Echocardiographic Evaluation of Aortic Valve Prosthesis
|
|
|
- Winfred Jacobs
- 5 years ago
- Views:
Transcription
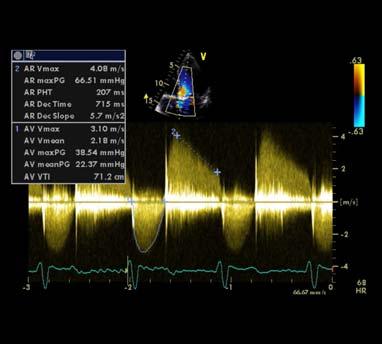
1 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine, OUWB School of Medicine ASCeXAM/ReASCE 2017 Philadelphia, PA Pre Questions (1) Regarding Aortic Prosthetic Valves A. A routine echocardiogram is required very two years after AVR B. An elevated gradient with a decreased EOA is always suggestive of valvular stenosis C. Transthoracic echocardiogram alone is always sufficient to diagnose valvular stenosis D. It is more challenging to quantify para valvular versus valvular aortic regurgitation. 1

2 Pre Questions (2) Patients with Prosthesis Patient Mismatch A. Have abnormal prosthetic valve function B. Progressively worsen with time C. Have a small valve compared to the demands of their body and cardiac output D. Have a benign condition JASE September

3 Topics of Discussion Types and Flow Profiles of Prosthetic Valves Echocardiographic Evaluation: Key Points Challenges for Evaluation Prosthetic Valves Evaluation Elevated gradients Regurgitation Endocarditis Thrombosis versus pannus Types & Flow Profiles of Prosthetic Valves Mechanical Vs. Bioprosthetic Vs. Autografts Copyright American Heart Association Pibarot P, Dumesnil J G Circulation 2009;119:



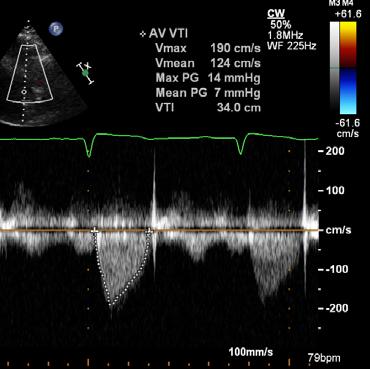
 AV max3.")
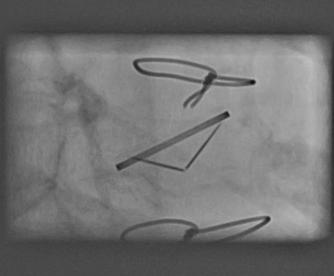
4 Types & Flow Profiles of Prosthetic Valves Mechanical Vs. Bioprosthetic Flow Localized Pressure Loss and High Gradient in Central Orifice of Bileaflet Mechanical Valve (?Pressure Recovery) AV max3.6 m/s MIG = 53 mmhg P Mean=30 mmhg Fluoroscopy 4
5 CLASS I ECHO EVALUATION Guidelines Initial TTE after AVR (2 4 weeks or sooner if concern for follow up and transfer) Repeat TTE for AVR if there is a change in clinical symptoms or signs suggesting dysfunction TEE for AVR if there is a change in clinical symptoms or signs suggesting dysfunction CLASS II Annual TTE in bioprosthetic valves after the first 10 years (5 years in prosthetic statement 2008) Nishimura et al 2014 but not mechanical valves ECHO EVALUATION: Key Points Clinical picture Baseline study Type and size of valve LV chamber BP/HR Height/weight/BSA Exercise echo may be helpful Cinefluoroscopy, CT, MRI 5

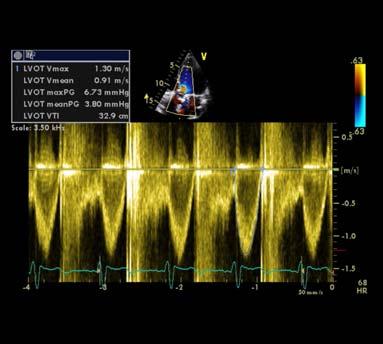
6 ECHO EVALUATION: Key Points Opening and Closing of leaflets or occluders Abnormal densities (calcium/mass/vegetation) Stability versus rocking motion May use Modified versus Simplified Bernoulli 4V 22 4V 12 Vs. 4V 2 2 Attention to flow states & adequate Doppler signals Echo Evaluation: Key Points Adequate Doppler Signals LVOT obtained away from flow acceleration (0.5 to 1 cm below sewing ring) Multiple planes Off axis view in parasternal view to obtain LVOT diameter/tavr versus SAVR Eccentric aortic regurgitant jets may require different angles to Doppler 6
7 Evaluation of Prosthetic Valves: Challenges Large range in what is considered normal Mean Gradients produced depend on size and type of valve. For any particular patient it is difficult to differentiate normal from abnormal, hence the need for comparison to older studies Shadowing may interfere with assessment of location and amount of regurgitation Bioprosthetic Valve Abnormalities Elevated Gradients Regurgitation Endocarditis Thrombosis Pannus 7
8 Echocardiographic Evaluation of Elevated Prosthetic Valve Gradients DVI 0.30 DVI DVI <0.25 Jet contour AT (ms) >100 <100 >100 <100 Consider PrAV stenosis with: Sub valve narrowing Underestimated gradient Improper LVOT velocity Normal PrAV EOA index Suggests prosthetic aortic valve stenosis Consider improper LVOT velocity High flow PPM JASE 2009;22(9):975 8


9 Parameters Utilized Peak prosthetic aortic velocity Normal < 3 m/sec Abnormal > 3 m/sec Parameters Utilized Doppler Velocity Index 9




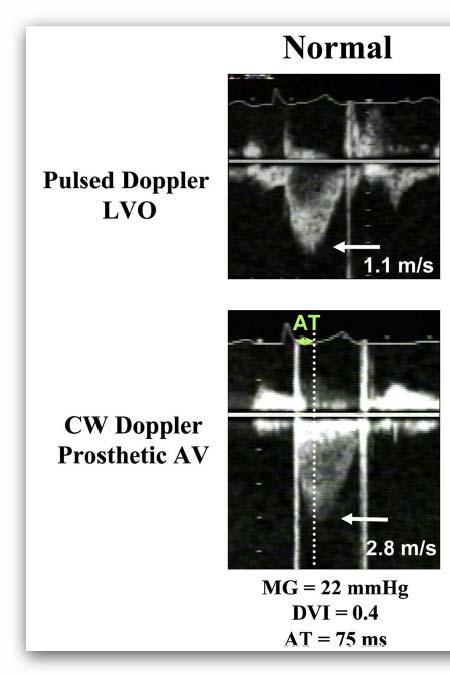
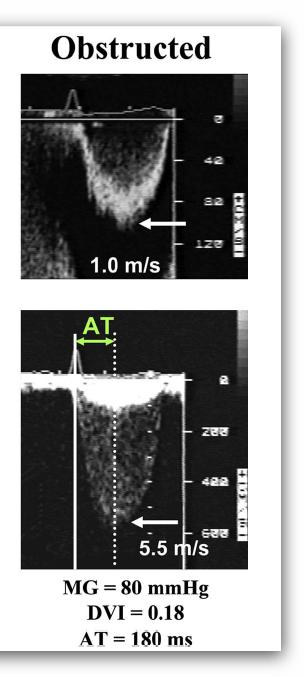
10 Doppler Velocity Index 1.1/2.8 = 0.39 Normal > 0.3 1/5.5 = 0.18 Abnormal < 0.25 Jet Contour Parameters Utilized Triangular Rounded 10
11 Acceleration Time Parameters Utilized msec Normal < 100 msec 150 msec Abnormal > 100 msec Parameters Utilized Acceleration time/ ejection time AT/ET > 0.4: Prosthetic valve obstruction No Obstruction:0.31 Obstruction:
 Assessment Increased")
12 Parameters Utilized Effective Orifice Area and ieoa A 2 (EOA)= A 1 x V 1 V 2 ieoa = AVA/BSA Normal > 1.2 cm 2 Abnormal < 0.8 cm 2 Abnormal < 0.6 cm 2 /m 2 Cause of Elevated Gradients Across Aortic Prosthesis Errors in Measurement Improper LVOT Velocity Taken too far from flow acceleration Improper AV Velocity (Gradient) Assessment Increased Flow Pressure Recovery Prosthesis patient mismatch Prosthesis stenosis 12
13 NORMAL PROSTHESIS FUNCTION 13
14 PROSTHETIC STENOSIS 14

15 Doppler of Prosthetic Aortic Valve Function Normal Possible Stenosis Suggests Stenosis Peak Velocity < 3 m/s 3 4 m/sec > 4 m/s Mean Gradient < 20 mmhg mmhg > 35 mmhg Doppler Velocity Index Effective Orifice area Contour of Jet > < 0.25 > 1.2 cm cm 2 < 0.8 cm 2 Triangular Early Peaking Triangular to intermediate Rounded Symmetrical contour Acceleration Time < 80 ms ms > 100 ms Mechanisms of Prosthetic Valve Dysfunction 15
 TTE: Difficult to visualize")
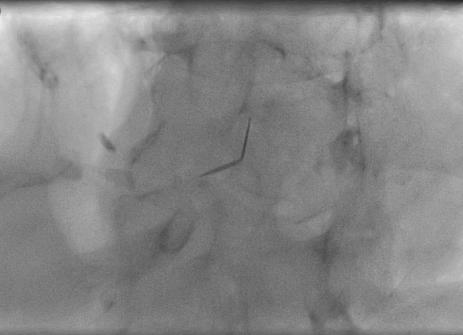
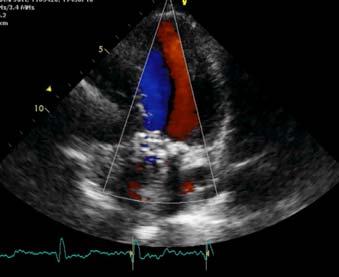
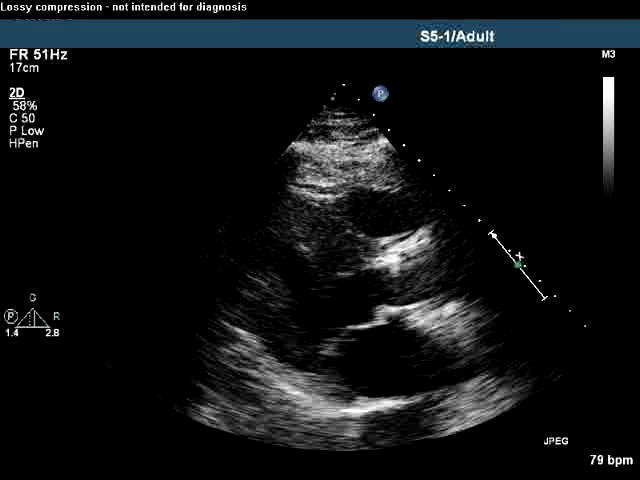
16 CASE PRESENTATIONS CASE PRESENTATION (1): 81 Y/O with progressive DOE PMHx: Rheumatic valve disease, CABG + Mechanical AVR 2003 (19 St Jude Regent Valve) TTE: Difficult to visualize mechanical AV 16



17 AV VEL=3.2 DI=0.58/3.2=0.18 AT=150msec Jet Contour: Circular An approach to prosthetic AV stenosis 17
18 An approach to prosthetic AV stenosis Doppler Parameters of Prosthetic Aortic Valve Function Normal Suggests Stenosis Peak Velocity < 3 m/s > 4 m/s Mean Gradient < 20 mmhg > 35 mmhg Doppler Velocity Index >= 0.3 < 0.25 Effective Orifice area > 1.2 cm2 < 0.8 cm2 Contour of Jet Triangular Early Peaking ms Rounded Symmetrical contour Acceleration Time < 80 ms > 100 ms 18
19 What is your diagnosis? A) Normal Prosthetic Valve Function B) Prosthesis Patient Mismatch C) High Flow State D) Prosthetic Valve Stenosis E) Errors of Measurement: Improper LVOT Velocity Additional Studies Needed? 19




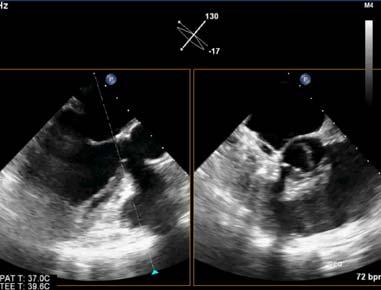
20 TEE Helpful with high gradients and normal motion by Fluoro 20

 On Coumadin,")

21 CASE PRESENTATION (2): 67 Y/O F Hx AVR (Bi Leaflet Mechanical Valve 1998) On Coumadin, difficulty maintaining therapeutic INR Progressive DOE 6 mos 21


22 AV VEL = 3.6 DVI = 1.19 / 3.60 DVI = 0.33 Acceleration Time 0.11 sec 22
23 Doppler Parameters of Prosthetic Aortic Valve Function Normal Suggests Stenosis Peak Velocity < 3 m/s > 4 m/s Mean Gradient < 20 mmhg > 35 mmhg Doppler Velocity Index >= 0.3 < 0.25 Effective Orifice area > 1.2 cm2 < 0.8 cm2 Contour of Jet Triangular Early Peaking ms Rounded Symmetrical contour Acceleration Time < 80 ms > 100 ms An approach to prosthetic AV stenosis 23
")
24 An approach to prosthetic AV stenosis Original LVOT Velocity Taken Too Close to the AV Prosthesis (region of subvalvular acceleration) 24

25 DVI = LVO / AV Jet DVI = 0.82 / 3.60 DVI = 0.22 Original LVOT Velocity Taken Too Close to the AV Prosthesis Doppler Parameters of Prosthetic Aortic Valve Function Normal Suggests Stenosis Peak Velocity < 3 m/s > 4 m/s Mean Gradient < 20 mmhg > 35 mmhg Doppler Velocity Index >= 0.3 < 0.25 Effective Orifice area > 1.2 cm2 < 0.8 cm2 Contour of Jet Triangular Early Peaking ms Rounded Symmetrical contour Acceleration Time < 80 ms > 100 ms 25
26 An approach to prosthetic AV stenosis An approach to prosthetic AV stenosis 26


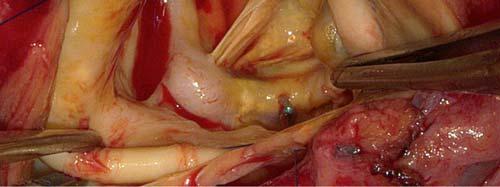
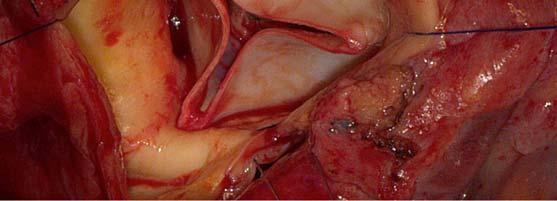
27 Surgical Findings Well seated valve with a large amount of tissue ingrowth beneath the valve resulting in a frozen leaflet An approach to prosthetic AV stenosis 27
28 What is your diagnosis? A) Patient Prosthesis Mismatch B) Normal Prosthetic Valve Function C) High Flow State D) Prosthetic Valve Stenosis E) Improper LVOT Velocity What is your diagnosis? A) Patient Prosthesis Mismatch B) Normal Prosthetic Valve Function C) High Flow State D) Prosthetic Valve Stenosis E) Improper LVOT Velocity (Prosthetic valve stenosis) 28


")
29 CASE PRESENTATION (3): 66 Y/O F Hx AVR (St Jude Valve Conduit 2002 for AR) Progressive DOE 29




30 LVOT VELOCITY = 0.85 AVA VELOCITY = 3.4 DVI= 0.85/3.4 = 0.25 AVA VELOCITY = 3.4 m/s AT= 0.09 sec 30
31 Doppler Parameters of Prosthetic Aortic Valve Function Normal Suggests Stenosis Peak Velocity < 3 m/s > 4 m/s Mean Gradient < 20 mmhg > 35 mmhg Doppler Velocity Index >= 0.3 < 0.25 Effective Orifice area > 1.2 cm2 < 0.8 cm2 Contour of Jet Triangular Early Peaking Rounded Symmetrical contour Acceleration Time < 80 ms > 100 ms Doppler Parameters of Prosthetic Aortic Valve Function Normal Suggests Stenosis Peak Velocity < 3 m/s > 4 m/s Mean Gradient < 20 mmhg > 35 mmhg Doppler Velocity Index >= 0.3 < 0.25 Effective Orifice area > 1.2 cm2 < 0.8 cm2 Contour of Jet Triangular Early Peaking ms Rounded Symmetrical contour Acceleration Time < 80 ms > 100 ms 31
32 An approach to prosthetic AV stenosis An approach to prosthetic AV stenosis EOA Index 32

33 An approach to prosthetic AV stenosis Indexed EOA = 0.78 PPM occurs when: ieoa < 0.85 Severe if ieoa < 0.65 An approach to prosthetic AV stenosis 33
 Prosthesis Patient Mismatch B) Normal Prosthetic Valve Function C) High")
 Patient Prosthesis Mismatch AVA velocity:4.")
34 What is your diagnosis? A) Prosthesis Patient Mismatch B) Normal Prosthetic Valve Function C) High Flow State D) Prosthetic Valve Stenosis E) Improper LVOT Velocity (Prosthetic valve stenosis) Patient Prosthesis Mismatch AVA velocity:4.6 DVI: 1.14/4.6 = 0.25, AVA= 0.4 cm 2 Acceleration Time: 60 msec B 34


35 Doppler Parameters of Prosthetic Aortic Valve Function Normal Suggests Stenosis Peak Velocity < 3 m/s > 4 m/s Mean Gradient < 20 mmhg > 35 mmhg Doppler Velocity Index >= 0.3 < 0.25 Effective Orifice area > 1.2 cm2 < 0.8 cm2 Contour of Jet Triangular Early Peaking TRI 60 ms Rounded Symmetrical contour Acceleration Time < 80 ms > 100 ms Patient Prosthesis Mismatch 35
36 Patient Prosthesis Mismatch P = Q 2 /(K x EOA 2 ) Q = Flow, K = Constant For gradients to remain low, EOA has to accommodate and be proportionate to flow At rest, Q is determined by BSA, bigger people have bigger flow In patients with large BSA and increased flow, a too small of a valve with a small EOA will produce a high gradient: Small valves + Big people = High gradients Patient Prosthesis Mismatch Moe common in SAVR versus TAVR PARTNER 28% vs 20% In smaller annulus even more pornounced 36% Vs 19% 36



37 ECHOCARDIOGRAM CASE PRESENTATION 69 Y/O F Hx AVR (BIOPROSTHETIC BIOCOR 23 MM 2006) SOB, FATIGUE, NEVER FELT MUCH BETTER AFTER SAVR BSA 2.2, 6 2 Doppler Parameters of Prosthetic Aortic Valve Function Normal Suggests Stenosis Peak Velocity < 3 m/s > 4 m/s Mean Gradient < 20 mmhg > 35 mmhg Doppler Velocity Index >= 0.3 < 0.25 Effective Orifice area > 1.2 cm2 < 0.8 cm2 Contour of Jet Triangular Early Peaking Rounded Symmetrical contour Acceleration Time < 80 ms > 100 ms 1 TRI 74 ms 37

38 An approach to prosthetic AV stenosis Indexed EOA = 0.5 PPM occurs when: ieoa < 0.85 Severe if ieoa < 0.65 TEE 38


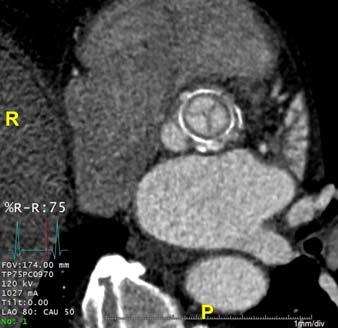


39 CTA SYSTOLE CTA DIASTOLE 39

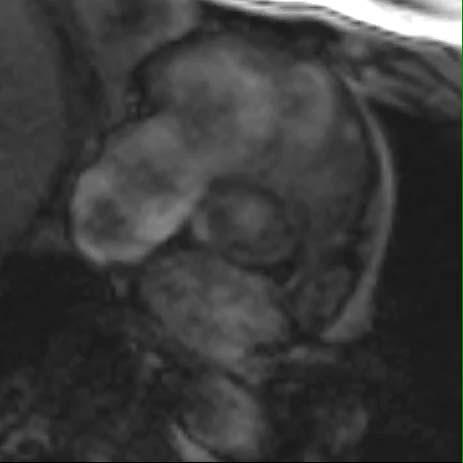

40 MRI SURGERY PRE 40

41 SURGERY POST ECHO POST 41
42 Echocardiographic Evaluation of Prosthetic Valve Regurgitation Types of Regurgitation Regurgitation may be Physiological Pathological Physiological regurgitation Closing volume (blood displacement by occluder motion) At the hinges of occluder 42
43 Pathological Central Types of Regurgitation Mostly with bioprosthetic Technical or infection related Paravalvular Either type, usually the site with mechanical Mild is common after surgery (5 20%) and likely insignificant in the absence of infection Usually after calcium debridement, redo, older patients Hemolytic anemia TAVR Central Aortic Regurgitation 43
44 Central Aortic Regurgitation Central Aortic Regurgitation 44
45 Paravalvular Aortic Regurgitation Paravalvular Aortic Regurgitation 45
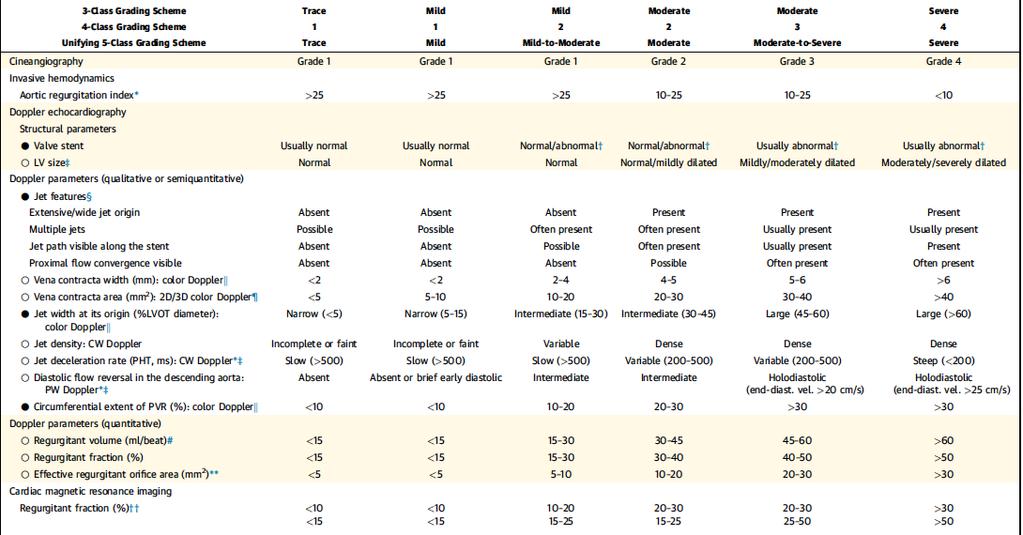
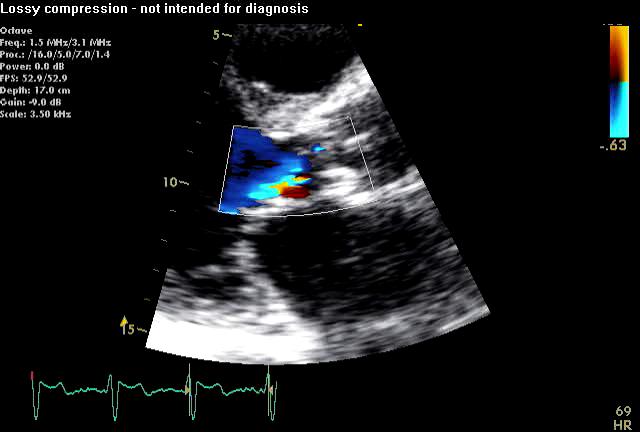
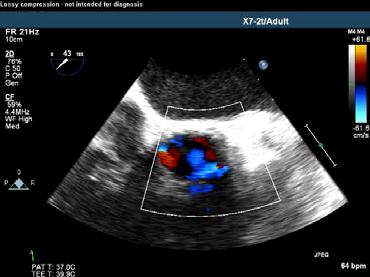
46 Assessment of Prosthetic Aortic Valve Regurgitation: TTE Challenging due to Shadowing Eccentric Jet Difficult to quantify paravalvular leak Width of vena contracta may be difficult to measure Off axis views may be required Assessment of Prosthetic Aortic Valve Regurgitation Jet diameter/lvo diameter <25% in PS views Pressure Half Time < 200 ms Holodiastolic flow reversal in Descending aorta Neck in the short axis view < 10% of sewing ring is mild 10 20% moderate > 20% severe > 40% rocking motion 46

47 Assessment of Prosthetic Aortic Valve Regurgitation PROSTHETIC VALVE REGURGITATION 47



48 Assessment of Prosthetic Aortic Valve Regurgitation 75 ml 75 ml NORMAL Assessment of Prosthetic Aortic Valve Regurgitation 120 ml 70 ml AORTIC REGURGITATION R Volume = = 50 ml R Fraction = 50/120 = 42% 48

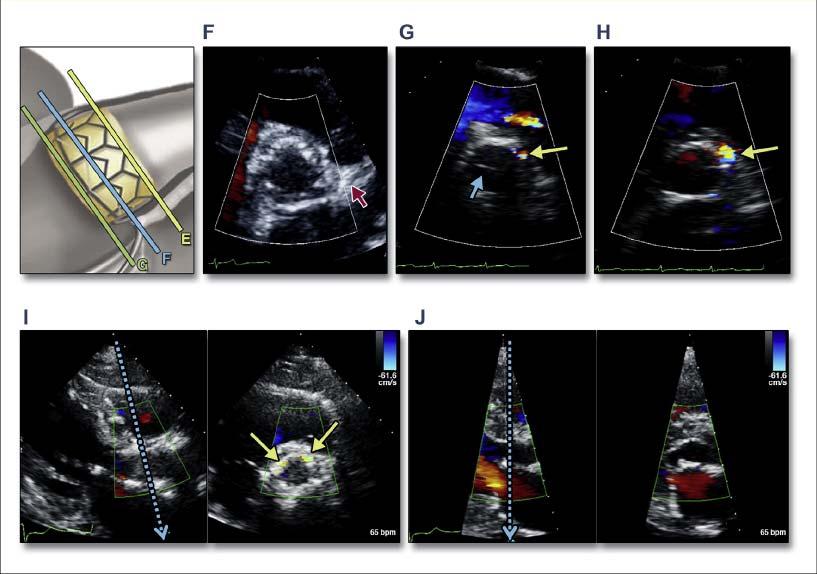
49 Assessment of Prosthetic Aortic Valve Regurgitation: TEE Identifies: Location, Mechanism, AR width to LVOT width, Posterior jets may be identified LVOT obscured by accompanied MV prosthesis 3D: value? Especially for transcatheter repair, challenging for AV versus MV TAVR ASSESSMENT 49



50 Trans Catheter Valves CORE VALVE SELF EXPANDING Sapien Balloon Expandable Trans Catheter Valves 50


51 Trans Catheter Valves Technical Points PW at inferior border of stent LVOT diameter Use baseline numbers prior to TAVR BE TAVR: inferior border of stent SE TAVR: inferior border of stent/ 5 mm below leaflets 51
52 Echocardiographic Outcomes Mean Gradient and Aortic Valve Area Mean Gradient p< Aortic Valve Area p = NS mmhg cm² 20 p< p = NS Baseline Days Year Mean ±SD All-Cause Mortality Has Decreased Overall 20% ALL-CAUSE MORTALITY at 30 DAYS PARTNER I Trial and PARTNER II Trial 15% 10% 5% 6.3% 5.2% 3.7% 4.4% 3.5% 1.6% 0% PARTNER I B (TF) PARTNER I A (All) PARTNER I A (TF) PARTNER II B (TF) PARTNER II B (TF) PARTNER II HR (TF) SAPIEN Valve SAPIEN XT Valve SAPIEN 3 Valve

53 All Stroke at 30 Days % % 4.9% 4.0% % 1 0 PARTNER IA PARTNER IB CoreValve High Risk CoreValve Extreme Risk Sapien S3 Intermediate Risk PARAVALVULAR REGURGITATION 53
 Valve Design Mortality Impact of")
54 Determinants of PVR after TAVR Patient Characteristics: Tissue characteristics such as calcium burden and location, annular dimensions, etc. Assessment Modality: Echo, angiography, hemodynamics, and cardiac MR Procedural Factors: Sizing Algorithm; deployment technique (positioning and postdilatation) Valve Design Mortality Impact of Aortic Regurgitation on Mortality: PARTNER Trial 70% 60% 50% 40% 30% 20% None Trace Mild Moderate Severe 60.8% 44.6% 35.3% 10% 0% Months post Procedure 12 15% of patients with moderate AR 5/1/

 P1A (Overall) P2B (TF) P2B XT")

55 Moderate/Severe PVL at 30 Days Edwards SAPIEN Valves 50% PARTNER I and II Trials 40% 30% 24.2% 20% 16.9% 12.0% 11.5% 10% 2.9% 4.2% 0% P1B (TF) P1A (Overall) P2B (TF) P2B XT (TF) S3HR (Overall) S3i (Overall) SAPIEN SAPIEN XT SAPIEN 3 INVASIVE ASSESSMENT 55
56 ECHOCARDIOGRAPHIC ASSESSMENT ECHOCARDIOGRAPHIC ASSESSMENT 56
57 ECHOCARDIOGRAPHIC ASSESSMENT TAVR PVR ASSESSMENT 57

58 ECHOCARDIOGRAPHIC ASSESSMENT OTHER TAVR ISSUES Infective endocarditis 1.1% 62% 60 days 1 year RF: DM, CKD, infections, Performance in cathlab ABX, Surgical survival (38 75% Thrombosis 0.8% RF Cancer, incomplete expansion, oveerhanging leaflets Anticoagulation Structural failure 13 cases 24 months (up to 5 years Valve in valve 58
59 Echocardiographic Evaluation of Prosthetic Valve Endocarditis Endocarditis Incidence < 1% and has declined with perioperative antibiotics Form in valve ring and extend to and spread to stent, occluder, or leaflet Irregular and independently mobile Can not adequately differentiate between vegetations, thrombus, pledgets, sutures, etc 59


60 Endocarditis TEE has better sensitivity and specificity for Vegetations Abscess in the posterior but not anterior location Combined TEE and TTE have a NPV of 95% If clinical suspicion high and studies negative, repeat studies in 7 10 days Parasternal Long 60


61 Color TEE Short 61

62 TEE Long Doppler 62


63 Pathology Echocardiographic Evaluation of Prosthetic Valve Thrombosis/Pannus 63




64 Thrombus versus Pannus Thrombus Larger Soft density similar to myocardium More likely to encounter abnormal valve motion Short duration of symptom Poor anticoagulation Size < 0.85 cm2 less likely to embolize More with mechanical Pannus Small Dense, 30% may not be visualized Longer duration More common in aortic Pannus TEE 64
 thrombus Recent onset (<14d) NYHA I II Small thrombus (<0.")
65 11.6 Prosthetic Valve Thrombosis Suspect Prosthetic Valve Thrombosis Class I Class IIa TTE to evaluate hemodynamic severity CT or fluoroscopy to evaluate valve motion Left Sided Prosthetic Valve Thrombosis Right Sided Prosthetic Valve Thrombosis TEE for thrombosis size NYHA III IV symptoms Mobile or large (>0.8cm 2 ) thrombus Recent onset (<14d) NYHA I II Small thrombus (<0.8cm 2 ) Emergency Surgery Emergency Surgery Fibrinolytic Rx if persistent valve thrombosis after IV heparin therapy 65
66 Pre Questions (1) Regarding Aortic Prosthetic Valves A. A routine echocardiogram is required very two years after AVR B. An elevated gradient with a decreased EOA is always suggestive of valvular stenosis C. Transthoracic echocardiogram alone is always sufficient to diagnose valvular stenosis D. It is more challenging to quantify para valvular versus valvular aortic regurgitation. Answer (1) D. It is more challenging to quantify para valvular versus valvular aortic regurgitation. 66
67 Pre Questions (2) Patients with Prosthesis Patient Mismatch A. Have abnormal prosthetic valve function B. Progressively worsen with time C. Have a small valve compared to the demands of their body and cardiac output D. Have a benign condition Answer (2) C. Have a small valve compared to the demands of their body and cardiac output 67
68 Conclusions Elevated gradients across prosthetic aortic valves may be due to other factors besides stenosis Regurgitation may be physiological or pathological and may be valvular or paravalvular Endocarditis, pannus, and thrombosis may be difficult to distinguish based solely on echocardiographic findings TAVR has its unique problems 68
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
A Practical Approach to Prosthetic Valves
 A Practical Approach to Prosthetic Valves Bonita Anderson DMU (Cardiac), MApplSc (Med Ultrasound), ACS, AMS, FASE https://doi.org/10.1161/circulationaha.108.778886 Disclosures None 1 Know the Product Know
A Practical Approach to Prosthetic Valves Bonita Anderson DMU (Cardiac), MApplSc (Med Ultrasound), ACS, AMS, FASE https://doi.org/10.1161/circulationaha.108.778886 Disclosures None 1 Know the Product Know
Echocardiographic Evaluation of Mitral Valve Prostheses
 Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Cases of Abnormal Prosthetic Valves
 Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Comments restricted to Sapien and Corevalve 9/12/2016. Disclosures: Core Lab contracts with Edwards Lifesciences, Middlepeak, Medtronic
 Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Patient/prosthesis mismatch: how to evaluate and when to act?
 Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Echo Assessment Pre-TAVI
 Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
PARAVALVULAR LEAK POST TAVR. Elements of Follow-up Post TAVR
 PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis
 Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies
 ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, :00 11:25 PM 25 min
 2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
TAVR IN INTERMEDIATE-RISK PATIENTS
 TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC
 TAVR: When Things go Wrong Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC Disclosures Academic Echo Core Lab Abbott / St Jude Medical Edwards Medtronic
TAVR: When Things go Wrong Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC Disclosures Academic Echo Core Lab Abbott / St Jude Medical Edwards Medtronic
CARDIOLOGY GRAND ROUNDS
 CARDIOLOGY GRAND ROUNDS Presentation: Speakers: Percutaneous Repair of Paravalvular Prosthetic Regurgitation Paul Sorajja, MD Director of the Center for Valve and Structural Heart Disease Minneapolis Heart
CARDIOLOGY GRAND ROUNDS Presentation: Speakers: Percutaneous Repair of Paravalvular Prosthetic Regurgitation Paul Sorajja, MD Director of the Center for Valve and Structural Heart Disease Minneapolis Heart
PVL Assessment. Is paravalvular regurgitation after TAVR still an important consideration in 2018?
 Joint Meeting 1 Aortic and Mitral Club Chairpersons: S.Adamopoulos, M. Vavuranakis, L. Michalis, P. Nihoyannopoulos PVL Assessment. Is paravalvular regurgitation after TAVR still an important consideration
Joint Meeting 1 Aortic and Mitral Club Chairpersons: S.Adamopoulos, M. Vavuranakis, L. Michalis, P. Nihoyannopoulos PVL Assessment. Is paravalvular regurgitation after TAVR still an important consideration
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
An Update on the Edwards TAVR Results. Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St.
 An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
2/15/2018 DISCLOSURES OBJECTIVES. Consultant for BioSense Webster, a J&J Co. Aortic stenosis background. Short history of TAVR
 TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
Severity of AS Degree of AV calcification (? Bicuspid AV), annulus size, & aortic root
, annulus size, & aortic root") The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Relevant Financial Relationship(s) Off Label Usage. None. None
 Off Label Usage. None. None") Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018
Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018
ASCeXAM / ReASCE. Practice Board Exam Questions. Monday Afternoon
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Afternoon Aortic Valve Prostheses Aortic Regurgitation Stress Echocardiography Ischemic Heart Disease and Myocardial Infarction 3D Echocardiography
ASCeXAM / ReASCE Practice Board Exam Questions Monday Afternoon Aortic Valve Prostheses Aortic Regurgitation Stress Echocardiography Ischemic Heart Disease and Myocardial Infarction 3D Echocardiography
Procedural Guidance of TAVR: How to Assure it Goes Right and What to Do If It Doesn t
 Procedural Guidance of TAVR: How to Assure it Goes Right and What to Do If It Doesn t James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute Cleveland Clinic
Procedural Guidance of TAVR: How to Assure it Goes Right and What to Do If It Doesn t James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute Cleveland Clinic
Percutaneous Therapy for Calcific Mitral Valve Disease
 31 st Annual State of the Art Echocardiography San Diego, CA February 18, 2018 5:00 5:15 PM 15 min Percutaneous Therapy for Calcific Mitral Valve Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive
31 st Annual State of the Art Echocardiography San Diego, CA February 18, 2018 5:00 5:15 PM 15 min Percutaneous Therapy for Calcific Mitral Valve Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification. Rheumatic Mitral Stenosis 76yo male
 MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Διαδερμική θεραπεία των παραβαλβιδικών διαφυγών Σ.Ράμμος
 ΔΜΙΝΑΡΙΟ ΔΠΙΣΗΜΟΝΙΚΩΝ ΔΝΩΔΩΝ ΔΛΛΗΝΙΚΟΤ ΚΟΛΛΔΓΙΟΤ ΚΑΡ ΙΟΛΟΓΙΑ 2-4.10.2015 Δπιζηημονική Ένωζη Δπεμβαηικής Καρδιολογίας Βαλβιδοπάθειες, Γιαδερμικές παρεμβάζεις Διαδερμική θεραπεία των παραβαλβιδικών διαφυγών
ΔΜΙΝΑΡΙΟ ΔΠΙΣΗΜΟΝΙΚΩΝ ΔΝΩΔΩΝ ΔΛΛΗΝΙΚΟΤ ΚΟΛΛΔΓΙΟΤ ΚΑΡ ΙΟΛΟΓΙΑ 2-4.10.2015 Δπιζηημονική Ένωζη Δπεμβαηικής Καρδιολογίας Βαλβιδοπάθειες, Γιαδερμικές παρεμβάζεις Διαδερμική θεραπεία των παραβαλβιδικών διαφυγών
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
TAVR SPRING 2017 The evolution of TAVR
 TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
TAVR TTE INTERROGATION BY ALAN MATTHEWS
 TAVR TTE INTERROGATION BY ALAN MATTHEWS KEYS TO ACCURATE ASSESSMENT EDWARDS SAPIEN VALVE 3 PHASES OF TAVR TTE Evaluation (Qualifying) Placement (Intraoperative) Follow-up (Post-Op) GOALS High quality TTE
TAVR TTE INTERROGATION BY ALAN MATTHEWS KEYS TO ACCURATE ASSESSMENT EDWARDS SAPIEN VALVE 3 PHASES OF TAVR TTE Evaluation (Qualifying) Placement (Intraoperative) Follow-up (Post-Op) GOALS High quality TTE
How to Avoid Prosthesis-Patient Mismatch
 How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON
 THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON INTRODUCTION History of heart valve intervention Current indications
THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON INTRODUCTION History of heart valve intervention Current indications
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
PROSTHETIC. V PROSTHETIC.V
 PROSTHETIC. V PROSTHETIC.V VALVE TYPE The valve types now implanted include: 1-bileaflet and tilting disc mechanical valves, 2-stented porcine and pericardial xenografts, 3-stentless porcine xenografts,
PROSTHETIC. V PROSTHETIC.V VALVE TYPE The valve types now implanted include: 1-bileaflet and tilting disc mechanical valves, 2-stented porcine and pericardial xenografts, 3-stentless porcine xenografts,
Case Presentations TAVR: The Good Bad and The Ugly
 Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy
 TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative
 Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Paravalvular Regurgitation is a Risk Factor Following TAVI
 Paravalvular Regurgitation is a Risk Factor Following TAVI Philippe Pibarot, DVM, PhD, FACC, FESC, FASE Canada Research Chair in Valvular Heart Disease INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE
Paravalvular Regurgitation is a Risk Factor Following TAVI Philippe Pibarot, DVM, PhD, FACC, FESC, FASE Canada Research Chair in Valvular Heart Disease INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Endocarditis and Its Complications: The Role of Echocardiography
 Endocarditis and Its Complications: The Role of Echocardiography Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz School of Medicine
Endocarditis and Its Complications: The Role of Echocardiography Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz School of Medicine
DISCLOSURE. Relevant Financial Relationship(s) Off Label Usage. None. None
 Off Label Usage. None. None") Echo for TAVR Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo
Echo for TAVR Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient
 Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients
 Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Cedars Sinai Heart Institute, Los Angeles, CA Potential
Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Cedars Sinai Heart Institute, Los Angeles, CA Potential
Questions of the webinar "Imaging in TAVI procedures" Answered by Andreas Hagendorff, Victoria Delgado and Bernard Cosyns
 Questions of the webinar "Imaging in TAVI procedures" Answered by Andreas Hagendorff, Victoria Delgado and Bernard Cosyns 1. The incidence in AR I think that this question focuses on the incidence in AR
Questions of the webinar "Imaging in TAVI procedures" Answered by Andreas Hagendorff, Victoria Delgado and Bernard Cosyns 1. The incidence in AR I think that this question focuses on the incidence in AR
Experience with 500 Stentless Aortic Valve Replacements
 Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Aortic Regurgitation & Aorta Evaluation
 VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
*Core lab for numerous trials, for which I receive no direct compensation from sponsors.
 Rebecca T. Hahn, MD, FACC, FASE Director of Interventional Echo Professor of Medicine Columbia University Company Abbott Vascular Gore&Assoc NaviGATE Medtronic Boston Scientific GE Medical Philips Healthcare
Rebecca T. Hahn, MD, FACC, FASE Director of Interventional Echo Professor of Medicine Columbia University Company Abbott Vascular Gore&Assoc NaviGATE Medtronic Boston Scientific GE Medical Philips Healthcare
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
Transcatheter Aortic Valve Implantation. SSVQ November 23, 2012 Centre Mont-Royal 15:40
 Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
ΔΙΑΔΕΡΜΙΚΗ ΑΝΣΙΚΑΣΑΣΑΗ ΑΟΡΣΙΚΗ ΒΑΛΒΙΔΑ αντιμετώπιση επιπλοκών ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC IICE 2012
 ΔΙΑΔΕΡΜΙΚΗ ΑΝΣΙΚΑΣΑΣΑΗ ΑΟΡΣΙΚΗ ΒΑΛΒΙΔΑ αντιμετώπιση επιπλοκών ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC IICE 2012 TAVR Technologies Current Generation Devices ~ 50,000 patients treated thru 2011 in > 500 interventional centers
ΔΙΑΔΕΡΜΙΚΗ ΑΝΣΙΚΑΣΑΣΑΗ ΑΟΡΣΙΚΗ ΒΑΛΒΙΔΑ αντιμετώπιση επιπλοκών ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC IICE 2012 TAVR Technologies Current Generation Devices ~ 50,000 patients treated thru 2011 in > 500 interventional centers
Transcatheter heart valve thrombosis
 Transcatheter heart valve thrombosis Jeroen J Bax Dept Cardiology Leiden, The Netherlands New York, 2017 The department of Cardiology of the Leiden University Medical center received research grants from
Transcatheter heart valve thrombosis Jeroen J Bax Dept Cardiology Leiden, The Netherlands New York, 2017 The department of Cardiology of the Leiden University Medical center received research grants from
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
Mixed aortic valve disease
 Mixed aortic valve disease IOANNIS NTALAS MD, PhD Cardiologist, Clinical Fellow in Cardiovascular Imaging & Non-Invasive Cardiology, St Thomas Hospital School of Biomedical Engineering & Imaging Sciences
Mixed aortic valve disease IOANNIS NTALAS MD, PhD Cardiologist, Clinical Fellow in Cardiovascular Imaging & Non-Invasive Cardiology, St Thomas Hospital School of Biomedical Engineering & Imaging Sciences
April 16, 09:00-09:15 중앙대학교 윤신원
 April 16, 09:00-09:15 중앙대학교 윤신원 When to perform Echocardiography in IE? Vegetations?(pathologic Whatever the level hallmark) of suspicion Intracardiac abscess? Confirm or R/O at the Earliest opportunity.
April 16, 09:00-09:15 중앙대학교 윤신원 When to perform Echocardiography in IE? Vegetations?(pathologic Whatever the level hallmark) of suspicion Intracardiac abscess? Confirm or R/O at the Earliest opportunity.
Optimal Imaging Technique Prior to TAVI -Echocardiography-
 2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Imaging in TAVI. Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013
 Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Structural Heart Disease Transcatheter Aortic Valve Replacement (TAVR)
") Structural Heart Disease Transcatheter Aortic Valve Replacement (TAVR) Kathleen Harper DO FACC FACP 87 Chief, Cardiology Section VA Maine Healthcare Kathleen.Harper@va.gov Prevalence of Aortic Stenosis
Structural Heart Disease Transcatheter Aortic Valve Replacement (TAVR) Kathleen Harper DO FACC FACP 87 Chief, Cardiology Section VA Maine Healthcare Kathleen.Harper@va.gov Prevalence of Aortic Stenosis
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
 Hans R. Figulla, M.D., PhD ; Ali Hamadanchi, M.D. Medicine, Pneumology Universitity Hospital, Jena, Germany Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
Hans R. Figulla, M.D., PhD ; Ali Hamadanchi, M.D. Medicine, Pneumology Universitity Hospital, Jena, Germany Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
SAPIEN 3 Sizing Considerations:
 SAPIEN 3 Sizing Considerations: Oversizing, Undersizing, or Volume reduction? John Webb MD St Paul s Hospital University of British Columbia Vancouver Disclosure Statement of Financial Interest Within
SAPIEN 3 Sizing Considerations: Oversizing, Undersizing, or Volume reduction? John Webb MD St Paul s Hospital University of British Columbia Vancouver Disclosure Statement of Financial Interest Within
Outline. EuroScore II. Society of Thoracic Surgeons Score. EuroScore II
 SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
DISCLOSURE. Mitral ViV: why? Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? UW Medicine NONE.
 Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? G. Burkhard Mackensen, MD, PhD, FASE Professor & Chief, Division of Cardiothoracic Anesthesia, Department of Anesthesiology
Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? G. Burkhard Mackensen, MD, PhD, FASE Professor & Chief, Division of Cardiothoracic Anesthesia, Department of Anesthesiology
Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison
 Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison Mauri, V. et al.: Circ Cardiovasc Interv. 2017;10:e005013 All trademarks are the property
Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison Mauri, V. et al.: Circ Cardiovasc Interv. 2017;10:e005013 All trademarks are the property
Edwards Sapien. Medtronic CoreValve. Inoperable FDA approved High risk: in trials. FDA approved
 Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
Update on Percutaneous Therapies for Structural Heart Disease. William Thomas MD Director of Structural Heart Program Tucson Medical Center
 Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
PPM: How to fit a big valve in a small heart
 PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
CoreValve in a Degenerative Surgical Valve
 CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes
 SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes Howard C. Herrmann, MD on behalf of The PARTNER II Trial
SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes Howard C. Herrmann, MD on behalf of The PARTNER II Trial
Emergency TAVI: Does It Exist? Is the Risk Higher?
 Emergency TAVI: Does It Exist? Is the Risk Higher? Gerald Yong MBBS (Hons) FRACP FSCAI Interventional Cardiologist Royal Perth Hospital Western Australia APCASH 12 October 2014 Disclosure Statement of
Emergency TAVI: Does It Exist? Is the Risk Higher? Gerald Yong MBBS (Hons) FRACP FSCAI Interventional Cardiologist Royal Perth Hospital Western Australia APCASH 12 October 2014 Disclosure Statement of
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial