THE HEART AND HYPERTENSION. Philippe Gosse Hypertension Unit University Hospital Bordeaux
|
|
|
- Brook Ray
- 5 years ago
- Views:
Transcription
1 THE HEART AND HYPERTENSION Philippe Gosse Hypertension Unit University Hospital Bordeaux

2
3 INCREASED LVM Cardiomyocytes hypertrophy is a response to pressure overload This response is influenced by many factors and genes It has long been viewed as an adaptative process to normalize wall stress and restore heart muscle economy. But this view is now seriously challenged Increased LVM is not muscle only
4 INCREASED LVM HYPERTROPHY Requires mechanical stress Modulated by non mechanical factors Hormones Salt Genes May show regression within weeks FIBROSIS (>6%, up to 30%) Independent of mechanical stress Influence of AII Aldosterone? Regression may require months
5 LVH DIAGNOSIS ECG Voltage Sokolow: Sv1+Rv5 or Rv6 > 35(8) mm Cornell: RavL + Sv3 + 8 mm(f)> 28 Cornell Voltage*QRS duration >2440 Repolarization abnormalities ECHO M mode 2D, 3D Magnetic Resonance Imaging BNP?
 Posterior Wall")
6 2D guided M Mode recording of LV parasternal view Septal Thickness (ST) AVOID: Oblique recording Recording of «non wall structures» End Diastolic Diameter (EDD) Posterior Wall Thickness (PWT)
7 HOW TO READ M MODE RECORDINGS? ASE PENN ST ST EDD EDD PWT PWT
8 LIMITS LINKED TO GEOMETRY HYPOTHESIS LVM=1.04((EDD+ST+PWT) 3 -EDD 3 )-13.6 WALL MOTION ABNORMALITIES ASYMETRIC HYPERTROPHY LV DILATATION do not calculate if EDD>60mm
9 REPRODUCIBILITY AUTHOR POPULATION Mean DIFF. SDD CV GOSSE Misc 30g 40g 15.6% DEVEREUX Normal 26g 29g GOTTDIENER HT 27g 27g 8.3% GOSSE HT 27g 32g 14.6%
10 LVH CUT OFF INDEXATION FOR LVM BSA Height Height 2.7 Gender influence Influence of physical training? Cut off, usually based on 95 th percentile in normal subjects M: g/m 2, F:110g/m 2 M: 50 g/m 2.7, F:47 g/m 2.7
11 CUTOFF For prediction of CVE CVE cut off Sens Spé AUC BX cohort M+F (637) 95 52g/m % 51% 0.69 M (395) 70 55g/m % 53% 0.66 F (242) 25 47g/m % 51% 0.72 ARIC Black (57%HT) Nunez, Hypertension 2005 M (570)+F (1046) g/m % 62%
12 LVH PREVALENCE Bordeaux cohort of never treated hypertensives (n=500) ECG SOKOLOW > 35 mm : 6 %, > 38mm : 3 % CORNELL product > 2440 : 10 % ECG LIFE : 12 % M mode ECHO g/m 2 : M 134, F 110 : 36 % g/m 2.7 : M 53, F 47 : 51 %
13 LV REMODELING NORMAL h=10 mm r=25 mm RWT=0.4 LVM=213 g h CONCENTRIC h=14 mm r=22.5 mm RWT=0.62 LVM=296 g ECCENTRIC h=10 mm r=30 mm RWT=0.33 LVM=294 g r
14 REMODELAGE VG ET HTA HVG CONCENTRIQUE: MVG, H/R: 8% HVG EXCENTRIQUE: MVG, H/R=: 27% REMODELAGE CONCENTRIQUE: H/R, MVG Nale: 13% VG NORMAL: 52% GANAU, JACC 1992, 19:
15 THE CASE AGAINST THE VALIDITY OF WALL-STRESS HYPOTHESIS LVH IS A STRONG AND INDEPENDENT RISK FACTOR WITH A CONTINUOUS RELATIONSHIP BETWEEN LVM AND RISK SYSTOLIC FUNCTION IS OFTEN IMPAIRED DESPITE NORMAL REST EJECTION FRACTION MIDWALL FRACTIONNAL SHORTENING TISSUE DOPPLER IMAGING LEFT VENTRICULAR FILLING IS IMPAIRED RELAXATION COMPLIANCE CORONARY PERFUSION IS OFTEN IMPAIRED IN HYPERTENSION EXPERIMENTAL DATA SHOW THAT CARDIAC HYPERTROPHY IS NOT AN ADAPTATIVE RESPONSE
16 4 year age-adjusted incidence (/100 pts) of cardiovascular disease according to LVM/h (Framingham) 20,00 15,00 men Women 12,20 16,10 10,00 5,00 4,70 4,10 7,30 5,30 7,50 6,10 0,00 < >140 LVM (g/m) Levy, NEJM 1990, 322:
17 PIUMA STUDY Schillaci, Hypertension 2000,35: ,5 4 3,5 3 2,5 2 1,5 1 0,5 0 0,85 Q1 50±10 Events 1,66 Q2 92± HT, mean FU:4±2 years, 181 CV events 4,34 2,24 Q3 104±9 MVG/SC 2,86 Q4 119±11 Q5 150±27

18 Age, sex and BP adjusted event free survivals curves for LVM/h 2.7 quintiles in Bordeaux cohort n=520 Mean follow-up= 102±42 months 56 CV events
19 LVH: MARKER OF RISK INFLUENCED BY SEVERAL RISK FACTORS: Age, gender, BP(central), Blood viscosity, overweight, alcool, salt, cholesterol?... INTEGRATES THEIR VARIATIONS WITH TIME
20 LVM as a witness of BP over time BP LVM
21 Inappropriate LVH LVM ADVERSE EFFECTS ISCHIEMIA IMPAIRED FILLING ARRYTHMIAS ADVERSE EFFECTS IMPAIRED SYSTOLIC FUNCTION STROKE WORK
22 Prognostic impact of inappropriate LVM in hypertension: the MAVI study de Simone, Hypertension 2002, 40:470 CV event free survival curves at mean of covariates (age, sex, BMI, SBP...) according to LVM Predicted LVM= height SW gender SW=SBP*Stroke volume
23 HYPERTENSION = PATHOLOGIC LVH IMPAIRED CORONARY RESERVE WHY? vascular remodeling Impaired endothelial function Capillaries rarefaction Increase aortic stiffness and reduced perfusion pressure CONSEQUENCES Unbalanced offer and demand Ischemic heart disease Impaired relaxation and LV filling Impaired systolic function
24 HYPERTENSION = PATHOLOGIC LVH IMPORTANCE OF FIBROSIS Diez (circulation 2002: ) 34 HT with LVH, transvenous endomyocardial biopsies for assessment of Collagen Volume Fraction and pulsed doppler mitral flow Correlation between CVF and reduced deceleration time of early mitral filling wave
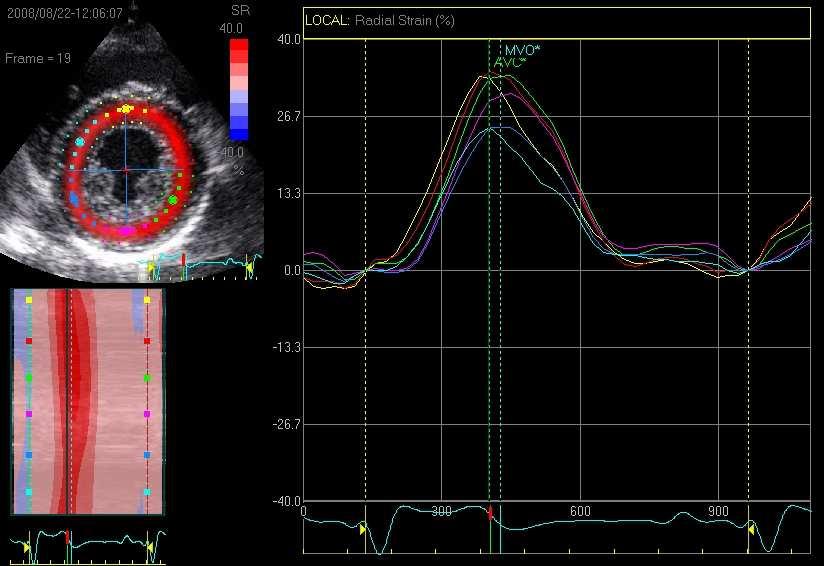
25 THE LEVER EFFECT OF MYOCARDIAL FIBERS ORGANISATION 15% fiber shortening along the long axis leads to only an 8% increase in myocyte diameter. Yet, 40% radial LV wall thickening and 60% ejection fraction are typically observed. Myocardial fibers are grouped into lamina (sheets) 3*4 cells thick interconnected by extracellular matrix Radial and longitudinal shear of these sheets play a role of lever to increase wall thickening

26 Cheng, Circulation 2008, 118:713-21
27 Fibrosis and systolic function? Even small changes in the initial sheet angle may have large effects on wall thickening pathological changes in macrostructure of the ventricular wall may influence sheet motion and, therefore, wall thickening and synchronicity
28

29 Genetic alterations that inhibit in vivo pressure overload hypertrophy prevent cardiac dysfunction despite increased wall stress. Esposito, Circulation 2002, 105:85-92 Genetically altered mice unable to develop LVH Transverse aortic constriction to increase afterload Despite high parietal stress these mice showed significantly less deterioration in cardiac function than the wild type banded mice developing LVH
30 ANTIHYPERTENSIVE TREATMENT REDUCES LVH MANY STUDIES BUT OFTEN WITH FEW PATIENTS, SHORT DURATION ALL DRUGS ARE EFFICIENT WITH THE EXCEPTION OF MINOXIDIL AND HYDRALAZINE POOR CORRELATIONS BETWEEN BP AND LVM REDUCTIONS: IS THERE A SPECIFIC DRUG ACTION??
31 IS THERE A SPECIFIC DRUG ACTION ON LVH?? COMPARATIVE STUDIES EXIST BUT FEW SHOW SUFFICIENT POWER META-ANALYSIS SHOW GREATER EFFICACY OF ARAII and ACE INHIBITORS VERSUS β BLOCKERS AND DIURETICS BUT Many studies of poor quality Diuretics often added to ACE inhibitors and ARAII Publication bias WE NEED WELL DESIGNED AND POWERFULL COMPARATIVE STUDIES
32 LVH Régression Meta-analysis Klingbeil : 80 studies / Dahlöf : 109 studies Régression Progression ARAII K Placebo D Calcium antagonist K D ACEI D K K D Klingbeil: Am J Med. 2003;115: Dahlöf B : Am J Hypertens. 1992;5: Diurétics K D β-blockers D K Variation (%)
33 OPTIMAL TRIAL DESIGN FEATURES Devereux, Dahlof: J Human Hypertens 1994, 8:735-9 ADEQUATE GENDER, AGE AND ETHNIC MIX DOUBLE BLIND, RANDOMISED COMPARATIVE TRIAL ADEQUATE SAMPLE SIZE ( /Gp with echo) ADEQUATE DURATION: >= 1 YEAR CENTRAL BLIND MEASUREMENTOF LVM BY TRAINED ECHOCARDIOGRAPHISTS
34 RECOMMANDATIONS FOR MULTICENTRIC LVH REGRESSION TRIALS Gosse J;Hypertens 2003, 21: CENTRALIZED CONTROL OF INCLUSION CRITERIA CENTRALIZED CONTROL OF QUALITY FOR ALL RECORDINGS FINAL CENTRALIZED READING BLIND TO TREATMENT AND temporal SEQUENCE ALL TRACINGS OF THE SAME Pt READ BY THE SAME READER ALL TRACINGS MIXED TOGETHER 2 INITIAL ECHO separated by a 2-4 weeks placebo run-in SDD as an OVERALL QUALITY INDICE QUANTIFICATION OF REGRESSION TO THE MEAN
35 MAIN ECHO STUDIES ON LVH REGRESSION n Drugs LVMI g/m2 LIFE 825 Los Vs Aten -22±22 (+Htz in 90%) -18±20* PICXEL 679 Per/ind Vs Ena -14±24-4±24* LIVE 411 Ind Vs Ena -8±30 (+prazosin in 20%) -2±28* CATCH 196 Cande Vs Ena -15±23 (+Htz in 47-54%) -13±23 PRESERVE 235 Ena Vs Nife -15±21 (+Htz in 34-59%) -17±18 REGAAL 219 Los Vs Aten -7±20 (+Htz in 86-78%) -4±21 BP mmhg -30/-16-29/-16-22/-10-18/-8* -25/-13-25/-12-27/-16-26/-16-22/12-21/13-24/-11-24/-14 Duration (weeks)
36 Study Month 8 Stroke Atenolol Losartan LIFE Change from Baseline in LVH Regression mmhg Systolic Mean Arterial Diastolic Study Month Mean change from baseline (%) Cornell Product 10.2 % 4.4 % p< Sokolow-Lyon 15.3 % 9.0 % p< Losartan Atenolol

37 LIFE: ECHO RESULTS n=878
 LIFE STUDY (Devereux, JAMA 2004,292:2350-6) LVM seems to be a good surrogate end point")
38 LVH REGRESSION IMPROVES OUTCOME (Verdecchia AJH, 2003:16: ) Meta analysis of small cohorts (Verdecchia AJH, 2003:16: ) LIFE STUDY (Devereux, JAMA 2004,292:2350-6) LVM seems to be a good surrogate end point
39 LVM assessment in hypertensive patient. When? LVM seems to be a good surrogate end point But ECG is not sensitive enough echo assessment of LVM shows insufficient reproducibility MRI cannot be proposed for routine evaluation No study demonstrates the cost effectiveness of systematic LVM assessment
40 ECG NORMAL Dont eliminate LVH LVH LOW RISK HIGH RISK ECHO USELESS IF ASYMPTOMATIC Normal REPOLARISATION High RISK ECHO To assess LV function?? Abnormal REPOLARISATION VERY HIGH RISK ECHO? Better assessment of risk but cost/effectiveness unknown Look for ischemic heart disease ECHO
Evaluation of Left Ventricular Function and Hypertrophy Gerard P. Aurigemma MD
 Evaluation of Left Ventricular Function and Hypertrophy Gerard P. Aurigemma MD Board Review Course 2017 43 year old health assistant Severe resistant HTN LT BSA 2 Height 64 1 Here is the M mode echocardiogram
Evaluation of Left Ventricular Function and Hypertrophy Gerard P. Aurigemma MD Board Review Course 2017 43 year old health assistant Severe resistant HTN LT BSA 2 Height 64 1 Here is the M mode echocardiogram
HYPERTENSION AND HEART FAILURE
 HYPERTENSION AND HEART FAILURE Kenya Cardiac Society Symposium Feb 2017 Dr Jeilan Mohamed No conflict of interests . Geoffrey, 45 yr old hypertensive office worker male from Nairobi, has just watched his
HYPERTENSION AND HEART FAILURE Kenya Cardiac Society Symposium Feb 2017 Dr Jeilan Mohamed No conflict of interests . Geoffrey, 45 yr old hypertensive office worker male from Nairobi, has just watched his
Danno d organo bersaglio e rischio CV. Persiste un ruolo prognostico oltre la patologia d organo?
 Danno d organo bersaglio e rischio CV. Persiste un ruolo prognostico oltre la patologia d organo? Prof. Massimo Salvetti Clinica Medica University of Brescia Percieved risk Actual risk Sehestedt et al,
Danno d organo bersaglio e rischio CV. Persiste un ruolo prognostico oltre la patologia d organo? Prof. Massimo Salvetti Clinica Medica University of Brescia Percieved risk Actual risk Sehestedt et al,
Allopurinol reduces left ventricular hypertrophy and endothelial dysfunction in patients with chronic kidney disease
 Allopurinol reduces left ventricular hypertrophy and endothelial dysfunction in patients with chronic kidney disease Michelle P Kao, Donald S Ang, Steve Gandy, Chim C Lang, Allan D Struthers Division of
Allopurinol reduces left ventricular hypertrophy and endothelial dysfunction in patients with chronic kidney disease Michelle P Kao, Donald S Ang, Steve Gandy, Chim C Lang, Allan D Struthers Division of
Aortic valve Stenosis: Insights in the evaluation of LV function. Erwan DONAL Cardiologie CHU Rennes
 Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
PRELIMINARY STUDIES OF LEFT VENTRICULAR WALL THICKNESS AND MASS OF NORMOTENSIVE AND HYPERTENSIVE SUBJECTS USING M-MODE ECHOCARDIOGRAPHY
 Malaysian Journal of Medical Sciences, Vol. 9, No. 1, January 22 (28-33) ORIGINAL ARTICLE PRELIMINARY STUDIES OF LEFT VENTRICULAR WALL THICKNESS AND MASS OF NORMOTENSIVE AND HYPERTENSIVE SUBJECTS USING
Malaysian Journal of Medical Sciences, Vol. 9, No. 1, January 22 (28-33) ORIGINAL ARTICLE PRELIMINARY STUDIES OF LEFT VENTRICULAR WALL THICKNESS AND MASS OF NORMOTENSIVE AND HYPERTENSIVE SUBJECTS USING
Echocardiographic definition of left ventricular hypertrophy in the hypertensive: which method of indexation of left ventricular mass?
 Journal of Human Hypertension (1999) 13, 505 509 1999 Stockton Press. All rights reserved 0950-9240/99 $12.00 http://www.stockton-press.co.uk/jhh ORIGINAL ARTICLE Echocardiographic definition of left ventricular
Journal of Human Hypertension (1999) 13, 505 509 1999 Stockton Press. All rights reserved 0950-9240/99 $12.00 http://www.stockton-press.co.uk/jhh ORIGINAL ARTICLE Echocardiographic definition of left ventricular
Review of Cardiac Imaging Modalities in the Renal Patient. George Youssef
 Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Cardiovascular Diseases in CKD
 1 Cardiovascular Diseases in CKD Hung-Chun Chen, MD, PhD. Kaohsiung Medical University Taiwan Society of Nephrology 1 2 High Prevalence of CVD in CKD & ESRD Foley RN et al, AJKD 1998; 32(suppl 3):S112-9
1 Cardiovascular Diseases in CKD Hung-Chun Chen, MD, PhD. Kaohsiung Medical University Taiwan Society of Nephrology 1 2 High Prevalence of CVD in CKD & ESRD Foley RN et al, AJKD 1998; 32(suppl 3):S112-9
Gender-Adjustment and Cutoff Values of Cornell Product in Hypertensive Japanese Patients
 CLINICAL STUDY Gender-Adjustment and Cutoff Values of Cornell Product in Hypertensive Japanese Patients Joji Ishikawa, 1 MD, Yuko Yamanaka, 2 MD, Ayumi Toba, 1 MD, Shintaro Watanabe, 3 MD and Kazumasa
CLINICAL STUDY Gender-Adjustment and Cutoff Values of Cornell Product in Hypertensive Japanese Patients Joji Ishikawa, 1 MD, Yuko Yamanaka, 2 MD, Ayumi Toba, 1 MD, Shintaro Watanabe, 3 MD and Kazumasa
HTA ET DIALYSE DR ALAIN GUERIN
 HTA ET DIALYSE DR ALAIN GUERIN Cardiovascular Disease Mortality General Population vs ESRD Dialysis Patients 100 Annual CVD Mortality (%) 10 1 0.1 0.01 0.001 25-34 35-44 45-54 55-64 66-74 75-84 >85 Age
HTA ET DIALYSE DR ALAIN GUERIN Cardiovascular Disease Mortality General Population vs ESRD Dialysis Patients 100 Annual CVD Mortality (%) 10 1 0.1 0.01 0.001 25-34 35-44 45-54 55-64 66-74 75-84 >85 Age
Brachial artery hyperaemic blood flow velocity and left ventricular geometry
 (2011), 1 5 & 2011 Macmillan Publishers Limited All rights reserved 0950-9240/11 www.nature.com/jhh ORIGINAL ARTICLE Brachial artery hyperaemic blood flow velocity and left ventricular geometry SJ Järhult,
(2011), 1 5 & 2011 Macmillan Publishers Limited All rights reserved 0950-9240/11 www.nature.com/jhh ORIGINAL ARTICLE Brachial artery hyperaemic blood flow velocity and left ventricular geometry SJ Järhult,
Dr. Dermot Phelan MB BCh BAO PhD European Society of Cardiology 2012
 Relative Apical Sparing of Longitudinal Strain Using 2- Dimensional Speckle-Tracking Echocardiography is Both Sensitive and Specific for the Diagnosis of Cardiac Amyloidosis. Dr. Dermot Phelan MB BCh BAO
Relative Apical Sparing of Longitudinal Strain Using 2- Dimensional Speckle-Tracking Echocardiography is Both Sensitive and Specific for the Diagnosis of Cardiac Amyloidosis. Dr. Dermot Phelan MB BCh BAO
Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient
 Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient The Issue of Primary Prevention of A.Fib. (and Heart Failure) and not the Prevention of Recurrent A.Fib. after Electroconversion
Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient The Issue of Primary Prevention of A.Fib. (and Heart Failure) and not the Prevention of Recurrent A.Fib. after Electroconversion
Coronary artery disease (CAD) risk factors
 risk factors") Background Coronary artery disease (CAD) risk factors CAD Risk factors Hypertension Insulin resistance /diabetes Dyslipidemia Smoking /Obesity Male gender/ Old age Atherosclerosis Arterial stiffness precedes
Background Coronary artery disease (CAD) risk factors CAD Risk factors Hypertension Insulin resistance /diabetes Dyslipidemia Smoking /Obesity Male gender/ Old age Atherosclerosis Arterial stiffness precedes
Martin G. Keane, MD, FASE Temple University School of Medicine
 Martin G. Keane, MD, FASE Temple University School of Medicine Measurement of end-diastolic LV internal diameter (LVIDd) made by properly-oriented M-Mode techniques in the Parasternal Long Axis View (PLAX):
Martin G. Keane, MD, FASE Temple University School of Medicine Measurement of end-diastolic LV internal diameter (LVIDd) made by properly-oriented M-Mode techniques in the Parasternal Long Axis View (PLAX):
Nancy Goldman Cutler, MD Beaumont Children s Hospital Royal Oak, Mi
 Nancy Goldman Cutler, MD Beaumont Children s Hospital Royal Oak, Mi Identify increased LV wall thickness (WT) Understand increased WT in athletes Understand hypertrophic cardiomyopathy (HCM) Enhance understanding
Nancy Goldman Cutler, MD Beaumont Children s Hospital Royal Oak, Mi Identify increased LV wall thickness (WT) Understand increased WT in athletes Understand hypertrophic cardiomyopathy (HCM) Enhance understanding
In Vivo Animal Models of Heart Disease. Why Animal Models of Disease? Timothy A Hacker, PhD Department of Medicine University of Wisconsin-Madison
 In Vivo Animal Models of Heart Disease Timothy A Hacker, PhD Department of Medicine University of Wisconsin-Madison Why Animal Models of Disease? Heart Failure (HF) Leading cause of morbidity and mortality
In Vivo Animal Models of Heart Disease Timothy A Hacker, PhD Department of Medicine University of Wisconsin-Madison Why Animal Models of Disease? Heart Failure (HF) Leading cause of morbidity and mortality
Heart Failure in Women: Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre
 Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
Does the reduction in systolic blood pressure alone explain the regression of left ventricular hypertrophy?
 (24) 18, S23 S28 & 24 Nature Publishing Group All rights reserved 95-92/4 $3. www.nature.com/jhh ORIGINAL ARTICLE Does the reduction in systolic blood pressure alone explain the regression of left ventricular
(24) 18, S23 S28 & 24 Nature Publishing Group All rights reserved 95-92/4 $3. www.nature.com/jhh ORIGINAL ARTICLE Does the reduction in systolic blood pressure alone explain the regression of left ventricular
Individual Study Table Referring to Part of Dossier: Volume: Page:
 Synopsis Abbott Laboratories Name of Study Drug: Paricalcitol Capsules (ABT-358) (Zemplar ) Name of Active Ingredient: Paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For
Synopsis Abbott Laboratories Name of Study Drug: Paricalcitol Capsules (ABT-358) (Zemplar ) Name of Active Ingredient: Paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For
Prospective Study of the Changes in Left Ventricular Mass and Geometry Patterns in Hypertensive Patients During 5 Years of Follow-up
 Circ J 2005; 69: 1374 1379 Prospective Study of the Changes in Left Ventricular Mass and Geometry Patterns in Hypertensive Patients During 5 Years of Follow-up Alexandra O. Conrady, MD; Oleg G. Rudomanov,
Circ J 2005; 69: 1374 1379 Prospective Study of the Changes in Left Ventricular Mass and Geometry Patterns in Hypertensive Patients During 5 Years of Follow-up Alexandra O. Conrady, MD; Oleg G. Rudomanov,
Regression of Electrocardiographic Left Ventricular Hypertrophy by Losartan Versus Atenolol
 Regression of Electrocardiographic Left Ventricular Hypertrophy by Losartan Versus Atenolol The Losartan Intervention For Endpoint reduction in hypertension (LIFE) Study Peter M. Okin, MD; Richard B. Devereux,
Regression of Electrocardiographic Left Ventricular Hypertrophy by Losartan Versus Atenolol The Losartan Intervention For Endpoint reduction in hypertension (LIFE) Study Peter M. Okin, MD; Richard B. Devereux,
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION
 LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
Ref 1. Ref 2. Ref 3. Ref 4. See graph
 Ref 1 Ref 2 Ref 3 1. Ages 6-23 y/o 2. Significant LVM differences by gender 3. For males 95 th percentiles: a. LVM/BSA = 103 b. LVM/height = 100 4. For females 95 th percentiles: a. LVM/BSA = 84 b. LVM/height
Ref 1 Ref 2 Ref 3 1. Ages 6-23 y/o 2. Significant LVM differences by gender 3. For males 95 th percentiles: a. LVM/BSA = 103 b. LVM/height = 100 4. For females 95 th percentiles: a. LVM/BSA = 84 b. LVM/height
Imaging in Heart Failure: A Multimodality Approach. Thomas Ryan, MD
 Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
Clinical Investigations
 Clinical Investigations Echocardiographic Serial Changes of Hypertensive Cardiomyopathy With Severely Reduced Ejection Fraction: Comparison With Idiopathic Dilated Cardiomyopathy Address for correspondence:
Clinical Investigations Echocardiographic Serial Changes of Hypertensive Cardiomyopathy With Severely Reduced Ejection Fraction: Comparison With Idiopathic Dilated Cardiomyopathy Address for correspondence:
Chamber Quantitation Guidelines: What is New?
 Chamber Quantitation Guidelines: What is New? Roberto M Lang, MD J AM Soc Echocardiogr 2005; 18:1440-1463 1 Approximately 10,000 citations iase in itune Cardiac Chamber Quantification: What is New? Database
Chamber Quantitation Guidelines: What is New? Roberto M Lang, MD J AM Soc Echocardiogr 2005; 18:1440-1463 1 Approximately 10,000 citations iase in itune Cardiac Chamber Quantification: What is New? Database
Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling. What is the pathophysiology at presentation?
 Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling What is the pathophysiology at presentation? Ventricular-arterial coupling elastance Central arterial pressure
Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling What is the pathophysiology at presentation? Ventricular-arterial coupling elastance Central arterial pressure
Hypertensive heart disease and failure
 Hypertensive heart disease and failure Prof. Dr. Alan Fraser Cardiff University The heart in hypertension Pathophysiology of LV adaptation Regional development of hypertrophy Stress testing - inducible
Hypertensive heart disease and failure Prof. Dr. Alan Fraser Cardiff University The heart in hypertension Pathophysiology of LV adaptation Regional development of hypertrophy Stress testing - inducible
Effects of Renin-Angiotensin System blockade on arterial stiffness and function. Gérard M. LONDON Manhès Hospital Paris, France
 Effects of Renin-Angiotensin System blockade on arterial stiffness and function Gérard M. LONDON Manhès Hospital Paris, France Determinants of vascular overload (afterload) on the heart Peripheral Resistance
Effects of Renin-Angiotensin System blockade on arterial stiffness and function Gérard M. LONDON Manhès Hospital Paris, France Determinants of vascular overload (afterload) on the heart Peripheral Resistance
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Heart Failure with Preserved Ejection Fraction: Mechanisms and Management
 Heart Failure with Preserved Ejection Fraction: Mechanisms and Management Jay N. Cohn, M.D. Professor of Medicine Director, Rasmussen Center for Cardiovascular Disease Prevention University of Minnesota
Heart Failure with Preserved Ejection Fraction: Mechanisms and Management Jay N. Cohn, M.D. Professor of Medicine Director, Rasmussen Center for Cardiovascular Disease Prevention University of Minnesota
How does the heart pump? From sarcomere to ejection volume
 How does the heart pump? From sarcomere to ejection volume Piet Claus Cardiovascular Imaging and Dynamics Department of Cardiovascular Diseases University Leuven, Leuven, Belgium Course on deformation
How does the heart pump? From sarcomere to ejection volume Piet Claus Cardiovascular Imaging and Dynamics Department of Cardiovascular Diseases University Leuven, Leuven, Belgium Course on deformation
DIASTOLIC HEART FAILURE
 DIASTOLIC HEART FAILURE M Mohsen Ibrahim, MD Alexandria, Proposed Criteria for Diastolic Heart Failure ESC Working Group (EHJ 1998) CHF signs/symptoms EF 45% Hemodynamic or echo evidence of diastolic dysfunction
DIASTOLIC HEART FAILURE M Mohsen Ibrahim, MD Alexandria, Proposed Criteria for Diastolic Heart Failure ESC Working Group (EHJ 1998) CHF signs/symptoms EF 45% Hemodynamic or echo evidence of diastolic dysfunction
Central Pressures and Prehypertension
 Central Pressures and Prehypertension Charalambos Vlachopoulos Associate Professor of Cardiology 1 st Cardiology Dept Athens Medical School Central Pressures and Prehypertension Charalambos Vlachopoulos
Central Pressures and Prehypertension Charalambos Vlachopoulos Associate Professor of Cardiology 1 st Cardiology Dept Athens Medical School Central Pressures and Prehypertension Charalambos Vlachopoulos
Which method is better to measure arterial stiffness; augmentation index, pulse wave velocity, carotid distensibility? 전북의대내과 김원호
 Which method is better to measure arterial stiffness; augmentation index, pulse wave velocity, carotid distensibility? 전북의대내과 김원호 Arterial stiffness Arterial stiffness is inversely related to arterial
Which method is better to measure arterial stiffness; augmentation index, pulse wave velocity, carotid distensibility? 전북의대내과 김원호 Arterial stiffness Arterial stiffness is inversely related to arterial
Η σημασία της αρτηριακής σκληρίας στην εκτίμηση της διαστολικής δυσλειτουργίας στην υπέρταση. Θεραπευτικές παρεμβάσεις
 Η σημασία της αρτηριακής σκληρίας στην εκτίμηση της διαστολικής δυσλειτουργίας στην υπέρταση. Θεραπευτικές παρεμβάσεις Ελένη Τριανταφυλλίδη Επιμελήτρια Α Β Πανεπιστημιακή Καρδιολογική Κλινική Αττικό Νοσοκομείο
Η σημασία της αρτηριακής σκληρίας στην εκτίμηση της διαστολικής δυσλειτουργίας στην υπέρταση. Θεραπευτικές παρεμβάσεις Ελένη Τριανταφυλλίδη Επιμελήτρια Α Β Πανεπιστημιακή Καρδιολογική Κλινική Αττικό Νοσοκομείο
DIFFERENTE RELAZIONE TRA VALORI PRESSORI E MASSA VENTRICOLARE SX NEI DUE SESSI IN PAZIENTI IPERTESI.
 DIFFERENTE RELAZIONE TRA VALORI PRESSORI E MASSA VENTRICOLARE SX NEI DUE SESSI IN PAZIENTI IPERTESI. Franco Cipollini, Carlo Porta, Enrica Arcangeli, Carla Breschi, & Giuseppe Seghieri Azienda USL 3, Ambulatorio
DIFFERENTE RELAZIONE TRA VALORI PRESSORI E MASSA VENTRICOLARE SX NEI DUE SESSI IN PAZIENTI IPERTESI. Franco Cipollini, Carlo Porta, Enrica Arcangeli, Carla Breschi, & Giuseppe Seghieri Azienda USL 3, Ambulatorio
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Quantification of Cardiac Chamber Size
 2017 KSE 2017-11-25 Quantification of Cardiac Chamber Size Division of Cardiology Keimyung University Dongsan Medical Center In-Cheol Kim M.D., Ph.D. LV size and function Internal linear dimensions PLX
2017 KSE 2017-11-25 Quantification of Cardiac Chamber Size Division of Cardiology Keimyung University Dongsan Medical Center In-Cheol Kim M.D., Ph.D. LV size and function Internal linear dimensions PLX
Echocardiographic Correlates of Pulmonary Artery Systolic Pressure
 Echocardiographic Correlates of Pulmonary Artery Systolic Pressure The Role of Left Ventricular Diastolic Function Yoram Agmon MD, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc, Izhak Kehat
Echocardiographic Correlates of Pulmonary Artery Systolic Pressure The Role of Left Ventricular Diastolic Function Yoram Agmon MD, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc, Izhak Kehat
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)
of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)") Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Introduction. In Jeong Cho, MD, Wook Bum Pyun, MD and Gil Ja Shin, MD ABSTRACT
 ORIGINAL ARTICLE DOI 10.4070 / kcj.2009.39.4.145 Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright c 2009 The Korean Society of Cardiology The Influence of the Left Ventricular Geometry on the Left
ORIGINAL ARTICLE DOI 10.4070 / kcj.2009.39.4.145 Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright c 2009 The Korean Society of Cardiology The Influence of the Left Ventricular Geometry on the Left
Internet Journal of Medical Update, Vol. 3, No. 2, Jul-Dec 2008
 Evaluation of left ventricular structures in normotensive and hypertensive subjects by two-dimensional echocardiography: Anthropometric correlates in hypertension Mr. Ugwu Anthony Chukwuka * MSc, Mr. Okwor
Evaluation of left ventricular structures in normotensive and hypertensive subjects by two-dimensional echocardiography: Anthropometric correlates in hypertension Mr. Ugwu Anthony Chukwuka * MSc, Mr. Okwor
Diastolic Heart Failure (HFpEF) Felix J. Rogers, DO, FACOI April 29, 2018
 Felix J. Rogers, DO, FACOI April 29, 2018") Diastolic Heart Failure (HFpEF) Felix J. Rogers, DO, FACOI April 29, 2018 Case presentation MSO, an 81 year old woman was admitted to HFWH because of progressive dyspnea and difficult to control hypertension
Diastolic Heart Failure (HFpEF) Felix J. Rogers, DO, FACOI April 29, 2018 Case presentation MSO, an 81 year old woman was admitted to HFWH because of progressive dyspnea and difficult to control hypertension
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Relevance of sympathetic overactivity in hypertension and heart failure Therapeutic Implications
 Relevance of sympathetic overactivity in hypertension and heart failure Therapeutic Implications Uta C. Hoppe, MD, FESC Dep. of Internal Medicine II Paracelsus University Salzburg Austria Disclosures Within
Relevance of sympathetic overactivity in hypertension and heart failure Therapeutic Implications Uta C. Hoppe, MD, FESC Dep. of Internal Medicine II Paracelsus University Salzburg Austria Disclosures Within
Diastolic Dysfunction: Hypertension to Hypertrophy to Heart Failure
 Diastolic Dysfunction: Hypertension to Hypertrophy to Heart Failure Dr. Shelley Zieroth FRCPC Assistant Professor, Cardiology, University of Manitoba Director of Cardiac Transplant and Heart Failure Clinics
Diastolic Dysfunction: Hypertension to Hypertrophy to Heart Failure Dr. Shelley Zieroth FRCPC Assistant Professor, Cardiology, University of Manitoba Director of Cardiac Transplant and Heart Failure Clinics
Left ventricular hypertrophy: why does it happen?
 Nephrol Dial Transplant (2003) 18 [Suppl 8]: viii2 viii6 DOI: 10.1093/ndt/gfg1083 Left ventricular hypertrophy: why does it happen? Gerard M. London Department of Nephrology and Dialysis, Manhes Hospital,
Nephrol Dial Transplant (2003) 18 [Suppl 8]: viii2 viii6 DOI: 10.1093/ndt/gfg1083 Left ventricular hypertrophy: why does it happen? Gerard M. London Department of Nephrology and Dialysis, Manhes Hospital,
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
THE DIASTOLIC STRESS TEST: A NEW CLINICAL TOOL? THE CONCEPT OF DIASTOLIC RESERVE
 Thierry C. Gillebert University of Ghent ESC Education Committee THE DIASTOLIC STRESS TEST: A NEW CLINICAL TOOL? THE CONCEPT OF DIASTOLIC RESERVE 1 Case: Ann, 63 years Suffered from metabolic syndrome
Thierry C. Gillebert University of Ghent ESC Education Committee THE DIASTOLIC STRESS TEST: A NEW CLINICAL TOOL? THE CONCEPT OF DIASTOLIC RESERVE 1 Case: Ann, 63 years Suffered from metabolic syndrome
Cardiovascular Imaging Endpoints in Oncology Clinical Trials
 Cardiovascular Imaging Endpoints in Oncology Clinical Trials Bonnie Ky, MD, MSCE Assistant Professor of Medicine and Epidemiology Director, Penn Cardio-Oncology Center of Excellence Director, Penn Center
Cardiovascular Imaging Endpoints in Oncology Clinical Trials Bonnie Ky, MD, MSCE Assistant Professor of Medicine and Epidemiology Director, Penn Cardio-Oncology Center of Excellence Director, Penn Center
Table of Contents RECOMMENDATION PAPER
 European Heart Journal Cardiovascular Imaging (2015) 16, 577 605 doi:10.1093/ehjci/jev076 RECOMMENDATION PAPER Recommendations on the use of echocardiography in adult hypertension: a report from the European
European Heart Journal Cardiovascular Imaging (2015) 16, 577 605 doi:10.1093/ehjci/jev076 RECOMMENDATION PAPER Recommendations on the use of echocardiography in adult hypertension: a report from the European
Left ventricular mass in offspring of hypertensive parents: does it predict the future?
 ISPUB.COM The Internet Journal of Cardiovascular Research Volume 7 Number 1 Left ventricular mass in offspring of hypertensive parents: does it predict the future? P Jaiswal, S Mahajan, S Diwan, S Acharya,
ISPUB.COM The Internet Journal of Cardiovascular Research Volume 7 Number 1 Left ventricular mass in offspring of hypertensive parents: does it predict the future? P Jaiswal, S Mahajan, S Diwan, S Acharya,
Left atrial function. Aliakbar Arvandi MD
 In the clinic Left atrial function Abstract The left atrium (LA) is a left posterior cardiac chamber which is located adjacent to the esophagus. It is separated from the right atrium by the inter-atrial
In the clinic Left atrial function Abstract The left atrium (LA) is a left posterior cardiac chamber which is located adjacent to the esophagus. It is separated from the right atrium by the inter-atrial
Body Mass Index and Blood Pressure Influences on Left Ventricular Mass and Geometry in African Americans
 Body Mass Index and Blood Pressure Influences on Left Ventricular Mass and Geometry in African Americans The Atherosclerotic Risk In Communities (ARIC) Study Ervin Fox, Herman Taylor, Michael Andrew, Hui
Body Mass Index and Blood Pressure Influences on Left Ventricular Mass and Geometry in African Americans The Atherosclerotic Risk In Communities (ARIC) Study Ervin Fox, Herman Taylor, Michael Andrew, Hui
Early Detection of Damaged Organ
 Early Detection of Damaged Organ Regional Cardiovascular Center, Chungbuk National University Kyung-Kuk Hwang Contents NICE guideline 2011 - Confirm the diagnosis of HT ambulatory blood pressure monitoring
Early Detection of Damaged Organ Regional Cardiovascular Center, Chungbuk National University Kyung-Kuk Hwang Contents NICE guideline 2011 - Confirm the diagnosis of HT ambulatory blood pressure monitoring
HIGHLIGHT SESSION. Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips
 Disclosures: Speaker Philips") Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
Impact of Echocardiographic Left Ventricular Geometry on Clinical Prognosis
 Accepted Manuscript Impact of Echocardiographic Left Ventricular Geometry on Clinical Prognosis Carl J. Lavie, Dharmendrakumar A. Patel, Richard V. Milani, Hector O. Ventura, Sangeeta Shah, Yvonne Gilliland
Accepted Manuscript Impact of Echocardiographic Left Ventricular Geometry on Clinical Prognosis Carl J. Lavie, Dharmendrakumar A. Patel, Richard V. Milani, Hector O. Ventura, Sangeeta Shah, Yvonne Gilliland
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES
 CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES C. Liakos, 1 G. Vyssoulis, 1 E. Karpanou, 2 S-M. Kyvelou, 1 V. Tzamou, 1 A. Michaelides, 1 A. Triantafyllou, 1 P. Spanos, 1 C. Stefanadis
CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES C. Liakos, 1 G. Vyssoulis, 1 E. Karpanou, 2 S-M. Kyvelou, 1 V. Tzamou, 1 A. Michaelides, 1 A. Triantafyllou, 1 P. Spanos, 1 C. Stefanadis
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
Little is known about the degree and time course of
 Differential Changes in Regional Right Ventricular Function Before and After a Bilateral Lung Transplantation: An Ultrasonic Strain and Strain Rate Study Virginija Dambrauskaite, MD, Lieven Herbots, MD,
Differential Changes in Regional Right Ventricular Function Before and After a Bilateral Lung Transplantation: An Ultrasonic Strain and Strain Rate Study Virginija Dambrauskaite, MD, Lieven Herbots, MD,
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Left Ventricular Hypertrophy New Insights
 Left Ventricular Hypertrophy New Insights Athanasios J. Manolis MD, FACC, FESC, FAHA Director of Cardiology Dept, Asklepeion General Hospital, Athens Greece Overview Introduction and Factors promoting
Left Ventricular Hypertrophy New Insights Athanasios J. Manolis MD, FACC, FESC, FAHA Director of Cardiology Dept, Asklepeion General Hospital, Athens Greece Overview Introduction and Factors promoting
Importance of Ambulatory Blood Pressure Monitoring in Adolescents
 Importance of Ambulatory Blood Pressure Monitoring in Adolescents Josep Redon, MD, PhD, FAHA Internal Medicine Hospital Clinico Universitario de Valencia University of Valencia CIBERObn Instituto de Salud
Importance of Ambulatory Blood Pressure Monitoring in Adolescents Josep Redon, MD, PhD, FAHA Internal Medicine Hospital Clinico Universitario de Valencia University of Valencia CIBERObn Instituto de Salud
How clinically important are the results of the large trials in hypertension?
 How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
The Athlete s Heart. Role of Echo. Neil J. Weissman, MD MedStar Health Research Institute & Professor of Medicine Georgetown University
 The Athlete s Heart Role of Echo Neil J. Weissman, MD MedStar Health Research Institute & Professor of Medicine Georgetown University Washington, D.C. Disclosures Grant support (to institution) for Core
The Athlete s Heart Role of Echo Neil J. Weissman, MD MedStar Health Research Institute & Professor of Medicine Georgetown University Washington, D.C. Disclosures Grant support (to institution) for Core
Impedance Cardiography (ICG) Application of ICG for Hypertension Management
 Application of ICG for Hypertension Management") Application of ICG for Hypertension Management 1mA @ 100 khz Impedance Cardiography (ICG) Non-invasive Beat-to-beat Hemodynamic Monitoring Diastole Systole Aortic valve is closed No blood flow in the aorta
Application of ICG for Hypertension Management 1mA @ 100 khz Impedance Cardiography (ICG) Non-invasive Beat-to-beat Hemodynamic Monitoring Diastole Systole Aortic valve is closed No blood flow in the aorta
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Υπέρταση στις γυναίκες
 Υπέρταση στις γυναίκες Ελένη Τριανταφυλλίδη Διευθύντρια ΕΣΥ Καρδιολογίας Υπεύθυνη Αντιυπερτασικού Ιατρείου Β Πανεπιστημιακή Καρδιολογική Κλινική Νοσοκομείο ΑΤΤΙΚΟΝ Cardiovascular disease is the Europe
Υπέρταση στις γυναίκες Ελένη Τριανταφυλλίδη Διευθύντρια ΕΣΥ Καρδιολογίας Υπεύθυνη Αντιυπερτασικού Ιατρείου Β Πανεπιστημιακή Καρδιολογική Κλινική Νοσοκομείο ΑΤΤΙΚΟΝ Cardiovascular disease is the Europe
Cardiac Care in pa+ents with Duchenne muscular dystrophy
 Cardiac Care in pa+ents with Duchenne muscular dystrophy Linda Cripe, M.D. Professor of Pediatrics The Heart Center.... Why are cardiologists interested in patients with Duchenne muscular dystrophy?....
Cardiac Care in pa+ents with Duchenne muscular dystrophy Linda Cripe, M.D. Professor of Pediatrics The Heart Center.... Why are cardiologists interested in patients with Duchenne muscular dystrophy?....
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality
 Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
3/27/2014. Introduction.
 Introduction. Myocardial perfusion & contractility becomes abnormal immediately after the onset of ischaemia, even before the development of the symptoms & ST segment changes. 1 Myocardial Wall Motion
Introduction. Myocardial perfusion & contractility becomes abnormal immediately after the onset of ischaemia, even before the development of the symptoms & ST segment changes. 1 Myocardial Wall Motion
Quantitation of right ventricular dimensions and function
 SCCS Basics of cardiac assessment Quantitation of right ventricular dimensions and function Tomasz Kukulski, MD PhD Dept of Cardiology, Congenital Heart Disease and Electrotherapy Silesian Medical University
SCCS Basics of cardiac assessment Quantitation of right ventricular dimensions and function Tomasz Kukulski, MD PhD Dept of Cardiology, Congenital Heart Disease and Electrotherapy Silesian Medical University
Identifying Changes in Myocardial Microstructure via a Novel Sonographic Imaging Algorithm
 Identifying Changes in Myocardial Microstructure via a Novel Sonographic Imaging Algorithm The Harvard community has made this article openly available. Please share how this access benefits you. Your
Identifying Changes in Myocardial Microstructure via a Novel Sonographic Imaging Algorithm The Harvard community has made this article openly available. Please share how this access benefits you. Your
Is normal ejection fraction equivalent to normal systolic function?
 Is normal ejection fraction equivalent to normal systolic function? D. Vinereanu University of Medicine, Bucharest, Romania EAE course, Bucharest No 2 nd criterion (out of 3) for the diagnosis of HFNEF:
Is normal ejection fraction equivalent to normal systolic function? D. Vinereanu University of Medicine, Bucharest, Romania EAE course, Bucharest No 2 nd criterion (out of 3) for the diagnosis of HFNEF:
Strain Imaging: Myocardial Mechanics Simplified and Applied
 9/28/217 Strain Imaging: Myocardial Mechanics Simplified and Applied John Gorcsan III, MD Professor of Medicine Director of Clinical Research Division of Cardiology VECTORS OF CONTRACTION Shortening Thickening
9/28/217 Strain Imaging: Myocardial Mechanics Simplified and Applied John Gorcsan III, MD Professor of Medicine Director of Clinical Research Division of Cardiology VECTORS OF CONTRACTION Shortening Thickening
Highlights from EuroEcho 2009 Echo in cardiomyopathies
 Highlights from EuroEcho 2009 Echo in cardiomyopathies Bogdan A. Popescu University of Medicine and Pharmacy, Bucharest, Romania ESC Congress 2010 Hypertrophic cardiomyopathy To determine the differences
Highlights from EuroEcho 2009 Echo in cardiomyopathies Bogdan A. Popescu University of Medicine and Pharmacy, Bucharest, Romania ESC Congress 2010 Hypertrophic cardiomyopathy To determine the differences
Prevalence of left ventricular hypertrophy in a hypertensive population
 European Heart Journal (1996) 17, 143-149 Prevalence of left ventricular hypertrophy in a hypertensive population J. Tingleff, M. Munch, T. J. Jakobsen, C. Torp-Pedersen, M. E. Olsen, K. H. Jensen, T.
European Heart Journal (1996) 17, 143-149 Prevalence of left ventricular hypertrophy in a hypertensive population J. Tingleff, M. Munch, T. J. Jakobsen, C. Torp-Pedersen, M. E. Olsen, K. H. Jensen, T.
Endurance Exercise and Cardiovascular Health
 Endurance Exercise and Cardiovascular Health Professor Sanjay Sharma St George s University of London St George s Hospital NHS Trust sasharma@sgul.ac.uk @SSharmacardio Conflicts/Disclosures: None Objectives
Endurance Exercise and Cardiovascular Health Professor Sanjay Sharma St George s University of London St George s Hospital NHS Trust sasharma@sgul.ac.uk @SSharmacardio Conflicts/Disclosures: None Objectives
Should all patients with hypertension have echocardiography?
 (2000) 14, 417 421 2000 Macmillan Publishers Ltd All rights reserved 0950-9240/00 $15.00 www.nature.com/jhh REVIEW ARTICLE Should all patients with hypertension have echocardiography? G de Simone 1,2,
(2000) 14, 417 421 2000 Macmillan Publishers Ltd All rights reserved 0950-9240/00 $15.00 www.nature.com/jhh REVIEW ARTICLE Should all patients with hypertension have echocardiography? G de Simone 1,2,
Diagnosis is it really Heart Failure?
 ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
Exercise Testing/Echocardiography in Asymptomatic AS
 Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Cardiac Magnetic Resonance in pregnant women
 Cardiac Magnetic Resonance in pregnant women Chen SSM, Leeton L, Dennis AT Royal Women s Hospital and The University of Melbourne, Parkville, Australia alicia.dennis@thewomens.org.au Quantification of
Cardiac Magnetic Resonance in pregnant women Chen SSM, Leeton L, Dennis AT Royal Women s Hospital and The University of Melbourne, Parkville, Australia alicia.dennis@thewomens.org.au Quantification of
Influence of RAAS inhibition on outflow tract obstruction in hypertrophic cardiomyopathy
 ORIGINAL ARTICLE 5 RAAS inhibitors should be avoided if possible in patients with obstructive HCM Influence of RAAS inhibition on outflow tract obstruction in hypertrophic cardiomyopathy Katrin Witzel,
ORIGINAL ARTICLE 5 RAAS inhibitors should be avoided if possible in patients with obstructive HCM Influence of RAAS inhibition on outflow tract obstruction in hypertrophic cardiomyopathy Katrin Witzel,
Diastolic Heart Failure Uri Elkayam, MD
 Diastolic Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu Diastolic Heart Failure Clinical Definition A
Diastolic Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu Diastolic Heart Failure Clinical Definition A
Athlete s Heart: Clinical Relevance. Athlete's Heart vs. Cardiac Pathology Clinical Approaches. Echo Florida Conflicts of Interest: None
 Athlete's Heart vs. Cardiac Pathology Clinical Approaches Echo Florida 2012 Aaron L. Baggish MD Cardiovascular Performance Program Cardiac Ultrasound Laboratory Division of Cardiology Massachusetts General
Athlete's Heart vs. Cardiac Pathology Clinical Approaches Echo Florida 2012 Aaron L. Baggish MD Cardiovascular Performance Program Cardiac Ultrasound Laboratory Division of Cardiology Massachusetts General
Hypertension in Aortic Valve Disease
 Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Left ventricular hypertrophy (LVH) carries a substantial
 carries a substantial") New Gender-Specific Partition Values for ECG Criteria of Left Ventricular Hypertrophy Recalibration Against Cardiac MRI Khaled Alfakih, Kevin Walters, Tim Jones, John Ridgway, Alistair S. Hall, Mohan Sivananthan
New Gender-Specific Partition Values for ECG Criteria of Left Ventricular Hypertrophy Recalibration Against Cardiac MRI Khaled Alfakih, Kevin Walters, Tim Jones, John Ridgway, Alistair S. Hall, Mohan Sivananthan
Changes in Blood Pressure and Vascular Physiology: Markers for Cardiovascular Disease
 ...SYMPOSIUM PROCEEDINGS... Changes in Blood Pressure and Vascular Physiology: Markers for Cardiovascular Disease Based on a presentation by Joseph L. Izzo, Jr., MD Presentation Summary Changes in systolic
...SYMPOSIUM PROCEEDINGS... Changes in Blood Pressure and Vascular Physiology: Markers for Cardiovascular Disease Based on a presentation by Joseph L. Izzo, Jr., MD Presentation Summary Changes in systolic
Correlation of novel cardiac marker
 Correlation of novel cardiac marker and mortality in EGAT population. Soluble ST2 hscrp Poh Chanyavanich, MD SukitYamwong, MD Piyamitr Sritara, MD Ramathibodi hospital Background hscrp - the most widely
Correlation of novel cardiac marker and mortality in EGAT population. Soluble ST2 hscrp Poh Chanyavanich, MD SukitYamwong, MD Piyamitr Sritara, MD Ramathibodi hospital Background hscrp - the most widely
Arterial Pressure in CKD5 - ESRD Population Gérard M. London
 Arterial Pressure in CKD5 - ESRD Population Gérard M. London INSERM U970 Paris 150 SBP & DBP by Age, Ethnicity &Gender (US Population Age 18 Years, NHANES III) 150 SBP (mm Hg) 130 110 80 Non-Hispanic Black
Arterial Pressure in CKD5 - ESRD Population Gérard M. London INSERM U970 Paris 150 SBP & DBP by Age, Ethnicity &Gender (US Population Age 18 Years, NHANES III) 150 SBP (mm Hg) 130 110 80 Non-Hispanic Black
Masked Hypertension and Aortic Coarctation: Impact on Ventricular Function and Morphology
 Masked Hypertension and Aortic Coarctation: Impact on Ventricular Function and Morphology Giovanni Di Salvo MD, PhD, MMSc, FESC BACKGROUND MASKED HYPERTENSION Masked hypertension (MH) consists of an elevated
Masked Hypertension and Aortic Coarctation: Impact on Ventricular Function and Morphology Giovanni Di Salvo MD, PhD, MMSc, FESC BACKGROUND MASKED HYPERTENSION Masked hypertension (MH) consists of an elevated
Cardiac Output MCQ. Professor of Cardiovascular Physiology. Cairo University 2007
 Cardiac Output MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 90- Guided by Ohm's law when : a- Cardiac output = 5.6 L/min. b- Systolic and diastolic BP
Cardiac Output MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 90- Guided by Ohm's law when : a- Cardiac output = 5.6 L/min. b- Systolic and diastolic BP
HFPEF Echo with Strain vs. MRI T1 Mapping
 HFPEF Echo with Strain vs. MRI T1 Mapping Erik Schelbert, MD MS Director, Cardiovascular Magnetic Resonance Assistant Professor of Medicine Heart & Vascular Institute University of Pittsburgh Disclosures
HFPEF Echo with Strain vs. MRI T1 Mapping Erik Schelbert, MD MS Director, Cardiovascular Magnetic Resonance Assistant Professor of Medicine Heart & Vascular Institute University of Pittsburgh Disclosures
Age-related changes in cardiovascular system. Dr. Rehab Gwada
 Age-related changes in cardiovascular system Dr. Rehab Gwada Objectives explain the main structural and functional changes in cardiovascular system associated with normal aging Introduction aging results
Age-related changes in cardiovascular system Dr. Rehab Gwada Objectives explain the main structural and functional changes in cardiovascular system associated with normal aging Introduction aging results