical
FFR vs icecg in Coronary Bifurcations FIESTA ClinicalTrials.gov Identifier: NCT01724957 Dobrin Vassilev MD, PhD Assoc. Prof. in Cardiology Head Cardiology Clinic, Alexandrovska University Hospital Medical
I have no financial disclosures
 Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
FFR-CT Not Ready for Primetime
 FFR-CT Not Ready for Primetime Leslee J. Shaw, PhD, MASNC, FACC, FAHA, FSCCT R. Bruce Logue Professor of Medicine Co-Director, Emory Clinical CV Research Institute Emory University School of Medicine Atlanta,
FFR-CT Not Ready for Primetime Leslee J. Shaw, PhD, MASNC, FACC, FAHA, FSCCT R. Bruce Logue Professor of Medicine Co-Director, Emory Clinical CV Research Institute Emory University School of Medicine Atlanta,
FFR in unstable angina and after MI F
 FFR in unstable angina and after MI F June-Hong Kim, MD. PhD Cardiovascular center Pusan National University Yangsan Hospital FFR tells you physiologic stenosis severity rather than anatomical stenosis
FFR in unstable angina and after MI F June-Hong Kim, MD. PhD Cardiovascular center Pusan National University Yangsan Hospital FFR tells you physiologic stenosis severity rather than anatomical stenosis
FFR and ifr: Similarities, Differences, and Clinical Implication
 Annals of Nuclear Cardiology Vol. 3No. 1 53-60 REVIEW ARTICLE : Similarities, Differences, and Clinical Implication Hitoshi Matsuo, MD, PhD, Yoshiaki Kawase, MD and Itta Kawamura, MD, PhD Received: July
Annals of Nuclear Cardiology Vol. 3No. 1 53-60 REVIEW ARTICLE : Similarities, Differences, and Clinical Implication Hitoshi Matsuo, MD, PhD, Yoshiaki Kawase, MD and Itta Kawamura, MD, PhD Received: July
Side Branch Occlusion
 Side Branch Occlusion Mechanism, Outcome, and How to avoid it From COBIS II Registry Hyeon-Cheol Gwon Cardiac&Vascular Center, Samsung Medical Center Sungkyunkwan University School of Medicine SB occlusion
Side Branch Occlusion Mechanism, Outcome, and How to avoid it From COBIS II Registry Hyeon-Cheol Gwon Cardiac&Vascular Center, Samsung Medical Center Sungkyunkwan University School of Medicine SB occlusion
Cindy L. Grines MD FACC FSCAI
 Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
IVUS vs FFR Debate: IVUS-Guided PCI
 IVUS vs FFR Debate: IVUS-Guided PCI Gary S. Mintz, MD Cardiovascular Research Foundation New York, NY Disclosure Statement of Financial Interest Within the past 12 months, I have had a financial interest/arrangement
IVUS vs FFR Debate: IVUS-Guided PCI Gary S. Mintz, MD Cardiovascular Research Foundation New York, NY Disclosure Statement of Financial Interest Within the past 12 months, I have had a financial interest/arrangement
CT or PET/CT for coronary artery disease
 CT or PET/CT for coronary artery disease Rotterdam 2012 Juhani Knuuti, MD, PhD, FESC Turku PET Centre University of Turku Turku, Finland Juhani.knuuti@utu.fi Turku PET Centre University of Turku Åbo Akademi
CT or PET/CT for coronary artery disease Rotterdam 2012 Juhani Knuuti, MD, PhD, FESC Turku PET Centre University of Turku Turku, Finland Juhani.knuuti@utu.fi Turku PET Centre University of Turku Åbo Akademi
Coronary Artery Disease: Revascularization (Teacher s Guide)
") Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)?
 or Coronary Artery Bypass Graft Surgery (CABG)?") Cronicon OPEN ACCESS CARDIOLOGY Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)? Valentin Hristov* Department of Cardiology, Specialized
Cronicon OPEN ACCESS CARDIOLOGY Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)? Valentin Hristov* Department of Cardiology, Specialized
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
THE COMPLEX RELATION BETWEEN VULNERABILITY AND ISCHEMIA a paradigm shift
 THE COMPLEX RELATION BETWEEN VULNERABILITY AND ISCHEMIA a paradigm shift Angioplasty Summit TCT ASIA Seoul, Korea, april 23rd, 2008 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands
THE COMPLEX RELATION BETWEEN VULNERABILITY AND ISCHEMIA a paradigm shift Angioplasty Summit TCT ASIA Seoul, Korea, april 23rd, 2008 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands
EAE Teaching Course. Magnetic Resonance Imaging. Competitive or Complementary? Sofia, Bulgaria, 5-7 April F.E. Rademakers
 EAE Teaching Course Magnetic Resonance Imaging Competitive or Complementary? Sofia, Bulgaria, 5-7 April 2012 F.E. Rademakers Complementary? Of Course N Engl J Med 2012;366:54-63 Clinical relevance Treatment
EAE Teaching Course Magnetic Resonance Imaging Competitive or Complementary? Sofia, Bulgaria, 5-7 April 2012 F.E. Rademakers Complementary? Of Course N Engl J Med 2012;366:54-63 Clinical relevance Treatment
FAME STUDY: 2-year Follow-Up & CLINICAL SUBGROUP ANALYSIS
 Coronary Physiology In The Cathlab FAME STUDY: 2-year Follow-Up & CLINICAL SUBGROUP ANALYSIS Educational Training Program ESC European Heart House april 7th 9th 2011 Nico H.J.Pijls, MD, PhD Catharina Hospital,
Coronary Physiology In The Cathlab FAME STUDY: 2-year Follow-Up & CLINICAL SUBGROUP ANALYSIS Educational Training Program ESC European Heart House april 7th 9th 2011 Nico H.J.Pijls, MD, PhD Catharina Hospital,
Better CABGs vs Better PCI Devices
 CABG vs PCI 2017 Multivessel Coronary Disease Better CABGs vs Better PCI Devices ACC New York, Dec 8, 2017 No Disclosures CABG vs PCI 2017 Stable Multivessel Coronary Disease 1. Are These The two Critical
CABG vs PCI 2017 Multivessel Coronary Disease Better CABGs vs Better PCI Devices ACC New York, Dec 8, 2017 No Disclosures CABG vs PCI 2017 Stable Multivessel Coronary Disease 1. Are These The two Critical
Fractional Flow Reserve from Coronary CT Angiography (and some neat CT images)
") Fractional Flow Reserve from Coronary CT Angiography (and some neat CT images) Victor Cheng, M.D. Director, Cardiovascular CT Oklahoma Heart Institute 1 Disclosures Tornadoes scare me 2 Treating CAD Fixing
Fractional Flow Reserve from Coronary CT Angiography (and some neat CT images) Victor Cheng, M.D. Director, Cardiovascular CT Oklahoma Heart Institute 1 Disclosures Tornadoes scare me 2 Treating CAD Fixing
The SYNTAX-LE MANS Study
 The SYNTAX-LE MANS Study Synergy Between PCI with TAXUS Express and Cardiac Surgery: Late (15-month) Left Main Angiographic Substudy A. Pieter Kappetein, MD, PhD Erasmus MC, Rotterdam, NL SYNTAX-LE MANS
The SYNTAX-LE MANS Study Synergy Between PCI with TAXUS Express and Cardiac Surgery: Late (15-month) Left Main Angiographic Substudy A. Pieter Kappetein, MD, PhD Erasmus MC, Rotterdam, NL SYNTAX-LE MANS
Fractional Flow Reserve (FFR)
") Non-invasive FFR using coronary CT angiography and computational fluid dyn amics predicts the hemodynamic signifi cance of coronary lesions First in man experience with CT-Flow Andrejs Erglis, Sanda Jegere,
Non-invasive FFR using coronary CT angiography and computational fluid dyn amics predicts the hemodynamic signifi cance of coronary lesions First in man experience with CT-Flow Andrejs Erglis, Sanda Jegere,
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users
 Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
Should we be using fractional flow reserve more routinely to select stable coronary patients for percutaneous coronary intervention?
 REVIEW C URRENT OPINION Should we be using fractional flow reserve more routinely to select stable coronary patients for percutaneous coronary intervention? Seung-Jung Park and Jung-Min Ahn Purpose of
REVIEW C URRENT OPINION Should we be using fractional flow reserve more routinely to select stable coronary patients for percutaneous coronary intervention? Seung-Jung Park and Jung-Min Ahn Purpose of
Which Test When? Avoid the Stress of Stress Testing. Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute
 Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
CARDIOLOGY GRAND ROUNDS
 CARDIOLOGY GRAND ROUNDS Title: Fractional flow reserve (FFR) Computed tomography (CT) Speaker: John R. Lesser, MD Senior Consulting Cardiologist, Medical Director CT/CMR Minneapolis Heart Institute at
CARDIOLOGY GRAND ROUNDS Title: Fractional flow reserve (FFR) Computed tomography (CT) Speaker: John R. Lesser, MD Senior Consulting Cardiologist, Medical Director CT/CMR Minneapolis Heart Institute at
Important LM bifurcation studies update
 8 th European Bifurcation Club 12-13 October 2012 - Barcelona Important LM bifurcation studies update I Sheiban E-mail: isheiban@yahoo.com Unprotected LM Percutaneous Revascularization What is important
8 th European Bifurcation Club 12-13 October 2012 - Barcelona Important LM bifurcation studies update I Sheiban E-mail: isheiban@yahoo.com Unprotected LM Percutaneous Revascularization What is important
Coronary Physiology in the Cath Lab: Beyond the Basics
 Coronary Physiology in the Cath Lab: Beyond the Basics Morton J. Kern, MD, FSCAI KEYWORDS Coronary artery disease Cardiac catheterization laboratory Translesional pressure measurement In-lab coronary physiology
Coronary Physiology in the Cath Lab: Beyond the Basics Morton J. Kern, MD, FSCAI KEYWORDS Coronary artery disease Cardiac catheterization laboratory Translesional pressure measurement In-lab coronary physiology
Percutaneous Intervention of Unprotected Left Main Disease
 Percutaneous Intervention of Unprotected Left Main Disease Technical feasibility and Clinical outcomes Seung-Jung Park, MD, PhD, FACC Professor of Internal Medicine Asan Medical Center, Seoul, Korea Unprotected
Percutaneous Intervention of Unprotected Left Main Disease Technical feasibility and Clinical outcomes Seung-Jung Park, MD, PhD, FACC Professor of Internal Medicine Asan Medical Center, Seoul, Korea Unprotected